Exclusive preview carr neurologic rehabiltation 2e
18
77 Chapter Standing up and sitting down 4 CHAPTER CONTENTS Introduction 77 Biomechanical description 78 Standing up 78 Sitting down 82 Age-related changes 82 Motor dysfunction 82 Task-oriented training 83 Functional strength training 89 Measurement 92 INTRODUCTION Standing up from a seat is one of the most commonly performed functional activities. The ability to stand up effectively is essential to independent living and is a criti- cal prerequisite for upright mobility. In standing up, the feet act as a fixed base of support over which the body mass is rotated and raised to reposition the centre of body mass (COM) over the feet in standing (Fig. 4.1). Bending the knees to lower the body mass over the feet, moving the hips back until they reach the seat, also requires fine control of the lower limb muscles working eccentrically. These tasks are particularly difficult for individuals with neurological and/or lower limb musculoskeletal prob- lems. Standing up is one of the most physically demand- ing actions we perform regularly, requiring greater lower limb strength and range of motion than walking and stair climbing (Berger et al 1988). Lack of independence in standing up and sitting down is one of the most likely factors associated with risk of institutionalization (Branch & Meyers 1987) and is a common source of falls (Nyberg & Gustafson 1995; Cheng et al 1998). Standing up requires the ability to translate the body mass forward from a relatively stable sitting position (thighs and feet) to a small base of support, the feet. Gen- erating angular and linear momentum sufficient to perform this smooth translatory movement is potentially destabilizing. Therefore, the ability to balance the body mass by segmental movement and lower limb muscle activity while propelling it away from the seat is an impor- tant feature of standing up. The individual with motor impairment has to learn not only how to generate and control considerable muscle forces but also how to harness the interactional effects of segmental rotations so that the action becomes balanced and energy efficient. Support, propulsion and balance are major attributes of the lower limbs. Standing up (STS) and sitting down (SIT) belong to a group of significant weightbearing actions in which the feet act as a fixed segment over which the lower limbs flex and extend. Other significant weightbearing actions include stance phase of gait, walking up and down stairs, squatting and rising from squats, and the initial weightbearing phase of jumping and hopping. Lack of practice of this flexion/extension synergy in rela- tively immobile individuals is associated with weakness of lower limb extensor muscles and adaptive stiffening of calf muscles, particularly the soleus, making it mechani- cally more difficult or impossible to perform the actions. Repetitive practice and training of STS and SIT under dif- ferent varied task and contextual conditions can strengthen weak muscles using body weight resistance concentrically and eccentrically, also providing an active stretch to the © 2010 Elsevier Ltd DOI: 10.1016/B978-0-7020-4051-1.00012-6
-
date post
19-Oct-2014 -
Category
Education
-
view
1.992 -
download
0
description
The new edition continues to advance thismodel while identifying and incorporating the many advances that have occurred in the last decade in the understanding and treatment of adults with neurological conditions, whethercaused by accident or disease. Among theseadvances is the knowledge that the brainretains a plastic potential to reorganize, evenin old and/or lesioned brains, and that neuralplasticity can be influenced by task-relatedmental and physical practice in a stimulatingenvironment. There is also an increasing bodyof knowledge related to the musculoskeletalsystem's adaptability and the need to preventlength and stiffness- related changes in musclecontractility, together with loss of aerobicfitness and endurance. There is an expandingbody of clinical research that appears tosupport the model provided here.
Transcript of Exclusive preview carr neurologic rehabiltation 2e

77
Chapter
Standing up and sitting down
4
CHAPTER CONTENTS
Introduction 77 Biomechanical description 78
Standing up 78
Sitting down 82
Age-related changes 82 Motor dysfunction 82 Task-oriented training 83 Functional strength training 89 Measurement 92
INTRODUCTION
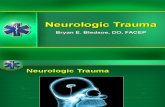
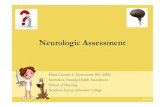
Standing up from a seat is one of the most commonly performed functional activities. The ability to stand up effectively is essential to independent living and is a criti-cal prerequisite for upright mobility. In standing up, the feet act as a fi xed base of support over which the body mass is rotated and raised to reposition the centre of body mass (COM) over the feet in standing ( Fig. 4.1 ). Bending the knees to lower the body mass over the feet, moving the hips back until they reach the seat, also requires fi ne control of the lower limb muscles working eccentrically.
These tasks are particularly diffi cult for individuals with neurological and/or lower limb musculoskeletal prob-lems. Standing up is one of the most physically demand-ing actions we perform regularly, requiring greater lower limb strength and range of motion than walking and stair
climbing ( Berger et al 1988 ). Lack of independence in standing up and sitting down is one of the most likely factors associated with risk of institutionalization ( Branch & Meyers 1987 ) and is a common source of falls ( Nyberg & Gustafson 1995 ; Cheng et al 1998 ).
Standing up requires the ability to translate the body mass forward from a relatively stable sitting position (thighs and feet) to a small base of support, the feet. Gen-erating angular and linear momentum suffi cient to perform this smooth translatory movement is potentially destabilizing. Therefore, the ability to balance the body mass by segmental movement and lower limb muscle activity while propelling it away from the seat is an impor-tant feature of standing up. The individual with motor impairment has to learn not only how to generate and control considerable muscle forces but also how to harness the interactional effects of segmental rotations so that the action becomes balanced and energy effi cient.
Support, propulsion and balance are major attributes of the lower limbs. Standing up (STS) and sitting down (SIT) belong to a group of signifi cant weightbearing actions in which the feet act as a fi xed segment over which the lower limbs fl ex and extend. Other signifi cant weightbearing actions include stance phase of gait, walking up and down stairs, squatting and rising from squats, and the initial weightbearing phase of jumping and hopping. Lack of practice of this fl exion/extension synergy in rela-tively immobile individuals is associated with weakness of lower limb extensor muscles and adaptive stiffening of calf muscles, particularly the soleus, making it mechani-cally more diffi cult or impossible to perform the actions. Repetitive practice and training of STS and SIT under dif-ferent varied task and contextual conditions can strengthen weak muscles using body weight resistance concentrically and eccentrically, also providing an active stretch to the
©2010 Elsevier LtdDOI: 10.1016/B978-0-7020-4051-1.00012-6

