Fracture healing by pawan shaw
59
Fracture Healing 2/17/2015 1
Transcript of Fracture healing by pawan shaw
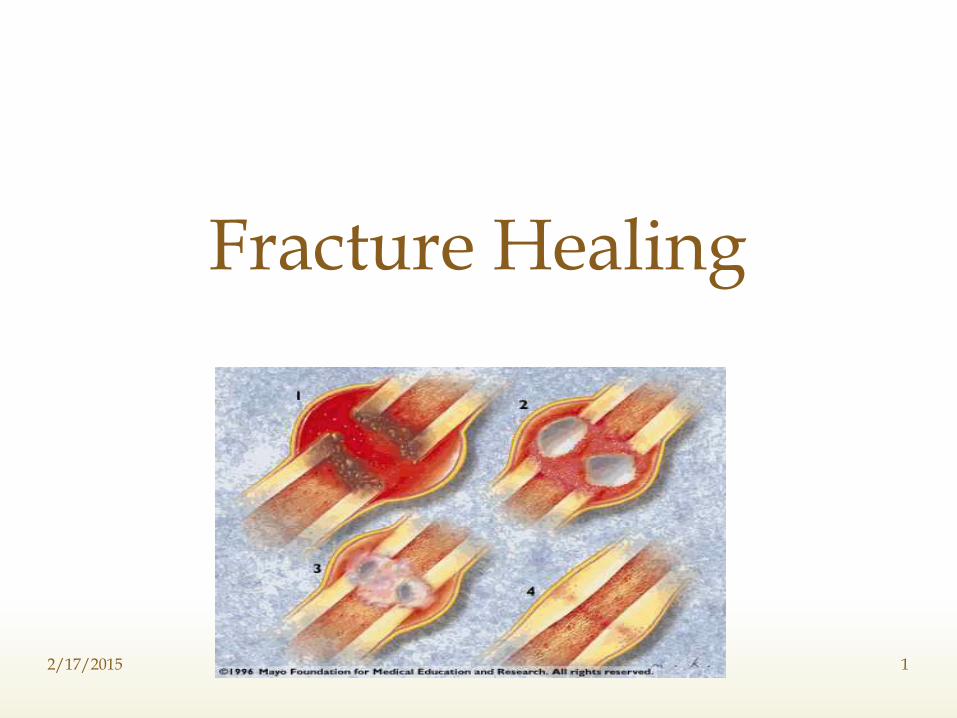
Fracture Healing
2/17/2015 1
Highly vascular , constantly changing mineralised connective tissue.
Consists of cells (osteocytes) and intercellular matrix.
Matrix : Composed of
a) Organic materials (40%) mainly collagen fibres.
b) Inorganic salts rich in calcium and phosphate.
Anatomy of Bone
2/17/2015 2
Bone is made of two components:
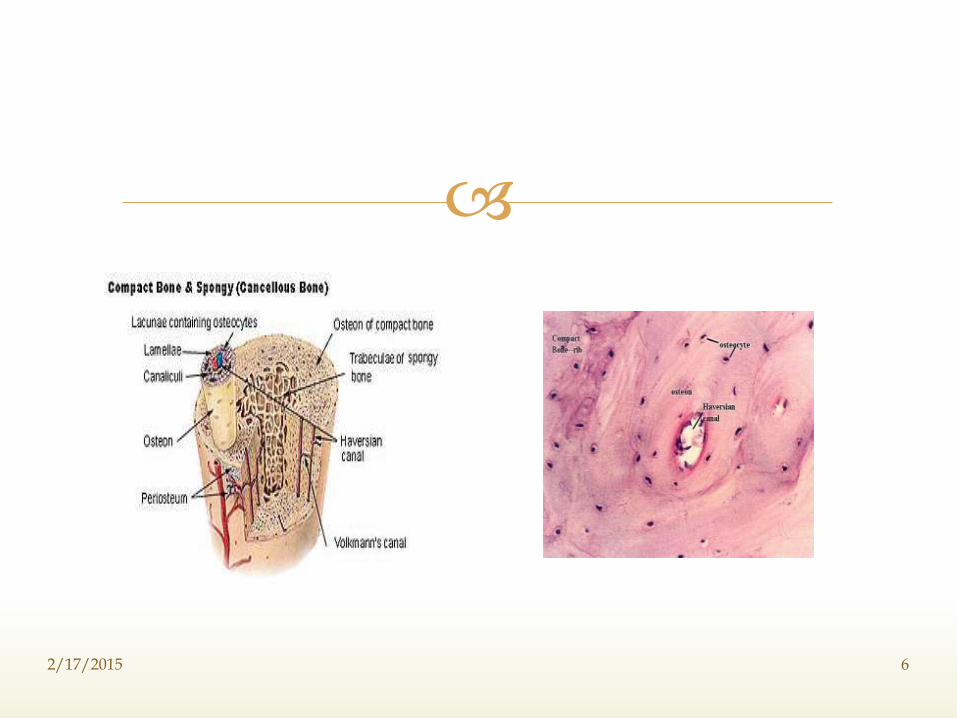
1) Outer dense,compact / cortical bone.
- Forms the outer wall or supporting structures.
- Supreme importance in providing strength.
2) Inner spongiosa / trabecular / cancellous bone
- Forms the inner wall
- Provides additional strength to cortices and support the bone marrow at the end of long bones.
Macroscopically
2/17/2015 3
Two types:-
Woven / Immature bone:-
• Characterised by random arrangement of cells and collagen,associated with period of rapid bone formation,such as initial stage of fracture healing.
Lamellar / Mature bone:-
• Characterised by an orderly cellular distribution and properly oriented collagen fibres. This constitutes organised bone both cortical and cancellous.
Microscopically
2/17/2015 4
Basic architectural unit of lamellar bone.Consists of central Haversian canal which runs longitudinally, is surrounded by concentric lamellar of bony tissue.Numerous lacunae intervene between the lamellae.This lacunae communicate with each other and with central canal by numerous radiating canaliculi.The lacunae are filled with osteocytes and canaliculi contains protoplasmic process of osteocytes and convey outwards the nutritive materials.The haversian canal communicate with medullary cavity and with surface of bone by numerous oblique channels known as Volkmann’s canal which consists of neurovascular bundle.
