February 18, 2003: I. Sim Overview Medical Informatics Ida Sim, MD, PhD February 18, 2003 Division...
63
February 18, 2003: I. Sim Overview Medical Informatics Medical Informatics Ida Sim, MD, PhD February 18, 2003 Division of General Internal Medicine, and Graduate Group in Biological and Medical Informatics UCSF Copyright Ida Sim, 2003. All federal and state rights reserved for all original material presented in this course through any medium, including lecture or print.
-
date post
22-Dec-2015 -
Category
Documents
-
view
213 -
download
0
Transcript of February 18, 2003: I. Sim Overview Medical Informatics Ida Sim, MD, PhD February 18, 2003 Division...
February 18, 2003: I. Sim OverviewMedical Informatics
Medical Informatics
Ida Sim, MD, PhD
February 18, 2003
Division of General Internal Medicine, andGraduate Group in Biological and Medical Informatics
UCSF
Copyright Ida Sim, 2003. All federal and state rights reserved for all original material presented in this course through any medium, including lecture or print.

February 18, 2003: I. Sim OverviewMedical Informatics
Outline
• Introduction
• Course Goals and Overview
• Computing Infrastructure for Health Care– data storage– networking

February 18, 2003: I. Sim OverviewMedical Informatics
Introduction: Ida Sim, MD, PhD• PhD in Medical Informatics, Stanford• Assistant Professor
– General Internal Medicine
• Associate Director for Medical Informatics– Program in Biological and Medical Informatics
• Interests– computer-assisted clinical decision-making– electronic scientific publication– economics of health information technology– meta-analysis, and evidence-based decision making

February 18, 2003: I. Sim OverviewMedical Informatics
Informatics and Clinical Care• Institute of Medicine (IOM) report on med errors
– calls for electronic prescribing– Leapfrog initiative: financial rewards for hospitals
that use e-prescribing
• IOM report on “quality chasm”– “A nationwide effort is needed to build a technology-
based information infrastructure that would lead to the elimination of most handwritten clinical data within the next 10 years…”; asks for $1 billion for health informatics
• Rise of consumer health informatics– consumer may be next “driver” for health care
February 18, 2003: I. Sim OverviewMedical Informatics
Informatics and Clinical Research• Human genome findings will need to be
translated into population and clinical medicine• RCTs now a $3.6 billion business (C. Scott, 7/00)
– in 1988, 95% of RCTs conducted by academics– now, over 80% conducted by industry– industry is seeking increased efficiency in a very
fragmented and complex business• Computers needed to help translate research
results to practice– over 10,000 RCTs indexed in 1999 Medline

February 18, 2003: I. Sim OverviewMedical Informatics
Yet...• Only ~12% of outpatient clinics have an EMR;
only 30% of hospitals have a website• Much clinical research is still done using chart
abstraction and paper forms• Medicine and medical research is information
intensive, but– health sector invests only 2.5% of gross
revenue on information technologies (Gartner Group, 2003)
– vs. 6% in comparable information-intensive sectors (e.g., banking)

February 18, 2003: I. Sim OverviewMedical Informatics
Course Goals (1)• Understand the clinical, economic, and social
context in which information technologies are being developed and deployed in health care
• Be familiar with core concepts in medical informatics: vocabularies, interchange standards, decision support systems
• Understand key concepts about electronic medical records (EMRs) and data warehouses, and their uses for clinical research
February 18, 2003: I. Sim OverviewMedical Informatics
Course Goals (2)
• Be familiar with – trends in consumer health informatics– organizational aspects of successfully using
health information technology– intellectual property and electronic privacy
issues
• Have an overview of the research, funding, and training opportunities in medical informatics

February 18, 2003: I. Sim OverviewMedical Informatics
Context
• Few students working directly in informatics
• Desired outcome– that you be able to understand and converse
with “tech” folks– that you have a better chance of recognizing
and taking advantage of opportunities in • using informatics for your research work
• participating in innovative informatics projects
February 18, 2003: I. Sim OverviewMedical Informatics
Course Overview• 5 Lectures
– PowerPoint file up few days before lecture– class participation expected
• Field trip: Palo Alto Medical Foundation– Tues. Mar. 11, 1:00 to 3:00 pm
• Assignments– 4 homeworks, no final exam
• Office “hours”: [email protected]– http://www.epibiostat.ucsf.edu/courses/schedule/med_informatics.html
February 18, 2003: I. Sim OverviewMedical Informatics
Outline
• Introduction
• Course Goals and Overview
• Computing Infrastructure for Health Care– data storage– networking

Computing Infrastructure
Clinic 2003
FrontDesk
Radiology
Claims
MedicalInformation
Bureau
Archive
Walgreens
Prescribing
Pharm BenefitManager
Benefits Check
HealthNetFormulary Check
Lab
UniLab
B&TEligibility Authorization
Personal HealthRecord
LogicianEMR
OutsourcedElectronic Medical
Record
Specialist
Referral
ReferralAuthorization
Internet Intranet Phone/Paper

February 18, 2003: I. Sim OverviewMedical Informatics
Understanding the Infrastructure
• Clients and servers (the components)
• Data storage (how data is stored)– flat file versus relational model
• Networking (how data gets back and forth)

