
Expansion/Facemask Treatment of an Adult Class III ... · Expansion/Facemask Treatment of an Adult...
7
Case Report Expansion/Facemask Treatment of an Adult Class III Malocclusion Gregory W. Jackson 1 and Neal D. Kravitz 2 Department of Orthodontics (M/C ), College of Dentistry, University of Illinois at Chicago, S. Paulina Street, Chicago, IL , USA Riding Plaza, No. , South Riding, VA , USA Correspondence should be addressed to Gregory W. Jackson; [email protected] Received December ; Accepted January ; Published February Academic Editors: M. H. K. Motamedi and H. Oktay Copyright © G. W. Jackson and N. D. Kravitz. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. e orthodontic treatment of class III malocclusion with a maxillary deciency is oen treated with maxillary protraction with or without expansion. Skeletal and dental changes have been documented which have combined for the protraction of the maxilla and the correction of the class III malocclusion. Concerning the ideal time to treat a developing class III malocclusion, studies have reported that, although early treatment may be the most eective, face mask therapy can provide a viable option for older children as well. But what about young adults? Can the skeletal and dental changes seen in expansion/facemask therapy in children and adolescents be demonstrated in this age group as well, possibly eliminating the need for orthodontic dental camouage treatment or orthognathic surgery? A case report is presented of an adult class III malocclusion with a Class III skeletal pattern and maxillary retrusion. Treatment was with nonextraction, comprehensive edgewise mechanics with slow maxillary expansion with a bonded expander and protraction facemask. 1. Introduction e orthodontic treatment of Class III malocclusion with a maxillary deciency is oen treated with maxillary pro- traction either with or without maxillary expansion [–]. Studies on both humans and experimental animals have demonstrated the orthopedic advancement of the maxilla. ese studies have shown that a signicant component of skeletal class III malocclusion includes maxillary retrusion in combination with a normal or mildly prognathic mandible [–]. Skeletal and dental changes have been documented in these studies which have combined for the protraction of the maxilla and the correction of the class III malocclusion. Is there an ideal time to treat a developing class III maloc- clusion? Just a few studies have examined the eect of age on maxillary protraction therapy. Takada et al. [] examined Japanese female patients with class III malocclusion, divided into three groups ( to years, to years, and to years). ey concluded that a greater orthopedic eect was observed when therapy was applied before or during the pubertal growth spurt ( to years). Baik [] studied maxillary expansion and protraction in Korean subjects, divided into three groups (< years, to years, and years or older). He concluded that age did not show any statistically signicant dierence in treatment eects of expansion/facemask therapy. Braun [] studied subjects aged – and found that expansion/facemask therapy pro- duces dentofacial changes that combine to improve class III malocclusion. ey reported that, although early treatment may be the most eective, facemask therapy can provide a viable option for older children as well. But what about young adults? Can the skeletal and dental changes seen in expansion/facemask therapy in children and adolescents be demonstrated in this age group as well, possibly eliminating the need for orthodontic dental camouage treatment or orthognathic surgery? 2. Case Report A -year- -month-old Caucasian female presented with a chief complaint of “I do not like my underbite.” Her medical Hindawi Publishing Corporation Case Reports in Dentistry Volume 2014, Article ID 270257, 6 pages http://dx.doi.org/10.1155/2014/270257
Transcript of Expansion/Facemask Treatment of an Adult Class III ... · Expansion/Facemask Treatment of an Adult...

Case ReportExpansion/Facemask Treatment of an AdultClass III Malocclusion
Gregory W. Jackson1 and Neal D. Kravitz2
! Department of Orthodontics (M/C "#!), College of Dentistry, University of Illinois at Chicago,"$! S. Paulina Street, Chicago, IL %$%!&, USA
& &'$'' Riding Plaza, No. !!$, South Riding, VA &$!'&, USA
Correspondence should be addressed to Gregory W. Jackson; [email protected]
Received !" December !#$%; Accepted $& January !#$'; Published $( February !#$'
Academic Editors: M. H. K. Motamedi and H. Oktay
Copyright © !#$' G. W. Jackson and N. D. Kravitz. )is is an open access article distributed under the Creative CommonsAttribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work isproperly cited.
