Forensic Psychiatry and Prison Mental Health 2009

of 32
-
Upload
fiona-kumari-campbell -
Category
Documents
-
view
222 -
download
0
Transcript of Forensic Psychiatry and Prison Mental Health 2009
-
7/30/2019 Forensic Psychiatry and Prison Mental Health 2009
1/32
-
7/30/2019 Forensic Psychiatry and Prison Mental Health 2009
2/32
EditorialBy Robert van Voren
Developing Prison Mental HealthServices in Countries in Transition:Challenges, Constraints andOpportunitiesBy Dick Raes and Robert van Voren
Seven Years in Kresti Prison:A Unique Project to Develop Modern PrisonMental Health Services in St. PetersburgBy Konstantin Antsierov, Rob Hollander and Wendy Weijts
Risk Assessment inPost-Soviet CountriesBy Virginija Klimukiene
Developing Partnerships in ForensicPsychiatry: The Pompe Foundation asPartner in GIP projectsBy Thieu Verhagen and Dick Raes
Initiating Reorm in Prison MentalHealth & Forensic Psychiatry inSerbiaBy Robert van Voren
Bulgaria: A European Union MemberLagging Behind in ForensicsBy Petar Marinov and Vladimir Velinov
Convicted Juveniles in GeorgiaProblems and ProspectsBy Lela Tsiskarishvili
From Lunatic Asylum to National Instituteo Mental Health in Sri LankaBy Dr. Neil Fernando, Marieke de Vries, and NanthiniSivanesan
Goals o GIP in Sri Lankas ForensicHospital SystemBy Robert van Voren
Russian SummariesBy Elena Mozhaeva
3
4
10
12
14
16
18
22
25
27
28
EditorEllen Mercer
Editorial BoardKatja Assoian
Elena Mozhaeva
Robert van Voren
Florence Baingana
Margi Kirschenmann
Graphic Design/ PrintingBADE creatieve communicatie
www.bade.nl
Mental Health Reorms is a publication o
Global Initiative on Psychiatry (GIP).
While MHR is distributed ree o charge,we are dependent on your support to
sustain the journal. Contributions arethereore welcome and may be made to:
ABN AMRO Bank
s Gravelandseweg BranchHilversum, The Netherlands
BIC: ABNANL2AEuro account:62.07.29.074
IBAN: NL16 ABNA 0620 7290 74USD account: 62.07.29.244
IBAN: NL82 ABNA 0620 7292 44
To request additional copies pleasecontact:
Global Initiative on Psychiatry
P.O. Box 1282
1200 BG HilversumThe Netherlands
Tel.: +31 35 683 8727
Fax: +31 35 683 3646e-mail: [email protected]
www.gip-global.org
Cover photo: ChernyakhovskSpecial Psychiatric Hospital,
Kaliningrad, Russia
July 2009
Special issue:
Forensic Psychiatry and
Prison Mental Health
A Global InitiativeonPsychiatry publication
09No. 2MentalHealthReforms
MentalHealthReorms
Contents
2
-
7/30/2019 Forensic Psychiatry and Prison Mental Health 2009
3/32
July2009 3
Editorial
In most countries around the globe,mental health service users arestigmatized in ways that can aecttheir quality o lie and position in so-ciety. However, or those who havea mental illness and have also com-mitted a crime, there is a doublestigma: he/she is mad, and bad.Virtually everywhere these individu-als receive less treatment and carethan needed.
Global Initiative on Psychiatry hasbeen involved in the development oprojects in the eld o orensic psy-chiatry and prison mental health orthe past eight years. In those years,we have managed to support theinitiation o reorm in more than hala dozen countries, mainly in EasternEurope and the ormer Soviet Union,but also in Sri Lanka. In addition,there is good reason to believe thatprojects will be implemented in
several other countries in the nearuture.
It is dicult to get programs o thissort started; governments are oten
not very interested in this group o pa-tients they are mad and bad, arentthey? and society usually doesnot like the idea o orensic patientsreintegrating into society ater theirtreatment has been concluded. Themajority o the population believesthat such people should be lockedup as long as possible, preerablyor the rest o their lives. Penitentiarysystems are, by denition, repressive
in nature, and prisoners with mentalhealth problems are oten consideredto be simulators who should be dealtwith in only one way: put them undersuch horrible living conditions thatthey want to go back to their regularcells as soon as possible.
Part o the work o Global Initiativeon Psychiatry is to convince authori-ties to take prison mental health andorensic psychiatry seriously. First oall, orensic psychiatric patients who
have not received adequate treat-ment remain a threat to society, so itis in the interest o the population asa whole that good orensic psychi-atric care programs are developed.
Prisoners with mental health prob-lems badly aect the atmosphere inpenitentiary acilities which may, inturn, lead to security risks. In addi-tion, bad treatment and living condi-tions almost invariably lead to humanrights violations, and it is the duty oeach government to do everythingpossible to prevent such violationsrom taking place.
We realize that our job is not an easyone; yet over the past years, we haveseen many positive developmentsand concrete results o the work oour partners and ourselves. Thisissue o our journal Mental HealthReorms provides you with a kalei-doscope o such projects, dealingwith a wide range o issues in diversecountries. We do not attempt to coverall that has been accomplished oris being accomplished but we dohope that this issue provides the
reader with a good overview and, bydoing so, convincingly argues whythis work needs to be undertaken.Robert van Voren
-
7/30/2019 Forensic Psychiatry and Prison Mental Health 2009
4/32
July2009 4
Developing Prison Mental Health Servicesin Countries in Transition: Challenges,Constraints and Opportunities
In most countries - including those that meet the criteria or
democracy- the execution o criminal law, its procedures and its
institutions can be characterized as a rather closed system.
A closed system in this sense is regarded as a complex o
interdependent organizations, regulations and acilities within
society, but with ew possibilities or society to have insight,
control and inuence concerning what is really going on within
this system. At the same time, this system, including the criminal
law, is usually a reection o the attitude o governments,
politicians and citizens towards crimes and criminals.
Legislation in each country should be regarded as the source o
protection o rights, i.e. the psychological, physical and material
integrity o each individual citizen. Criminal law provides the cri-
teria, procedures and measures or punishment o persons who
violate the above-mentioned rights and integrity. The criminal law
should address the criteria o proportionality and efciency and
should also saeguard the legal rights o the individuals who are
conronted with the criminal law.
When a person is ound guilty o an oense, the aims o punish-
ment are retaliation, as well as specifc and general prevention,
including probation and rehabilitation especially ater prison
sentences, to prevent recidivism. The closed system o the crimi-
nal law, its procedures and institutions stretches rom the time
the suspect is brought to a police station to his/her release rom
prison.
This article pays attention to the prison system as part o a chaino provisions within the criminal law, the inuence o the peni-
tentiary system on prison mental health and provides examples
o eorts to improve prison mental health care in countries in
transition.
By Dick Raes and Robert van Voren
Prison mental health as
part o a consecutive chain
o provisionsEach person under suspiciono having committed an oenseshould be considered not guiltyuntil an independent court has as-
sessed his guilt and pronounceda verdict. This implies that such a
person should be treated accor-ding human rights standards.
The career o a suspect usuallystarts when he is brought to a police
station and possibly ormally arres-ted and taken into custody. There is
hardly any control on the manner inwhich police ocers deal with suchindividuals. Next, the investigationphase starts when evidence aboutthe oense in question is collected.
Keys to Kresti
Prison Ward
-
7/30/2019 Forensic Psychiatry and Prison Mental Health 2009
5/32
The main part o this investigationconsists o interrogation o the sus-pect. In many countries, the crimi-nal investigators can interrogate theindividual without his having beneto an attorney. They will try to get aconession, sometimes using meth-ods that are not allowed according
international standards. The writtenreport by the interrogators is notalways a true representation o howa conession was achieved and isbeyond control o the court. A wellknown error during the investiga-tion is the so called conrmationbias: the investigators are selec-tively looking or inormation whichconrms their suspicion and tendto neglect inormation that orms anindication o the innocence o thesuspect.
The public prosecutor is respon-sible or what takes place duringthe investigation phase and has toprepare the indictment or the courtsession. It should be stressed thatthe state is and remains responsi-ble or the physical and psychologi-cal condition o the suspect. Whenneeded, he should get the samemedical/psychological care as hewould i not in custody.
In cases o more serious oenses,
the suspect will be admitted to apre-trial prison (or remand prison),in most countries a penitentiary a-cility with a very restricted regime.The time spent in a pre-trial prisonshould be as short as possible,depending on the time neededor preparation o the case or thecourt session, the seriousness othe oense and the risk that thedeendant will escape and hide inorder to avoid urther prosecutionand sentencing.
During the trial, the court will inter-rogate the deendant, eventual wit-nesses and evaluate other aspectso proo, as presented by the publicprosecutor. During the court ses-sion, there should be a so-calledbalance o power, meaning thatthe deendant and his lawyer haveequal rights to access all materialcollected by the public prosecutorand the lawyer o the deendanthas the right to cross examine the
witnesses and to bring orward hisown witnesses. In many countries,this balance o power does not ex-ist and the public prosecutor is themost powerul party during the trial,
especially in Russia and the newindependent states o the ormerSoviet Union. Basically the mem-bers o the court should be inde-pendent, but in many countries thismight not be true (e.g. appointedselectively by the government). Incase the deendant is convicted
o the crime and sentenced toprison, he will be sent to a laborcamp or another penitentiary acil-ity, oten ar away rom his place oresidence.
