For Self-Presenting Patients HAZMAT/CBRN For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015...
40
1 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015 SH NCP 68 Standard Operating Procedure For Self-Presenting Patients HAZMAT/CBRN Version 1 Summary: The Health and Safety team have developed (SOP) Standard Operating Procedure for Self presenting patients from a possible HAZMAT/CBRN Incident and identifies arrangements for managing the safety, health and welfare of SHFT staff, clients, patients, visitors and anyone else who can be affected. It outlines the organisational structure and arrangements to ensure the Trust fulfils its legal responsibilities from NHS England Core standards Emergency planning and duty of care to protect people from hazards associated with incidents. The HAZMAT/CBRN SOP is an integral component of SHFT safety management systems. This should also be aligned with the Trusts Lockdown, IRP (Incident Response Plan) policies. Keywords (minimum of 5): (To assist policy search engine) CBRN/HAZMAT, Chemicals Target Audience: All Trust Staff Next Review Date: December 2018 Approved & Ratified by: Health and Safety Forum Date of meeting: 27 April 2015 Date issued: May 2015 Author: Darren Hedges AISFM, Tech IOSH, MCGI Health & Safety Advisor David White CMIOSH. FIFSM. MIIRSM. GIFireE Health and Safety/Fire Safety/ Security Manager Sponsor: Mark Brooks Chief Finance Officer
Transcript of For Self-Presenting Patients HAZMAT/CBRN For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015...

1 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
SH NCP 68
Standard Operating Procedure
For Self-Presenting Patients HAZMAT/CBRN
Version 1
Summary:
The Health and Safety team have developed (SOP) Standard Operating Procedure for Self presenting patients from a possible HAZMAT/CBRN Incident and identifies arrangements for managing the safety, health and welfare of SHFT staff, clients, patients, visitors and anyone else who can be affected. It outlines the organisational structure and arrangements to ensure the Trust fulfils its legal responsibilities from NHS England Core standards Emergency planning and duty of care to protect people from hazards associated with incidents. The HAZMAT/CBRN SOP is an integral component of SHFT safety management systems. This should also be aligned with the Trusts Lockdown, IRP (Incident Response Plan) policies.
Keywords (minimum of 5): (To assist policy search engine)
CBRN/HAZMAT, Chemicals
Target Audience:
All Trust Staff
Next Review Date: December 2018
Approved & Ratified by:
Health and Safety Forum
Date of meeting: 27 April 2015
Date issued:
May 2015
Author:
Darren Hedges AISFM, Tech IOSH, MCGI Health & Safety Advisor David White CMIOSH. FIFSM. MIIRSM. GIFireE Health and Safety/Fire Safety/ Security Manager
Sponsor:
Mark Brooks Chief Finance Officer
2 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
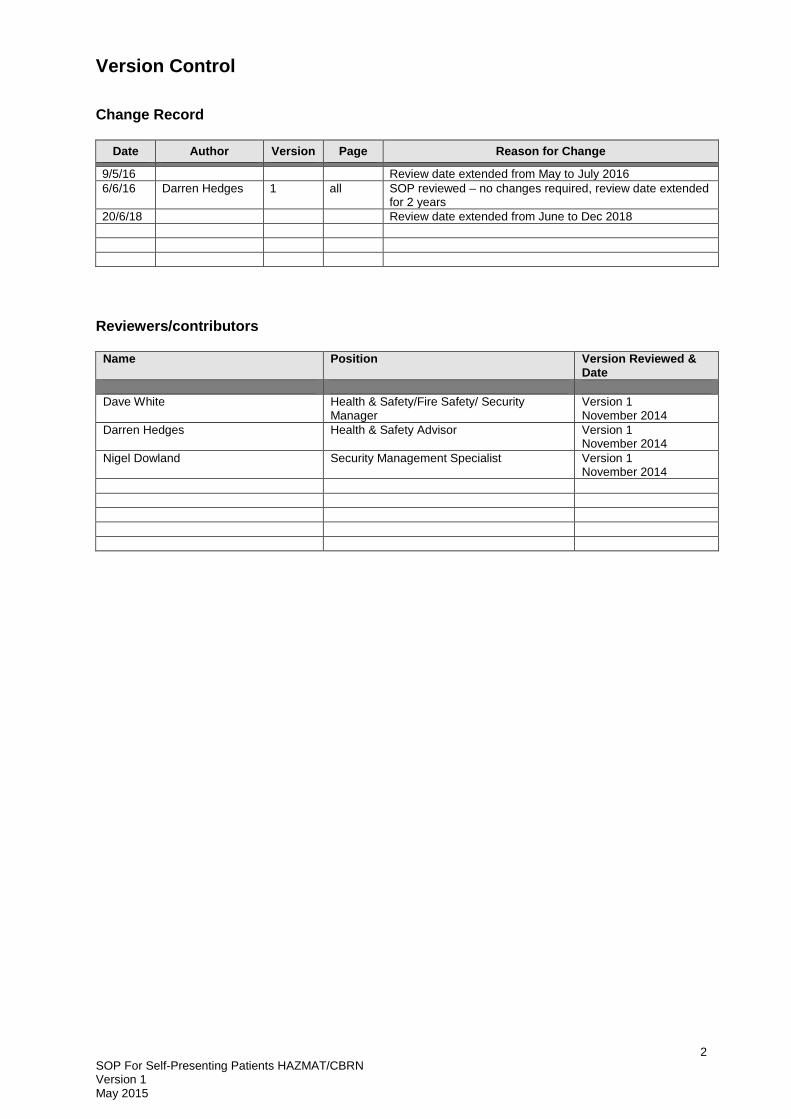
Version Control
Change Record
Date Author Version Page Reason for Change
9/5/16 Review date extended from May to July 2016
6/6/16 Darren Hedges 1 all SOP reviewed – no changes required, review date extended for 2 years
20/6/18 Review date extended from June to Dec 2018
Reviewers/contributors
Name Position Version Reviewed & Date
Dave White Health & Safety/Fire Safety/ Security Manager
Version 1 November 2014
Darren Hedges Health & Safety Advisor Version 1 November 2014
Nigel Dowland Security Management Specialist Version 1 November 2014

3 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
CONTENTS
Page
1. Introduction
5
2.
Definitions
5
3.
Legal Responsibilities
6
4.
Decontamination Infrastructure
7
5.
Incident Response
12
6.
Post Incident
17
Appendices
A1
Preparation for Incidents involving Hazardous Materials and Guidance for Primary and Community Care Facilities
19
A2
Chemical Exposure Form
34
A3
Equality Impact Assessment / Equality Analysis Screening Tool
35

4 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
SOP For Self-Presenting Patients HAZMAT/CBRN
Forward This document provides Trust management and staff within Southern Health NHS Foundation Trust, with guidance in respect of their responsibilities for the decontamination and treatment of persons who may self- present or attend sites within SHFT following exposure to hazardous materials, or suspected exposure, to chemicals, biological agents, or radioactive material. This document also provides guidance on how SHFT staff should provide appropriate health care to such patients who may be so contaminated whilst protecting themselves, the site and other members of staff, other patients, and the public from exposure or cross-contamination from these substances. SHFT has a statutory duty to provide care for patients when and wherever required. SHFT also has a legal duty to protect staff from harm whilst carrying out their duties. Incidents involving chemicals, biological agents, and radiological materials by their nature can bring severe disruption to services and pose serious health risks to staff. In preparing this guidance clinical, nursing, and management, will be consulted to ensure that it is both appropriate and proportionate. The contents of the policy are intended to ensure that the effects of such an incident on normal SHFT services are minimised. It should be noted that this Policy is guidance only and it is for the board to determine how this should be implemented based on local risk assessment (contained within the Lockdown policy).

5 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
1. Introduction
This practical guidance document is aimed at preparing primary and community-based health facilities to be able to manage the consequences of a hazardous incident occurring somewhere else (also referred to as a chemical, biological, radiological, nuclear or explosive incident – CBRNE). In these incidents there is a need to care for people, but also to be aware of the safety risk to staff and patients from secondary contamination as a result of people self-presenting at their facility seeking assistance. Contamination can result from the accidental release of hazardous material (HAZMAT) from industrial and commercial premises, transport accidents, the illegal disposal of contaminated waste, or from the deliberate release of these hazardous materials e.g. by terrorist group or individual. A number of initiatives designed to improve the response to such incidents have been introduced. These include the provision of mass decontamination facilities to the Fire & Rescue Services, and clinical Decontamination Units to the NHS Ambulance Service (for use at the scene of incidents. These initiatives complement the decontamination equipment available. Any Hazmat or CBRN event should be appropriately risk assessed, planned for and managed as part of a multi-agency response. Decontamination is not an automatic or inevitable response to CBRN or Hazmat events. Whether or not to initiate decontamination procedures will depend on the initial assessment of the nature of the event by first responders and subsequently by Health Professionals. This SOP will also provide guidance on the roles and responsibilities of the emergency services in relation to the decontamination of casualties following a release of hazardous materials.
2. Definitions
Definitions related to decontamination are provided below. 2.1 Decontamination
Decontamination is defined as the removal or reduction of hazardous materials to lower the risk of further harm to casualties and/or cross contamination. Decontamination can range from self-help to full clinical decontamination by the Department.
2.2 HAZMAT
A non-criminal accidental release of a substance, agent or material, which results in illness or injury to the public, the denial of access to an area or the interruption to the food chain. The commercial, industrial, medical, or military substances involved in a Hazmat incident could be from any of the CBRN categories outlined below. Strict guidelines exist for the storage, handling and transport of these materials and the number of incidents involving their accidental release or spillage is low, although likely to be the most common type of incident involving contamination.
2.3 Background on CBRN (Chemical, Biological, Radiological, Nuclear)
A deliberate and malicious act, the intention of which is to cause harm or fear amongst a population by using or threatening to use CBRN materials. The incident is crime

