
Example for an early drug-device development plan for an early drug-device development plan Dr....
36
Example for an early drug-device development plan Dr. Barbara Schug SocraTec R&D, Oberursel www.socratec-pharma.de Joint Conference of European Human Pharmacological Societies and 20 th Anniversary of AGAH Berlin, Germany, March 31 – April 01, 2011
Transcript of Example for an early drug-device development plan for an early drug-device development plan Dr....
Example for an early drug-device development plan
Dr. Barbara SchugSocraTec R&D, Oberursel
www.socratec-pharma.de
Joint Conference of European Human Pharmacological Societies and 20th Anniversary of AGAH
Berlin, Germany, March 31 – April 01, 2011
Why early drug-device combinations ?
Potential reasons for early drug-device combinations
intended drug targeting due toimproved therapeutic effect when the site of action is difficult to reachimproved tolerability when the side-effect pattern constrains regular use
intended local application for locally acting drugs
necessity to overcome drug substance limitationshigh–first pass metabolismpoor absorption due to solubility problems or molecule size

Locally acting / applied: ciclesonide
A. Weinbrenner: J Clin Endo 87(5): 2160-2163, 2002
Structural formula of ciclesonide
Metered dose inhaler for treatment of asthma
R-epimer

Locally acting / applied: ciclesonide
RM1 has approximately 100-fold greater affinity for glucocorticoid receptor
Metered dose inhaler for treatment of asthma
Proposed metabolic pathway of ciclesonide R-epimer
CDER Document: Application Number: 21-658
B9207-015
B9207-021(M1)
B9499-010(16-hydroxyprednislone)
M3 familyM2
anidentified metabolites
CYP3A4CYP2C8
CYP3A4CYP2D6
Esterase
CYP3A4CYP2D6
CYP3A4CYP2C8

Questions answered for ciclesonide (1)
Pharmacokinetic development program of ciclesonide with assessment of
absolute oral bioavailabilityabsolute inhaled bioavailabilitysingle dose (inhaled) dose proportionality (40-3250µg) in healthy subjects and asthmaticssteady state (inhaled) dose proportionality(250-1000µg)

Absolute oral bioavailability
Contribution of swallowed ciclesonide to be assessed primarily for safety reasons
single dose administrations6.9mg (oral) vs 0.64mg (i.v.) [14c] – ciclesonide separated by wash-out phase of 14 days6 healthy male subjects aged 19 to 40 yearsassessment of total radioactivity …… and of ciclesonide and RM1 in whole blood, plasma, urine and faeces

Absolute oral bioavailabilityStudy results
ciclesonide < 1%budesonide 10.7%fluticasone ≅ 1%
conclusion: swallowed ciclesonide of minor importance
after oral administration the parent compound was not detectable in plasma …… only traces of RM1 were determined resulting oral bioavailability below 1% for the parent compound

Absolute oral bioavailability
Nave R. et al: Int J Clin Pharm (2006) , 1-7
Fig 2. Cumulative excretion of radioactivity in urine and faeces after administration of 0.64mg of [14C]ciclesonide as a 10-minute intravenous infusion (IV) or 6.9mg of [14C]ciclesonide as an oral capsule (PO). Values are means ± standard error.
Due to poor systemic availability evaluation focuses on urine and faeces data

Oral systemic availability
in contrast to orally administered drugs with intended systemic availability, exposure after administration of such a drug-device combination for locally acting / locally applied drugs is only of relevance for the swallowed fraction
Conclusions from study results
thus, absolute bioavailability after oral administration in this case is assessed for safety reasons onlyabsolute bioavailability after inhaled administration is also determined for safety reasons

Questions answered for ciclesonide (2)Clinical pharmacology development program of ciclesonide with assessment of
absolute oral bioavailability (safety)absolute inhaled bioavailability (safety)single dose (inhaled) dose proportionality (40-3250µg) steady state (inhaled) dose proportionality(250-1000µg)PK in asthmatics and healthy subjectsPK in adults, children, male, female, whites, Japanese, black, elderly, patients with renal or hepatic impairment
PK after inhalation – patients ?
underlying disease influences site of absorption (obstruction and inflammation)PK may be different in patient population
Comparison healthy vs. asthmatics
12 patients with persistent asthma were matched with 12 healthy subjects (sex, age, BMI)single inhaled dose of 1280µg (8 puffs)
Target population is a special PK population per definition
Parallel group study performed for ciclesonide