It should be clear that this chain oacilities and provisions put a heavypsychological burden on the deen-dants and convicted persons, es-pecially or people who are alreadysuering rom mental problems.They are robbed o most o theircivil rights, the circumstances inthe prison system are usually verypoor, medical and psychologicalassistance is oten non-existentand there is no possibility or theindividual to complain about thetreatment he/she receives. Manyinternational studies have shownthat the number o oenders suer-ing rom minor or major psychiatricdisorders is very high (the mad andbad).
In general, this chain o regulations
and acilities is very repressive; aprison sentence robs one o his/herreedom. But the circumstanceswithin this chain add a lot o extrasuering. Prison mental health careshould deal with all elements o thischain, starting at the police station.Trying to improve one element othe chain will likely raise resistancein other parts o the chain. Chang-ing legislation is not enough. Imple-mentation o a more humane ap-proach in the whole chain is more
important, otherwise it will remainas window-dressing.
The infuence o the peni-
tentiary system on prison
mental health
People who enter the criminal jus-tice system run the risk o beingconronted with all kinds o nega-tive psychological eects becauseo the way the system deals withthem.Being taken away rom home with-
out the possibility o contact withtheir nearest amily, being bullied atthe police station, the stress o be-ing interrogated in certain ways, thelack o psychological and juridical
assistance, the uncertainty aboutthe uture, including the result othe court session and ending up ina repressive prison climate, otenin crowded cells without any pri-vacy. As mentioned earlier, quitea number o oenders are alreadysuering rom mental disorderswhen entering the criminal justicesystem. Forms o need assessmentare absent. Quiet prisoners are thebest prisoners.
The psychological eects o impris-onment are well known: depression,sel harm, suicidality and com-pleted suicide. These conditionsare increased because o bullyingby guards and other prisoners,ending low on the pecking order
list that exists in every prison, ag-gressive and sexual assault. Theseindividuals oten urther experienceanger without outlet because othe repressive and dehumanizingregime, isolation rom their nearestand dearest, lack o contact withthe outside world, poor hygienicand nutritional conditions accom-panied by increased vulnerabilityor all kind o contagious diseases.
To insure the rights and the needs
o individual prisoners, the peni-tentiary system should developwithin the system a dierentiation inregimes, based on the availabilityand the level o medical/psycho-logical/psychiatric/nursing care.This dierentiation should be madeor special groups o vulnerableprisoners: prisoners with mentaldisorders, with learning disabilities,adolescents, rst oenders, pedo-philes and other child molesters.
The criminal law and its proceduresshould insure high quality pre-trialpsychiatric assessments to makea distinction between deendantswho are non- or diminished ac-
5 MentalHealthReorms
Exterior o
Kresti Prison
1 S. Fazel & J.
Danesh, Seriousmental disorders in23000 prisoners: asystematic review o62 surveys, Lancet2002, 545-550
-
7/30/2019 Forensic Psychiatry and Prison Mental Health 2009
6/32
July2009 6
countable or the crime or whichthey are indicted, based on theirmental status while committingthe crime. The psychiatrists andpsychologists involved in such as-sessments should be independentexpert witnesses to the court andnot contribute to the investigations
o the public prosecutor. Whenthe court accepts the non- or dimin-ished accountability, these personsshould not be punished in a regularprison but reerred or treatmentto special orensic psychiatrichospitals.
The starting point: condi-
tions in penitentiary insti-
tutions in the NIS at the
end o the 20th century
The history o the Soviet Uniono the twentieth century is one obloodshed, terror and mass deten-tion o large segments o society,starting with the revolutions o theRussian Empire in 1917, a viciouscivil war with mass arrests, and ol-lowed by the State terror unleashedby Stalin in 1924. By 1941, one-tenth o the population was incar-cerated in a vast Gulag o campsscattered all across the country,but predominantly in the endlessstretches o orests, tundras anddeserts o Siberia and Central Asia.
Millions o citizens were murderedby execution or hard labor in orcedlabor projects.
During the Second World War, mil-lions o Soviet citizens again per-ished as a result o acts o war, theNazi-German killing machine andthe unrelenting meat grinder o theNKVD. The next phase o historysaw a new wave o terror that sentmillions o so-called collaboratorsto the camps. And shortly beore
the death o Josi Stalin, anotherwave o terror was under prepara-tion. The Doctors Plot, allegedly aplan o Jewish doctors to kill Sta-lin, was, in reality, concocted bythe NKVD in order to make massarrests, in particular o people oJewish background.
In 1953-1955, millions o prison-ers were set ree, and many o theGulag camps were abandoned.NKVD director Lavrenti Beria was
executed as were many o his ac-complices, and successor NikitaKhrushchev publicly denouncedthe terror that his predecessor hadunleashed against his nation or
more than twenty years. However,millions o people remained in thecamps, either because they wereconsidered to be hostile to theSoviet regime, or because theirorced labor was needed or theeconomy. Much o the constructionand industry in Siberia was devel-
oped by orced laborers and com-pletely ending this ree workorcewould have ruined the country.
The rst description o the Gulagater Stalin was written by AnatolyMarchenko, and published in 1969.Marchenkos book showed thatalthough the regime had sotenedand mortality rates in the deathcamps o Vorkuta and Kolymahad decreased considerably, liein the Soviet penitentiary systemremained harsh and dangerous.In the 1970s, most dissidents wereincarcerated in the prison o Vladi-mir and the camps in Mordovia,later Chistopol prison became themain prison or politicals whilemale political prisoners were sentto the camp complex near Perm;Mordovia was then earmarked oremale political prisoners.
Ater the death o Stalin, out-right torture o political prisonersstopped. Indirectly, however, torture
or maltreatment continued throughinhumane living circumstances,dangerous working conditions,malnourishment and insucientmedical care. However, lie orcriminals was usually more di-cult, and since ordinary prisonershad no ambassadors in the West,their maltreatment went much lessnoticed. In the mid-1980s, how-ever, lie or political prisoners alsohad become much more dicultand the number o deaths in-
creased quickly. In protest againstthe bad living conditions, AnatolyMarchenko, then serving a termo teen years o camp and exile,went on hunger strike, which costhim his lie in November 1986. Hisdeath triggered the release o allpolitical prisoners in the USSR.
Throughout the Soviet period, andactually up to this very day, the phe-nomenon o vor v zakone ormedan integral part o lie within the
penitentiary system. Vor v zakoneis best described as a separatecriminal class that placed itsel out-side regular society and maintainedits own hierarchy and laws. Vor v
zakone was a potent orce withinthe penitentiary system; they main-tained a strict regime and deter-mined to a large degree the qualityo lie in a cell or barrack: who sleptwhere and with whom, who gotthe best ood and other privileges.The act that they maintained strict
discipline made them an ally o theadministration, and oten their orcewas used as a means to keep disci-pline, the way the Nazis made useo kapos. Even though these werehardened criminals with severepunishments or those who broketheir laws, they also had a romanticair surrounding them. Their attitudeo untouchability was enhanced bythe many tattoos on their bodies,indicating their crime history andvarious preerences, rom sexual topolitical. Although the power o thevor v zakone is not as strong asit was in Stalin times, they currentlyremain a orce to be reckoned with,and their relationship with the ad-ministration is a combination orespect, ear and collaboration.
Another important aspect o thepenitentiary system in the (ex-)USSR worth mentioning is that otransit prisons. Camp memoirs areull o horrendous stories about liein these prisons. Prisoners weresometimes or weeks and evenmonths na etap, in transit, and
moved rom one transit prison to thenext. The prisons were oten hugeholding tanks with large commu-nal cells where dozens o prisonersare locked up together, oten underthe rule o the vor v zakone andwhere living conditions are suchthat by the time prisoners reachedtheir nal destination they areexhausted and in bad health. Put-ting a prisoner on a lengthy etapcould and was used as a orm opunishment, and a very eective
one indeed.It is this penitentiary system thatormed part o the heritage o theSoviet Union when the country col-lapsed in 1991 and ell apart into
The history of the Soviet Union
in the 20th Century is one of blood-
shed, terror and mass detentions oflarge segments of society.
>
>
2 Probably the bestdescription o Sta-lins regime o terroris Conquest, R., TheGreat Terror, Pimlico,UK., 1992, a revisededition o his originalbook with the sametitle published in1968.
3 Marchenko, Anatoly,My Testimony, PallMall Press, London1969.
-
7/30/2019 Forensic Psychiatry and Prison Mental Health 2009
7/32
teen separate countries. The waythe countries dealt with this heritagediered rom one country to theother, but without exception they allstill suer rom the Soviet past.
Case study: changing at-
titudes within a resisting
system (Russia)It was an alcoholic representativeor human rights o President Putinin North-West Russia who openedthe doors to Kresti prison or us. Hehad recently been to the psychiat-ric department o Kresti prison inSt. Petersburg, the largest pre-trialprison in Europe that at that timeheld close to 12,000 prisoners. Hehad let in shock, and rom conver-sations it was clear that his indig-nation was sincere, the situation inthe psychiatric department o Krestiprison had really touched him.
And there was reason enoughor that. About three hundred typsychiatric patients were crampedtogether in small moist cells, wherewater was running down the walls,ventilation was absent and wherein winter it was too cold and insummer too hot. Sometimes morethan nine persons were locked upin one cell o two by three meters,sometimes with only six bunks.
