
Family-Centered Care (FCC) and Patient Safety Thursday, June 21, 2007 12:00 – 1:00 p.m. EDT.
74
Family-Centered Care (FCC) and Patient Safety Thursday, June 21, 2007 12:00 – 1:00 p.m. EDT
-
Upload
rosamund-ray -
Category
Documents
-
view
221 -
download
3
Transcript of Family-Centered Care (FCC) and Patient Safety Thursday, June 21, 2007 12:00 – 1:00 p.m. EDT.

Family-Centered Care (FCC)and Patient Safety
Thursday, June 21, 200712:00 – 1:00 p.m. EDT

Moderator: Erin R. Stucky, MD, FAAPPediatric HospitalistChildren’s Specialists of San DiegoRady Children’s HospitalSan Diego, California

This activity was funded through an educational grant from the Physicians’ Foundation for
Health Systems Excellence.

Disclosure of Financial Relationships and Resolution of Conflicts of Interest for AAP CME Activities Grid
The AAP CME program aims to develop, maintain, and increase the competency, skills, and professional performance of pediatric healthcare professionals by providing high quality, relevant, accessible and cost-effective educational experiences. The AAP CME program provides activities to meet the participants’ identified education needs and to support their lifelong learning towards a goal of improving care for children and families (AAP CME Program Mission Statement, August 2004).
The AAP recognizes that there are a variety of financial relationships between individuals and commercial interests that require review to identify possible conflicts of interest in a CME activity. The “AAP Policy on Disclosure of Financial Relationships and Resolution of Conflicts of Interest for AAP CME Activities” is designed to ensure quality, objective, balanced, and scientifically rigorous AAP CME activities by identifying and resolving all potential conflicts of interest prior to the confirmation of service of those in a position to influence and/or control CME content. The AAP has taken steps to resolve any potential conflicts of interest.
All AAP CME activities will strictly adhere to the 2004 Updated Accreditation Council for Continuing Medical Education (ACCME) Standards for Commercial Support: Standards to Ensure the Independence of CME Activities. In accordance with these Standards, the following decisions will be made free of the control of a commercial interest: identification of CME needs, determination of educational objectives, selection and presentation of content, selection of all persons and organizations that will be in a position to control the content, selection of educational methods, and evaluation of the CME activity.
The purpose of this policy is to ensure all potential conflicts of interest are identified and mechanisms to resolve them prior to the CME activity are implemented in ways that are consistent with the public good. The AAP is committed to providing learners with commercially unbiased CME activities.
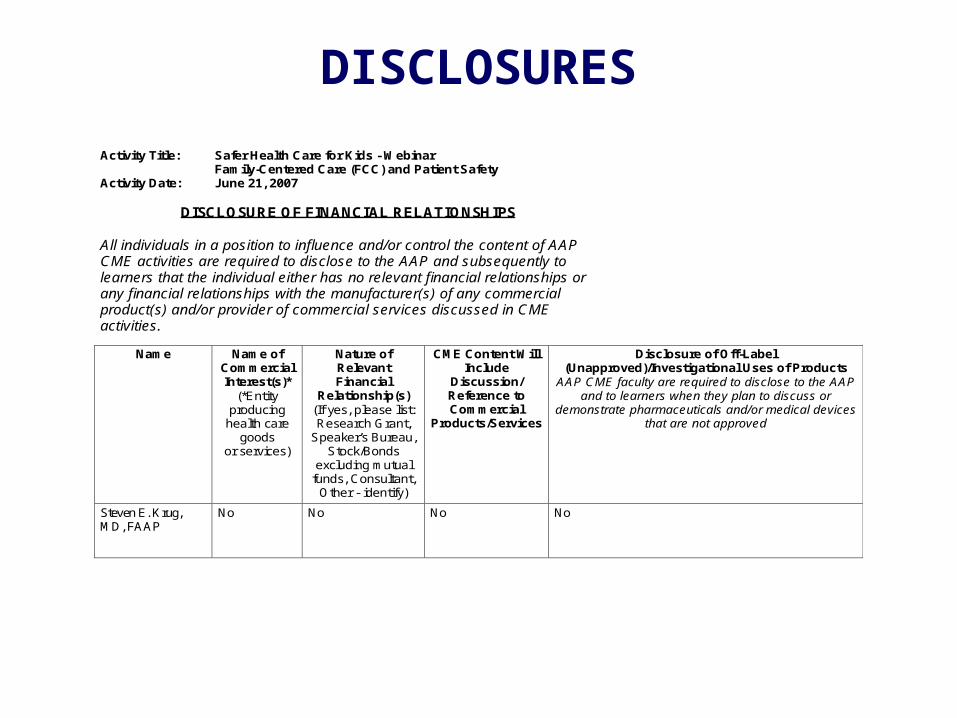
DISCLOSURES
Activity Title: Safer Health Care for Kids - Webinar Family-Centered Care (FCC) and Patient Safety Activity Date: June 21, 2007
DISCLOSURE OF FINANCIAL RELATIONSHIPS All individuals in a position to influence and/or control the content of AAP CME activities are required to disclose to the AAP and subsequently to learners that the individual either has no relevant financial relationships or any financial relationships with the manufacturer(s) of any commercial product(s) and/or provider of commercial services discussed in CME activities.
Name Name of Commercial Interest(s)*
(*Entity producing
health care goods
or services)
Nature of Relevant Financial
Relationship(s) (If yes, please list: Research Grant,
Speaker’s Bureau, Stock/Bonds
excluding mutual funds, Consultant,
Other - identify)
CME Content Will Include
Discussion/ Reference to Commercial
Products/Services
Disclosure of Off-Label (Unapproved)/Investigational Uses of Products
AAP CME faculty are required to disclose to the AAP and to learners when they plan to discuss or
demonstrate pharmaceuticals and/or medical devices that are not approved
Steven E. Krug, MD, FAAP
No No No No