PK after inhalation
R. Nave: Clin Pharm 43 (7): 479-486, 2004
Fig 1. Mean ± standard error of the mean serum concentrations of ciclesonide and desisobutyril ciclesonide in healthy subjects and patients with asthma after receiving a single inhaled dose of ciclesonide 1,280 µg.
Primary parameter:AUC of des-CIC1.003 (0.815-1.234)

Questions answered for ciclesonide (3)
Clinical pharmacology development program of ciclesonide with assessment of
“classical” drug-drug interaction studies with erythromycin, ketoconazole and formoterolsingle dose lung deposition with 99mTc-labeled ciclesonide in adults with moderate asthmasingle dose lung deposition with 99mTc-labeled ciclesonide in healthy volunteers
Lung-deposition
Local Pharmacokinetics to be assessed in addition
99mTc-labeled ciclesonide administered to healthy subjects and asthmaticsassessment of percent deposition in mouth and pharynxassessment of percent deposition in the lungcharacterisation of deposition pattern for peripheral and lower central regions of lung
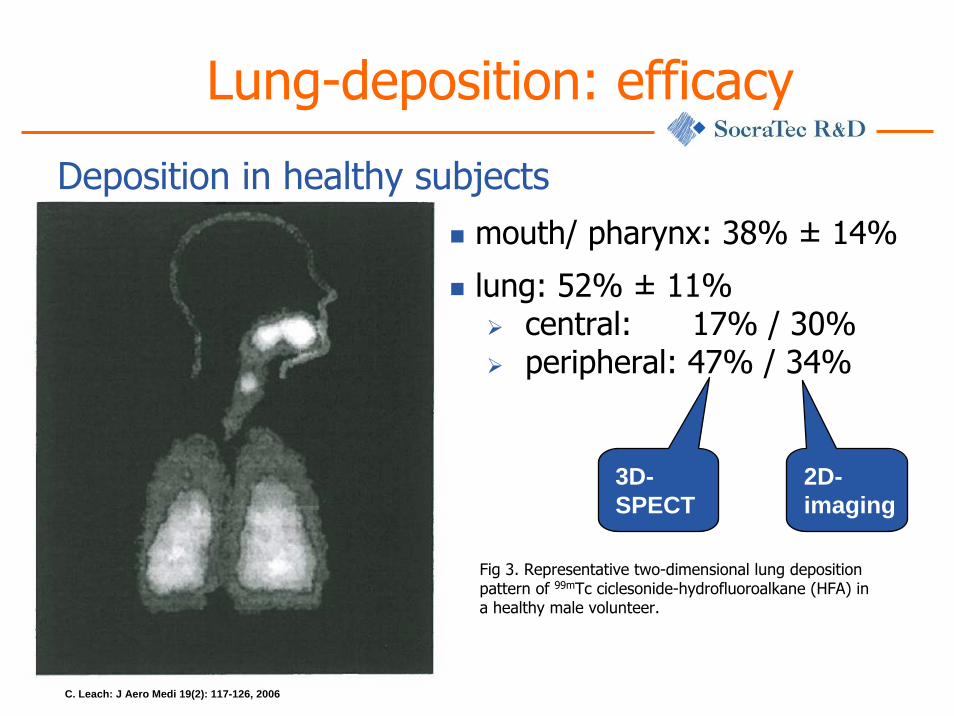
Lung-deposition: efficacy
C. Leach: J Aero Medi 19(2): 117-126, 2006
Fig 3. Representative two-dimensional lung deposition pattern of 99mTc ciclesonide-hydrofluoroalkane (HFA) in a healthy male volunteer.
Deposition in healthy subjectsmouth/ pharynx: 38% ± 14%
lung: 52% ± 11%central: 17% / 30%peripheral: 47% / 34%
2D-imaging
3D-SPECT

Questions answered for ciclesonide (4)
HPA-axis suppression determined in adults12 healthy male volunteers4-period-changeover design over 7 days each
800 µg morning administration800 µg evening administration400 µg BID
Cortisol suppression as safety marker
Hypothalamic-Pituitary-Adrenocortical-axis suppression also assessed in asthmatic children
comparison with placebo

Influence on HPA-axis
Cortisol suppression as safety markerprimary endpoints (cortisol in serum)
24h mesor (AUC(0-24h) / 24h)24h amplitude (1/2 Δ max / min)acceptance criterion: 80 – 125%assay: fluorescence polarisation immunoassay
A. Weinbrenner: J Clin Endo 87(5): 2160-2163, 2002
Dose Ratio / Confidence intervalmorning dose 800µg 0.94 / 0.86 – 1.02evening dose 800µg 0.98 / 0.90 – 1.07BID 400µg 0.93 / 0.86 – 1.02
study results (PE in comparison to placebo)