That meant sleeping in turns andtwenty-three hours behind lockeddoors, with the only relaxation be-ing one hour airing in a small court-yard that only oered a view to thesky. The stench was unbearable,ood outright disgusting, prisonerswere seriously neglected and whena psychosis would result in toostrong reactions, the prisoner con-cerned would be isolated and tiedto a rusty metal bed rame becausemedicine was unavailable.
Our conversations with the prison di-rector went unexpectedly smoothly;he had the impossible task o run-ning an overcrowded prison withoutsucient support rom Moscow,and, at the same time, trying to hu-manize conditions. All support waswelcome, he said, and he acceptedit with open arms. The task aheadseemed to be an impossible one. Itwas very clear that the psychiatricdepartment needed a thorough re-
construction. In addition, sta wasinsucient, medicine almost neveravailable and the space made itcompletely impossible to createany therapeutic environment. What
7 MentalHealthReorms
ollowed were years o negotiating,sometimes without any result. Evenwhen the unds were released, wecouldnt do anything becauseevery step orward was blocked un-til we delivered. Delivering meantto pay bribes and when we reused,the project came to a standstill
In the end, we managed to nd away out o this dilemma, and ateralmost our years o struggling wecould see our temporary success:the reconstruction o the psychiat-ric department had been nishedand the new unit could be opened.True miracles had happened. Whatbeore had been a dark, moistcave now had been transormedinto a prison department that couldalso have t in a prison in WesternEurope. The architects had suc-ceeded bringing in much moredaylight, as a result o which thecentral part looked much nicer. Thecells were dry, well heated, and thenumber o beds had been reducedto maximally our per cell. On topo that, tness equipment had beenplaced in the department, as wellas table tennis and other games;a revolutionary development in aprison system that hadnt changedsince the beginning o the twentiethcentury.
For several months, the sta o thedepartment carried out a daytimeprogram or the psychiatric patientslike nowhere else in Russia. Pris-oners were taken out o the cell insmall groups, played table tennis,exercised on the tness equipmentor played chess at the tables in thecenter court between the cells. Atruly humane department had beencreated within a terribly repressiveprison system. It seemed our proj-
ect had nally succeeded.
Unortunately, Russia wound upincreasingly in dictatorial waterswhich had immediate conse-quences or the Kresti project. Theprojects main goal was to bringabout attitudinal change, exactly inthe opposite direction than that ocurrent Russian politics. We strivedto humanize the system, to help thepenitentiary system start dealingwith prisoners with mental health
problems as human beings, to seethem rst as patients, and only aterthat as prisoners. However, the sys-tem continued to view the person asa criminal, someone who needed to
be taught a lesson. The ill prisonerwas preerably seen as being asimulator; with the worst simulatorbeing the prisoner who pretendedhe had a mental illness. He wasdealt with double harshly, and wasoten locked up under even moreinhumane circumstances than therest.
Change in leadership o the peni-
tentiary system in St. Petersburgendangered the project even more.It was probably a combination oorders rom Moscow to straightenthings out and the natural reactiono a leader in such a repressiveorganization to create ear througha temporary reign o terror and toshow who is boss. Using a confictwith one o the prisoners as a pre-text, the prison administration tookthe tness equipment away andstopped the day program, allegedly
because an aggressive patient hadmade all this impossible. But atera while the day program resumed;this cycle repeated many times.
Kresti Prison
Psychiatric
Ward Beore
and Ater
Renovation
4 The best books onthe subject are Bal-daev, D.S., TatuirovkiZ a k l y u c h e n n y k h ,Limbus Press, St Pe-tersburg, 2001, andLambert, Alex, Rus-sian Prison Tattoos,Schier Publishers,Altgen PA, 2003
5 See or instanceAppelbaum, Anne,Gulag A History,Penguin, London,2003, pp.261-270,and Solzhenitsyn,Aleksandr, The Gu-lag Archipelago I,Harper & Row, NewYork, 1973
6 An extensive de-scription o the transitcamps and their e-ect on the prisonerspsychological and
physical state can beound in the chapterThe Pots o the Gu-lag Archipelago inA. Solzhenitsyns TheGulag Archipelago I.
The projects main goal was
to bring about attitudinal change,
exactly opposite of current Rus-
sian politics.
>
>
-
7/30/2019 Forensic Psychiatry and Prison Mental Health 2009
8/32
July2009 8
This was our dilemma. Is it at allpossible to hope that Russia willbecome more humane, or do wehave to accept that a democraticRussia has or the time being be-come a ata morgana again? Thearticle by Konstantin Antsierov,Rob Hollander and Wendy Weijts
ollows with some additional detailson this project.
Case study: indierence
as the main obstacle
(Lithuania)
Lithuanians are a proud people,proud o their history and alsoproud o their constant resis-tance to oreign oppressors. InSoviet times, it was a Lithuanianunderground publication that waspublished uninterruptedly until thecollapse o the regime; the Lithu-anians were the rst to declarethemselves independent in 1990,and managed to hold on in spiteo strong pressure, an economicblockade and military action bythen-President Gorbachev. Inorder to prevent a storming o theparliamentary building, ocialsplaced huge concrete orticationsaround the building - a portion owhich is still visible in the orm o amonument.
In 2004, Lithuania joined NATO andthe European Union. It was truly amilestone in the history o the nation,marking a denite reintegration intoEurope and ending the ear o u-ture Russian domination; yet, at thesame time, it also marked the end tomany o the reorm processes. Ateraccession to the European Union,the developments in the countryslowed down and eventually cameto a standstill.
The penitentiary system in Lithu-ania was inherited rom the SovietUnion as an outdated network oprisons and labor colonies, and aworkorce that had been educatedas a Soviet militarized machinery tokeep prisoners locked up and outo society. In the late 1990s, manyyoung people joined the peniten-tiary service and questioned manyo the approaches. These youngpeople had enlightened mindseducated in post-Soviet Lithuania
with additional trainings abroad.They started introducing new ser-vices such as those or prisonerswith alcohol and substance abuse,and humanized lie in many o the
places o detention. Clearly, sinceindependence, the Lithuanianprison system made enormousprogress in shedding the Sovietpast and strives to reach Europeanstandards as soon as possible.
At the same time, it is also clear that
much work still needs to be doneand that prisoners with mentalhealth problems are no less stig-matized in the prison system thanin society at large and that extraeorts are needed to change thatsituation. In spite o assurancesthat new premises will be built, theprison psychiatric department is stillhoused in the pre-trial investigationprison in Vilnius (Lukiskes prison).Symbolically, the psychiatric de-partment has the worst possibleaccommodation in this acility - ina wing o the pre-trial prison butunder much worse conditions thanthe pre-trial prison acility itsel orthe rest o the prison hospital. Thecells are damp without any ventila-tion, housing our to ve prisonersin one cell. The department hassucient medication available, butthe quality o services provided isquestionable. The perimeter is sur-rounded by ve ences and walls,with prison dogs running aroundbetween the rst ence and the
actual prison building, creating aneerie atmosphere with their con-stant barking.
It is hard to explain why a EuropeanUnion country such as Lithuaniahas no interest in improving prisonmental health services and endingsuch unacceptable conditions in aprison located less than 500 me-ters rom the Lithuanian parliamentbuilding. Protests and complaints,including by a WHO delegation in
2005, have not led to any results.Persons with mental illness are no
priority, and neither are imprisonedcriminals; those who are a combi-nation are double stigmatized, andsuer the consequences.
Case study: when desire
exceeds the possibilities
(Georgia)
Georgia also inherited a Sovietpenitentiary system, housed in di-lapidated buildings with some o themost inhumane living conditions wehad seen over the years. In no waycould a therapeutic atmosphere beestablished in the existing premises,the proessional level o the ewavailable sta was excruciatinglylow and the conditions were so badthat, in our view, only one solutionwas possible: close the departmentdown and start a new one some-where else, under better conditions.
We had been asked by the Geor-gian Ministry o Health to reormorensic psychiatric services in thecountry ater a corruption scandalhad resulted in the dismissal o allorensic psychiatrists by the Minis-ter; yet the Ministrys understandingo the scope o their request wasminimal. We were acing not only lowproessional standards, corruption,lack o proessionals and bad livingconditions, but also the absence o
collaboration between the Ministrieso Health and Justice and completelack o coordination within the minis-tries themselves.
What we had, however, were veryenthusiastic and reorm-mindedocials, including actively involveddeputy ministers and young mentalhealth proessionals. The ministersand their deputies also were young,which resulted in an interestingcombination o lack o experience
in governance, a quick grasp o theneeds due to rst-class Westerneducation, and a drive to changethings overnight.
However, there clearly was nochance o a quick solution to theimmense problems. We decidedthat the only way to help Georgiastructurally and sustainably wasby dealing with the issue in an all-encompassing manner, tackling thewhole chain o services. Georgia
became the only country wherewe managed to take this global ap-proach. An inter-Ministerial commit-tee was established, that met on aregular basis, involved all stakehold-
Typical
PsychiatricPrison Cell
-
7/30/2019 Forensic Psychiatry and Prison Mental Health 2009
9/32
9 MentalHealthReorms
ers including the deputy ministers ohealth and justice and discussed allthe issues collectively. Ater somecompromises, many decisions weretaken during these meetings.
In the course o our years, we man-aged to agree to develop a new
pre-trial assessment center in Tbilisi,built with Georgian money and ac-cording to European standards,the result o collaboration betweenDutch and Georgian architects.With a delay o hal a year due to theAugust Russian-Georgian war, wenow expect the center to open be-ore the end o 2009. Also, renova-tions started at a newly establishedcentral orensic psychiatric acility inQutiri, and in spite o the war, recon-structions are continuing, again withGeorgian unds. And, last but notleast, an agreement was reachedto open a new prison mental healthdepartment in the newly built prisonin Gldani just outside Tbilisi, andhopeully also this department willbe opened in 2009.