February 18, 2003: I. Sim OverviewMedical Informatics
Client/Server Model
• Computers can be servers and/or clients
• Web server “serves” web pages to “clients,” who view these pages using a browser – MS Internet Explorer or Netscape Communicator
Clients
WebServer
February 18, 2003: I. Sim OverviewMedical Informatics
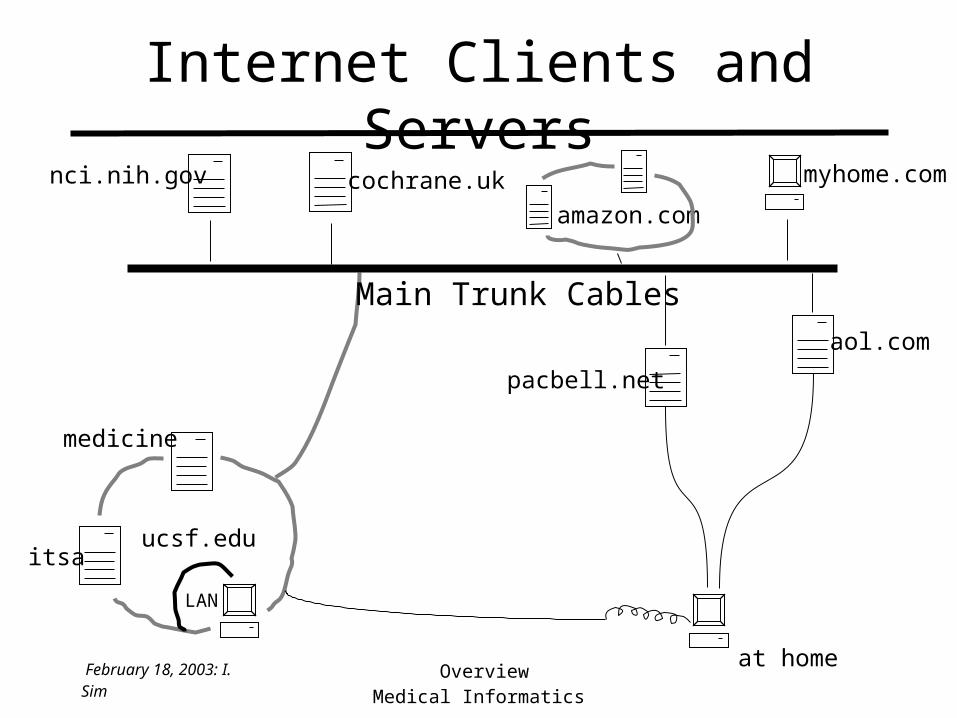
Internet Clients and Servers
itsa
medicine
ucsf.edu
nci.nih.gov cochrane.uk myhome.com
Main Trunk Cables
amazon.com
at home
pacbell.net
aol.com
LAN
February 18, 2003: I. Sim OverviewMedical Informatics
Data Storage
• Computers can help us– store, retrieve, query, compute, and report data
• For this to happen, we must describe the data in such a way that the computer– “understands” the data– can manipulate the data
• e.g., sort them, graph them, add numbers, perform analyses
– can retrieve the data for later use
February 18, 2003: I. Sim OverviewMedical Informatics
“Describing” the Data
• The extent to which the computer can help you manage your data depends on how well you described your data to it
• In JIFE database example, did you describe your data– correctly: did Baby Oscar have jaundice?
• accurate, clear, consistent, etc.– cleanly: with as little redundancy as possible
• don’t want Baby Oscar’s birthdate in 3 separate places– sufficiently: all that is needed for later analyses
• captured ethnicity for anticipated analysis by ethnicity?• what later analyses do you have in mind?
– understandably: for humans and for computers

February 18, 2003: I. Sim OverviewMedical Informatics
“Describing” Data: To Humans
• For understanding and communication– via a system for codifying meaning
• English language, mathematical notation,– making the “code” itself concrete
• skywriting, a graph drawn on a sandy beach
• text on paper, an oil painting, lecture on audiotape
• For later retrieval– a permanent or semi-permanent physical
embodiment of the description• papers in a file cabinet, museum of runes
24142 1083.9 96
February 18, 2003: I. Sim OverviewMedical Informatics
“Describing” Data: To Computers• For understanding and communication
– via a data model for describing data to computers• akin to “German prose on paper” or “Olde English
epic poetry on audiotape”– standard data models to choose from include
• flat file• relational• object-oriented
• For later retrieval– storage as 1’s and 0’s in
• random access memory: short term, until power off• permanent memory on a hard disk: longer term

February 18, 2003: I. Sim OverviewMedical Informatics
Data Model Choices• Data model should best allow you to
– do what you want to do with the data• query, manipulate, share, merge
– handle the amount of data that you have– handle the type of data that you have
• prose, numbers, xray images, audio files, etc.
• Standard data model choices– flat file: one long list of ASCII entries– relational: tables of columns and rows– object: data arranged in conceptual groups
• Usual clinical research choice is flat file/relational• Clinical databases are increasingly becoming
relational

February 18, 2003: I. Sim OverviewMedical Informatics
What is ASCII?
• Standard system for coding characters (A-Z, a-z, 1-0, etc.) in machine language– American Standard Code for Information
Interchange. – used in almost all present-day computers
• Since it encodes single characters one at a time, ASCII does not support any coding of word meaning

February 18, 2003: I. Sim OverviewMedical Informatics
Flat File Model• For understanding and communication
– data are encoded as ASCII
– BUT computers cannot understand the meaning of the ASCII text and numbers
• For storage– in a single file (e.g. a Word or STATA file)– “flat” structure: start with one baby’s data, and
keep adding data baby by baby
• Like writing all your data from beginning to end onto one piece of paper and putting that paper into your file drawer

February 18, 2003: I. Sim OverviewMedical Informatics
Word Text File
Carson Jackson 1 3/2/05 J 5
Hannah Hillary 2 1/2/05 C 2
Jonas Oscar 1 1/1/05 J 3
STATA File
Carson,Jackson,1,3/2/05,J,5
Hannah,Hillary,2,1/2/05,C,2
Jonas,Oscar,1,1/1/05,J,3
Flat File Examples

February 18, 2003: I. Sim OverviewMedical Informatics
Database Schema
• A database’s schema is a compact summary description your database’s contents
• Database schema = description of database– what type of data– how that data is conceptually arranged
• E.g., schema for research paper– intro, methods, results, discussion (text)– tables (table) and figures (graphic)– pictures (image)

February 18, 2003: I. Sim OverviewMedical Informatics
Flat File Data SchemaWord File
Carson Jackson 1 3/2/05 J 5
Hannah Hillary 2 1/2/05 C 2
Jonas Oscar 1 1/1/05 J 3
• Which fields are– first name, DOB, case status, last name, exam score, gender
• Flat file schemas are implicit– is in the mind of whoever is entering the data– can change from record to record
• maybe first baby’s name is Jackson Carson and the second baby’s name is Hannah Hillary

