
FINAL Value Based Health Care analysis of joint ...
1
Why take on a Value Based Healthcare transformation approach? • Elective hip replacement surgery pathway for primary osteoarthritis is clearly defined across two sites, with pathway specific outcome measures. • The aim is to understand the value (how well this pathway is doing) across the complete pathway of care. • Patient reported outcomes measures (PROMS) mandated by the NHS (Oxford Hip Score, EQ-5D, EQ- VAS) were extracted with a focus on understanding, measuring and sharing outcomes that matter to patients and carers. Ethics approval to use patient data was attained. • The cost of a service user moving through the hip replacement pathway was calculated. This was used to develop clinically-meaningful cost information for delivering outcomes. This information will inform changes that can be made to the pathway to improve outcomes, efficiency, and ensure better value. Value Based Healthcare analysis of joint replacement surgery for primary hip osteoarthritis Dr Lucinda Gabriel 1 , Darzi Fellow, Mr Joseph Casey 1 , Deputy Director Programme Delivery, Ms Claire Palmer 2 , Head of Patient Outcomes, Mr Matt Gee 2, Orthopaedic Lead, Prof John Moxham 1 , Director Value Based Healthcare, Mr Joydeep Sinha 2 , Consultant Orthopaedic and Trauma Surgeon, Mr Toby Colgate-Stone 2 , Consultant Orthopaedic and Trauma Surgeon. 1 King’s Health Partners 2 King’s College Hospital. Correspondence: [email protected]. Calculating value: understanding outcomes that matter to patients and carers and clinically- meaningful cost information Results • Each pathway n=25; no significant difference between groups with regard to age, sex, number of comorbidities Conclusion Understanding the value of pathways of care, is inherently difficult. However accurate clinical costing is a patient-centred issue with the potential to change the way healthcare is incentivised and funded in order to make it sustainable, equitable and effective. Accurate data capture is critical to achieving VBHC which has become an organisational priority and pathways of care are being modified to fit the higher value IPU model more closely. Understand pathway of care by condition (rather than procedure) VALUE = OUTCOMES COSTS • 100% survival and no significant differences in PROMS, • Improvements in EQ-5D, EQ-VAS and OHS exceeded the national expected average • Improvements were also noted when outcomes were rearranged • Multiple quality reviews required to ensure costs were accurate however outliers persisted • Model 1 was leaner with lower costs and a higher margin. • Model 1 was the higher value pathway. Traditional PROMS vs patient-centred outcomes Discussion The higher value of pathway 1 likely arose from the standardised nature of the Integrated Practice Unit (IPU) model characterised by a single entry point. This hastens the patient journey reducing the ill effect of protracted waits associated with clinical deterioration. This would reduce length of stay and is likely to aid recovery. Better communication amongst the multi- disciplinary team is a further advantage expediting diagnostic decision making and treatment processes. These factors all contribute to a reduction in the costs incurred. Who are we? • King’s Health Partners is an Academic Health Sciences Centre (AHSCs) in South London. Based on breaking down barriers and increasing cooperation and focus, AHSCs seek to combine basic and translational health research, clinical care and education to create world-leading improvements in healthcare. We serve a population of eight million across South London and south east England. Our goal is to deliver transformational health improvements that are patient-centred, population-based and sustainable. • The Value Based Healthcare (VBHC) programme is focused on supporting our partner organisations to deliver excellent and consistent health outcomes whilst protecting our stretched NHS resources. • VBHC prioritises patient experience and improved health, teaches staff how to identify best value and empowers them to deliver the best possible care to their patients resulting in improved work satisfaction. • It also ensures that commissioners of care are getting the best results for the money available. Discomfort (q4, EQ5D) Usual pain (q1, OHS) Pain standing up (q8, OHS) Sudden severe pain (q10, OHS) Night pain (q12, OHS) Mobility (q1, EQ5D) Self-care (q2, EQ5D) Usual activities (q3, EQ5D) Trouble washing (q2, OHS) Trouble transport (q3, OHS) Trouble putting on socks (q4, OHS) Household shopping (q5, OHS) Walk before pain severe (q6, OHS) Climb flight of stairs (q7, OHS) Limping on walking (q9, OHS) Pain interfere with usual work (q11, OHS) Anxiety and depression (q5, EQ5D) Health Scale (EQVAS) - 15, 0 00 - 10, 0 00 - 5, 00 0 0 5, 000 10, 000 15, 000 20, 000 25, 000 £ Pathway total cost, total income to provider (i.e., tariff and) margin by patient for pathway (Model 1) Tot al cost Tot al i n come Margi n Excluded from analysis of cost information due to issues of data accuracy (n=4) - 15, 0 00 - 10, 0 00 - 5, 00 0 0 5, 000 10, 000 15, 000 20, 000 25, 000 £ Pathway total cost, total income to provider (i.e., tariff and) margin by patient for pathway (Model 2) Tot al cost Tot al i n come Margi n Excluded from analysis of cost information due to issues of data accuracty(n=11)
Transcript of FINAL Value Based Health Care analysis of joint ...