Trainings were organized or doc-tors, nurses, social workers and oth-er personnel, including the guards.A permanent link was establishedbetween a Dutch orensic psychiat-ric hospital and the hospital in Qutiri,
and an agreement was reachedwith the Georgian government thatGIP will provide intellectual support,while all construction and materialneeds will be nanced by the Geor-gian government. Until now, theyhave stuck to their word. A true pro-essional exchange has developedwith the Georgians; implementationo the projects is based on real part-nership.Prison mental health as a
mirror o society: what isachievable in the coming
years?
The criminal law, its procedures andinstitutions, constitutes a closed sys-tem within the wider system o soci-ety, including politicians, bureaucratsand citizens. To start with the peni-tentiary system, the way the directordeals with his sta will be refectedin other layers o his organization, toend up with the attitude o the guardstoward the prisoners.
Where democracy is lacking, thereare hardly any possibilities o infu-encing the existing system. Eventualchanges should be implemented
top-down, but are even more dicultthan the opposite: changes rombottom-up. Basically, eorts to bringabout change should be aimed atall levels o a society but will meeta lot o resistance. For example, it isamazing that the expansion o theEuropean Union to include countriesin Eastern Europe neglects humanrights related to the ate o prisonersin these countries. Obviously thesehave a very low priority.
Nevertheless, NGOs try to nd like-minded partners in these countriesto create ways (and money) to workrom the bottom o the penitentiarysystem to bridgeheads higher inthe hierarchy. As described above,these eorts are not always success-ul and these changes take a lot otime, because experience shows
that changes only can be achievedin very small steps orward.
Conclusion what lessons
can be learned
It is our view that each project con-cerning the improvement o prisonmental health requires extensivepreparation to make the project ap-
plicable in each dierent country.Preerably this preparation shouldbe carried out together with localpartners who want to participate aschange agents. During this prepa-ration, attention should be paid topossible changes in each part othe chain that has been describedabove. Support o the project by theministries involved is very importantin the sense that the bureaucracytakes his own responsibility in theprocess o change. Unortunately,the regimes in these countries arenot as stable as we would like orimplementing the projects and theirsustainability.
Dick Raes is Proessor in Forensic
Psychiatry, member o the board o
GIP and his email is: d.raes@wxs.
nl. Robert van Voren is Chie Execu-
tive o Global Initiative on Psychiatry.
His email address is rvvoren@gip-
global.org. .
Editors Note: For urther back-
ground (and ascinating reading),
please note the attached inormation
o a new book by Robert Van Voren:
Lukiskis
Prison, Vilnius,
Lithuania
-
7/30/2019 Forensic Psychiatry and Prison Mental Health 2009
10/32
10 MentalHealthReorms
Seven Years in Kresti Prison:A Unique Project to Develop Modern PrisonMental Health Services in St. Petersburg
As mentioned in the previous
article, in 2002, a unique coop-
eration started between Dutch
and Russian proessionals
working in the prison system.
The goal o this project was
to improve the care or men-
tally disturbed prisoners in the
Kresti-prison St. Petersburg -
NW region Russian Federation.
Because o the uniqueness o
this project, we would like to
make a ew additions rom our
own experiences.
By Konstantin Antsierov, Rob
Hollander and Wendy Weijts
Activities or
Prisoners in
Kresti Prison
Psychiatric
Ward.
Photo taken by
Theo Lammers
The Kresti prison, built in 1827,is one o the largest prisons inEurope. At the banks o the riverNeva, the prison was originallybuilt or 950 prisoners. During ourrst visit, 12,000 prisoners wereheld in Kresti, and by the time ourproject started, still approximately7400 prisoners were detained. Inthe Kresti, there are several wardshousing prisoners with HIV/AIDS(1200), prisoners with tuberculosis(700) and prisoners with severe
psychiatric disorders (270).
We would like to point out here thatthe renovation o the prison ward,our rst priority, was accomplishedmostly through the work o the con-victed prisoners. They constructedtwo types o cells within the ward.One type o cell was built or pa-tients in an acute psychiatric phaseand hosted two prisoners. Theother type o cell was or stabilizedpatients and hosted our prisoners.
The light green walls, the windows,the clean environment and theequipment or activities made thetotal metamorphose complete. Thenew psychiatric department now
meets the international constructionstandards or prison mental health.
The daily activities introduced havebeen mentioned previously; thoseactivities were planned to create asense o purpose into the lives othe mentally disordered detainees.Through oering them regular andmeaningul activities in their lives,their sel-esteem would be raised. Itis also important to note that theseactivities create some ideal mo-
ments or observation - observa-tions that lead to very useul insightsand can be used in the assessmento behavior and possibilities otreatment o the (individual) patient.In the past seven years, we spokeabout this subject with many o ourRussian colleagues. Many timesthese talks seemed as useless asthe daily lives that the patients haveto endure. But, in the end, therewere some success stories to betold: daily programs or patients
were introduced and requently thepatients are now undertaking moremeaningul activities with eachother. As we have recently beentold, this is a unique development
in the Russian prison system.
It is hard to determine i and howall attitudes will be changed be-cause o this project. In the Rus-sian prison system, the convictedprisoners (sanitary) play a veryimportant role. The authoritiesconsider them as personnel orthe prison and they are employedin many dierent jobs. Not only dothey do the cleaning, cooking andmaintenance work, oten they are
also responsible or the securitywithin the prison. Once we visiteda prison with only eight guards whowere responsible or 2000 inmates.In reality, this is not manageable orthe guards, so special prisoners areassisting those guards in dierentways. The system where convictedprisoners take care o other pris-oners is highly undesirable but aharsh reality due to a lack o moneyor the prison authorities.
In the Kresti, the sanitary assist thedoctor in his/her consultation withpatients on the psychiatric prisonward. The sanitary are also respon-sible or discipline amongst the
-
7/30/2019 Forensic Psychiatry and Prison Mental Health 2009
11/32
July2009 11
patients with mental disorders. De-spite our eort to establish a xedteam o guards who are trained todeal with mentally ill prisoners, wedid not succeed in this. In the end,we chose to develop an instruc-tion manual or the sanitary thatwork in the psychiatric ward and
discussed the selection criteria othose sanitary with the prison di-rector. This manual was printed onbig key-shaped plastic cards. Thesymbolism o these keys is to opendoors and gave a small entranceto the psyche. The keys gave shortinstructions about how to deal withinmates with psychiatric problems.For example: how can one man-age his attitude when a prisoneris anxious or depressed. The keysmay result in attitude changes o thesanitary on the psychiatric depart-ment and give some sustainability.
The Kresti prison annually receivesmore than 3500 prisoners. It isimpossible or the psychologist tosee all new prisoners so we intro-duced a screening instrument todetect psychiatric problems at anearly stage. In a pilot setting, wehave trained some junior inspec-tors in using the questionnairewith newly arriving prisoners. Theoutcome o the screening can be
an indication that the new prisonerneeds consultation o the psy-chologist. The prison authoritiesound this screening instrument
eective and ecient and supportimplementation.
During the project we tried to in-troduce the subject prison mentalhealth in the Russian system. Wevisited the Pushkin Institute that isresponsible or training prison sta
throughout the Russian prison sys-tem in order to establish some sorto collaboration. Unortunately, thiswas an unullled goal.
Recommendations
Working in the Russian prison sys-tem is oten a matter o patience,improvising skills and good per-sonal relationships with importantkey holders. During this project,many o the key holders changed.One example is that the Kresti gota new director who was not as en-thusiastic as the ormer one. Thisresulted in a temporary withdrawal
o the day program and recreation-al acilities. It took a considerableamount o time or him to agree andsupport the project, especially the
day program. We had some niceconversations and peppered dis-cussions. Sometimes it elt like twosteps orward and one step back.However, every visit ended with atoast o vodka and the words: toour riendship.
In order to implement new meth-ods, those methods must beadapted to the Russian situation.The rst reaction rom the authori-ties is oten a negative one indicat-ing that they cannot implement newmethods; but when we insisted,their opinions changed complete-ly. We also needed to be fexiblein our approach; many times, weencountered changes within ourprogram and had to keep rombeing rustrated while adaptingto the new situation. Ater sevenyears o work within the Kresti, wedeveloped some unique relation-ships and accomplished many oour goals. This was not possiblewithout the support o many. Weare very thankul or that.
Konstantin Antsierov is the GIP
representative in St. Peters-
burg and his email address is
[email protected]. Wendy
Weijts and Rob Hollander work in
the Dutch prison mental health ser-
vice and are active in many o GIPs
projects. They can be reached at:
and [email protected].
>
>
Instruction
Manual or
Kresti Prison
Psychiatric
Ward.
Photo taken by
Theo Lammers
It is impossible for the
psychologist to see each of the
3500 patients who come to
Kresti each year.