February 18, 2003: I. Sim OverviewMedical Informatics
Flat File Advantages
• Easy, just start entering data, doesn’t need any preliminary database work or knowledge
• Can do with any word processor– Word, WordPerfect, editor for STATA or SAS,
Excel, SimpleText
• Cheap
• Can be exported to analysis programs
• Portable– almost all programs can read in an ASCII file

February 18, 2003: I. Sim OverviewMedical Informatics
Flat File Disadvantages• Description of the data isn’t clear, and may not
even be understandable– meaning of the data items is not explicit
• unclear that the last column is the neuropsych exam score
– structure is not explicit• does last name always precede first name?
• Inefficient and prone to error for representing repeating data fields– e.g., if each baby has more than one neuropsych
exam score

February 18, 2003: I. Sim OverviewMedical Informatics
Repeating Data in Flat File Model (1)
Word Text FileCarson Jackson 1 3/2/05 J 5
Hannah Hillary 2 1/2/05 C 2
Jonas Oscar 1 1/1/05 J 3
Carson Jackson 2 3/3/05 J 4
Jonas Oscar 1 1/3/05 J 4
Jonas Oscar 1 1/1/05 J 3
• Jackson/Carson’s gender might change from one record to another, or...

February 18, 2003: I. Sim OverviewMedical Informatics
Word Text FileCarson Jackson 1 3/2/05 J 5 x
4
Hannah Hillary 2 1/2/05 C 2
Jonas Oscar 1 1/1/05 J 3 43• Implicit structure to repeating data
– is the nth column always the nth neuropsych exam score?
• can a missed exam be denoted by an X?
• Whatever data schema there is, may vary from record to record
Repeating Data in Flat File Model (2)

February 18, 2003: I. Sim OverviewMedical Informatics
Flat File Disadvantages (cont.)• Inefficient at finding a particular baby
– must look at records one by one from beginning to end
– no guarantee that you have found all the information for that baby unless you look all the way to the end
• Inefficient at manipulating data– to see list of male babies, must make a new file
• Difficult to share since the database itself gives no clues about what data is in each field

February 18, 2003: I. Sim OverviewMedical Informatics
Summary of Flat File Data Model
Factor Flat File Relational ObjectHuman-understandable
Frequently Not
Computer-“understandable”
No
Complexity of data SimpleQuerying InefficientManipulating InefficientAmount of data SmallType of data Text, NumbersSharing and merging Very Difficult
February 18, 2003: I. Sim OverviewMedical Informatics
When Are Flat Files Useful?• For a small, simple, “quick and dirty” databases
– few data items, small number of records– one set of predictors and one set of outcomes per
participant/subject• i.e., no repeating data fields• i.e., only one-to-one relations, no one-to-many
– quick and dirty• for very few users (i.e. just you) • you’re not planning on reusing this database later• you’re not planning on sharing this database now or
later

February 18, 2003: I. Sim OverviewMedical Informatics
Flat Files in Clinical Care• Really no reason nowadays to build a flat file
system for clinical care databases– lots of one-to-many relationships
• Many flat file systems are leftover from early days of computerization– old VA system in Mumps (ANSI Standard M)– STOR, a pioneering system in the 1970s
• “STOR does not store data in a relational database - it is a flat file data structure. To obtain it's data, I run queries off it and download them into FileMaker Pro or Microsoft Access or Excel and then manipulate the data into a form more easy to read for providers.” Tirzah Gonzalez, DGIM STOR analyst

February 18, 2003: I. Sim OverviewMedical Informatics
Relational Data Model• Data are arranged in tables made up of
columns and rows– the columns are the types of data
• fixed number of columns• each column has a unique name (e.g., FirstName)• has a “domain” of values that may appear in that
column– domain=text for FirstName, domain=positive integers for
age
– the rows are the records themselves• there can be an arbitrary number of unique unnamed
rows (i.e., the table can be arbitrarily long)

February 18, 2003: I. Sim OverviewMedical Informatics
Flat File Admissions DatabaseRobert Lee, 000-01-001, M, 09-Jul-70,B/T Healthnet
31-Dec-94 to 12-Jan-95, admitted to Medicine with Acute MI, discharged with Acute MI, COPD, Diabetes, CHF
27-Mar-96 to 31-Mar-96, admitted to Medicine with COPD, discharged with Pneumonia, COPD, CHF, Diabetes
June Smith, 000-01-002,F,22-Oct-25,Medicare02-Feb-95 to 16-Feb-95, admitted to Surgery for Total Hip Replacement,
discharged with THR, Acute MI, Diabetes
27-Feb-95 to 20-Mar-95, admitted to Medicine with Acute MI, discharged with Acute MI,VF Arrest, Diabetes
Marissa Perez,000-01-003,F,13-Jun-57,B/T Pacificare
19-Nov-97 to 23-Nov-97, admitted to Gyn for metrorrhagia, discharged with uterine fibroids, Diabetes

February 18, 2003: I. Sim OverviewMedical Informatics
Review of Problems with Flat Files
• Implicit structure, implicit data schema
• Schema may change from record to record
• Inefficient for finding a particular admission
• Inefficient for pulling out all Acute MI admissions
• Difficult to share or to understand later
• etc.