Why take on a Value Based Healthcare transformation approach?
• Elective hip replacement surgery pathway for primaryosteoarthritis is clearly defined across two sites, withpathway specific outcome measures.
• The aim is to understand the value (how well thispathway is doing) across the complete pathway of care.
• Patient reported outcomes measures (PROMS)mandated by the NHS (Oxford Hip Score, EQ-5D, EQ-VAS) were extracted with a focus on understanding,measuring and sharing outcomes that matter to patientsand carers. Ethics approval to use patient data was
attained.
• The cost of a service user moving through the hipreplacement pathway was calculated. This was used todevelop clinically-meaningful cost information fordelivering outcomes. This information will informchanges that can be made to the pathway to improveoutcomes, efficiency, and ensure better value.
Value Based Healthcare analysis of joint replacement surgery for primary hip osteoarthritisDr Lucinda Gabriel1, Darzi Fellow, Mr Joseph Casey1, Deputy Director Programme Delivery, Ms Claire Palmer2, Head of Patient Outcomes, Mr Matt Gee2, Orthopaedic Lead, Prof John Moxham1, Director Value Based Healthcare, Mr Joydeep Sinha2, Consultant Orthopaedic and Trauma Surgeon, Mr Toby Colgate-Stone2, Consultant Orthopaedic and Trauma Surgeon. 1King’s Health Partners 2King’s College Hospital. Correspondence: [email protected].
Calculating value: understanding outcomes that matter to patients and carers and clinically-meaningful cost information
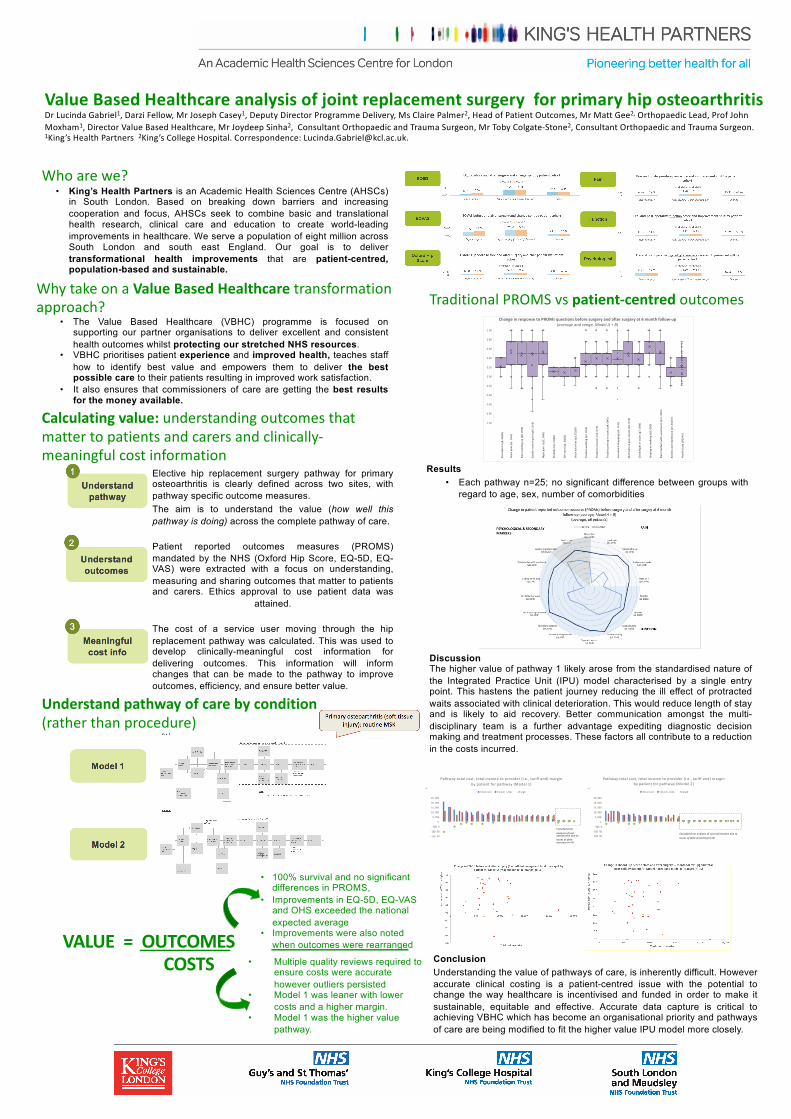
Results• Each pathway n=25; no significant difference between groups with
regard to age, sex, number of comorbidities
ConclusionUnderstanding the value of pathways of care, is inherently difficult. Howeveraccurate clinical costing is a patient-centred issue with the potential tochange the way healthcare is incentivised and funded in order to make itsustainable, equitable and effective. Accurate data capture is critical toachieving VBHC which has become an organisational priority and pathwaysof care are being modified to fit the higher value IPU model more closely.