Task-related exercise and trainingPart 2
78
ankle dorsifl exion as the knees move forward ( Fig. 4.3 ). In the extension phase, extensor muscles crossing the hips, knees and ankles accelerate the body mass vertically.
Kinematics and kinetics Optimal performance of standing up involves a mechani-cally effi cient movement pattern and a basic underlying coordination, regardless of the goal or the environmental context. In the pre-extension phase, STS requires an initial generation of horizontal linear momentum of the body mass to move it forward over the feet, and the translation of horizontal momentum to vertical momentum at the start of the extension phase that propels the body mass vertically into standing. Horizontal momentum is brought about principally by angular rotation of the trunk segment at the hips. Vertical momentum is brought about by exten-sion at the hips, knees and ankles (see Fig. 4.3 ). It should be noted that the trunk segment (pelvis, spine and head) behaves as one ‘ virtual ’ segment, with the spine erect as it rotates forward, almost in one piece in the pre-extension phase and then rotates backward at the hips during the extension phase. Biomechanical analysis indicates that movement at the spinal joints is minimal.
The extent of angular displacement at the hips varies depending on the height and type of seat, presence or not of chair arms, starting position (e.g., presence or not of a back rest), and whether the arms are free to move or used for support and balance. In spite of seat variations, there is a remarkable and repeatable consistency in performance in this relatively simple action brought about essentially by fl exion and extension at the hips, knees and ankles.
Flexion and extension at the hips, knees and ankles occur not only by muscle forces but also by gravitational, inertial and interactive forces. Major extensor force genera-tion in STS occurs around the time the thighs are lifted off the seat in order to accelerate the body mass vertically. On
soleus if the feet are placed optimally. Such training improves intersegmental control of the lower limbs and upper body.
BIOMECHANICAL DESCRIPTION
Over the past two decades there has been an increasing interest in examining the dynamics of STS and SIT. The majority of studies have focused on sagittal plane move-ment using two-dimensional video or optoelectric analy-sis systems, with the subject standing up with feet on one or two force plates. Laboratory studies of both able-bodied individuals and individuals with motor impairment provide biomechanical data from which we can gain insight into the nature of motor control and develop guidelines for training these actions.
Standing up STS can be divided into a pre-extension and an extension phase ( Carr & Gentile 1994 ; Shepherd & Gentile 1994 ), the transition occurring at the time the thighs are lifted off the seat, called thighs-off (TO). There are other methods of identifying phases of STS ( Kralj et al 1990 ; Pai & Rogers 1990 ; Schenkman et al 1990 ) but this may be the simplest classifi cation for clinical purposes and it has some mechanical validity. In reality, the pre-extension and extension phases form a continuous movement that can be seen from the smooth curved path of the shoulder as the person moves from sitting to standing erect ( Fig. 4.2 ).
In the pre-extension phase, the feet are moved backward to position the ankle joint posterior to the knee joint. The upper body (head, arms, trunk) rotates forward by fl exion at the hips and dorsifl exion at the ankles. Reactive forces generated by the angular velocity of the upper body cause
Figure 4.1 This drawing illustrates in a simplifi ed form the essential kinematic features of standing up in the sagittal plane.
Figure 4.2 Note the smooth continuous curvilinear path of the shoulder marker, recorded as an able-bodied person moved from sitting to standing.

Standing up and sitting down Chapter
79
4
average, peak support moments of force (an algebraic summation of hip, knee and ankle moments of force) range from 4.00 to 5.50 Nm/kg in young able-bodied sub-jects, that is approximately four to fi ve times body weight, when standing up at their preferred speed ( Shepherd & Gentile 1994 ). When conditions demand it, able-bodied subjects can stand up with weight evenly distributed between the two lower limbs. However, in everyday life, the distribution of weight borne between the lower limbs varies depending on environmental demands and context of the action.
Since the thighs and feet are supported, ground reaction forces play an important part in the movement. STS requires coordinated muscle activity to generate forces against both the seat and ground. These ground or sup-portive reaction forces (GRFs) enable the propulsion of the body mass in the desired direction horizontally and
Sit-to-stand Stand-to-sit
A
Sit-to-stand Stand-to-sit
B
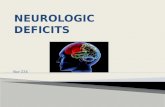
Figure 4.3 Sagittal plane stick fi gures taken from a biomechanical study of standing up and sitting down. (A) A typical young adult. (B) A typical older adult. Note: 1) movement of the shank segment (ankle dorsifl exion) in both activities. 2) Greater hip fl exion in SIT in younger compared to older person. (Reproduced from Dubost et al 2005, with permission).
vertically in standing up and the control of the body mass during descent. Peak vertical GRFs under the feet occur immediately following TO and reach over 100% body weight. These peak forces immediately decrease after TO and eventually stabilize to body weight once the person has settled in standing ( Fig. 4.4 ). Anteroposterior horizon-tal forces are considerably smaller than vertical forces. Generated in a posterior direction, they propel the body mass forward and are followed by anterior forces of similar magnitude that brake the forward momentum of the body mass.
Muscle activity Many mono- and bi-articular muscles spanning the hip, knee and ankle joints are involved in STS and SIT. In addi-tion, trunk muscles, rectus abdominus and lumbar

Task-related exercise and trainingPart 2
80
-20 -10 0 10 20 30 40 50
Percentage of total movement
60 70 80 90 100 110 120
TA
RF
BF
VL
GAST
SOL
Figure 4.5 Mean and standard error of time-normalized onsets and durations of six lower limb muscles as able-bodied subjects stand up at their preferred speed. TA: tibialis anterior; RF: rectus femoris; BF: biceps femoris; VL: vastus lateralis; GAST: gastrocnemius; SOL: soleus. 0 % : movement onset, 31 % : thighs-off, 100 % : movement end. (Reproduced from Khemlani et al 1998, with permission).
Figure 4.6 Anterior view of the R psoas major – the major muscle contributing to fl exion of the trunk and pelvis at the hip in standing up. (Reprinted from Musculino 2005, with permission).
810.0 x = 1.18y = 536
630.0
450.0
270.0
90.0
0.500 1.500 2.500Time (sec)
Z to
tal N
t
3.500 4.500
Figure 4.4 Typical vertical (z) ground reaction force profi le of an able-bodied subject standing up at a preferred speed of approximately 1.5s. Vertical line indicates thighs-off. Arrows indicate movement onset and movement end.
paraspinal muscles are active to stabilize the erect trunk segment, turning it into a virtual segment. Extensor muscle strength is a major contributor to successful performance ( Cameron et al 2003 ; Eriksrud & Bohannon 2003 ; Bohannon 2007 ).
Muscles investigated using electromyogram (EMG) have included rectus abdominus, lumbar paraspinals, trape-zius, gluteus medius, quadriceps, hamstrings, tibialis ante-rior, gastrocnemius and soleus ( Munton et al 1984 ; Richards 1985 ; Arborelius et al 1992 ; Khemlani et al 1998 ). Tibialis anterior is one of the fi rst muscles to be activated refl ecting its role in foot placement backward and in stabilizing the heel on the ground as the trunk swings forward, driving forward movement of the shank ( Fig. 4.5 ). Lumbar paraspinal, hip and knee extensor muscles reach peak activity together at TO to accelerate the body mass vertically once preparatory muscle activity has ensured the centre of gravity (COG) is appropriately placed. Preparatory and ongoing postural adjustments are very important in complex multisegmental actions such as STS in which the individual changes from a position of stability to a much less stable position ( Goulart &
Valls-Sole 1999 ). Variable patterns of EMG activity have been found in gastrocnemius and soleus refl ecting their additional role in balancing the body mass during the extensor phase and in standing. A major goal of postural muscle activity is to keep the COG within the base of support.
Iliopsoas, by its action in fl exing the pelvis (and trunk) forward at the hip joints, probably initiates this hip fl exion ( Fig. 4.6 ), however this relatively deep muscle is diffi cult to monitor. Simultaneous onsets of bi-articular rectus femoris and biceps femoris contribute to the control of limb movement – rectus femoris contributing to hip fl exion and knee extension and biceps femoris exerting a