Osteon/haversian system
2/17/2015 5
2/17/2015 6
Osteoprogenitor cells: (osteogenic/pro-osteoblasts)
• Undifferentiated mesenchymal stem cells• Can differentiate into osteoblast,chondroblast and fibroblast.• Types: 1) Committed 2) Inducible
Osteoblasts:• Basophillic, cuboidal, mononuclear cell.• Derived from marrow stromal cells by differentiation of pre-osteoblasts.• Synthesize major protein of bone- type 1 collagen, osteocalcin and osteonectin.• Control mineralisation of bone by secretion of ALP.• Recent evidence suggest osteoblasts control osteoclastic function by secretion of PG’s and IL-6 and IL-11.
Bone cells
2/17/2015 7
Osteocytes:-
• Derived from osteoblasts,when they get incacerated in the matrix which they secrete and get burried deep within the bone.• Occupy spaces in matrix called as lacunae.• Secrete ALP to maintain calcification.
Osteoclasts:-• Large , multinucleated giant rounded cells.• Numerous mitochondria and lysosomes.• Osteoclasis – help in removing of living bone.• Osteoclastic resorption release bone matrix protein and cytokines which stimulate osteoblast production and bone formation.
Other cells:- Reticular cells, Endosteal cells and Fibroblasts.
Bone cells cont…
2/17/2015 8
Made up of:- a) Outer layer of fibrous and elastic tissue.
b) Inner Cambium layer
Functions:-• Serves as a limiting membrane for bone.
• Outer fibroblast layer provides fibrous attachment to subcutaneous connective tissue,muscles,tendons and ligaments.
• Inner cambium layer contains pools of undifferentiated cells tha support bone formation during embryogenic and post natal growth.
• Helps in fracture healing by forming periosteal callus.
Periosteum
2/17/2015 9
Nutrient artery
Epiphyseal/ metaphyseal arteries
Periosteal arteries
Muscular, ligamentous and capsular arteries.
Blood supply
2/17/2015 10
Fracture Healing
Introduction
Pathology & Stages
Local Factors influencing Osteogenesis
2/17/2015 11
Fracture is a break in the structural continuity of bone.
The healing of fracture is in many ways similiar to the healing in soft tissue wounds except that the end result is mineralised mesenchymal tissue i.e. BONE.
Fracture healing starts as soon as bone breaks and continues modelling for many years
Introduction
2/17/2015 12
Bone is unique in its ability to repair itself.,it can completely reconstitute itself by reactivating processes.
Bone repair is a highly regulated process that can be seperated into overlapping histologic,bio-chemical & bio-mechanical stages.
The completion of each stage initiates the next stage and this is accomplished by a series of interactions and communications among various cells and proteins located in healing zone.
2/17/2015 13
Pathology & Staging
In 1975, Cruess and Dumont proposed that fracture healing may be considered to consist of three overlapping phases: an inflammatory phase, a reparative phase, and a remodeling phase In 1989, FROST proposed the stages of fracture healing
five stages.stage of haematomastage of granulation tissue stage of callusstage of modellingstage of remodelling
2/17/2015 14
The events in the process of fracture healing can be divided into 3 phases.
1. Inflammatory Phase
a) Stage of Haematoma Formation.
b) Granulation tissue formation.
2.Reparative Phase
a) Cartilage callus formation
b) Lamellar bone deposition
3.Remodelling Phase
a) Remodelling to original bone contour
Pathology & Staging
2/17/2015 15
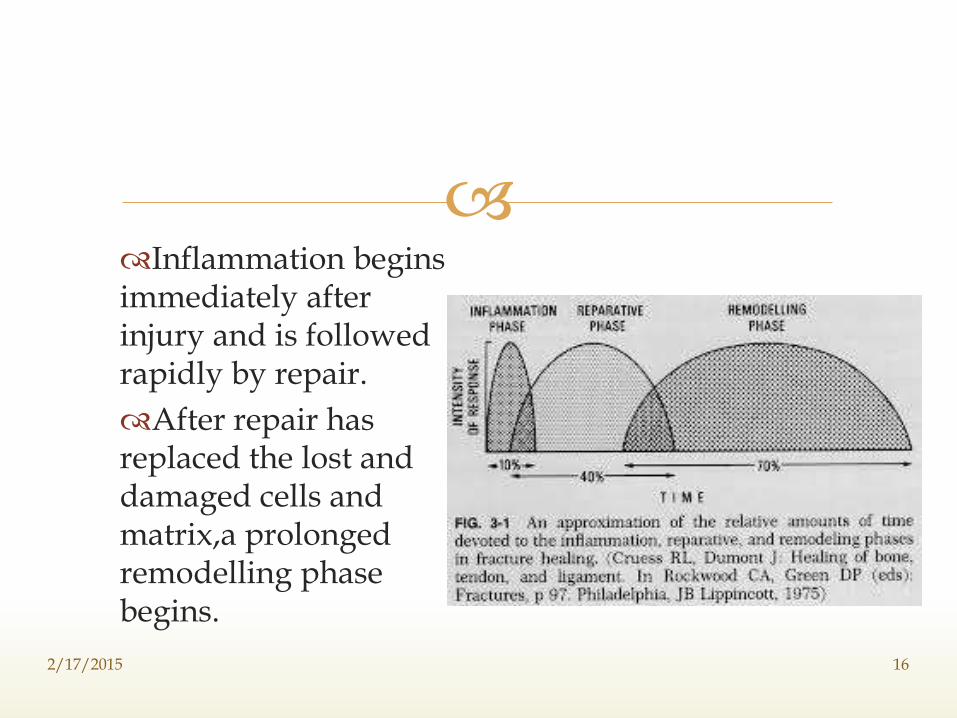
Inflammation begins immediately after injury and is followed rapidly by repair.
After repair has replaced the lost and damaged cells and matrix,a prolonged remodelling phase begins.