DISCLOSURES
Name Name of Commercial Interest(s)*
(*Entity producing
health care goods
or services)
Nature of Relevant Financial
Relationship(s) (If yes, please list: Research Grant,
Speaker’s Bureau, Stock/Bonds
excluding mutual funds, Consultant,
Other - identify)
CME Content Will Include
Discussion/ Reference to Commercial
Products/Services
Disclosure of Off-Label (Unapproved)/Investigational Uses of Products
AAP CME faculty are required to disclose to the AAP and to learners when they plan to discuss or
demonstrate pharmaceuticals and/or medical devices that are not approved
John M. Neff, MD, FAAP
No Dr. Neff has disclosed the following financial relationships, unrelated to the content of this CME activity:
Consultant – ACAMBIS, to serve on DSMB’s on the development of smallpox vaccine
Consultant – National Association of Children’s Hospitals and Related Institutions (NACHRI), to consult on development of classification research, e.g., how to classify children’s health issues in administrative data sets.
No No

DISCLOSURESSAFER HEALTH CARE FOR KIDS - PROJECT ADVISORY COMMITTEE AND STAFF DISCLOSURE OF FINANCIAL RELATIONSHIPS All individuals in a position to influence and/or control the content of AAP CME activities are required to disclose to the AAP and subsequently to learners that the individual either has no relevant financial relationships or any financial relationships with the manufacturer(s) of any commercial product(s) and/or provider of commercial services discussed in CME activities.
Name Name of Commercial Interest(s)*
(*Entity producing health care goods
or services)
Nature of Relevant Financial Relationship(s)
(If yes, please list: Research Grant, Speaker’s
Bureau, Stock/Bonds excluding mutual funds,
Consultant, Other - identify)
CME Content Will Include Discussion/
Reference to Commercial Products/Services
Disclosure of Off-Label (Unapproved)/Investigational Uses
of Products AAP CME faculty are required to
disclose to the AAP and to learners when they plan to discuss or
demonstrate pharmaceuticals and/or medical devices that are not approved
Karen Frush, MD, FAAP (PAC Member)
No No No No
Uma Kotagal, MD, MBBS, MSc, FAAP (PAC Member)
No No No No
Christopher Landrigan, MD, MPH, FAAP (PAC Member)
No No No No
Marlene R. Miller, MD, MSc, FAAP (PAC Chair)
No No No No
Paul Sharek, MD, MPH. FAAP (PAC Member)
No No No No
Erin Stucky, MD, FAAP (PAC Member)
No No Not sure No
Nancy Nelson (AAP Staff) No No No No
Melissa Singleton, MEd (Project Manager – AAP Consultant)
No No No No
Junelle Speller (AAP Staff) No No No No
Linda Walsh, MAB (AAP Staff)
No No No No
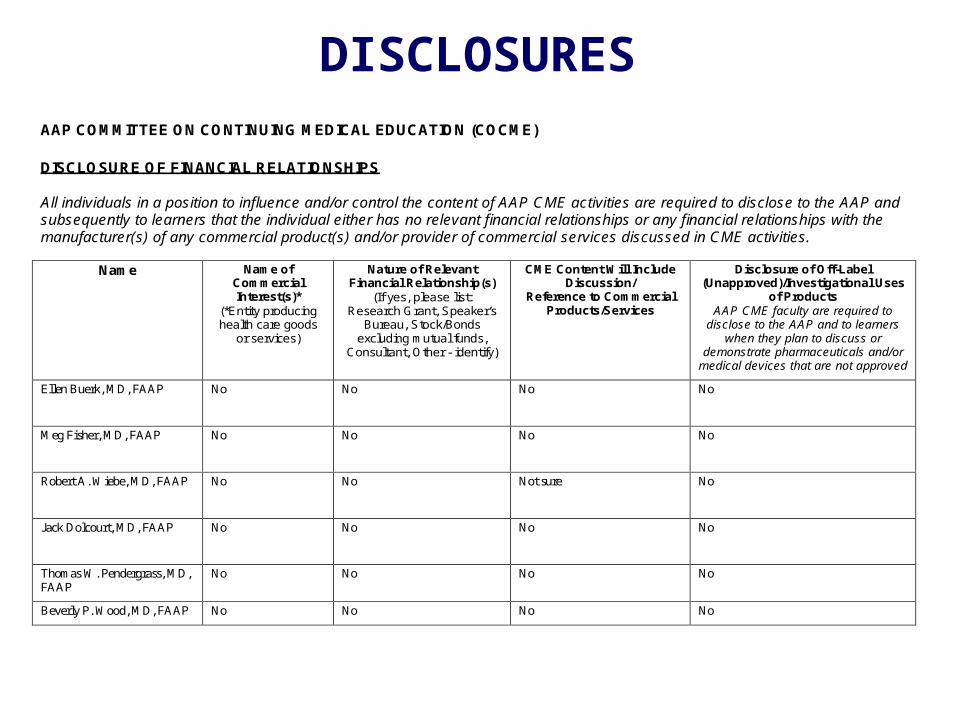
DISCLOSURESAAP COMMITTEE ON CONTINUING MEDICAL EDUCATION (COCME) DISCLOSURE OF FINANCIAL RELATIONSHIPS All individuals in a position to influence and/or control the content of AAP CME activities are required to disclose to the AAP and subsequently to learners that the individual either has no relevant financial relationships or any financial relationships with the manufacturer(s) of any commercial product(s) and/or provider of commercial services discussed in CME activities.
Name Name of Commercial Interest(s)*
(*Entity producing health care goods
or services)
Nature of Relevant Financial Relationship(s)
(If yes, please list: Research Grant, Speaker’s
Bureau, Stock/Bonds excluding mutual funds,
Consultant, Other - identify)
CME Content Will Include Discussion/
Reference to Commercial Products/Services
Disclosure of Off-Label (Unapproved)/Investigational Uses
of Products AAP CME faculty are required to
disclose to the AAP and to learners when they plan to discuss or
demonstrate pharmaceuticals and/or medical devices that are not approved
Ellen Buerk, MD, FAAP
No No No No
Meg Fisher, MD, FAAP
No No No No
Robert A. Wiebe, MD, FAAP
No No Not sure No
Jack Dolcourt, MD, FAAP
No No No No
Thomas W. Pendergrass, MD, FAAP
No No No No
Beverly P. Wood, MD, FAAP No No No No

CME CREDIT
The American Academy of Pediatrics (AAP) is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
The AAP designates this educational activity for a
maximum of 1.0 AMA PRA Category 1 Credit™. Physicians should only claim credit commensurate with the extent of their participation in the activity.
This activity is acceptable for up to 1.0 AAP credit.
This credit can be applied toward the AAP CME/CPD Award available to Fellows and Candidate Fellows of the American Academy of Pediatrics.