Standing up and sitting down Chapter
81
4
spontaneously adapting standing up when they can move only the non-paretic foot back. This response sets up the action to be performed principally by the non-paretic limb and must be discouraged in order to prevent the individ-ual from ‘ favouring ’ the stronger limb and neglecting the paretic or weaker limb.
Timing and speed of trunk rotation. Trunk angular momentum, produced as the large upper body swings forward at the hip joints, is the major contributor to hori-zontal momentum of the body mass. It facilitates lower limb extension, requiring less overall muscle force in the lower limbs in order to raise the body mass to the standing position ( Schenkman et al 1990 ; Shepherd & Gentile 1994 ). Standing up slowly, as many neurological patients do, reduces momentum, with the result that more lower limb muscle force must be produced for a longer period of time ( Carr et al 2002 ). There is a similar effect when a patient moves the upper body forward, pauses, and stands up from a hip fl exed position. That is to say, absence of the facilitating effect of horizontal momentum means that greater lower limb muscle forces are produced for a longer time, which is why, in training, the patient is advised to move a little faster.
Seat height infl uences STS. A higher seat requires lower moments of force at the hip and knee joints, with seat height having a greater infl uence on the moments of force at the knee than at the hip ( Fig. 4.8 ). Lowering seat height increases the amount of momentum, peak muscle force and muscle strength required to get into standing (see Janssen et al 2002 for review).
Contribution of upper limbs to balance and propul-sion. Able-bodied subjects have no diffi culty standing up with arm movement restricted. However, variations in the extent of arm movement do have an effect on the dynam-ics of the action. When the arms are free to move, a lower level of extensor force is produced for a shorter time than when the arms are constrained ( Carr & Gentile 1994 ). Holding the paretic upper limb in front of the body with
braking force in preparation for extension of the hips, knees and ankles to raise the body into standing.
Biomechanical factors infl uencing performance STS involves a mechanically effi cient movement pattern and a basic underlying musculoskeletal coordination, regardless of the goal or the environment. However, fl ex-ibility of performance is critical to meet the demands of daily life and we adapt the action to internal (changing weight in pregnancy) and external (seat height) con-straints. Although able-bodied subjects can stand up and sit down with weight evenly distributed between the two limbs, in everyday life the motor strategy employed to rise to standing may vary as it depends on the intention and on the relative loading of the limbs. For example, standing up does not always end in quiet standing. It is often a transitional movement, standing up merging into another action such as walking.
Investigations of standing up to walk have shown that the two tasks merge smoothly in healthy subjects ( Magnan et al 1996 ). One study showed that when subjects were asked to stand up, forward momentum of the body ’ s COM ended in standing. When standing up to walk, however, forward momentum continued into the fi rst step, before the erect standing position was reached ( Malouin & Richards 2005 ). Many stroke patients are unable to merge the two tasks, probably because they have diffi culty con-trolling forward momentum. Instead they stand up fi rst and only then walk off ( Dion et al 1999 ; Malouin & Rich-ards 2005 ). In measuring functional motor performance, the timed up-and-go test is particularly useful as an indica-tion of functional progress as it tests the ability to adapt the basic STS pattern to the task of standing up and walking.
Mechanical effect of different foot placements. Foot placement specifi es the distance the body mass has to be moved forward in order to position the COM over the feet. Foot placement is a major factor in lower limb muscle force production and therefore in the amount of effort required. Standing up from sitting with the feet drawn back, the ankle joint posterior to the knee joint, is easier than with the feet forward. It reduces the distance the body mass has to move in a forward direction and requires less force generation from muscles crossing the hips and knees compared with more anterior foot placements ( Shepherd & Koh 1996 ). Standing up with the ankles dorsifl exed (approximately 75 ° ) puts an active stretch on the soleus ( Fig. 4.7 ), thus preserving length and extensibility – another reason for ensuring the paretic foot is bearing weight.
Standing up with one foot in front of the other increases the loading through the posterior limb and decreases it through the anterior limb. GRFs and magnitude of EMG activity in quadriceps and tibialis anterior increase signifi -cantly in the posterior limb with corresponding decreases in the forward limb ( Brunt et al 2002 ). Stroke patients are
10 cm
Figure 4.7 Preferred foot placement (approximately 75 ° ankle dorsifl exion) requires less force generation to stand up.

Task-related exercise and trainingPart 2
82
adults, although they have a tendency toward an increased trunk – thigh angle resulting in a more anterior position of the COM at TO. Movement time may be increased, however the action can be speeded up when required ( Vander Linden et al 1994 ). Older subjects sitting down showed a decreased trunk – thigh angle (i.e., decreased fl exion at the hips) compared with young adults ( Dubost et al 2005 ).
Lower limb muscle force generally correlates with balance and is the strongest predictor of success in STS for older individuals with impairments ( Schenkman et al 1996 ). In frail elderly subjects, sitting down is character-ized by diffi culty in movement initiation followed by rapid descent to the seat that is comparable to a backward fall ( Dubost et al 2005 ). Factors such as joint pain, reduced range of movement, muscle stiffness, muscle weakness and poor vision adversely affect performance. The minimum seat height for successful standing up for com-munity-dwelling and nursing home individuals with standing up diffi culties (aged 64 – 105 years) appears to be about 120% of lower leg length ( Weiner et al 1993 ) – this increased seat height minimizes the effort required.
In a group of older community-dwelling adults (age range 75 – 90 years), Lord and colleagues (2002) found that a diverse number of physiological and psychological factors were associated with the time taken to stand up. Visual contrast sensitivity, lower limb proprioception, tactile sensitivity, simple reaction time, postural sway, body weight, knee fl exor, extensor and ankle dorsifl exor strength, and pain, anxiety and vitality were all signifi cant and independent predictors of standing up performance. However, quadriceps isometric strength was the most reli-able predictor and correlated with movement time ( Lord et al 2002 ). This was consistent with Schenkman and col-leagues ’ fi nding (1996) that isometric strength was rela-tively more important than balance (functional reach test, static standing postural sway) in predicting movement time in older subjects. Another group of older individuals generated less isokinetic knee extensor strength than young subjects when standing up, using up to 87% of their available knee extensor torque compared with about 49% in the young adults ( Alexander et al 1995 ). Muscle strength is further impaired in individuals who have had a stroke and they may take longer to stand up compared with older subjects without neurological impairments ( Adams et al 1990 ).
MOTOR DYSFUNCTION
Individuals vary in their capacity to stand up and sit down, depending on their impairments and overall level of activ-ity. However, common problems arising from muscle weakness and lack of motor control can be observed as the individual attempts to stand up, and these problems
the non-paretic limb, a common clinical practice, restricts movement of both arms and is not effective as an aid to standing up, and it does not encourage more symmetrical weightbearing ( Seelen et al 1995 ).
Sitting down Although sitting down appears to be the same as STS only in reverse, there are some important differences. Each is performed under different mechanical constraints. Sitting down is performed by gravity, and movement from the start involves eccentric (lengthening) contractions of extensor muscles that cross the hips, knees and ankles in order to slow descent of the body mass. Just before the seat is reached, forward rotation of the trunk at the hips increases and the knees fl ex as the body mass moves back at the ankles. This is a particularly destabilizing move-ment, and the balancing, muscular and mechanical con-straints are challenging. As the hips near the seat, tibialis anterior contracts strongly to control the backward path of descent, while quadriceps control the fl exing knees, otherwise the individual would ‘ fall ’ back onto the seat. Maximum shank angle (dorsifl exion) occurs just before seat-on; maximum trunk fl exion angle (at the hips) at seat-on ( Dubost et al 2005 ).
AGE-RELATED CHANGES
Healthy elderly subjects standing up without using arm rests demonstrate motor performance similar to young
65%0
20
40
60
80
100
120
80%
Chair height(% knee height)
Mom
ent
(%Bw
× H
t)
Hip Knee Ankle
100% 115%
Figure 4.8 As seat height is raised, note that moments of force at the knee decrease. (Reproduced from Rodosky et al (1989), with permission).