>
>
-
7/30/2019 Forensic Psychiatry and Prison Mental Health 2009
12/32
12 MentalHealthReorms
Risk Assessment in
Post-Soviet Countries
A risk assessment is a statementon the likelihood that a certain un-desirable event will take place inthe uture.1 Risk assessment is aroutine practice in the eld o oren-sic psychiatry: every 6 months, thecourt receives the reports rom thehospital and must make decisions,based on these reports, as to eitherprolong the present compulsorytreatment measures or to changethem into lighter or stricter ones. Inmost o the post-Soviet countries,the court will release a orensicpsychiatric patient rom the hospitalonly when it is obvious that the men-tal state o the patient has changed;in other words, when his/her risk oreoending is signicantly reduced.However, one could argue that thechanges in mental state and the re-duction o risk to reoend is not thesame. These actors depend on theapproach to Mental Health we take
as a baseline: a biological approachemphasizes the medical treatmento mental disorder as a keystoneto prevent criminal behavior in theuture. A bio-psycho-social ap-proach to Mental Health takes intoconsideration all biological, socialand psychological actors, whichdetermine (uture) oenses, there-ore a reduction o risk will be relatedto both medical treatment and re-socialization, i.e. management o allrisk actors.
Post-Soviet countries gained theirindependence 15-18 years agoand have taken their unique way odevelopment. However, the neigh-boring countries oten take rathersimilar steps and speed in develop-ment. Taking into consideration thelack o the precise knowledge aboutthe situation o risk assessment inevery particular Post-Soviet country,the author presumes to group thecountries and present one state
rom each group: the Baltic Statesin this article will be representedby Lithuania; Russian Federation,Republic o Belarus and Ukraine willbe represented by the Russian Fed-
eration; and Caucasian and CentralAsian countries by Georgia.
LithuaniaIn 2004 2007, GIP implemented aproject titled Reorganizing orensicpsychiatric services in Lithuaniananced by MATRA (hereinaterRokiskis MATRA Project). This proj-ect aimed to develop a contempo-rary system o orensic psychiatricservice delivery in the Republic oLithuania that adequately providescare to this specic group o pa-tients and protects society rom thecriminally insane. The provision o
adequate care to orensic psychiat-ric patients and protection o societyrom the criminally insane is directlyrelated to the assessment o risk tooend in the uture, because o theollowing:1. Risk assessment helps to ascer-
tain the main actors contributingto the criminal behavior o theparticular patient;
2. It serves as a background or thedevelopment o individual plans otreatment and risk management;
3. It enables the evaluation o theeectiveness o measures takenduring the treatment;
4. It helps in reporting to the courtregarding the changes o obser-
vational conditions and prolonga-tion or end o hospitalization.
In Lithuania, as in most Post-Sovietcountries, risk is mainly assessed onthe basis o so-called unstructuredclinical judgment approach, whichimplies, that the clinician is, as itwere, his own risk assessment tool(M.Philipse, 2005). It means thatthe nal conclusion is determinedsubjectively (and oten implicitly) byeach individual clinician. The abovementioned project has revealed adeep need to develop Lithuanianversions o world-widely recognized
and used risk assessment tools.HCR-20 Violence Risk AssessmentScheme 2nd version (developed in1997) was chosen rom a long list oinstruments, because it is designedto assess the risk o people whohave some Mental Health distur-bances. In addition, it is quite easyto understand and apply. HCR-20represents the structured clinicaljudgement approach rather thenactuarial one; it does not requirea long validation process and the
creation o local norms; and it alsoimpacted the decision to pilot therisk assessment in Lithuanian oren-sic psychiatric setting on the basiso this instrument.
The Author
Presenting on
HCR-20
By Virginija Klimukiene
1 M.W.G.Philipse. Pre-dicting Criminal Re-cidivism. Empirical
studies and clinicalpractice in orensicpsychiatry. Printedin The Netherlandsby Febodruk, En-schede, 2005.
-
7/30/2019 Forensic Psychiatry and Prison Mental Health 2009
13/32
July2009 13
In June 2006, two representatives oLithuania, Pro.Rita ukauskien andthe author o this article, receivedthe ocial permission to translateinto Lithuanian, edit, and print themanual or the HCR-20, Version 2(Webster, Douglas, Eaves, & Hart,1997) rom the Mental Health, Law
and Policy Institute o Simon FraserUniversity (Canada), which holds thecopyright o the abovementioned in-strument. During the next two years,400 copies o HCR-20 Lithuanianversion was published ollowingthe requirements described in theocial permission. The longitudinalvalidation research has been con-ducted and in the middle o 2009, itis anticipated that the rst results othe ollow-up o orensic psychiatricpatients released rom the hospitalat least 12 months ago will be gath-ered.
In May 2007, three groups o 20proessionals each rom Rokiskisorensic psychiatric hospital weretrained on risk assessment andapplication o HCR-20 in practice.Participants o these trainings haddierent educational backgrounds:including psychiatrists, psycholo-gists, social workers, occupationaltherapists and nurses. RokiskisMATRA Project had a undamental
impact on creating multidisciplinaryteam work in Rokiskis hospital andtrainings on HCR-20 were designedto teach ways that this instrumentcould be handled by all team mem-bers (one o the indirect tasks oHCR-20 is to structure the meetingso multidisciplinary teams). Thus wemay conclude that Rokiskis MATRAproject acilitated an essential turn orisk assessment in orensic psychi-atric settings in Lithuania, becauseit initiated the implementation o
structured clinical judgment instru-ments as an alternative to subjectiveconsiderations.
Risk assessments might also beseriously considered in correctionalsettings. We may boast about theLithuanian Prison Department,which has developed and currentlyis implementing the Probation Con-cept. Such risk assessment instru-ments as HCR-20, PCL-R (HaresPsychopathy Checklist Revised),
SVR-20 (Sexual Violence Riskassessment instrument), OASys(Oender, Assessment System),Static-99, SARA, SORAG and oth-ers are planned to be introduced
Arkhangelsk where permission wasgiven in 1995 or developing the rstRussian language version o theHCR-20, we may assume that theremight be other initiatives to developrisk assessment methods that arenot yet known to us. It is possible thatthese initiatives are not embraced
by the two main institutes in RussianFederation charged with coordinat-ing all orensic psychiatric issues:Serbsky Institute in Moscow andBekhterev Institute in St.Petersburg.We hope that this inormation will behelpul in avoiding double work andenhance cooperation among institu-tions at the local and internationallevel, particularly considering thequite strict requirements and pro-cedures to obtain the permission ordeveloping a national version o theparticular instrument.
Georgia
Unstructured clinical judgment isthe only method used to assess therisk o orensic psychiatric patientsin Georgia. This country is lackingpsychologists, social workers andother members o a multidisciplinaryteam; thereore the report to the courtis oten based on the description othe patients mental state and prog-ress o medical treatment. The cur-rent situation in the country requires
ocusing mainly on coping withtrauma, psychosocial rehabilitationo reugees and internally displacedpeople, and on strategies that sup-port the process o recovery.
On the other hand, the increasinglevel o oenses (especially amongjuveniles) is observed in Georgia asan outcome o the traumatic eventso last summer. Thus, it is the righttime to address the implementationo risk assessment instruments as a
background or development andapplication o risk managementstrategies.
It is our hope that these valuable riskassessment tools, already translatedinto Russian and Lithuanian, will beurther translated and used through-out the ormer Soviet Union. Thesetools represent the best o objec-tive judgment or the uture and willhopeully replace the unstructuredclinical judgment used in the past.
Virginija Klimukiene is the Project
Manager or GIP-Vilnius ofce and
her email address is
into the Correctional System oLithuania.
In summary, the handling o risk as-sessment tools in Lithuania showsthat the provision o modern oren-sic psychiatric and prison mentalhealth services has been started in
Lithuania and we are very hopeulthat this process will be continuedby implementing the appropriaterisk management strategies in bothorensic psychiatric and correctionalsettings in order to reduce the levelo re-oenders in the Lithuanianpopulation.
Russian Federation
In 2007, Global Initiative on Psychia-try started a new project Develop-ment o orensic psychiatric andprison mental health services inKaliningrad Region, also nancedby MATRA. On the basis o the ex-perience gained during the RokiskisMATRA Project regarding the impor-tance o risk assessment providingservices or oenders with mentalhealth problems, it was decided toimplement HCR-20 in the orensicpsychiatric and penitentiary institu-tions in Kaliningrad Region.
It was ound that the permission orthe Russian version o HCR-20 has
already been given to some proes-sionals working in the North-Western
part o Russia. The leader o the
team, Dr. Oleg Ponomarev, agreed tocooperate with GIP in such a way thathe permits GIP to publish 1000 cop-ies o HCR-20 Russian version andGIP covers the costs o translationand editing and also provides train-ings to specialists o ArkhangelskRegional Clinical Psychiatric Hospitalon the use o the instrument in dailypractice. GIP also commits to trans-er 100 copies o HCR-20 Manual toArkhangelsk Hospital and to providesupport in training the trainers o ap-
plication o HCR-20 in Russia.
Since Russia is such a large countryand the Kaliningrad specialists didnot know about developments in
These risk assessment tools
represent the best of objective
judgment for the future.
>
>
-
7/30/2019 Forensic Psychiatry and Prison Mental Health 2009
14/32
14 MentalHealthReorms
Developing Partnerships in Forensic
Psychiatry: The Pompe Foundation asPartner in GIP projects
At a congress in Prague in 2000,the rst author (T.V.) met a medicalsexologist rom Lutz in the western
part o the Ukraine. This individualwas invited to the Pompe Founda-tion, gave inormation on the situationo orensic psychiatry in the Ukraineand asked or assistance to improvethe conditions in orensic psychiatryin his country. This resulted in a visito a delegation o the board o thePompe Foundation to the Ukraine.