2/17/2015 16
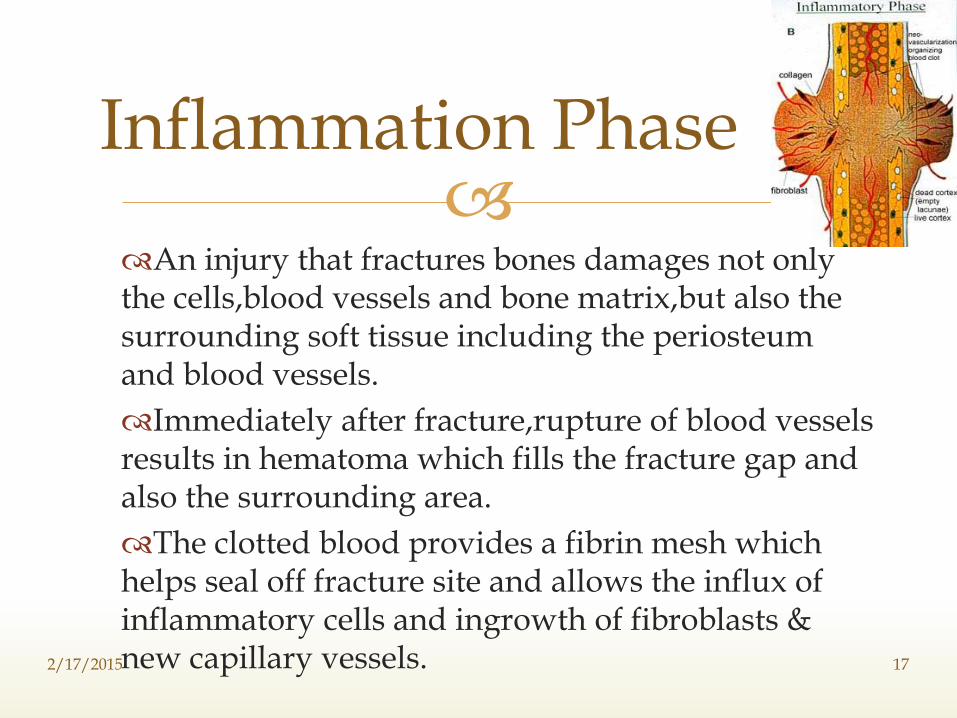
An injury that fractures bones damages not only the cells,blood vessels and bone matrix,but also the surrounding soft tissue including the periosteum and blood vessels.
Immediately after fracture,rupture of blood vessels results in hematoma which fills the fracture gap and also the surrounding area.
The clotted blood provides a fibrin mesh which helps seal off fracture site and allows the influx of inflammatory cells and ingrowth of fibroblasts & new capillary vessels.
Inflammation Phase
2/17/2015 17
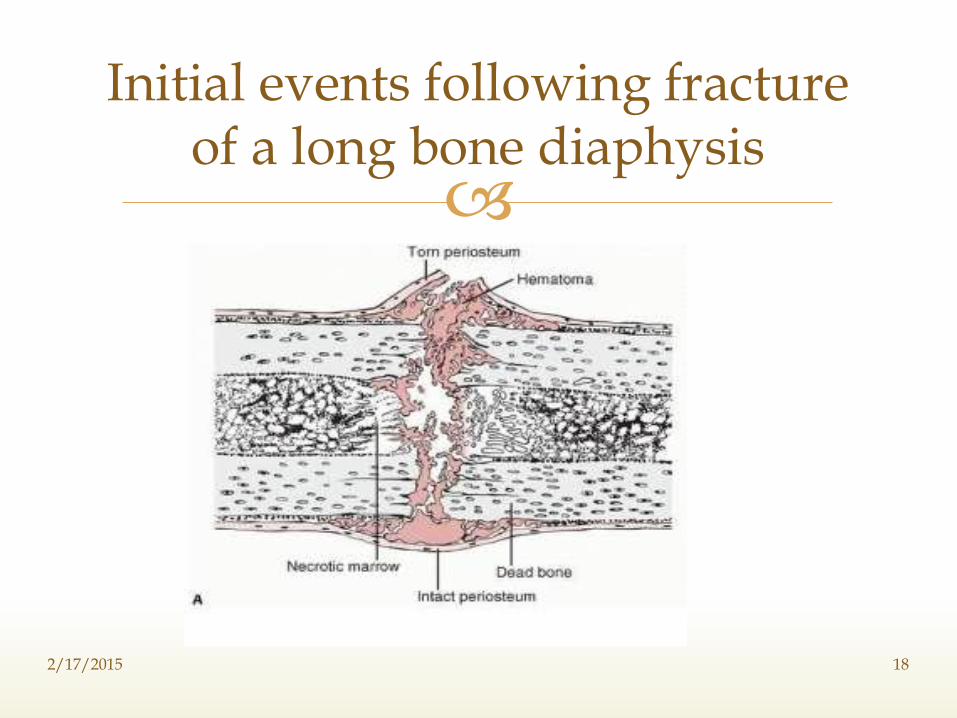
Initial events following fracture of a long bone diaphysis
2/17/2015 18
The degranulated platelets and migrating inflammatory cells release PDGF, TGF-BETA, FGF and other cytokines,which activates the osteoprogenitor cells in the periosteum,medullary cavity,and surrounding soft tissues and stimulate the production of osteoclastic and osteoblastic activity.
Thus by the end of first week,the hematoma is organizing,the adjacent soft tissue is being modulated for future matrix production.
This fusiform & predominantly uncalcified tissue called soft tissue callus or procallus provides some anchorge between ends of fractured bones but offers no structural rigidity for weight bearing.