February 18, 2003: I. Sim OverviewMedical Informatics
InpatientMasterTableID Name Sex Birthdate Insurance
000-01-001 Lee M 09-Jul-70 B/T Healthnet000-01-002 Smith F 22-Oct-25 Medicare000-01-003 Perez F 13-Jun-57 B/T Pacificare
AdmissionsTableID Admit
ServiceAdmit Date Discharge
DateAdmit
DiagnosisPrincipalDischargeDiagnosis
SecondaryDischargeDiagnoses
SecondaryDischargeDiagnoses
000-01-001 Med 31-Dec-94 12-Jan-95 Acute MI Acute MI COPD Diabetes (CHF)000-01-001 Med 27-Mar-96 31-Mar-96 COPD Pneumonia COPD CHF (Diabetes)000-01-002 Surg 03-Feb-95 16-Feb-95 THR THR Acute MI Diabetes000-01-002 Med 27-Feb-95 20-Mar-95 Acute MI Acute MI VF Arrest Diabetes000-01-003 Gyn 19-Nov-97 23-Nov-97 Menorrhagia von Willebrand's Diabetes
• Doesn’t handle secondary diagnoses very well– for many admissions, there are either too few or
too many columns
Relational Admissions Database (#1)
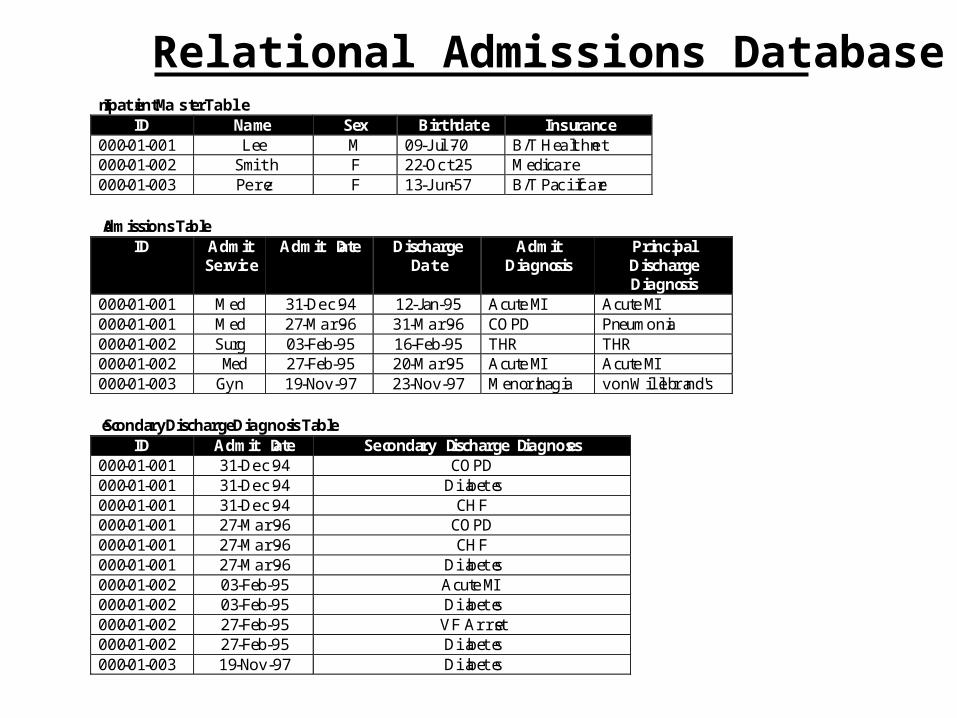
Relational Admissions Database InpatientMasterTable
ID Name Sex Birthdate Insurance000-01-001 Lee M 09-Jul-70 B/T Healthnet000-01-002 Smith F 22-Oct-25 Medicare000-01-003 Perez F 13-Jun-57 B/T Pacificare
AdmissionsTableID Admit
ServiceAdmit Date Discharge
DateAdmit
DiagnosisPrincipalDischargeDiagnosis
000-01-001 Med 31-Dec-94 12-Jan-95 Acute MI Acute MI000-01-001 Med 27-Mar-96 31-Mar-96 COPD Pneumonia000-01-002 Surg 03-Feb-95 16-Feb-95 THR THR000-01-002 Med 27-Feb-95 20-Mar-95 Acute MI Acute MI000-01-003 Gyn 19-Nov-97 23-Nov-97 Menorrhagia von Willebrand's
SecondaryDischargeDiagnosisTableID Admit Date Secondary Discharge Diagnoses
000-01-001 31-Dec-94 COPD000-01-001 31-Dec-94 Diabetes000-01-001 31-Dec-94 CHF000-01-001 27-Mar-96 COPD000-01-001 27-Mar-96 CHF000-01-001 27-Mar-96 Diabetes000-01-002 03-Feb-95 Acute MI000-01-002 03-Feb-95 Diabetes000-01-002 27-Feb-95 VF Arrest000-01-002 27-Feb-95 Diabetes000-01-003 19-Nov-97 Diabetes
February 18, 2003: I. Sim OverviewMedical Informatics
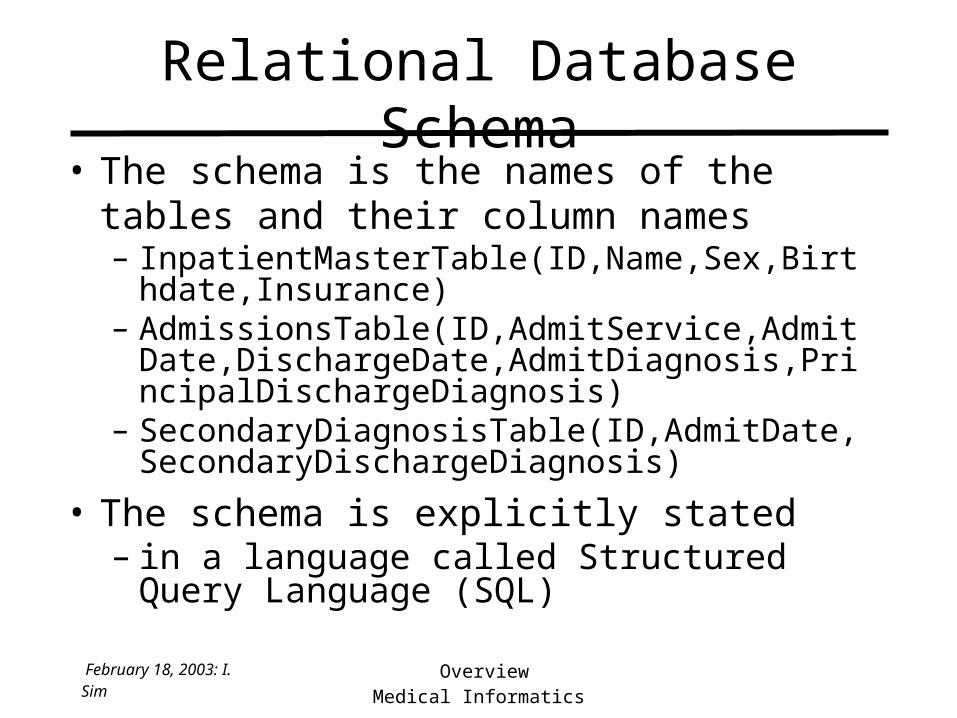