Standing up and sitting down Chapter
83
4
TASK-ORIENTED TRAINING
Standing up is one of the most common daily activities we perform and independence in this action, a critical goal for rehabilitation, is dependent on getting the training right. Training involves repetitive practice of standing up and sitting down, from seats with different characteristics (height, shape) and with a variety of different goals. This provides opportunities for the individual to learn to adapt to task and environmental demands. Varied practice of standing up and sitting down is essential in order to train balance. Functional strength training is included in order to increase concentric and eccentric strength of lower limb extensors and ankle dorsifl exors, and intersegmental control of lower limbs.
Successful standing up and sitting down is critical to the achievement of many different functional goals. Although muscle weakness and lack of vigour may be limiting factors, training and repetitive practice of standing up and sitting down, with other weightbearing exercises to
provide the focus for training. Lower limb muscle weak-ness (particularly of quadriceps and dorsifl exors) and con-tracture of the soleus muscle are common factors that interfere with performance of standing up and sitting down. So too are hip and knee fl exion contractures that may occur during a prolonged period of coma associated with traumatic brain injury.
When individuals have muscle weakness, and diffi culty generating, timing and sustaining muscle forces, certain limitations are evident as they try to stand up. The most signifi cant adaptation seen in stroke patients is asymmetri-cal weightbearing during both standing up and sitting down ( Fig. 4.9 ). These individuals are particularly prone to falling because of muscle weakness and slowness in making postural adjustments that are essential in balanc-ing the body mass throughout these destabilizing move-ments. It is interesting to note that there is some evidence that increased loading through the paretic limb, that is more symmetrical weightbearing, following postural sym-metry and repetitive STS – SIT training is associated with a reduction in falls ( Cheng et al 2001 ). Common limita-tions and resultant adaptations are listed in Box 4.1
Figure 4.9 Asymmetrical weight-bearing. Failure to move paretic L foot back forces his weight on to the stronger R. leg. Note also the wide base of support.
Box 4.1 Common limitations and resultant adaptations
Standing up • Weightbearing through a weaker limb is avoided due
to limb instability and weakness ( Engardt & Olsen 1992 ; Hesse et al 1994 ; Cheng et al 1998 ; Lomaglio & Eng 2005 ): – Foot of stronger limb is spontaneously moved back,
weaker limb is not (see Fig. 4.9 ) – If feet are parallel, stronger limb is spontaneously
loaded as weight shifts to that side ( Fig. 4.10B ) – Shift to stronger leg may not occur until TO
• Moving the body far enough forward prior to TO is avoided due to inability to stabilize the foot of the weaker leg, fear of falling forward, lack of vigour ( Fig. 4.11 ): – Hands are used for support, balance and upward
lift ( Fig. 4.12 ) – Upper body is moved forward, with a pause,
before extension phase begins – Feet are placed wide apart for balance
• Movement is performed slowly – stroke patients, for example, take 25 – 60% longer to stand up than able-bodied adults ( Engardt & Olsson 1992 ; Cheng et al 1998 )
Sitting down • Body mass moves back too soon with reduced shank
angle (dorsifl exion), hip fl exion and knee fl exion ( Fig. 4.13 ): – Hands may be used on chair arms

Task-related exercise and trainingPart 2
84
Figure 4.10 Although she can stand up independently, note that she loads the more posterior (stronger) L leg more than R, evident as early as thighs-off.
A
B
Figure 4.11 Failure to move her body mass far enough forward – she fl exes her lumbar spine instead of her hips. Note the use of her arms – using the arms interferes with learning of independent standing up – it prevents the generation of horizontal momentum.
Figure 4.12 Failure to move his COM far enough forward ( ↓ hip fl exion and ↓ ankle dorsifl exion). Note how he uses his R arm as he attempts to stand up.

Standing up and sitting down Chapter
85
4
increase muscle strength and endurance, should enable the majority of people to learn again how to stand up independently and effi ciently. Effective standing up and sitting down obviates the necessity for a person to be ‘ pulled up ’ into standing by others, with the possibility of damage to soft tissues around the shoulder ( Wanklyn et al 1996 ). Safety procedures in hospitals may result in a weak person after stroke being lifted from bed to chair in a hoist. Once the person is sitting on a suitable seat, training standing up can begin.
Practice of the whole action is necessary in order to develop the necessary sequencing and timing of segmental rotations to both generate and utilize momentum. Use of the hands is discouraged. Those individuals who have diffi culty activating and sustaining leg muscle activity may require simple exercises to help them get the idea of acti-vating key muscle groups. Repetition is necessary for three reasons: to strengthen the extensor muscles of the lower limbs, to improve intersegmental control of the lower limbs by training linked segment mechanics, and to optimize learning. The individual is learning again, with an altered nervous system, how to utilize the characteris-tics of the segmental linkage in order to optimize interseg-mental transfer of power and to minimize energy requirements.
Invariant biomechanical characteristics of standing up that are critical to successful performance provide the ‘ rules ’ of standing up, from which a standardized set of guidelines can be developed for all members of the therapy and nursing staff, the patient and relatives to follow. The
A
B
Figure 4.14 The therapist models the action to demonstrate the extent of trunk fl exion at the hips (A) beside the patient so he can line his trunk up with hers, (B) providing a sagittal plane view to show him how far forward shoulders are moved.
therapist models the action for the patient to demonstrate the ‘ shape ’ or form of the action ( Fig. 4.14 ). Nurses are trained in the STS guidelines so they develop confi dence in their ability to give the necessary assistance and advice. Barreca and colleagues (2004) found that a coordinated effort on the part of all staff helped stroke survivors with multiple problems learn to stand up effectively. The prac-tice environment, combined with consistent feedback from all staff, resulted in more stroke patients learning to stand up independently than a control group who had usual care.
Figure 4.13 Sitting down. Failure to control descent causes her to ‘ fall ’ back on to the seat. Her hips, knees and ankles should be fl exed. Note tibialis anterior should be working strongly to stabilize the ankle, keeping the knees forward and controlling the backward path of descent.