2/17/2015 19
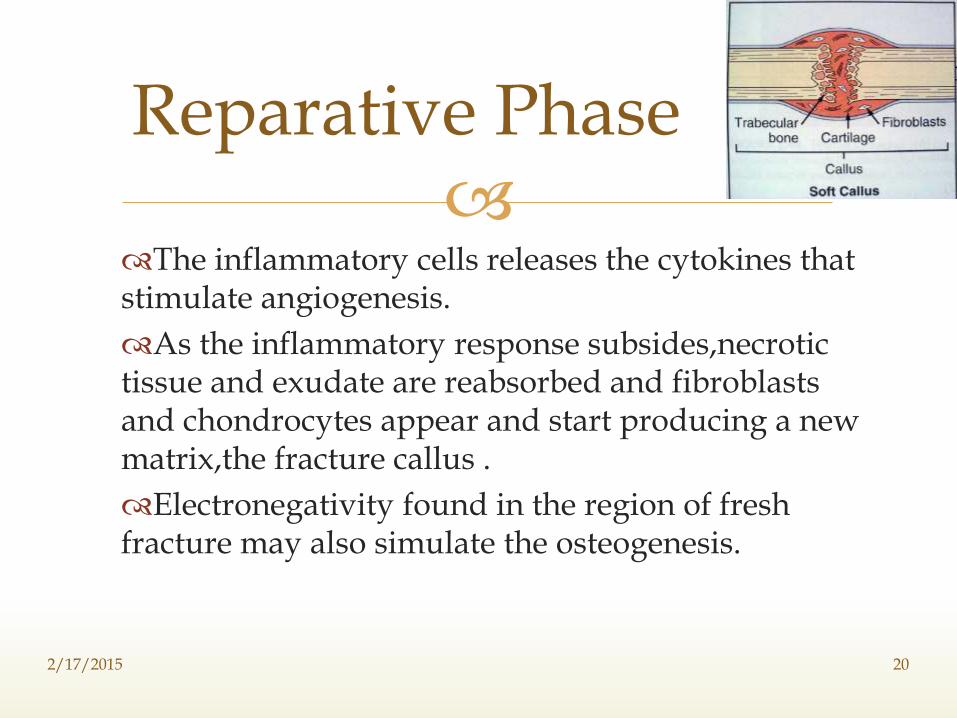
The inflammatory cells releases the cytokines that stimulate angiogenesis.
As the inflammatory response subsides,necrotic tissue and exudate are reabsorbed and fibroblasts and chondrocytes appear and start producing a new matrix,the fracture callus .
Electronegativity found in the region of fresh fracture may also simulate the osteogenesis.
Reparative Phase
2/17/2015 20
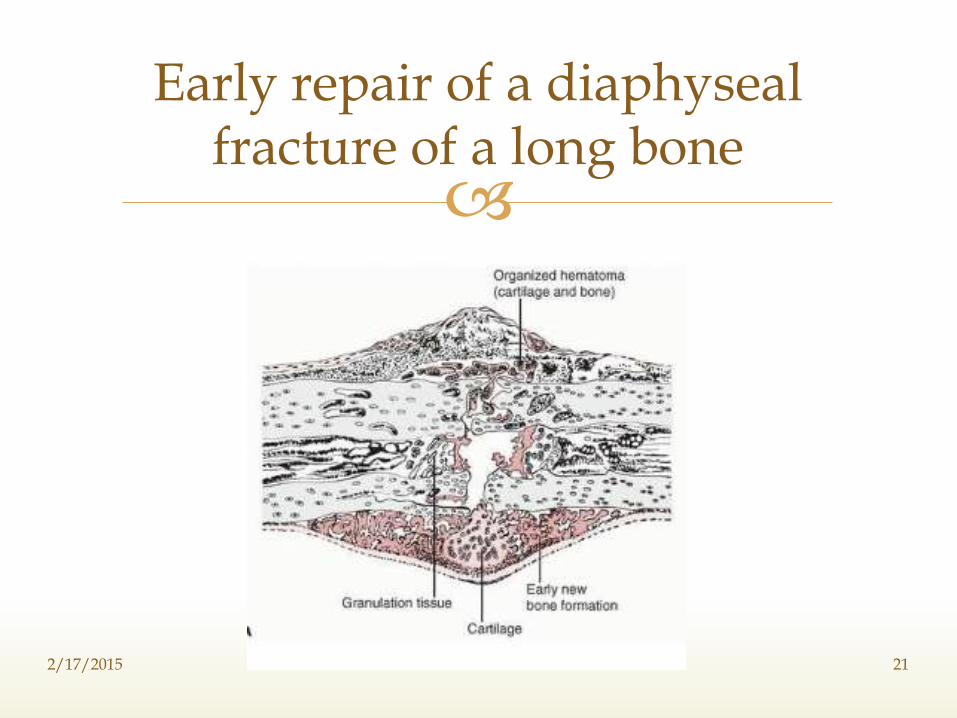
Early repair of a diaphyseal fracture of a long bone
2/17/2015 21
The activated osteoprogenitor cells deposit sub-periosteal trabeculae of woven bone oriented perpendicular to cortical axis and within the medullary cavity.
In some cases the activated mesenchymal cells in soft tissue and bone surrounding the fracture line also differentiate into chondroblasts that make fibrocartilge and hyaline cartilage.
The newly formed cartilage undergoes enchondral ossification forming a network of bone
In this fashion,the fractured ends are bridged by a bony callus and as it mineralizes,the stiffness and strength of callus increase to point where controlled weight bearing can be tolerated.
2/17/2015 22
As the callus matures and transmits weight-bearing forces,the portions that are not physically stressed are reabsorbed,and in this manner the callus is reduced in size until the shape and outline of fractured bone has been reestablished.
The medullary cavity is also restored.
