Fract Exo Pediat.

of 16
-
Upload
gabigonzalezp470 -
Category
Documents
-
view
224 -
download
0
Transcript of Fract Exo Pediat.
-
8/7/2019 Fract Exo Pediat.
1/16
The PDF of the article you requested follows this cover page.
This is an enhanced PDF from The Journal of Bone and Joint Surgery
87:2784-2798, 2005. doi:10.2106/JBJS.E.00528J. Bone Joint Surg. Am.David G. Stewart, Jr., Robert M. Kay and David L. Skaggs Open Fractures in Children. Principles of Evaluation and Management
This information is current as of December 5, 2006
Reprints and Permissions
Permissions] link.and click on the [Reprints andjbjs.orgarticle, or locate the article citation on
to use material from thisorder reprints or request permissionClick here to
Publisher Information
www.jbjs.org20 Pickering Street, Needham, MA 02492-3157The Journal of Bone and Joint Surgery
on December 5, 2006www.ejbjs.orgDownloaded from
http://www.jbjs.org/https://s100.copyright.com/AppDispatchServlet?PublisherName=JBJS&Publication=JBJS&Title=Open+Fractures+in+Children.+Principles+of+Evaluation+and+Management&PublicationDate=12/01/2005&Author=David+G.+Stewart%2C+Jr.&StartPage=2784&ContentID=87%2F12%2F2784&OrderBeanReset=truehttp://www.jbjs.org/https://s100.copyright.com/AppDispatchServlet?PublisherName=JBJS&Publication=JBJS&Title=Open+Fractures+in+Children.+Principles+of+Evaluation+and+Management&PublicationDate=12/01/2005&Author=David+G.+Stewart%2C+Jr.&StartPage=2784&ContentID=87%2F12%2F2784&OrderBeanReset=truehttp://www.jbjs.org/http://www.jbjs.org/http://www.jbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/http://www.jbjs.org/http://www.jbjs.org/https://s100.copyright.com/AppDispatchServlet?PublisherName=JBJS&Publication=JBJS&Title=Open+Fractures+in+Children.+Principles+of+Evaluation+and+Management&PublicationDate=12/01/2005&Author=David+G.+Stewart%2C+Jr.&StartPage=2784&ContentID=87%2F12%2F2784&OrderBeanReset=true -
8/7/2019 Fract Exo Pediat.
2/16
COPYRIGHT 2005 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED
2784
Current Concepts Review
Open Fractures in Children
Principles of Evaluation and Management
BY DAVID G. STEWART JR., MD, ROBERT M. KAY, MD, AND DAVID L. SKAGGS, MD
Open fractures in children often have a better prognosis than similar injuries in adults, and treatment may be dif-
ferent from that for adults.
Emergent administration of appropriate antibiotics is essential to decrease the risk of infection.
Stabilization of unstable fractures is usually beneficial, although children may require less rigidity than adults.
If viability of soft tissue is in doubt, dbridement should be deferred until a later operation, as the superior heal-
ing potential of young children may produce unexpected recovery.
Associated injuries are common with open fractures in children, and serial examinations over time often uncover
these injuries.
Most open fractures in children result from motor-vehicle acci-dents (including those in which the child is an occupant of themotor vehicle or is struck by an automobile while riding a bicy-cle or as a pedestrian) or falls from heights. The reported demo-graphics and injury mechanisms have varied widely from center
to center. Most investigators have reported a preponderanceof boys and a predilection for the forearm and tibia. In amulticenter study of 554 open fractures in children, the sites ofinjury were the tibia or fibula (190 fractures; 34%), radius orulna (178; 32%), hand or metacarpals (fifty-four; 10%), femur(thirty-seven; 6.7%), humerus (thirty-six; 6.5%), foot or meta-tarsals (twenty-four; 4.3%), elbow (fourteen; 2.5%), ankle (thir-teen; 2.3%), and other sites (eight; 1.4%)1. In another study, ofchildren presenting to one hospital, thirty-two (80%) of fortyopen fractures involved the forearm2. In yet another study, 9%of fractures in children admitted to a tertiary pediatric traumacenter were open3, although we suspect that open injuries con-stitute a substantially smaller percentage of pediatric fractures
outside of tertiary care centers.Open fractures in children differ from open fractures inadults in many ways. Thicker and more active periosteum pro-vides greater fracture stability and leads to more rapid and re-liable fracture-healing in young children compared with thatin older children and adults4. Young children have a greaterpotential for periosteal bone formation5. Healing is usuallyfaster and more reliable in children than it is in adults withsimilar injuries, and children can even have reconstitution ofbone in the face of bone loss6. Infection rates in children withopen fractures have been reported to be lower than those inadults with such fractures7.
There is a gradual progression from childhood to adult-hood. As children of the same chronologic age often demon-strate widely different physiologic or bone ages, it is notpossible to make comprehensive recommendations based ex-clusively on age. Our discussion of children refers to skeletally
immature patients. Patients with closed physes can often betreated according to adult algorithms.
Initial Evaluation and Management
The initial treatment of patients with open fractures requirescare of the so-called trauma ABCs (airway, breathing, and cir-culation) and achieving control of the cervical spine8,9. Arolled towel or pad is typically placed under the shoulders ofyoung children to avoid neck flexion, as the proportionatelylarge head of a child leads to neck flexion and a risk of neuro-logic injury when an adult board is used10.
The Pediatric Advanced Life Support (PALS)11 and Ad-vanced Trauma Life Support (ATLS)12 manuals provide help-
ful guidelines for the evaluation and care of children who havesustained traumatic injuries. Patients with a high-energy in-jury or multiple injuries should be evaluated by a traumasurgeon13. Intravenous lines are started, fluid resuscitation isbegun, and intravenous antibiotics are given promptly. If in-travenous access is not readily obtainable, intraosseous infu-sion can be performed with a large bone-marrow needle witha stylet placed in the proximal part of the tibia, approximately1 cm distal to the tibial tubercle to avoid physeal injury14. In-vestigators studying a rabbit model noted no physeal distur-bance following intraosseous infusion15. Intraosseous infusionhas been reported to be safe and effective in children16, al-
on December 5, 2006www.ejbjs.orgDownloaded from
http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/ -
8/7/2019 Fract Exo Pediat.
3/16
2785
THE JO U R N A LOF BON E & JOINT SU R G E R Y J BJ S .O RG
VO L U M E 87-A NUMBER 12 DECEMBER 2005
OP EN FR A C T U R E S IN CHILDREN
though there have been case reports describing compartmentsyndrome following prolonged or rapid infusions17,18. If intra-osseous infusion is used, care should be taken to avoid pro-longed or excessively rapid infusions and to change to a standard
venous access as soon as feasible.Patients who have not had a tetanus immunizationwithin the past five years and those whose immunization sta-tus is unknown are given a dose of tetanus toxoid. Many chil-dren do not receive their routine immunizations on time19,and underimmunization was demonstrated to be prevalent inone study of patients seen at an adult emergency department20.The orthopaedic surgeon cannot assume that the child is up todate with regard to tetanus immunizations or that tetanusprophylaxis has been given by other care providers. Humantetanus immune globulin provides immediate protection, butsome authors have concluded that it is indicated only for pa-tients who have never received primary immunization againsttetanus21, and its indications for children are unclear.
Neurologic evaluation of all of the major nerves or mus-cle groups is performed in both the injured and the unin-volved extremities. If the patient is not able to cooperate witha full neurologic examination because of age, mentation, ortrauma, he or she is observed for spontaneous motion, andany apparent deficit is noted. This may require some patiencewhen an injured and frightened child is being examined.Small children may not answer questions regarding sensationbut will often react to sensory stimuli. The results of the exam-ination, including a notation of any portions that could not beadequately performed, are recorded. The parents also shouldbe notified preoperatively if the patients neurologic statuscould not be fully ascertained. The vascular evaluation should
include assessment of capillary refill as well as the color of theskin and digits; palpation of distal pulses; and, when the in-jury is severe or pulses are questionable, assessment of distalarteries for Doppler pulses. Compartments should be pal-pated to ensure that they are supple. If compartments aretense or there is disproportionate pain with passive stretch ofthe digits, a compartment syndrome should be suspected andcompartment pressures should be measured.
After wound assessment, a sterile dressing is applied.Repeat inspections involving dressing changes are minimizedto avoid additional contamination or tissue trauma. Gross de-formities are realigned with gentle traction to reduce the ten-sion on soft tissues. Early splinting before the patient is taken
to the operating room minimizes ongoing injury to soft tis-sues and decreases pain.