Cortisol suppression: safety
A. Weinbrenner: J Clin Endo 87(5): 2160-2163, 2002
Fig 2. Mean 24-h profiles of serum cortisol of 12 healthy volunteers treated for 7 d with (A) placebo twice daily, (B) 800 µg ciclesonide in the morning and placebo in the evening, (C) 800 µg ciclesonide in evening and placebo in the morning, and (D) 400 µg ciclesonide in the morning and 400 µg ciclesonide in the evening in a randomized, double-blind, change-over, equivalence study with at least 7 d wash-out.
Deficiency letter for HPA-axis in children
Comments to sponsorreferring to study in children with mild persistent asthma
more than 40% of the subjects included had a 24h-urine volume < 250mlanalytical method for cortisol in urine showed no adequate validationpatient compliance could not be a assured
new study requested with children aged 4-11 y24h urine cortisol and24h serum cortisol
CDER Document: Application Number: 21-658

Summary ciclesonide (1)Early development plan – major steps
underlying disease interferes with site of absorption
“bridging” study healthy vs. patients necessary
characterisation of site-of-action deposition in addition to systemic availability needed
99mTc-marker lung deposition study needed
“classical” pharmacokinetic program, but primarily for safety reasons
established PD-model for safety assessment commonly required
HPA-axis study regulatory requirementCDER Document: Application Number: 21-658
Deficiency letter refers to basic methodologicalissues

Summary ciclesonide (2)Development plan strongly influenced by site of action
ciclesonide has also been developed as nasal formulation (“seasonal allergic rhinitis”) with (different) study package necessary
systemic availability (safety reasons)influence of underlying disease not characteriseddeposition at site of action commonly not assessed…but local tolerabilitymetabolism in human epithelial cells for activation of the pro-drug needed (and assessed in cell cultures)
Product monograph “Omnaris”, Nycomed Canada
SMPC Nycomed: “Interactions with food have not been assessed… and are unlikely with nasal corticosteroids”

rhBMP-2 for bone tissue induction
treatment of acute, open tibial shaft fractures stabilized with intramedullary nail fixationafter appropriate wound management
Recombinant human bone morphogenetic protein
within 14 days after the initial fracturepatients must be skeletally mature
above 18 yearsradiographic evidence of epiphyseal closure
no active infection at the operative site
INFUSE® bone graft induces new bone tissue at the site of implantation
Summary of safety and efficacy data, INFUSE ® bone graft, Whyeth Pharmaceutical Inc., Pennsylvania

rhBMP–2: therapeutic principle
disulfide – linked dimeric proteintwo major subunit species of 114 and 131 amino acidseach subunit glycosylated with high mannose–type glycansproduced by genetically engineered Chinese hamster ovary cell line
rhBMP-2 as active moiety
Need for local, but not systemic availability
placed to bone within 15min after preparationsolution applied to absorbable collagen spongelyophilised drug + excipients for reconstitution

rhBMP–2: absorbable collagen sponge

rhBMP-2 / ACS – pre-clinical tests
single/ multiple dose general toxicity studies after intravenous administration
no treatment related toxicityno disseminated bone formation when systemically appliedpotent bone inducing activity only at implantation site
no evidence for carcinogenicity / genotoxicity
no delayed skin sensitizationno intracutanous toxicity / no dermal irritation
no mortality / no systemic toxicity
no cell lysis (cytotoxicity tests)no hemolysis / no cellular mutagenicityhard, granular formation in muscle irritation test
Animal studies
rh BMP-2: PK in animals
extensive metabolismrapid uptake in highly perfused tissues
rapid elimination from systemic circulationf ½ (rat) : 16 minf ½ (primates) : 6.7 min
rapid renal excretion
local retention of rh BMP-2 / ACS
Studies with iv-administration and implantation
Several / comprehensive pre-clinical trials conducted

rh BMP-2: PK in animals
Retention and clearance from systemic circulation:iv administration (left) and after implantation (right)
Presentation Gerard Riedel, Wyeth-Genetics Institute
rhBMP-2: clinical trials
safety / effectiveness in patient population150 subjects per treatment group ( 2 doses of rhBMP-2 vs. control)follow-up: 12 months after wound closureclinical endpoint: fracture healingtesting for antibodies (9 / 149) antibody formation depends on location of implantation
Summary of clinical trials
No further studies in human for initial submission