)e orthodontic treatment of class III malocclusion with a maxillary de*ciency is o+en treated with maxillary protraction with orwithout expansion. Skeletal and dental changes have been documented which have combined for the protraction of the maxillaand the correction of the class III malocclusion. Concerning the ideal time to treat a developing class III malocclusion, studies havereported that, although early treatment may be the most e,ective, face mask therapy can provide a viable option for older childrenas well. But what about young adults? Can the skeletal and dental changes seen in expansion/facemask therapy in children andadolescents be demonstrated in this age group as well, possibly eliminating the need for orthodontic dental camou-age treatmentor orthognathic surgery? A case report is presented of an adult class III malocclusion with a Class III skeletal pattern and maxillaryretrusion. Treatment was with nonextraction, comprehensive edgewise mechanics with slow maxillary expansion with a bondedexpander and protraction facemask.
1. Introduction
)e orthodontic treatment of Class III malocclusion witha maxillary de*ciency is o+en treated with maxillary pro-traction either with or without maxillary expansion [$–'].Studies on both humans and experimental animals havedemonstrated the orthopedic advancement of the maxilla.)ese studies have shown that a signi*cant component ofskeletal class III malocclusion includes maxillary retrusion incombination with a normal or mildly prognathic mandible[.–$"]. Skeletal and dental changes have been documentedin these studies which have combined for the protraction ofthe maxilla and the correction of the class III malocclusion.Is there an ideal time to treat a developing class III maloc-clusion? Just a few studies have examined the e,ect of age onmaxillary protraction therapy. Takada et al. [(] examined &$Japanese female patients with class III malocclusion, dividedinto three groups (" to $# years, $# to $! years, and $! to$. years). )ey concluded that a greater orthopedic e,ectwas observed when therapy was applied before or duringthe pubertal growth spurt (" to $! years). Baik [$'] studied
maxillary expansion and protraction in '" Korean subjects,divided into three groups (<$# years, $# to $! years, and$! years or older). He concluded that age did not showany statistically signi*cant di,erence in treatment e,ects ofexpansion/facemask therapy. Braun [$/] studied &% subjectsaged '–$% and found that expansion/facemask therapy pro-duces dentofacial changes that combine to improve class IIImalocclusion. )ey reported that, although early treatmentmay be the most e,ective, facemask therapy can providea viable option for older children as well. But what aboutyoung adults? Can the skeletal and dental changes seen inexpansion/facemask therapy in children and adolescents bedemonstrated in this age group as well, possibly eliminatingthe need for orthodontic dental camou-age treatment ororthognathic surgery?
2. Case Report
A $(-year-$-month-old Caucasian female presented with achief complaint of “I do not like my underbite.” Her medical
Hindawi Publishing Corporation
Case Reports in Dentistry
Volume 2014, Article ID 270257, 6 pages
http://dx.doi.org/10.1155/2014/270257
! Case Reports in Dentistry
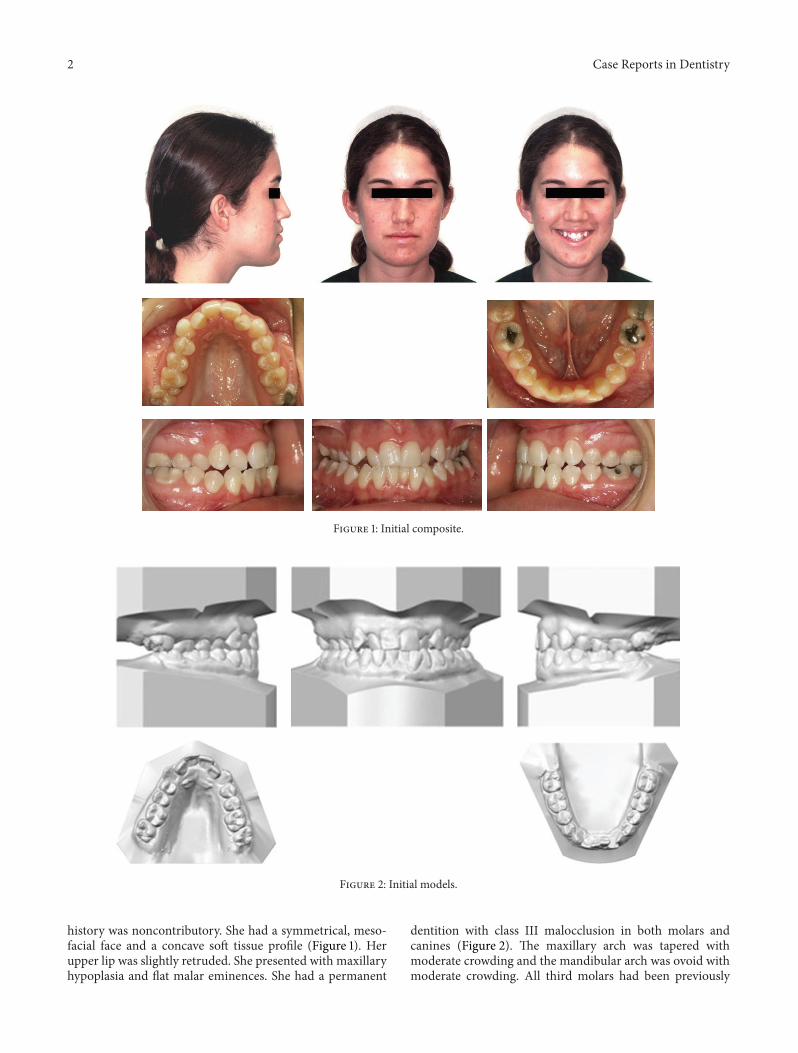
F01234 $: Initial composite.
