Family Practice Endocrinology Rounds: Pearls of...
67
Family Practice Endocrinology Rounds: Pearls of Menopausal Hormone Replacement Therapy and Osteoporosis Dr. Priya Manjoo, MD, FRCPC Endocrinology, Diplomat of the American Board of Obesity Medicine Clinical Assistant Professor, University of British Columbia, Department of Endocrinology
-
Upload
trinhxuyen -
Category
Documents
-
view
214 -
download
0
Transcript of Family Practice Endocrinology Rounds: Pearls of...
Family Practice Endocrinology Rounds:Pearls of Menopausal Hormone
Replacement Therapy and OsteoporosisDr. Priya Manjoo,
MD, FRCPC Endocrinology,Diplomat of the American Board of Obesity Medicine
Clinical Assistant Professor,University of British Columbia, Department of Endocrinology

OUTLINE
HRT• HRT and CVD• HRT and Breast Cancer
OSTEOPOROSIS• Selection of cases for
treatment• Duration of therapy• Bisphosphonates• New data

CASE 143 female presents to your office asking for an opinion onHRT. She has hot flushes keeping her up at night andinterfering with her energy levels and ability to functionduring the day starting a few months ago and getting worse.
She had a TAH for dysmenorrhea 2 years ago. She did nothave an oopherectomy. She has no personal or familyhistory of breast cancer or venous thromboembolic disease.She does not smoke and exercises regularly. Her BMI is 24kg/m2, BP 120/70; Her framingham score places her in thelowest risk category. FSH is 56.

CASE 1She has read the USPSTF recommendations stating:“The chronic disease prevention benefits of estrogen areunlikely to outweigh the harms in most postmenopausalwomen who have had a hysterectomy.”
She is concerned about the risks of HRT but very muchwants relief of her symptoms so she can “get back to herlife”.

CASE 1Which of the following advice is appropriate for her:A. Advise against HRT because of the increased risk of
cardiovascular disease and breast cancer risk.B. Advise against HRT because of the increased risk of
venous thromboembolic diseaseC. Advise that she may be a good candidate for HRT
because of benefits in symptomatic relief of hermenopausal symptoms and potential benefit oncardiovascular disease risk and bone health
D. Suggest treatment with complimentary therapies such asblack cohosh, Soy and evening primrose

Important HRT study features
WHI Observational Studies
Vasomotor symptoms Absent Present
Age at start of HRT 63 yrs 52 yrs
Time since menopause 12 yrs 2 yrs
BMI (kg/m2) 28-30 24-25

Important HRT study featuresAge CEE CEE/MPA50-59 0.63 (CI 0.36–1.09) 1.29 (CI 0.79 –2.12)
60-69 0.94 (CI 0.71–1.24) 1.03 (CI 0.74 –1.43)
70-79 1.13 (CI 0.82–1.54) 1.48 (CI 1.04 –2.11)
P value for trend 0.12 0.70
Time since menopause CEE CEE/MPA
<10 years 0.48 (CI 0.20–1.17) 0.88 (CI 0.54 –1.43)
10-19 0.96 (CI 0.64–1.44) 1.23 (CI 0.85–1.77)
≥ 20 1.12 (CI 0.86–1.46) 1.66 (CI 1.14 –2.41)
P value for trend 0.15 0.05
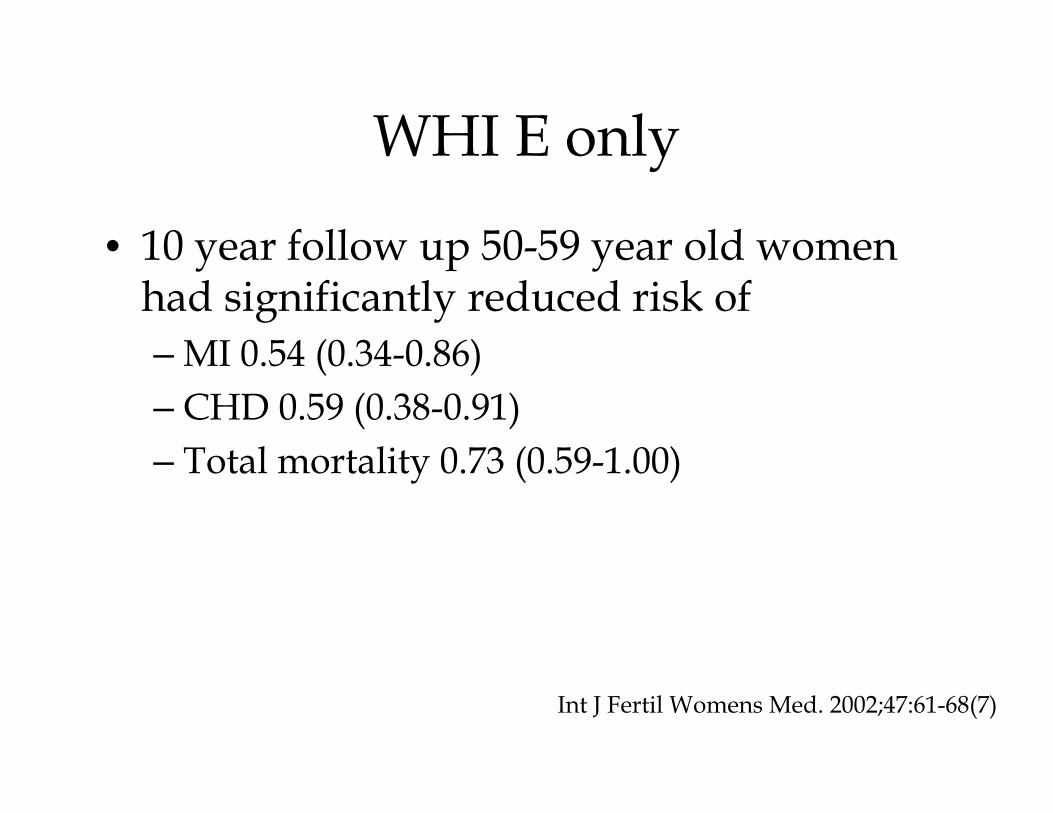
WHI E only
• 10 year follow up 50-59 year old women had significantly reduced risk of– MI 0.54 (0.34-0.86)– CHD 0.59 (0.38-0.91)– Total mortality 0.73 (0.59-1.00)
Int J Fertil Womens Med. 2002;47:61-68(7)
Timing Hypothesis
• Younger symptomatic women at onset of menopause may be protected from CHD
• Older women treated for the first time have no benefit and may have early harm