rhBMP-2: deficiency letter
in-vitro investigations – tumor promotionrabbit studies - embryonic development better in-vitro release characterisationtraining plan for surgeons requested
Additional investigations requested Centre for Devices and radiological health at FDA
No further prospective clinical trials requested !
Summary: rhBMP-2
comprehensive in vitro testscomprehensive animal tests1 clinical trial with a total of 2*150 patients with efficacy and safety assessments
(Pre-)Clinical development plan
Additional post-approval studies to be performed for characterisation of immunological response
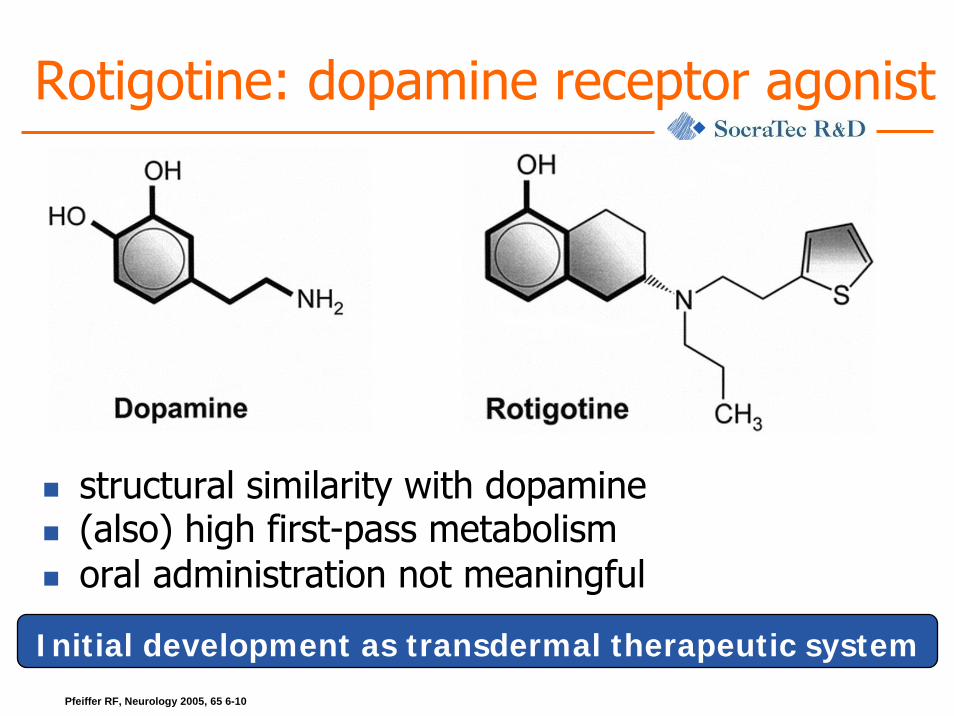
Rotigotine: dopamine receptor agonist
Initial development as transdermal therapeutic systemPfeiffer RF, Neurology 2005, 65 6-10
structural similarity with dopamine(also) high first-pass metabolismoral administration not meaningful

Rotigotine – development programSummary of study designs
sequential repeated measurement design with increasing i.v. doses in PK/PD trial (patients)
dose finding done with i.v. administrationtitration against the L-dopa dose needed
ADME with i.v. administration in healthy subjectsearly characterisation of absorption site
abdomenflankupper armshoulderthighhip
CDER Document: Application Number: 21-658
All absorption sites demonstrate adequate systemic availability
PK – characterisation of rotigotine
“Classical” PK-program due to systemic action after patch administration
single dose
multiple dosedrug-drug interactionsspecial populationsdifferent patches: bioavailability / bioequivalence

Summary: rotigotine
Relevant aspects of the clinical development program
systemic availability is prerequisite for efficacyi.v. administration for proof-of-concept study and early dose findingtransdermal administration to overcome first-pass metabolism“classical” PK program“classical” PD programcharacterisation of route of administration incl. influence of body area used for application
Conclusion: early drug-device
Development program strongly depends on necessity of systemic availability
Systemic availability means high similarity to classical development programs with additional assessment of specific influence of deviceLocally acting means comprehensive evaluation of application site and systemic exposureProgram also depends on classification “drug-device-combination” vs “medical device”
No “cookery book” approach …
… “playing field” for human pharmacology instead
Many thanks to …
Dr. Ramón Villalobos Hernández, SocraTec R&D
Katrin Jäger, SocraTec R&D


















