Fracture healing
32
FRACTURE HEALING & COMPLICATIONS DR PANNA LAL SAHA PROFESSOR DEPARTMENT OF SURGERY BGC TRUST MEDICAL COLLEGE
-
Upload
panna-saha -
Category
Healthcare
-
view
207 -
download
0
Transcript of Fracture healing

FRACTURE HEALING & COMPLICATIONS
DR PANNA LAL SAHA PROFESSOR
DEPARTMENT OF SURGERY
BGC TRUST MEDICAL COLLEGE

INTRODUCTION
• Fracture is a break in the structural continuity of bone or periosteum.
• The healing of fracture is in many ways similiar to the healing in soft tissue wounds except that the end result is mineralised mesenchymal tissue i.e. BONE.
• Fracture healing starts as soon as bone breaks and continues modelling for many years.
The essential event in fracture healing is the creation of a bony bridge between the two fragments which can be readily be built upon and modified to suit the particular functional demands .

Components of BONE Formation
Cortex
Periosteum
Bone marrow
Soft tissue

FACTORS EFFECTING
The TYPE , AMOUNT and LOCATION of bone formed depends upon-----
FRACTURE TYPE GAP CONDITION FIXATION RIGIDITY LOADING BIOLOGICAL ENVIRONMENT

STAGES OF FRACTURE HEALING
TISSUE DESTRUCTION AND HAEMATOMA FORMATION
INFLAMATION AND CELLULAR PROLIFERATION
STAGE OF CALLUS FORMATION STAGE OF COSOLIDATION STAGE OF REMODELLING

Tissue destruction and Hematoma formation
– Torn blood vessels hemorrhage
– A mass of clotted blood (hematoma) forms at the fracture site
– Site becomes swollen, painful, and inflamed

Tissue destruction and Hematoma formation

INFLAMATION AND CELLULAR PROLIFERATION
• Within 8 hours inflammatory reaction starts.
• Proliferation and Differntiation of mesenchymal stem cells.
• Secretion of TGF-B , PDGF and various BMP factors.

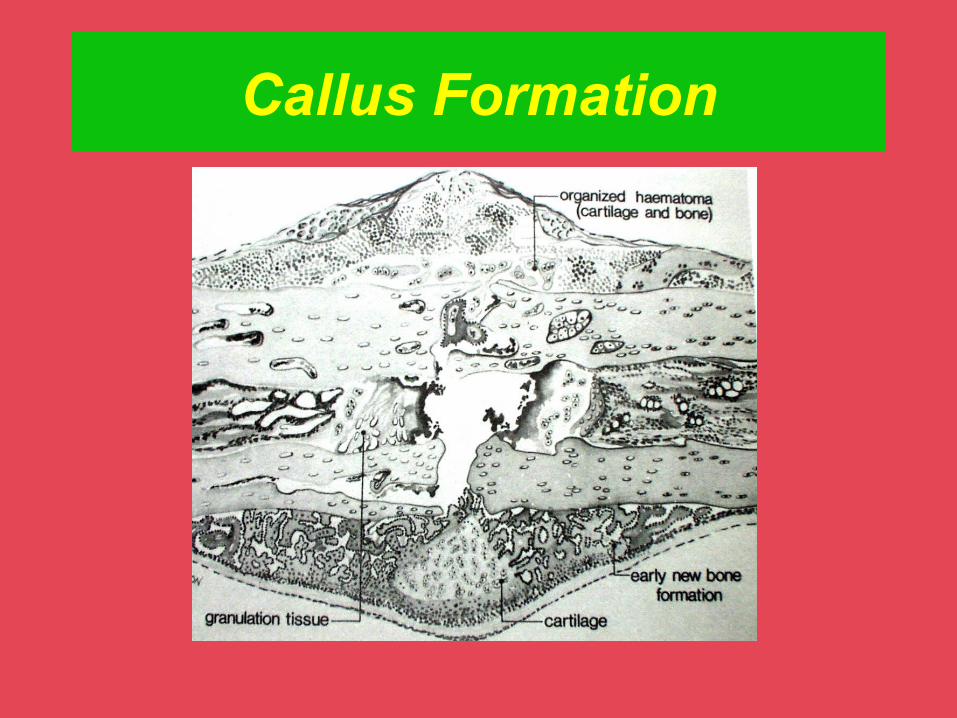
Callus Formation
• Fibrocartilaginous callus forms
• Granulation tissue (soft callus) forms a few days after the fracture
• Capillaries grow into the tissue and phagocytic cells begin cleaning debris

Callus Formation Theory
• OSTEOPROGENITOR CELL present in all ENDOSTEAL and SUBPERIOSTEAL surface give rise to CALLUS.
• CALLUS arises from NON-SPECIALISED CONNECTIVE TISSUE CELLS in the region of fracture which are induced into conversion to OSTEOBLASTS.
Callus Formation

STAGE OF CONSOLIDATION
– New bone trabeculae appear in the fibrocartilaginous callus
– Fibrocartilaginous callus converts into a bony (hard) callus
– Bone callus begins 3-4 weeks after injury, and continues until firm union is formed 2-3 months later

STAGE OF REMODELLING
Excess material on the bone shaft exterior and in the medullary canal is removed
Compact bone is laid down to reconstruct shaft walls