Progression of atherosclerosis by age in postmenopausal women
Int J Fertil Womens Med. 2002;47:61-68(7)

KRONOS Early Estrogen prevention study (KEEP)
• Surrogate markers evaluated among young women on HRT at onset of menopause.
• RCT in women within 3 years of menopause• Placebo VEE or transdermal estrogen• Uterus =micronized progesterone for 12 days each
month• CIMT increase similar in all groups• Non-significant trend for Coronary Calcium score
to progress less in the 2 estrogen groups compared with placebo.
• (Low coronary calcium score at entry)

KRONOS Early Estrogen prevention study (KEEP)
• CIMT increase similar in all groups• Non-significant trend for Coronary
Calcium score to progress less in the 2 estrogen groups compared with placebo.
• (Low coronary calcium score at entry)
Danish Osteoporosis Study
• RCT of 1006 younger women at the onset of menopause
• Open-label fashion with oral estradiol and norethindrone acetate or estradiol alone for 10 years
• 16 year follow upSchierbeck et al. BMJ 345:e6409 (30)

Danish Osteoporosis Study
• Combined endpoint of mortality and hospitalization for heart failure or MI significantly was reduced in those women randomized to HRT compared to the control women randomized to no treatment.
• Younger the women were in trial the greater the benefit with no increase in thrombosis, stroke or cancer.
Schierbeck et al. BMJ 345:e6409 (30)

Consensus from Endocrine Society
• Based on Grade B level Evidence• Basic science. Animal models and
observational studies support the hypothesis that MHT may prevent atherosclerosis and reduce CHD events
• Subgroups analysis suggested that the lack of benefit or increase in CHD risk observed in the overall analysis of WHI results from harmful effects of MHD in older women starting therapy many years after the onset of menopause

Breast Cancer• Potential risk of breast cancer into
perspective is extremely important indiscussing HT with women
• Estrogen alone may decrease the risk• Probably does not increase the risk unless
large doses are used for prolonged time in susceptible women with unknown occult tumors
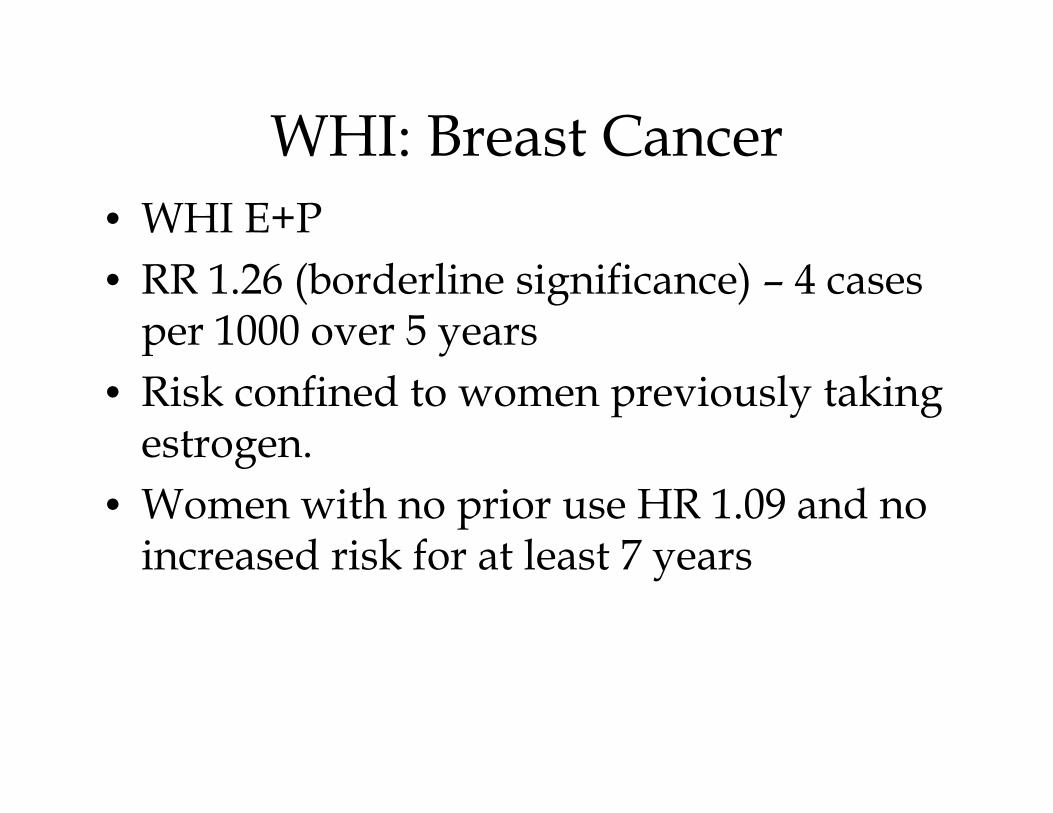
WHI: Breast Cancer• WHI E+P • RR 1.26 (borderline significance) – 4 cases
per 1000 over 5 years• Risk confined to women previously taking
estrogen. • Women with no prior use HR 1.09 and no
increased risk for at least 7 years

WHI: Breast Cancer• Estrogen only: • No increased risk/slight decrease in risk
(Stefanick JAMA 2006)• After 10.7 years total follow up, the
decreased risk in breast cancer persisted (median 5.9 years of use). La Croix 2011
• Observational studies showed increased risk of breast cancer during 15 year follow up suggesting that longer duration of use is associated with breast cancer.