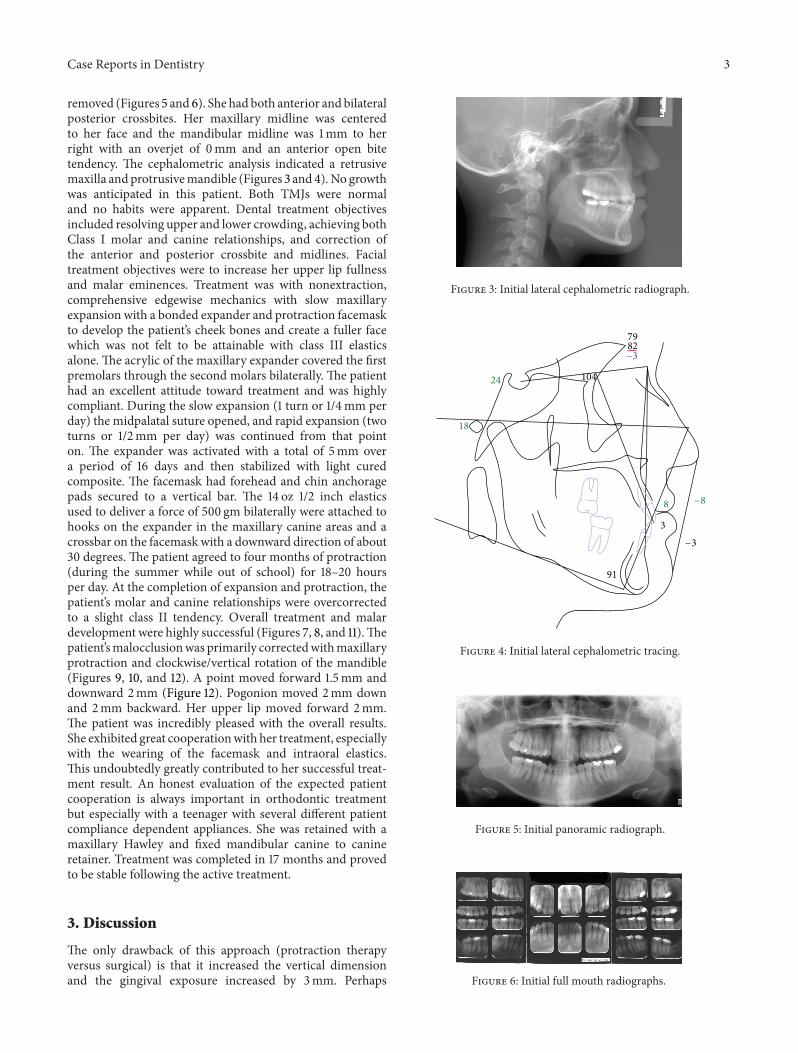
F01234 !: Initial models.