Classification
The modified Gustilo-Anderson system continues to bewidely used for the classification of open fractures in bothchildren and adults22,23, although its reproducibility has beenquestioned24. A type-I open injury is a low-energy puncturewound that measures
-
8/7/2019 Fract Exo Pediat.
4/16
2786
THE JO U R N A LOF BON E & JOINT SU R G E R Y J BJ S .O RG
VO L U M E 87-A NUMBER 12 DECEMBER 2005
OP EN FR A C T U R E S IN CHILDREN
Patzakis and Wilkins performed a randomized prospec-tive study of adults and children who had a total of 1104 openfracture wounds, seventy-seven of which became infected, andfound that early administration of antibiotics with activities
against both gram-positive and gram-negative organisms wasthe most important factor in reducing the infection rate7. Theinfection rate was 2% for patients who had been given a ceph-alosporin, 10% for those who had been given penicillin andstreptomycin, and 14% for those who had not been givenantibiotics. The factors that influenced the infection rate in-cluded a failure to administer antibiotics, resistance of wound-contaminant organisms to the antibiotics, increased time fromthe injury to the administration of antibiotics, extent of soft-tissue damage, and open tibial fracture. Factors found to haveno effect on the infection rate included the time from injury todbridement, type of wound closure, and duration of anti-biotic treatment (three compared with five to ten days).
The appropriate duration of antibiotics following dbri-
dement of open fractures remains controversial. In a double-blind prospective trial of adult patients with an open fracturewho received intravenous cefamandole, Dellinger et al. dem-onstrated no difference in infection rates between thosetreated for one day and those treated for five days 28. In moststudies of open fractures in children, the authors have re-ported the practice of administering intravenous antibioticsfor at least forty-eight hours, although this has not been con-clusively demonstrated to be superior to twenty-four hours ofadministration.
Choice of Antibiotics
Cefazolin (100 mg/kg/day, divided into doses given every eight
hours, up to a maximum dose of 2 g every eight hours) is typi-cally administered to all patients with an open fracture. Pa-tients with a severe type-II or III injury typically are givengentamicin (5 to 7.5 mg/kg/day divided into doses given everyeight hours) in addition to cefazolin. Penicillin (150,000 units/kg/day divided into doses given every six hours, up to a maxi-mum dose of 24 million units/day) is added to cover Clostrid-ium species and anaerobes in patients with farm or vascularinjuries. Clindamycin (15 to 40 mg/kg/day divided into dosesgiven every six to eight hours, up to a maximum dose of 2.7 g/day) is commonly used instead of cefazolin for patients withallergies to cephalosporins or penicillin. Patzakis et al. re-ported that the infection rates following oral administration
of ciprofloxacin were similar to the rates following intrave-nous administration of cefamandole and gentamicin in adultpatients with a type-I or II open fracture, but the ciprofloxacinyielded inferior results in patients with a type-III fracture29.However, ciprofloxacin has not been approved for use in pa-tients under the age of eighteen years because animal datahave suggested that ciprofloxacin has adverse effects on bone-healing30 and a possible relationship with chondropathy. Somedata suggest a 2% to 3% prevalence of articular side effects inchildren receiving ciprofloxacin compared with a 0.1%preva-lence in adults31, although other studies have not demon-strated an increased risk in children32,33. Ciprofloxacin is used
extensively for children with cystic fibrosis, but routine use forchildren cannot be recommended at this time.
The increasing incidence of community-acquired methi-cillin-resistant Staphylococcus aureus infections has led someto wonder whether recommendations for initial antibioticsshould be altered. We are aware of no studies demonstratinga benefit to the use of clindamycin, vancomycin, or other
agents instead of cefazolin for prophylaxis for patients with anopen fracture, and these alternatives do not have the same recordof proven efficacy for preventing infection of open fractures.There is also concern about fostering additional bacterial re-sistance by the indiscriminate use of second-tier antibioticsthat are best administered to treat established infections, asincreasing resistance of community-acquired methicillin-resistant Staphylococcus aureus isolates to clindamycin in chil-dren has been demonstrated34. Clindamycin, vancomycin, orother substitutes for cefazolin cannot be routinely recom-mended for first-line prophylaxis, except for patients with al-lergies to cephalosporins.
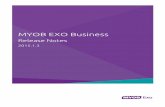
Fig. 1-A
Radiograph of a ten-year-old boy who sustained a type-III open frac-
ture of the tibia and fibula with severe soft-tissue loss medially
when he was dragged along the road. The shear injury to the me-
dial malleolus and physis was initially not appreciated by the treat-
ing physicians. (Figs. 1-A, 1-B, and 1-C reprinted, with permission,
from: Skaggs DL, Flynn JM. Staying out of trouble in pediatric or-
thopaedics.Philadelphia: Lippincott Williams and Wilkins; 2005.)
on December 5, 2006www.ejbjs.orgDownloaded from
http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/ -
8/7/2019 Fract Exo Pediat.
5/16
2787
THE JO U R N A LOF BON E & JOINT SU R G E R Y J BJ S .O RG
VO L U M E 87-A NUMBER 12 DECEMBER 2005
OP EN FR A C T U R E S IN CHILDREN
Local antibiotic therapy is safe, and high local antibioticconcentrations but low systemic levels are achieved35. Ami-noglycoside-impregnated polymethylmethacrylate beads ap-pear to further reduce the risk of infection in type-III opentibial fractures in adults36. These beads have also been success-fully used in children, although additional studies may be in-dicated to evaluate their efficacy in populations consistingonly of children. There are no standardized recommendationsregarding whether antibiotic-impregnated beads should beused prophylactically during the first dbridement of injuriesat high risk for infection, such as type-III open femoral frac-tures, or only at a later dbridement, when an established in-
fection is evident. Our practice generally is to use antibioticbeads only in severe established infections.
Timing of Surgery
Traditional teaching is that open fractures must be operatedon within six to eight hours after the injury. However, a litera-ture review calls this recommendation into question. In a ret-rospective multicenter study of 554 open fractures in childrenpresenting to a pediatric trauma center, an infection devel-oped in association with 3% (twelve) of 344 fractures that hadbeen treated with irrigation and dbridement within six hoursafter the injury compared with 2% (four) of 210 treated seven
hours or more after the injury (p = 0.43)1. When the fractureswere separated into groups according to whether they wereGustilo-Anderson type I, II, or III,there was no significant dif-ference in the infection rate between the fractures that hadbeen treated within six hours after the injury and those thathad been treated at least seven hours after the injury in anygroup. The authors concluded that irrigation and dbride-ment of open fractures in children can be performed withinthe first twenty-four hours after injury without increasing therisk of infection as long as intravenous antibiotics are startedon presentation to the emergency department. A prior retro-spective single-institution study of 104 children also demon-
strated no increase in the risk of infection for surgery as thesurgical delay increased from six to twenty-four hours37. In asimilar study of 103 adults with an open tibial fracture,Khatod et al. reported no relationship between infection rateand surgical delay38.
We are aware of only one retrospective study of childrenthat demonstrated an increased risk of infection when opera-tive treatment was performed more than six hours after injuryrather than less than six hours after injury39, and the authors ofthat study did not report the time at which antibiotics wereinitially administered. The study, by Kreder and Armstrong,involved open tibial fractures in children, and an infection de-
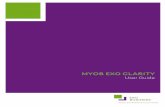
Fig. 1-B
Fig. 1-B Thirteen months later, medial growth arrest of the physis is demonstrated by the angulation of the growth plate. It can also be seen
that the medial malleolus is not of normal size. Fig. 1-C Twenty-two months later, 26 of varus is present.
Fig. 1-C
on December 5, 2006www.ejbjs.orgDownloaded from
http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/ -
8/7/2019 Fract Exo Pediat.
6/16
2788
THE JO U R N A LOF BON E & JOINT SU R G E R Y J BJ S .O RG
VO L U M E 87-A NUMBER 12 DECEMBER 2005
OP EN FR A C T U R E S IN CHILDREN
veloped in two of eight cases in which the time between the in-jury and surgery was more than six hours compared with five(12%) of forty-two cases in which the operation was per-formed within six hours39. We interpret these results with cau-tion, as the numbers were so small that if one less patient hadbeen infected in the late-treatment group, the infection rateswould have been identical.