GAP Time• WHI E+P RR 1.26 – 4 cases per 1000 over 5
years of use in young women (Santen)• Women who started within 5 years of last
menses: may experience a higher risk of breast cancer than those who wait for 10 years.
• Combined analysis (WHI with observational studies): Women who started within 5 years of use RR (1.64 (1.00, 2.68) vs. 0.99 if started 5 years or more years after last menses (would be excess of 10 per 1000)

GAP Time• Context of other risk factors• High risk (i.e. 4% chance of breast cancer in
5 years ) excess risk 20/1000/5 years (Santen JCEM 2010)
• Gail Model• Early menarche, late age at first pregnancy,
2 1st degree relatives with breast cancer, 2 breast biopsies (but no=atypical hyperplasia): 5 year risk is 4.1%

WHI: Breast Cancer• Estrogen only: • No increased risk/slight decrease in risk
(Stefanick JAMA 2006)• omen who started within 5 years of last
menses: for 5 years of use RR (1.64 (1.00, 2.68) vs. ).99 if started 5 years or more years after last menses (would be excess of 10 per 1000)

Breast Cancer• E+P in young women initializing standard
dose therapy for the first time at the onset of menopause do not appear to have an increased risk of breast cancer for at least 5 years and probably for up to 7 years.
• The risk does increase thereafter (using regime studied in WHI)

Breast Cancer• Observational data from France (1) suggest
that the risk is not increased with micronized progesterone dihydrogesterone
• DOPS using estradiol and norethindrone there was no increase in breast cancer for up to 11 years and a 16 year follow up. (small trial).
1. Fournier et al. Breast Cancer Res Treat. 2008;107; 103-111

Breast CancerGail Model can be used to estimate cancer risk –http://www.cancer.gov.bcrisktoolmobile
Gail MH, Brinton LA, Byar DP, Corle DK, Green SB, Shairer C, Mulvihill JJ. J Natl Cancer Inst 81(24):1879-86, 1989.
Breast Cancer• For the subgroup of first-time hormone users of
estrogen plus a progestogen, the overall WHI data indicate no increased risk after 5.2 yr, particularly in those starting MHT several years after the onset of menopause.
• The risk of breast cancer in association with estrogens alone and estrogens plus a progestogen returns to approximately that of nonusers within 3–5 yr of cessation.
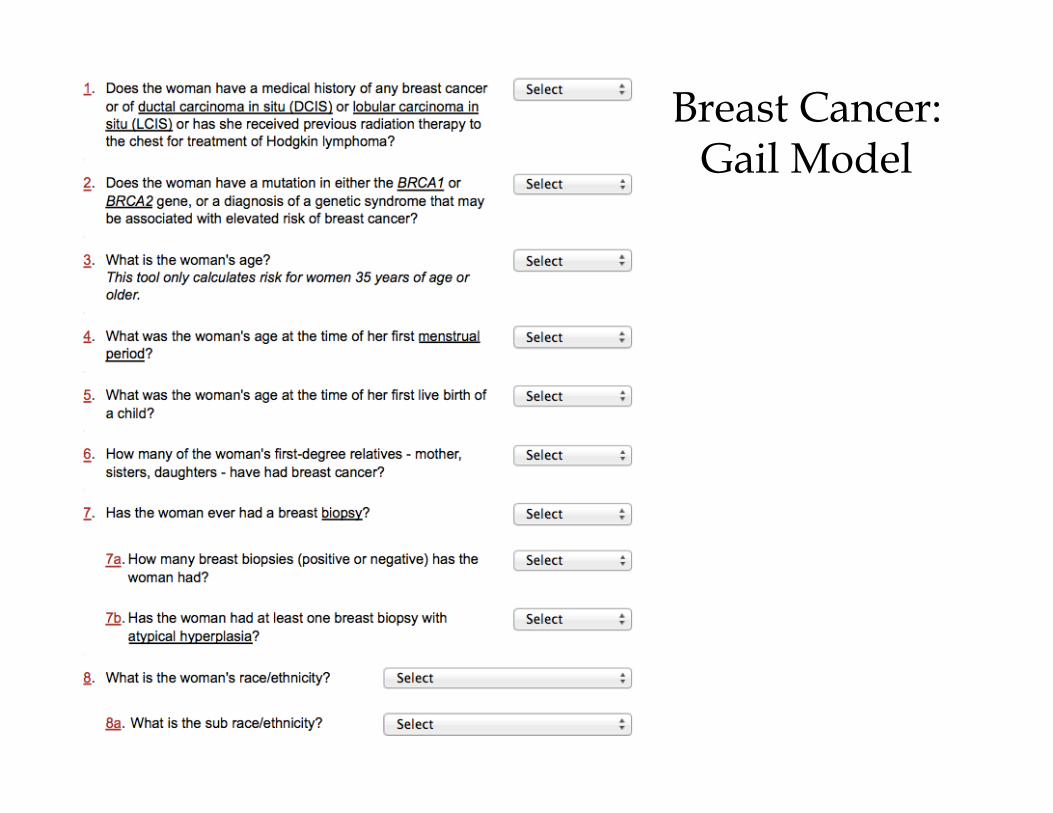
Breast Cancer: Gail Model

Consensus from Endocrine Society
• Reanalyzes of the WHI • Available data on women starting MHT
<10 years postmenopausal• Summarized as the excess number of
women experiencing benefit or risk per 1000 women using MHT for 5 years or more.