Understand pathway of care by condition (rather than procedure)
VALUE = OUTCOMESCOSTS
• 100% survival and no significant differences in PROMS,
• Improvements in EQ-5D, EQ-VAS and OHS exceeded the national expected average
• Improvements were also noted when outcomes were rearranged
• Multiple quality reviews required to ensure costs were accurate however outliers persisted
• Model 1 was leaner with lower costs and a higher margin.
• Model 1 was the higher value pathway.
Traditional PROMS vs patient-centred outcomes
DiscussionThe higher value of pathway 1 likely arose from the standardised nature ofthe Integrated Practice Unit (IPU) model characterised by a single entrypoint. This hastens the patient journey reducing the ill effect of protractedwaits associated with clinical deterioration. This would reduce length of stayand is likely to aid recovery. Better communication amongst the multi-disciplinary team is a further advantage expediting diagnostic decisionmaking and treatment processes. These factors all contribute to a reductionin the costs incurred.
Who are we?• King’s Health Partners is an Academic Health Sciences Centre (AHSCs)
in South London. Based on breaking down barriers and increasingcooperation and focus, AHSCs seek to combine basic and translationalhealth research, clinical care and education to create world-leadingimprovements in healthcare. We serve a population of eight million acrossSouth London and south east England. Our goal is to delivertransformational health improvements that are patient-centred,population-based and sustainable.
• The Value Based Healthcare (VBHC) programme is focused onsupporting our partner organisations to deliver excellent and consistenthealth outcomes whilst protecting our stretched NHS resources.
• VBHC prioritises patient experience and improved health, teaches staffhow to identify best value and empowers them to deliver the bestpossible care to their patients resulting in improved work satisfaction.
• It also ensures that commissioners of care are getting the best resultsfor the money available.
-1.00
-0.80
-0.60
-0.40
-0.20
0.00
0.20
0.40
0.60
0.80
1.00
Change in response to PROMs questions before surgery and after surgery at 6 month follow-up (average and range, Model A + B)
Dis
com
fort
(q4,
EQ
5D)
Usu
al p
ain
(q1,
OH
S)
Pain
sta
ndin
g up
(q8,
OH
S)
Sudd
en s
ever
e pa
in (q
10, O
HS)
Nig
ht p
ain
(q12
, OH
S)
Mob
ility
(q1,
EQ
5D)
Self
-car
e (q
2, E
Q5D
)
Usu
al a
ctiv
ities
(q3,
EQ
5D)
Trou
ble
was
hing
(q2,
OH
S)
Trou
ble
tran
spor
t (q3
, OH
S)
Trou
ble
putt
ing
on s
ocks
(q4,
OH
S)
Hou
seho
ld s
hopp
ing
(q5,
OH
S)
Wal
k be
fore
pai
n se
vere
(q6,
OH
S)
Clim
b fli
ght o
f sta
irs
(q7,
OH
S)
Lim
ping
on
wal
king
(q9,
OH
S)
Pain
inte
rfer
e w
ith u
sual
wor
k (q
11, O
HS)
Anx
iety
and
dep
ress
ion
(q5,
EQ
5D)
Hea
lth S
cale
(EQ
VAS)
- 15,0 00
- 10,0 00
- 5,00 0
0
5, 000
10, 000
15, 000
20, 000
25, 000
£
Pathway total cost, total income to provider (i.e., tariff and) margin by patient for pathway (Model 1)
Tot al cost Tot al in come M ar gin
Excluded from analysis of cost information due to issues of data accuracy (n=4)
- 15,0 00
- 10,0 00
- 5,00 0
0
5, 000
10, 000
15, 000
20, 000
25, 000
£
Pathway total cost, total income to provider (i.e., tariff and) margin by patient for pathway (Model 2)
Tot al cost Tot al in come M ar gin
Excluded from analysis of cost information due to issues of data accuracty(n=11)


