6 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
focussed and may range from cases of relatively minor harassment and alarm through to terrorist acts of mass murder or genocide. CBRN is a term that covers a distinct range of hazards:
i. Chemicals
Poisoning or injury caused by chemical substances, including chemical warfare agents, or misuse of legitimate but harmful household or industrial chemicals
ii. Biological
Illnesses caused by the deliberate release of dangerous bacteria, viruses, fungi, or toxins (e.g. the plant toxin, ricin).
iii. Radiological
Illnesses caused by exposure to harmful, radioactive materials, possibly inhaled or ingested from food or drink.
iv. Nuclear
Where the explosion of a nuclear device causes widespread effects due to blast, heat, and large amounts of harmful radiation. All of the above categories also pose a threat of environmental contamination. (Although it is important that the terminology relating to Hazmat and CBRN is understood, the type of initial incident does not alter the role or procedures that should be adopted by a Hospital Decontamination Team as the effects of any release and the measures required to mitigate them, will be broadly the same.)
2.4 Contamination
A person is contaminated when they have a hazardous substance in or on them. This document only refers to surface contamination.
2.4 Exposure
A patient who has been exposed to a hazardous substance may be suffering from the effects of that exposure but only need to be decontaminated if they are contaminated, e.g. a patient exposed to radiation from a remote source, or to a gas such as carbon monoxide does not need to be decontaminated.
2.5 Infectious Disease/Exposure to a Biological Substance
The dangers to others posed by a patient harbouring an infectious illness are not changed by decontamination. However, a patient contaminated with a biological material such as fungal spores does require decontamination.
3. Legal Responsibilities
The Trust is identified as a category 1 responder and has a statutory duty to provide care for patients including those that may be contaminated with chemical, biological, radiological material (or where the explosion of a nuclear device causes widespread effects due to the blast, heat and large amounts of harmful radiation). An incident involving the presence of such contaminated patients could, however, result in the contamination of an area and the subsequent closure of a facility or an entire site, and
7 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
thus impair the trusts capability to fulfil its statutory duty to provide healthcare for the community. As an employer we have a statutory duty to protect our staff and members of the public who might be affected by their activities from risk to health [Health and Safety at Work Act (1974)]. This duty includes a requirement to ensure that:
Appropriate Hazmat / Lockdown Risk Assessment has been carried out (within Lockdown policy)
Staff are provided with suitable facilities and equipment to carry out their duties (including personal protective equipment PPE)
Staff are adequately trained in their duties (including the use of any equipment)
The Civil Contingency Act (2004) (CCA) established the legislative framework for civil protection within the UK.
Deal with any emergency
Deal with any threat to the provision of normal services during an emergency.
Since the presence of self-presenting patients can be the result of an emergency that can pose a threat to the provision of normal service, The Trust should have plans in place to deal with such patients, and have such business contingency plans to deal with the consequential impact on normal service provision from such a scenario.
4. Decontamination Infrastructure 4.1 Board Responsibilities
The Trust must have adequate measures in place to ensure that, as far as reasonably practical, they can continue to provide their critical services in the event that potentially contaminated patients self-present at receiving sites. We must ensure that:
At strategic level there is a designated person (normally a Board Director, referred to here as the ‘Decontamination Policy Lead’ Emergency Planning Director) responsible to the Board for ensuring that appropriate decontamination arrangements are in place and are properly maintained a documented Hazmat/ CBRN Incident Plan is in place that is proportionate, practical, and clinically effective
The plan is subject to regular exercise (a minimum of at least once every 3 years) and review, and is maintained as a quality assured document appropriate equipment and facilities are provided suitable and sufficient quantities of Personal Protective Equipment (PPE) are provided
Staffs have been identified to carry out the various operations required to safely decontaminate patients (including a Decontamination Lead Officer who will lead the decontamination response). Such staff must be suitably trained. This requirement includes the provision of regular refresher training. There is sufficient resource available to implement the plan whenever necessary in a timely manner
Contingency Plans should account for self-presenters who arrive at SHFT facilities that do not have decontamination facilities. The Trust has no capability to deliver decontamination facilities.

8 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
4.2 Hazmat/CBRN Incident Plan and Risk Assessment
The Boards’ Hazmat/ CBRN Incident Plans, including plans to deal with self-presenting casualties from a Hazmat or CBRN incident should be developed with the involvement of appropriate experts and local multi-agency partners contained within the (Incident Response Plan) IRP (e.g. Ambulance Service, local Fire and Rescue Service, local Police Force, Local Authority,) and based on robust local risk assessments. NHS England with NHS London has developed Guidance for Primary and Community Care Facilities in preparation for incidents involving hazardous materials, which is included within this SOP at Annex 1. Plans should be held as quality controlled documents authorized by the Decontamination Policy Lead, and be subject to regular exercise and review. It is recommended that such plans dovetail with the Trust’s IRP which should include details of the appropriate communications arrangements. It is a requirement that the trust has a plan to lock down areas or an entire hospital to protect staff, patients, and facilities from possible cross contamination (see Trust Lockdown – Policy). The procedures in the plan should accommodate a range of circumstances ranging from those where casualties are brought in by the Ambulance Service (usually, although not always, already decontaminated) from the site of a major incident to contaminated individuals arriving by personal transport. Local plans should also take account of circumstances where provisions for Clinical Decontamination may be overwhelmed and should therefore provide for Improvised or Interim Decontamination and the option of Mass Decontamination (see 4.4 for definitions). Where decontamination requirements exceed site capability there should be pre-agreed arrangements in place with local partner agencies on what support can be provided to the hospital. These agreements should be made locally; this is listed within the IRP.
4.3 Decontamination Option
The majority of contaminated casualties will be decontaminated at the scene by the Fire and Rescue Services (this is also the case for Hazmat incidents). However causalities may present at SHFT sites with secondary contamination several hours after the incident. Our Community hospitals may be required by the FRS to help with decontamination of patients if a Major Incident has been issued by PHE (Public Health England). This will be directed by the on the on call director at suitable risk assed sites within the trust. (Lymington, Petersfield ,GWMH). Decontamination can take several forms ranging from improvised decontamination by persons responding to an immediate and necessary need, through to full Clinical decontamination. Any decision to decontaminate should be taken after appropriate assessments. Plans should include the full range of decontamination options available to sites and any response should be proportionate and reasonable. In some cases removing outer garments might be sufficient to remove the majority of contaminant present.
I. Improvised Decontamination:
The use of an immediately available method of decontamination prior to the use of specialist resources. It may be appropriate to initiate improvised decontamination prior to establishment of full procedure at a Hospital.

9 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
Dry decontamination should be used for self - presenting patients. This is contained within the (Appendix – 1). Contaminated clothing should be removed as soon as possible in accordance with the provisions in section 5.7.2. the person and dressed in appropriate clothing re-robe packs should be available for this purpose. Following any improvised decontamination, the decontamination lead should decide on any further appropriate action. This might involve further, more rigorous decontamination, referral for medical care or discharge.
II. Clinical Decontamination:
The process where contaminated persons are treated individually by trained healthcare professionals using purpose designed decontamination equipment. This is full wet decontamination using Clinical Decontamination Units. SHFT sites who are trained in Infectious disease are Lymington, Petersfield MIU/MAU are not equipped or designed to carry-out Clinical decontamination.
III. Mass Decontamination:
The planned and structured procedure delivered by the Fire and Rescue Service using purpose designed decontamination equipment, where there are large numbers of casualties.
4.4 Decontamination Equipment
a. First Strike Equipment (for improvised or Interim Decontamination)
This equipment may include buckets (designated clear and dirty)/sponges (individual to each casualty)/ towels/blankets/contaminated clothing bags (clear)/labelled bags for personal effects/dignity packs/cordon tape to mark off “dirty” and “clean” areas and should be used in a designated area outside the building. The Trust should consider the provision of equipment that can be deployed as a “First Strike” response. This is held at Moorgreen Hospital by the Duty Estates Manager on 0701 0072 516 in working hours. The duty engineer will be contacted and instructed to deliver the HAZMAT box where needed. The use of such equipment may be appropriate if it appears that there is a need for urgent decontamination and can be used alone or as an initial measure that is provided while other facilities are readied if required by PHE.
4.5 Decontamination Area
SHFT should consider the following when deciding where to carry out dry decontamination operations. The area selected should:
Allow for the creation of secure areas that allow proper flow of patients both pre and post decontamination
Where practical, ensure that patients are treated with dignity and respect
Ensure that access is maintained to the site for both the Ambulance Service and non-contaminated patients