Consensus from Endocrine Society
• Benefits and Risks of MHT in Women Recently Menopausal (i.e. ages 50–59 or <10 yr postmenopausal)
• Reanalyzes of the WHI indicated the important influences of age and time since initiation of MHT on benefits and risks. Because most women start MHT shortly after menopause, available data regarding these women were specifically analyzed.

Consensus from Endocrine SocietyExcess number of women experiencing benefit or risk per 1000 women using MHT for 5 years or more.
Harm from Standard Oral Estrogen Alone Excess number0 –1 Increase in colorectal cancer , ovarian cancer 1.1–5 Increase in venothrombotic episodes, stroke 5.1–10 None>10 Increase in cholecystitis
Harm from Oral Estrogen Plus a Progestogen Excess number0–1 Increase in stroke1.1–5 Increase in coronary heart disease (subgroup ages, 50–59 yr)5.1–10 Increase in breast cancer, venothrombotic episodes, cholecystitis >10 None

Consensus from Endocrine SocietyExcess number of women experiencing benefit or risk per 1000 women using MHT for 5 years or more.
Benefits of Estrogen Alone (excess number of women per 1000 per 5 yr of use who experienced event attributable to use of MHT)Excess number 0-1 None1.1-5 Reduction in breast cancer, coronary heart disease5.1-10 Reduction in type 2 diabetes
Benefits of Estrogen Plus a Progestogen Excess number 0 –1 Reduction in coronary heart disease (sub- group <10 yr postmenopausal),
endometrial cancer 1.1–5 Reduction in fractures, colorectal cancer 5.1–10 Reduction in overall mortality >10 Reduction in overall mortality
Osteoporosis

CASE 2
56 year old 2 years postmenopausal female weightof 50 kg, height 155 cm, with previous wristfracture and family history of osteoporosispresents for discussion of BMD results andosteoporosis prevention. She moved here fromEngland 2 years ago. No steroid use, rheumatoidarthritis, alcohol use or secondary causes ofosteoporosis.Her BMD shows T-score at the spine of -1.5 and at the hip of -1.9. She exercises regularly and is compliant with Vitamin D and calcium in her diet.

CASE 3
How would you advise her?A. No pharmacotherapy because her
bone density is >-2.5B. Treat her with anti-resorptive therapy
because she has a fractureC. Ask more information to determine
whether her fracture was a fragilityfracture
D. Monitor and repeat BMD in 3 years

CASE 2

CASE 3
Similar patient from Tunisia. 56 year old, 2 yearspostmenopausal female weight of 50 kg, height 155cm, with previous wrist fracture and family historyof osteoporosis presents for discussion of BMDresults and osteoporosis prevention. She moved herefrom Tunisia 5 years ago. No steroid use,rheumatoid arthritis, alcohol use or secondarycauses of osteoporosis.Her BMD shows T-score at the spine of -1.5 and at the hip of -1.9. She exercises regularly and is compliant with Vitamin D and calcium in her diet.

CASE 3

CASE 3
How would you advise her?A. No pharmacotherapy because her
bone density is >-2.5B. Treat her with anti-resorptive therapy
because she has a fractureC. Ask more information to determine
whether her fracture was a fragilityfracture
D. Monitor and repeat BMD in 3 years
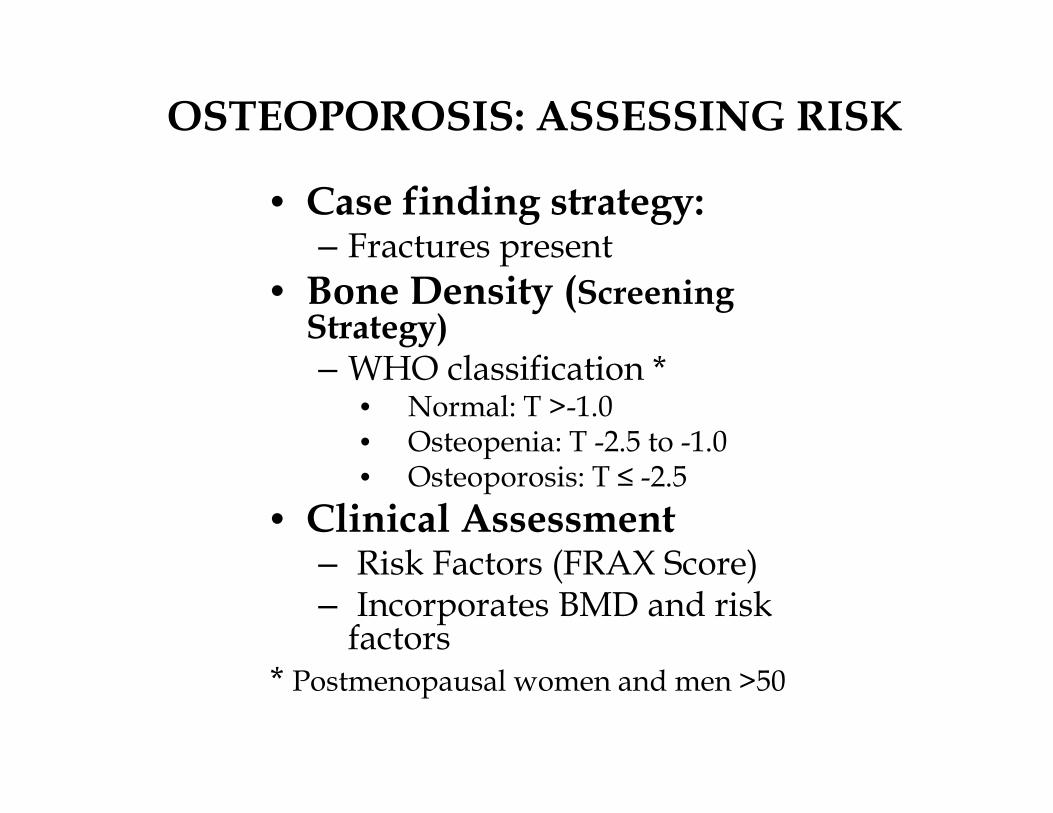
OSTEOPOROSIS: ASSESSING RISK
• Case finding strategy: – Fractures present
• Bone Density (Screening Strategy)– WHO classification *
• Normal: T >-1.0• Osteopenia: T -2.5 to -1.0• Osteoporosis: T ≤ -2.5
• Clinical Assessment – Risk Factors (FRAX Score)– Incorporates BMD and risk
factors* Postmenopausal women and men >50