OTHER CREDIT
This webinar is approved by the National Association of Pediatric Nurse Practitioners (NAPNAP) for 1.2 NAPNAP contact hours of which 0.0 contain pharmacology (Rx) content. The AAP is designated as Agency #17. Upon completion of the program, each participant desiring NAPNAP contact hours should send a completed certificate of attendance, along with the required recording fee ($10 for NAPNAP members, $15 for nonmembers), to the NAPNAP National Office at 20 Brace Road, Suite 200, Cherry Hill, NJ 08034-2633.
The American Academy of Physician Assistants accepts
AMA PRA Category 1 Credit(s)TM from organizations accredited by the ACCME .

LEARNING OBJECTIVES
Upon completion of this activity, you will be able to:
Describe the relationship between FCC and pediatric patient safety.Recognize the importance of providing FCC when treating Children with Special Health Care Needs (CSHCN), as they are a very diverse population with very individual safety requirements.Educate parents and caregivers about patient safety, and engage them as true members of the health care team.

Steven E. Krug, MD, FAAPHead, Division of Emergency Medicine, Children’s Memorial
HospitalProfessor of Pediatrics, Northwesten University Feinberg School
of MedicineChicago, Illinois

John M. Neff, MD, FAAPProfessor of PediatricsDirector, Center for Children with Special Health Care NeedsUniversity of Washington/Children’s Hospital & Regional Medical
Ctr.Seattle, Washington

Patient Safety and Patient and Patient Safety and Patient and Family Centered Care of Family Centered Care of
Children in the Emergency Children in the Emergency DepartmentDepartment
American Academy of PediatricsAmerican Academy of PediatricsSafer Health Care for Kids WebinarSafer Health Care for Kids Webinar
June 21, 2007 June 21, 2007
Steven E. Krug, MDSteven E. Krug, MDChair, AAP Committee on Pediatric Emergency MedicineChair, AAP Committee on Pediatric Emergency Medicine
Professor of Pediatrics, Northwestern University Feinberg School of MedicineProfessor of Pediatrics, Northwestern University Feinberg School of MedicineHead, Division of Emergency Medicine, Children’s Memorial HospitalHead, Division of Emergency Medicine, Children’s Memorial Hospital

Patient Safety in HealthcarePatient Safety in Healthcare
To Err is Human: Building a Safer Health To Err is Human: Building a Safer Health SystemSystem (Institute of Medicine, 2000) (Institute of Medicine, 2000)
44,000 to 98,000 die each year in 44,000 to 98,000 die each year in US hospitals due to preventable US hospitals due to preventable medical errorsmedical errors
An even greater number suffer An even greater number suffer morbidity related to medical errormorbidity related to medical error
This is likely a underestimate of This is likely a underestimate of the true occurrence of patient the true occurrence of patient safety concernssafety concerns

National Quality ForumNational Quality ForumFactors associated with increased risk for Factors associated with increased risk for medical error in health caremedical error in health care
Multiple individuals involved in the care of a single Multiple individuals involved in the care of a single patientpatientPatients with high acuity illness or injuryPatients with high acuity illness or injuryRapid health care decisions under severe time Rapid health care decisions under severe time constraintsconstraintsHigh volume of patients and unpredictable flowHigh volume of patients and unpredictable flowBarriers to communication with patients, families and Barriers to communication with patients, families and other healthcare professionalsother healthcare professionalsInteractions with multiple types of diagnostic and/or Interactions with multiple types of diagnostic and/or treatment technologytreatment technology
Source: Kizer KW. Patient safety: a call to action. A consensus statement from the National Quality Forum. Medscape General Medicine 2001; 3:1-11.

Do These Factors Sound Familiar?Do These Factors Sound Familiar?

ACEP: Factors Placing Providers ACEP: Factors Placing Providers and Patients at Risk in the EDand Patients at Risk in the ED
OvercrowdingOvercrowding
Complexity of emergency patient and family needsComplexity of emergency patient and family needs
Shortage of healthcare workersShortage of healthcare workers
Uncontrollable nature of workflowUncontrollable nature of workflow
Declining health status of patient populationsDeclining health status of patient populations
Language barriersLanguage barriers
Limited access to primary and specialty care providersLimited access to primary and specialty care providers
Lack of established relationships between ED staff Lack of established relationships between ED staff and patientsand patients
Source: American College of Emergency Physicians. Patient safety in the emergency department environment report, 2001. Available at: http://www.acep.org.

Patient Safety Risks Unique to Patient Safety Risks Unique to Children in the EDChildren in the ED
Lack of standardized dosing due to broad range Lack of standardized dosing due to broad range in size in size →→ weight-based dosing of medications weight-based dosing of medications
Increased risk for medication errors Increased risk for medication errors (e.g. 10-fold errors)(e.g. 10-fold errors)
Inability of children to communicate complaints or Inability of children to communicate complaints or provide a medical historyprovide a medical history
Children unaccompanied by a parentChildren unaccompanied by a parent
Poor localization of painPoor localization of pain
Limited on-going exposure of many ED care Limited on-going exposure of many ED care providers to ill and injured childrenproviders to ill and injured children
Failure/delay in recognizing critical illness or injuryFailure/delay in recognizing critical illness or injury
Children with special health care needs Children with special health care needs

IOM: Attributes of High Quality CareIOM: Attributes of High Quality Care
Source: Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. Washington, DC: National Academies Press, 2001.