10 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
Allow location of the “dirty side” such that it is both accessible for incoming contaminated patients and that it is away from entry and exit routes used for “clean” patients, other patients, and staff
Allow location of the “clean side” such that “clean” patients can move into the hospital building through a designated access point
Take cognisance of the direction of the prevailing wind and, where possible, the designated area should be down-wind of buildings. Similarly, with regard to the orientation of the decontamination unit/area, the “clean-side” should be up-wind of the “dirty-side”
Access to water and power supply from the hospital where applicable
Provide shelter and protection from the elements. 4.6 Personal Protective Equipment (PPE)
SHFT have a statutory obligation to protect the health and safety of their staff. As such, Boards must provide suitable Personal Protective Equipment for use by staff who may become exposed during decontamination operations and provide appropriate training in its use (including refresher training). This is included within Appendix – 1 The need for personal protective equipment, the type required (and the protection it offers) will be subject to local risk assessment and will depend on the contaminant involved. However the following provides a suitable baseline. Although the minimum requirements for PPE vary with the type of contamination present, it should be noted that, in the case of a terrorist incident, it may not be possible to tell if there is a single contaminant present or indeed what that contaminant is. A risk assessment may determine that the use of full PPE is most appropriate. If SHFT are in doubt then as a precaution full clinical decontamination (or in circumstances where numbers dictate, mass decontamination by FRS) using the appropriate PPE would be a reasonable course of action. For Airborne and VHF viruses (EBOLA) boxes are held at Lymington NFH MAU/MIU, Petersfield MIU, HAZMAT strike box Moorgreen Hospital.
a. Patient Potentially Exposed to Chemical Contamination
To protect staff from health risks arising from casualties who might have been exposed to chemical contamination the following PPE should be available:
Chemical resistant overall with integral hood
Chemical resistant gloves
Chemical resistant boots
Suitable respiratory protective equipment to protect against hazardous gasses, vapours, and airborne particles.
b. Patient Potentially Exposed to a Biological Agent which may Present a Risk of
Airborne Infection
For casualties who might have been exposed to a biological agent that presents a risk of infection, the following PPE should be available: See SHFT EBOLA Policy.
Full length fluid impermeable gown, apron, hair, and foot cover
Suitable respiratory protective equipment to protect against hazardous airborne particles to FFP3 standard
Face shield, visor, or goggles
Latex/vinyl/nitrile single use disposable gloves
11 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
c. Patient Potentially Contaminated with Radioactive Material
For casualties who might be contaminated by radioactive material, the following PPE should be available:
Disposable plastic apron
Full length fluid impermeable gown
Suitable respiratory protective equipment to protect against hazardous airborne particles to FFP3 standard
Latex/vinyl/nitrile double layer disposable gloves 4.7 Decontamination Team Roles
There are a number of roles that will need to be filled during a response to an incident involving potentially contaminated self-presenting casualties and it will therefore be necessary to form a multi-disciplinary team. SHFT should consider carefully the makeup of their decontamination team. Decontamination team members must have an appropriate background where they have patient contact as part of their normal duties. Everyone with a role within the response should receive appropriate training which must reflect the possibility that patients may arrive unannounced at any time of the day. Some of the roles that should be considered are listed below (note, this list is not intended to be exhaustive). Where appropriate, some of these roles may be combined.
a. Decontamination Lead Officer (Duty Nurse/Matron)
The Decontamination Lead Officer should assume command of the management of the overall decontamination response and is responsible for the overall management and recovery of the incident. In anticipation of the incident occurring without warning at any time, this role should be allocated, at least in the initial period, to an on-duty member of staff such as the nurse in charge. He/she should follow the Primary or Community Care Lead Action Card 4 (Appendix – 1) to determine whether there is a need to decontaminate self-presenters. If necessary expert advice should be sought to ensure that a suitable and sufficient risk assessment is carried out, based on the information available from self-presenting patients, the Ambulance Service, Medical Incident Officer (if deployed), Local Police, and other relevant professionals (i.e. on-call Public Health Professional, Radiation Protection Advisor etc.). The Decontamination Lead should take the lead role in determining the appropriate response with the support of relevant individuals. The factors that should be considered are the risk assessments, the number of casualties either present or expected, and the possible need to start decontamination urgently. This response could range from provision on buckets and sponges, the deployment of the decontamination facility, or the request for assistance from the Fire Rescue Service. b. Entry Control Officer
The function of the ‘Entry Control Officer’ is to log in and out staff undertaking decontamination of casualties and consider any safety requirements. SHFT should ensure that the staff that might be allocated this role are provided with specific training and equipment.
c. Decontamination Team (as directed by management)
SHFT should identify and train staff to carry out the decontamination of contaminated casualties. Consideration should be given to the make-up of this team. Decontamination

12 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
teams should include ‘safety teams’ i.e. staff in PPE ready to assist should a member of the Decontamination team get into difficulty. All staff in the decontamination or ‘safety team’ must be trained in the use of PPE and decontamination techniques
d. Crowd Control/Security
It may be necessary to control the movement of the public, patients, and staff, to ensure “clean” and “dirty” areas are clearly separated and, in particular, to prevent contaminated patients entering the hospital. It will be necessary to allocate staff duties associated with the creation of such zones (e.g. setting up barriers, directing traffic). Other roles that need to be considered include arrangements for staff call-out/incident alert, and arrangements to implement lockdown. Staff training should be augmented by the provision of Action Cards for each individual role, which provide users with clear, concise, and unambiguous instructions. These Action Cards must be easily accessible in the event of an incident (see Appendix 1 for suggested Action Card examples).
4.8 Other Healthcare Facilities
It is likely that, following a Hazmat/CBRN incident, most self-presenting patients will attend an Emergency Department although some casualties may attend other health facilities, e.g. Health Clinics, GP Surgeries. In these circumstances it is not practical for such facilities to have formal arrangements in place to deal with these casualties. However, such facilities are recommended to have:
The ability to lockdown should they receive a warning that self-presenting patients may arrive
The ability to quarantine any self-presenting patient that may enter the facility to minimise the risk of cross contamination of staff and other patients
Mechanisms in place to summon help from the emergency services
Provide appropriate staff training
The ability to undertake first strike if urgent decontamination required. 5. Incident Response 5.1 General Principles
SHFT’s incident response should reflect the following general principles: all persons who self-present from the scene of a Hazmat/CBRN incident should be considered contaminated until the UK CBRN and Hazmat Decontamination Algorithm/ decontamination triage has determined otherwise the need for critical medical care should take priority over decontamination provisions but should, to the maximum extent possible, be subject to risk assessment to determine the appropriate precautions notwithstanding the need for medical intervention, early decontamination remains a priority, and should be done before a casualty enters any part of a hospital building.
5.2 Incident Response Trigger
An incident involving chemical, biological, or radiological contamination can be heralded by one or more of the following triggers:
Receipt of a warning from the emergency services, an industrial site, the military, or other source
The arrival of patients giving a history of exposure
The unannounced presentation of a small or large number of casualties exhibiting collapse, skin blistering/burns, visual disturbance, sweating, breathing difficulties,

13 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
lachrymatory symptoms, salivation, convulsions, muscle tremors, hoarseness, or major gastro intestinal disturbance. (It is important to note that exposure to some dangerous substances may not result in symptoms in the initial period).
In circumstances where the first notification of an event involving CBRN/ Hazmat materials is the unannounced presentation of casualties, SHFT have a requirement to notify other agencies. (ie PHE Wessex Health Protection Team 0345 055 2022 / OoH 0844 967 0082)
5.3 Incident Plan Activation
Any of the triggers discussed in Sub-section 5.2 should activate the Business continuity plan and where appropriate the Trusts Hazmat/CBRN Incident Plan. The initial phase of such a plan should include a procedure which involves the notification of key departments/individuals. These include:
Site responsible person
“On-call” Duty Manager for service provided
The Decontamination Lead Officer (on call director)
The initial response might be to establish a Control and Management Team to make strategic decisions and communicate with other organisations. The team should be based at Tatchbury Mount Sterne 7. It might also be appropriate to initiate the Hospital Lockdown Plan as a temporary measure, pending receipt of further information relating to the extent of the incident. These arrangements can be revoked or extended as required. Plans should address what support will be available from the Police in locking down a hospital should it be required.
5.4 Casualty Reception
Decontamination Plans should provide that, where there is adequate warning, of their impending arrival, contaminated casualties should be received out-with the hospital, in an area that prevents cross contamination of other patients, staff, and the public. Where there is no warning, it is possible that potentially contaminated self-presenting patients will gain access to the hospital building. Plans should include arrangements to remove such patients to an appropriate area, which might be outside the hospital, for triage and possible decontamination, and should also include arrangements to deal with any area of the hospital that might have become contaminated (see Sub-section 5.7.5 for further details). Specific awareness training should be provided to those staff that may either receive the first notification of an incident or come into first contact with self-presenting patients (e.g. Receptionist, Porters).
5.5 Incident Intelligence
Following activation of the Incident Plan, the Decontamination Lead Officer or appropriate on-call manager should seek the following information:
The likely number of self-presenting casualties
The type/identity of the contaminant symptoms
Precautions necessary
Preferred method for decontamination
14 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
The Decontamination Lead Officer/appropriate on-call manager might need to contact some or all of the organisations listed below, and up to date contact numbers should be readily available for:
The local Emergency Services
Ambulance Services/NHS Staff at scene of the incident (i.e. Medical Incident Officer)
On-call Public Health Professional
Radiation Protection Advisor
National Poisons Information Service
Police National CBRN Centre
Centre for Radiation, Chemical and Environmental Hazards
This information will assist the Decontamination Lead Officer/appropriate on-call manager to undertake a robust risk assessment, and to determine:
The level of response that is required
The decontamination equipment required
The level of PPE required
The nature and extent of any lockdown
In cases where there is a lack of warning and a need for urgent action, prompt risk assessment and decision making based on limited information and advice from other organisations might be required. This may result in a decision for urgent decontamination of casualties whose contamination status is not clear.
5.6 SHFT Sites Preparation
Plans to deal with the arrival of self-presenting contaminated or potentially contaminated casualties should include arrangements to segregate them from other patients. Decontamination should not be an automatic response to the arrival of potentially contaminated casualties. An initial assessment of self- presenting, potentially contaminated, casualties should be carried out by a suitably trained and suitably protected Decontamination Triage Officer.
5.7 Patient Care Prior to Decontamination
Since the bulk of any contamination is likely to be present on casualties’ clothing, plan should include provision of the removal of clothing as soon as possible on arrival at hospital. Contaminated clothing should be placed in double (clear) plastic bags, sealed, and labelled. Personal belongings should also be placed in appropriately labelled bags. Plans must also consider the need to protect, as far as possible, patient dignity and be flexible enough to accommodate the needs of vulnerable persons (see section 5.7.4). In addition, plans should include arrangements to provide some protection from the elements. It should be noted that certain groups of patients may be unwilling to undress in public due to cultural and/or modesty issues and, where practical, alternate arrangements should be considered to accommodate such individuals. Only basic life support and first aid (simple airway opening manoeuvers, bag-value-mask ventilation, and pressure on wounds) might be possible prior to and during decontamination (notwithstanding the fact that clinical needs should determine the priority of life saving intervention if necessary). An emergency bag containing appropriate disposable equipment should therefore be available for this purpose. Staff conducting such interventions must be appropriately trained and wearing protective equipment where appropriate.