history was noncontributory. She had a symmetrical, meso-facial face and a concave so+ tissue pro*le (Figure $). Herupper lip was slightly retruded. She presented with maxillaryhypoplasia and -at malar eminences. She had a permanent
dentition with class III malocclusion in both molars andcanines (Figure !). )e maxillary arch was tapered withmoderate crowding and the mandibular arch was ovoid withmoderate crowding. All third molars had been previously
Case Reports in Dentistry %
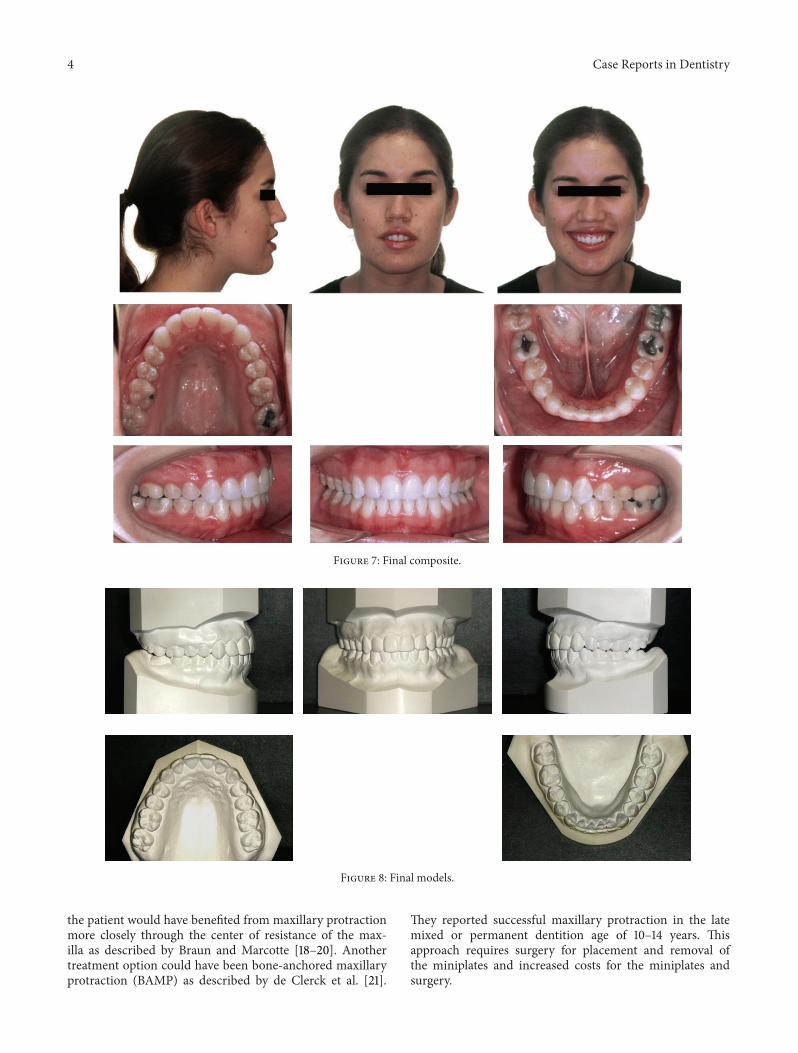
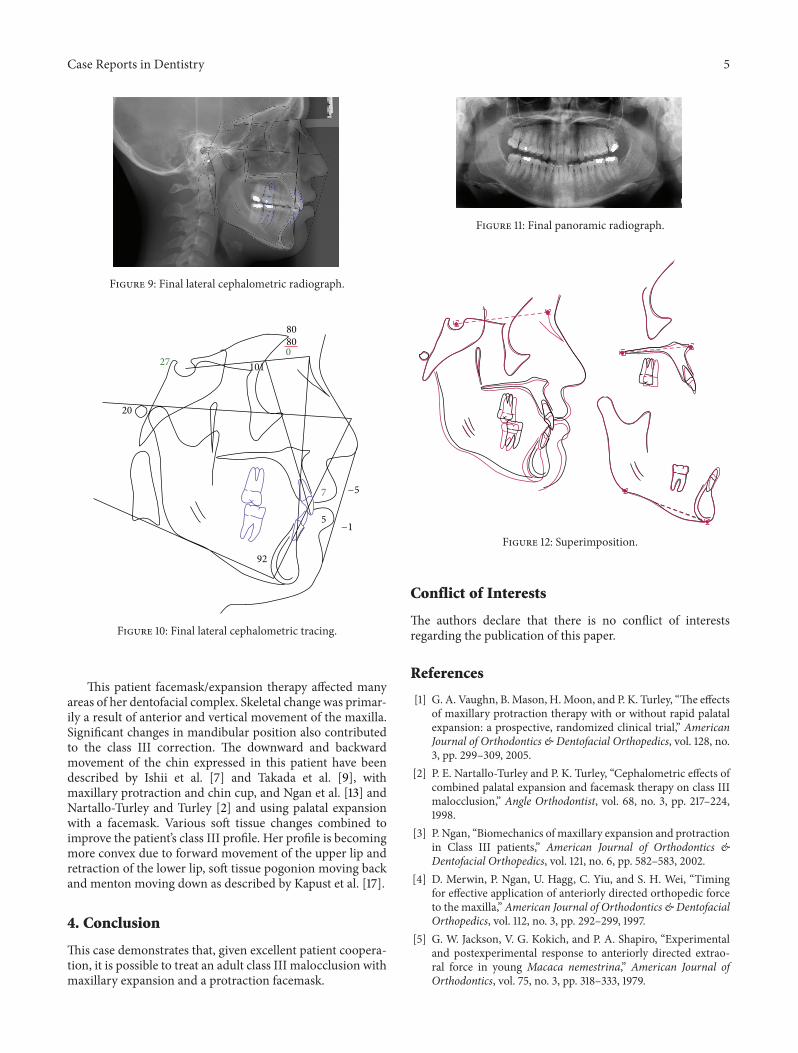
removed (Figures . and &). She had both anterior and bilateralposterior crossbites. Her maxillary midline was centeredto her face and the mandibular midline was $mm to herright with an overjet of #mm and an anterior open bitetendency. )e cephalometric analysis indicated a retrusivemaxilla andprotrusivemandible (Figures % and '). No growthwas anticipated in this patient. Both TMJs were normaland no habits were apparent. Dental treatment objectivesincluded resolving upper and lower crowding, achieving bothClass I molar and canine relationships, and correction ofthe anterior and posterior crossbite and midlines. Facialtreatment objectives were to increase her upper lip fullnessand malar eminences. Treatment was with nonextraction,comprehensive edgewise mechanics with slow maxillaryexpansion with a bonded expander and protraction facemaskto develop the patient’s cheek bones and create a fuller facewhich was not felt to be attainable with class III elasticsalone.)e acrylic of the maxillary expander covered the *rstpremolars through the second molars bilaterally.)e patienthad an excellent attitude toward treatment and was highlycompliant. During the slow expansion ($ turn or $/'mm perday) the midpalatal suture opened, and rapid expansion (twoturns or $/!mm per day) was continued from that pointon. )e expander was activated with a total of .mm overa period of $& days and then stabilized with light curedcomposite. )e facemask had forehead and chin anchoragepads secured to a vertical bar. )e $' oz $/! inch elasticsused to deliver a force of .