IOM: Patient and Family Centered IOM: Patient and Family Centered Care and Pediatric Emergency CareCare and Pediatric Emergency Care
Failure to incorporate PFCC and culturally Failure to incorporate PFCC and culturally effective care into ED practice “can result in effective care into ED practice “can result in multiple adverse consequences, including multiple adverse consequences, including difficulties with informed consent, difficulties with informed consent, miscommunication, inadequate miscommunication, inadequate understanding of diagnoses and treatment understanding of diagnoses and treatment by families, dissatisfaction with care, by families, dissatisfaction with care, preventable morbidity and mortality, preventable morbidity and mortality, unnecessary child abuse evaluations, lower unnecessary child abuse evaluations, lower quality care, clinician bias, and ethnic quality care, clinician bias, and ethnic disparities in prescriptions, analgesia, test disparities in prescriptions, analgesia, test ordering and diagnostic evaluation”ordering and diagnostic evaluation”
Source: Institute of Medicine. Emergency care for children: growing pains, Washington, DC: National Academies Press, 2006.

AHRQ: 20 Tips to Help Prevent AHRQ: 20 Tips to Help Prevent Medical Errors in ChildrenMedical Errors in Children
#1 - Be an active #1 - Be an active member of member of your child’s your child’s health teamhealth team
Source: Agency for Healthcare Research and Quality. 20 Tips to Help Prevent Medical Errors in Children. Patient Fact Sheet. AHRQ Publication No. 02-P034, 2002. Rockville, MD. Available at: www.ahrq.gov/consumer/20tipkid.htm

Core Principles of Patient- and Core Principles of Patient- and Family-Centered Care (PFCC)Family-Centered Care (PFCC)
Treating patients and families with Treating patients and families with dignity and dignity and respectrespectCommunication and Communication and sharing of unbiased sharing of unbiased informationinformationPatient and family participationPatient and family participation in in experiences that enhance control and experiences that enhance control and independence and build on their strengthsindependence and build on their strengthsCollaborationCollaboration in the delivery of care, policy in the delivery of care, policy and program development, and in professional and program development, and in professional educationeducation
Source: Institute for Family Centered Care. Core principles of family-centered heath care. Advances in Family Centered Care 1998; 4:2-4.

PFCC: Conceptual TransitionsPFCC: Conceptual Transitions
Family deficits Family deficits Family strengths Family strengths
Control Control Collaboration Collaboration
Expert model Expert model Partnerships Partnerships
Information gate-keeping Information gate-keeping Sharing Sharing
Negative support Negative support Positive support Positive support
Rigidity Rigidity Flexibility Flexibility
Patient/family dependence Patient/family dependence Empowerment Empowerment
Source: Emergency Nurses Association. Assessment of family-centered care in the emergency department. 2001. Available at: http://www.ena.org.

AAP & ACEP: PFCC in the EDAAP & ACEP: PFCC in the ED
An innovative approach to health care that An innovative approach to health care that recognizes the integral role of the family and is recognizes the integral role of the family and is grounded in a respectful and mutually beneficial grounded in a respectful and mutually beneficial collaboration among the patient, family, and collaboration among the patient, family, and health care professionals health care professionals PFCC embraces the concepts thatPFCC embraces the concepts that
We are providing care for a person, not a conditionWe are providing care for a person, not a conditionThe patient is best understood in the context of his or The patient is best understood in the context of his or her family, culture, values and goalsher family, culture, values and goalsHonoring the context will result in better health care, Honoring the context will result in better health care, safety, and patient satisfactionsafety, and patient satisfactionTo optimize child’s care, ED providers, parents and To optimize child’s care, ED providers, parents and the child are all on the same teamthe child are all on the same team
Source: AAP Committee on Pediatric Emergency Medicine & ACEP Pediatric Committee. Patient and family centered care and the role of the emergency physician providing care to a child in the emergency department. Pediatrics 2006; 118:2242-4.

ED Challenges to Providing PFCC ED Challenges to Providing PFCC
ED overcrowding and acuityED overcrowding and acuity
Lack of prior relationship with familyLack of prior relationship with family
Previous patient/family experiencesPrevious patient/family experiences
Cultural and social variations among familiesCultural and social variations among families
Language barriers and health literacy concernsLanguage barriers and health literacy concerns
Patient arrival to ED without parent/familyPatient arrival to ED without parent/family
Unaccompanied minor seeking careUnaccompanied minor seeking care
Visits related to child abuse and neglectVisits related to child abuse and neglect
Resuscitation and other urgent interventionsResuscitation and other urgent interventions
Unanticipated death of a child in the EDUnanticipated death of a child in the ED

Opportunities for PFCC in the EDOpportunities for PFCC in the ED
Family presence throughout ED careFamily presence throughout ED careDuring clinical decision-making and teaching During clinical decision-making and teaching During invasive proceduresDuring invasive proceduresDisposition and discharge planningDisposition and discharge planning
Linkage to the medical homeLinkage to the medical home
Comfort careComfort careCulturally effective careCulturally effective careLanguage translation supportLanguage translation supportChild life & social servicesChild life & social servicesED physical plant designED physical plant designPatient and family input into ED policiesPatient and family input into ED policies

Family Presence During Invasive Family Presence During Invasive Procedures and ResuscitationProcedures and Resuscitation
Literature base consists primarily of Literature base consists primarily of surveys of provider beliefs & practicessurveys of provider beliefs & practices
60 to 80% of families believe they want to be 60 to 80% of families believe they want to be present during ED carepresent during ED care
Providers are somewhat less supportiveProviders are somewhat less supportiveRNs generally more supportive than MDsRNs generally more supportive than MDsSenior MDs more supportive than traineesSenior MDs more supportive than traineesSupport decreases with increasing acuity Support decreases with increasing acuity and/or intensity of the procedureand/or intensity of the procedure
Source: Eppich WJ, Arnold LD. Family member presence in the pediatric emergency department. Current Opinion in Pediatrics 2003; 15:294-8.