The current literature seems to indicate that delayingoperative treatment of open fractures does not increase therate of infection if antibiotics are administered early. How-ever, such studies have not addressed the risk to the soft-tissue envelope when operative intervention is delayed. Thistopic remains controversial, and some surgeons strongly be-
lieve that all open fractures should undergo emergent irriga-tion and dbridement within six hours in spite of the lack ofevidence supporting this approach in the medical literature.Our practice is to operatively dbride all open fractureswithin the first twenty-four hours and to operate emergentlywhen a fracture is associated with neurovascular compro-mise, severe soft-tissue injury, or another urgent operativeindication. At times, when a patient with a type-I or II openfracture without neurovascular compromise, soft tissue atrisk, or a risk of compartment syndrome comes in after 10p.m., we will wait until the next morning to provide opera-tive treatment.
Irrigation and Dbridement
The initial irrigation and dbridement of open fractures inyoung children should be different from that of similarwounds in adults, largely because of the better healing poten-
tial in children. After the wound is extended and irrigated andareas of gross contamination are removed, the tourniquet (ifused) is deflated to identify tissue viability. Muscle that bleedsor contracts when pinched by a forceps should be retained. Incontrast to our practice with adults, we recommend retainingtissue of questionable viability in young children at the time ofthe initial dbridement if a second dbridement is planned, aswe have been surprised many times by the healing in youngchildren. Both bone ends should be visualized and cleaned, asdebris may be found here even in type-I injuries.
Periosteum in young children can reconstitute boneeven when there is bone loss. Devitalized bone stripped of allsoft-tissue attachments usually should be removed in an adult,whereas this bone may be left in place and will usually incor-
porate in young children. The incised area can be gently reap-proximated with simple nylon or Prolene (polypropylene)sutures, while the traumatic wound can be closed over a drainor left open40. Low-grade open fractures can usually be treatedadequately with a single procedure, whereas type-III and severetype-II injuries typically should undergo dbridement everyforty-eight to seventy-two hours until the soft tissues have stabi-
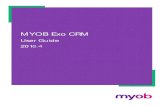
Fig. 2-A
Open distal fractures of the tibia and fibula sustained in a motor-ve-
hicle accident by a five-year-old boy.
Fig. 2-B
In contrast to the more rigid fixation that is standard in adults, sim-
ple Kirschner-wire fixation was used.
on December 5, 2006www.ejbjs.orgDownloaded from
http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/ -
8/7/2019 Fract Exo Pediat.
7/16
2789
THE JO U R N A LOF BON E & JOINT SU R G E R Y J BJ S .O RG
VO L U M E 87-A NUMBER 12 DECEMBER 2005
OP EN FR A C T U R E S IN CHILDREN
lized, the remaining tissue appears viable, and the wound isconsidered clean on the basis of visual inspection. For severe
type-III injuries, a multidisciplinary approach including plasticsurgery and, at times, a vacuum-assisted closure is beneficial.
If little additional dissection is needed, a compartmentrelease should be done for most high-energy open fractures inwhich extensive soft-tissue injury can be expected, such as anopen tibial fracture sustained in a motor-vehicle accident.Pain associated with a compartment syndrome may be diffi-cult to discern from the pain associated with an open fracturein a child, so we recommend an aggressive prophylactic ap-proach. Compartments should be palpated intraoperatively toensure that they are supple. Pallor, paresthesias, and absentpulses are late signs of compartment syndrome.
While animal studies have demonstrated that high-pres-
sure lavage with saline solution is more effective than low-pressure lavage for removing bacteria from contaminatedwounds, especially when the irrigation is performed morethan four hours after the injury41, high-pressure irrigation hasbeen found in vivo to have a deleterious effect on the earlystages of bone-healing42. In an animal model, low-pressure la-vage with liquid soap was reported to be more effective thanlow-pressure irrigation with saline solution or a detergent so-lution for removing adherent bacteria from bone, and it pre-served osteoblasts and osteoclasts better than povidone iodine,bacitracin wash, chlorhexidine solution, or detergent alone43.Soap or detergent irrigation is more effective than saline solu-
tion or antibiotic irrigation for removing bacteria from woundswith bone injury or soft-tissue damage44-46. Caution must be
exerted when irrigation is used through a small wound as in-creased fluid under pressure may contribute to compartmentsyndrome.
Dbridement Compared with
Lavage for Type-I Open Fractures
Two recent studies have suggested that operative dbridementmay not be necessary for all type-I open fractures. Yang andEisler reported no infections in a series of ninety-one patients,including thirteen children, in whom a type-I open fracturehad been treated nonoperatively47. In the only study of whichwe are aware that evaluated nonoperative treatment of openfractures in an entirely pediatric population, a deep infection
was found in one (3%) of forty children48
.We view nonoperative management of open fractures aspotentially dangerous. Because the numbers in the abovestudies were so small, there was a realistic potential for a type-II error (a false-negative finding) as a result of inadequatesample size. There have been rare anecdotes of children havinggas gangrene or even dying after having been sent home with-out operative treatment for an open fracture. At an absoluteminimum, patients with a type-I open fracture should receivein-hospital intravenous antibiotics and observation for forty-eight hours following irrigation of the fracture. Whether ir-rigation of a presumably clean type-I open fracture in an
Fig. 2-C
Figs. 2-C and 2-D Healing was uneventful, and good union is demonstrated on these radiographs made
four months following the injur y.
Fig. 2-D
on December 5, 2006www.ejbjs.orgDownloaded from
http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/ -
8/7/2019 Fract Exo Pediat.
8/16
2790
THE JO U R N A LOF BON E & JOINT SU R G E R Y J BJ S .O RG
VO L U M E 87-A NUMBER 12 DECEMBER 2005
OP EN FR A C T U R E S IN CHILDREN
emergency room is sufficient is open to debate, but some sur-geons have described finding pieces of gravel or other contam-inants during the operative dbridement of even tiny, nearlypinpoint wounds that appeared to be clinically benign. In the
absence of definitive studies proving the contrary, we believethat surgical irrigation and dbridement are indicated for allopen fractures.
Wound Cultures
Routine cultures before or after dbridement are not indicatedfor patients with an open fracture. Cultures should be per-formed only after an infection has developed. In one study, aninfection subsequently developed in twenty-four (20%) of 119wounds for which cultures had been positive prior to dbride-ment and nine (28%) of thirty-two for which cultures hadbeen positive after dbridement49. More importantly, only23% of the subsequent infections were caused by organismsidentified by the cultures performed before dbridement and
42% (eight of nineteen) were caused by organisms identifiedby cultures performed after dbridement. Other authors havealso noted little correlation between positive pre-dbridementand post-dbridement cultures and later infection50. Thus rou-tine cultures for patients who have no infection are morelikely than not to identify an organism that is not responsiblefor a subsequent infection and may lead to the administrationof incorrect antibiotics.
Soft-Tissue Care
In a study of eighty-three children with an open tibial fracture,Cullen et al. reported that a type-I or II open fracture in a childmay be closed over a drain in the absence of gross contamina-
tion or extensive soft-tissue damage40. Our practice is to closethe surgically created extension of the wound primarily and toeither leave the traumatic wound open or close it over a drain.
Early local or free-flap coverage may be indicated for largeopen wounds with exposed bone51. Closed fractures associatedwith severe soft-tissue injuries may also behave like open frac-tures. Bumper injuries, high-energy or comminuted fractures,and fractures in patients with polytrauma can be challenging, astenuous soft tissues may die under a cast. Delayed soft-tissuecoverage of bone has been reported to increase the risk of com-plications, including infection and soft-tissue problems52.
Open physeal fractures present special difficulties andhave been excluded from many series of open fractures in chil-
dren. Bae et al. reported on two open physeal fractures withsevere soft-tissue loss that were successfully treated with vas-cularized flap coverage53. New techniques, such as use of com-bined pedicle flaps, have been described54. Severe deglovinginjuries about a joint may result in unrecognized physeal in-jury and growth arrest (Figs. 1-A, 1-B, and 1-C).
Vacuum-assisted closure55,56 has been found to be safeand effective for closure of open fractures in children, and itmay obviate the need for free tissue transfers in some cases. Itis thought that the vacuum-assisted closure system may im-prove the local wound environment and promote granulationby removing debris and soluble inflammatory mediators that
may inhibit wound-healing. Use of vacuum-assisted closure inthe treatment of lawnmower injuries in children led to a trendfor fewer revision amputations and better post-treatmentfunction with no treatment-related complications or adverse
reactions
57
. We use vacuum-assisted closure during the firstdbridement for many open fractures with large or severesoft-tissue defects that expose bone or tendon, such as ankleinjuries resulting from road-dragging. We have been im-pressed with the results of this treatment in our practice.
Because 0.5 to 2 cm of overgrowth is generally expectedfollowing a femoral58 or tibial40 fracture in a young child, it hasbeen stated that initial shortening of not greater than 2 cm canbe accepted, although we recommend
-
8/7/2019 Fract Exo Pediat.