The youth prison in Kovel espe-cially made a deep impression onthe visitors. Hundreds o boys were
incarcerated without any activities,with lack o proper ood and medi-cal care and hardly any possibilitiesor rehabilitation. Back in The Neth-erlands, the delegation succeededin raising philanthropic unds or aproject to improve the conditions inthis youth prison.
The result was that, ater our years,this acility had its own kitchenwhere the boys were baking theirown bread, a shoe reparation work-
place, a garage and several smallerwork places. The boys were trainedin these new acilities as part otheir rehabilitation.
A visit rom Holland in 2007 madeclear that these changes wouldbe maintained. Inspired by these
results, the Pompe Foundation de-cided to go urther on this way, but asit appeared, getting more ormalizedunding rom the Dutch governmentwas met with too many complicatedadministrative procedures. This ledto a structural cooperation betweenthe Pompe Foundation and GIP, thelatter with its longstanding experi-ence with projects in Eastern Europeand the New Independent States othe ormer Soviet Union, as well as itsexperience writing project proposals
to the Dutch government.
It is the intention o GIP to extendtheir activities in these elds to Asiaand Arica.
A steering group was ormed to leadthe project since there were many as-pects o orensic psychiatry to be in-cluded: pre-trial assessment, prisonmental health, and the execution ocriminal law. In addition, the numbero projects in this eld was increasing;
currently, the Pompe Foundation isinvolved in three ongoing projects - inLithuania, Russia and Georgia. Newprojects are in preparation in Serbia/Montenegro, Bulgaria and Sri Lanka.
In this article the results so ar inthe rst mentioned countries will bedescribed.
Forensic Psychiatric Hospi-
tal Rokiskis, Lithuania
The rst project involving the PompeFoundation started in the only psy-chiatric hospital in Lithuania, situatedin Rokiskis, a ar away village in thenorthern part o the country. It was anold psychiatric hospital with prison-like characteristics, comparablewith Dutch psychiatric acilities romabout 1950. Its sta was low paid, ingeneral poorly trained and its motiva-
tion to change not very high, with theexception o the medical director.
Patients stayed in their rooms dur-ing the day, shared with our or veother patients. No daily activity pro-gram was oered and their treatmentmainly consisted o medication.The Pompe Foundation oered sev-eral trainings to dierent groups oworkers, including a multidisciplinaryapproach to each individual patientsproblems, patient-sta interaction
and psychopathology. Together withlocal partners, the risk assessmentinstrument, the HCR-20, widely usedin the West and described in the pre-vious article, was translated into Lith-
Forum GGz Nijmegen is a large
organization or mental health
care in the eastern part o The
Netherlands. Part o this orga-
nization is the Pompe Founda-
tion, which consists o a high
security orensic psychiatric
clinic with acilities or reso-
cialization, a policlinique or
ambulant care and treatment
o orensic psychiatric patients
and a center or research and
development.
The Authors
Visiting
Forensic Facility
in Serbia
By Thieu Verhagen and
Dick Raes
-
7/30/2019 Forensic Psychiatry and Prison Mental Health 2009
15/32
July2009 15
uanian, according to the regulationsand an expert o the Pompe Founda-tion gave training in the application othis instrument or psychiatrists andpsychologists rom Rokiskis and theRomero University in Vilnius.
The three-year nancing o the proj-
ect by the Dutch Ministry o ForeignAairs (the so called Matra nancing,Matra meaning Social Transorma-tion) ended in 2007. But the activitieso the Pompe Foundation will be con-tinued, based on a Memorandumo Understanding between RokiskisHospital and the Pompe Foundation(twinning) resulting in ongoing sup-port by the Pompe Foundation. It isimportant that the progress achievedwill go on. The project has movedRokiskis at least 25 years ahead owhere it was; a great deal has beenachieved but still more is to be done.
It should be mentioned that apartrom the activities o the PompeFoundation, GIP was able to use theopportunity to organize workshopswith members o the court and thepublic prosecutors oce.
Forensic Psychiatry in Kalin-
ingrad (Russian Federation)
This Matra project started in 2007and involves the three areas men-
tioned above. Kaliningrad is a prov-ince o the Russian Federation, buthas become an enclave, separatedrom the main country. In our view,based on earlier experiences, thisis an advantage because o the actthat all aspects o orensic psychiatryare centrally directed rom Moscow.Because o its more isolated positiontowards Moscow, we expect to havemore cooperation with the local au-thorities and colleagues.
The rst visit o a Pompe delega-tion took place in 2007 to the highsecurity orensic psychiatric clinic inChernyakovsk. The treatment o the400 patients consists only in the ap-plication o medication, aimed at sta-bilizing the condition o the patients.The average duration o the patientsstay in the hospital is 10 years (twiceas long as in the Pompe Clinic). Theyare allowed to be in contact with theiramilies by mail or telephone butnever get permission to visit them.
Family members were never involvedin the treatment; patients and, espe-cially, those admitted or political rea-sons as happened in the old regime,were as a rule admitted as ar away
as possible rom their original placeo living. Because o the isolatedlocation o Kaliningrad, most o thepatients are nowadays admitted romthe Kaliningrad area. Thus, it is easieror amily members to visit the hospi-tal and oer also better opportunitiesor rehabilitation and resocialization.
The director and his sta are verymotivated or changes, but there is alack o skills and knowledge. A lot othe potential o the sta is not usedbecause o the strict hierarchical re-lations in the organization and insu-cient proessional education.
It is clear that the nursing sta needstraining on working with the patientsin a therapeutic way, methods orplanning, eectuating and evaluationo the treatment, also in a multidis-ciplinary context. But also improve-ment o the position and involvementin the treatment by the psychologistsis rather urgent, including the intro-duction o the HCR-20. Between2007 and 2010, The Pompe team willoer three trainings each year. Apartrom these activities, the Prison Men-tal Health Team o GIP succeededin organizing activities with peniten-tiary psychologists to improve mentalhealth care in the prison system inKaliningrad.
GeorgiaGeorgia appeared to be one o thecountries where the departure o theold Soviet system let the country ina state o almost anarchy. This situ-ation oered advantages and disad-vantages. Due to total corruption inthe system o pretrial assessment,GIP was asked to establish a newapproach to psychiatric expertise toadvise the courts. Because o theresults o a new expertise center orpretrial assessment and a series
o seminars or the sta, GIP wasasked to assist in the arrangement oa new centralized clinic or orensictreatment and as well or the care omentally disturbed prisoners in a newprison center.
A Dutch developmental agency (Cor-daid) was willing to support a projectto improve the circumstances andtreatment in the orensic psychiatrichospital in Quitiri. Recently, all oren-sic psychiatric patients rom Georgiawere brought together in this hospital.Because o the isolated situation o
the hospital, it lacks enough qualiedpersonnel which, in turn, is refectedin the quality o treatment. Also inthis situation, the Pompe team has todeal with implementing knowledgein nurses and as well in psychiatristsand psychologists, regarding basicprinciples o psychopathology, mul-tidisciplinary treatment, risk assess-ment and risk management. Thereis a positive perspective on coopera-tion with the local proessionals.
General recommendations
1. It is very important beore startinga project with real interventions toget the trust o the local partners,as well the people we try to workwith as the authorities that have thenal responsibilities. The Russiansespecially do not trust the infu-ence o western involvement underthe name o NGOs and MATRA.
2. It is our experience that the expec-tations o at least beginning train-ers are too high as to what theycan achieve.
3. Administrative and logistic tasksshould be taken care o by oth-ers than the proessional trainersinvolved. These tasks would taketime rom the work needed to meettheir primary goals.
4. Be prepared or the specicproblems concerning trac andtransport. Local people are usu-ally very hospitable but not awareo the stress their driving behaviorprovokes.
5. Be aware o drinking habits. Do
not be surprised when vodkais served at breakast or lunch.Restrict yoursel regarding this todinner situations.
6. Be prepared that many intendedactivities will work out in a dierentway. This requires improvisationand creativity. (T.V.: Nothing iscertain until it has happened.)
Thieu Verhagen is Head Concern
Sta, Forum GGz Nijmegen and
part-time consultant with GIP. E-mail:
[email protected]. BCM (Dick) Raes is Proessor in
Forensic Psychiatry, member o the
board o GIP. E-mail: [email protected]
The average duration of a
patients stay in the hospital is 10
years; they can receive mail from
family members but are unable to
visit with them.
>
>
-
7/30/2019 Forensic Psychiatry and Prison Mental Health 2009
16/32
16 MentalHealthReorms
Forensic psychiatry: visit
to Gornja Toponica
In March 2008, John Kobes-sen and Roland van Rooij o thePompe clinic in Nijmegen (TheNetherlands) visited the specialistpsychiatric hospital Bolnica GornjaToponica (Nis, Serbia). This hos-
pital accommodates nearly 700general psychiatric patients and120 orensic patients, the lattergroup o which consists o 80men and 40 women. The assign-ment rom GIP was to take a closeand unprejudiced look at BolnicaGornja Toponicas vision, method,patients and building, and to makeas much contact as possible withthe proessionals at work. Specialattention was paid to meaningulpastime: what current activities are
there and where do opportunitiesor growth lie?
The Dutch experts were cordiallyreceived by the general manager,
Dr. Milan Stanoskovic, and bythe unit managers (Dr. SnezanaVladejic, Dr. Dragana Arandelovic,Dr. Sanja Stanojrovic) and sta.Everything is done optimally withthe possibilities at hand (e.g. us-ing medication as eectively aspossible). The atmosphere is open
and there is direct contact withthe patients, who are treated withrespect and care, and at the sametime there is a balanced relation-ship between sta and patients.Every eort is made to provide so-cial saety, taking into account thatthere are as ew as one to six stamembers at a unit, or a maximumpopulation o 80 patients, residingin 5 dormitories. There are no com-puters and, thus, no ast and directcommunication. Patients records
are still kept on paper.