OSTEOPOROSIS: WHEN TO TREAT
Assess Risk Factors and BMD if suitable
Hip or vertebral fracture or BMD
T-score <2.5 (spine, FN or total hip
T-score between -2.5 and -1.0
FRAX Score
10 year probability of hip fracture >3% or major
osteoporotic fracture >20%
Treat
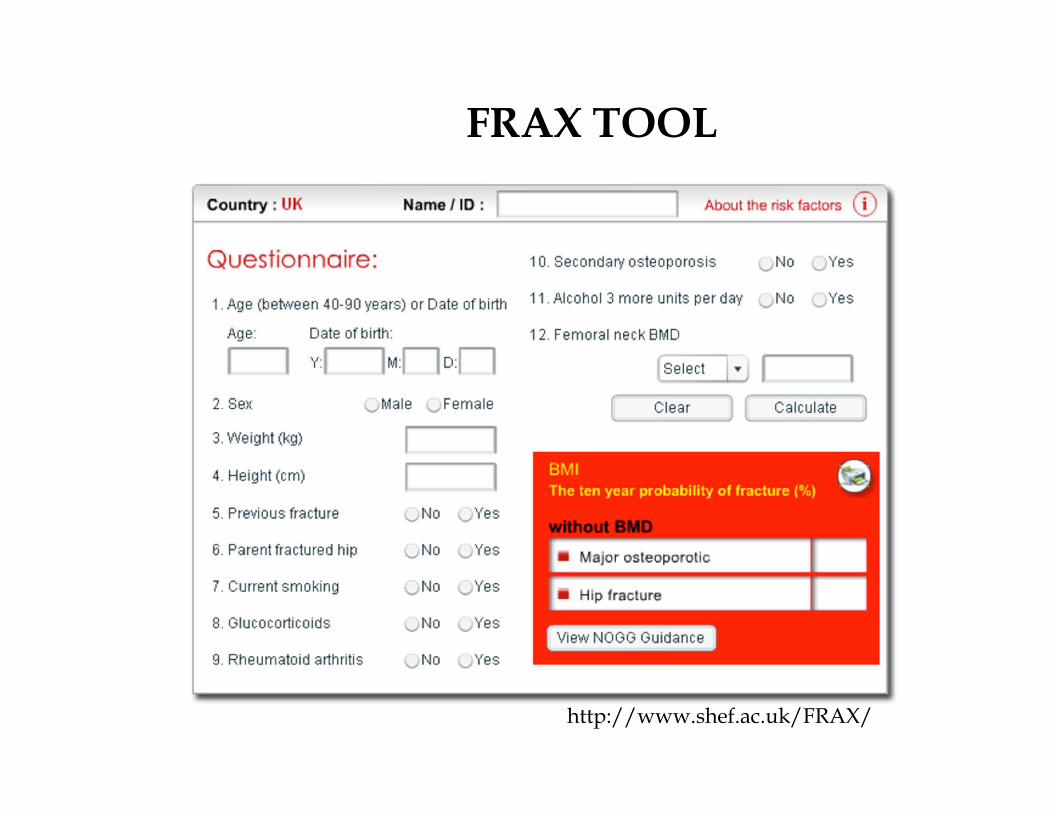
FRAX TOOL
http://www.shef.ac.uk/FRAX/

FRAX PROBABILITIES BY COUNTRY
Baims et al. 2012

CHANGES IN BONE MASS

CASE 4
56 year old female was 2 years postmenopausal attime of initiation of aledronate for osteoporosistreatment. She has a previous vertebral fractureand family history of osteoporosis. Her femoralneck BMD was -2.6 at the time of initiation oftherapy. She has not had any interval fractures orheight loss. No steroid use, rheumatoid arthritis,alcohol use or secondary causes of osteoporosis.Her BMD shows T-score at the spine of -1.9 and at the hip of -2.5. She exercises regularly and is compliant with Vitamin D and calcium in her diet.
CASE 4
She would like to know if she can stop thealendronate now. How would you advise her:
1. Continue treatment for another 5 years2. Stop therapy and repeat BMD in 3 year3. Switch to a different agent4. Stop for 2 years and reinitiate therapy
with another agent.

BISPHOSPHONATES
Duration of therapy of concern because of the longer retention of bone with recycling of drug leaving a reservoir within bone

BISPHOSPHONATESFew data available for assessing theefficacy of long- term bisphosphonate use(>5 years) in reducing the risk of fractures.
Two randomized trials with a combinedsample size of 2342 women
FLEX Trial (Aledronate vs. Placebo)HORIZON-extension trial (ZA)
The FLEX and HORIZON extensionstudies used changes in bone mineraldensity as their primary end points andreported fractures as exploratory endpoints.