15 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
5.7.1 Decontamination Response
The response to the arrival of self-presenting casualties requiring decontamination might range from the deployment of:
a. First Strike Equipment
The Decontamination Lead Officer might decide that the appropriate response to an incident may be the issue of first strike equipment. This response may be appropriate when:
There is perceived need for urgent decontamination and /or treatment which cannot wait until a Decontamination Unit is deployed (further decontamination may then be undertaken within the Decontamination Unit depending on the risk assessment)
a small number self-present at SHFT sites
as a first response whilst awaiting deployment of the Decontamination Unit from local FRS (such decontamination may either be carried out by SHFT staff or by the patient).
It will then be the subject of a local risk assessment as to whether an individual who has been through interim or improvised decontamination needs further decontamination.
b. Assistance from Other Agencies
If the numbers of self-presenting casualties is assessed as likely to exceed the capacity that the Decontamination Unit can cope with, it might be necessary to revert to ‘First Strike’ provisions or to call for assistance from the Ambulance Service, the local Fire and Rescue Service and/or other Trusts. It should be noted that the resources of the Ambulance Service and the Fire and Rescue Service may already be deployed at the scene of the incident and their capability to respond to any call for assistance may be limited in the first instance. However, it is important that, in such circumstances, contact is made with the emergency services (including the Police) and any appropriate action can be determined by risk assessment of the overall situation. Prior multi-agency planning should consider what support will be made available to Hospitals. If the emergency services cannot provide the necessary support within a suitable time-frame, it is recommended that plans should include the ability to provide improvised decontamination (e.g. the provision of buckets and sponges, the facility to hose down patients etc.).
c. Radiological Contamination
Although the arrangements for dealing with persons contaminated with a radioactive substance will, in general, be the same as for those contaminated with a chemical or biological contaminant, the following should be noted:
The radiation dose rate from contamination is usually small
The risk to staff involved in decontamination of such patients is normally low
The use of a radiation detection device by appropriately trained staff can determine initial levels of radiation and the efficiency of decontamination
Patient’s treatment can take priority over decontamination (however, in this cases where the need for treatment is not urgent, it may be prudent to decontaminate first to reduce the likelihood of cross contamination).
It may be necessary to carry out secondary decontamination to remove residual contamination. Such decontamination is best carried out with the shower area and the use of a radiation detection device may assist in this progress. These instruments must only be used by appropriately trained staff.

16 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
Although the risk may be reduced, precautions should be in place to prevent/minimise potential cross contamination of persons/facilities.
(Note: contamination with radiological material may be accompanied by chemical or biological contamination and appropriate precautions and decontamination procedures must be in place in such cases.)
5.7.2 Vulnerable Persons
The specific needs of vulnerable persons (as defined in the Protection of Vulnerable Groups (is recognised within the CCA (2004) and plans should include arrangements to deal with such groups. Vulnerable persons requiring consideration are:
i. Children under the age of 16 may either attend the Emergency Department as a
casualty or as a member of a family or group caught up in the event. Plans need to reflect procedures for dealing with children and young people that may arise directly or indirectly from an incident (including cohorting of family groups).
ii. Persons inhibited in physical movement caused by age, illness (including mental illness), disability, pregnancy, or other reasons.
iii. Deaf, blind, and visually and hearing impaired persons.
iv. Those persons from non-English (or non-Gaelic) speaking communities and faith
groups.
v. Persons with learning disabilities or mental illness.
5.7.3 Decontamination Methodology
National Ambulance Resilience Unit (NARU) Initial Operating Response (IOR) for Community based services should be by the dry de-contamination method the link below explains the methodology behind this contained within Appendix 1.
Initial Operational Response (IOR) for the wider NHS | NARU
5.7.4 Patient Care Post
Plans should include provision for re-robing, and appropriate aftercare. This may involve admission to Hospital for treatment or observation, transfer to local Rest Centres or other place of safety (for continuing aftercare or observation) or discharge. Clothing and valuables will not be returned to individuals until appropriate scientific advice regarding decontamination has been received and plans should bear this in mind. Although externally decontaminated there may still be internal contamination. The Trust’s Plan should provide provision for the isolation of such patients to avoid potential cross-contamination of staff and other patients. (Such a provision should also be in place for relevant patients transferred to hospital by the Ambulance Service). Staff should remain vigilant for ill effects in the decontaminated person and in potentially contaminated colleagues. Patients who self-present following a CBRN incident may have been witness to a criminal act. Although the need to preserve life remains the priority in such cases, plans should include arrangements to record contact details of those persons that do not require further treatment following decontamination prior to discharge. Plans should also consider aftercare requirements (i.e. follow up by Public Health).

17 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
5.7.5 Southern Health Staff
Plans must address the need to consider those staff that may have come into first contact with self-presenting casualties (e.g. receptionists, porters, nurses) and who may have become contaminated. Arrangements should be in place to quarantine such staff, assess them for potential contamination, and if necessary decontaminate, and provide any medical treatment and counselling as necessary.
6. Post Incident 6.1 Staff Debrief
A staff debrief should be held as soon as practical after the incident has been concluded and a report issued. This report should include lessons identified and any relevant actions. The trust Decontamination Plan should be amended as appropriate to reflect these lessons learnt. Where other agencies were involved a multi-agency debrief may be beneficial.
6.2 Management of Decontamination Equipment
Equipment used during the decontamination process should be considered as potentially contaminated and should be quarantined until decontamination can be carried out. Advice on the appropriate method for equipment decontamination can be obtained from: the company responsible for the contamination (post a Hazmat incident at an industrial site/transport spillage etc.) other industry experts (i.e. the manufacturer) The Government Decontamination Service (GDS) Public Health Department
6.3 Building Decontamination
When contaminated patients have gained entry to an SHFT site and/or other parts of the site, these areas should be considered as potentially contaminated and should be subject to quarantine/restricted access (see 5.7.5 for measures) until the area can be decontaminated. Hospital Buildings should be treated in line with The Strategic National Guidance on the Decontamination of buildings, infrastructure and open environment exposed to chemical, biological, radiological or nuclear materials (Cabinet Office, 2011).
6.3 Contaminated Clothing and Personal effects
Clothing, valuables and personal items removed from self-presenting casualties must be considered as contaminated and expert advice should be sought prior to their return to their owner (e.g. Public Health, HPS, GDS) or as to the appropriate means for disposal. It should be noted that, in those cases where there has been a CBRN incident, such items of clothing may be required by the Police as criminal evidence. Any equipment that cannot subsequently be decontaminated effectively and economically should be disposed of as contaminated waste. The final disposal of this waste should only be undertaken after the hazard has been identified and specialist advice taken on the safest disposal options to prevent further contamination or harm.
6.4 Transportation of Contaminated Waste
Depending on the type of contaminated waste, advice must be sort from PHE guidance as mentioned 5.7.3 b. A reputable and licenced waste contractor must undertake transport to the incinerator. Prior to collection by the contractor waste must be stored securely and access restricted to authorised and trained personal. To arrange waste collection please contact:

18 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
Veolia Helpdesk on 0845 606 0460 or [email protected] (working hours) Roger Scott 07407 734611 or Andy Higgins 07425 620954 (out of hours for Ebola waste only)
19 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
Appendix 1
Preparation for Incidents involving Hazardous Materials Guidance for Primary and Community Care Facilities
This document has been adapted from the NHS London guidance for Southern Health NHS Foundation Trust.

20 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
Introduction
1
This practical guidance document is aimed at preparing primary and community-based health facilities to be able to manage the consequences of a hazardous incident occurring somewhere else (also refer to as chemical, biological, radiological, nuclear or explosive incident – CBRNE). In these incidents there is a need to care for people, but also to be aware of the safety risk to staff and patients from secondary contamination as a result of people self-presenting at their facility seeking assistance. Primary and community care facilities include GP practices, pharmacies, dentists, opticians, health clinics, walk-in-centres (WIC’s), minor injury units (MIU’s) and community hospitals without emergency departments. Aim of the guidance:
To enable primary and community care practitioners to adopt simple
planning and response principles that would enable care to be provided to
people self-presenting as a consequence of a hazardous incident, at the
same time as protecting staff, patients and property from secondary
contamination.
To support primary and community care practitioners in the planning for a
hazardous incident by providing a resource pack, including:
Action cards for front line responding staff
Guidance for primary and community care leads to follow in the
preparation and response to an incident.
To promote an understanding of the implications of a hazardous incident on
the business continuity of the primary or community care facility.
Background: Experience from hazardous or potentially hazardous incidents such as the Tokyo sarin attacks of 1994 and 1995, and the London bombing of 2005, demonstrate that large numbers of people may self-evacuate, if they can, and leave the scene without first coming into contact with the responding emergency services. Later, once symptoms have developed, or as a result of widespread media coverage, they may self-present to primary or community care health facilities in search of treatment, advice and reassurance. A proportion of these people will be ‘worried well’ who have not been contaminated, but still concerned about their possible exposure to toxic substances. However, some will have been exposed and may need treatment, and may retain a degree of contamination on their bodies or clothing, posing a risk to healthcare staff that they come in to contact with. It is likely that the resources of the emergency services would be fully committed at the scene of the incident. Primary and community care facilities should, therefore, plan for unsupported management of self-presenters in the initial stages, obtain specialist advice, provide information to keep people calm, and wait for the emergency services to release resources to provide assistance.