Schematic drawing of the callus healing process. Early intramembranous bone formation (a), growing callus volume and diameter mainly by enchondral ossification (b), and bridging of the fragments (c).
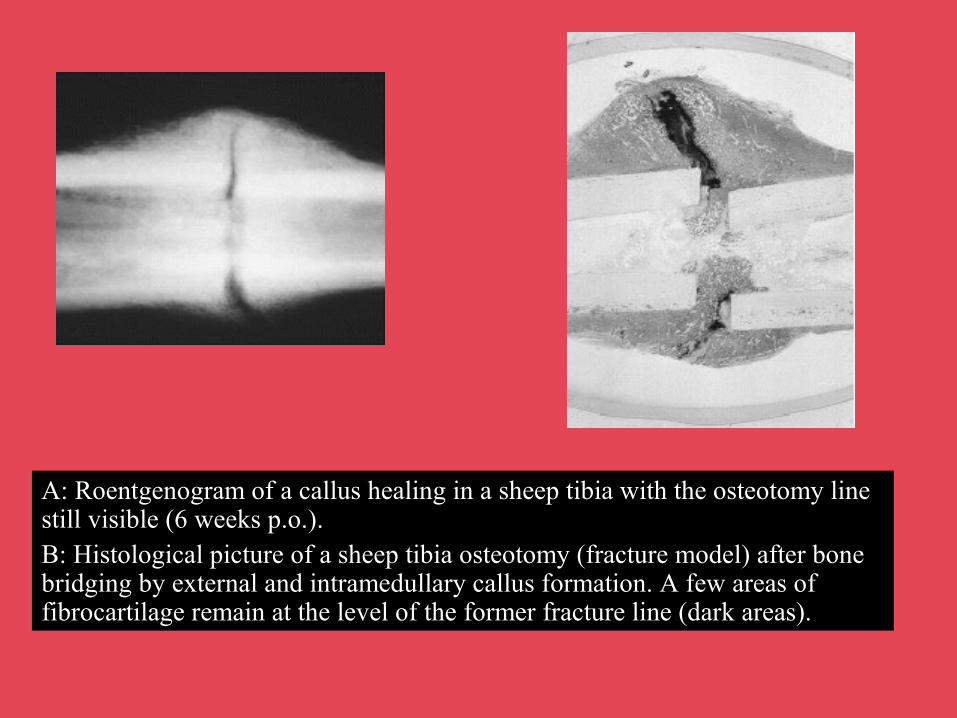
A: Roentgenogram of a callus healing in a sheep tibia with the osteotomy line still visible (6 weeks p.o.). B: Histological picture of a sheep tibia osteotomy (fracture model) after bone bridging by external and intramedullary callus formation. A few areas of fibrocartilage remain at the level of the former fracture line (dark areas).
COMPLICATIONS OF FRACTURE HEALING
• MALUNION
• DELAYED UNION
• NONUNION

MAL UNION
A MALUNITED Fracture is one that has healed with the fragments in a non anatomical position.
CAUSES1 INACCURATE REDUCTION
2 INEFFECTIVE IMMOBILIZATION
MALUNION contd…
MALUNION can IMPAIR FUCNTION by
ABNORMAL JOINT SURFACEROTATION or ANGULATIONOVERRIDINGMOVEMENT OF NEIGHBOURING
JOINT MAY BE BLOCKED
CHARACTERISTICS FOR ACCEPTABILITY OF FRACTURE REDUCTION
ALIGNMENT (MOST IMPORTANT) ROTATION RESTORATION OF NORMAL
LENGTHACTUAL POSITION OF FRAGMENTS
(LEAST IMPORTANT)
Delayed Union
• The exact time when a given fracture should be united cannot be defined
• Union is delayed when healing has not advanced at the average rate for the location and type of fracture (Btn 3-6 mths)
• Treatment usually is by an efficient cast that allows as much function as possible can be continued for 4 to 12 additional weeks

Delayed Union cont.
• If still nonunited a decision should be made to treat the fracture as nonunion
• External ultrasound or electrical stimulation may be considered
• Surgical treatment should be carried out to remove interposed soft tissues and to oppose widely separated fragments
• Iliac grafts should be used if plates and screws are placed but grafts are not usually needed when using intramedullary nailing, unless reduction is done open

Nonunion
• FDA defined nonunion as “established when a minimum of 9 months has elapsed since fracture with no visible progressive signs of healing for 3 months”
• Every fracture has its own timetable (ie long bone shaft fracture 6 months, femoral neck fracture 3 months)

Delayed/Nonunion
Factors contributing to development:
• Systemic
• Local

Delayed/Nonunion cont.
Systemic factors:
• Metabolic
• Nutritional status
• General health
• Activity level
• Tobacco and alcohol use
Delayed/Nonunion cont.
Local factors• Open• Infected• Segmental (impaired blood supply)• Comminuted• Insecurely fixed• Immobilized for an insufficient time• Treated by ill-advised open reduction• Distracted by (traction/plate and screws)• Irradiated bone• Delayed weight-bearing > 6 weeks• Soft tissue injury > method of initial treatment

Nonunion cont.
Nonunited fractures form two types of pseudoarthrosis:
• Hypervascular or hypertrophic
• Avascular or atrophic
Nonunion cont.
Treatment:1. Elecrical2. Electromagnatic3. Ulrasound4. External fixation (ie deformity, infection, bone loss)5. Surgical
• Hypertrophic: stable fixation of fragments• Atrophic: decortication and bone grafting• According to classification: type A : restoration of alignment, compression type B : cortical osteotomy, bone transport or
lengthening

Nonunion cont.
Surgical guidelines:
• Good reduction
• Bone grafting
• Firm stabilization

Nonunion cont.
Specific Bones • Metatarsals• Tibia• Fibula• Patella• Femur• Pelvis and acetabulum• Clavicle• Humerus• Radius• Ulna

THANK YOU