Task-related exercise and trainingPart 2
86
a raised box support, height-adjusted to 25% of seat height. The results showed that patients increased loading of the paretic limb in conditions B and C compared with the normal condition. Peak vertical force under the paretic foot was increased, and EMG amplitude was increased in quadriceps (B, 34%; C, 41%), and tibialis anterior (B, 29%; C, 51%). No instructions were given to the patients to increase the use of the paretic limb – the load increased naturally because the stronger leg was at a biomechanical disadvantage.
A more recent study measured the vertical ground reac-tion forces under the feet and thighs in stroke patients during standing up and sitting down under four condi-tions: 1) spontaneous foot placement; 2) symmetrical foot placement; 3) paretic foot placed backward; and 4) non-paretic foot placed backward. Similar to Brunt ’ s fi ndings, when the paretic foot was placed behind the non-paretic foot, asymmetrical loading was reduced, reaching values similar to those reported in able-bodied subjects ( Chou et al 2003 ). The condition in which the non-paretic foot was placed behind the paretic foot resulted in the greatest loading asymmetry. In other words, positioning the paretic foot behind reduced asymmetry whereas position-ing the non-paretic foot behind increased asymmetry.
Both studies make it clear that loading asymmetry favouring the non-paratic limb must be avoided if the goal of training is to prevent non-use of the paretic limb. It is interesting to note that asymmetrical loading was evident
Figure 4.15 She is practicing STS/SIT with the paretic leg placed well back, loading the L leg. Here, she is focusing on swinging her shoulders and trunk forward a little faster in order to develop the momentum to rise to stand.
Box 4.2 Training guidelines at a glance
Standing up • ‘ Pull your feet back. ’ Feet placed 10 cm behind the
knees. To load the weaker leg, the foot of the stronger leg is placed in front of the other
• Seat height adjusted to match lower limb strength • Flat seat with no arms or back rest • Start movement from a trunk vertical position • ‘ Swing upper body forward, push down through the
feet and stand up ’ to create horizontal momentum of body mass
• ‘ Speed up ’ if too slow • Focus eyes on an object at sitting eye height • Do three sets of maximum number of repetitions
(e.g., if 5 = max, do three sets of fi ve repetitions) and increase number as soon as possible
Sitting down • Place feet back near the seat – the foot of the
weaker leg back further than the other foot to force limb loading through that leg and eccentric contraction of muscles (particularly quadriceps)
• Flexion at hips, knees fl ex, ankles dorsifl ex to lower the body mass down and back to the seat
• If necessary, assist the fi nal lowering stage by steadying the knees as the person moves the hips back to the seat
Key biomechanical features incorporated into the train-ing guidelines are shown in Box 4.2 .
Standing up: foot placement and loading the weaker leg The patient sits on a fl at surface, feet together. To load the weaker leg, the foot of the stronger leg is placed in front of the other. This will force loading of the weaker leg ( Fig. 4.15 ).
The feet placed approximately 10 cm behind the knee facili-tates lower limb extensor muscle force production and requires less effort. The therapist positions the paretic foot back if the patient cannot, to ensure that standing up is practised from an optimal starting position. The foot can be stabilized with the heel on the ground by pushing down along the shank ( Fig. 4.16 ).
Brunt and colleagues (2002) studied standing up with a group of people after stroke in order to investigate the effects of foot placement on loading the paretic limb. There were three conditions: A, normal condition – feet parallel, both knees in 100 ° fl exion; B, foot of non-paretic limb placed in front of paretic foot with non-paretic knee in 75 ° fl exion; and C, foot of non-paretic limb placed on

Standing up and sitting down Chapter
87
4
just before thighs-off in standing up and at thighs-on in sitting down in all foot conditions (spontaneous, sym-metrical, paretic foot back, non-paretic foot back) except when the paretic foot was placed back ( Roy et al 2006 ).
Seat height Seat height is adjusted to match the individual ’ s lower limb ’ s strength – a higher seat makes it possible to stand up when the lower limb muscles are very weak. Seat height is progres-sively lowered as performance improves.
Adjusting seat height is used to make the action easier or progressively harder in order to strengthen the lower limb extensor muscles concentrically and eccentrically using body weight resistance; that is, by progressively increasing the load (resistance), dynamic strength through range is increased. Adjusting seat height increases or decreases the distance the body weight must be raised to achieve the standing position. It also changes the length at which the quadriceps generates peak force and the joint angle at which inertia is overcome. The lower the seat height, the greater the distance body mass has to be raised and the further it has to move in order to get forward over the feet.
A B C
Figure 4.16 Practice of standing up and sitting down. (A) Therapist stabilizes paretic foot on the fl oor by pushing down along the shank. (B) As she stands up therapist moves the L leg sideways to increase loading of this leg. (C) Lateral view – she has not moved her shoulders far enough forward (i.e. fl exed at the hips suffi ciently) – she can focus on this during her next set of repetitions.
Pivoting the trunk forward Pivoting the upper body forward at the hips is initiated from a trunk vertical position. Increasing the amplitude of angular rotation in this way optimizes forward and upward momen-tum. Instructions are given to speed up the action so that forward momentum merges into upward momentum making a smooth translational movement. The instruction can be: ‘ Swing your shoulders forward, push down through your feet and stand up ’ .
Directing vision and attention toward a target during STS/SIT provides an external focus for erect body align-ment by affecting the path of the head and shoulders forward and up. Attention can be drawn to a target a few metres ahead at sitting eye level. Encourage an increase in speed – a slow performance requires more effort.
Controlling descent in sitting down Clinical observation suggests that individuals with motor impairment who are not able to stand up may be able to sit down. However, their attempts may be comparable to a backward fall. It is therefore essential to train both stand-ing up and sitting down specifi cally. Sitting down may appear to be an easier action than standing up. However,

Task-related exercise and trainingPart 2
88
although not so much effort is involved, controlling the descent requires good coordination and good balance.
The feet are placed back near the seat. Flexion at the hips, knees and ankles lower the body down and back to the seat. The paretic foot can be stabilized on the fl oor ( Fig. 4.17 ).
Specifi c attention to loading the weaker limb is necessary to ensure an eccentric contraction of quadriceps through-out the action. In a study by Engardt and colleagues (1995) , stroke patients who received feedback about loading the paretic limb during sitting down training improved loading more than those who received no feedback.
Repetitions There is evidence that greater strength gains may be achieved when repetitions are carried out without a rest between each repetition ( Rooney et al 1994 ). The number of repetitions can be prescribed at the beginning of the session. The individual is encouraged to perform three sets of his/her maximum number, taking a rest between sets, not after each stand up. Using a counter enables the physi-otherapist and patient to record the number of repetitions during the session ( Fig. 4.18 ), providing feedback and incentive. The number of repetitions during the day can
Figure 4.17 Sitting down on to a high seat. The therapist is stabilizing the paretic foot on the fl oor while keeping his knee forward. This gives him the idea of the amount of fl exion necessary. The exercise trains the ability to control descent of the body by eccentric muscle activity of the quadriceps.
Figure 4.18 Partially supervised repetitive practice of STS and SIT. She is getting feedback about loading the limb from a limb load monitor and is recording the number of repetitions on a hand-held counter.
be monitored using an activity monitor (ActivPal ™ single-axis accelerometry).
Several studies have demonstrated positive effects of repetitive STS/SIT practice ( Dean et al 2000 ; Cheng et al 2001 ; Monger et al 2002 ; Britten et al 2008). In a recent pilot study, Britten and colleagues (2008) tested a training protocol for patients following stroke in a UK rehabilita-tion unit. They assessed the effect of a 30-minute pro-gramme each day over 2 weeks. STS/SIT practice with training was provided by a physiotherapy assistant. People were included if they could stand up with ‘ standby ’ super-vision without using their hands for support, but were unable to stand up more than three times in 10 seconds. The control group received an equivalent period of arm therapy. In the STS/SIT training group, training empha-sized foot placement at the start of the movement, speed (particularly of forward movement of the trunk), with increased weightbearing through the paretic leg to gener-ate symmetrical GRFs. Visual feedback of GRF was pro-vided to the patients with a balance performance monitor. The assistant gave instructions and verbal feedback to aid learning. Practice was varied by changes in seat height and sitting surfaces. The aim of each session was to increase the number of repetitions and the number of STS each day was recorded using an ActivPal ™ single-axis accelerometry activity monitor. Other strengthening exercises were incor-porated if a patient fatigued. The assistant kept a log of training times for analysis of frequency of STS/SIT.