One example o the involvement osta is the weekly group meetingwhere 60 male patients are hosted
by 6 sta members (doctors andtherapists). This group (that haspatients in the positions o chair-man and secretary) is used to letpatients react to each other, toinorm them (e.g. about treatment)and to correct them i necessary.Another striking example is a morn-
ing meeting that requires patientsto stand next to their neatly madebeds at 8 am and be scrutinizedby the ull sta o the ground andrst foors, who point out any pecu-liarities (there is no privacy).
While an inormal culture hasdeveloped, there is hardly anyormal culture. No protocols existor incidents or hostage situationsand understang, nor are thereany written house rules or job de-
scriptions. Psychotic patients andpatients with personality disordersare mixed. (Our impression wasthat on these units the psychoticpatients were the vast majority;
Visiting Gornja
Toponica
Forensic
Department
In October 2007, a team o experts o Global Initiative on Psychiatry
visited Serbia or the frst assessment o the situation in orensic
psychiatry and prison mental health. Several institutions were visited,
including the orensic department o the Gornja Toponica hospital in
Nis and the Central Prison Hospital in Belgrade. The report o the visit
was received positively by all parties concerned, as it oered a wide
range o possible felds o collaboration. The Dutch Embassy agreed
to fnance a continuation o the assessment as well as some frst
activities in this feld. Within the ramework o this project, a urther
inventory o the situation in orensic psychiatry in Gornja Toponica
would be carried out and proessional exchanges between Serbian
and Dutch orensic psychiatry proessionals would be started. Also,
a second assessment visit to the Specialized Prison Hospital in Bel-
grade would take place ollowed by a frst step in the direction o an
exchange o views and experiences. In addition, materials to stimu-
late day time activities and rehabilitation work at the orensic depart-
ment o the hospital Gornja Toponica would be bought and a seminar
on orensic psychiatry and prison mental health would be organized
or all stakeholders in Serbia.
By Robert van Voren
Initiating Reorm in Prison Mental
Health & Forensic Psychiatry in
Serbia
-
7/30/2019 Forensic Psychiatry and Prison Mental Health 2009
17/32
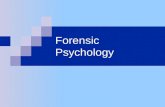
July2009 17
Distribution
o patients
in Belgrade
Special Prison
Hospital
75% versus 25% personality dis-orders).
Expansion o patients leave hasto be requested directly at thecourthouse, upon which a judgereacts with a simple yes or no.However, i anything happens to
the patient while on leave (fight,recidivism), the sole responsibilityalls on the hospital and the gen-eral manager. The consequence isthat patients have little chance omoving out o the secured building;and rehabilitation oten consists onothing more than being droppedback into society at a certain mo-ment, at which point patients com-pletely depend upon their (otendecient) social network.
The logical consequence is a highpercentage o (risk o) recidivismand patients returning to society inan oten highly unstable condition.There are ew social workers whocan guide patients and their so-cial network. The travel distancesare also unavorable; patientsliving 300 km rom the hospitalcan oten be consulted by meanso telephone only. Serbia has noater-care and resettlement orga-nizations.
It is true that there are activities ororensic patients inside the build-ing and sometimes on the hospitalgrounds. An impeding actor isthat patients cannot be employedin real work because it is consid-ered by outsiders to be exploitationo patients; however, it is this kindo work that oers opportunities orpatients to develop themselves. Itis important to educate patientsindividually in certain basic skills(cleaning, kitchen, garden, mainte-
nance, etc., but also basic knowl-edge o language, mathematics,writing, etc.): positive experiencescreate positive energy.
The second reason why there is somuch hesitation to extend patientsmovements beyond the hospitalgates is the negative public imageo (orensic) psychiatric patients.Time and energy is invested inmaking contact with society, withsome success.
Prison Mental Health: Visit
to the Specialized Prison
Hospital
In June 2008, Wendy Weijts, Theo
Lammers and Rob Hollander vis-ited the Special Prison Hospitalin Belgrade. This hospital has 4dierent specializations with atotal o sometimes more than 600patients.
The largest group, the department
with compulsory treatment, is in abuilding unsuitable or this popula-tion and without a good treatmentenvironment. In some cases,patients stay or over 20 years inthis prison hospital. When patientshave no social network ater theirtreatment, the court will not releasethem because they still considerthem as a danger to society. Forthose patients, a normal resocial-ization program cannot take placeat all.
Within this restricted acility, thesta was very committed to the pa-tients; the occupational therapiststry to make the residence o thosepatients a bit less miserable. Oneguard is responsible or one ward
which sometimes contains morethan 120 patients and, at timesmay be responsible or two ormore wards at the same time. Mosto the patients receive tranquil-izing medication (most commonuse is Bentazin) and have nothingmuch to do other than staying intheir beds. Sometimes (in case osevere aggression) patients getrestraint measures (special roomwhere the patient is tied to a bed).Within a prison system, this is an
accepted measure, even in west-ern countries. The main problem isthat, when in restraints, the patientis actually under the observationo another patient. In our opinion,
this is not an acceptable situation;patients should be accompaniedby a proessional.
At this moment, ve out o sevenwards (hallways) are renovated.The hallway is a 50 meter corridorwith cells on the side housing 6 to
10 patients each. Most o the timepatients are in the corridor or intheir beds. Every ward is closedby a ence with the guard sitting ina small room in ront o that ence.This is the only way to enter theward. The guard has absolutely noview o the cells or at the end o thecorridor. When a patient is requiredor some reason (medication, visi-tors, etc) the guard will shout thepersons name through the ence.In the morning, the doctors andnurses visit the patients on the wardmostly or the purpose o checkingto see i anyone is having too manyside eects rom the prescribedmedication. We hope to redesignthe wards to a more therapeuticlevel which also considers saetyissues.
Over the past two years, GlobalInitiative has become involvedin orensic psychiatry and prisonmental health in Serbia, and al-though much needs to be done, a
positive working relationship and asincere desire to change has beenthe cornerstone o our work. Asa result o our collaboration withSerbian partners, a major proposalhas been submitted or undingto the Dutch Ministry o ForeignAairs. The project will oer theopportunity o laying the ground-work or a contemporary chain oorensic psychiatric services. Theproject enjoys the support o allparties involved, both at the gov-
ernmental and local level. It willcreate a model that changes thesystem o orensic psychiatric ser-vices rom a purely custodial oneto a service directed at treating,curing and saely re-integrating thementally disturbed oender. At thesame time, it provides a treatmentmodel that adequately addressesthe mental health needs o theprison population.
Robert van Voren is the Chie
Executive o Global Initiative onPsychiatry. His email address is
around 450patients
around 50 patients
around 50 patients
around 66 patients 400 admissions per
year
somaticward
pre trialassessments
Acute crisisintervention
CompulseryTreatment,incl drugsand alcohladiction
-
7/30/2019 Forensic Psychiatry and Prison Mental Health 2009
18/32
18 MentalHealthReorms
Bulgaria: A European Union MemberLagging Behind in Forensics
Lovech Prison
Hospital
During the last two decades, severalalarming tendencies in Bulgarianorensic work have emerged. Thequality o expert work has decreased
while corruption increased, includ-ing among some psychiatrists. TheForensic Psychiatry Clinic made aseries o proposals to the Dean oMedical Faculty in Soa, the Rectoro the Medical University in Soaand the Minister o Justice or the im-provement o the quality o orensicwork, the continuing education andpromoting an inter-institutional bodyor control in orensic psychiatricpractice. No measures were ac-cepted and the passivity remained
the main institutional behavior. Thissituation became more and morechaotic.
Through the eorts o the Clinic, thespecialty o orensic psychiatry wasintroduced in 2001 as required bythe EU rules or basic medical spe-cialties. This step decisively creatednew opportunities or proessionalgrowth in experience o specialistsin the area. However, Bulgarian leg-islation annihilates this opportunity.
There is no dierentiation o levels ocompetence in orensic psychiatricpractice. Every specialist in psychia-try has the right to prepare orensicassessments and reports and is ac-
cepted as equally competent by thejudicial system. There are no ideasor stimulation and requirements orcontinuing education and improve-
ment o orensic work. The systemeven introduced discriminative age-related exclusion criterion in orensicwork, although it is a reelance pro-ession.
On the other hand, the organiza-tion o the specialization in orensicpsychiatry in the only place theClinic o Forensic Psychiatry andPsychology in Soa - is nancedon the general rule o the number opatients per month. This rule orced
the Clinic to accept more and moregeneral psychiatric patients and haslimited the time or orensic work toonly around 20%. The State Spe-cialized Hospital o Neurology andPsychiatry St. Naum red many othe proessionals in clinical psychol-ogy; there is currently only one clini-cal psychologist, who is responsibleor 200 neurological and psychiatricbeds. Judicial institutions are notdiscussing other possibilities orunding orensic work although it is
essential or the survival o orensiceducation and practice.