BISPHOSPHONATESFLEX STUDYFracture Intervention Trial Long-Term Extension (FLEX), 1099 postmenopausal women who had received aledronate for 5 years Randomized to treatment for another 5 years versus placebo

FLEX

BISPHOSPHONATES
Health Outcomes and Reduced Incidence with Zoledronic Acid Once Yearly (HORIZON) Exten-sion trial
~1200 Postmenopausal women who had received 3 years of treatment were randomized to another 3 years of placebo or active extension

BISPHOSPHONATESHORIZON-PFT
• Zoledronic acid (ZA) 5 mg used annually for 3 years has beenshown to be effective in increasing BMD and decreasingfractures
• The extension trial of HORIZON-PFT evaluated the effect ofcontinuing ZA for 3 more years
• All patients eligible for the extension trial had to have receivedall 3 annual infusions of ZA
• A total of 1233 women were randomized to either ZA for 3 moreyears (Z6 group) or to placebo (Z3P3 group)
Baseline characteristics of the two groups were similar with abouthalf of each group having bone mineral density (BMD) T-scores atthe femoral neck <-2.5 and about 60% having 1 or more vertebralfractures.

HORIZON - Extension

HORIZON - Extension

HORIZON - Extension
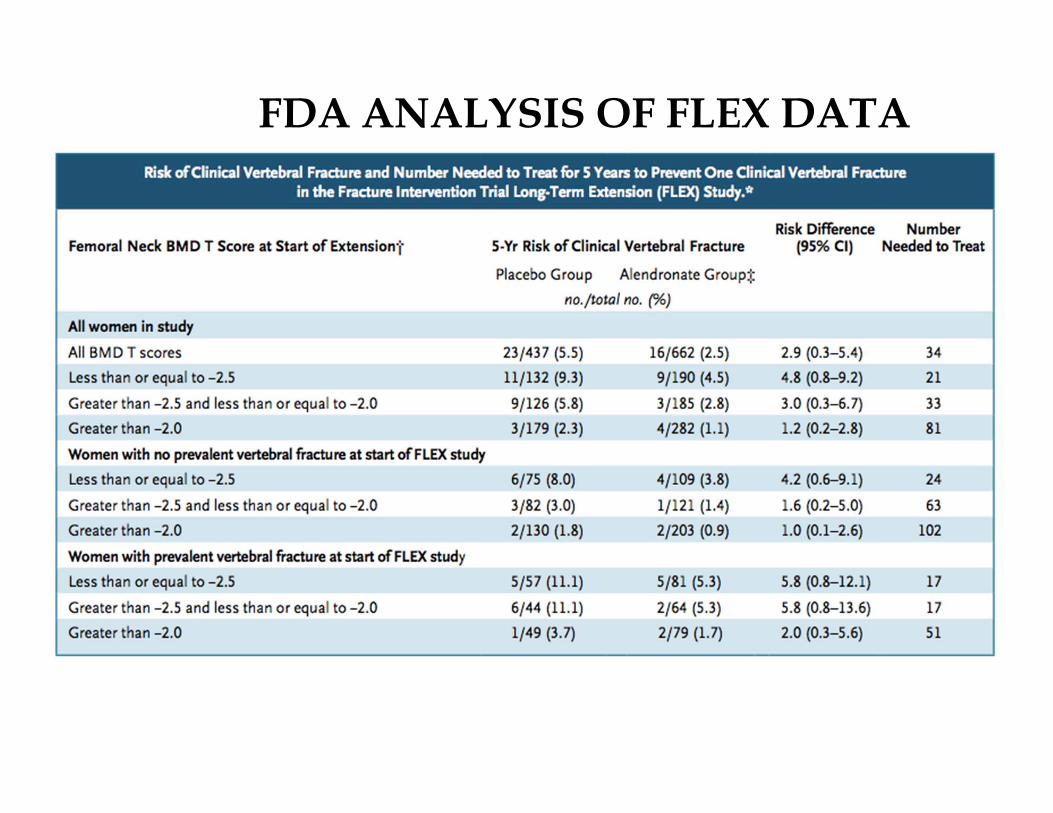
FDA ANALYSIS OF FLEX DATA
Conclusions from FLEX and HORIZON
Bone loss after discontinuation of therapy was only modest as compared with that during continued drug therapy suggesting persistence of bisphosphonate effects
Patients likely to benefit from extended therapy:
• low BMD at femoral neck (T <-2.5) after 3-5 years of treatment
• Existing vertebral fracture and T score <-2.0 may also benefit
• Femoral neck of above -2.0 have low risk of fracture are unlikely to benefit form continued treatment.

Conclusions from FLEX and HORIZON
No further reduction in non-vertebral fractures
Continued benefit for reduction of vertebral fracturesConfidence intervals were wideFracture numbers were low
BUT
Some guidance on treatment

BISPHOSPHONATESNumbers needed to treat are much higher forthose with no preexisting fracture who have afemoral neck T score above −2.0 after aninitial treatment period,
Suggests that such women can discontinuetreatment and have a relatively low risk ofsubsequent vertebral fracture.
This group of patients would include many ofthose who originally began receivingbisphosphonates when they had a bone mineraldensity above the osteoporotic range or for theprevention of bone loss
New Data