Standing up and sitting down Chapter
89
4
The results of this interesting study showed that the number of repetitions of STS/SIT increased on average from as few as 18 stands per day to 50 stands. There was a signifi cant mean difference of 10% body weight through the paretic leg after 1 week of training. In contrast, the control group reduced the weight they put through the paretic leg during the period of the clinical trial. The strength of this study comes from the use of a standardized protocol so that the results can provide a clear indication of the effects resulting from what the patients actually did and how much they did (the dosage).
This study demonstrates that 1 week of extra practice can improve performance of patients who can stand up but who are unsteady. After this study, there is absolutely no reason why all neurological patients who can partici-pate do not immediately start on such a programme. The challenge now is to use a training protocol in clinical practice with people with varied impairments who are unable to stand without help and see how many achieve independence in this important action.
Simple exercises to encourage muscle activation and encourage movement Diffi culty activating the plantarfl exors and hamstrings of the paretic leg to move the foot back behind the knee may require specifi c training. A slippery surface or roller skate decreases resistance and encourages the patient to slide the foot backward. A line on the fl oor marking the distance to be moved provides an external focus ( Fig. 4.19 ). The indi-vidual is reminded to position the feet to prepare for standing up. This is also important before sitting down, in order to avoid having too great a distance to move the body mass back to the seat.
Early post-stroke, fear of falling forward may be a major barrier to swinging the body mass forward. Practice of reach-ing forward with the hands on a table or reaching forward beyond arm ’ s length enables the patient to get the idea of the extent of movement so it can be incorporated into standing up practice ( Fig. 4.20 ). The table needs to be far enough forward to ensure the shoulders move well forward of the feet.
Loading the paretic leg and training balance When we reach forward beyond arm ’ s length, ground reac-tion forces increase under the foot indicating increased loading of one or both legs depending on the direction of the reach ( Dean & Shepherd 1997 ) ( Fig. 4.21 ). Alternate leg lifting gives the idea of loading and unloading ( Fig. 4.22 ).
FUNCTIONAL STRENGTH TRAINING
Effective standing up depends on strength and coordina-tion of muscles that cross the hips, knees and ankles. There is some evidence that knee extensor strength is a major
Figure 4.19 A towel reduces the friction between the shoe and fl oor while she practises activating hamstrings and muscles crossing the ankle to move her foot back. Her goal is to move her toes behind a line on the fl oor.
Figure 4.20 This woman was afraid of moving forward over her feet to stand up. With a table to rest her arms on, she is getting the idea of moving the shoulders forward and backward over her feet (fl exion and extension at the hips) to improve her confi dence.
contributor to successful STS ( Cameron et al 2003 ; Erik-srud & Bohannon 2003 ; Bohannon 2007 ). Knee extension strength may only be a predictor of standing up ability when considered in combination with synergic control of other muscles. In addition to knee extensor strength, Lomaglio & Eng (2005) have identifi ed two additional muscle groups, ankle dorsifl exors and plantarfl exors, that relate signifi cantly to standing up performance. They point

Task-related exercise and trainingPart 2
90
A
B
Figure 4.21 Reaching forward beyond arm ’ s length. (A) Initially she does not move her foot back and therefore cannot reach the bottle. (B) She can now extend her reach and is loading her L leg. Note her thighs are leaving the seat. This type of exercise boosts confi dence in use of lower limbs.
Figure 4.22 Reciprocal leg lifting – as one leg lifts, the other loads. Note she is moving backward. She tries to keep her knee fl exed – if it is too diffi cult the therapist can place a block in front of the foot. She also needs to practice lifting her knees higher.
Figure 4.23 Repetitive practice with arms folded increases lower limb extensor force strength. Focus can also be on increasing speed. (Courtesy of K Schurr and S Dorsch, Physiotherapy Department, Bankstown-Lidcombe Hospital, Sydney).
out that other muscles, for example gluteus medius, must also be active in standing up to provide lateral stability. At the start of standing up, tibialis anterior actively stabilizes the foot on the ground, explaining its signifi cance and correlation with STS performance. In fast-paced standing up, activation of plantarfl exors controls forward momen-tum of the body mass ( Lomaglio & Eng 2005 ).
Since the lower limb joints and muscles are harnessed together to act as a functional unit, an effi cient strength
training method is repetitive performance of the action: standing up and sitting down, positioning the stronger foot in front of the weaker foot, progressively increasing diffi -culty by lowering the height of the seat, folding the arms ( Fig. 4.23 ), and even adding a weighted belt or vest.

Standing up and sitting down Chapter
91
4
Additional functional weightbearing exercises are discussed in Chapter 2 , and include squats, step-ups and step-downs.
Seat selection Appropriate chair design makes a considerable contribu-tion to an individual ’ s wellbeing and independence, par-ticularly for the less mobile. Britton and colleagues (2008) have observed that when STS is not a specifi c focus of training, seat height may not be optimal for an individu-al ’ s height or strength, and patients are often encouraged or allowed to push on the chair arm with their non-paretic hand. This is a common observation. Similarly, teaching a person to ‘ transfer ’ is common clinical practice, in our opinion taking valuable therapy time away from a specifi c focus on training standing up and sitting down.
The most important features in chair design to assist standing up are seat height adjusted to the individual ’ s height and strength, and absence of any structural block to posterior foot placement. A survey in which elderly people were asked to rank in order of importance the fi ve factors they considered important in chair design, ‘ easy to get out of ’ was considered to be the most important and was ranked before comfort ( Munton et al 1981 ). Toilet seat raises should also be provided in rehabilitation centres and on discharge if needed.
Mental practice There may be several factors that limit the amount of physical practice in rehabilitation, including physical frailty, poor balance and lack of endurance, or lack of staff time. The addition of mental practice as a means of increasing practice time has been investigated by Malouin et al (2004) . In this study, stroke patients were trained with mental practice to increase loading of the paretic limb while standing up and sitting down, initially using a visual display, then relying on their memory. A single training session of 30 minutes included seven physical repetitions combined with 35 mental rehearsals. This session resulted in improved loading of the paretic limb and improvement was retained 24 hours later, suggesting a learning process. The amount of motor improvement in follow-up was strongly associated with working memory ability, particularly in the visuospatial domain.
Maximizing skill As the patient improves, gets stronger and more vigorous, and has a clear idea of the movement, emphasis changes from foot placement and speed of trunk rotation to train-ing fl exible performance. Practice is varied by incorporat-ing the sort of goals normally encountered in daily life, and provides the opportunity for the individual to perform different tasks and adapt to different environmental con-texts. Examples include talking while standing up and sitting down, holding a large object with both hands, steadying a glass of water or a tray ( Fig. 4.24 ), stopping and changing direction without losing balance during
A
B
Figure 4.24 Balancing the mugs changes the focus of attention from standing up to steadying the tray. It encourages keeping the body mass forward over the feet at thighs-off.