FP: What Do ED Providers BelieveFP: What Do ED Providers Believe
A frequently offered concern by healthcare A frequently offered concern by healthcare providers is that family presence (FP) may providers is that family presence (FP) may result in a delay or disruption of careresult in a delay or disruption of care
Reports of FP trials in EDs have not Reports of FP trials in EDs have not demonstrated this to be a significant concerndemonstrated this to be a significant concern
Oddly enough, healthcare providers who Oddly enough, healthcare providers who initially oppose FP commonly become initially oppose FP commonly become fierce advocates after trying itfierce advocates after trying it

Proponents for Family PresenceProponents for Family PresenceAmerican Heart AssociationAmerican Heart AssociationAmerican Academy of PediatricsAmerican Academy of PediatricsAmbulatory Pediatric AssociationAmbulatory Pediatric AssociationEmergency Nurses Association*Emergency Nurses Association*Emergency Medical Services for ChildrenEmergency Medical Services for Children11
Published guidelines/coursesPublished guidelines/coursesEMSC FCC Guidelines (2000)EMSC FCC Guidelines (2000)AHA CPR Guidelines (2000, 2005)AHA CPR Guidelines (2000, 2005)Pediatric Advanced Life Support (2002)Pediatric Advanced Life Support (2002)Advanced Pediatric Life Support (2004)Advanced Pediatric Life Support (2004)Emergency Nursing Pediatric Course (2004)Emergency Nursing Pediatric Course (2004)Trauma Nursing Core Course (2002)Trauma Nursing Core Course (2002)
(1) Emergency Medical Services for Children. Guidelines for providing family-centered care. 2000.

FP: Reported Benefits for FamilyFP: Reported Benefits for Family
Continued patient-family bonding and Continued patient-family bonding and connectednessconnectednessFacilitation of the grieving processFacilitation of the grieving processSense of closure on a life shared togetherSense of closure on a life shared togetherRemoval of doubt about what was happening to Removal of doubt about what was happening to the patient and the knowledge that everything the patient and the knowledge that everything possible was being donepossible was being doneA spiritual experienceA spiritual experienceFeeling that they had been supportive and Feeling that they had been supportive and helpful to the patienthelpful to the patientReduced fear and anxietyReduced fear and anxiety
Source: Guzzetta CE, Clark AP, Wright JL. Family presence in emergency medical services for children. Clinical Pediatric Emergency Medicine 2006; 7:15-24.

FP: Benefits for Care ProvidersFP: Benefits for Care Providers
Improved clinical-decision makingImproved clinical-decision makingImproved clinical efficiency/ED patient through-putImproved clinical efficiency/ED patient through-put
Greater satisfaction with workplace environmentGreater satisfaction with workplace environmentImproved patient satisfaction Improved patient satisfaction Lower burn-out/turnoverLower burn-out/turnover
Improved understanding of social, ethnic and Improved understanding of social, ethnic and cultural diversity cultural diversity Improved awareness of children with special Improved awareness of children with special healthcare needshealthcare needsReductions in medical error and liability riskReductions in medical error and liability risk
Are we more careful or deliberate with FP ?Are we more careful or deliberate with FP ?Are we better informed abut our patients?Are we better informed abut our patients?
This may be especially valuable for special needs childrenThis may be especially valuable for special needs children

The Swiss Cheese ModelThe Swiss Cheese Model
Model for accident causation Model for accident causation used in risk analysis used in risk analysis Views human systems as Views human systems as successive layers of “cheese” successive layers of “cheese” or defenses against erroror defenses against error
Redundancy helps prevent errorsRedundancy helps prevent errorsHoles represent defense weaknessHoles represent defense weakness
Some hazards manage to find Some hazards manage to find the holes and bypass these the holes and bypass these defenses, resulting in lossesdefenses, resulting in lossesIs PFCC another “slice of Is PFCC another “slice of cheese” or defense against cheese” or defense against medical errors ?medical errors ?
Source: Reason JT. Human Error. Cambridge University Press, 1990

Culturally Effective CareCulturally Effective Care
Delivery of care within the context of Delivery of care within the context of appropriate physician knowledge, appropriate physician knowledge, understanding, and appreciation of all understanding, and appreciation of all cultural distinctions leading to optimal cultural distinctions leading to optimal health outcomeshealth outcomes
Requires the acquisition of knowledge, development Requires the acquisition of knowledge, development of skills, and demonstration of behaviors and attitudes of skills, and demonstration of behaviors and attitudes that are appropriate to care for patients and families that are appropriate to care for patients and families from a wide variety of cultural attitudesfrom a wide variety of cultural attitudes
AKA “cultural competency” & “cultural sensitivity”AKA “cultural competency” & “cultural sensitivity”
Source: AAP Committee on Pediatric Workforce. Ensuring culturally effective pediatric care: implications for education and health policy. Pediatrics 2004; 114:1677-85.

ED Communication ConcernsED Communication Concerns
Language translationLanguage translationInterpretationInterpretation
Cultural variations in Cultural variations in verbal and non-verbal verbal and non-verbal communicationcommunication
Communication Communication anxiety anxiety
““Imbalance of power”Imbalance of power”
Health literacyHealth literacy Performance of a Lifetime

Health Literacy: The Silent EpidemicHealth Literacy: The Silent Epidemic
DefinitionDefinition: Health literacy is the degree to : Health literacy is the degree to which individuals have the capacity to which individuals have the capacity to obtain, process, and understand basic obtain, process, and understand basic health information and services needed health information and services needed to make appropriate health decisions to make appropriate health decisions
21% of the American Public cannot read the 21% of the American Public cannot read the headlines of a newspaperheadlines of a newspaper48% cannot decipher messages with words 48% cannot decipher messages with words and numbers, i.e. instructions about a bus and numbers, i.e. instructions about a bus routeroute
Source: Institute of Medicine. Health literacy: a prescription to end confusion. Source: Institute of Medicine. Health literacy: a prescription to end confusion. Washington, DC: National Academies Press, 2004Washington, DC: National Academies Press, 2004

Health Literacy: A Barrier to PFCCHealth Literacy: A Barrier to PFCC
How many patients understand what we tell them How many patients understand what we tell them or give them to read? or give them to read?
About 52%, according to researchAbout 52%, according to research
How do we know parents understand discharge How do we know parents understand discharge instructions instructions
We often don’tWe often don’tParents/patients are quite ashamed of low literacy and Parents/patients are quite ashamed of low literacy and they are very good at hiding the problem they are very good at hiding the problem
Asking “Asking “Do you understand what we’ve talked about?”Do you understand what we’ve talked about?” won’t won’t get you very farget you very far
We need to hear it in their wordsWe need to hear it in their wordsThere is a big difference between asking There is a big difference between asking “Do you understand”“Do you understand” and and “Take a minute and tell me what we’ve talked about”“Take a minute and tell me what we’ve talked about”

Comfort Care & ED Physical PlantComfort Care & ED Physical Plant

Future Directions in PFCCFuture Directions in PFCC
EducationEducationPost-graduate Post-graduate
Trainee levelTrainee level
Patients and Patients and familiesfamilies
Advocacy and Advocacy and leadershipleadership
Research !!Research !!