The Effect of 6 vs. 9 Years of Zoledronic Acid Treatment in Osteoporosis: A Randomized Extension
to the HORIZON‐Pivotal Fracture Trial (PFT)
Objective: Extension of a 6‐year study to evaluate efficacy and long‐term safety of ZOL (5 mg) after 9 consecutive annual doses in post‐menopausal women with osteoporosis (n = 190)
BMD, bone mineral density; β‐CTx, β‐C‐terminal telopeptides of type 1 collagen; BSAP, bone‐specific alkaline phosphatase; FN, femoral neck; P1NP, procollagen type 1 amino‐terminal propeptide; TH, total hip; ZOL, zoledronic acid.
Black D, et al. San Francisco, USA. The Effect of 6 versus 9 Years of Zoledronic Acid Treatment in Osteoporosis: A Randomized Extension to the HORIZON‐Pivotal Fracture Trial (PFT). Abstract [SA0389]. Presented at the 2013 Annual Meeting of The American Society for Bone and Mineral Research. October 4, 2013.
Primary end point
Comparison of ZOL (Z9) with placebo (Z6P3) for percentage change in TH BMD at 9 years vs. 6 years
Secondary end point
Comparison of TH and FN BMD at 7, 8, and 9 years vs. 0 year; at 7 and 8 years vs. 6 years; FN BMD at 9 years vs. 6 years
Comparison of biochemical markers (β‐CTx, P1NP, BSAP) at 7, 8, and 9 years vs. 6 years
TOC

The Effect of 6 vs. 9 Years of Zoledronic Acid Treatment in Osteoporosis: A Randomized Extension to the
HORIZON‐Pivotal Fracture Trial (PFT) Results
• Mean age 78 years, with 28% over 80 years of age• 63% from Europe, 32% from N/S America, 6% from Asia• No differences in the biochemical markers Z6P3 vs. Z9• No difference in BMD (THip :‐1.31% in Z6P3 vs..‐0.54% in Z9, p=n.s.) Z6P3 vs. Z9• Incidence of fractures was low and similar in both groups (morphometric vertebral
fractures: 5.2% in Z6P3 vs. 3.2% in Z9)
BMD: Bone mineral density; N/S: North/South; n.s., not significant; Z6P3, placebo; Z9, zoledronic acid.
TOC
Black D, et al. San Francisco, USA. The Effect of 6 versus 9 Years of Zoledronic Acid Treatment in Osteoporosis: A Randomized Extension to the HORIZON‐Pivotal Fracture Trial (PFT). Abstract [SA0389]. Presented at the 2013 Annual Meeting of The American Society for Bone and Mineral Research. October 4, 2013.

The Effect of 6 vs. 9 Years of Zoledronic Acid Treatment in Osteoporosis: A Randomized Extension to the
HORIZON-Pivotal Fracture Trial (PFT) Conclusions
Authors
• Extension study provides data on the effect of 9 annual injections of ZOL • Little evidence for further benefit after 6 years of treatment
BMD, bone mineral density; ZOL, zoledronic acid.
• Zoledronic acid beyond 6 years in patients with osteoporosis shows no further benefit
Clinical impact from reviewer’s perspective
TOC
Black D, et al. San Francisco, USA. The Effect of 6 versus 9 Years of Zoledronic Acid Treatment in Osteoporosis: A Randomized Extension to the HORIZON‐Pivotal Fracture Trial (PFT). Abstract [SA0389]. Presented at the 2013 Annual Meeting of The American Society for Bone and Mineral Research. October 4, 2013.

Objective: To report the results from the first 5 years of Fracture REduction Evaluation of Denosumab in Osteoporosis Every 6 Months (FREEDOM) extension study (a 7‐year extension study of the 3‐year FREEDOM study), representing up to 8 years of continued DMAb treatment in postmenopausal women with osteoporosis
DMAb, denosumab; Q6M, every 6 months.
Papapoulos S, et al. Leiden University Medical Center, The Netherlands. Eight Years of Denosumab Treatment in Postmenopausal Women With Osteoporosis: Results From the First Five Years of the FREEDOM Extension. Abstract [LB‐MO26].Presented at the 2013 Annual Meeting of The American Society for Bone and Mineral Research. October 7, 2013.
• Extension study: All subjects (N = 3046) received 60 mg DMAb Q6M and daily calcium and vitamin D
• Overall, 2678 (88%) subjects completed dosing at year 8 (1382 subjects in the long‐term group and 1296 subjects in the cross‐over group)
Long‐term group
Eight years of DMAb treatment
Three years in the FREEDOM study
Five years in the extension study
Cross‐over group
Five years of DMAb treatment
Three years of placebo in the FREEDOM study
Five years of DMAb in the extension study
TOC
Eight Years of Denosumab Treatment in Postmenopausal WomenWith Osteoporosis: Results From the First Five Years of the
FREEDOM Extension