Relational Database Schema• The schema is the names of the tables and their
column names– InpatientMasterTable(ID,Name,Sex,Birthdate,Insuran
ce)– AdmissionsTable(ID,AdmitService,AdmitDate,Disch
argeDate,AdmitDiagnosis,PrincipalDischargeDiagnosis)
– SecondaryDiagnosisTable(ID,AdmitDate,SecondaryDischargeDiagnosis)
• The schema is explicitly stated– in a language called Structured Query Language
(SQL)
February 18, 2003: I. Sim OverviewMedical Informatics
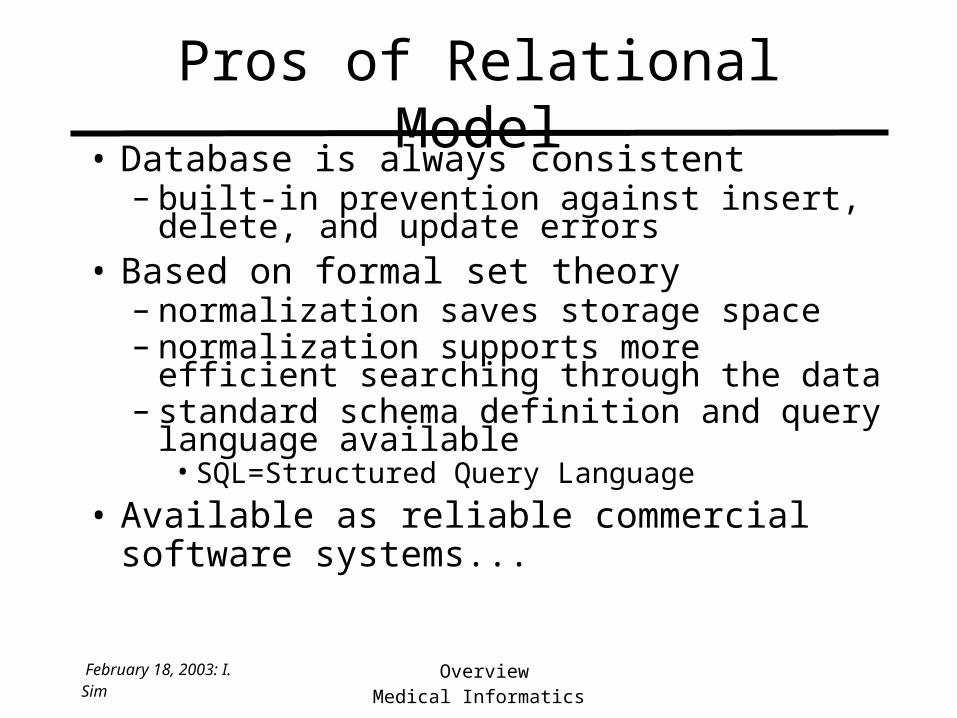
Pros of Relational Model• Database is always consistent
– built-in prevention against insert, delete, and update errors
• Based on formal set theory– normalization saves storage space– normalization supports more efficient searching
through the data– standard schema definition and query language
available • SQL=Structured Query Language
• Available as reliable commercial software systems...
February 18, 2003: I. Sim OverviewMedical Informatics
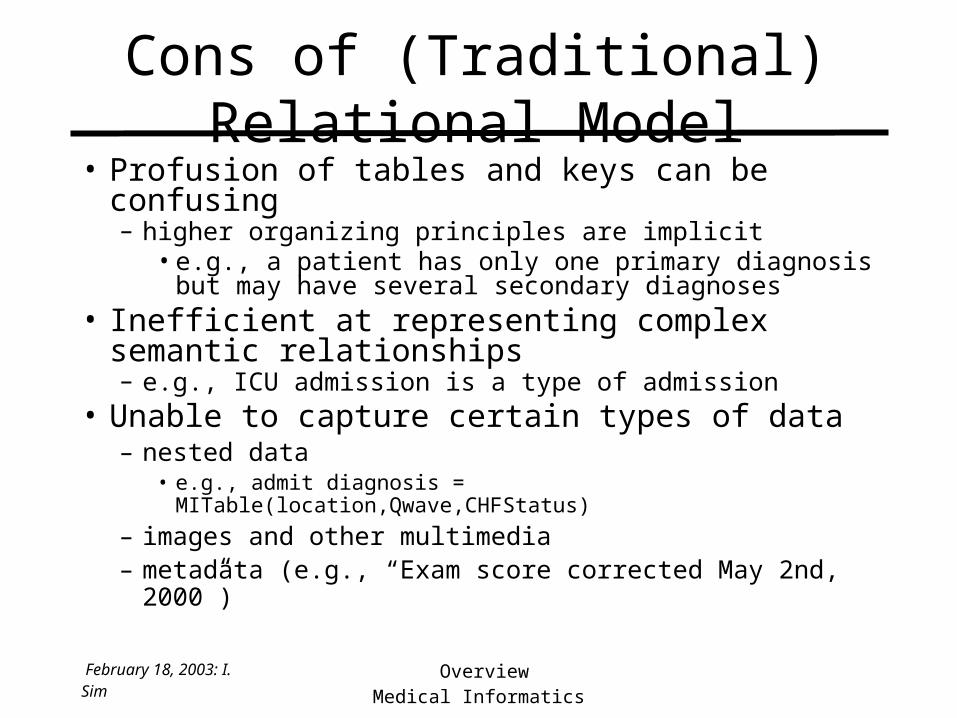
Cons of (Traditional) Relational Model• Profusion of tables and keys can be confusing
– higher organizing principles are implicit • e.g., a patient has only one primary diagnosis but
may have several secondary diagnoses• Inefficient at representing complex semantic
relationships– e.g., ICU admission is a type of admission
• Unable to capture certain types of data– nested data
• e.g., admit diagnosis = MITable(location,Qwave,CHFStatus)
– images and other multimedia– metadata (e.g., “Exam score corrected May 2nd, 2000”)
February 18, 2003: I. Sim OverviewMedical Informatics
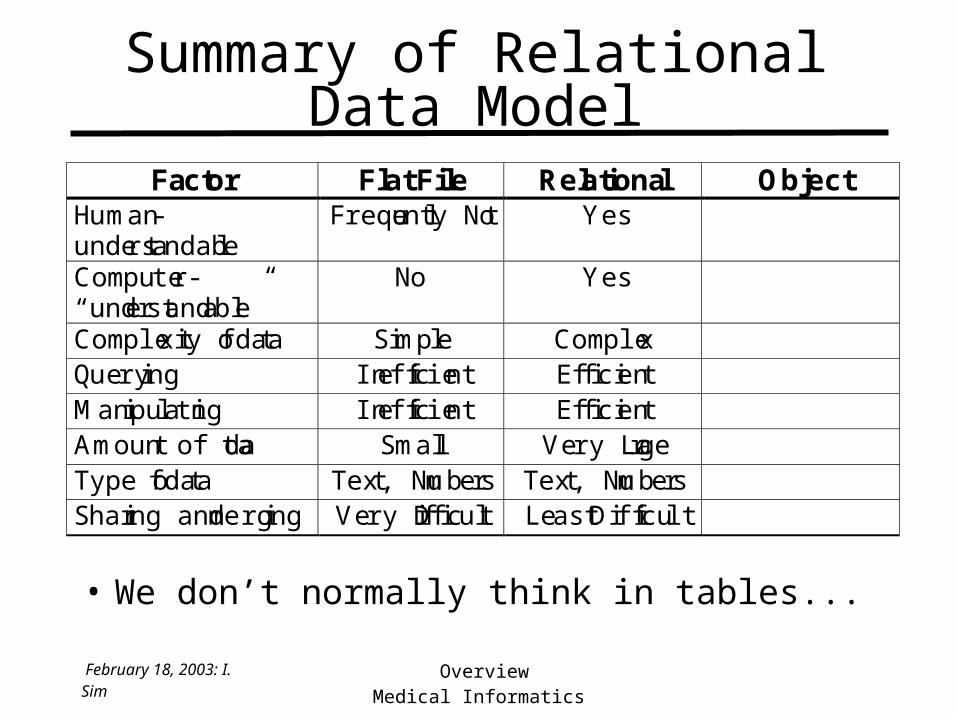
Summary of Relational Data Model
Factor Flat File Relational ObjectHuman-understandable
Frequently Not Yes
Computer-“understandable”
No Yes
Complexity of data Simple ComplexQuerying Inefficient EfficientManipulating Inefficient EfficientAmount of data Small Very LargeType of data Text, Numbers Text, NumbersSharing and merging Very Difficult Least Difficult
• We don’t normally think in tables...

