Experience with 500 Stentless Aortic Valve Replacements · 2020. 12. 24. · Experience with 500...
36
Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine
Transcript of Experience with 500 Stentless Aortic Valve Replacements · 2020. 12. 24. · Experience with 500...
-
Experience with 500 Stentless Aortic Valve Replacements
Dimitrios C. Iliopoulos, MD
Cardiac Surgeon
Ass. Professor of Surgery
University of Athens, School of Medicine
-
I declare no conflict of interest
-
Burden of Valve Disease in the US
Year 2000 ➔ 2030
Disease
AS 2.5 millions ➔ 4.6 millions MR 2.7 millions ➔ 4.8 millions
-
Stentless Aortic Valves Ideal for:
• Patients > 60 years old
• Patients < 60 years old with ↑ risk of thromboembolism
• Small annulus
• Concomittant procedures (↓ cross – clamp time)
-
Freedom SOLO • Superior haemodynamics
• Faster to implant (one suture line)
• Maximization of flow in small annuli
• Outflow side already scalloped
• May avoid annulus enlargement
• No fabric reinforcement
• Soft and pliable tissue
• Detoxified valve and ready for use
• Expected reduction of calcification
• Clinically proven design
(18 yrs of Pericarbon stented model and
10 yrs of stentless) Native at Heart
-
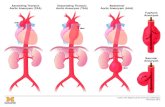
Different Implant Techniques
Outflow suture line
-
Freedom SOLO: Technique
Supra-Annular
• No material within the annulus
• 100% orifice-to-annulus ratio
-
Implant Technique: Suturing
Suggested order
• Each suture is tied at the midpoint
• Running suture from the midpoint to the top of the post, taking large bites
-
Implant Technique: Suturing
• Once at the top, each suture is passed through the patient aortic wall
• Adjacent sutures are then tied
-
Our published initial experience…
128 patients
-
Protocol
500 patients undergoing AVR with SOLO Freedom aortic valve ± Concomitant procedures
U/S: preoperatively, immediate – 3 months – 6 months – 12 months postoperatively
Mean follow up: 57 months
-
Patient Demographics
Age (y) 78.5±4.4
Gender (M:F) 271:229
BSA, mean±SD 1.8±0.17
NYHA, mean±SD 2.3±0.8
I-II, n(%) 379 (76)
III-IV, n(%) 121 (24)
Euroscore II, mean±SD 9.04±2.7
High Euroscore Patients, n(%) 410 (82)
-
AV Pathology: Stenosis
3%
24%
73%
Mild
Moderate
Severe
-
Valves Pathology
Aortic Valve (%) Mitral Valve (%)
AV Regurgitation 21.1 MV Stenosis 9
Mixed Lesion 18.2
MV
Regurgitation 48.5
BAV 2.7 Mixed Lesion 3
Endocarditis 3
-
Risk factors
Comorbidities (%)
CAD 45.5
Hypertension 75.8
DM 42.2
Renal dysfunction 12.1
Dyslipidemia 36.4
Pulmonary hypertension 12.1
AFib 27.3
Previous Cardiac Surgery (%)
CABG 6
AVR 6
-
Pre-op Medication Drug Treatment (%)
Beta Blockers 73
ACE Inhibitors 39
AT Inhibitors 12
Diuretics 55
Digoxin 6
Calcium Channel Blockers
6
Statins 27
ASA 24
Clopidogrel 12
Coumadin 18
-
Laboratory Work-up
Pre-op Work-up, mean±SD
Hemoglobin 12.4 ± 1.7 HCT 38.3 ± 5 RBC 4471562 ± 726933 PLT 200250 ± 50211
Post-op Work-up, mean±SD
min Hgb 9.2 ± 0.9 min HCT 27.9 ± 2.9 min RBC 3215312 ± 378519 min PLT 65219 ± 31322 Post-op Day 3.7 ± 1.4
Significantly lower in all cases
-
Size of prosthesis
0
10
20
30
40
50
60
70
80
21mm 23mm 25mm 27mm
SOLO Freedom
-
Intra-operative data
Transfusion, mean±SD FFP 3.9 ± 2 RBC 2.8 ± 1.6 PLT 2.9 ± 3.8
Cross-clamp time (min), mean±SD 89 ± 30 CBP time (min), mean±SD 121 ± 38 SOLO time (min), mean±SD 42.7 ± 12.4
Concomitant Operation, (%) CABG 30 MVR 21 Other 18
Solely AVR only in the 40% of the patients !!
-
Post-operative data
ICU Stay (h), mean±SD 68 ± 17 Hospital Stay (d), mean±SD 8.3±2.7
In-hospital mortality (%) 4.2 Time to death (d), mean±SD 7.2±11.2 Cause of death, % Cardiogenic shock 33 Bleeding 33 Infection 33 Re-operation (%) 2 Reason for re-op (%) Bleeding 100
All patients had high Euroscore II
-
U/S Data
Preoperative Postoperative 3m 6m 12m p-value
LVEDD (mm) 51.2 ± 8.23 48.4 ± 5.8 47.3 ± 7.5 46.3 ± 6.4 45.5 ± 7.9 ns
LVESD (mm) 34.3 ± 7.9 32.4 ± 8.2 31.1 ± 8.2 30.3 ± 5.8 30.1 ± 8.7 ns
IVS(mm) 12.3 ± 2.1 12.4 ± 1.9 10.3 ± 1.3 10.4 ± 1.5 10.1 ± 1.3
-
0
10
20
30
40
50
60
Preoperative Postoperative 3m 6m 12m
LV End-diastolic Diameter (mm)
-
0
5
10
15
20
25
30
35
40
45
Preoperative Postoperative 3m 6m 12m
LV End-systolic Diameter (mm)
-
0
2
4
6
8
10
12
14
Preoperative Postoperative 3m 6m 12m
Intra-ventricular Septum (mm)
p
-
0
2
4
6
8
10
12
14
Preoperative Postoperative 3m 6m 12m
Posterior Wall (mm)
-
0
20
40
60
80
100
120
Preoperative Postoperative 3m 6m 12m
Peak Gradient (mmHg)
p
-
0
10
20
30
40
50
60
70
Preoperative Postoperative 3m 6m 12m
Mean Gradient (mmHg)
p
-
0
1
2
3
4
5
6
Preoperative Postoperative 3m 6m 12m
Peak Velocity (cm/sec)
p
-
Post-op AV Regurgitation
Postoperative 3 months 6 months 12 months
Relative frequency (%)
1,6 2,2 1 1
Mean Grade
1 1 1 1
Type Left Sinus Of Valsalva
Left Sinus of Valsalva –
Paravalvular
Left Sinus Of Valsalva
Left Sinus Of Valsalva
-
Kaplan-Meier Analysis
-
Mortality Hazard
-
Surgical tips for easy implantation
Use 4-0 for thick or 5-0 prolene for thin aortic wall Oversize the aortic root (1 or 2 size bigger) Do not hesitate to stabilize the valve with external pledgeted sutures (especially
after local decalcification) Do not hesitate to implant in calcified roots (local decalcification) 1-2 mm higher in non-coronary sinus to avoid prosthetic aortic valve replacement
insufficiency Be flexible:
no one root is perfectly symmetrical modify the implantation
-
Take-home message
Easy and fast implantation
Ideal for small annulus
Excellent Hemodynamics
Earlier Left Ventricular Reverse Remodelling
-
Thank you !