EBM Review of PFCC for ChildrenEBM Review of PFCC for Children
Cochrane review of literature assessing the Cochrane review of literature assessing the effects of PFCC models of care on the effects of PFCC models of care on the outcomes of hospitalized childrenoutcomes of hospitalized childrenStudy methods – literature search for RCTs, Study methods – literature search for RCTs, CCTs, etc comparing PFCC to other modelsCCTs, etc comparing PFCC to other modelsStudy results – Study results – nono studies met inclusion studies met inclusion criteria – no analysis could be performedcriteria – no analysis could be performedThis review highlights the dearth of high This review highlights the dearth of high quality quantitative research on PFCCquality quantitative research on PFCC
Source: Pratt SL, Davis LM, Hunter J. Family centered care for children in the Hospital. Cochrane Database of Systematic Reviews, 2007.

One Example: PFCC Bedside RoundsOne Example: PFCC Bedside Rounds
Recommended in Recommended in AAP/IFCC policy AAP/IFCC policy statement (2003)statement (2003)
Piloted on an inpatient Piloted on an inpatient unit at CCHMCunit at CCHMC
RWJF RWJF Pursuing PerfectionPursuing Perfection
IssuesIssuesTeachingTeaching
TimeTime
ConfidentialityConfidentiality
Source: Muething SE, Kotagal UR, et al. Family-centered bedside rounds: a new approach to patient care and teaching. Pediatrics 2007; 119:829-32.

ED Patient Safety ResourcesED Patient Safety ResourcesFrush KS, Krug SE, AAP COPEM: Patient safety in the Frush KS, Krug SE, AAP COPEM: Patient safety in the pediatric emergency care setting. (in press) pediatric emergency care setting. (in press) – Look for this policy statement in Pediatrics !Look for this policy statement in Pediatrics !
IOM Committee on the Future of Emergency Services in the IOM Committee on the Future of Emergency Services in the US Healthcare System: US Healthcare System: Emergency care for children: growing pains. Washington, DC: National Academies Press, 2006.Institute of Medicine. Crossing the quality chasm. A new Institute of Medicine. Crossing the quality chasm. A new health system for the 21st centuryhealth system for the 21st century.. Washington, DC: National Washington, DC: National Academies Press, 2001.Academies Press, 2001.Frush KS, Hohenhaus SM (eds). Patient safety in pediatric Frush KS, Hohenhaus SM (eds). Patient safety in pediatric emergency medicine. Clinical Pediatric Emergency Medicine emergency medicine. Clinical Pediatric Emergency Medicine 2007; 7:213-75.2007; 7:213-75.American Academy of Pediatrics: www.aap.orgEmergency Nurses Association: www.ena.orgInstitute for Healthcare Improvement: www.ihi.orgJoint Commission on Accreditation of Healthcare Joint Commission on Accreditation of Healthcare Organizations: Organizations: www.jointcommission.orgwww.jointcommission.org

PFCC ResourcesPFCC ResourcesO’Malley P, AAP Committee on Pediatric Emergency Medicine, ACEP Pediatric Committee. Patient and family centered care and the role of the emergency physician providing care to a child in the emergency department. Pediatrics 2006; 118:2242-4. – Look for the companion Technical Report -- to be published soon !
AAP Committee on Hospital Care. Family-centered care and the pediatrician’s role. Pediatrics 2003; 112:691-6.Guzzetta CE, Clark AP, Wright JL. Family presence in emergency medical services for children. Clinical Pediatric Emergency Medicine 2006; 7:15-24.Henderson DP, Knapp JF. Report of the national consensus conference on family presence during pediatric cardiopulmonary resuscitation and procedures. Journal of Emergency Nursing 2006; 32:23-9.American Academy of Pediatrics: American Academy of Pediatrics: www.aap.orgwww.aap.orgEmergency Medical Services for Children: Emergency Medical Services for Children: //bolivia.hrsa.gov/emsc///bolivia.hrsa.gov/emsc/Emergency Nurses Association: Emergency Nurses Association: www.ena.org www.ena.orgInstitute for Family-Centered Care: Institute for Family-Centered Care: www.familycenteredcare.orgwww.familycenteredcare.org


Family Centered CareFamily Centered CareChildren with Special Health Children with Special Health
Care Needs and Patient Care Needs and Patient SafetySafety
Safer Health Care for KidsSafer Health Care for Kids
John Neff MDJohn Neff MDCenter for Children with Special NeedsCenter for Children with Special NeedsChildren’s Hospital and Regional Medical CenterChildren’s Hospital and Regional Medical CenterSeattle, WashingtonSeattle, Washington

ObjectivesObjectives Gain an Understanding of the:Gain an Understanding of the:
Relationship between Families of Children with Special Relationship between Families of Children with Special Needs and their Children’s SafetyNeeds and their Children’s Safety
The Importance of Providing Family Centered Care (FCC) The Importance of Providing Family Centered Care (FCC) for Children with Special Health Care Needs (CSHCN)for Children with Special Health Care Needs (CSHCN)
The Unique Differences between Mother’s and Father’s in The Unique Differences between Mother’s and Father’s in Relation to Safety IssuesRelation to Safety Issues
Understand the Specific Home and Hospital Safety Issues Understand the Specific Home and Hospital Safety Issues of CSHCNof CSHCN

Relationship between Families of Relationship between Families of Children with Special NeedsChildren with Special Needs and their Children’s Safety and their Children’s Safety
Families know their child best and their Families know their child best and their child’s strengths and limitationchild’s strengths and limitation
Families know the developmental and Families know the developmental and physical challenges that their child has physical challenges that their child has better than any specific care giverbetter than any specific care giver