February 18, 2003: I. Sim OverviewMedical Informatics
Object Data Model
• Data arranged in conceptual groups, with prototypes and their attributes
Patient
-name-gender-b-day-address-insurance-primary MD-etc
Admission
-admit date-discharge date-attending MD-admit, primary, secondary dx-etc.
Diagnosis
-code-name-modifiers
February 18, 2003: I. Sim OverviewMedical Informatics
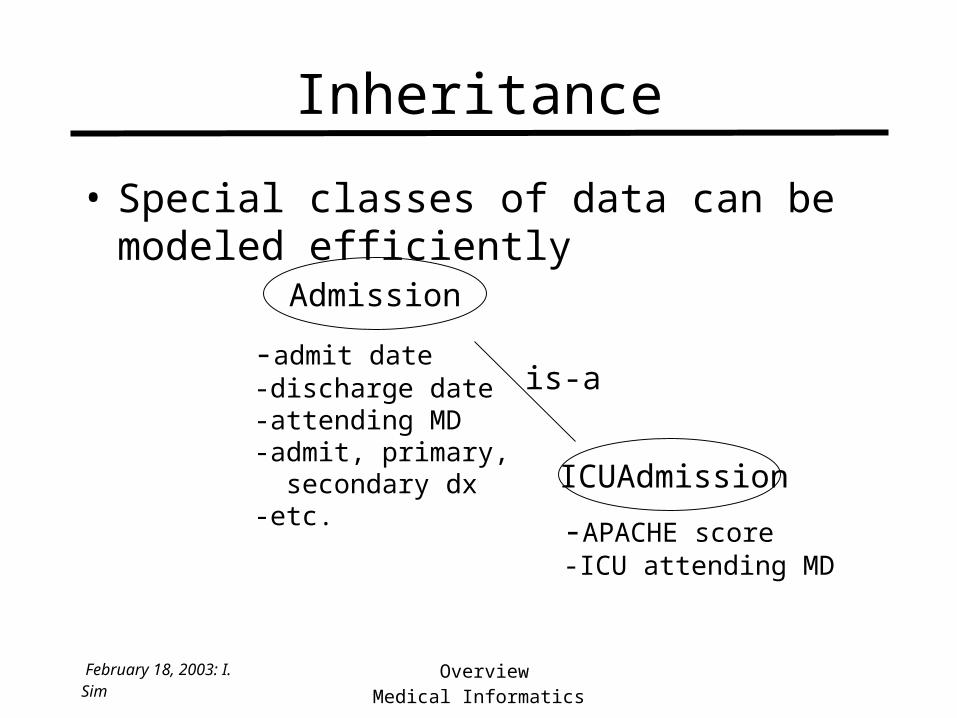
Inheritance
• Special classes of data can be modeled efficiently
Admission
-admit date-discharge date-attending MD-admit, primary, secondary dx-etc.
ICUAdmission
-APACHE score-ICU attending MD
is-a