9/16
2791
THE JO U R N A LOF BON E & JOINT SU R G E R Y J BJ S .O RG
VO L U M E 87-A NUMBER 12 DECEMBER 2005
OP EN FR A C T U R E S IN CHILDREN
severely comminuted (Figs. 3-A through 3-E). Compared withexternal fixation, flexible intramedullary nails allow bettersoft-tissue access, provide better cosmetic results, and requireless patient and family care. Other anatomy-specific consider-
ations are discussed below.
Humeral FracturesAlthough supracondylar fractures of the humerus are com-mon in children, there have been few reports specifically ad-dressing open humeral fractures in children. Haasbeek andCole reported on a series of fifteen patients with an open su-pracondylar, T-type, or diaphyseal humeral fracture63. Sevenpatients presented with associated nerve injuries, and two pa-tients had arterial injury. Two children were lost to follow-up.The long-term result was good or excellent for eleven childrenand fair for two. Our experience has been that the infectionrate associated with open supracondylar fractures is low as aresult of abundant blood supply about the elbow. We have
found treatment consisting of irrigation and dbridement,fracture reduction, and lateral-entry pinning to be adequatefor the vast majority of open supracondylar fractures.
Forearm FracturesRecent research suggests that fracture stabilization can mini-mize the risk of malunion or nonunion. Luhmann et al. re-ported on a series of sixty-five children with an open forearmfracture, including fifty-two with a type-I fracture, twelve witha type-II fracture, and one with a type-III fracture 64. None ofthirty-eight fractures treated primarily with operative in-tramedullary stabilization, Kirschner wires, or plates andscrews required subsequent realignment, whereas five of
twenty-seven fractures treated without stabilization requiredadditional realignment. This study supports our belief thatwhen a child is already undergoing anesthesia for irrigationand dbridement, fracture fixation adds little risk and proba-bly provides substantial benefit by maintaining fracture re-duction. Greenbaum et al. provided further support for thisbelief in their study of sixty-two children with an open fore-arm fracture65. A trend for internal fixation to minimize angu-lar deformity and reduce the need for realignment procedureswas noted regardless of the fixation method (transcutaneousor intramedullary pin fixation or plates and screws), althoughthis finding was not significant. Pins may be left protrudingthrough the skin and then pulled out in the physicians office
in four to six weeks, when early fracture callus is seen on ra-diographs. Alternatively, pins may be buried under the skinand removed at a later date.
Haasbeek and Cole noted that, in a series of forty-sixchildren with an open forearm fracture, a compartment syn-drome developed in five, five presented with nerve injury, andone had an arterial injury63. Ten of the forty-six children had adelayed union, malunion, nonunion, or refracture. Thesecomplications were more common in association with type-IIand III open injuries. Of thirty-eight patients available for fol-low-up, thirty-three had a good or excellent outcome, fourhad a fair outcome, and one had a poor outcome.
Femoral FracturesOpen femoral fractures are rare but severe injuries. Hutchinset al. reported that thirty-two (4%) of 712 femoral fracturestreated at a large urban pediatric trauma center from 1985 to
1996 were open
26
. Of forty-three children with a total of forty-four open femoral fractures (twenty-five type I, nine type II,and ten type III) treated at two centers, thirteen were treatedwith a spica cast; twelve, with external fixation; fourteen, withlocked intramedullary nailing; three, with open reduction andinternal fixation; and two, with pins and a plaster cast. Com-plications in the patients with a type-I fracture included twocases of malalignment requiring manipulation followingtreatment with a spica cast, one case of osteonecrosis of thefemoral head following rigid intramedullary nailing, and onecase of unacceptable shortening requiring conversion from aspica cast to external fixation. One patient with a type-II frac-ture required an osteotomy and intramedullary nailing fol-
Fig. 3-A
An open tibial fracture sustained by a ten-year-old boy who also
sustained multiple other injuries. Following irrigation and dbri-
dement, the fracture was treated with a flexible intramedullary
rod that was placed proximally to avoid the tibial physis and tibial
tubercle. (Figs. 3-A through 3-E reprinted, with permission, from:
Skaggs DL, Flynn JM. Staying out of trouble in pediatric ortho-
paedics.Philadelphia: Lippincott Williams and Wilkins; 2005.)
on December 5, 2006www.ejbjs.orgDownloaded from
http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/ -
8/7/2019 Fract Exo Pediat.
10/16
2792
THE JO U R N A LOF BON E & JOINT SU R G E R Y J BJ S .O RG
VO L U M E 87-A NUMBER 12 DECEMBER 2005
OP EN FR A C T U R E S IN CHILDREN
lowing a malunion after initial treatment with a spica cast.Osteomyelitis developed at the sites of five of the ten type-IIIfractures, and two type-III fractures treated with an externalfixator went on to malunion requiring corrective osteotomy26.The authors concluded that type-I and II fractures can typi-cally be treated with irrigation and dbridement followed byage-appropriate fixation methods, whereas the optimal fixa-tion for type-III fractures remains unresolved. Another series,of eleven open femoral fractures, demonstrated faster healingof lower-grade injuries and in younger children66.
Open femoral shaft fractures in children younger thanthe age of six years may be treated with irrigation and dbride-ment and a spica cast, although soft-tissue management is of-ten a problem when a spica cast is used. Fixation with atraditional compression plate is an option for comminutedopen diaphyseal fractures of the femur in children 67, althoughit is rarely the treatment of choice. Early results in small seriesin which a submuscular bridge plate was used for open andcomminuted femoral fractures in children68,69 appear encour-aging, as these procedures require less initial soft-tissue dissec-tion than does traditional plate fixation. External fixation waswidely used for open femoral fractures in children in the past.
However, because of a high refracture rate, substantial scar-ring, and delayed unions, the present trend is for external fixa-tion to be employed primarily for fractures that are notamenable to flexible nailing because of their location, theirconfiguration, or soft-tissue considerations.
Few other authors have exclusively examined open femo-ral fractures in children, but most major series of femoral frac-tures in children have included both open and closed injuries.Flexible intramedullary nailing has become a preferred treat-ment for diaphyseal femoral fractures in children70, especially
those between the ages of six and twelve years. Numerous stud-ies have demonstrated excellent results, with no nonunions ormalunions, in children treated with flexible intramedullaryfemoral nailing71-74. Those studies have shown dramatically ear-lier walking, shorter hospital stays, decreased healing times, andearlier return to school compared with those results followingtreatment with either external fixation72 or a spica cast74 in age-matched patient groups.
Open Tibial FracturesSuccessful treatment of open tibial fractures in children hasbeen achieved with a variety of means, including external fixa-
Fig. 3-B
Figs. 3-B and 3-C Radiographs made at four weeks after treatment show substantial callus. The flexible rod was removed in the
physicians office, and weight-bearing in the cast was encouraged.
Fig. 3-C
on December 5, 2006www.ejbjs.orgDownloaded from
http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/ -
8/7/2019 Fract Exo Pediat.
11/16
2793
THE JO U R N A LOF BON E & JOINT SU R G E R Y J BJ S .O RG
VO L U M E 87-A NUMBER 12 DECEMBER 2005
OP EN FR A C T U R E S IN CHILDREN
tion, internal fixation, cast immobilization, and hybrid tech-niques75. External fixation has been the traditional choice foropen fractures with severe comminution or segmental boneloss and in medically unstable patients76. External fixation hasbeen used, with good results, for high-grade (type-II and III)tibial fractures, including those with a segmental or butterflypattern6. High rates of pin-track infection, unsightly scars, soft-tissue tethering, delayed union, and refracture make externalfixators less attractive for stable fractures. In one study, rigidexternal fixation was associated with a 21% refracture rate atthe time of frame removal77. Another study demonstrated a
1.4% refracture rate in patients treated with a unilateral,more flexible fixator78. The refracture rate is low if healing isnoted on three cortices at the time of fixator removal79. Theeffect of dynamization on the refracture rate is controversial80.We find external fixators to be particularly helpful for main-taining a plantigrade foot while providing osseous stabiliza-tion and soft-tissue access in patients with a degloving injuryabout the foot and ankle (Fig. 4). Thin wire hybrid fixatorsare less useful for children than for adults because of the opengrowth plates near articular surfaces. The Ilizarov bone trans-port technique may be useful for the late reconstruction ofinjuries with large osseous defects,but it is used infrequently
for acute pediatric trauma in the United States81.Intramedullary fixation with flexible titanium nails is
becoming the treatment of choice for many fractures of thetibial diaphysis in children82,83. Kubiak et al. presented a retro-spective report on a series of children with a tibial fracture84.Sixteen fractures (including five that were open) were treatedwith flexible intramedullary nailing, and fifteen (includingeight that were open) were managed with external fixation.The authors found that flexible nailing resulted in fasterunion (mean, seven weeks) than did external fixation (mean,eighteen weeks) and yielded significantly better outcomes in
terms of global function, pain, happiness, and sports activity(p < 0.01).Cullen et al. reported on a series of eighty-three children
who had an open tibial fracture40. Forty fractures were fixedpercutaneously with Steinmann pins and supplemental castimmobilization, thirty-two were treated with a cast only, ninewere treated with external fixation, and one each was treatedwith internal fixation and intramedullary nailing. Of the fortyfractures treated with percutaneous pinning and a cast, 23%(nine) had delayed union and 10% (four) had malunion of>10; no malunions were reported in the patients treated withthe other methods. These data suggest that, while percutane-
Fig. 3-D
Figs. 3-D and 3-E There was excellent healing at three months.