Other negative tendencies haveappeared in recent years. Some
academic psychiatrists expressedtheir personal and unexplainednegativism towards the Clinic. Themain point was the opinion that the
clinic should be moved into theprison system. The culmination othese ideas was the organized vot-ing in the Department o Psychiatry,under the leadership o the Head othe Department and also NationalConsultant in Psychiatry Pro. VihraMilanova, MD, PHD. The nal deci-sion was that there is no need or theClinic o Forensic Psychiatry, and noneed or the Senior Educator (Asso-ciated Proessor) to lead the Clinic.The main argument o Pro. Milanova
was that every specialist in psy-chiatry is equally competent to pre-pare complex orensic assessmentsand reports and every proessor inpsychiatry is competent to conducteducation in that area. These ideaswere accepted by a small majority,but it caused highly destructive e-ects on the specialization in orensicpsychiatry and atal consequencesor the existence o the Clinic o Fo-rensic Psychiatry and Psychology.Gradually the personnel o the clinic
were reduced to only one orensicpsychiatrist, which was detrimentalto the possibilities o organizing o-rensic assessments and educationin the eld. All interested judicial and
Bulgarian orensic psychiatry
has its roots in the beginning
o 20th century with the leading
Bulgarian and European books
o Vladov, Danadjiev and Schip-
kowensky. An in-patient univer-
sity clinic was created in the
second hal o the century or
complex expert assessments,
requiring more experience and
complex psychiatric and psy-
chological investigations.
By Petar Marinov and Vladimir
Velinov
-
7/30/2019 Forensic Psychiatry and Prison Mental Health 2009
19/32
July2009 19
Response rom GIPGlobal Initiative has been involved inmental health care development inBulgaria or almost teen years. Inthe mid-1990s, it started its involve-
ment by assisting in the training omental health care personnel, con-centrating on the younger generationo uture psychiatric leaders. It devel-oped a publication program with theBulgarian Psychiatric Association, inthe course o which a dozen booksand manuals were published, andsponsored the annual meetingso the Bulgarian Psychiatric As-sociation. Subsequently, it set up aDay Care Center in Soa, assistedin the development o the Bulgarian
Institute o Human Relations as parto the New Bulgarian University,developed training programs or vari-ous specialists, helped organize anENMESH Conerence in Soa and,in 2001, set up a Regional Oce inthe Bulgarian capital, responsible orprojects in South Eastern Europe. In2005, in partnership with the StabilityPact, GIP commenced a project ordevelopment o a consecutive chaino community mental health care ser-vices in Blagoevgrad, which is used
as a pilot or the rest o the country.Currently the GIP-Soa oce is in-volved in developing community ser-vices in the Soa suburb o Slatina.
In 2004, GIP supported the SocialActivities and Practices Institute tomake an assessment o the psychi-atric, psychological and social ser-
vices provided to prisoners and stain the places o imprisonment. Thereport was published in the PrisonAairs, (XXXVIII, book3/2004) andsince then remains the only nationalresearch done on mental health in theprison. The research evaluated boththe satisaction with the general healthservices and mental health care inparticular and the stress related com-plaints o the prison sta. The reportconcludes that there is a lack o anintegral conception about the treat-
ment o prisoners with special needs(training o the personnel, programs,care, etc.). The report considers theunder-unding o the system and thelack o autonomy o the prison medi-cal sta as main structural reasons orthe observed shortcomings within theprison health care.
Except or this report, GIP has notbeen active in the eld o orensicand prison mental health servicesin Bulgaria. GIP has assessed the
situation with the goal o seeing howand where Global Initiative could beo assistance. GIP has been activein the eld o orensic psychiatry andprison mental health or quite a ew
years and in a growing number ocountries. It is hoped that this expe-rience and expertise might make adierence in Bulgarian orensic and
prison psychiatry.
The main problems o Sofa Prisoninclude: Purely a medical approach;
Lack of multi-disciplinary teamwork
and resocialization programs; Lack of psychiatric knowledge of
sta, especially guards and nurs-es need an education program onmental health problems;
Lack of psychiatrists. Each prison
has vacancies or psychiatrists
because o the low salaries; Attitudinal problems of staff to-
wards patients, e.g. not being ableto see the inmates as patients;
Stress and burnout among the
sta. The sta works in shits o 24hours with a three-day intervals,and the other three days are usedor other part-time jobs to supple-ment the salaries;
Acquisition of medication. Generic
medication is too expensive; Increase of inmates with HIV/
AIDS; Inmates with a drug and/or alcoholproblems;
The general quality of care in the
prison is low.
academic institutions were inormedwithout response; a typical reactionor the systems in Bulgaria.
Using SWOT analysis several as-pects could be described:1. Strengths. In Bulgaria, the edu-
cational system and specialty in
orensic psychiatry was estab-lished. There are several resi-dents in this specialty who wereon their way to being promotedto specialists. A good numbero judges and prosecutors inBulgaria acknowledge the needor the specialty and or the Fo-rensic Psychiatry and PsychologyClinic.
2. Weaknesses. There is an ex-tremely low number o specialistsin orensic psychiatry and a verylow level o inter-institutional col-laboration as well as interest inthe institutions to help the uture
o orensic expertise.3. Opportunities. One o the main
opportunities is the potential in-volvement o proessionals andexperts rom EU countries inadvising Bulgaria on the utureo orensic psychiatry. Anotheropportunity is the potential o in-
volvement in the monitoring o thejudicial system in Bulgaria. Thethird opportunity is the prepara-tion o proessional teams in o-rensic psychiatry and justice whocan prepare a National programor development o orensic psy-chiatry and orensic psychologyin collaboration with EU experts.Another opportunity is the prepa-ration o a new law on orensicpsychiatry and orensic psychol-ogy.
4. Threats. The principle threat isthe resistance o some socialgroups who are against orensic
psychiatry and the judicial systemas a whole. Another risk is that EUcountries could view the problemas an internal Bulgarian issueand neglect the importance oorensic sciences and their aca-demic and practical developmentin the judicial system in Bulgaria.
Promoting ideas about the re-placement o the clinic by prisonscould change the basic concepto orensic assessment in all othe phases o investigation andcould be contradictory to its inde-pendence.
Dr. Petar Marinov, MD, PhD is Past
President o Bulgarian Psychiatric
Association. Pro. Vladimir Velinov
is proessor emeritus o orensic
psychiatry in Sofa. They can be
reached at [email protected] and
-
7/30/2019 Forensic Psychiatry and Prison Mental Health 2009
20/32
20 MentalHealthReorms
After working 15 years in
prison, the staff develops a va-
riety of problems, such as seri-
ous neuroses, stress, insomnia,
headache, and cardio-vascular
problems.
>Soa prison with 2,100 inmateshas only 4 psychologists. In caseswhere alcohol, psychological orphysical problems are detected, thepsychiatrist and general practitionerdevelop a treatment program or theprisoners stay in prison.
The Prison mental health depart-ment in Sofa prison is part o theinternal diseases unit and has asmall capacity or patients with men-tal health problems. About 5% o theinmates in the Bulgarian prison sys-tem are identied with mental healthproblems and/or addiction prob-lems. This 5% is under supervisiono a psychiatrist. Suspected mentalhealth problems are registered.Evidence rom many countries con-sistently shows that the prevalenceo mental health problems amongstprisoners is signicantly higher thanamongst the general population.This is especially true or personalitydisorders, substance abuse, depres-sion and psychotic disorders. Preva-lence rates among emale prisonersare higher in many countries. Mostprobably, the estimated 5% preva-lence in the Bulgarian prison systemindicates that there are serious fawsin the (mental) health assessmentsystem. According to legislation,inmates can attain services outside
the prison i they need proper careor wish to have a second opinion.Each inmate has the right o accessto any medical services but has topay or them himsel.
Lovech prison hospital connect-
ed to Sofa prison receives inmateswith mental health problems whoare transerred rom the Soa prison.About 200 patients are treated hereannually. According to the Regula-tion or medical service in prisons,
people who are considered by acourt decision to be unaccountableare sent to Lovech psychiatric hos-pital or compulsory treatment. HIV/AIDS has a small prevalence andthe Soa prison keeps a record onthe persons who are inected. Per-sons living with HIV/AIDS can attainthe services anonymously and theirmedical status is condential. Withinthe prison, VCT - Voluntary Commit-tee Testing - tests the inmates whowant to be tested. In case a person
needs medical assistance, accessto the hospital is provided; all per-sons with contagious inections aretreated in state programs in nearbyhospitals. Prisoners dependent on
drugs have access to methadonetherapy. Psychiatrists receive train-ing on how to supply the methadoneprogram.
The possibilities o improving thecircumstances were discussed withour Bulgarian colleagues and anumber o items were listed: There should be a broader thera-
peutic approach, and not only amedical approach. In Bulgaria, toomuch stress is currently put on themedical aspect.
The department should develop
operative multi-disciplinary team-work, with each team consisting oa general practitioner, psychiatrist,social worker, nurses and the psy-chologists.
Rehabilitation programs should be
developed. Education and acceptance pro-
grams should be developed orprison sta, as well as or inmatesand their amilies, in order to in-crease tolerance or inmates ingeneral and inmates with mentalhealth problems in particular.
Intervention and support programs
should be developed or the sta.Work in prison is a hard job andin many respects the sta has todeal with the same situation as the
inmates. Ater working 15 years inprison, the sta develops a varietyo problems, such as serious neu-roses, stress, insomnia, headache,
and cardio-vascular problems. Upto now psychological care is main-ly or prisoners and not or sta.
According to one o the main psy-chiatrists in the hospital, Dr. Nesh-kov, the prison hospital encountersthe ollowing problems:
Burnout problems of the staff; thereis neither attention to this issue norprevention o burnout.
Bad material conditions related
to inconvenient accommodation(leakage); construction o thecurrent building or the hospitalstarted in 1982 but cou