21 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
Although primary and community care practitioners have access to HPA guidance’ they have
received little or no practical guidance on how to apply this locally, or support with staff
training. This is supported by learning from exercises, which among other things has shown
that there is a lack of specific guidance on the management of self-presenters, and not
enough consideration given to primary or community care preparedness for each type of
incidents.
Findings from a number of exercises, studies and workshops carried out across the country and in London since 2005 that focused of primary care preparedness to hazardous incidents identified that the majority of staff felt unprepared; were concerned that their views (especially frontline staff most at risk) had not been considered; and had not received any training. For example interviews with frontline staff in South West London revealed that receptionists and nurses at GP practices were concerned that plans should include assurance that their families would not suffer from cross-contamination when staff members return home.
If further assistance is
required this can be
supported by those
responsible for NHS
emergency
preparedness; providing
advice on localising the
guidance and assistance
with staff training
where required.

22 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
Contents
Ref
No.
Content Use and suggested storage
1
Contextual document – outlining
the purpose of the guidance
For all staff – contextualises the risk and
explains the purpose of planning.
2
Receptionist Action Card
Gives clear and direct actions for reception
staff (or person in first contact) to follow
when an incident occurs. To be kept
accessible but out of public sight behind
reception.
3
Preparation guidance and checklist
for the primary or community care
lead
An aide memoire for the primary or
community care lead person giving
information and guidance on local planning.
Used in advance of an incident occurring for
preparation of the staff and building.
4
Primary or community care lead
Action Card
A flow diagram for the primary or
community care lead to follow when
suspected contaminated people begin to
arrive. One copy to be kept easily
accessible.
5
Actions to follow after an incident
involving a hazardous material
Provides recovery considerations for your
patients, staff and buildings after an incident
has finished.
6
Patient content template
For recording the details of people who are
affected by the incident. Should be
photocopied and copies kept in the Response
box for ease of access.
A1
Additional information
Providing further information on Lockdown,
Personal Protective Equipment requirements
and the Response Box (that is recommended
you consider developing).
A2
Signage Template
Template to allow you to create specific local
signage to direct people when an incident
occurs. To be kept in your Response Box.

23 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
Receptionist Action Card
Preparation for incidents involving Hazardous Materials
2
Something unusual has happened
Which makes you suspicious
Think through the following steps 1-2-3
STEP 1
One casualty
Manage us
STEP 2
Two casualties with similar symptoms and no apparent cause
Manage with caution and consider
risk to staff and others
STEP 3
Three or more casualties with similar symptoms and no apparent
cause
Manage as an incident involving hazardous materials risk assess
before intervening Isolate and seel specialist help
immediately
IMMEDIATE CONTACT/LEAD PERSON INSERT NAME AND CONTACT DETAILS HERE
Director on Call: Flextel: 070 1703 1107 Public Health England HPU: 0345 055 2022 Out of Hours: 0844 967 0082
FOLLOW YOUR ACTION CARDS
Think of your own safety and that of your colleagues. Call for help. Isolate your area.
Inform patients that help is on the way.
24 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
Receptionist Action Card
Preparation for incidents involving Hazardous Materials
2
Something unusual has happened
Which makes you suspicious
FOLLOW STEPS 1-2-3
Alert primary/community cares leads using internal communication system and follows any advice provided
Agree who calls 999 for the emergency services
Consider yourself and others lose by as contaminated
Lock down reception area – see locally developed lockdown plan
Prevent other staff from entering reception area
Direct contaminated patients to isolation area
Open response box
Put on personal protective equipment (PPE) if available
Put up pre-printed laminated signs
Advise all patients that help is on the way
Record patient details on the patient contact template
Wait for assistance
Keep patients informed
Follow specialist advice provided by the emergency services or local health
protection unit (PHE)

25 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
Aide Memoire
Preparation for incidents involving Hazardous Materials
3
Preparation guidance and checklist 1
st – PREPARE THE BUILDING
TICK
Identify an area where you can isolate people who self-present having been potentially exposed to a hazardous material or substance
Identify how you would lock-down’ areas to protect staff and patients
Produce signage for front of building, entrance area, reception area and isolation room to inform patients on actions they should take
Place preparation and response cards in reception and back office
2
nd – PREPARE MANAGEMENT AND LOGISTICS
TICK
Agree management arrangements with senior staff – who will be in charge?
Prepare a response box to be held near reception containing:
A Map – A drawing of the layout of the building showing isolation area marked, doors to be locked and where signage should be placed
B Laminated signage – Clearly identifying where they should be placed
C Action Cards – Identifying who will do what, where and when
D Pre-printed forms – List of effected people, patient contact template
E
Personal protection and cleaning equipment – Gloves, aprons, masks, tissues
Contact numbers – Consider who you need to inform and who can provide advice and guidance:
Insert contact details
Director on call: Flextel 070 1703 1107
Public Health England HPU: 0145 055 2022
Prepare a management pack containing copies of this guidance, HPA CBRN guidance, contact numbers, map/layout drawing and pre-printed forms
Consider staff welfare arrangements – see recovery details (section 5)
3
rd – PREPARE THE STAFF
TICK
Ensure all staff, in particular frontline staff, know how: to assess the risk, to lockdown the building, to obtain information and advice, to keep patients informed and who performs which role in the practice
Ensure all staff know where the response box is held and what it contains
Ensure all staff are aware of procedures and protocols for assessment and treatment of contaminated staff and patients
Ensure all staff are familiar with (and can access) business continuity plans for the practice, know what they entail, and how and when to activate them
Rehearse the plan with your staff regularly

26 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
OVERVIEW
Aim
For primary and community care facilities to be able to take necessary actions to prepare themselves for the consequences of an incident involving hazardous materials
Objectives
To care for self-presenters; to maintain staff safety; to recognise the role of frontline ‘first receivers’; to maintain essential services; to return to normal business as soon as possible.
Why prepare
Following an incident where people have been exposed to hazardous materials many worried well and potentially contaminated people self-present at primary and community care facilities without having been assessed or treated by emergency services at the scene. Evidence shows that frontline healthcare staff can suffer secondary contamination if they are not prepared for such incidents.
PRINCIPLES OF PREPAREDNESS FOR PRIMARY AND COMMUNITY CARE
Recognise unusual circumstances and be aware of the risks Manage the incident and limit the spread of contamination Give priority to minimising exposure and safety risks to staff Provide care and information to patients Communicate and obtain guidance from external agencies and other primary care facilities Maintain business continuity and recover to normal business as early as possible
KEY PREPARATION ACTIONS
1st
– PREPARE THE BUILDING
How do you lock down your facility to prevent people entering?
Produce a lockdown procedure starting with the reception area and train staff.
How to isolate people and limit the spread of contamination?
Identify an isolation area. Have signage ready. Train staff in isolation procedure
2nd
– PREPARE MANAGEMENT AND LOGISTICS
How are you alerted to the risk? Coordinate with NHS and health partners. Make sure that systems to alert you are correct and are tested regularly.
How to assess the risks to your staff and facility?
Train staff to understand the range of risks. Produce a quick reference checklist. Further support will be available from your HPU (PHE) or local emergency planner.
How to manage the incident? Identify who will be in charge. Produce an action card for the incident manager. Train staff and conduct exercises.
How to cascade alerts and information?
Produce a contact list for external agencies and primary care organisations. Test alerting cascades regularly.
Who to contact to obtain advice and guidance?
Produce a contact list of who can provide you with advice and guidance. Ensure that you know how to contact your local HPU (PHE), where further advice will be given at the time.
How to continue business as usual? Maintain a current and tested business continuity plan.
3rd
– PREPARE SATAFF
How to prepare frontline staff (first receivers) to be aware of and recognise risk?
Train frontline staff in Steps 1-2-3 safety code previously described.
How to prepare back office staff to support frontline staff and manage these incidents?
Train staff in how to support frontline staff.
How to minimise exposure and keep staff safe?
Train frontline staff in infection control procedures and to minimise contamination risk.
How to care for self-presenters? Produce procedure for frontline staff assess patients, then to advise on what information to give patients, and what treatment to provide if advised to do so. Ensure that staff are aware that expert information will be provided about when and how it is safe for staff and patients to leave.
What equipment to have ready? Consider the preparation of a response box to be available at reception with suitable personal protection equipment and selected items (forms etc.). Ensure that PPE is reviewed and updated regularly. Provide action cards to staff. Test internal alarming six monthly (recommended). Consider conducting exercises with local partners.