Fig. 3-E
on December 5, 2006www.ejbjs.orgDownloaded from
http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/ -
8/7/2019 Fract Exo Pediat.
12/16
2794
THE JO U R N A LOF BON E & JOINT SU R G E R Y J BJ S .O RG
VO L U M E 87-A NUMBER 12 DECEMBER 2005
OP EN FR A C T U R E S IN CHILDREN
ous pinning of open tibial fractures in children is possible,
there may be a high risk of malunion. In our practice, we pre-fer to use flexible intramedullary nails for this injury.
Many reports suggest that open tibial fractures have amore benign course in children under the age of eleven ortwelve years, and especially in those under the age of sixyears85-87. Blasier and Barnes reported complication rates of27% in children younger than twelve years and 69% in olderchildren88. Court-Brown et al. noted that even thirteen to six-teen-year-old patients may have better healing than adults89.Buckley et al. identified a relationship between the time tofracture union and the severity of the soft-tissue injury, frac-ture configuration, segmental bone loss, and infection inchildren75. In a series of children with a total of ninety open
tibial fractures (thirty-eight type I, thirty-five type II, andseventeen type III), Grimard et al. found ten delayed unionsand seven nonunions87. Patient age and fracture type wereassociated with the time to unionthat is, the risk of de-layed union or nonunion was significantly higher in childrenolder than the age of twelve years than in those younger thanthe age of six years (p = 0.02).
Robertson et al. reported on a series of open tibial frac-tures. Sixteen were treated with a cast alone; ten, with externalfixation and a supplemental short leg cast; two, with in-tramedullary nailing; two, with open reduction and internalfixation; and one, with amputation66. The authors reported a
significant correlation between patient age and time to union
(p < 0.001). All fractures united and the fixators were removedat an average of seven weeks, with no pin-track infections. Theauthors concluded that, when an open tibial fracture is not as-sociated with segmental bone deficiency or soft-tissue loss re-quiring major reconstruction, osseous healing can be expectedwithin six months.
The long-term outcome of open tibial fractures in chil-dren may not be as benign as has been presumed. Reportedcomplications have included compartment syndrome in 2%to 4% of patients, delayed union in 11% to 22%, and infec-tion in up to 10%87-89. Nonunion has been rare in most seriesof open tibial fractures, although it was reported in seven ofninety children in one study88. Limb-length discrepancy is
another known complication. Overgrowth of at least 1 cmwas reported following five of eighty-three open tibial frac-tures in one series40. In a series of ninety-two children withopen tibial fractures of all types, sixty-five of which weretreated with a cast, twenty-six of which were treated with ex-ternal fixation, and one of which was treated with internalfixation, Hope and Cole reported a limb-length discrepancyof at least 0.5 cm in sixty patients between 1.5 and 9.7 yearspostoperatively90. Of seventy-four patients seen at the time offinal follow-up, half reported pain at the fracture site andseventeen each had restriction of sports activity, joint stiff-ness, or cosmetic defects.
Fig. 4
A child was hit by an automobile as a pedestrian and was dragged, which caused open distal tibial
and fibular fractures in addition to severe soft-tissue loss exposing bone and joints. An external fix-
ator across the ankle helped to maintain the stability of the tibial fracture, prevent ankle equinus,
and immobilize the area of soft-tissue injury to maximize the chance of a future skin graft being
successful. A wound vacuum-assisted closure was used to prepare the area of exposed bone and
joints prior to skin-grafting. (Reprinted, with permission, from: Skaggs DL, Flynn JM. Staying out of
trouble in pediatric orthopaedics.Philadelphia: Lippincott Williams and Wilkins; 2005.)
on December 5, 2006www.ejbjs.orgDownloaded from
http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/ -
8/7/2019 Fract Exo Pediat.
13/16
2795
THE JO U R N A LOF BON E & JOINT SU R G E R Y J BJ S .O RG
VO L U M E 87-A NUMBER 12 DECEMBER 2005
OP EN FR A C T U R E S IN CHILDREN
Open Pelvic FracturesA study of fifteen open pelvic fractures in children treated atone institution over a twelve-year period demonstrated that,after a minimum of two years of follow-up, ten were vertically
unstable
91
. Fourteen of the fifteen fractures had been caused byan automobile-pedestrian accident, and thirteen of the four-teen had been caused by a run-over mechanism. Three of thefifteen patients died, and sepsis and infection from bowel andgenitourinary sources were the most common complications.The authors recommended fracture fixation, dbridement,and intravenous antibiotics for all patients, and they recom-mended diverting colostomies and cystostomies as indicated.External fixation can provide provisional stability while allow-ing abdominal access in patients with multiple injuries (Figs.5-A and 5-B).
Special Cases
Polytrauma
Associated injuries are common in children with open frac-tures, especially those of the femur and tibia. Hutchins et al.reported that thirty-three of forty-three children with an openfemoral fracture had associated injuries (most commonlyother fractures)26, and Robertson et al. reported that nine ofeleven children with an open femoral fracture and eighteen ofthirty-two with an open tibial fracture had other majorinjuries66. Cullen et al. reported that 58% of open tibial frac-tures in children treated in their center over a ten-year periodwere associated with other major injuries40.
Motor-vehicle accidents and falls from heights are themost common mechanisms of multiple injuries inchildren.Up to 76% of patients with polytrauma have extremity frac-
tures92, and approximately 9% to 10% of these fractures areopen3,92. Patients with pelvic or vertebral fractures were found tohave an average of five other associated injuries93. In a study of149 children who had sustained polytrauma (a total of 494 in-
juries), Letts et al. identified thirteen missed injuries and fifty-seven complications, most commonly due to fractures94. Onestudy suggested that treatment at a pediatric trauma centermay result in lower mortality, although such centers are not
available in all areas
95.
Polytrauma is a relative indication for the operativetreatment of displaced fracture. Treatment of a patient withpolytrauma with a spica cast limits access to the abdomen forserial examination, and children with a head injury who aretreated with casts are at increased risk for unrecognized skinbreakdown. Early stabilization of open fractures is recom-mended. However, although there is a relationship betweendelayed stabilization of a long-bone fracture, especially one ofthe femur, and an increased risk of acute respiratory distresssyndrome, fat emboli, and deep venous thrombosis in adultpatients with polytrauma, there does not appear to be a simi-lar degree of association in children. Reporting on a series ofseventy-eight children who had sustained polytrauma, Loder
noted that early fracture stabilization decreased stays in thehospital and the intensive care unit, ventilator time, and over-all complications96. In a separate study, Loder et al. found thatchildren with polytrauma in whom a fracture was treatedmore than seventy-two hours following the injury had a trendfor an increased rate of immobilization-related complications,although the increase did not reach significance97.
Traumatic AmputationsTraumatic amputation is the most severe form of open injury.At one Midwestern center, lawnmower injuries were reportedto be responsible for 29% (sixty-nine) of 256 amputations in235 children; farm machinery, for 24% (fifty-seven); motor-
vehicle accidents, for 16% (thirty-eight); train accidents, for9% (twenty); and other mechanisms, for the remaining 22%(fifty-one)98. Seasonal variation in the types of injuries hasbeen noted, with farming injuries being more common in the
Fig. 5-A
Figs. 5-A and 5-B An open pelvic fracture in the setting of high-energy polytrauma. Note that the external fixator on the pelvis allows adequate room
for abdominal swelling and access for operative procedures.
Fig. 5-B
on December 5, 2006www.ejbjs.orgDownloaded from
http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/ -
8/7/2019 Fract Exo Pediat.