Task-related exercise and trainingPart 2
92
Figure 4.25 An exercise for improving balance that involves stopping and changing direction without losing balance.
Hip and knee angular velocity at MAS 6
HipKnee
HipKnee
0
0 1 2 3Time (s)
4 5 6
0.5
1
1.5
Angu
lar v
eloc
ity (R
ad/s
) 2
2.5
A
Hip and knee angular velocity at MAS 2
0
0 1 2 3Time (s)
4 5 6
0.5
1
1.5
Angu
lar v
eloc
ity (R
ad/s
) 2
2.5
B
Figure 4.26 Hip (solid line) and knee (dashed line) joint velocities are almost perfectly coupled at MAS 6 (A) whereas there was signifi cant independent activity (lack of coordination) at MAS 2 (B). (Ada L, O ’ Dwyer, NJ, Neilson PD (1992) Improvement in kinematic characteristics and coordination following stroke quantifi ed by linear systems analysis. Human Move Sci, 12 , 137 – 153, by kind permission of Elsevier Science, Amsterdam, The Netherlands).
sitting down practice ( Fig. 4.25 ), and merging standing up into walking off in different directions.
There is no evidence that repetitive practice of STS increases physical fi tness. However, for the frail elderly, ability to stand up may be initially limited by poor fi tness and endurance. It may be wise to monitor heart rate while increasing the number of repetitions each day.
MEASUREMENT
The following functional tests (see Ch. 3 ) have been found reliable when performed under standardized conditions:
• Standing up item of Motor Assessment Scale (MAS) • Timed up-and-go test • Rise-to-walk test ( Malouin et al 2003 ).
Strength of quadriceps is tested using a hand-held dynamometer or spring scale. Despite the signifi cance of strength in the performance of standing up, no readily available clinical test can measure strength as it is func-tionally used ( Buchner & de Lateur 1991 ). Number of repetitions can, however, be used as an indicator of func-tional strength.
The MAS is a valid and reliable indicator of perform-ance. A biomechanical study to test the effectiveness of training standing up after stroke demonstrated that as patients progressed from 2 to 6 on the scale, hip and knee joint velocity profi les became smooth and bell shaped, typical of well-coordinated movement ( Ada & Westwood
1992 ). Further analysis showed that the hip and knee joints had become perfectly coupled at MAS 6 ( Fig. 4.26 ), the highest score, similar to skill acquisition in able-bod-ied subjects ( Ada et al 1993 ).
In conclusion, lack of independence in standing up limits participation in everyday activities, including socializing and recreation, and it contributes to the overall deteriora-tion of lower limb muscle strength, fl exibility and func-tion. Standing up and sitting down are important actions to train in rehabilitation, not only for increasing the indi-vidual ’ s independence but also for the role of these actions in increasing muscle strength, motor control of the lower limbs and balance and preventing falls. There is some evidence of increased symmetrical weightbearing during standing up resulting in a reduction in falls ( Engardt et al 1995 ; Cheng et al 2001 ).

Standing up and sitting down Chapter
93
4
REFERENCES
Ada L , Westwood P 1992 A kinematic analysis of recovery of the ability to stand up following stroke . Aust J Physiother 38 : 135 – 142 .
Ada L , O ’ Dwyer N , Neilson PD 1993 Improvement in kinematic characteristics and coordination following stroke quantifi ed by linear systems analysis . Hum Mov Sci 12 : 137 – 153 .
Adams RW , Gandevia SC , Skuse NF 1990 The distribution of muscle weakness in upper motorneuron lesions affecting the lower limb . Brain 113 : 1459 – 1476 .
Alexander NB , Gu MJ , Branch M et al 1995 Geriatrics: does leg torque infl uence rising from a chair in older adults . Rehabil R D Prog Rep 32 : 101 – 102 .
Arborelius UP , Wretenberg P , Lindberg F 1992 The effects of armrests and high seat heights on lower-limb joint load and muscular activity during sitting and rising . Ergonomics 35 : 1377 – 1391 .
Barreca S , Sigouin CS , Lambert C et al 2004 Effects of extra training on the ability of stroke survivors to perform an independent sit-to-stand: a randomized controlled trial . J Geriatr Phys Ther 27 : 59 – 64 .
Berger RA, Riley PO, Mann RW et al 1988 Total body dynamics in ascending stairs and rising from a chair following total knee arthroplasty. In: Proceedings of the 34th Annual Meeting of the Orthopedic Research Society, Atlanta, GA.
Bohannon RW 2007 Knee extension strength and body weight determine sit-to-stand independence after stroke . Physiother Theory Pract 23 : 291 – 297 .
Branch LG , Meyers AR 1987 Assessing physical function in the elderly . Clin Geriatr Med 3 : 29 – 51 .
Britton E , Harris N , Turton A 2008 An exploratory randomized controlled trial of assisted practice for improving sit-to-stand in stroke patients in the hospital setting . Clin Rehabil 22 : 458 – 468 .
Brunt D , Greenberg B , Wankadia S et al 2002 The effect of foot placement on sit to stand in healthy young subjects and patients with hemiplegia . Arch Phys Med Rehabil 83 : 924 – 929 .
Buchner DM , de Lateur BJ 1991 The importance of skeletal muscle strength to physical function in older adults . Ann Behav Med 13 : 91 – 98 .
Cameron DM , Bohannon RW , Garrett GE et al 2003 Physical impairments related to kinetic energy during sit-to-stand and curb-climbing following stroke . Clin Biomech 18 : 332 – 340 .
Carr JH , Gentile AM 1994 The effect of arm movement on the biomechanics of standing up . Hum Mov Sci 13 : 175 – 193 .
Carr JH , Ow JE , Shepherd RB 2002 Some biomechanical characteristics of standing up at three different speeds: implications for functional training . Physiother Theory Pract 18 : 47 – 53 .
Cheng P-T , Liaw M-Y , Wong M-K et al 1998 The sit-to-stand movement in stroke patients and its correlation with falling . Arch Phys Med Rehabil 79 : 1043 – 1046 .
Cheng P-T , Wu S-H , Liaw M-Y et al 2001 Symmetrical body-weight distribution training in stroke patients and its effect on fall prevention . Arch Phys Med Rehabil 82 : 1650 – 1654 .
Chou SW , Wong AMK , Leong CP et al 2003 Postural control during sit-to-stand and gait in stroke patients . Am J Phys Med Rehabil 82 : 42 – 47 .
Dean CM , Shepherd RB 1997 Task-related training improves performance of a seated reaching task after stroke: a randomized controlled trial . Stroke 28 : 722 – 728 .
Dean CM , Richards CL , Malouin F 2000 Task-related circuit training improves performance of locomotor tasks in chronic stroke: a randomized, controlled pilot trial . Arch Phys Med Rehabil 81 : 409 – 417 .
Dion L , Malouin F , McFadyen BJ et al 1999 Assessment of the sit-to-walk capacity after stroke: a validation study . Gait Posture Suppl 1 : S24 .
Dubost V , Beauchet O , Manckoundia P et al 2005 Decreased trunk angular displacement during sitting down: an early feature of aging . Phys Ther 85 : 404 – 412 .
Engardt M , Olsson E 1992 Body weight-bearing while rising and sitting down in patients with stroke . Scand J Rehabil Med 24 : 67 – 74 .
Engardt M , Knutsson E , Johnsson M et al 1995 Dynamic muscle strength training in stroke patients: effects on knee extension torque, electromyographic activity, and motor function . Arch Phys Med Rehabil 76 : 419 – 425 .
Eriksrud O , Bohannon RW 2003 Relationship of knee extension force to independence in sit-to-stand performance in patients receiving acute rehabilitation . Phys Ther 83 : 544 – 551 .
Goulart FR , Valls-Sole J 1999 Patterned electromyographic activity in the sit-to-stand movement . Clin Neurophysiol 110 : 1634 – 1640 .
Hesse S , Schauer M , Malezic M et al 1994 Quantitative analysis of rising from a chair in healthy and hemiparetic subjects . Scand J Rehabil Med 26 : 161 – 166 .
Janssen WGM , Bussmann HBJ , Stam HJ 2002 Determinants of the sit-to-stand movement: a review . Phys Ther 82 : 866 – 879 .
Khemlani M , Carr JH , Crosbie WJ et al 1998 Muscles synergies and joint linkages in sit-to-stand under two different initial foot positions . Clin Biomech 14 : 236 – 246 .
Kralj A , Jaeger RJ , Munih M 1990 Analysis of standing up and sitting down in humans: defi nitions and normative data presentation . J Biomech 23 : 1123 – 1138 .
Lomaglio MJ , Eng JJ 2005 Muscle strength and weight-bearing symmetry relate to sit-to-stand performance in individuals with stroke . Gait Posture 22 : 126 – 131 .
Lord SR , Murray SM , Chapman K et al 2002 Sit-to-stand performance depends on sensation, speed, balance, and psychological status in addition to strength in older people . J Gerontol 57A : M539 – M543 .
Magnan A , McFadyen BJ , St-Vincent G 1996 Modifi cation of the sit-to-stand task with the addition of gait initiation . Gait Posture 4 : 232 – 241 .
Malouin F , Richards CL 2005 Assessment and training of locomotion after stroke: evolving concepts . In: Refshauge K , Ada L , Ellis E (eds) Science-based rehabilitation . Butterworth Heinemann , Oxford : 185 – 222 .