Remodelling Phase
2/17/2015 23
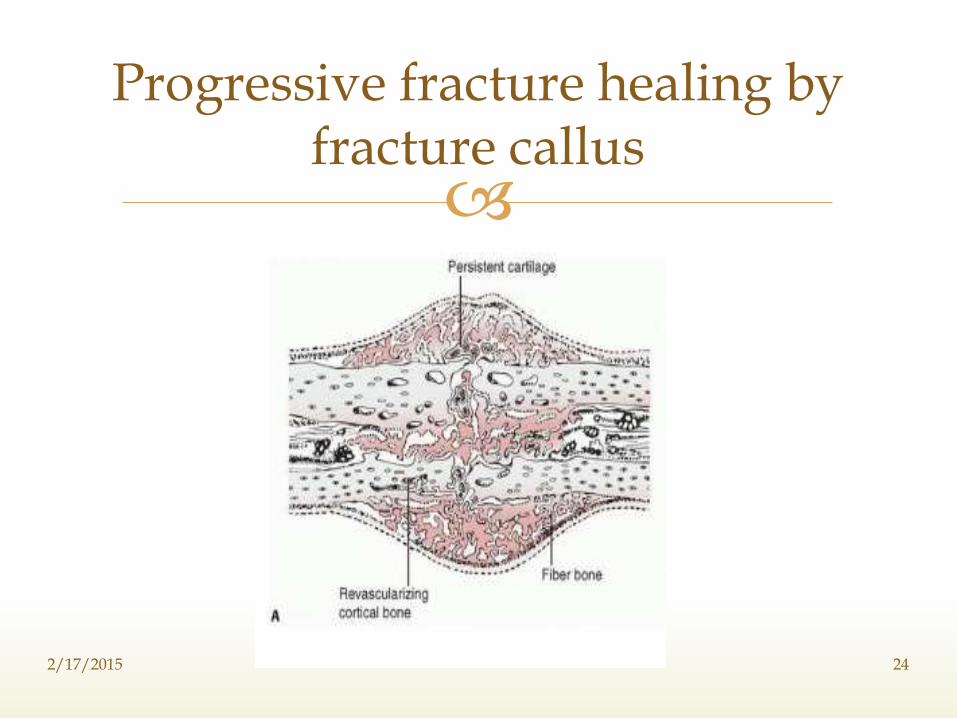
Progressive fracture healing by fracture callus
2/17/2015 24
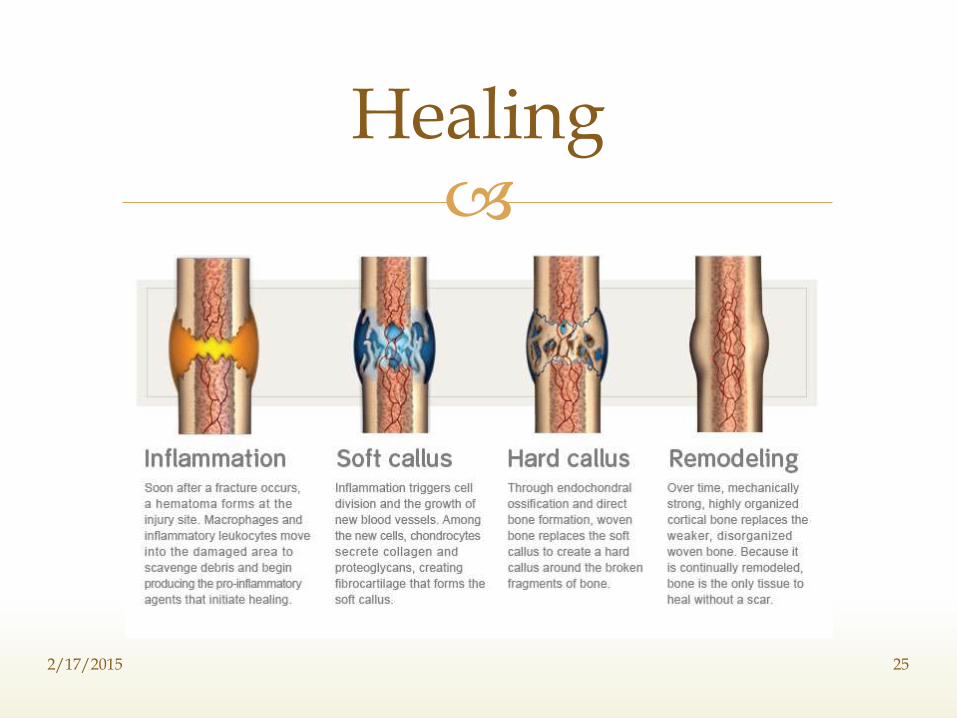
Healing
2/17/2015 25
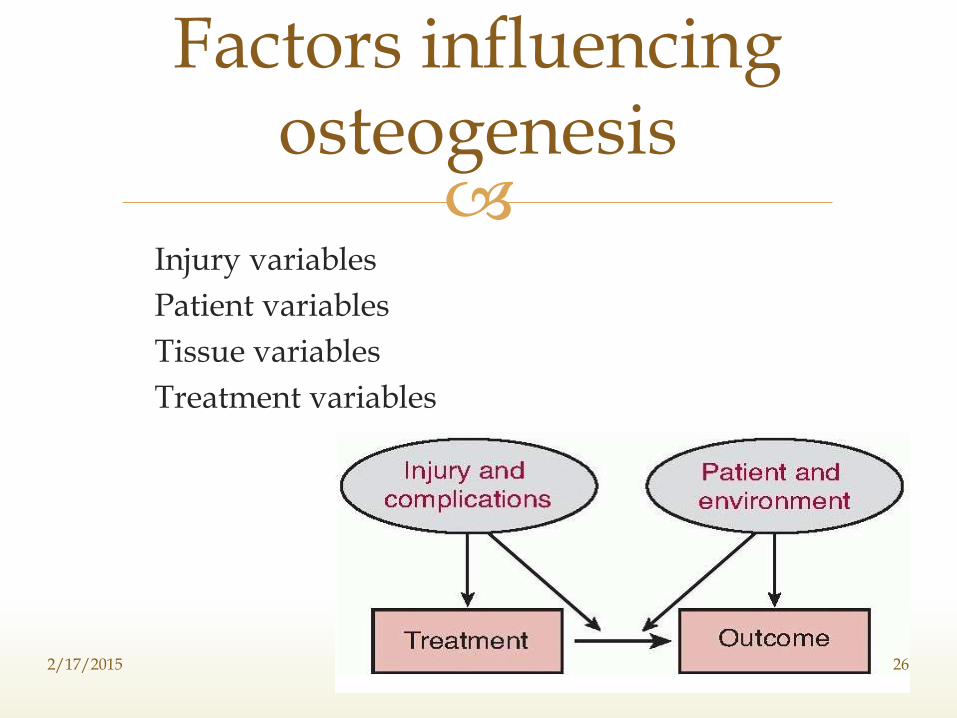
1.Injury variables
2.Patient variables
3.Tissue variables
4.Treatment variables
Factors influencing osteogenesis
2/17/2015 26
I).OPEN FRACTURES:-
Severe open fractures cause soft tissue disruption, fracture displacement, and, in some instances, significant bone loss.
Extensive tearing or crushing of the soft tissue disrupts the blood supply to the fracture site, leaving necrotic bone and soft tissue, impeding or preventing formation of a fracture hematoma, and delaying formation of repair tissue
1.Injury variables
2/17/2015 27

II).SEVERITY OF INJURY:-
They may be associated with large soft tissue wounds, loss of soft tissue, displacement and comminution of the bone fragments, loss of bone, and decreased blood supply to the fracture site.
Comminution of bone fragments usually indicates that there is also extensive soft tissue injury.