## gm bilaterally were attached tohooks on the expander in the maxillary canine areas and acrossbar on the facemask with a downward direction of about%# degrees.)e patient agreed to four months of protraction(during the summer while out of school) for $/–!# hoursper day. At the completion of expansion and protraction, thepatient’s molar and canine relationships were overcorrectedto a slight class II tendency. Overall treatment and malardevelopment were highly successful (Figures ", /, and $$).)epatient’smalocclusionwas primarily correctedwithmaxillaryprotraction and clockwise/vertical rotation of the mandible(Figures (, $#, and $!). A point moved forward $..mm anddownward !mm (Figure $!). Pogonion moved !mm downand !mm backward. Her upper lip moved forward !mm.)e patient was incredibly pleased with the overall results.She exhibited great cooperationwith her treatment, especiallywith the wearing of the facemask and intraoral elastics.)is undoubtedly greatly contributed to her successful treat-ment result. An honest evaluation of the expected patientcooperation is always important in orthodontic treatmentbut especially with a teenager with several di,erent patientcompliance dependent appliances. She was retained with amaxillary Hawley and *xed mandibular canine to canineretainer. Treatment was completed in $" months and provedto be stable following the active treatment.
3. Discussion
)e only drawback of this approach (protraction therapyversus surgical) is that it increased the vertical dimensionand the gingival exposure increased by %mm. Perhaps
F01234 %: Initial lateral cephalometric radiograph.
24
18
8
91
3
!3
!8
7982!3
104
F01234 ': Initial lateral cephalometric tracing.