February 18, 2003: I. Sim OverviewMedical Informatics
Pros and Cons of Object Model• Pros: Can represent very complex data
types and data relationships– images, audio, inheritance, procedural
data (e.g., how to draw a graph of given data)
• Cons: Very complex– inefficient since no formal mathematical
basis for storage and querying– more difficult to share since data is more
complex– commercial systems are flaky

February 18, 2003: I. Sim OverviewMedical Informatics
Summary of Data Models
Factor Flat File Relational ObjectHuman-understandable
Frequently Not Yes Partially
Computer-“understandable”
No Yes Yes
Complexity of data Simple Complex Very ComplexQuerying Inefficient Efficient InefficientManipulating Inefficient Efficient InefficientAmount of data Small Very Large LargeType of data Text, Numbers Text, Numbers AllSharing and merging Very Difficult Least Difficult Rather Difficult
February 18, 2003: I. Sim OverviewMedical Informatics
Summary of Data Model Choices• Generally, use the RELATIONAL MODEL for storing
clinical and clinical research data• Exceptions
– you have only one-to-one relations in your database, which you are not intending on sharing or reusing
• use a flat file (e.g., Excel, STATA)– you need to store complex, multimedia data
• consider an extended-relational database (aka object-relational)– database designed using the object model– data is stored and queried as a relational database
• but could probably work around this using a standard relational database

February 18, 2003: I. Sim OverviewMedical Informatics
The Model vs. The System• Data model
– the generic abstract structure of the information• domain independent, not a “product” per se
• Database management system– is a real-world program that you can buy
– stores information using a data model – provides additional functionality
Example Database Management SystemsData Model Small Scale (PC’s) Large Scale (Mainframes)
Flat file Filemaker Pro VA system (enhanced)
Relational Access, MySQL Oracle, Sybase, MySQL,SQL Server
Object Informix Objectivity

February 18, 2003: I. Sim OverviewMedical Informatics
DBMS Features for System Selection
• Memory capacity
• Multi-user support and transaction management
• Data entry forms
• Triggers and rules
• Security
• Backup and archiving

February 18, 2003: I. Sim OverviewMedical Informatics
Other DBMS Features
• Security– can have logins and different levels of access
• only database administrator can change data schema• data entry person can only enter data into certain fields
• Backup and archiving– safer if this is automatically done on a regular schedule– standard for health care data is at least 7 years of
archiving

Computing Infrastructure
Modern U.
FrontDesk
Radiology
Claims
MedicalInformation
Bureau
Archive
Walgreens
Prescribing
Pharm BenefitManager
Benefits Check
HealthNetFormulary Check
Lab
UniLab
B&TEligibility Authorization
Personal HealthRecord
LogicianEMR
OutsourcedElectronic Medical
Record
Specialist
Referral
ReferralAuthorization
Internet Intranet Phone/Paper

February 18, 2003: I. Sim OverviewMedical Informatics
HealthSystem Minnesota
• 1.6 million patient visits per year, 270,000 capitated lives, 460 physicians, 4700 employees, 31 clinics, and over $400 million in revenues (1998)
– over 50 computer and 50 paper systems
• “Maintaining the consistency of these tables in various systems is impossible and creates enormous problems for understanding let alone improving our performance.”
February 18, 2003: I. Sim OverviewMedical Informatics
Summary on Data Storage• How a computer stores information can have
serious implications for– data integrity– speed– ability to share data– security (via enhancements available to relational
database management systems)
• Relational model is generally the best choice for storing clinical data– but making sense of multiple databases is still
non-trivial