14/16
2796
THE JO U R N A LOF BON E & JOINT SU R G E R Y J BJ S .O RG
VO L U M E 87-A NUMBER 12 DECEMBER 2005
OP EN FR A C T U R E S IN CHILDREN
spring and fall and lawnmower injuries seen more frequentlyin the summer months. There are also differences in themechanisms of injury seen at different ages, with most burnsoccurring in younger children and boating injuries occurring
primarily in adolescents.Because of the increased wound-healing ability in chil-dren, every effort should be made to preserve all extremities ofchildren, even those with severe type-III open fractures. Thereis a poor correlation between the Mangled Extremity SeverityScore (MESS) and the need for amputation in a child99. Whenamputation is required, the physis should be preserved with asmuch length as possible. Even a stump that initially appearsvery short after a traumatic amputation in a growing childmay achieve substantial length by skeletal maturity if the phy-sis is preserved.
Children have remarkable regenerative potential that al-lows replantation of some amputated parts that would not besalvageable in adults. Replantation following hand and upper-
extremity amputations require careful postoperative coopera-tion of the patient and family and intensive rehabilitation100.However, replanted structures in children tend to have slightlylower survival rates than those in adults because of lower se-lectivity by the surgeon, less favorable mechanisms of injury(including crush and avulsion mechanisms), and the in-creased technical challenges associated with small anatomicstructures101. Reimplantations also require highly specializedcare that may not be available at all centers.
McClure and Shaughnessy reported that, in a series oftwelve children with a farm-related amputation of an upper orlower limb, an infection developed in all six who had under-gone replantation and in none of those who had not102. Only
two of the six replanted parts survived, with the remainderfailing because of infection or vascular compromise.
Lawnmower InjuriesPower lawnmowers inflict substantial numbers of prevent-able fractures and amputations in children103. In a series ofchildren seen with lawnmower injuries at one center, eight ofsixteen patients had sustained a traumatic amputation, fif-teen of twenty nonamputation fractures involved the foot,and an average of 2.9 operative procedures were required104.Five patients required free-flap transfers for soft-tissue cov-erage. Dormans et al. reported that, in their series of sixteenchildren with lawnmower injuries, all patients with a shred-
ding-type injury had a poor result following limb salvage orultimately required amputation105. In a study of twenty-fourchildren with lower-extremity injuries caused by a ridinglawnmower, Farley et al. reported fractures in eight patients,amputations in ten, and fractures combined with amputa-tions in six106. The patients were an average of 4.7 years old atthe time of injury, and they underwent an average of threeirrigation and dbridement procedures over a two-week hos-pitalization period following the injury. Sixteen children re-quired completion of an amputation, and eleven underwentsplit-thickness skin-grafting of open wounds. Five patientswere treated with open reduction and internal fixation of
fractures, and six underwent closed reduction and cast im-mobilization. Five children required readmission to the hos-pital, and three required a third admission. At the time of athree-year follow-up, the children demonstrated a high level
of athletic ability, but twelve stated that the injury affectedtheir plans and goals for the future.
Long-Term Problems
Some patients with open fractures experience psychologicalproblems and chronic pain. In a long-term follow-up studyof eighteen children with an open tibial fracture, Levy et al.determined that missed school time averaged 4.1 monthsand six children had to repeat a year of school107. Seven pa-tients had a limp, five had chronic pain in spite of osseousunion, and four had nightmares involving the accident. Earlypsychosocial intervention for severely traumatized children maybe helpful to assist the patient and family in coping with the re-covery process.
Overview
Open fractures in children present special challenges. The im-mediate administration of appropriate antibiotics on presenta-tion is crucial to minimize the risk of infection. Formaloperative dbridement of all open fractures is a time-honoredprinciple, although whether operative treatment within sixhours rather than twenty-four hours influences the infectionrate is controversial. Thorough dbridement and irrigation ofthe wound with careful soft-tissue management are recom-mended. Open fractures in children have better healing poten-tial than those in adults. For this reason, tissue of questionableviability should not be dbrided at the first operative interven-
tion. Unstable fractures require some form of fixation, althoughthe fixation does not always need to be rigid, and fixation tech-niques should respect the physis of growing children.
David G. Stewart Jr., MDChildrens Bone and Spine Surgery, 10001 South Eastern Avenue,Suite 407, Henderson, NV 89052
Robert M. Kay, MDDavid L. Skaggs, MDChildrens Hospital Los Angeles, 4650 Sunset Boulevard, MS 69,Los Angeles, CA 90027. E-mail address for D.L. Skaggs:[email protected]
The authors did not receive grants or outside funding in supportof their research or preparation of this manuscript. They did notreceive payments or other benefits or a commitment or agreementto provide such benefits from a commercial entity. No commercialentity paid or directed, or agreed to pay or direct, any benefits toany research fund, foundation, educational institution, or other char-itable or nonprofit organization with which the authors are affiliatedor associated.
doi:10.2106/JBJS.E.00528
on December 5, 2006www.ejbjs.orgDownloaded from
http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/ -
8/7/2019 Fract Exo Pediat.
15/16
2797
THE JO U R N A LOF BON E & JOINT SU R G E R Y J BJ S .O RG
VO L U M E 87-A NUMBER 12 DECEMBER 2005
OP EN FR A C T U R E S IN CHILDREN
References
1. Skaggs DL, Friend L, Alman B, Chambers HG, Schmitz M, Leake B, Kay RM,Flynn JM. The effect of surgical delay on acute infection following 554 open frac-tures in children. J Bone Joint Surg Am. 2005;87:8-12.
2. Iobst CA, Tidwell MA, King WF. Nonoperative management of pediatric type I
open fractures. J Pediatr Orthop. 2005;25:513-7.
3. Buckley SL, Gotschall C, Robertson W Jr, Sturm P, Tosi L, Thomas M, Eichel-berger M. The relationships of skeletal injuries with trauma score, injury severityscore, length of hospital stay, hospital charges, and mortality in children admittedto a regional pediatric trauma center. J Pediatr Orthop. 1994;14:449-53.
4. Rodriguez-Merchan EC. Pediatric skeletal trauma: a review and historical per-spective. Clin Orthop Relat Res. 2005;432:8-13.
5. Parfitt AM, Travers R, Rauch F, Glorieux FH. Structural and cellular changes dur-ing bone growth in healthy children. Bone. 2000;27:487-94.
6. Bartlett CS 3rd, Weiner LS, Yang EC. Treatment of type II and type III open tibiafractures in children. J Orthop Trauma. 1997;11:357-62.
7. Patzakis MJ, Wilkins J. Factors influencing infection rate in open fracturewounds. Clin Orthop Relat Res. 1989;243:36-40.
8. Armstrong PF. Initial management of the multiply injured child: the ABCs. InstrCourse Lect. 1992;41:347-50.
9. Shires GT, Jones RC. Initial management of the severely injuried patient. JAMA.1970;213:1872-8.
10. Herzenberg JE, Hensinger RN, Dedrick DK, Phillips WA. Emergency transportand positioning of young children who have an injury of the cervical spine. Thestandard backboard may be hazardous. J Bone Joint Surg Am. 1989;71:15-22.
11. Chameides L, Hazinski MF, editors. Pediatric advanced life suppor t. Dallas:American Heart Association; 1997.
12. American College of Surgeons, Committee on Trauma. Advanced trauma lifesupport manual. Chicago: American College of Surgeons; 1997.
13. Pryor JP, Reilly PM. Initial care of the patient with blunt polytrauma. Clin Or-thop Relat Res. 2004;422:30-6.
14. Boon JM, Gorry DL, Meiring JH. Finding an ideal site for intraosseous infusionof the tibia: an anatomical study. Clin Anat. 2003;16:15-8.
15. Bielski RJ, Bassett GS, Fideler B, Tolo VT. Intraosseous infusions: effectson the immature physisan experimental model in rabbits. J Pediatr Orthop.1993;13:511-5.
16. Guy J, Haley K, Zuspan SJ. Use of intraosseous infusion in the pediatrictrauma patient. J Pediatr Surg. 1993;28:158-61.
17. Wright R, Reynolds SL, Nachtsheim B. Compartment syndrome secondary toprolonged intraosseous infusion. Pediatr Emerg Care. 1994;10:157-9.
18. Galpin RD, Kronick JB, Willis RB, Frewen TC. Bilateral lower extremity com-partment syndromes secondary to intraosseous fluid resuscitation. J Pediatr Or-thop. 1991;11:773-6.
19. Luman ET, Barker LE, Shaw KM, McCauley MM, Buehler JW, Pickering LK.Timeliness of childhood vaccinations in the United States: days undervaccinatedand number of vaccines delayed. JAMA. 2005;293:1204-11.