2/17/2015 28
Displacement of the fracture fragments and severe trauma to the soft tissues retard fracture healing, probably because the extensive tissue damage increases the volume of necrotic tissue, impedes the migration of mesenchymal cells and vascular invasion, decreases the number of viable mesenchymal cells, and disrupts the local blood supply.
2/17/2015 29
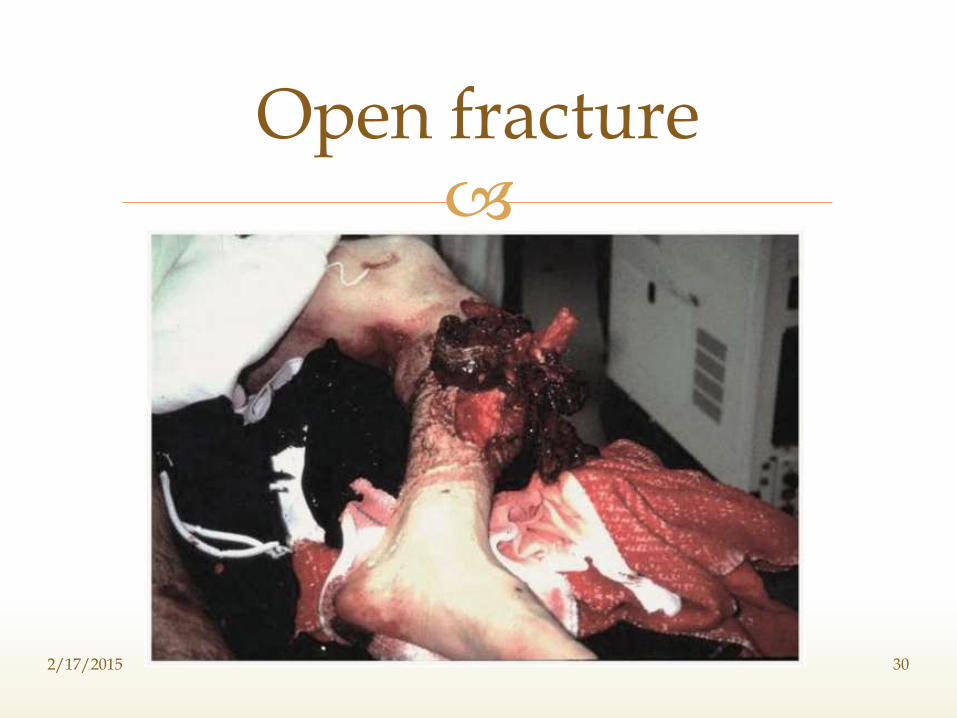
Open fracture
2/17/2015 30
III).INTRA-ARTICULAR FRACTURES:-
Because they extend into joint surfaces and joint motion or loading may cause movement of the fracture fragments, intra-articular fractures can present with challenging problems.
Most intraarticular fractures heal, but if the alignment and congruity of the joint surface is not restored, the joint may be unstable, and,in some instances, especially if the fracture is not rigidly stabilized, healing may be delayed or nonunion may occur.
2/17/2015 31
IV).SEGMENTAL FRACTURES:-
A segmental fracture of a long bone impairs or disrupts the intramedullary blood supply to the middle fragment.
If there is severe soft tissue trauma, the periosteal blood supply to the middle fragment may also be compromised.,possibly because of this, the probability of delayed union or nonunion, proximally or distally, may be increased.
These problems occur most frequently in segmental fractures of the tibia, especially at the distal fracture site.
2/17/2015 32
V).SOFT TISSUE INTERPOSITION:-
Interposition of soft tissue, including muscle, fascia, tendon, and occasionally nerves and vessels, between fracture fragments compromises fracture healing.
Soft tissue interposition should be suspected when the bone fragments cannot be brought into apposition or alignment during attempted closed reduction.
If this occurs, an open reduction may be necessary to extricate the interposed tissue and achieve an acceptable position of the fracture.
2/17/2015 33
VI).DAMAGE TO BLOOD SUPPLY:-
Lack of an adequate vascular supply can significantly delay or prevent fracture healing.
Insufficient blood supply for fracture healing may result from a severe soft tissue and bone injury or from the normally limited blood supply to some bones or bone regions.
For example, the vulnerable blood supplies of the femoral head,scaphoid, and talus may predispose these bones to delayed union or nonunion, even in the absence of severe soft tissue damage or fracture displacement.
2/17/2015 34
I)AGE:-
Infants have the most rapid rate of fracture healing.
The rate of healing declines with increasing age up to skeletal maturity, but after completion of skeletal growth the rate of fracture healing does not appear to decline significantly with increasing age, nor does the risk of non-unions significantly increase.
The rapid bone remodelling that accompanies growth allows correction of a greater degree of deformity in children.
2.Patient Variables
2/17/2015 35
II)NUTRITION:-
The cell migration and proliferation and matrix synthesis necessary to heal a fracture require substantial energy.
Furthermore, to synthesize large volumes of collagens, proteoglycans, and other matrix macromolecules, the cells need a steady supply of proteins and carbohydrates, the components of these molecules.
As a result, the metabolic state of the patient can alter the outcome of injury, and in severely malnourished patients, injuries that would heal rapidly in well nourished people may fail to heal.
2/17/2015 36
III).SYSTEMIC HORMONES:-
A variety of hormones can influence fracture healing.
Corticosteroids may compromise fracture healing possibly by inhibiting differentiation of osteoblasts from mesenchymal cells and by decreasing synthesis of bone organic matrix components necessary for repair.
Prolonged corticosteroid administration may also decrease bone density and compromise the surgeon's ability to achieve stable internal fixation, leading to nonunion.
2/17/2015 37
The role of growth hormone in fracture healing remains uncertain.
Thyroid hormone, calcitonin, insulin, and anabolic steroids have been reported in experimental situations to enhance the rate of fracture healing.
Diabetes, hypervitaminosis D, and rickets have been shown to retard fracture healing in experimental situations.
Nicotine and nicotine products(cigarette smoking) inhibits fracture healing.
2/17/2015 38
I)FORM OF BONE(CORTICAL OR CANCELLOUS):-
Healing of cancellous and cortical fractures differs probably because of the differences in surface area, cellularity and vascularity.