Relationship between Families of Relationship between Families of Children with Special NeedsChildren with Special Needs and their Children’s Safety and their Children’s Safety
Practitioners know medical and therapeutic Practitioners know medical and therapeutic needs and related safety issues that should needs and related safety issues that should be shared with families as partnersbe shared with families as partners
Safety must be a shared effort by both Safety must be a shared effort by both practitioners and familiespractitioners and families

The Importance of Providing The Importance of Providing FCC for CSHCNFCC for CSHCN
Families are the protectors of the childFamilies are the protectors of the child
Families have aspirations that their child will Families have aspirations that their child will reach his or her maximum level of achievement reach his or her maximum level of achievement and pleasure through play and interaction with and pleasure through play and interaction with othersothers
Families expect that their child will continue to Families expect that their child will continue to develop at his or her own pacedevelop at his or her own pace

Differences between the Mother’s Differences between the Mother’s and Father’s Role in FCCand Father’s Role in FCC
(generalities)(generalities)MothersMothers tend to be the ones who interact most tend to be the ones who interact most with health professionalswith health professionals
MothersMothers are the organizers of the health plan are the organizers of the health plan
MothersMothers tend to be the protectors tend to be the protectors
FathersFathers are expected to be the providers are expected to be the providers
FathersFathers have a special interest in play activities have a special interest in play activities as the child develops; they encourage risk takingas the child develops; they encourage risk taking
FathersFathers take special pride in child’s development take special pride in child’s development
FathersFathers sometimes feel or are left out of FCC sometimes feel or are left out of FCC

Important to Involve and Important to Involve and Empower both Parents Equally Empower both Parents Equally in Safety Issues for the Child in Safety Issues for the Child
with Special Health Care Needswith Special Health Care Needs

Families should take the Lead Families should take the Lead on Safety Issues with on Safety Issues with
Appropriate Professional Appropriate Professional GuidanceGuidance

Practitioners Role is to CoordinatePractitioners Role is to Coordinate Family Centered Care Family Centered Care
Understand Specific Safety Understand Specific Safety Concerns and Guidelines for the Concerns and Guidelines for the
Child Child
Obtain Input from Child’s Specialty Obtain Input from Child’s Specialty ProvidersProviders

Family Centered Care is more Family Centered Care is more Difficult to Accomplish Difficult to Accomplish
but just as but just as Important for non-English Important for non-English
Speaking Families Speaking Families

Definition of Children with Definition of Children with Special Health Care NeedsSpecial Health Care Needs

Maternal Child Health Bureau 1990Maternal Child Health Bureau 1990Definition of Children Definition of Children
with Special Health Care Needs (CSHCN) with Special Health Care Needs (CSHCN)
Those children who have or are at an Those children who have or are at an increased risk for a chronic increased risk for a chronic
physical, developmental, behavioralphysical, developmental, behavioral or emotional conditionor emotional condition and who require and who require
health and related services of a type health and related services of a type or amount beyond that required by or amount beyond that required by
children generallychildren generally

General ConsiderationGeneral Consideration of Safety Issues of Safety Issues
Physical ConditionsPhysical Conditions – Issues: mobility, weaknesses – Issues: mobility, weaknesses and strengths, challenges around specific conditionsand strengths, challenges around specific conditionsDevelopmental ConditionsDevelopmental Conditions – Issues: developmental – Issues: developmental stages and cognitive abilitiesstages and cognitive abilitiesBehavioral / Emotional ConditionsBehavioral / Emotional Conditions – Issues: fears and – Issues: fears and anxieties, judgmental abilities and emotional stabilityanxieties, judgmental abilities and emotional stabilityTechnology DependenceTechnology Dependence – Issues: mobility devices, – Issues: mobility devices, I.V. lines, respiratory support , medications, nutritional I.V. lines, respiratory support , medications, nutritional formulasformulasCombination of ConditionsCombination of Conditions – Issues: all of the above – Issues: all of the above as appropriateas appropriate

Medical CareMedical CareAssumptionsAssumptions
Parents and their primary care providers in Parents and their primary care providers in the medical home will know the child the medical home will know the child better than the hospital teambetter than the hospital team
Primary care providers can help by Primary care providers can help by empowering both parents to be advocates empowering both parents to be advocates for their child and by informing the hospital for their child and by informing the hospital team that the families are knowledgeableteam that the families are knowledgeable
about their child’s needs about their child’s needs

Hospital / MedicalHospital / MedicalPreparationPreparation
Parents can work out with their medical home Parents can work out with their medical home providers to develop a care note book with providers to develop a care note book with specific items that will make a hospital specific items that will make a hospital experience safer (preferably electronic format) experience safer (preferably electronic format)
Parents can bring this care note book to the Parents can bring this care note book to the hospital and be sure that the admitting hospital and be sure that the admitting physicians see it, are familiar with the child and physicians see it, are familiar with the child and incorporate the material into hospital records incorporate the material into hospital records and orders.and orders.

Specific IssuesSpecific IssuesHospital Hospital (Home)(Home) Medical Care Medical Care
Medications, dosages and routes of admin.Medications, dosages and routes of admin.Formulas and NutritionFormulas and NutritionIntravenous linesIntravenous linesEquipment useEquipment useInfectionsInfectionsSkin care and hygienic practicesSkin care and hygienic practicesSpecial emotional, developmental and Special emotional, developmental and physical needsphysical needsPain and sedationPain and sedation

Contents of Care Note BookContents of Care Note Book
List of medications, dosages, side effects List of medications, dosages, side effects and reasons for useand reasons for use
Equipment information and how it has Equipment information and how it has been adapted for the childbeen adapted for the child
Specifics recommendations about child’s Specifics recommendations about child’s vulnerabilities and needs (such as skin, vulnerabilities and needs (such as skin, GU, bones, emotional, cognitive, allergies)GU, bones, emotional, cognitive, allergies)
Nutritional requirementsNutritional requirements