20. Talan DA, Abrahamian FM, Moran GJ, Mower WR, Alagappan K, Tiffany BR,Pollack CV Jr, Steele MT, Dunbar LM, Bajani MD, Weyant RS, Ostroff SM. Tetanusimmunity and physician compliance with tetanus prophylaxis practices amongemergency department patients presenting with wounds. Ann Emerg Med. 2004;43:305-14.
21. Rhee P, Nunley MK, Demetriades D, Velmahos G, Doucet JJ. Tetanus andtrauma: a review and recommendations. J Trauma. 2005;58:1082-8.
22. Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thou-sand and twenty-five open fractures of long bones: retrospective and prospectiveanalyses. J Bone Joint Surg Am. 1976;58:453-8.
23. Gustilo RB, Mendoza RM, Williams DN. Problems in the management oftype III (severe) open fractures: a new classification of type III open fractures.J Trauma. 1984;24:742-6.
24. Brumback RJ, Jones AL. Interobserver agreement in the classification ofopen fractures of the tibia. The results of a survey of two hundred and forty-fiveorthopaedic surgeons. J Bone Joint Surg Am. 1994;76:1162-6.
25. Faraj AA. The reliability of the pre-operative classification of open tibial fracturesin children a proposal for a new classification. Acta Orthop Belg. 2002;68:49-55.
26. Hutchins CM, Sponseller PD, Sturm P, Mosquero R. Open femur fractures inchildren: treatment, complications, and results. J Pediatr Orthop. 2000;20:183-8.
27. Wilkins J, Patzakis M. Choice and duration of antibiotics in open fractures. Or-thop Clin North Am. 1991;22:433-7.
28. Dellinger EP, Caplan ES, Weaver LD, Wertz MJ, Droppert BM, Hoyt N, Brum-
back R, Burgess A, Poka A, Benirschke SK, et al. Duration of preventive antibiotic
administration for open extremity fractures. Arch Surg. 1988;123:333-9.
29. Patzakis MJ, Bains RS, Lee J, Shepherd L, Singer G, Ressler R, Harvey F, Hol-tom P. Prospective, randomized, double-blind study comparing single-agent antibi-otic therapy, ciprofloxacin, to combination antibiotic therapy in open fracturewounds. J Orthop Trauma. 2000;14:529-33.
30. Huddleston PM, Steckelberg JM, Hanssen AD, Rouse MS, Bolander ME, PatelR. Ciprofloxacin inhibition of experimental fracture healing. J Bone Joint Surg Am.2000;82:161-73.
31. Gendrel D, Chalumeau M, Moulin F, Raymond J. Fluoroquinolones in paediat-rics: a risk for the patient or for the community? Lancet Infect Dis. 2003;3:537-46.
32. Grady R. Safety profile of quinolone antibiotics in the pediatric population.Pediatr Infect Dis J. 2003;22:1128-32.
33. Drossou-Agakidou V, Roilides E, Papakyriakidou-Koliouska P, Agakidis C, Ni-kolaides N, Sarafidis K, Kremenopoulos G. Use of ciprofloxacin in neonatal sep-sis: lack of adverse effects up to one year. Pediatr Infect Dis J. 2004;23:346-9.
34. Kaplan SL, Hulten KG, Gonzalez BE, Hammerman WA, Lamberth L, Versalovic
J, Mason EO Jr. Three-year sur veillance of community-acquired Staphylococcusaureus infections in children. Clin Infect Dis. 2005;40:1785-91.
35. Zalavras CG, Patzakis MJ, Holtom P. Local antibiotic therapy in the treatmentof open fractures and osteomyelitis. Clin Orthop Relat Res. 2004;427:86-93.
36. Ostermann PA, Seligson D, Henry SL. Local antibiotic therapy for severe openfractures. A review of 1085 consecutive cases. J Bone Joint Surg Br. 1995;77:93-7.
37. Skaggs DL, Kautz SM, Kay RM, Tolo VT. Effect of delay of surgical treatment onrate of infection in open fractures in children. J Pediatr Orthop. 2000;20:19-22.
38. Khatod M, Botte MJ, Hoyt DB, Meyer RS, Smith JM, Akeson WH. Outcomesin open tibia fractures: relationship between delay in treatment and infection.J Trauma. 2003;55:949-54.
39. Kreder HJ, Armstrong P. A review of open tibia fractures in children. J PediatrOrthop. 1995;15:482-8.
40. Cullen MC, Roy DR, Crawford AH, Assenmacher J, Levy MS, Wen D. Openfracture of the tibia in children. J Bone Joint Surg Am. 1996;78:1039-47.
41. Bhandari M, Thompson K, Adili A, Shaughnessy SG. High and low pressureirrigation in contaminated wounds with exposed bone. Int J Surg Investig. 2000;2:179-82.
42. Adili A, Bhandari M, Schemitsch EH. The biomechanical effect of high-pressure irrigation on diaphyseal fracture healing in vivo. J Or thop Trauma.2002;16:413-7.
43. Bhandari M, Adili A, Schemitsch EH. The efficacy of low-pressure lavage withdifferent irrigating solutions to remove adherent bacteria from bone. J Bone JointSurg Am. 2001;83:412-9.
44. Anglen JO, Gainor BJ, Simpson WA, Christensen G. The use of detergent irri-gation for musculoskeletal wounds. Int Orthop. 2003;27:40-6.
45. Anglen JO. Wound irrigation in musculoskeletal injury. J Am Acad Orthop Surg.2001;9:219-26.
46. Anglen JO. Comparison of soap and antibiotic solutions for irrigation of lower-limb open fracture wounds. A prospective, randomized study. J Bone Joint SurgAm. 2005;87:1415-22.
47. Yang EC, Eisler J. Treatment of isolated type I open fractures: is emergent op-erative debridement necessary? Clin Orthop Relat Res. 2003;410:289-94.
48. Iobst CA, Tidwell MA, King WF. Nonoperative management of pediatric type Iopen fractures. J Pediatr Orthop. 2005;25:513-7.
49. Lee J. Efficacy of cultures in the management of open fractures. Clin OrthopRelat Res. 1997;339:71-5.
50. Valenziano CP, Chattar-Cora D, ONeill A, Hubli EH, Cudjoe EA. Efficacy of pri-mary wound cultures in long bone open extremity fractures: are they of any value?Arch Orthop Trauma Surg. 2002;122:259-61.
51. Gopal S, Majumder S, Batchelor AG, Knight SL, De Boer P, Smith RM. Fix andflap: the radical orthopaedic and plastic treatment of severe open fractures ofthe tibia. J Bone Joint Surg Br. 2000;82:959-66.
52. Stewart KJ, Tytherleigh-Strong G, Bharathwaj S, Quaba AA. The soft tissue man-agement of childrens open tibial fractures. J R Coll Surg Edinb. 1999;44:24-30.
on December 5, 2006www.ejbjs.orgDownloaded from
http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/http://www.ejbjs.org/ -
8/7/2019 Fract Exo Pediat.
16/16
2798
THE JO U R N A LOF BON E & JOINT SU R G E R Y J BJ S .O RG
VO L U M E 87-A NUMBER 12 DECEMBER 2005
OP EN FR A C T U R E S IN CHILDREN
53. Bae DS, Waters PM, Montgomery K, Pribaz J. The use of early flap coveragein severe open physeal fractures: a report of two cases. J Orthop Trauma. 2003;17:450-8.
54. Skoll PJ, Hudson DA. Combined pedicled flaps for grade IIIB tibial fractures inchildren: a report of two patients. Ann Plast Surg. 2000;44:422-5.
55. Webb LX. New techniques in wound management: vacuum-assisted woundclosure. J Am Acad Orthop Surg. 2002;10:303-11.
56. Mooney JF 3rd, Argenta LC, Marks MW, Morykwas MJ, DeFranzo AJ. Treat-
ment of soft tissue defects in pediatric patients using the V.A.C. system. Clin Or-thop Relat Res. 2000;376:26-31.
57. Shilt JS, Yoder JS, Manuck TA, Jacks L, Rushing J, Smith BP. Role of vacuum-assisted closure in the treatment of pediatric lawnmower injuries. J Pediatr Or-thop. 2004;24:482-7.
58. Corry IS, Nicol RO. Limb length after fracture of the femoral shaft in children.J Pediatr Orthop. 1995;15:217-9.
59. Blick SS, Brumback RJ, Poka A, Burgess AR, Ebraheim NA. Compartment syn-drome in open tibial fractures. J Bone Joint Surg Am. 1986;68:1348-53.
60. McLauchlan GJ, Cowan B, Annan IH, Robb JE. Management of completely dis-placed metaphyseal fractures of the distal radius in children. A prospective, ran-domised controlled trial. J Bone Joint Surg Br. 2002;84:413-7.