Opposed cancellous bone surfaces usually unite rapidly., possibly because the large surface area of cancellous bone per unit volume creates many points of bone contact rich in cells and blood supply and because osteoblasts form new bone directly on existing trabeculae.
3.Tissue Variables
2/17/2015 39
In contrast, cortical bone has a much smaller surface area per unit volume and usually a less extensive internal blood supply, and regions of necrotic cortical bone must be removed before new bone can form.
2/17/2015 40
II)BONE NECROSIS:-
Normally, healing proceeds from both sides of a fracture,but if one fracture fragment has lost its blood supply, healing depends entirely on ingrowth of capillaries from the living side or surrounding soft tissues.
If a fracture fragment is avascular the fracture can heal, but the rate is slower and the incidence of healing is lower than if both fragments have a normal blood supply.
2/17/2015 41
If both fragments are avascular, the chances for union decrease further.
Traumatic or surgical disruption of blood vessels, infection, prolonged use of corticosteroids, and radiation treatment can cause bone necrosis.
2/17/2015 42
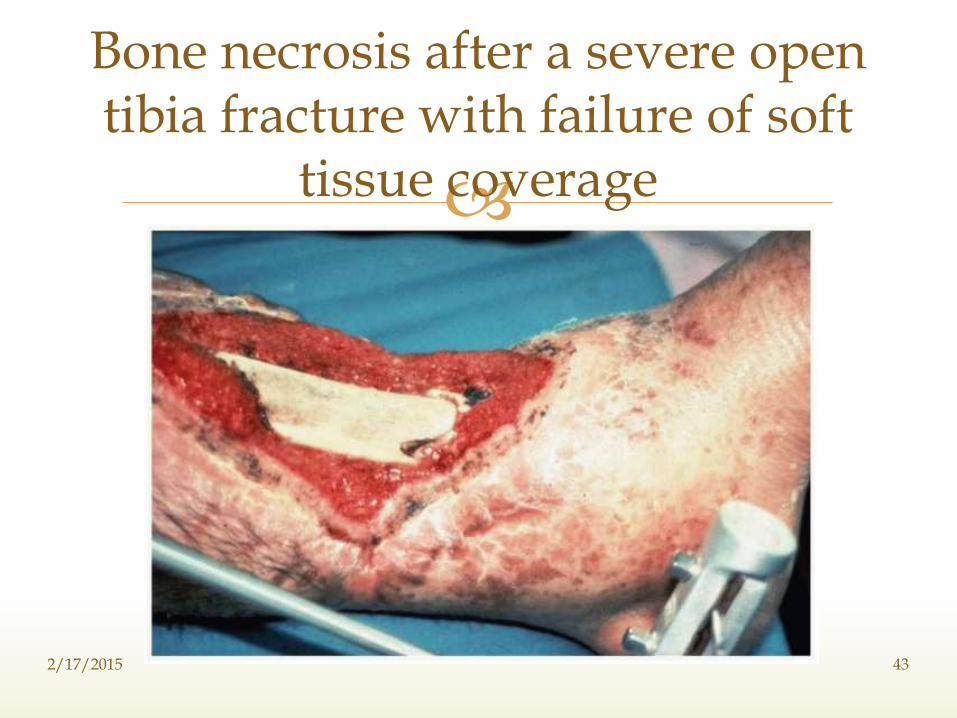
Bone necrosis after a severe open tibia fracture with failure of soft
tissue coverage
2/17/2015 43
III)BONE DISEASE:-
Fractures through bone involved with primary or secondary malignancies usually do not heal if the neoplasm is not treated.
Subperiosteal new bone and fracture callus may form,but the mass of malignant cells impairs or prevents fracture healing,particularly if the malignant cells continue to destroy bone.
2/17/2015 44
Fractures through infected bone present a similar problem.
Thus, healing of fractures through malignancies or infections usually requires treatment of the underlying local disease or removal of the involved bone.
Depending on the extent of bone involvement and the aggressiveness of the lesion, fractures through bones with nonmalignant conditions like simple bone cysts and Paget's disease will heal.
2/17/2015 45
The most prevalent bone disease, osteoporosis, does not impair fracture healing, but where there is diminished surface contact of opposing cortical or cancellous bone surfaces because of decreased bone mass, the time required to restore normal bone mechanical strength may be increased.
2/17/2015 46
IV)INFECTION:-Infection can slow or prevent healing.
For fracture healing to proceed at the maximum rate, the local cells must be devoted primarily to healing the fracture.
If infection occurs after fracture or if the fracture occurs as a result of the infection, many cells must be diverted to attempt to wall off and eliminate the infection and energy consumption increases.
Furthermore, infection may cause necrosis of normal tissue, edema, and thrombosis of blood vessels, thereby retarding or preventing healing.
2/17/2015 47
Apposition of fracture fragments,decreasing the fracture gap decreases the volume of repair tissue needed to heal a fracture.
Restoring fracture fragment apposition is especially important.
Fracture stabilization by traction, cast immobilization, external fixation, or internal fixation can facilitate fracture healing by preventing repeated disruption of repair tissue.