AE, adverse events; BMD, bone mineral density; CTX, C-telopeptide; DMAb, denosumab; SAE, serious adverse events.
• Serum CTX decreased rapidly after each DMAb dose with a characteristic attenuation effect at the end of the dosing period
• Incidence of new vertebral and non‐vertebral fractures remained low throughout the extension
– Hip fracture incidences during 8 years were 0.2% and <0.1% for the long‐term and cross‐over groups, respectively
• Incidence of AEs and SAEs was consistent with the previously reported data in the extension study
TOC
Papapoulos S, et al. Leiden University Medical Center, The Netherlands. Eight Years of Denosumab Treatment in Postmenopausal Women With Osteoporosis: Results From the First Five Years of the FREEDOM Extension. Abstract [LB‐MO26]. Presented at the 2013 Annual Meeting of The American Society for Bone and Mineral Research. October 7, 2013.
Eight Years of Denosumab Treatment in Postmenopausal WomenWith Osteoporosis: Results From the First Five Years of the
FREEDOM ExtensionResults
a
aa
ab
bb
b
b
bb
b
a
Long-term
Cross-over
18.5%
Lumbar Spine
FREEDOM Extension
a
13.8%
Perc
ent C
hang
e Fr
om B
asel
ine 22
201816141210
86420
-20 .5 1 2 3 4 5 6 8
Long-term
Cross-over
FREEDOM Extension
Total Hip
Perc
ent C
hang
e Fr
om B
asel
ine 8.2%
4.8%
b
bb
bbb
bb
aa
aa
aa
aa
109876543210
-1-2
0 .5 1 2 3 4 5 6 8
Placebo DenosumabaP<.05 compared with FREEDOM baseline.bP<.05 compared with FREEDOM baseline and extension baseline.
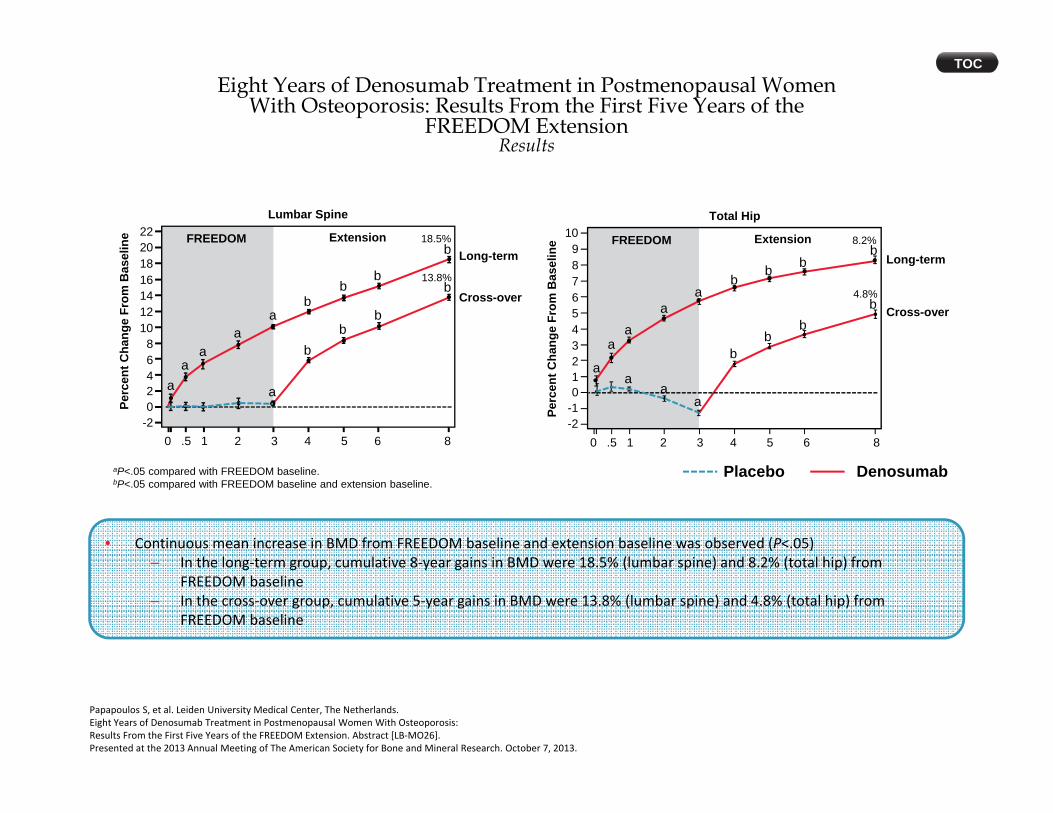
• Continuous mean increase in BMD from FREEDOM baseline and extension baseline was observed (P<.05)– In the long‐term group, cumulative 8‐year gains in BMD were 18.5% (lumbar spine) and 8.2% (total hip) from
FREEDOM baseline– In the cross‐over group, cumulative 5‐year gains in BMD were 13.8% (lumbar spine) and 4.8% (total hip) from
FREEDOM baseline
TOC
Papapoulos S, et al. Leiden University Medical Center, The Netherlands. Eight Years of Denosumab Treatment in Postmenopausal Women With Osteoporosis: Results From the First Five Years of the FREEDOM Extension. Abstract [LB‐MO26]. Presented at the 2013 Annual Meeting of The American Society for Bone and Mineral Research. October 7, 2013.
Eight Years of Denosumab Treatment in Postmenopausal WomenWith Osteoporosis: Results From the First Five Years of the
FREEDOM ExtensionResults

Eight Years of Denosumab Treatment in Postmenopausal WomenWith Osteoporosis: Results From the First Five Years of the
FREEDOM ExtensionConclusions
Authors
Treatment with DMAb for up to 8 years was associated with continuous improvement in BMD, reduction in bone turnover, and decreased incidence of fracture in postmenopausal women with osteoporosis
BMD, bone mineral density; DMAb, denosumab.
Clinical impact from reviewer’s perspective
• The increase in BMD associated with long‐term DMAb treatment is clearly remarkable.
• The relationship of the increase in BMD to long‐term nonvertebral fracture risk reduction needs further study.
TOC
Papapoulos S, et al. Leiden University Medical Center, The Netherlands. Eight Years of Denosumab Treatment in Postmenopausal Women With Osteoporosis: Results From the First Five Years of the FREEDOM Extension. Abstract [LB‐MO26]. Presented at the 2013 Annual Meeting of The American Society for Bone and Mineral Research. October 7, 2013.

PROGRESSION TO OSTEOPOROSIS

PROGRESSION TO OSTEOPOROSIS
Screening interval of 15 years 10% of older, postmenopausal women with
normal bone density or mild osteopenia (T score, > −1.5) at the initial assessment
would progress to osteoporosis Screening interval of 5 years
10% of women with moderate osteopenia (T score, −1.50 to −1.99) would progress to osteoporosis
Screening interval of 1 year 10% of women with advanced osteopenia T score, −2.00 to −2.49) would progress to osteoporosis