61. Skaggs DL, Hale JM, Bassett J, Kaminsky C, Kay RM, Tolo VT. Operative treat-ment of supracondylar fractures of the humerus in children. The consequences ofpin placement. J Bone Joint Surg Am. 2001;83:735-40.
62. Janarv PM, Wikstrom B, Hirsch G. The influence of transphyseal drilling andtendon grafting on bone growth: an experimental study in the rabbit. J Pediatr Or-thop. 1998;18:149-54.
63. Haasbeek JF, Cole WG. Open fractures of the arm in children. J Bone JointSurg Br. 1995;77:576-81.
64. Luhmann SJ, Schootman M, Schoenecker PL, Dobbs MB, Gordon JE. Com-plications and outcomes of open pediatric forearm fractures. J Pediatr Orthop.2004;24:1-6.
65. Greenbaum B, Zionts LE, Ebramzadeh E. Open fractures of the forearm inchildren. J Orthop Trauma. 2001;15:111-8.
66. Rober tson P, Karol LA, Rab GT. Open fractures of the tibia and femur in chil-dren. J Pediatr Orthop. 1996;16:621-6.
67. Caird MS, Mueller KA, Puryear A. Compression plating of pediatric femoral
shaft fractures. J Pediatr Orthop. 2003;23:448-52.
68. Hedequist DJ, Sink E. Technical aspects of bridge plating for pediatric femurfractures. J Orthop Trauma. 2005;19:276-9.
69. Kanlic EM, Anglen JO, Smith DG, Morgan SJ, Pesantez RF. Advantages of sub-muscular bridge plating for complex pediatric femur fractures. Clin Orthop RelatRes. 2004;426:244-51.
70. Flynn JM, Schwend RM. Management of pediatric femoral shaft fractures.J Am Acad Orthop Surg. 2004;12:347-59.
71. Ligier JN, Metaizeau JP, Prevot J, Lascombes P. Elastic stable intramedullarynailing of femoral shaft fractures in children. J Bone Joint Surg Br. 1988;70:74-7.
72. Carey TP, Galpin RD. Flexible intramedullary nail fixation of pediatric femoralfractures. Clin Orthop Relat Res. 1996;332:110-8.
73. Bar-On E, Sagiv S, Porat S. External fixation or flexible intramedullary nailingfor femoral shaft fractures in children. A prospective, randomised study. JBone Joint Surg Br. 1997;79:975-8. Erratum in: J Bone Joint Surg Br. 1998;80:749.
74. Greisberg J, Bliss MJ, Eberson CP, Solga P, dAmato C. Social and economic
benefits of flexible intramedullary nails in the treatment of pediatric femoral shaftfractures. Orthopedics. 2002;25:1067-70.
75. Buckley SL, Smith GR, Sponseller PD, Thompson JD, Robertson WW Jr, GriffinPP. Severe (type III) open fractures of the tibia in children. J Pediatr Orthop.1996;16:627-34.
76. Hull JB, Bell MJ. Modern trends for external fixation of fractures in children:a critical review. J Pediatr Orthop B. 1997;6:103-9.
77. Tolo VT. External skeletal fixation in childrens fractures. J Pediatr Orthop.1983;3:435-42.
78. Blasier RD, Aronson J, Tursky EA. External fixation of pediatric femur frac-tures. J Pediatr Orthop. 1997;17:342-6.
79. Skaggs DL, Leet AI, Money MD, Shaw BA, Hale JM, Tolo VT. Secondary frac-tures associated with external fixation in pediatric femur fractures. J Pediatr Or-thop. 1999;19:582-6.
80. Domb BG, Sponseller PD, Ain M, Miller NH. Comparison of dynamic versusstatic external fixation for pediatric femur fractures. J Pediatr Orthop. 2002;22:428-30.
81. Birch JG, Samchukov ML. Use of the Ilizarov method to correct lower limb de-formities in children and adolescents. J Am Acad Orthop Surg. 2004;12:144-54.
82. OBrien T, Weisman DS, Ronchetti P, Piller CP, Maloney M. Flexible titaniumnailing for the treatment of the unstable pediatric tibial fracture. J Pediatr Orthop.2004;24:601-9.
83. Flynn JM, Skaggs D, Sponseller PD, Ganley TJ, Kay RM, Leitch KK. The opera-tive management of pediatric fractures of the lower extremity. J Bone Joint SurgAm. 2002;84:2288-300.
84. Kubiak EN, Egol KA, Scher D, Wasserman B, Feldman D, Koval KJ. Operativetreatment of tibial fractures in children: are elastic stable intramedullary nails animprovement over external fixation? J Bone Joint Surg Am. 2005;87:1761-8.
85. Jones BG, Duncan RD. Open tibial fractures in children under 13 years ofage10 years experience. Injury. 2003;34:776-80.
86. Song KM, Sangeorzan B, Benirschke S, Browne R. Open fractures of the tibiain children. J Pediatr Orthop. 1996;16:635-9.
87. Grimard G, Naudie D, Laberge LC, Hamdy RC. Open fractures of the tibia inchildren. Clin Orthop Relat Res. 1996;332:62-70.
88. Blasier RD, Barnes CL. Age as a prognostic factor in open tibial fractures inchildren. Clin Orthop Relat Res. 1996;331:261-4.
89. Court-Brown CM, Byrnes T, McLaughlin G. Intramedullary nailing of tibial dia-physeal fractures in adolescents with open physes. Injury. 2003;34:781-5.
90. Hope PG, Cole WG. Open fractures of the tibia in children. J Bone Joint SurgBr. 1992;74:546-53.
91. Mosheiff R, Suchar A, Porat S, Shmushkevich A, Segal D, Liebergall M. Thecrushed open pelvis in children. Injury. 1999;30 Suppl 2:B14-8.
92. Schalamon J, v Bismarck S, Schober PH, Hollwarth ME. Multiple trauma inpediatric patients. Pediatr Surg Int. 2003;19:417-23.
93. Galano GJ, Vitale MA, Kessler MW, Hyman JE, Vitale MG. The most frequenttraumatic orthopaedic injuries from a national pediatric inpatient population. J Pe-diatr Orthop. 2005;25:39-44.
94. Letts M, Davidson D, Lapner P. Multiple trauma in children: predicting out-come and long-term results. Can J Surg. 2002;45:126-31.
95. Smith JS Jr, Martin LF, Young WW, Macioce DP. Do trauma centers improveoutcome over non-trauma centers: the evaluation of regional trauma care using
discharge abstract data and patient management categories. J Trauma.1990;30:1533-8.
96. Loder RT. Pediatric polytrauma: orthopaedic care and hospital course. J Or-thop Trauma. 1987;1:48-54.
97. Loder RT, Gullahorn LJ, Yian EH, Ferrick MR, Raskas DS, Greenfield ML. Fac-tors predictive of immobilization complications in pediatric polytrauma. J OrthopTrauma. 2001;15:338-41.
98. Loder RT. Demographics of traumatic amputations in children. Implicationsfor prevention strategies. J Bone Joint Surg Am. 2004;86:923-8.
99. Fagelman MF, Epps HR, Rang M. Mangled extremity severity score in children.J Pediatr Orthop. 2002;22:182-4.
100. Buncke GM, Buntic RF, Romeo O. Pediatric mutilating hand injuries. HandClin. 2003;19:121-31.
101. Kim JY, Brown RJ, Jones NF. Pediatric upper extremity replantation. Clin
Plast Surg. 2005;32:1-10, vii.
102. McClure SK, Shaughnessy WJ. Farm-related limb amputations in children.
J Pediatr Orthop. 2005;25:133-7.
103. Robertson WW Jr. Power lawnmower injuries. Clin Orthop Relat Res. 2003;409:37-42.
104. Erdmann D, Lee B, Roberts CD, Levin LS. Management of lawnmower injuries tothe lower extremity in children and adolescents. Ann Plast Surg. 2000;45:595-600.
105. Dormans JP, Azzoni M, Davidson RS, Drummond DS. Major lower extremitylawn mower injuries in children. J Pediatr Orthop. 1995;15:78-82.
106. Farley FA, Senunas L, Greenfield ML, Warschausky J, Loder RT, Kewman DG,Hensinger RN. Lower extremity lawn-mower injuries in children. J Pediatr Orthop.1996;16:669-72.
107. Levy AS, Wetzler M, Lewars M, Bromberg J, Spoo J, Whitelaw GP. Theorthopedic and social outcome of open tibia fractures in children. Orthopedics.1997;20:593-8.