27 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
Primary or Community Care Lead Action Card 4 You need to be aware that:
It may not be obvious that someone has been in contact with a hazardous material Patients may arrive with no prior warning Their symptoms may be non-specific e.g. itchy skin, watering eyes, respiratory problems, dizziness or nausea. History taking will identify if the patient believes they have been involved in:
an explosion, fire, cloud of smoke or gas,
being covered in dust, powder or liquid as the result of an accident,
an industrial or agricultural incident ; spillage or transport accident or something similar.
Manage self-presenters according to specific guidance received from Local HPU (PHE) if applicable on
general guidance (see Note 2). Establish communications with Public Health and Local HPU (PHE) for further information Protect yourself and other patients/staff and premises by using isolation procedures. PPE (if applicable),
cleaning, lockdown etc. according to general guidance (see Note 3) Keep accurate details of patients seen. Your response will be supported by the Emergency Services, following your call to them.
STEP 1 One casualty
Manage using normal protocols
STEP 2 Two casualties with similar symptoms and no apparent cause
Manage with caution and consider risk to staff and others
STEP 3 Three or more casualties with similar symptoms and no apparent cause
Manage as an incident involving hazardous materials risk assess before intervening Isolate and seel specialist help immediately
Ambulance service/Health Protection Agency/ Public Health England: Identify hazardous substances Assess impact on health HPA (PHE) – formulate specific guidance for primary and
community care Issue guidance to GP’s, Walk in Centres (WIC’s) etc.
via email/fax no. decided by locality
GP, WIC assessment of location etc. Are we likely to be involved?
Receive telephone call from Receptionist/ member of staff alerting you to problem
Ensure you: 1. Call 999 if there is a medical emergency 2. Contact local HPU (PHE) – 24 hour
number Insert contact details here 0345 055 2022
INCIDENT OCCURS EXTERNAL ACTIONS INTERNAL ACTIONS
SEE NOTE
1
NO YES
Monitor
situation
Actions to prepare for self-presenters Before self-presenters arrive 1. Consider locking down the practice and/or building, inform and prepare staff 2. Position signage outside of building – requesting presenting patient to contact reception and
remain outside the building. 3. Inform PCT Director on call of the situation If self-presenters have already arrived: 1. If contaminated patients have already arrived then the Receptionist of person in first contact
should now be considered contaminated and must not leave the ‘dirty’ contaminated area. 2. Lockdown the building; establish ‘clean’ and ‘dirty’ segregation areas within the building; put up
signage outside; keep patients and staff informed. 3. Cancel non-urgent appointments and undertake any other business continuity actions. 4. Have you received guidance? (see Note 1).
YES NO
NO YES Self-presenters arrive?
SEE
NOTE 2
SEE
NOTE 3

28 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
Notes Preparation for incidents involving Hazardous Materials 4 Note 1 Whenever an incident resulting in contamination (or possible contamination) of people, animals, air,
water, food etc. is known to have taken place, identification of the substance is a priority. Several agencies can be involved in making this identification and in assessing the impact on human life and the environment, once the substance is known. The HPA (PHE) will assess the impact on Public Health and will provide advice to the affected premises as well as advice and communications to the Local Authority and local NHS.
If the incident may have implications for the community, information will be developed by the HPU (PHE) regarding the contaminating substance (if known) and the risks and action to be taken in the event of self-presenters. This will be sent out as quickly as possible to primary and community care providers.
The message will be sent widely, not just to premises in the immediate vicinity because contaminated people may have travelled some distance before deciding to seek help.
Self-presenters should be managed according to the instructions in the guidance. Note 2 If advised by your Local HPU/PHE to commence decontamination, the following guidance may apply: General Decontamination Guidance: In the absence of any decontamination equipment /PPE etc. isolate the patient and call for
assistance. Decontamination should begin as soon as possible. All outer clothing should be removed, put into a plastic bag and sealed. Up to 80% of any
contamination will be removed in this way. Clean gowns could be provided if available. Any valuables e.g. wrist watch or phone should be put into a plastic bag and sealed. Depending on
the decontaminant it may be possible to decontaminate these at a later date. If the contamination is in dust form, the skin should be dusted off first to remove as much as
possible. The person should immediately be offered wipes for face and hands, and a tissue to blow their nose.
These should be disposed of into a plastic bag. If available, offer soap and water for the person to begin washing. Contamination will be washed
into the water and dilute enough to allow it to be safely poured into drains. Provide clean gowns/blankets for the person to use after washing. Previous ‘dirty’ laundry should be
placed in a bag and sealed. Once washed, ensure that the person remains in the designated ‘clean’ area, preventing re-
contamination. Reassure the patient and provide any relevant information. Clinical need will determine whether transfer to hospital is required. Be aware that the ambulance
service may be under severe pressure during a large scale incident. Once decontaminated ask the patient to stay in the clean area until further information/advice is
available regarding the contaminant. Allow the person access to the telephone (if possible) for them to inform relatives.
Note 3 Protecting yourself, others patients/staff and premises: The aim is to minimise the contact that the potentially contaminated patient has with other people
and parts of your premises. Immediate action – isolate the person in a separate room – preferably somewhere without soft
furnishing. Do not touch them. Cordon off the part of the premises they have walked through and anything they have touched. If
necessary lock the doors and put notices up outside the premises to redirect other patients away from the area.
Those involved in patient contact should wear the following Personal Protective Equipment (PPE) if available:
Apron or gown
Gloves
Mask (highest specification available) *PPE will usually only be affected during clinical contamination incidents.
PPE should be disposed of as contaminated waste. Re-route other patients away from the area. Staff and patients who have come into contact should be reassured and asked to stay on the
premises until further information is received about the contaminant.
29 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
Preparation for incidents Involving Hazardous Materials 5 PATIENTS – Recovery Information
1. Ensure detailed records of all patients involved within your premises have taken and are kept. Include name, DOB, home address, contact telephone number, GP, symptoms and any action taken – see Patient Contact Template.
2. Keep in contact with the ambulance service and your local Health Protection Unit (PHE) for updates and further advice on sending patients home or moving patients for further care.
3. Continuing sensitive and timely communication with your patients and the public will help ensure their on-going cooperation and provide reassurance.
Explain the current situation and your on-going plans Set out options for the different categories of patients (i.e. exposed patients, worried well, urgent
regular cases, regular non-urgent cases). Consider introducing clinical triage (assessment) at reception Use sign-posting at the front entrance and within the building Create a temporary answer-phone message for the recovery phase 4. Consider the welfare of your patients: Provide hydration and refreshments if at all possible Provide clean clothing and blankets. ‘Dirty’ clothing should be sealed in plastic bags if advised by the
Local HPU (PHE) Ensure they have access to regular medications they may be on Ensure access to telephones for the purpose of contacting friends and relatives and making
arrangements for dependents STAFF – Recovery Information
1. Consider staff welfare: Provide refreshments and regular breaks where possible Provide clean clothing blankets Consider arrangements for transporting staff home when it is safe to do so Ensure they have access to any regular medication they may be on Ensure access to telephone for the purpose of contacting friends and relatives and making
arrangements for dependents Consider the potential need for ongoing psychological support for staff involved in the incident 2. Maintain service continuity Review workforce plans – including the availability of staff/critical resources and staffing
arrangements for the next working days Consider when normal services can continue and how long contaminated staff might be off work.
Refer to your service business continuity plan and liaise with your ‘buddy’ practices/local pharmacies/partner clinics etc.
Review any missed or cancelled appointment later in the day to cancel their appointment and/or redirect them to another practice
If you have a ‘buddying’ system in place then contact your ‘buddy’ practice to arrange for them to support your recovery actions – which may include allocating space for you to continue seeing your own patients
Prioritise your essential services and urgent patients until normal service can resume 3. Consider any financial impacts to your business 4. Afterwards, consider undertaking a full review of the incident and response plans, and update as
necessary. BUILDINGS – Post Incident Information
1. Take advice from the Local HPU (PHE) on identifying areas in the building that require deep cleaning or decontamination.
2. The contaminated area should not be re-opened until advice has been taken from the Government Decontamination Service (GDS), or other designated provider of specialised decontamination information. There may need to be a specialised thorough decontamination of the area. The HPU (PHE) will provide this information locally.
3. Any contaminated clothing and washing products or used PPE should be double bagged and stored in the ‘dirty’ zone within the isolation area. Advice on how to deal with, or dispose of the contaminated clothing should be taken as it may be required as evidence by the police.
4. Significant contamination incidents will initially be treated as crime scenes for the preservation of evidence relevant to subsequence investigations. Therefore, no property or documentation should be discarded.
5. Take advice about potential contamination of the water supply from the HPU (PHE) or water supplier.
30 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
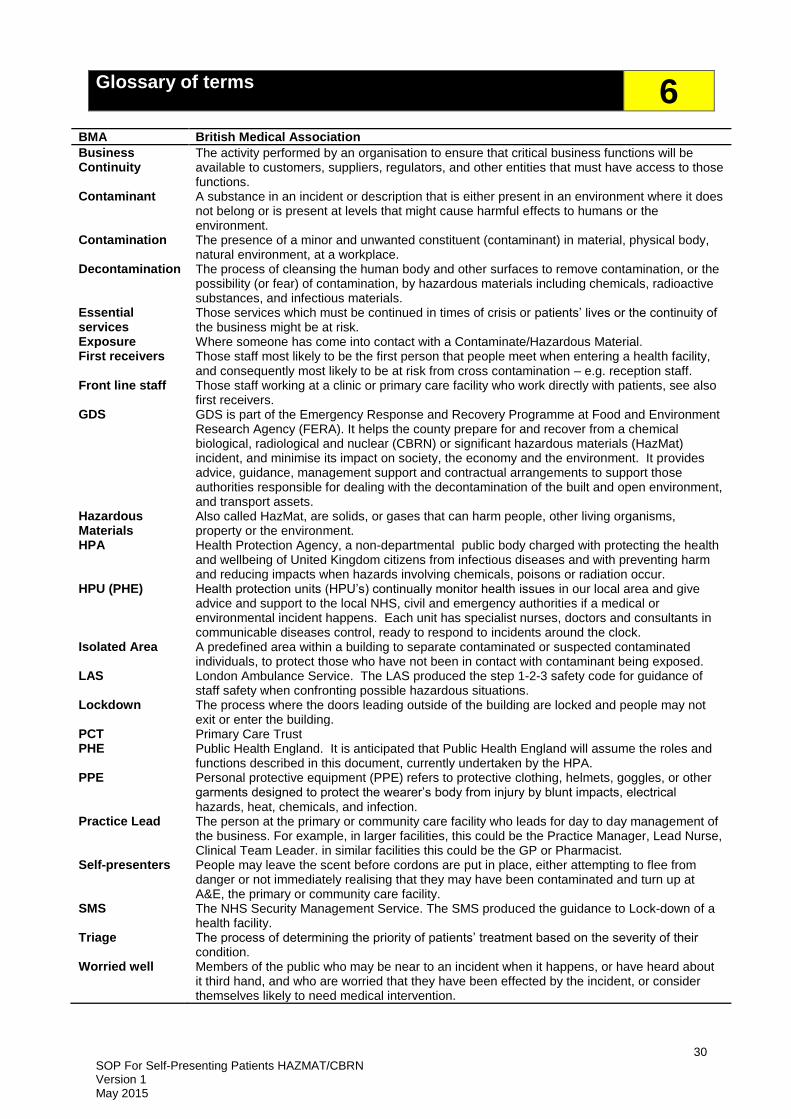
Glossary of terms 6
BMA British Medical Association
Business Continuity
The activity performed by an organisation to ensure that critical business functions will be available to customers, suppliers, regulators, and other entities that must have access to those functions.
Contaminant A substance in an incident or description that is either present in an environment where it does not belong or is present at levels that might cause harmful effects to humans or the environment.
Contamination The presence of a minor and unwanted constituent (contaminant) in material, physical body, natural environment, at a workplace.
Decontamination The process of cleansing the human body and other surfaces to remove contamination, or the possibility (or fear) of contamination, by hazardous materials including chemicals, radioactive substances, and infectious materials.
Essential services
Those services which must be continued in times of crisis or patients’ lives or the continuity of the business might be at risk.
Exposure Where someone has come into contact with a Contaminate/Hazardous Material. First receivers Those staff most likely to be the first person that people meet when entering a health facility,
and consequently most likely to be at risk from cross contamination – e.g. reception staff. Front line staff Those staff working at a clinic or primary care facility who work directly with patients, see also
first receivers. GDS GDS is part of the Emergency Response and Recovery Programme at Food and Environment
Research Agency (FERA). It helps the county prepare for and recover from a chemical biological, radiological and nuclear (CBRN) or significant hazardous materials (HazMat) incident, and minimise its impact on society, the economy and the environment. It provides advice, guidance, management support and contractual arrangements to support those authorities responsible for dealing with the decontamination of the built and open environment, and transport assets.
Hazardous Materials
Also called HazMat, are solids, or gases that can harm people, other living organisms, property or the environment.
HPA Health Protection Agency, a non-departmental public body charged with protecting the health and wellbeing of United Kingdom citizens from infectious diseases and with preventing harm and reducing impacts when hazards involving chemicals, poisons or radiation occur.
HPU (PHE) Health protection units (HPU’s) continually monitor health issues in our local area and give advice and support to the local NHS, civil and emergency authorities if a medical or environmental incident happens. Each unit has specialist nurses, doctors and consultants in communicable diseases control, ready to respond to incidents around the clock.
Isolated Area A predefined area within a building to separate contaminated or suspected contaminated individuals, to protect those who have not been in contact with contaminant being exposed.
LAS London Ambulance Service. The LAS produced the step 1-2-3 safety code for guidance of staff safety when confronting possible hazardous situations.
Lockdown The process where the doors leading outside of the building are locked and people may not exit or enter the building.
PCT Primary Care Trust PHE Public Health England. It is anticipated that Public Health England will assume the roles and
functions described in this document, currently undertaken by the HPA. PPE Personal protective equipment (PPE) refers to protective clothing, helmets, goggles, or other
garments designed to protect the wearer’s body from injury by blunt impacts, electrical hazards, heat, chemicals, and infection.
Practice Lead The person at the primary or community care facility who leads for day to day management of the business. For example, in larger facilities, this could be the Practice Manager, Lead Nurse, Clinical Team Leader. in similar facilities this could be the GP or Pharmacist.
Self-presenters People may leave the scent before cordons are put in place, either attempting to flee from danger or not immediately realising that they may have been contaminated and turn up at A&E, the primary or community care facility.
SMS The NHS Security Management Service. The SMS produced the guidance to Lock-down of a health facility.
Triage The process of determining the priority of patients’ treatment based on the severity of their condition.
Worried well Members of the public who may be near to an incident when it happens, or have heard about it third hand, and who are worried that they have been effected by the incident, or consider themselves likely to need medical intervention.