February 18, 2003: I. Sim OverviewMedical Informatics
Understanding the Infrastructure
• Clients and servers (the components)
• Data storage (how data is stored)– flat file versus relational model
• Networking (how data gets back and forth)
February 18, 2003: I. Sim OverviewMedical Informatics
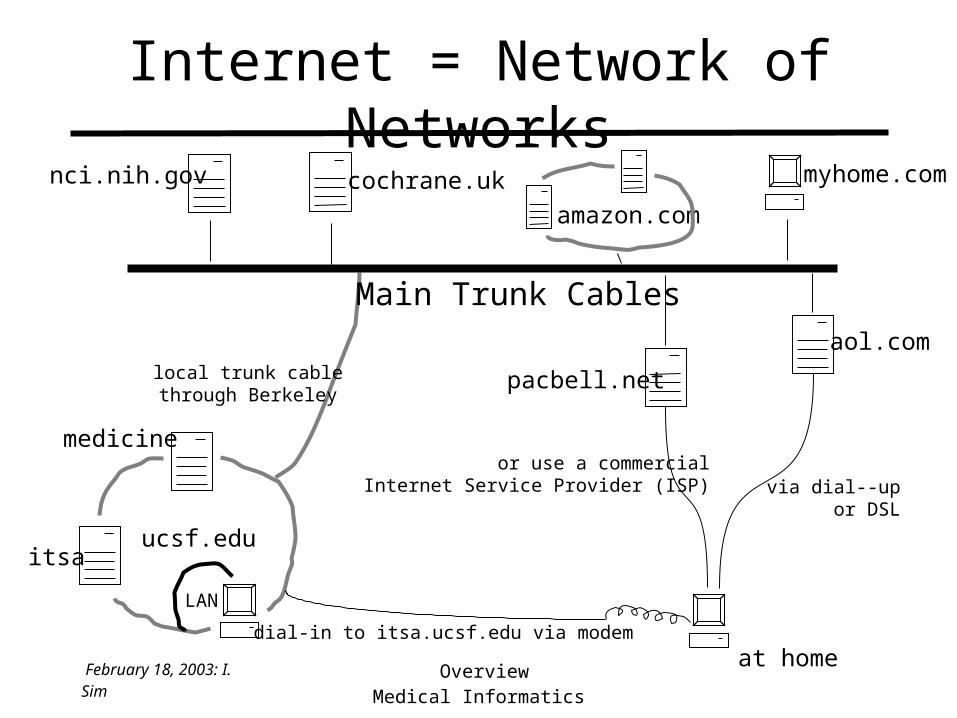
Internet = Network of Networks
itsa
medicine
ucsf.edu
nci.nih.gov cochrane.uk myhome.com
Main Trunk Cables
local trunk cablethrough Berkeley
amazon.com
at homedial-in to itsa.ucsf.edu via modem
pacbell.net
aol.com
or use a commercialInternet Service Provider (ISP) via dial--up
or DSL
LAN
February 18, 2003: I. Sim OverviewMedical Informatics
Networking Media• Copper wire (twisted pair)
– generally not well suited to high bandwith transmission
• Coaxial cable– can carry high frequencies without leak– cable industry has “more bandwidth by accident than
the telephone people have on purpose”
• Fiber optic– highest bandwidth, but expensive and de novo
• Curb-to-home problem– only phone and coax cables now run from curb to home– hybrid fiber/coax cables and approaches coming
February 18, 2003: I. Sim OverviewMedical Informatics
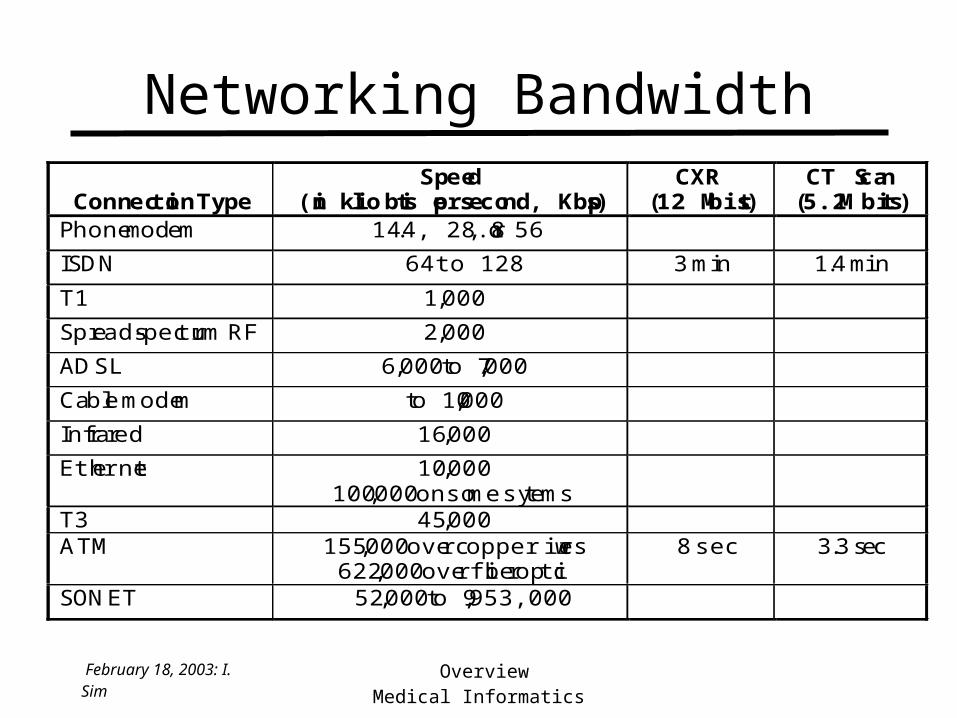
Networking BandwidthSim: Computer Infrastructure 1/26/00
Connection TypeSpeed
(in kilo bits per second, Kbps)CXR
(12 Mbits)CT Scan
(5.2 Mbits)Phone modem 14.4, 28.8, or 56
ISDN 64 to 128 3 min 1.4 min
T1 1,000
Spread-spectrum RF 2,000
ADSL 6,000 to 7,000
Cable modem to 10,000
Infrared 16,000
Ethernet 10,000100,000 on some sytems
T3 45,000ATM 155,000 over copper wires
622,000 over fiberoptic8 sec 3.3 sec
SONET 52,000 to 9,953,000

February 18, 2003: I. Sim OverviewMedical Informatics
What Happens over Network Cables?
itsa
medicine
ucsf.edu
nci.nih.gov cochrane.uk myhome.com
Main Trunk Cables
amazon.com
at home
pacbell.net
aol.com
LAN

February 18, 2003: I. Sim OverviewMedical Informatics
• Protocol = grammar for machines talking to each other– e..g, protocol for the WWW = http
• WWW vs. Internet vs. Intranet vs. VPN– WWW = http-based communication on Internet– Intranet = network of networks restricted to
within an organization (usually implies only http-based communication)
– Virtual Private Network is an Intranet that physically uses part of the Internet
• Health-specific protocols needed (e.g., HL-7)
Networking Protocols

February 18, 2003: I. Sim OverviewMedical Informatics
Significant Issue in HealthCare
• UCSF spent ~$100 million on networking in the late 1990’s
• Health-specific networking “grammars” add to complexity of infrastructure
• Many interactive services (e.g., realtime teleconsultation) would need more bandwidth than is commonly available

February 18, 2003: I. Sim OverviewMedical Informatics
Conclusions
• Computing infrastructure for health care is very complex, very fragmented, has lots of gaps, and is saddled with lots of old technology
• Clinical (and research) databases are generally more reliable and efficient if they are relational rather than flat file
• Networking involves both hardware (cable) and software (protocols); bandwidth limits wide deployment of interactive technologies

February 18, 2003: I. Sim OverviewMedical Informatics
Teaching Points• If you want computers to do “smart” things with
your data (e.g., retrieve, sort, graph), you must describe that data very explicitly– what you don’t say the computer does not know
• Data models are standard abstract ways of describing data
• To send data back and forth, you also need very explicit “grammars” for communication
• Today = how of infrastructure; next class = what

February 18, 2003: I. Sim OverviewMedical Informatics
References
• L.T. Kohn, J.M. Corrigan, M.S. Donaldson, To Err is Human: Building a Safer Health System (Washington: National Academy Press, 1999.)
• Crossing the Quality Chasm: A New Health System for the 21st Century (Washington: National Academy Press, 2001)