4.Treatment Variables
2/17/2015 48
Some fractures (e.g., displaced femoral neck and scaphoid fractures) rarely heal if they are not rigidly stabilized. Fracture stability appears to be particularly important for healing when there is extensive associated soft tissue injury, when the blood supply to the fracture site is marginal, and when the fracture occurs within a synovial joint
2/17/2015 49
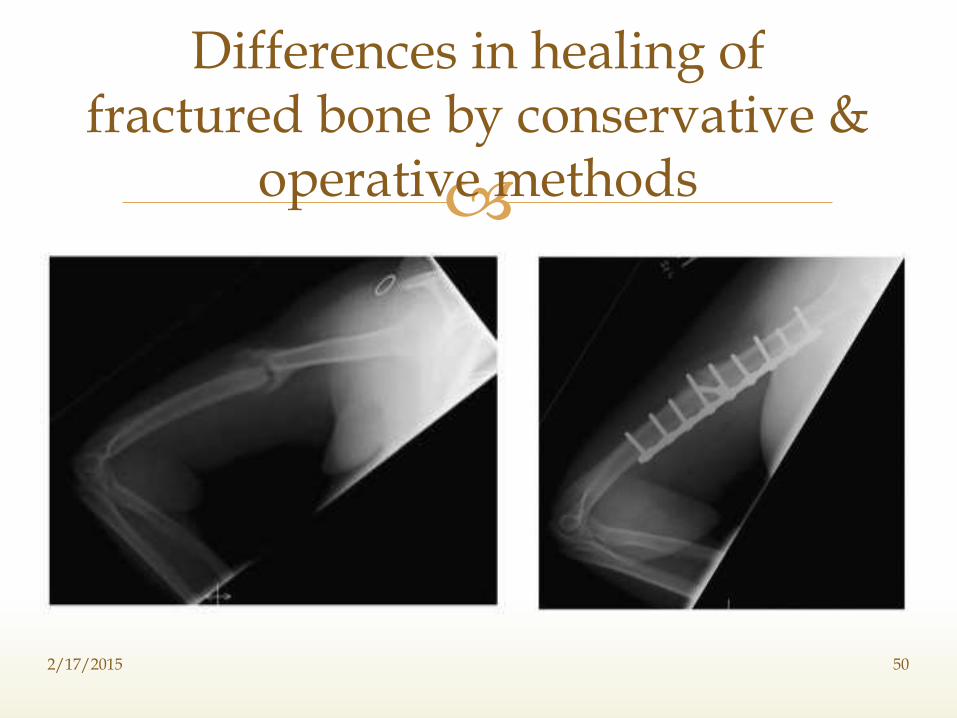
Differences in healing of fractured bone by conservative &
operative methods
2/17/2015 50
Treatment by closed methods:-
1.The process of fracture healing differs only when the fractures are manipulated at the end of few weeks after mobilisation even when before the mineralisation starts.
2.Due to distraction of fragments.,the traction forces tend to induce fibroblastic rather than osteoblastic conversion in uncomminuted connective tissue cells.
2/17/2015 51
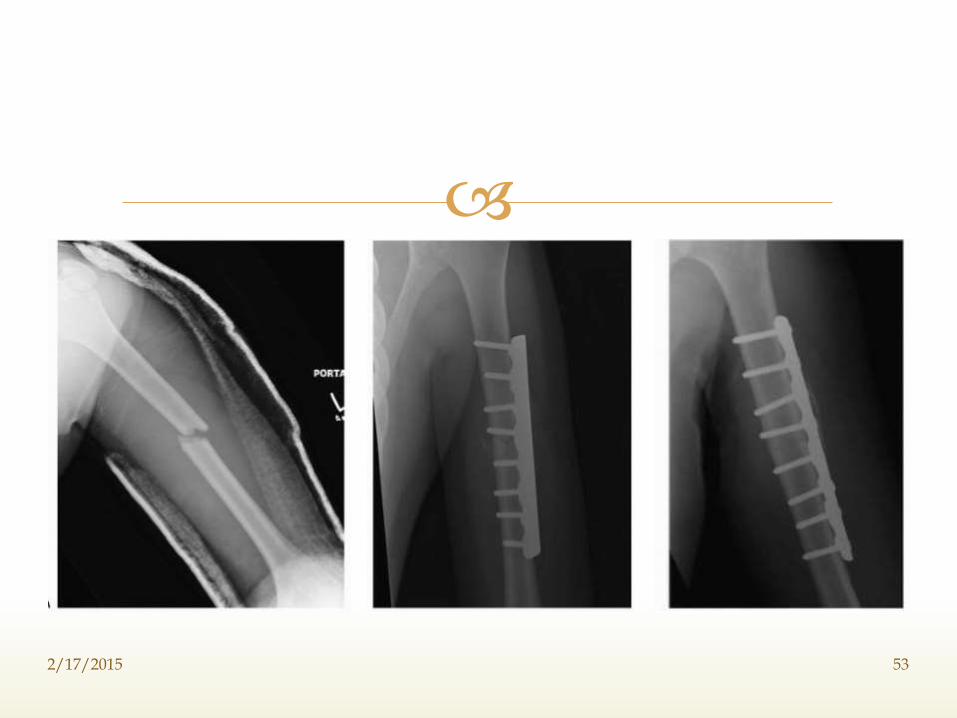
External callus is still the medium by which the fragments are first bridged although it is often reduced in quantity when compared with fixation by external means alone.
In cases of fractures fixed with rigid immobilizaton.,the modification in the healing process are first noted by Dr.Danis in 1949 when he observed radiologically that in rigidly fixed forearm bones external callus did not form,but instead fracture line gradually disappeared.
Healing progress for fracture
fixation done by plates and screws
2/17/2015 52
2/17/2015 53
He coined the term ‘SOUDRE AUTOGENE or PRIMARY BONE HEALING’ to describe this type of union.
When the fracture surfaces are rigidly held in contact, fracture healing can occur without any grossly visible callus. This type of fracture healing has been referred to as primary bone healing, indicating that it occurs without the formation and replacement of visible fracture callus
2/17/2015 54
When there is contact between the bone ends, lamellar bone can form directly across the fracture line by extension of osteons.
Osteoblasts following the osteoclasts deposit new bone; and blood vessels follow the osteoblasts. The new bone matrix, enclosed osteocytes, and blood vessels form new haversian systems.
2/17/2015 55
Where gaps exist that prevent direct extension of osteons across the fracture site, osteoblasts first fill the defects with woven bone. After the gap fills with woven bone, haversian remodeling begins, reestablishing the normal cortical bone structure, so called ‘GAP HEALING’ and this inturn acted as a conducting medium for the new osteones.
2/17/2015 56
The main disadvantage of this method is the damage which it inflicts on the medullary blood supply.
In few cases where narrow implants are used and reaming is not required.,vascular damage will be minimal & rapid regeneration of blood vessels occur.
When bigger and wider implants are used,vascular damage will be high and the medullary blood supply is poor and for the fracture healing to occur.,the sebsequent blood supply is through the periosteal blood supply from the surrounding soft tissue.
Healing in Intra-medullary Fixation
2/17/2015 57
1.Rockwood & Green’s-Fractures in Adults (VOL-1)
2.Watson-Jones Fractures and Joint Injuries
3.Chapman’s Textbook Of Orthopaedics (VOL-1)
4.Campbell’s Textbok of Operative Orthopaedics (VOL-3)
5.Robbin’s Textbook of Clinical Pathology.
References
2/17/2015 58

2/17/2015 59