Task-related exercise and trainingPart 2
94
Malouin F , McFadyen B , Dion L et al 2003 A fl uidity scale for evaluating the motor strategy of the rise-to-walk task after stroke . Clin Rehabil 17 : 674 – 684 .
Malouin F , Belleville S , Richards CL et al 2004 Working memory and mental practice outcomes after stroke . Arch Phys Med Rehabil 85 : 177 – 183 .
Monger C , Carr JH , Fowler V 2002 Evaluation of a home-based exercise and training program to improve sit-to-stand in patients with chronic stroke . Clin Rehabil 16 : 361 – 367 .
Munton JS , Ellis MI , Chamberlain MA et al 1981 An investigation into the problems of easy chairs used by the arthritic and the elderly . Rheumatol Rehabil 20 : 164 – 173 .
Munton JS , Ellis MI , Wright V 1984 Use of electromyography to study leg muscle activity in patients with arthritis and in normal subjects during rising from a chair . Ann Rheumatic Dis 43 : 63 – 65 .
Muscolino JE 2005 The muscular system manual: the skeletal muscles of the human body , 2nd edn . Elsevier Mosby , St Louis, MO .
Nyberg L , Gustafson Y 1995 Patient falls in stroke rehabilitation. A challenge to rehabilitation strategies . Stroke 26 : 838 – 842 .
Pai Y , Rogers MW 1990 Control of body mass transfer as a function of
speed of ascent in sit-to-stand . Med Sci Sports Exerc 22 : 378 – 384 .
Richards CL 1985 EMG activity level comparisons in quadriceps and hamstrings in fi ve dynamic activities . In: Winter DA , Norman RW , Wells RP eds International series on biomechanics, IX-A . Human Kinetics , Champaign, IL : 313 – 317 .
Rodosky MV , Andriacchi TP , Andersson GBJ 1989 The infl uence of chair height on lower limb mechanics during rising . J Orthoped Res 7 : 266 – 271 .
Rooney KJ , Herbert RD , Balnave RJ 1994 Fatigue contributes to the strength training stimulus . Med Sci Sports Exerc 26 : 1160 – 1164 .
Roy G , Nadeau S , Gravel D et al 2006 The effect of foot position and chair height on the asymmetry of vertical forces during sit-to-stand and stand-to-sit tasks in individuals with hemiparesis . Clin Biomech 21 : 585 – 593 .
Schenkman M , Berger RA , O ’ Riley P et al 1990 Whole-body movements during rising to standing from sitting . Phys Ther 70 : 638 – 651 .
Schenkman M , Hughes MA , Samsa G et al 1996 The relative importance of strength and balance in chair rise by functionally impaired older individuals . J Am Geriatr Soc 44 : 1441 – 1446 .
Seelen HAM , van Wiggen KL , Halfens JHG et al 1995 Lower limb postural responses during sit-to-stand transfer in stroke patients during neurorehabilitation . In: Hakkinen K , Keskinen KL , Komi PV et al (eds) Book of abstracts of the XVth Congress of the International Society of Biomechanics . University of Jyvaskyla , Jyvaskyla, Finland : 826 – 827 .
Shepherd RB , Gentile AM 1994 Sit-to-stand: functional relationships between upper body and lower limb segments . Hum Mov Sci 13 : 817 – 840 .
Shepherd RB , Koh HP 1996 Some biomechanical consequences of varying foot placement in sit-to-stand in young women . Scand J Rehabil Med 28 : 79 – 88 .
Vander Linden DW , Brunt D , McCulloch MU 1994 Variant and invariant characteristics of the sit-to-stand task in healthy elderly adults . Arch Phys Med Rehabil 75 : 653 – 660 .
Wanklyn P , Forster A , Young J 1996 Hemiplegic shoulder pain (HSP): natural history and investigation of associated features . Dis Rehabil 18 : 497 – 501 .
Weiner DK , Long R , Hughes MA et al 1993 When older adults face the chair-rise challenge . J Am Geriatr Soc 41 : 6 – 10 .