F01234 .: Initial panoramic radiograph.
F01234 &: Initial full mouth radiographs.
' Case Reports in Dentistry
F01234 ": Final composite.
F01234 /: Final models.
the patient would have bene*ted from maxillary protractionmore closely through the center of resistance of the max-illa as described by Braun and Marcotte [$/–!#]. Anothertreatment option could have been bone-anchored maxillaryprotraction (BAMP) as described by de Clerck et al. [!$].
)ey reported successful maxillary protraction in the latemixed or permanent dentition age of $#–$' years. )isapproach requires surgery for placement and removal ofthe miniplates and increased costs for the miniplates andsurgery.
Case Reports in Dentistry .
F01234 (: Final lateral cephalometric radiograph.
20
27 101
92
7
!1
!5
80800
5
F01234 $#: Final lateral cephalometric tracing.
)is patient facemask/expansion therapy a,ected manyareas of her dentofacial complex. Skeletal change was primar-ily a result of anterior and vertical movement of the maxilla.Signi*cant changes in mandibular position also contributedto the class III correction. )e downward and backwardmovement of the chin expressed in this patient have beendescribed by Ishii et al. ["] and Takada et al. [(], withmaxillary protraction and chin cup, and Ngan et al. [$%] andNartallo-Turley and Turley [!] and using palatal expansionwith a facemask. Various so+ tissue changes combined toimprove the patient’s class III pro*le. Her pro*le is becomingmore convex due to forward movement of the upper lip andretraction of the lower lip, so+ tissue pogonion moving backand menton moving down as described by Kapust et al. [$"].
4. Conclusion
)is case demonstrates that, given excellent patient coopera-tion, it is possible to treat an adult class III malocclusion withmaxillary expansion and a protraction facemask.
F01234 $$: Final panoramic radiograph.
F01234 $!: Superimposition.
Conflict of Interests
)e authors declare that there is no con-ict of interestsregarding the publication of this paper.
References
[$] G. A. Vaughn, B.Mason, H.Moon, and P. K. Turley, “)e e,ectsof maxillary protraction therapy with or without rapid palatalexpansion: a prospective, randomized clinical trial,” AmericanJournal of Orthodontics & Dentofacial Orthopedics, vol. $!/, no.%, pp. !((–%#(, !##..
[!] P. E. Nartallo-Turley and P. K. Turley, “Cephalometric e,ects ofcombined palatal expansion and facemask therapy on class IIImalocclusion,” Angle Orthodontist, vol. &/, no. %, pp. !$"–!!',$((/.
[%] P. Ngan, “Biomechanics of maxillary expansion and protractionin Class III patients,” American Journal of Orthodontics &Dentofacial Orthopedics, vol. $!$, no. &, pp. ./!–./%, !##!.
['] D. Merwin, P. Ngan, U. Hagg, C. Yiu, and S. H. Wei, “Timingfor e,ective application of anteriorly directed orthopedic forceto the maxilla,” American Journal of Orthodontics & DentofacialOrthopedics, vol. $$!, no. %, pp. !(!–!((, $((".
[.] G. W. Jackson, V. G. Kokich, and P. A. Shapiro, “Experimentaland postexperimental response to anteriorly directed extrao-ral force in young Macaca nemestrina,” American Journal ofOrthodontics, vol. "., no. %, pp. %$/–%%%, $("(.
& Case Reports in Dentistry
[&] J. A. McNamara Jr., “An orthopedic approach to the treatmentof Class III malocclusion in young patients,” Journal of ClinicalOrthodontics, vol. !$, no. (, pp. .(/–&#/, $(/".
["] H. Ishii, S. Morita, Y. Takeuchi, and S. Nakamura, “Treatmente,ect of combinedmaxillary protraction and chincap appliancein severe skeletal Class III cases,”American Journal of Orthodon-tics andDentofacial Orthopedics, vol. (!, no. ', pp. %#'–%$!, $(/".
[/] P. K. Turley, “Orthopedic correction of Class III malocclusionwith palatal expansion and custom protraction headgear,”Journal of Clinical Orthodontics, vol. !!, no. ., pp. %$'–%!., $(//.
[(] K. Takada, S. Petdachai, andM. Sakuda, “Changes in dentofacialmorphology in skeletal Class III children treated by a modi*edmaxillary protraction headgear and a chin cup: a longitudinalcephalometric appraisal,” European Journal of Orthodontics, vol.$., no. %, pp. !$$–!!$, $((%.