Hospital / Medical TeamHospital / Medical Team
Consider the family to be an integral Consider the family to be an integral member of the medical teammember of the medical team
Incorporate their concerns and specific Incorporate their concerns and specific recommendation on how best to provide recommendation on how best to provide carecare
Interpreters should be available for Interpreters should be available for families whose primary language is not families whose primary language is not English, English,
Hospital / Medical TeamHospital / Medical Team
Parents can serve as helpful monitors on the care Parents can serve as helpful monitors on the care the child is receiving in the hospitalthe child is receiving in the hospital
Observe hand washing and other measures to Observe hand washing and other measures to prevent nosocomial infectionprevent nosocomial infectionCheck medication dosages and ask questions Check medication dosages and ask questions when treatment measures are not clear to themwhen treatment measures are not clear to themSpeak up about concernsSpeak up about concernsInform staff about special vulnerabilities and Inform staff about special vulnerabilities and pleasures of the childpleasures of the child
Nutritional and Oral Concerns Nutritional and Oral Concerns
Use appropriate foods and position for Use appropriate foods and position for CSHCNCSHCN
Know about formula contents Know about formula contents
CSHCN should generally eat at a table CSHCN should generally eat at a table and not be walking around when eatingand not be walking around when eating
Be aware of common small items that Be aware of common small items that should be kept away from childshould be kept away from child

Equipment and Electrical SafetyEquipment and Electrical Safety
Be aware of safety needs of the Be aware of safety needs of the equipment for the CSHCNequipment for the CSHCN
Special attention to electrical overload, Special attention to electrical overload, fires and other electrical accidentsfires and other electrical accidents
Follow carefully recommendations in Follow carefully recommendations in owner’s manualsowner’s manuals

Environment HomeEnvironment Home
Be sure that the child is appropriately supervisedBe sure that the child is appropriately supervisedAlways be sure that water temperature is appropriate for Always be sure that water temperature is appropriate for childchildBe sure that your local Fire Department knows about the Be sure that your local Fire Department knows about the special circumstances of your CSHCNspecial circumstances of your CSHCNHave available a special bag with medicinesHave available a special bag with medicinesDevelop an alarm system that the CSHCN can useDevelop an alarm system that the CSHCN can useKeep material near child to assist in escapeKeep material near child to assist in escape

Positive vs Negative ReinforcementPositive vs Negative Reinforcement
When we emphasize a safe environment it When we emphasize a safe environment it is often a list of negativesis often a list of negatives
Develop positive ways that we can Develop positive ways that we can encourage safe behavior for CSHCN that encourage safe behavior for CSHCN that encourages development of skills, encourages development of skills, teamwork, and appropriate and risks teamwork, and appropriate and risks

Follow up with FamilyFollow up with Family
ObservationsObservations
SuccessesSuccesses
New ConcernsNew Concerns
SuggestionsSuggestions (Use Check List for Guidance)(Use Check List for Guidance)

SummarySummary
Allow families to take the lead on safety planning Allow families to take the lead on safety planning for their child with as much attention to father’s for their child with as much attention to father’s issues as well as the mother'sissues as well as the mother'sProvide professional guidance and updated Provide professional guidance and updated safety information concerning the child’s specific safety information concerning the child’s specific conditionsconditionsInclude safety planning as part of the care Include safety planning as part of the care coordination processcoordination processEncourage the do’s as well as the don’ts when Encourage the do’s as well as the don’ts when providing information and adviceproviding information and advice

ResourcesResources
Safety Tips for Children with Special NeedsSafety Tips for Children with Special Needs: : www.cshcn.org/resources/infoanded.cfm#siwww.cshcn.org/resources/infoanded.cfm#si
Emergency Preparedness for Special NeedsEmergency Preparedness for Special Needs--American Red Cross: American Red Cross: www.prepare.org/disabilities/disabilities.htmwww.prepare.org/disabilities/disabilities.htm
Wheelchair Safety in VehiclesWheelchair Safety in Vehicles -University of Michigan -University of Michigan Transportation Research Institute: Transportation Research Institute: www.travelsafer.orgwww.travelsafer.org
Adapted Bicycle Products for Special NeedsAdapted Bicycle Products for Special Needs: : www.rileyhospital.org/document.jsp?locid=1416www.rileyhospital.org/document.jsp?locid=1416
Playground Safety for Children with Special NeedsPlayground Safety for Children with Special Needs::
www.cshcn.org/forms/PlaygroundSafety_English.pdfwww.cshcn.org/forms/PlaygroundSafety_English.pdf

Now What?!?Now What?!?Some take-away points from the Some take-away points from the
Webinar:Webinar:
Family-Centered Care (FCC) Family-Centered Care (FCC) and Patient Safetyand Patient Safety
June 21, 2007June 21, 2007

TAKE-AWAY POINTSTAKE-AWAY POINTSSteven E. Krug, MD, FAAPSteven E. Krug, MD, FAAP
PFCC has become recognized as the standard of PFCC has become recognized as the standard of practice resulting in high quality and practice resulting in high quality and safesafe care care– Requires a paradigm shift from traditional care modelsRequires a paradigm shift from traditional care models
Families should be present during the entire course Families should be present during the entire course of ED care, including procedures and teachingof ED care, including procedures and teaching– This practice will benefit patients, families and providers This practice will benefit patients, families and providers
Culturally effective care is an essential component Culturally effective care is an essential component of PFCC in all settingsof PFCC in all settings– Timely access to interpreter services is required Timely access to interpreter services is required
Health literacy represents a barrier to effective Health literacy represents a barrier to effective communication, patient safety and PFCCcommunication, patient safety and PFCC– We need to assure that patient families really understandWe need to assure that patient families really understand

TAKE-AWAY POINTSTAKE-AWAY POINTSJohn M. Neff, MD, FAAPJohn M. Neff, MD, FAAP
Involve families in hospital safety issuesInvolve families in hospital safety issues
Provide families with information and Provide families with information and empower them to be part of the teamempower them to be part of the team
Encourage families to develop and Encourage families to develop and maintain a transportable care note book maintain a transportable care note book that has child’s current health planthat has child’s current health plan
Make a special effort to include non Make a special effort to include non English speaking families in FCCEnglish speaking families in FCC

Care Note Book
Visit: http://www.cshcn.org/resources/carecoordination.cfm


