31 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
Patient contact template (additional copies may be made) Preparation for incidents involving Hazardous Materials 7
No.
Family Name
First Name
Date of Birth DD/MM/YY
Address (inc. postcode)
Telephone No.
GP
Contamination details/ Symptoms/Actions Taken
32 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
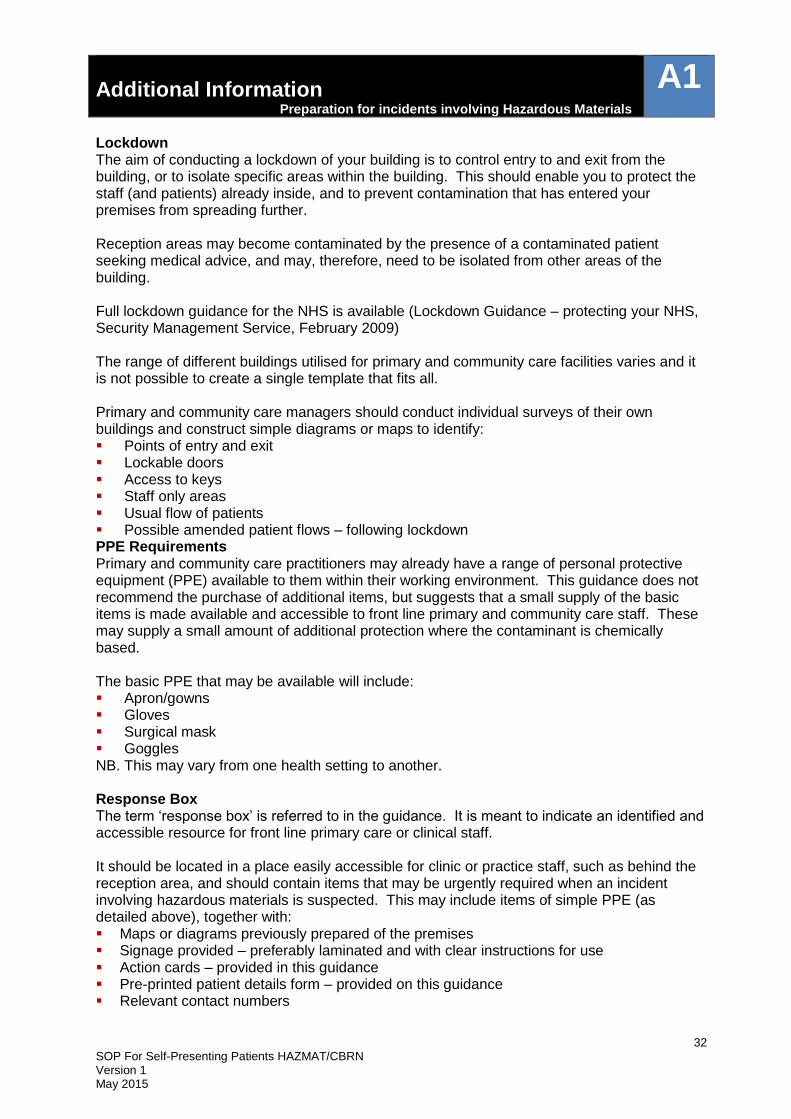
Additional Information Preparation for incidents involving Hazardous Materials
A1
Lockdown The aim of conducting a lockdown of your building is to control entry to and exit from the building, or to isolate specific areas within the building. This should enable you to protect the staff (and patients) already inside, and to prevent contamination that has entered your premises from spreading further. Reception areas may become contaminated by the presence of a contaminated patient seeking medical advice, and may, therefore, need to be isolated from other areas of the building. Full lockdown guidance for the NHS is available (Lockdown Guidance – protecting your NHS, Security Management Service, February 2009) The range of different buildings utilised for primary and community care facilities varies and it is not possible to create a single template that fits all. Primary and community care managers should conduct individual surveys of their own buildings and construct simple diagrams or maps to identify: Points of entry and exit Lockable doors Access to keys Staff only areas Usual flow of patients Possible amended patient flows – following lockdown PPE Requirements Primary and community care practitioners may already have a range of personal protective equipment (PPE) available to them within their working environment. This guidance does not recommend the purchase of additional items, but suggests that a small supply of the basic items is made available and accessible to front line primary and community care staff. These may supply a small amount of additional protection where the contaminant is chemically based. The basic PPE that may be available will include: Apron/gowns Gloves Surgical mask Goggles NB. This may vary from one health setting to another. Response Box The term ‘response box’ is referred to in the guidance. It is meant to indicate an identified and accessible resource for front line primary care or clinical staff. It should be located in a place easily accessible for clinic or practice staff, such as behind the reception area, and should contain items that may be urgently required when an incident involving hazardous materials is suspected. This may include items of simple PPE (as detailed above), together with: Maps or diagrams previously prepared of the premises Signage provided – preferably laminated and with clear instructions for use Action cards – provided in this guidance Pre-printed patient details form – provided on this guidance Relevant contact numbers