[$#] T. Kambara, “Dentofacial changes produced by extraoral for-ward force in theMacaca irus,” American Journal of Orthodon-tics, vol. "$, no. %, pp. !'(–!"", $("".
[$$] R. Nanda, “Protraction of maxilla in rhesus monkeys bycontrolled extraoral forces,” American Journal of Orthodontics,vol. "', no. !, pp. $!$–$'$, $("/.
[$!] R.Nanda andW.Hickory, “Zygomaticomaxillary suture adapta-tions incident to anteriorly-directed forces in rhesus monkeys,”Angle Orthodontist, vol. .', no. %, pp. $((–!$#, $(/'.
[$%] P. Ngan, H. Urban, C. Yiu, D. Merwin, and S. Wei, “So+ tissueand dentoskeletal pro*le changes associated with maxillaryexpansion and protraction headgear treatment,”American Jour-nal of Orthodontics &Dentofacial Orthopedics, vol. $#(, no. $, pp.%/–'(, $((&.
[$'] H. S. Baik, “Clinical results of the maxillary protraction inKorean children,” American Journal of Orthodontics & Dento-facial Orthopedics, vol. $#/, no. &, pp. ./%–.(!, $((..
[$.] R.Nanda, “Biomechanical and clinical considerations of amod-i*ed protraction headgear,” American Journal of Orthodontics,vol. "/, no. !, pp. $!.–$%(, $(/#.
[$&] W. M. Smalley, P. A. Shapiro, T. H. Hohl, V. G. Kokich,and P.-I. Branemark, “Osseointegrated titanium implants formaxillofacial protraction in monkeys,” American Journal ofOrthodontics and Dentofacial Orthopedics, vol. (', no. ', pp.!/.–!(., $(//.
[$"] A. Kapust, P. Sinclair, and P. K. Turley, “Cephalometric e,ectsof face mask/expansion therapy in Class III children: a compar-ison of three age groups,” American Journal of Orthodontics &Dentofacial Orthopedics, vol. $$%, no. !, pp. !#'–!$!, $((/.
[$/] S. Braun, “Extraoral appliances: a twenty-*rst century update,”American Journal of Orthodontics & Dentofacial Orthopedics,vol. $!., no. ., pp. &!'–&!(, !##'.
[$(] S. Braun, “Biomechanical considerations in the management ofthe vertical dimension,” Seminars in Orthodontics, vol. /, no. %,pp. $'(–$.', !##!.
[!#] M. Marcotte, Biomechanics in Orthodontics, B.C.Decker, $((#.[!$] H. J. deClerck,M.A.Cornelis, L.H.Cevidanes,G.C.Heymann,
and C. J. F. Tulloch, “Orthopedic traction of the maxillawith miniplates: a new perspective for treatment of midfacede*ciency,” Journal of Oral andMaxillofacial Surgery, vol. &", no.$#, pp. !$!%–!$!(, !##(.
Submit your manuscripts athttp://www.hindawi.com
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 201
Oral OncologyJournal of
DentistryInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 201
�,QWHUQDWLRQDO�-RXUQDO�RI
%LRPDWHULDOV+LQGDZL�3XEOLVKLQJ�&RUSRUDWLRQKWWS���ZZZ�KLQGDZL�FRP 9ROXPH�����
BioMed Research International
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 201H
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 201
Case Reports in Dentistry
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 201
Oral ImplantsJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 201
AnesthesiologyResearch and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 201
Radiology Research and Practice
Environmental and Public Health
Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 201
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 201
Dental SurgeryJournal of
Drug DeliveryJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 201
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 201
Oral DiseasesJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 201
Computational and Mathematical Methods in Medicine
ScientificaHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PainResearch and TreatmentHindawi Publishing Corporationhttp://www.hindawi.com Volume 201
Preventive MedicineAdvances in
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 201
,QWHUQDWLRQDO�-RXUQDO�RI
(QGRFULQRORJ\+LQGDZL�3XEOLVKLQJ�&RUSRUDWLRQKWWS���ZZZ�KLQGDZL�FRP
9ROXPH�����
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
OrthopedicsAdvances in


