33 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
Preparation for incidents involving Hazardous Materials
A2
THIS FACILITY IS CLOSED
If you have been involved in an incident, or are worried that you might have been, please wait
outside for assistance.
If you have not been involved in an incident, please go to another
facility.
The nearest alternative facility is:
…………………………………………
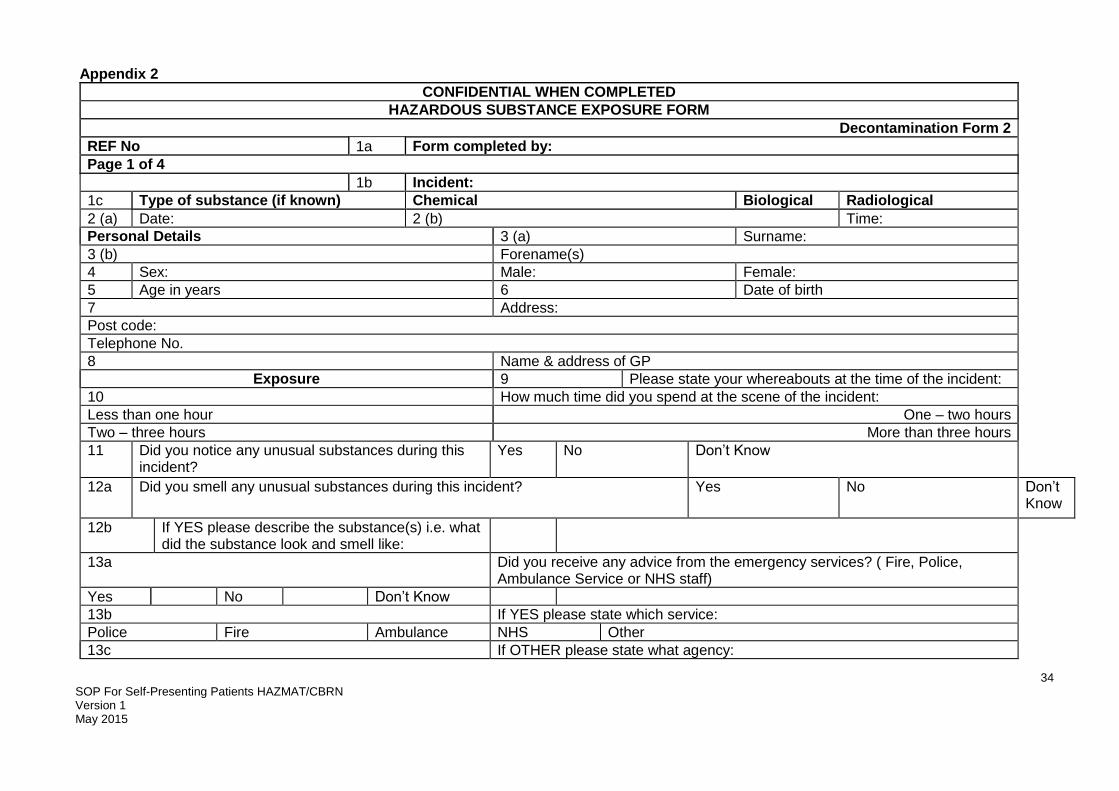
34 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
Appendix 2
CONFIDENTIAL WHEN COMPLETED
HAZARDOUS SUBSTANCE EXPOSURE FORM
Decontamination Form 2
REF No 1a Form completed by:
Page 1 of 4
1b Incident:
1c Type of substance (if known) Chemical Biological Radiological
2 (a) Date: 2 (b) Time:
Personal Details 3 (a) Surname:
3 (b) Forename(s)
4 Sex: Male: Female:
5 Age in years 6 Date of birth
7 Address:
Post code:
Telephone No.
8 Name & address of GP
Exposure 9 Please state your whereabouts at the time of the incident:
10 How much time did you spend at the scene of the incident:
Less than one hour One – two hours
Two – three hours More than three hours
11 Did you notice any unusual substances during this incident?
Yes
No Don’t Know
12a Did you smell any unusual substances during this incident? Yes No Don’t Know
12b If YES please describe the substance(s) i.e. what did the substance look and smell like:
13a Did you receive any advice from the emergency services? ( Fire, Police, Ambulance Service or NHS staff)
Yes No Don’t Know
13b If YES please state which service:
Police Fire Ambulance NHS Other
13c If OTHER please state what agency:

35 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
Appendix 3 - Equality Impact Assessment / Equality Analysis Screening Tool
Equality Impact Assessment (or ‘Equality Analysis’) is a process of systematically analysing a new or existing policy/practice or service to identify what impact or likely impact it will have on different groups within the community
Name of policy/service/project/plan:
Health and Safety Policy
Policy Number:
SH NCP 68
Department:
Health and Safety
Lead officer for assessment:
Dave White
Date Assessment Carried Out:
2015
1. Identify the aims of the policy and how it is implemented. Key questions Answers / Notes
Briefly describe purpose of the policy including
How the policy is delivered and by whom
Intended outcomes
The Health and Safety team have developed (SOP) Standard Operating Procedure for Self presenting patients from a possible HAZMAT/CBRN Incident and identifies arrangements for managing the safety, health and welfare of SHFT staff, clients, patients, visitors and anyone else who can be affected. It outlines the organisational structure and arrangements to ensure the Trust fulfils its legal responsibilities from NHS England Core standards Emergency planning and duty of care to protect people from hazards associated with incidents. The HAZMAT/CBRN SOP is an integral component of SHFT safety management systems.
2. Consideration of available data, research and information Monitoring data and other information involves using equality information, and the results of engagement with protected groups and others, to understand the actual effect or the potential effect of your functions, policies or decisions. It can help you to identify practical steps to tackle any negative effects or discrimination, to advance equality and to foster good relations. Please consider the availability of the following as potential sources:
Demographic data and other statistics, including census findings
Recent research findings (local and national)
Results from consultation or engagement you have undertaken
Service user monitoring data

36 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
Information from relevant groups or agencies, for example trade unions and voluntary/community organisations
Analysis of records of enquiries about your service, or complaints or compliments about them
Recommendations of external inspections or audit reports
Key questions
Data, research and information that you can refer to
2.1 What is the equalities profile of the team delivering the service/policy?
The Equality and Diversity team will report on Workforce data on an annual basis.
2.2 What equalities training have staff received? The Equality and Diversity team will report on Workforce data on an annual basis.
2.3 What is the equalities profile of service users?
The Trust Equality and Diversity team report on Trust patient equality data profiling on an annual basis
2.4 What other data do you have in terms of service users or staff? (e.g results of customer satisfaction surveys, consultation findings). Are there any gaps?
The Trust is preparing to implement the Equality Delivery System which will allow a robust examination of Trust performance on Equality, Diversity and Human Rights. This will be based on 4 key objectives that include:
1. Better health outcomes for all 2. Improved patient access and
experience 3. Empowered, engaged and
included staff 4. Inclusive leadership
2.5 What engagement or consultation has been undertaken as part of this EIA and with whom? What were the results?
2.6 If you are planning to undertake any consultation in the future regarding this service or policy, how will you include equalities considerations within this?

37 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
Positive impact (including examples of what the policy/service has done to promote equality)
Negative Impact Action Plan to address negative impact
Actions to overcome problem/barrier
Resources required Responsibility Target date
Age The Health and Safety steering group looks at matters/concerns raised from across all sectors of the organisation. These matters are followed up by the group and reported back to the group who meet regularly throughout the year. New/updated legislation is considered by the group and actioned accordingly giving consideration to the needs of not only staff, but any other user of the Trust buildings/premises
Applied to all protected characteristics: Support maybe required for staff who work lone working/night shifts. Risk assessments for Home visits must be undertaken if patients home has dangerous animals, for example Dogs.
Disability
The Trust will respond positively to requests of reasonable
There is a need to obtain more evidence of the
The Trust has adopted the Equality Delivery System
EDS/Workforce profile reports
Equality and Diversity Lead
January 2012-2016

38 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
adjustments. This includes: Interpreting and Translation provision, Hearing Loops and Personal Emergency Evacuation Plans (PEEP’s)
prevalence of different disabilities. This would enable the Trust to have more specific to understand and identify with employees with disabilities about resources that they require to function most effectively at the workplace (HSE)
(EDS) and has plans in place to improve workforce profile data across all protected characteristics The E&D Lead will work with the Health ans safety team to identify access audits that have been undertaken across Trust building/premises and address any gaps
Access Audits
Health and Safety
March 2013
Gender Reassignment
The Trust will ensure privacy, dignity and respect for Transgender people
Marriage and Civil Partnership
No adverse impacts have been identified at this stage of screening
Pregnancy and Maternity
New and expectant mothers will require risk assessments to determine if there are additional risks to the unborn child, and provisions will be made to accommodate the pregnant worker/new mother.
No adverse impacts have been identified at this stage of screening
Race The Trust will respond Staff may not Interpreting and Access to Health and Safety On-going

39 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
positively to reasonable adjustments. This includes providing information in alternative formats through Interpreting and Translation Equality and diversity implications are taken into account in relation to religion and belief when codes of practice and guidance notes are reviewed.
understand the Health and Safety policy if English is not their first language For example, Sikh head dress and the impact on wearing personal protection equipment (exempt for wearing a hard hat when wearing a turban)
Translation Advice will be sought from the E&D Lead and the Occupational Health Team if necessary
Communications
Officer Health & Safety Equality & Diversity
On-going
Religion or Belief
No adverse impacts have been identified at this stage of screening
Sex
No adverse impacts have been identified at this stage of screening
Sexual Orientation No adverse impacts have been identified at this stage of screening

40 SOP For Self-Presenting Patients HAZMAT/CBRN Version 1 May 2015
Sign Off and Publishing Once you have completed this form, it needs to be ‘approved’ by your Divisional Director or their nominated officer.
Name:
Designation:
Signature:
Date: