Evaluation of 4CEHR and Living Well Dying · PDF fileEvaluation of 4CEHR and Living Well Dying...
152
grosvenor management consulting a level 7 15 london circuit canberra act 2601 t (02) 6274 9200 abn 47 105 237 590 e [email protected] w grosvenor.com.au Evaluation of 4CEHR and Living Well Dying Well Final report 2 December 2014
Transcript of Evaluation of 4CEHR and Living Well Dying · PDF fileEvaluation of 4CEHR and Living Well Dying...

grosvenor management consulting
a level 7 15 london circuit canberra act 2601 t (02) 6274 9200 abn 47 105 237 590
w grosvenor.com.au
Evaluation of 4CEHR and Living Well Dying Well
Final report
2 December 2014

Department of Health and Human Services grosvenor management consulting 2
Table of contents
Glossary / Abbreviations ............................................................................................. 7
1 Executive Summary ............................................................................................... 9
2 Introduction ........................................................................................................... 15
2.1 Background .................................................................................................. 15
2.2 Evaluation scope ......................................................................................... 15
2.3 Terminology ................................................................................................. 15
3 Approach ............................................................................................................... 18
3.1 Review program material .......................................................................... 18
3.2 Develop evaluation criteria and questions .............................................. 19
3.3 Collect data................................................................................................... 19
3.4 Analyse results ............................................................................................ 20
3.5 Develop conclusions on future roll-out ................................................... 21
3.6 Evaluation limitations ................................................................................ 21
4 Structure of this report ......................................................................................... 22
5 Current situation and context ............................................................................. 23
5.1 Tasmania has an ageing population ......................................................... 23
5.2 Capacity on entry to RACF ........................................................................ 23
5.3 Length of stay in RACFs ............................................................................ 24
5.4 Individuals prefer not to die in hospital .................................................. 25
5.5 Low level of health literacy in Tasmania ................................................. 25
5.6 Tasmania has many internationally trained GPs ................................... 26
5.7 Shift in mindset required by many health professionals to adequately understand and appropriately care for the dying .................................. 27
5.8 Tasmanians’ families may be geographically distant ............................ 27

Department of Health and Human Services grosvenor management consulting 3
6 Living Well Dying Well ....................................................................................... 28
6.1 Description ................................................................................................... 28
6.1.1 Pilot sites ............................................................................................. 28
6.1.2 What is the Gold Standards Framework? ...................................... 29
6.1.3 Australian adaptation of the GSF .................................................... 30
6.1.4 Aims of LWDW .................................................................................. 31
6.1.5 LWDW implementation approach .................................................. 32
6.1.6 LWDW approach to advance care planning.................................. 33
6.2 Findings from the LWDW pilot ................................................................ 36
6.2.1 Project management .......................................................................... 36
6.2.2 Licencing arrangements .................................................................... 37
6.2.3 Not all project tasks were completed .............................................. 38
6.2.4 Who should be involved in advance care planning ..................... 39
6.2.5 Not everyone will be willing or have appropriate skills ............. 40
6.2.6 When to start advance care planning ............................................. 40
6.2.7 When to revisit Advance Care Plans and Advance Care Directives ............................................................................................ 41
6.2.8 Use of the LWDW approach and tools ........................................... 42
6.2.9 Feedback from residents and family members ............................. 46
6.2.10 Overall RACF view of the LWDW project ................................ 46
6.3 Outcomes of LWDW ................................................................................... 47
6.3.1 Ongoing use of the LWDW approach ............................................ 47
6.3.2 Culture change and staff empowerment ........................................ 47
6.3.3 Recognition of suffering, death and dying .................................... 48
6.3.4 Impact on hospitalisations................................................................ 48

Department of Health and Human Services grosvenor management consulting 4
7 4CEHR .................................................................................................................... 51
7.1 Background and purpose ........................................................................... 51
7.2 Development and design ........................................................................... 51
7.2.1 Timeframes ......................................................................................... 51
7.2.2 Scope and functionality .................................................................... 52
7.3.1 Successes ............................................................................................. 55
7.3.2 Barriers ................................................................................................ 56
7.4 Uptake and use ............................................................................................ 61
7.4.1 Functionality ....................................................................................... 61
7.4.2 Implementation support ................................................................... 62
7.4.3 Project certainty and stakeholder engagement ............................. 63
7.4.4 Cost to enhance and roll-out ............................................................ 64
8 Approaches to advance care planning .............................................................. 65
8.1.1 Respecting Patient Choices .............................................................. 66
8.1.2 Residential Aged Care Palliative Approach .................................. 67
8.1.3 Specialist Palliative Care and Advance Care Planning Advisory Service (Decision Assist) ................................................................... 70
8.1.4 Enhancing Aged Care through better Palliative Care .................. 71
8.1.5 Peak bodies and area specific programs ........................................ 72
8.1.6 Healthy Dying Framework .............................................................. 72
8.1.7 Medical Goals of Care Plan .............................................................. 73
8.1.8 COMPAC Guidelines ........................................................................ 74
8.1.9 TAHPC training ................................................................................. 75
8.1.10 Tasmanian HealthPathways ........................................................ 75
9 ICT support for advance care planning ............................................................ 76

Department of Health and Human Services grosvenor management consulting 5
9.1.1 Alternative ICT solutions ................................................................. 76
9.1.2 PCEHR ................................................................................................ 77
9.1.3 iPM ....................................................................................................... 77
9.1.4 DHHS ICT platform .......................................................................... 77
9.1.5 Comparison to 4CEHR ..................................................................... 78
10 A consistent approach for Tasmania ................................................................. 79
10.1 Developing a state-wide approach ........................................................... 79
10.2 Implementing a state-wide approach ...................................................... 87
11 Conclusions ........................................................................................................... 92
11.1 Is the LWDW the most appropriate approach to advance care planning in aged care for application across Tasmania? (KEQ5) ........ 92
11.2 What will it take to establish a sustainable LWDW program state-wide in Tasmania? (KEQ4) .................................................................................. 92
11.3 Does 4CEHR have the capacity to support the goals of LWDW in Tasmania? (KEQ2) ...................................................................................... 97
11.4 Is 4CEHR consistent with the approach of LWDW? (KEQ1) ............... 98
11.5 How does 4CEHR interface with the national program to implement a PCEHR? (KEQ3) ........................................................................................ 100
11.6 How can Tasmania move beyond trials and establish a state-wide program of coordinated communication for advance care planning? (KEQ6) ........................................................................................................ 100
12 Attachments ........................................................................................................ 102
12.1 Attachment A – Summary of RACF survey responses ....................... 102
12.2 Attachment B – Consultations ................................................................. 121
12.3 Attachment C - Example RACF workshop agendas ............................ 124
12.4 Attachment D - RACF Training Schedule ............................................. 129
12.5 Attachment E – LWDW implementation activities .............................. 130
12.6 Attachment F – Living Well Dying Well Content and Materials ....... 136
Department of Health and Human Services grosvenor management consulting 6
12.6.1 Illness trajectories ........................................................................ 136
12.6.2 Prognostic indicators .................................................................. 137
12.6.3 Coding and the ‘surprise question’ ........................................... 137
12.6.4 DPAG tool .................................................................................... 138
12.6.5 Clinical Pathways ........................................................................ 140
12.6.6 Clinical Action Plans ................................................................... 142
12.7 Attachment G – Evaluation activities ..................................................... 146
12.7.1 Before and after staff confidence assessment surveys ........... 146
12.7.2 After death Audits ....................................................................... 148
12.8 Attachment H – GP Training ................................................................... 152
Department of Health and Human Services grosvenor management consulting 7
Glossary / Abbreviations
4CEHR Cradle Coast Connected Care Electronic Health Record
Seven C’s Seven C’s of Care
ACAT Aged Care Assessment Team
AHHA Australian Healthcare and Hospitals Association
BAPC Better Access to Palliative Care
BSPCC Brisbane South Palliative Care Collaborative
CAP Clinical Action Plan
CCMS Collaborative Care Management Solution
COMPAC Guidelines for a Palliative Approach for Aged Care in the
Community Setting
Decision Assist Specialist Palliative Care and Advance Care Planning
Advisory Service
DHHS Department of Health and Human Services
DoH Department of Health
DoHA Department of Health and Ageing
DPAG Dignity, Preferences, Advance Care Directive, Goals of Care
(LWDW approach to advance care planning)
DSS Department of Social Services
EoLC End of Life Care
GP General Practitioner
GSF Gold Standards Framework
Hotel Staff Staff employed by a RACF to conduct hotel style services for
residents
ICT Information Communications Technology
IHI Individual Healthcare Identifier
iPM Tasmania’s hospital management information system
LWDW Living Well Dying Well
NeHTA National E-Health Transition Authority

Department of Health and Human Services grosvenor management consulting 8
NSW New South Wales
NWAHS North West Area Health Service (predecessor to THO-North
West)
NZ New Zealand
PCEHR Personally Controlled Electronic Health Record
RAC EoLCP Residential Aged Care End of Life Care Pathway
RACF Residential Aged Care Facility
RACPA Residential Aged Care Palliative Approach
RPC Respecting Patient Choices
TAHPC Tasmanian Association for Hospice and Palliative Care
THAP Tasmanian Health Assistance Package
THCI Tasmanian Health Client Index
THO Tasmanian Health Organisation
THO-North West Tasmanian Health Organisation – North West
US United States of America
Department of Health and Human Services grosvenor management consulting 9
1 Executive Summary
Grosvenor Management Consulting (Grosvenor) was engaged by Better
Access to Palliative Care (BAPC) within the Department of Health and Human
Services (DHHS) to conduct an evaluation of Living Well Dying Well (LWDW)
and the Cradle Coast Connected Care Electronic Health Record (4CEHR)
system. Both LWDW and 4CEHR were developed to improve the quality of
end of life care and support/facilitate advance care planning within
Residential Aged Care Facilities (RACFs) in North West Tasmania.
LWDW is an Australian adaption of the Gold Standards Framework (GSF)
approach to advance care planning. The LWDW project aimed to adapt and
utilise the GSF approach to implement person-centred advance care
planning processes within Tasmanian RACFs. LWDW was piloted at five
RACFs within North West Tasmania from late 2010 until early 2013.
The 4CEHR system was developed to pilot an electronic health record which
would facilitate advance care planning. The 4CEHR system was piloted in
conjunction with the LWDW project. Specifically, this system was designed
to support the development and communication of advance care planning
information between health care settings.
This evaluation was informed by a range of stakeholder consultations as well
as extensive desktop research and analysis and sought to answer the
following six Key Evaluation Questions (KEQ’s).
Is the LWDW the most appropriate approach to advanced care
planning in aged care for application across Tasmania? (KEQ5)
Overall, stakeholders were positive about LWDW, and the participating
RACFs have continued to incorporate elements of the approach into business
as usual activities. Despite this, the evaluation identified a range of
alternative approaches which are currently used within Tasmania and
mainland Australia.
Analysis revealed that the nationally supported Residential Aged Care
Palliative Approach (RACPA) to advance care planning is very similar to
LWDW. There are a number of advantages supporting use of RACPA over
LWDW:
RACPA is supported as the national approach in Australia
the RACPA tools and guidance are well developed, available online,
and free of charge (LWDW requires a licence fee and the adapted
tools are not well established)
RACPA has broader reach in Tasmania and nationally. As of
September 2014, 96 individuals from 44 Tasmanian RACFs had
attended an RACPA workshop.
there is ongoing support for the RACPA toolkit via the Department of
Health’s Decision Assist program.
Combined these advantages support RACPA as a more appropriate approach
for Tasmania.

Department of Health and Human Services grosvenor management consulting 10
What will it take to establish a sustainable LWDW program state-
wide in Tasmania? (KEQ4)
A number of key strengths and learnings from the LWDW pilot were
identified throughout the evaluation which could be used to inform the
establishment of a state-wide advance care planning program. It is believed
that these learnings would be relevant to the implementation of any advance
care planning approach and should not be considered specific to LWDW.
Learnings included, but were not limited to:
the importance of encouraging and supporting organisational change
the importance of ensuring advance care planning outputs are
recognised and accepted across health settings
roll-out of the approach should be staggered by ‘hubs’ of relevant
stakeholders within a geographical area, not setting type. These
‘hubs’ should include at least one RACF and all health providers
servicing that RACF (for example, local GPs, pharmacies, ambulance
services and hospitals)
all health settings and professionals should be engaged throughout
the development and implementation of the program
the support of senior management within the participating
organisations and all affected health care providers should be sought
at the commencement of the project
participants should be provided with clear expectations around the
project, including required resources, costs and timeframes.
Does 4CEHR have the capacity to support the goals of LWDW in
Tasmania? (KEQ2)
Note: In responding to this question, the evaluation also considered whether
4CEHR is the most appropriate system to support LWDW and advance care
planning in Tasmania.
Due to the limited 4CEHR project timeframes extensive pilot testing was not
undertaken. As a result, insufficient information is available to assess the
suitability of the system to support LWDW within Tasmania. Since
development, the 4CEHR system was not widely adopted by the participating
RACFs and is not currently being used in Tasmania.
While 4CEHR was able to deliver on some of its project aims, a number of
issues were encountered during development and implementation which
limited the uptake and use of the system. A number of system limitations
and barriers were identified during this evaluation which suggests that
4CEHR does not have the capacity to support the goals of LWDW. These
limitations and barriers would need to be rectified prior to conducting any
further pilot testing to assess the system’s suitability.
Should it be determined that 4CEHR does not have the capacity to support
LWDW (or an alternative approach), a number of other options are available
Department of Health and Human Services grosvenor management consulting 11
to support the communication of advance care planning information
including: the use of common forms; future capability of the PCEHR (based
on intended functionality) or use of the DHHS Connected Care Platform.
Is 4CEHR consistent with the approach of LWDW? (KEQ1)
While data collected as part of this evaluation suggested that 4CEHR is
consistent with the approach of LWDW, further piloting would be required to
validate and confirm this finding.
The system encompasses functionality which aligns with the LWDW
approach such as coding, the use of diagnostic tools and the storage of
enduring guardian and person responsible details. Despite this, a number of
gaps were identified in 4CEHR’s coverage of the LWDW approach.
The evaluation also identified that it is not clear if 4CEHR would be suitable
to support an LWDW approach which was adapted for different (non-RACF)
healthcare settings.
How does 4CEHR interface with the national program to implement a
PCEHR? (KEQ3)
While the 4CEHR system is technically capable of uploading information into
the PCEHR, this functionality has not been enabled. Additionally, at the time
of this evaluation, the PCEHR did not contain advance care plans. It is
unknown when this functionality will be introduced into the PCEHR and what
it will include.
How can Tasmania move beyond trials and establish a state-wide
program of coordinated communication for advance care planning?
(KEQ6)
With regard to the 4CEHR system, this evaluation identified that 4CEHR is
not ready to proceed to a state-wide rollout. During this evaluation
stakeholders identified:
features and functionality required in a state-wide approach to
advance care planning
activities and actions which would be required to successfully
implement a state-wide approach.
These actions focused on, but were not limited to; ensuring effective
communication, stakeholder engagement, and seeking support and approval
throughout the development and implementation of the approach. This was
identified as being particularly important to ensure the specific requirements
of the various health professionals are addressed and that the approach is
appropriately supported.
As a range of State and Commonwealth initiatives are gaining traction and
supporting advance care planning, the implementation a state-wide
approach should also:
take into account pre-existing programs and activities to avoid
duplication and achieve sufficient integration

Department of Health and Human Services grosvenor management consulting 12
address the acceptability of existing and alternative approaches
within a state-wide model
encourage and monitor uptake and implementation
leverage any existing relevant training materials (particularly those
approved under LWDW).
Recommendations:
It is recommended that DHHS:
1. Supports RACPA as the advance care planning approach for
Tasmanian RACFs.
2. Considers investing in a supported implementation model for RACPA
to embed and improve advance care planning in Tasmanian RACFs.
3. Ensures appropriate change management practices are utilised to
support the state-wide implementation of RACPA (or another
approach). Change management activities should focus upon
ensuring organisational readiness for the change, and draw upon the
strengths of LWDW in facilitating culture change and supporting on
the ground implementation.
4. In order to ensure the ongoing sustainability of a state-wide
approach, it is recommended that DHHS ensures the state-wide
approach:
is practical and appropriate for the capabilities and limitations of
each health care setting
is able to be supported from within the healthcare setting (ie.
within the available resources)
educates each health settings about the support which is
available, including from experts such as the Specialist Palliative
Care Service.
It is recommended that DHHS draws upon other projects such as
Enhancing Aged Care through better Palliative Care and the GSF to
inform how advance care planning can be implemented beyond
RACFs, that is, in the community and other health settings.
5. Engages sufficiently with all health settings to overcome barriers to
the recognition and use of advance care planning outputs across
health settings.
6. Engages more broadly with health professionals to implement a
system wide approach to advance care planning which includes the
community and acute care settings. DHHS should ensure all
stakeholders and health care settings are appropriately engaged and
commit to the state-wide approach. Any engagement should be
undertaken with clarity of purpose and requirements/commitments.
In particular DHHS should engage:
Department of Health and Human Services grosvenor management consulting 13
all relevant health professionals during the development and
implementation of the approach to ensure that their unique
needs are identified and appropriately addressed
senior management within affected health organisations to seek
endorsement of the implementation and ongoing use of the
approach within their facility.
7. Identify any data collection requirements during implementation of
the state-wide approach.
8. Implements a state-wide approach through a ‘hub’ model which
concurrently targets cross sector health professionals in the same
location at the same time as RACFs.
9. Considers how the hub-based implementation model can support the
sharing of experiences and practices between providers in the same
and across health settings to improve practices.
10. Integrates the roll-out of a state-wide advance care planning
approach with the BAPC framework to simultaneously raise
community awareness of advance care planning.
11. Targets those RACFs which have the greatest opportunity to improve
under the approach. This should be assessed against their willingness
to participate, quality of advance care planning and hospitalisation
rate.
12. Considers the options for supporting communication of advance care
directives in Tasmania and make a decision on the further investment
in a 4CEHR pilot. In making this decision, DHHS should analyse the
core functionality of the 4CEHR to determine whether it can be
integrated into existing systems, including the Connected Care
Platform.
If further investment in 4CEHR is supported:
it should be integrated with relevant software and platforms
it should be appropriately named in a descriptive manner and
have state-wide relevance (rather than a regional focus)
13. If further investment in 4CEHR is supported it is recommended that
DHHS:
review the existing content of 4CEHR and only retain that which
is considered to be a ‘core’ requirement by stakeholders/users
analyse the 4CEHR system to identify any duplication between its
functionality/content and existing DHHS tools and materials
provide appropriate linkages to existing DHHS materials within
the system rather than further developing the 4CEHR specific
content

Department of Health and Human Services grosvenor management consulting 14
conduct a gap analysis to identify any omissions in the system’s
ability to address the requirements of/support LWDW or the
RACPA and determine whether the inclusion of this capability is
required.
14. Actively seeks to avoid duplication and achieve integration with other
State and Commonwealth approaches to advance care planning
through the state-wide approach.
15. Reviews the appropriateness of any approved LWDW training
materials to the state-wide approach. If relevant and appropriate,
DHHS should refine and utilise these materials to support state-wide
implementation.
16. Monitors the uptake and implementation of the state-wide approach
to advance care planning to ensure it has been consistently adopted
across the various healthcare settings.

Department of Health and Human Services grosvenor management consulting 15
2 Introduction
2.1 Background
Living Well Dying Well (LWDW) and the Cradle Coast Connected Care
Electronic Health Record (4CEHR) system were developed to improve the
quality of end of life care within Residential Aged Care Facilities (RACFs) in
North West Tasmania. The LWDW approach and 4CEHR system were piloted
in five RACFs from late 2010 to early 2013.
The Australian Government has provided funding to government and non-
government agencies throughout Tasmania for the implementation of the
Better Access to Palliative Care Program (BAPC). This funding was provided
as part of the Tasmanian Health Assistance Package (THAP).
As part of BAPC, the Department of Health and Human Services (DHHS)
intend to develop a palliative care framework. This will include the
development of a Healthy Dying Framework which will underpin
improvements in the management of palliation and end of life care.
Grosvenor Management Consulting (Grosvenor) has been engaged by BAPC
within DHHS to conduct an evaluation of the LWDW pilot and the 4CEHR
system. This evaluation will inform the development and implementation of
the Healthy Dying Framework.
2.2 Evaluation scope
This evaluation is focused upon understanding the successes and challenges
of the LWDW and 4CEHR approach and implementation. Specifically, the
evaluation seeks to answer the following six evaluation questions, identified
by DHHS:
1. Is 4CEHR consistent with the approach of LWDW?
2. Does 4CEHR have the capacity to support the goals of LWDW in
Tasmania?
3. How does 4CEHR interface with the national program to implement a
PCEHR?
4. What will it take to establish a sustainable LWDW program state-wide
in Tasmania?
5. Is the LWDW the most appropriate approach to advanced care
planning in aged care for application across Tasmania?
6. How can Tasmania move beyond trials and establish a state-wide
program of coordinated communication for advanced care planning?
2.3 Terminology
There is a range of terminology used in relation to end of life care and
inconsistency in its use. The lack of consistency causes confusion and a lack

Department of Health and Human Services grosvenor management consulting 16
of clarity. These issues were still apparent among stakeholders consulted
during the evaluation.
This was raised as a key issue in the 2011 National Framework for Advance
Care Directives. The Framework recommended the adoption of the following
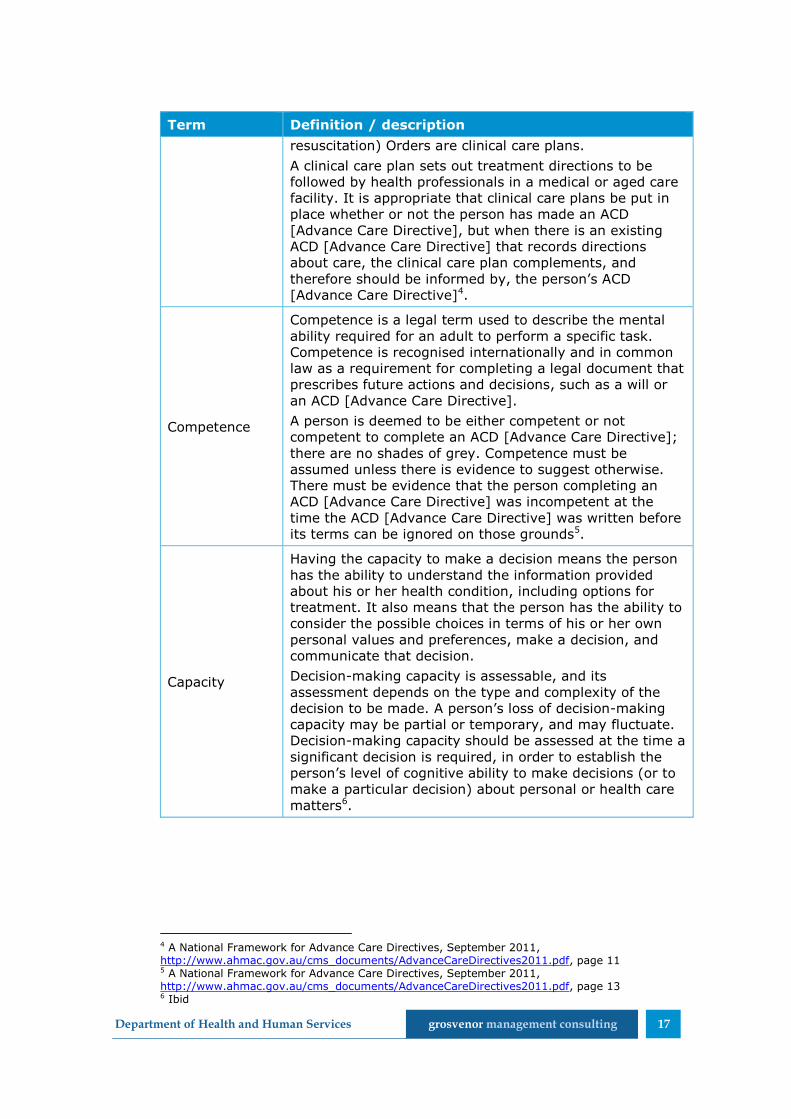
lexicon nationally (Table 1).This report is consistent with the recommended
lexicon.
Table 1 National lexicon for Advance Care Directives
Term Definition / description
Advance Care
Directive
ACDs [Advance Care Directives] are one way of formally
recording an advance care plan. An ACD [Advance Care
Directive] is a type of written advance care plan
recognised by common law or authorised by legislation
that is completed and signed by a competent adult. An
ACD [Advance Care Directive] can record the person’s
preferences for future care and appoint an SDM
[substitute decision maker] to make decisions about
health care and personal life management. ACDs [Advance
Care Directives] are focused on the future care of a person
not on the management of his or her assets1.
Advance care
planning
Advance care planning is a process of planning for future
health and personal care whereby the person’s values,
beliefs and preferences are made known so they can guide
decision-making at a future time when that person cannot
make or communicate his or her decisions.
Formal advance care planning programs usually operate
within a health, institutional or aged care setting after a
life-limiting condition has been diagnosed, frequently
requiring the assistance of trained professionals. However,
people can choose to discuss their advance care plans in
an informal family setting2.
Advance care
plan
An advance care planning discussion will often result in an
advance care plan. Advance care plans state preferences
about health and person care and preferred health
outcomes. They may be made on the person’s behalf, and
should be prepared from the person’s perspective to guide
decisions about care.
There are many ways of recording an advance care plan
including oral and written versions3.
Clinical care
plan
ACDs [Advance Care Directives] written by a person are
distinct from clinical care or treatment plans written by
health care professionals for a patient. Resuscitation
plans, treatment plans and No CPR (cardiopulmonary
1 A National Framework for Advance Care Directives, September 2011, http://www.ahmac.gov.au/cms_documents/AdvanceCareDirectives2011.pdf, page 10 2 A National Framework for Advance Care Directives, September 2011, http://www.ahmac.gov.au/cms_documents/AdvanceCareDirectives2011.pdf, page 9 3 A National Framework for Advance Care Directives, September 2011, http://www.ahmac.gov.au/cms_documents/AdvanceCareDirectives2011.pdf, page 9-10
Department of Health and Human Services grosvenor management consulting 17
Term Definition / description
resuscitation) Orders are clinical care plans.
A clinical care plan sets out treatment directions to be
followed by health professionals in a medical or aged care
facility. It is appropriate that clinical care plans be put in
place whether or not the person has made an ACD
[Advance Care Directive], but when there is an existing
ACD [Advance Care Directive] that records directions
about care, the clinical care plan complements, and
therefore should be informed by, the person’s ACD
[Advance Care Directive]4.
Competence
Competence is a legal term used to describe the mental
ability required for an adult to perform a specific task.
Competence is recognised internationally and in common
law as a requirement for completing a legal document that
prescribes future actions and decisions, such as a will or
an ACD [Advance Care Directive].
A person is deemed to be either competent or not
competent to complete an ACD [Advance Care Directive];
there are no shades of grey. Competence must be
assumed unless there is evidence to suggest otherwise.
There must be evidence that the person completing an
ACD [Advance Care Directive] was incompetent at the
time the ACD [Advance Care Directive] was written before
its terms can be ignored on those grounds5.
Capacity
Having the capacity to make a decision means the person
has the ability to understand the information provided
about his or her health condition, including options for
treatment. It also means that the person has the ability to
consider the possible choices in terms of his or her own
personal values and preferences, make a decision, and
communicate that decision.
Decision-making capacity is assessable, and its
assessment depends on the type and complexity of the
decision to be made. A person’s loss of decision-making
capacity may be partial or temporary, and may fluctuate.
Decision-making capacity should be assessed at the time a
significant decision is required, in order to establish the
person’s level of cognitive ability to make decisions (or to
make a particular decision) about personal or health care
matters6.
4 A National Framework for Advance Care Directives, September 2011, http://www.ahmac.gov.au/cms_documents/AdvanceCareDirectives2011.pdf, page 11 5 A National Framework for Advance Care Directives, September 2011, http://www.ahmac.gov.au/cms_documents/AdvanceCareDirectives2011.pdf, page 13 6 Ibid
Department of Health and Human Services grosvenor management consulting 18
3 Approach
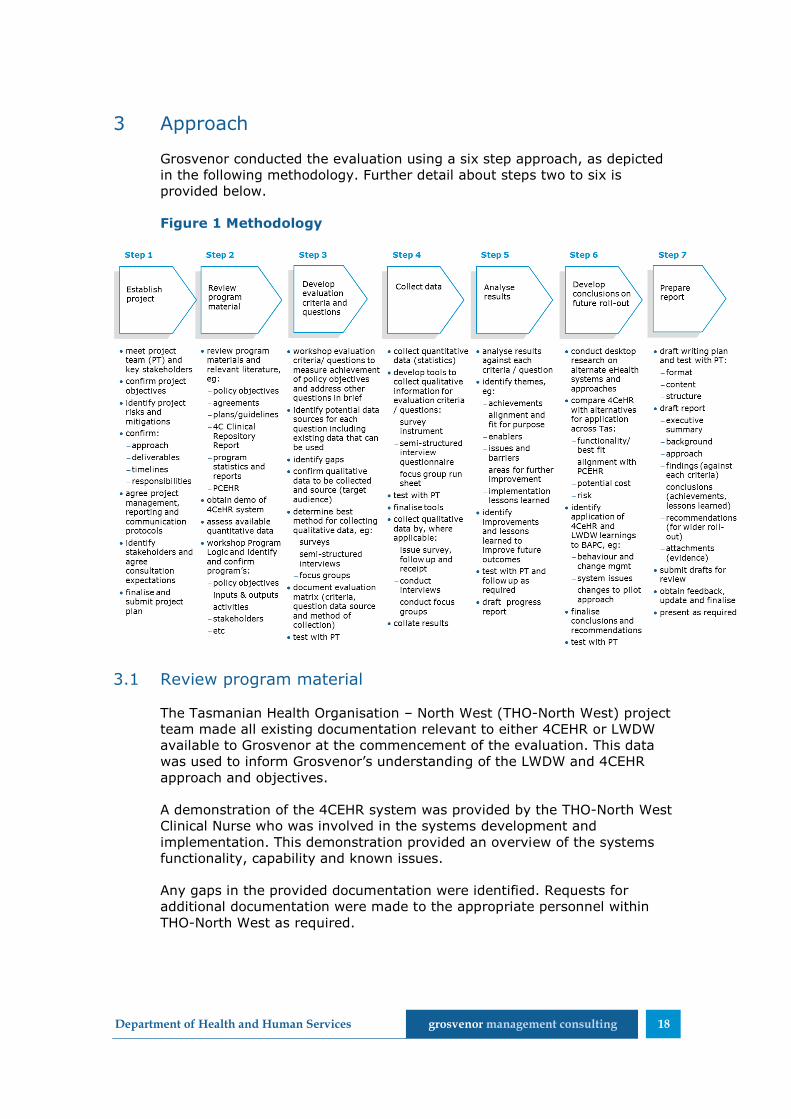
Grosvenor conducted the evaluation using a six step approach, as depicted
in the following methodology. Further detail about steps two to six is
provided below.
Figure 1 Methodology
3.1 Review program material
The Tasmanian Health Organisation – North West (THO-North West) project
team made all existing documentation relevant to either 4CEHR or LWDW
available to Grosvenor at the commencement of the evaluation. This data
was used to inform Grosvenor’s understanding of the LWDW and 4CEHR
approach and objectives.
A demonstration of the 4CEHR system was provided by the THO-North West
Clinical Nurse who was involved in the systems development and
implementation. This demonstration provided an overview of the systems
functionality, capability and known issues.
Any gaps in the provided documentation were identified. Requests for
additional documentation were made to the appropriate personnel within
THO-North West as required.

Department of Health and Human Services grosvenor management consulting 19
3.2 Develop evaluation criteria and questions
The evaluation addressed six key evaluation questions as outlined in the
original RFQ. Grosvenor analysed these questions to determine their
appropriateness and to identify data requirements and potential data
sources.
A workshop was held with the evaluation steering committee on 4 August
2014 to discuss and confirm:
Grosvenor’s understanding of the LWDW and 4CEHR
the evaluation questions
data to be collected
required data collection methods and activities.
3.3 Collect data
Data was collected through a range of stakeholder consultations and
desktop. Specific data collection activities included:
interviews and focus groups with key stakeholders
survey of RACFs throughout Tasmania (RACF Survey)
collection of documentation from the project team, stakeholders and
online research.
Focus Groups
Focus Groups were conducted at four of the five Residential Aged Care
Facilities which piloted the LWDW program and 4CEHR system. These focus
groups involved key staff from each RACF who had been involved in the
implementation and use of both LWDW and 4CEHR.
Interviews
A total of 22 interviews were conducted to inform the evaluation. This
included a range of face to face and telephone interviews with stakeholders
from the following groups:
RACF residents
families of existing and/or previous RACF residents
DHHS and THO-North West (including IT, My Aged Care, Home and
Community Care (HACC) and staff involved in 4CEHR and/or LWDW)
Cradle Coast Authority
Health Care Providers (including General Practitioners (GPs), RACF
management and Community Nurses)

Department of Health and Human Services grosvenor management consulting 20
UTAS personnel involved in LWDW, 4CEHR and/or palliative care
research
Tasmania Medicare Local (TML)
Tasmanian Association for Hospice and Palliative Care (TAHPC).
Where individuals were unable to participate in an interview written
feedback was requested. This was provided by two stakeholders from:
Primary Health Services within TML
Department of Health.
Future stakeholders workshop
Stakeholders who had not been directly involved in either 4CEHR or LWDW,
but would be impacted by any state-wide changes to advance care planning
were invited to attend a future stakeholders workshop. Three stakeholders
participated in this workshop.
Survey
An online survey was distributed to all RACFs who are members of Aged and
Community Services Tasmania (ACST). A total of 16 survey responses were
received. A summary of the survey responses is included in Attachment A
Desktop research
Grosvenor undertook desktop research to identify additional information
about the Tasmanian context and health care environment, 4CEHR and
LWDW.
Full details of the consultations conducted to inform this evaluation are
included in Attachment B.
3.4 Analyse results
All collected data was analysed against the six key evaluation questions to
confirm the appropriateness of the collected information. This allowed gaps
to be identified, informing the collection of additional data as required.
A series of key themes and findings were identified from the consultations
and data collection activities. Initial themes and findings were documented
in the project’s progress report. The progress report grouped the findings
against:
LWDW
4CEHR
alternative models and approaches
developing a state-wide approach.

Department of Health and Human Services grosvenor management consulting 21
Successes and barriers were identified for each theme.
3.5 Develop conclusions on future roll-out
Desktop research was undertaken to identify any alternative eHealth
systems and approaches with a similar focus to the 4CEHR system. This
research sought to identify both domestic and international systems.
The functionality of the identified systems was compared to 4CEHR to
determine whether an alternative approach would be suitable in Tasmania.
Conclusions and recommendations for the evaluation were developed based
on the analysis of the collected data and alternative systems and
approaches. The conclusions are structured around the six key evaluation
questions.
3.6 Evaluation limitations
A number of limitations were encountered during this evaluation which
should be considered when reading/utilising this report.
Limited GP engagement
Despite efforts to engage GPs during the consultation period, feedback and
input was only provided by a small number of GPs. This included feedback
from GPs working in General Practice and those working in a hospital and
other specialist healthcare settings. While the views expressed by these GPs
have been used to inform this evaluation, they should not be considered as
exhaustive or representative of all GPs.
Limited resident and family engagement
The four RACFs which were engaged as part of the consultation process were
asked to identify current residents and/or the family members of residents
who had been involved in the pilot to provide feedback.
Only one RACF was able to identify, and arrange for, consultations with
residents and family members. This resulted in a lower number of
consultations with these groups compared to what was originally planned.
The RACFs noted that:
the vast majority of residents who had been involved in the pilot had
passed away
there was limited (or no) ongoing engagement with the families of
former residents.
Incomplete LWDW data
The available data and documentation about the LWDW program was often
incomplete and/or in draft format. As a result, there were some gaps and
inconsistencies in the available data and program information/tools. While
every effort has been made to ensure that the LWDW information presented
in this report is accurate, some inconsistencies or gaps may be present.

Department of Health and Human Services grosvenor management consulting 22
4 Structure of this report
This report is structured around the following key topics:
current situation and context (Section 5)
Living Well Dying Well (Section 6)
4CEHR system (Section 7)
approaches to advance care planning (Section 8)
ICT support for advance care planning (Section 9)
a consistent approach for Tasmania (Section 10)
conclusions and recommendations (Section 11).

Department of Health and Human Services grosvenor management consulting 23
5 Current situation and context
There are a range of contextual factors relating to Tasmania’s demographics
and health care system which demonstrate the relevance and need for a
focus on end of life care. Those consulted with also raised other situational
and contextual issues which need to be addressed to facilitate dying well.
This section presents an overview of these issues and considerations.
5.1 Tasmania has an ageing population
The 2011 census identified that Tasmania has the oldest median age (40.4
years) of all Australian states and territories. The median age increased from
39 years in 2006 and is much higher than the 2011 Australian median age of
37 years7.
The Tasmanian population has been ageing for some time. Between 2001
and 2011 the number of Tasmanians aged 65 years or above increased by
27%, while those aged 80 years or above increased by 35%8.
In 2011, 16.3% (1 in 6) of the Tasmanian population were aged 65 years or
over. Projections detailed by the Council of the Ageing in the report ‘Facing
the Future’ suggest that the Tasmanian population will continue to age over
the next few decades. The proportion of Tasmanians aged over 65 is
projected to increase from 1 in 6 (2011) to 1 in 4 (2030)9.
Table 2 Proportion of the Tasmanian population aged 65 or above
2011 2020 2030
1 in 6 1 in 5 1 in 4
5.2 Capacity on entry to RACF
Elderly Tasmanians are remaining in their own homes for longer, with 79%
of Tasmanians aged 80 years or above residing in their own homes in 2011.
The Australian average age of admission to an RACF increased between
1997 and 2009 from 82.8 to 84.3 years for a female and 79.5 to 81.6 years
for a male10.
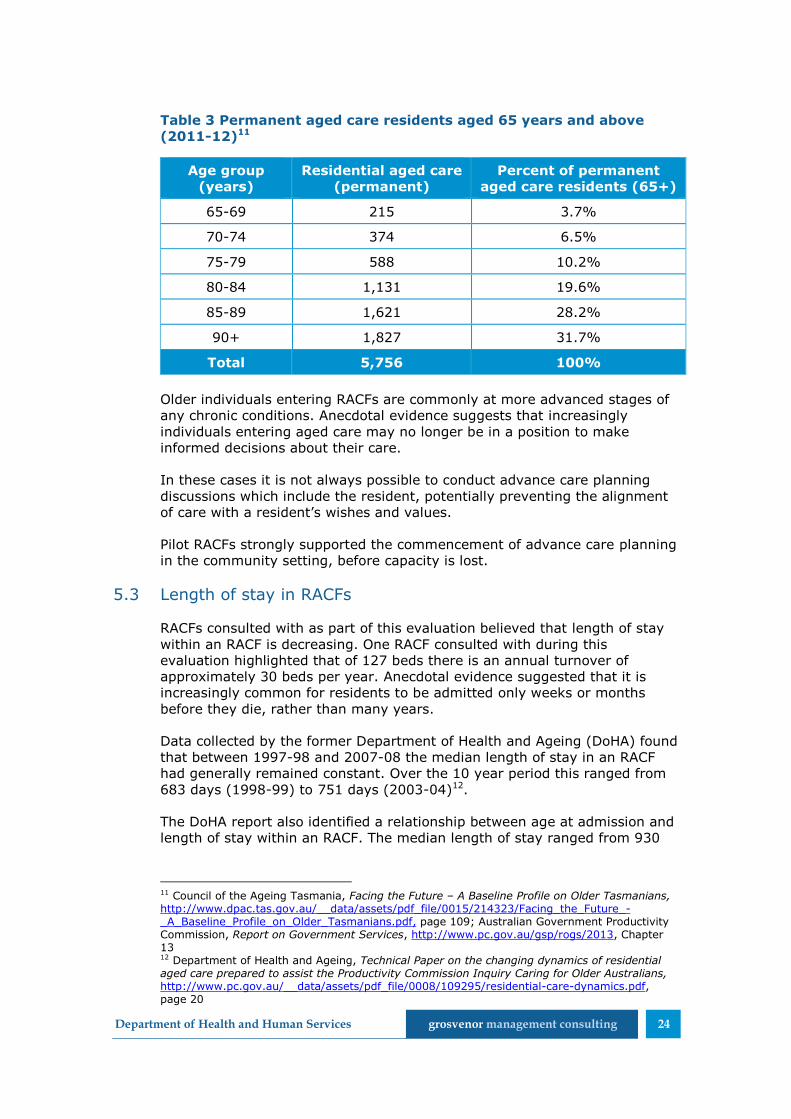
As shown in Table 3 over 50% of permanent aged care residents in
Tasmania in 2011-12 were aged 85 years or above.
7 Australian Bureau of Statistics, Census Data, http://www.censusdata.abs.gov.au/ 8 Council of the Ageing Tasmania, Facing the Future – A Baseline Profile on Older Tasmanians, http://www.dpac.tas.gov.au/__data/assets/pdf_file/0015/214323/Facing_the_Future_-_A_Baseline_Profile_on_Older_Tasmanians.pdf 9 Ibid 10 Department of Health and Ageing, Technical Paper on the changing dynamics of residential aged care prepared to assist the Productivity Commission Inquiry Caring for Older Australians, http://www.pc.gov.au/__data/assets/pdf_file/0008/109295/residential-care-dynamics.pdf, page 17
Department of Health and Human Services grosvenor management consulting 24
Table 3 Permanent aged care residents aged 65 years and above
(2011-12)11
Age group
(years)
Residential aged care
(permanent)
Percent of permanent
aged care residents (65+)
65-69 215 3.7%
70-74 374 6.5%
75-79 588 10.2%
80-84 1,131 19.6%
85-89 1,621 28.2%
90+ 1,827 31.7%
Total 5,756 100%
Older individuals entering RACFs are commonly at more advanced stages of
any chronic conditions. Anecdotal evidence suggests that increasingly
individuals entering aged care may no longer be in a position to make
informed decisions about their care.
In these cases it is not always possible to conduct advance care planning
discussions which include the resident, potentially preventing the alignment
of care with a resident’s wishes and values.
Pilot RACFs strongly supported the commencement of advance care planning
in the community setting, before capacity is lost.
5.3 Length of stay in RACFs
RACFs consulted with as part of this evaluation believed that length of stay
within an RACF is decreasing. One RACF consulted with during this
evaluation highlighted that of 127 beds there is an annual turnover of
approximately 30 beds per year. Anecdotal evidence suggested that it is
increasingly common for residents to be admitted only weeks or months
before they die, rather than many years.
Data collected by the former Department of Health and Ageing (DoHA) found
that between 1997-98 and 2007-08 the median length of stay in an RACF
had generally remained constant. Over the 10 year period this ranged from
683 days (1998-99) to 751 days (2003-04)12.
The DoHA report also identified a relationship between age at admission and
length of stay within an RACF. The median length of stay ranged from 930
11 Council of the Ageing Tasmania, Facing the Future – A Baseline Profile on Older Tasmanians, http://www.dpac.tas.gov.au/__data/assets/pdf_file/0015/214323/Facing_the_Future_-_A_Baseline_Profile_on_Older_Tasmanians.pdf, page 109; Australian Government Productivity Commission, Report on Government Services, http://www.pc.gov.au/gsp/rogs/2013, Chapter 13 12 Department of Health and Ageing, Technical Paper on the changing dynamics of residential aged care prepared to assist the Productivity Commission Inquiry Caring for Older Australians, http://www.pc.gov.au/__data/assets/pdf_file/0008/109295/residential-care-dynamics.pdf, page 20

Department of Health and Human Services grosvenor management consulting 25
days for those admitted between 0 and 59 years to 570 days for those
admitted at over 90 years of age.
As the length of stay within RACFs decreases, staff will have less time to
develop an understanding of the resident, making it increasingly important
to conduct advance care planning at, or soon after, admission.
5.4 Individuals prefer not to die in hospital
Studies have shown that many Australians have a preference to die in their
own homes13,14,15. A survey conducted by Palliative Care Australia found that
68% of respondents wanted to die in their own home, with only 13%
preferring to die in hospital.
Despite individual’s preferences to die at home, approximately 54% of
Australians currently die in hospitals. Of the remainder, 16% die in their own
homes, 20% in a hospice and 10% in an RACF16.
This suggests a need to ensure that appropriate care, processes and
systems are in place to support individuals to die in their preferred place and
avoid unnecessary hospitalisation at the end of life.
5.5 Low level of health literacy in Tasmania
Tasmanians have low levels of health literacy. In 2006, ABS data found that
63% of Tasmanians aged 15-74 did not have adequate health literacy to
meet the demands of everyday life. This was above the Australian figure of
59%17.
An individual’s level of health literacy informs their ability to understand
medical terms, conditions and treatments. Low health literacy may prevent a
person from comprehending and participating in discussions about their
medical conditions and/or treatments which they are receiving. This can
impact upon their ability to make informed decisions about their preferred
care.
13 Department of Health, The National Palliative Care Strategy – Supporting Australians to live well at the end of life, Introduction, http://www.health.gov.au/internet/publications/publishing.nsf/Content/ageing-npcs-2010-toc~ageing-npcs-2010-introduction 14 Palliative Care Australia, Australians aren’t ‘prepared’ to die – survey, http://www.palliativecare.org.au/Portals/46/NPCW/2014/140520%20NPCW%20Media%20Release%20-%20Consumer%20Media%20%28FINAL%29.pdf, page 4 15 Care Search, Preferred Place of Death, http://www.caresearch.com.au/caresearch/WhatisPalliativeCare/UnderstandingPalliativeCare/PreferredPlaceofDeath.aspx 16 Department of Health, The National Palliative Care Strategy – Supporting Australians to live well at the end of life, Introduction, http://www.health.gov.au/internet/publications/publishing.nsf/Content/ageing-npcs-2010-toc~ageing-npcs-2010-introduction 17 Department of Health and Human Services, Communication and Health Literacy, http://www.dhhs.tas.gov.au/about_the_department/your_care_your_say/publications/health_literacy; Australian Bureau of Statistics, 4233.0 – Health Literacy Australia 2006, http://www.abs.gov.au/AUSSTATS/[email protected]/Latestproducts/4233.0Main%20Features12006?opendocument&tabname=Summary&prodno=4233.0&issue=2006&num=&view=
Department of Health and Human Services grosvenor management consulting 26
The low level of health literacy has implications for the communication of all
health care information, including advance care planning.
5.6 Tasmania has many internationally trained GPs
Under section 19AB of the Health Insurance Act 1973 overseas trained
doctors and foreign graduates of accredited medical schools are subject to
Medicare number provider restrictions. These doctors and graduates are
required to work in designated districts of workforce shortage to access
Medicare benefits, referred to as the 10 year moratorium period.
The Rural Health Workforce Strategy (RHWS) Incentive Program enables
overseas trained doctors and foreign graduates to access scaling discounts.
These scaling discounts allow overseas trained doctors and foreign graduates
to reduce the 10 year restriction period to access Medicare benefits by
working in regional, rural and remote areas. As many areas of Tasmania are
classed as ‘outer regional’ (including North West Tasmania), doctors willing
to practice in these areas can reduce the moratorium from 10 to seven
years, incentivising practice in these areas18.
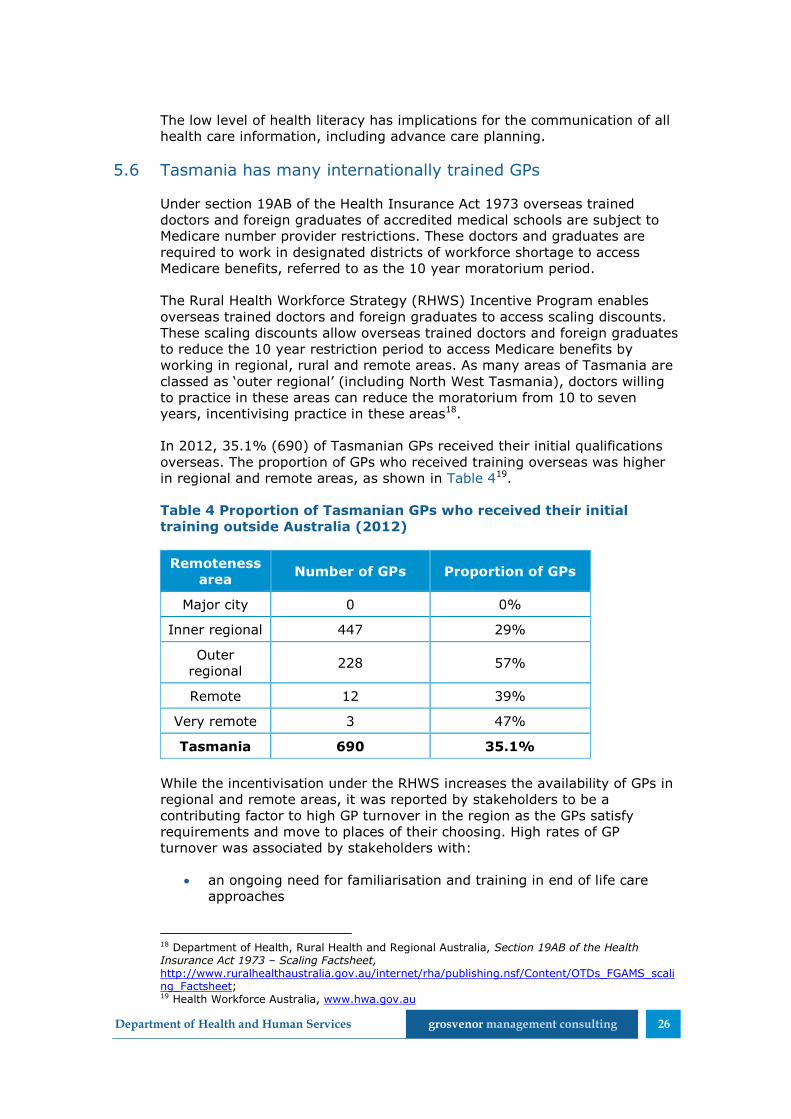
In 2012, 35.1% (690) of Tasmanian GPs received their initial qualifications
overseas. The proportion of GPs who received training overseas was higher
in regional and remote areas, as shown in Table 419.
Table 4 Proportion of Tasmanian GPs who received their initial
training outside Australia (2012)
Remoteness
area Number of GPs Proportion of GPs
Major city 0 0%
Inner regional 447 29%
Outer
regional 228 57%
Remote 12 39%
Very remote 3 47%
Tasmania 690 35.1%
While the incentivisation under the RHWS increases the availability of GPs in
regional and remote areas, it was reported by stakeholders to be a
contributing factor to high GP turnover in the region as the GPs satisfy
requirements and move to places of their choosing. High rates of GP
turnover was associated by stakeholders with:
an ongoing need for familiarisation and training in end of life care
approaches
18 Department of Health, Rural Health and Regional Australia, Section 19AB of the Health Insurance Act 1973 – Scaling Factsheet, http://www.ruralhealthaustralia.gov.au/internet/rha/publishing.nsf/Content/OTDs_FGAMS_scaling_Factsheet; 19 Health Workforce Australia, www.hwa.gov.au

Department of Health and Human Services grosvenor management consulting 27
individuals potentially having only a short history with their GP.
5.7 Shift in mindset required by many health professionals to
adequately understand and appropriately care for the dying
It is acknowledged that the skills and capability of health professionals to
provide high quality end of life care requires improvement. In particular,
health professionals may:
not adequately understand the dying process
be unfamiliar with care approaches for the last year of life
be uncomfortable holding discussions with patients and families about
death and dying
lack the skills to effectively communicate about death and dying
be unable or unwilling to manage care in a person-centred way either
due to structural barriers or differences in values and attitudes.
Health professionals may have difficulties reconciling their own, and their
patient’s, values and attitudes in relation to death and dying and therefore
effectively planning care which meets the patient’s needs.
The traditional medical paradigm focuses on saving or extending life. The
transition from treating a patient’s condition to managing their symptoms
can be a significant change in focus for a health professional, which some
have identified as being confronting.
“One of the fundamental barriers to achieving quality care at the end
of life arises from the inability or unwillingness of health professionals
to recognise those who are dying and treat them appropriately… Health
professionals have the ability and the strongly held desire to treat and
cure. Our systems of care and training limit our capacity to recognise
that a person is dying.”20
5.8 Tasmanians’ families may be geographically distant
The families of some elderly Tasmanians reside in mainland Australia or
overseas. As a result of the geographic distance, communication may be less
frequent and families may be unaware or have incomplete knowledge of the
individual’s wishes and preferences for end of life care.
This can present difficulties when wishes are known to RACF staff, or locally
residing friends, which differ from familial wishes, particularly when they
have not been documented and/or there is no clear substitute decision–
maker.
20 Palliative Care Australia, Health System Reform and Care at the End of Life: a Guidance Document, http://www.palliativecare.org.au/Portals/46/Policy/Health%20system%20reform%20-%20guidance%20document%20-%20web%20version.pdf, page 33

Department of Health and Human Services grosvenor management consulting 28
6 Living Well Dying Well
6.1 Description
The Living Well Dying Well (LWDW) project commenced in August 2010 as a
pilot implementation of the UK Gold Standards Framework (GSF) by the
North West Area Health Service (NWAHS) in Tasmania.
The LWDW project aimed to achieve the implementation of person-centred
advance care planning processes. It also sought to promote the delivery of
care during the last year of life which upholds a resident’s dignity by
respecting their values, wishes and preferences.
LWDW combines elements of the GSF program with tailored content and
materials to provide an integrated approach to end of life care. LWDW
includes the following elements:
Australian adaptation of the GSF
DPAG process (Dignity, Preferences, Advance Care Plan, Goals of
Care) used for advance care planning
supportive and palliative pathways and Clinical Action Plans (CAPs)
4CEHR system to support the approach.
The 4CEHR system is discussed separately in section 7 of this report.
The project was delivered to five RACFs, and involved education to GPs with
patients in those facilities.
6.1.1 Pilot sites
RACFs in North West Tasmania were able to apply to be one of the five pilot
sites for LWDW. The following five RACFs were selected from the initial
round of applications:
Umina Park, Burnie
Meercroft Care, Devonport
Baptcare Karingal, Devonport
Mount St Vincents, Ulverstone
Wynyard Care Centre, Wynyard (formerly known as Ibis Care)
Due to internal changes in leadership, Umina Park was unable to continue
with the pilot and withdrew from the project. Following the withdrawal of
Umina Park, Emmerton Park in Smithton commenced the project in March
2012.
Despite expressing significant interest in participating in the LWDW project,
Emmerton Park was not initially accepted as the project team felt that the
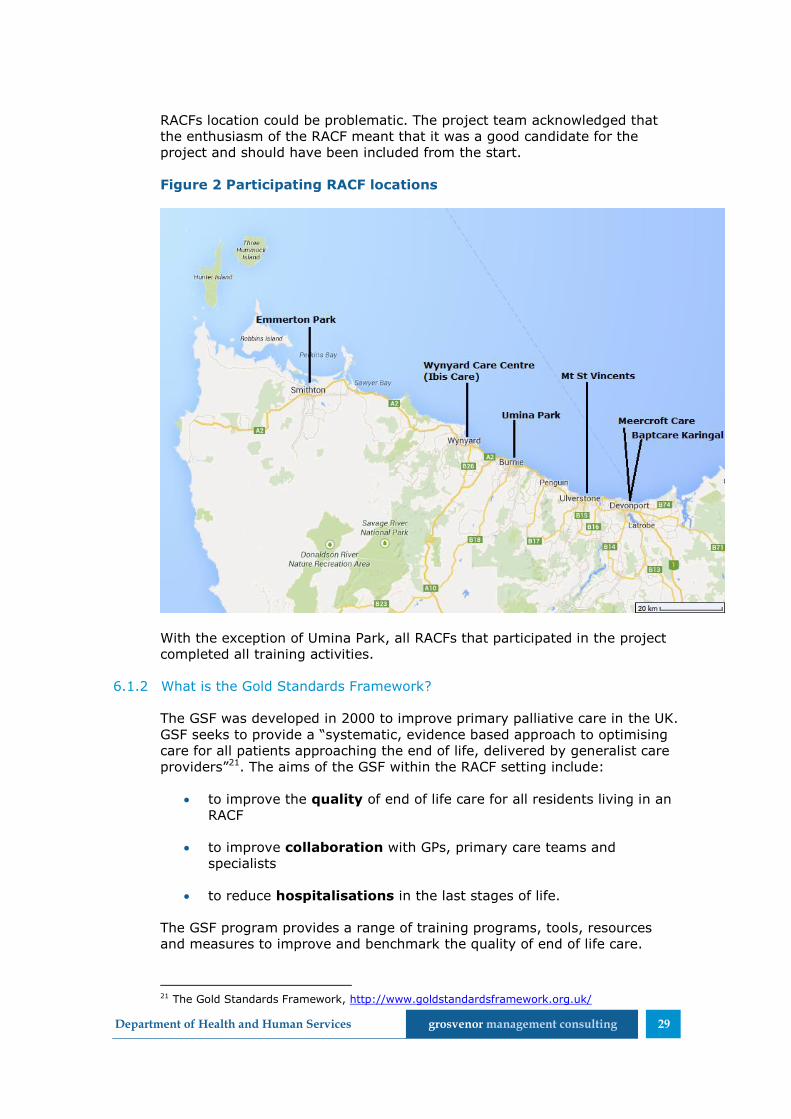
Department of Health and Human Services grosvenor management consulting 29
RACFs location could be problematic. The project team acknowledged that
the enthusiasm of the RACF meant that it was a good candidate for the
project and should have been included from the start.
Figure 2 Participating RACF locations
With the exception of Umina Park, all RACFs that participated in the project
completed all training activities.
6.1.2 What is the Gold Standards Framework?
The GSF was developed in 2000 to improve primary palliative care in the UK.
GSF seeks to provide a “systematic, evidence based approach to optimising
care for all patients approaching the end of life, delivered by generalist care
providers”21. The aims of the GSF within the RACF setting include:
to improve the quality of end of life care for all residents living in an
RACF
to improve collaboration with GPs, primary care teams and
specialists
to reduce hospitalisations in the last stages of life.
The GSF program provides a range of training programs, tools, resources
and measures to improve and benchmark the quality of end of life care.
21 The Gold Standards Framework, http://www.goldstandardsframework.org.uk/

Department of Health and Human Services grosvenor management consulting 30
Since 2000 the program has expanded to include programs for a range of
health care settings including hospices, primary care, care homes (RACFs)
and hospitals. The program is now widely used in the UK, and has been
piloted in a range of countries including Australia (through LWDW), New
Zealand, the USA, Canada, Belgium and Holland22.
GSF tools and processes are available to organisations under license. While
some materials and tools are provided for free non-commercial use in UK
National Health Service primary care, organisations outside the UK must
apply for use, and pay a licence fee.
6.1.3 Australian adaptation of the GSF
The LWDW project tailored the GSF content and tools for use within the
Australian context. Specific details of the adaptations were not recorded in
the project documentation made available. Nor were the original GSF
materials available for comparison to the LWDW materials.
During consultation the following general areas of adaptation were
identified:
changes to reflect different language use, health systems and legal
frameworks
alterations to the training package, including a reduction in content
detail, changes to clinical assessments and addition of an
introductory workshop.
The GSF care home training program includes four workshops spaced over
approximately 12 months and covering the seven core concepts of care (the
“Seven C’s”). Table 5 details the delivery of the Seven C’s within the LWDW
RACF workshops.
Table 5 Seven C's of Care
Communication
(C1)
LWDW
workshop 2
and 3
identify residents in the final 6-12
months of life
discuss patients at regular team
meetings
code residents to identify illness
stage
discuss proactive planning,
anticipate needs, prioritise care
offer and conduct advance care
planning discussions
Coordination
(C2)
LWDW
workshop 2
coordinate care across boundaries
share information and planning
between staff and GPs
align care with resident’s dignity and
preferences
22 The Gold Standards Framework, History, http://www.goldstandardsframework.org.uk/history

Department of Health and Human Services grosvenor management consulting 31
Control of
Symptoms (C3)
LWDW
workshop 3
assess physical symptoms
anticipate possible symptoms and
possible consequences of
deterioration with, for example,
anticipatory prescribing
use of CAPs
Continuity of
Care (C4)
LWDW
workshop 3
goals of comfort
prevention of crisis
outside hours care
anticipatory prescribing
Continued
Learning (C5)
LWDW
workshop 4
use event analysis to review deaths,
admissions and other events
identify and plan for learning needs
consider ongoing audits to clarify
areas requiring further improvement
Carer Support
(C6)
LWDW
workshop 4
inform and include carers as ‘care
partners’ if desired
discuss carer’s own needs and
concerns
develop bereavement plan after
every death
identify ‘pathological’ grief
debrief and support yourselves and
staff
Care in the
dying phase
(C7)
LWDW
workshop 4
recognise end of life
conduct anticipatory prescribing
keep carers informed
consider spiritual needs
The first LWDW workshop was introductory and aimed to identify concerns
about the program as well as desired outcomes.
The fifth LWDW workshop covers embedding and sustaining the approach
and explores quality of life, delirium, depression, demoralisation and
dementia. Example agendas for LWDW workshops two to five are included at
Attachment C.
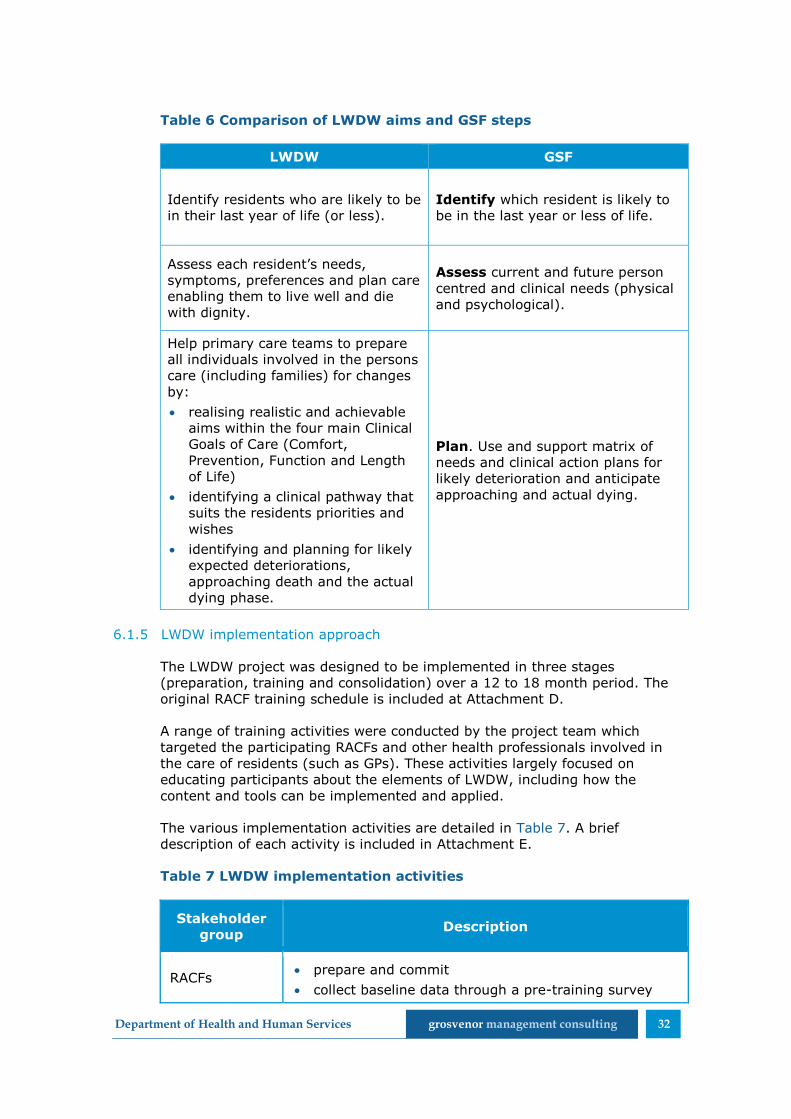
6.1.4 Aims of LWDW
While the aims of the two programs are similar in nature and concept, the
GSF aims are articulated in a much a simpler manner, focusing on the
outcomes that the program is seeking to achieve. The LWDW aims can be
directly aligned with the three GSF steps; identify, assess and plan (as
shown in Table 6).
Department of Health and Human Services grosvenor management consulting 32
Table 6 Comparison of LWDW aims and GSF steps
LWDW GSF
Identify residents who are likely to be
in their last year of life (or less).
Identify which resident is likely to
be in the last year or less of life.
Assess each resident’s needs,
symptoms, preferences and plan care
enabling them to live well and die
with dignity.
Assess current and future person
centred and clinical needs (physical
and psychological).
Help primary care teams to prepare
all individuals involved in the persons
care (including families) for changes
by:
realising realistic and achievable
aims within the four main Clinical
Goals of Care (Comfort,
Prevention, Function and Length
of Life)
identifying a clinical pathway that
suits the residents priorities and
wishes
identifying and planning for likely
expected deteriorations,
approaching death and the actual
dying phase.
Plan. Use and support matrix of
needs and clinical action plans for
likely deterioration and anticipate
approaching and actual dying.
6.1.5 LWDW implementation approach
The LWDW project was designed to be implemented in three stages
(preparation, training and consolidation) over a 12 to 18 month period. The
original RACF training schedule is included at Attachment D.
A range of training activities were conducted by the project team which
targeted the participating RACFs and other health professionals involved in
the care of residents (such as GPs). These activities largely focused on
educating participants about the elements of LWDW, including how the
content and tools can be implemented and applied.
The various implementation activities are detailed in Table 7. A brief
description of each activity is included in Attachment E.
Table 7 LWDW implementation activities
Stakeholder
group Description
RACFs prepare and commit
collect baseline data through a pre-training survey

Department of Health and Human Services grosvenor management consulting 33
Stakeholder
group Description
about RACF culture and conducting after death audits
introductory workshop
four GSF ‘gear’ workshops, implementation and
consolidation (note, these sessions included the DPAG
training)
ongoing training and support
after death audits (ongoing)
review (conducted following each workshop)
GPs GP engagement
GP training (after hours workshops)
Coordinators action learning groups
Consumers
and
Community
engagement
community forums
LWDW was primarily developed and implemented by a DHHS palliative care
nurse and palliative care doctor. A range of clinical, administrative and
project staff from the other participating organisations also provided support
to the project. All project management tasks were undertaken by the clinical
staff who reported directly to the CEO of the NWAHS.
The clinical staff were involved in all aspects of the LWDW project, including
developing the approach, refining content, delivering training and providing
ongoing support to the RACFs.
The development of the 4CEHR system was managed and delivered by the
same, broader project team in conjunction with a contracted service
provider.
Stakeholders identified that there was poor communication between the
LWDW and 4CEHR project team members and that they were often working
to separate timeframes.
6.1.6 LWDW approach to advance care planning
LWDW is an approach to delivering advanced care planning in the RACF
setting. A range of content and materials have been developed and adapted
from GSF as part of LWDW. This content specifically seeks to support the
three LWDW aims, as shown in Table 8.
Additional details about specific content and materials are provided in
Attachment F.
Department of Health and Human Services grosvenor management consulting 34
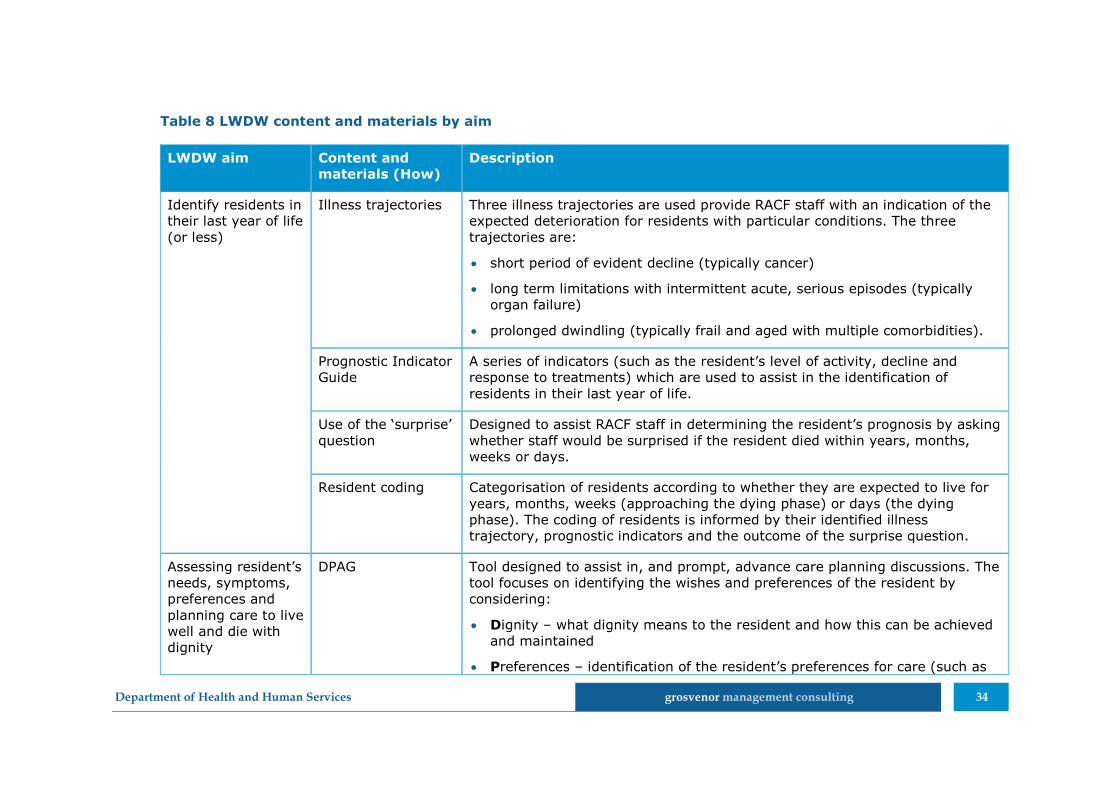
Table 8 LWDW content and materials by aim
LWDW aim Content and
materials (How)
Description
Identify residents in
their last year of life
(or less)
Illness trajectories Three illness trajectories are used provide RACF staff with an indication of the
expected deterioration for residents with particular conditions. The three
trajectories are:
short period of evident decline (typically cancer)
long term limitations with intermittent acute, serious episodes (typically
organ failure)
prolonged dwindling (typically frail and aged with multiple comorbidities).
Prognostic Indicator
Guide
A series of indicators (such as the resident’s level of activity, decline and
response to treatments) which are used to assist in the identification of
residents in their last year of life.
Use of the ‘surprise’
question
Designed to assist RACF staff in determining the resident’s prognosis by asking
whether staff would be surprised if the resident died within years, months,
weeks or days.
Resident coding Categorisation of residents according to whether they are expected to live for
years, months, weeks (approaching the dying phase) or days (the dying
phase). The coding of residents is informed by their identified illness
trajectory, prognostic indicators and the outcome of the surprise question.
Assessing resident’s
needs, symptoms,
preferences and
planning care to live
well and die with
dignity
DPAG Tool designed to assist in, and prompt, advance care planning discussions. The
tool focuses on identifying the wishes and preferences of the resident by
considering:
Dignity – what dignity means to the resident and how this can be achieved
and maintained
Preferences – identification of the resident’s preferences for care (such as

Department of Health and Human Services grosvenor management consulting 35
LWDW aim Content and
materials (How)
Description
depth of involvement in decisions and where they would like to be treated
and die)
Advance Care Directives – identifying and clarifying the meaning of any
existing ACDs
Clinical Goals of Care – identifying realistic outcomes for the resident
against the four main clinical goals (length of life, function, comfort and
prevention of avoidable crises).
Help primary care
teams to prepare all
individuals for
changes.
Clinical Pathways Clinical pathways which are aligned to the residents goals of care. These
pathways are used to inform the types of care which the resident receives.
The following three pathways are taught as part of the LWDW approach:
aggressive diseased focused pathways
less aggressive disease focused emphasising supporting care pathways
supportive and palliative pathways.
CAPs for
Deteriorations
Specific plans for the management and provision of care to a resident as they
deteriorate. The plans can be pre-authorised by the GP and actioned as
required by the RACF staff.
Department of Health and Human Services grosvenor management consulting 36
6.2 Findings from the LWDW pilot
6.2.1 Project management
Project management skills were needed
Stakeholders agreed that management of the LWDW project would have
benefitted from a greater level of project management skills and focus within
the LWDW team.
The core team had a high level of clinical skill and knowledge and the drive
to deliver high levels care. The skills, knowledge and drive of the team led
them to sometimes become the deliverers of the care rather than facilitating
delivery and implementation by the RACF staff.
The clinical skills of the core team were not sufficiently guided and directed
by an individual with the program management skill to effectively and
efficiently deliver the complete project.
Poor quality project documentation
Much of the LWDW documentation is poor quality and appears to be
incomplete. This is another area where the project would have benefited
from additional project management oversight.
In many areas the LWDW resources and documentation available to DHHS
Tasmanian Health Organisations (THO’s) is not sufficient to support future
delivery of the project without substantial effort to review and finalise the
documentation. The quality and availability of project documentation also
negatively impacted this evaluation.
Changes to the project name
The project name was changed to the NWAHS LWDW project in December
2011 to acknowledge that the program had been ‘Australianised’. Changing
the name of the project resulted in some confusion, with stakeholders being
unable to clearly articulate the differences between LWDW and GSF. This
was identified by both the participating RACFs and some members of the
project team.
Confusion around the name change is believed to have created some
challenges during implementation. Some participating RACFs expressed that
they felt uncertain around the future of the project at this time and felt
reluctant to commit large amounts of resources to a project which may
change without warning. They noted that they received little communication
about the name change, why it occurred, and what impact it would have on
the program and participating RACFs.
Department of Health and Human Services grosvenor management consulting 37
Communication and relationship management is vital
LWDW was primarily developed and implemented by a DHHS palliative care
nurse and palliative care doctor. A range of clinical, administrative and
project staff from the other participating organisations also provided support
to the project.
During consultations it was noted that the various members of the project
team often had different work schedules and availability. This presented a
challenge for the project team who needed to collaborate on the various
tools and activities associated with LWDW and the delivery of the 4CEHR
system. Stakeholders reported that, at times, they were unable to contact or
receive input from necessary team members within appropriate/required
timeframes.
Obtaining commitment
Prior to commencing the LWDW program, the boards of all participating
RACFs were engaged to ensure that the RACF was committed to
participation. All participating RACFs were required to gain a GSF licence
during this phase.
The commitment and engagement of management within each of the RACFs
was considered to be essential to the successful implementation of LWDW
and realisation of the required culture change. Consultations suggested that
RACFs whose management were more engaged and supportive of their staff
had greater success implementing and using the content and materials. The
LWDW project team noted that it was challenging to implement the
approach where appropriate preparation had not been undertaken.
Hands-on implementation support
The participating RACFs highly valued the input of the various LWDW team
members during the implementation period. The project team’s clinical
specialists were identified as being able to provide necessary support to the
RACFs.
Following the project, RACFs within North West Tasmania have continued to
receive part-time support from a palliative care specialist nurse (0.5FTE).
The ability to access this expert advice has provided ongoing benefits to the
RACFs in implementing the LWDW approach and providing appropriate care
to residents.
6.2.2 Licencing arrangements
The requirement to pay the GSF licence fee was considered to be a financial
burden by the participating RACFs. At the time of the project, the GSF
licence cost was a one-off payment of approximately $20 per bed.
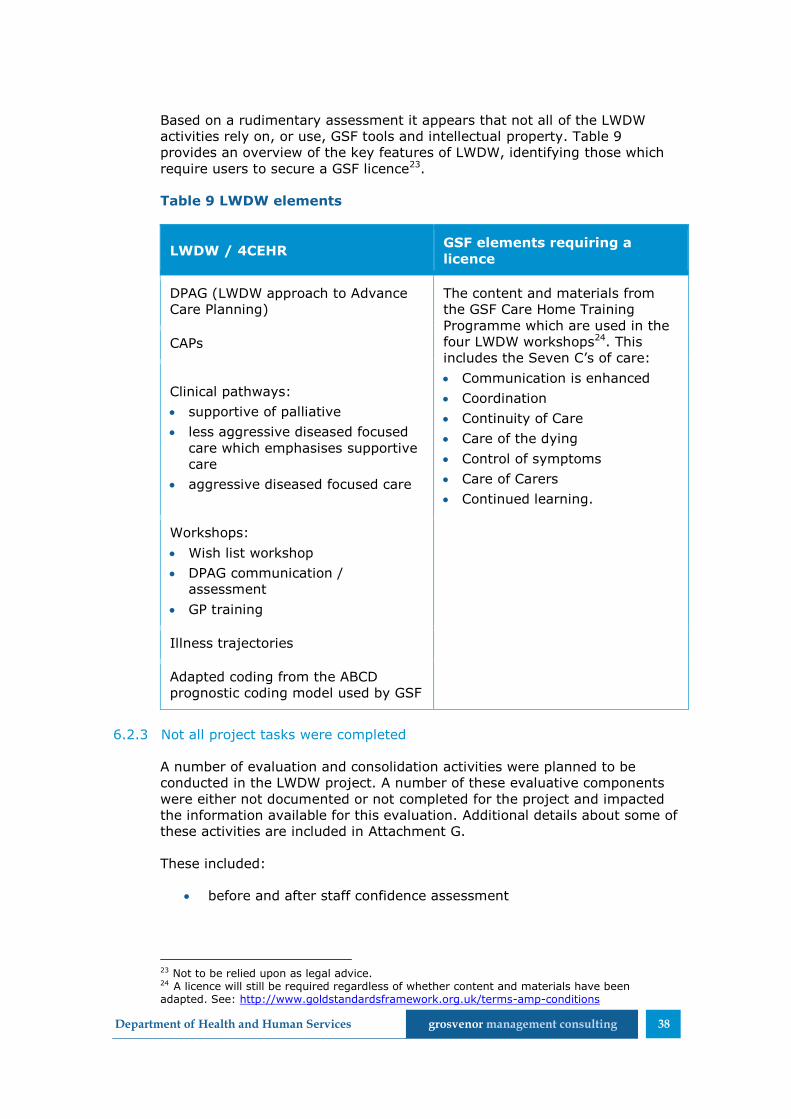
Department of Health and Human Services grosvenor management consulting 38
Based on a rudimentary assessment it appears that not all of the LWDW
activities rely on, or use, GSF tools and intellectual property. Table 9
provides an overview of the key features of LWDW, identifying those which
require users to secure a GSF licence23.
Table 9 LWDW elements
LWDW / 4CEHR GSF elements requiring a
licence
DPAG (LWDW approach to Advance
Care Planning)
The content and materials from
the GSF Care Home Training
Programme which are used in the
four LWDW workshops24. This
includes the Seven C’s of care:
Communication is enhanced
Coordination
Continuity of Care
Care of the dying
Control of symptoms
Care of Carers
Continued learning.
CAPs
Clinical pathways:
supportive of palliative
less aggressive diseased focused
care which emphasises supportive
care
aggressive diseased focused care
Workshops:
Wish list workshop
DPAG communication /
assessment
GP training
Illness trajectories
Adapted coding from the ABCD
prognostic coding model used by GSF
6.2.3 Not all project tasks were completed
A number of evaluation and consolidation activities were planned to be
conducted in the LWDW project. A number of these evaluative components
were either not documented or not completed for the project and impacted
the information available for this evaluation. Additional details about some of
these activities are included in Attachment G.
These included:
before and after staff confidence assessment
23 Not to be relied upon as legal advice. 24 A licence will still be required regardless of whether content and materials have been adapted. See: http://www.goldstandardsframework.org.uk/terms-amp-conditions

Department of Health and Human Services grosvenor management consulting 39
baseline and post-implementation after death audits
analysis of any cultural change that had been achieved at each RACF,
including changes to staff practice or systems
results of evaluation questions which formed part of the training
workshops.
Members of the project team noted that all LWDW consolidation and
evaluation activities had not been completed as originally intended. As at
January 2014, the LWDW project team noted that some of the participating
RACFs had completed up to three of the post-implementation after death
audits. No RACFs were reported to have completed the full five required as
part of the planned evaluation.
No results from the post-implementation after death audits or any
evaluation activities conducted in early 2014 were made available, or
referenced, during this evaluation.
6.2.4 Who should be involved in advance care planning
The pilot RACFs were highly supportive of LWDW’s multidisciplinary
approach, which allowed all interested staff to attend workshops. The
majority of RACFs indicated that attendance at all levels was supported.
However, at least one of the RACFs only allowed care staff to attend the
workshops which was seen as a barrier to LWDW’s adoption and
implementation.
Participation in the workshops was stated as having improved the quality of
care overall and that staff at all levels took more responsibility for providing
daily care in accordance with a resident’s wishes and preferences.
For example: hotel staff recognising and raising with care or nursing staff
that the lowest risk food texture option may not fit with an individual’s
wishes.
In relation to undertaking advance care planning discussions (e.g. DPAG)
with residents and their families, RACFs agreed that senior or specialist staff
are those most suited to this task. Overall it was felt by the majority of
RACFs that it is generally best if responsibility for ensuring that advance care
planning is completed rests with one or a few individuals. This does not
mean that others cannot be involved in the delivery, but that someone takes
overall responsibility for ensuring it is undertaken.
RACFs were highly supportive of the need for GP engagement and training in
the LWDW approach to achieve buy-in and successfully implement improved
advance care planning (rather than relying upon RACFs to convince and
educate GPs themselves). RACFs also supported concurrent GP training,
rather than offset training (which saw GPs receive training after the RACFs)
as occurred in the project. Specific information about the GP training is
included in Attachment H.
Furthermore RACFs indicated that concurrent engagement of hospitals would
have further improved the use of advance care planning and advance care
directives.

Department of Health and Human Services grosvenor management consulting 40
6.2.5 Not everyone will be willing or have appropriate skills
It was acknowledged that not every individual will be willing or necessarily
suited/skilled to undertake advance care planning. RACFs in the project
believed that the inclusiveness of the LWDW approach allowed for varying
levels of comfort and skill, while still promoting holistic culture change within
the organisation.
There was recognition that staff roles and responsibilities should take into
account skill sets and interests to promote good practice and positive
culture. All RACFs indicated that they felt confident that individual staff who
were not comfortable having a discussion themselves would act on a
resident’s concern or request by raising it with someone more appropriate.
Addressing GP resistance
It was indicated that not all GPs were receptive to the approach. RACFs
indicated that the following assisted in overcoming GP resistance:
closer engagement with and use of specialist palliative care services
to provide ‘expert advice’
the workshops and approach improved staff confidence in discussing
care with GPs
the person-centred approach empowered RACF staff to act as a
patient advocates ‘i.e. able to convince GP on the basis of the
patient’s wishes, rather than it being their (staff) view/opinion’.
6.2.6 When to start advance care planning
When to start Advance Care Planning (overall)
RACFs identified that waiting until admission to an RACF to commence
advance care planning is too late. All believed that there should be greater
awareness of advance care planning in the community, and advance care
planning should be facilitated in other health settings, particularly primary
care.
The main rationale was that (as discussed in section 5.2) increasingly
residents do not have the capacity to participate fully in this process upon
entry to a RACF.
GPs were commonly identified as being the most appropriate profession to
conduct advance care planning in the community. Limitations to GPs
conducting advance care planning in the community were identified, and
included:
GPs do not have sufficient time to conduct advance care planning
GPs are not able to bill for advance care planning discussions.
The engagement of a Practice Nurse or Care Coordinator with linkages to
chronic care models and programs could be used to conduct advance care
planning in conjunction with a GP. This would allow advance care planning to

Department of Health and Human Services grosvenor management consulting 41
occur within the General Practice setting without the limitations of GPs
standard consultation lengths.
It should also be noted that GPs are able to claim for time spent conducting
advance care planning for residents with chronic or terminal medical
conditions and/or complex care needs using chronic disease management
Medicare items25.
When to start Advance Care Planning (in RACFs)
The timing of commencing Advance Care Planning varied among the RACFs
in the pilot and those who responded to the RACF survey. Times ranged
from before admission to up to 6 weeks after admission. Some indicated
there was no ‘set’ time to commence discussions.
Some RACFs indicated that they had found it beneficial to introduce the topic
gradually. For example:
by including some information in pre-admission documentation or
having a brief conversation prior to admission
touching on the topic during the first days to gauge the level of
resident comfort for participating in these discussions
holding a detailed discussion once the resident is settled.
Two distinct viewpoints were expressed in relation to the appropriate time:
those who believed that introduction as early as possible was best
those who felt it inappropriate to discuss advance care planning prior
to, or at admission, as this is already a significant life event which
may be traumatic or overwhelming for the resident and/or their
family. It was suggested that discussing advance care planning may
increase the trauma associated with admission.
6.2.7 When to revisit Advance Care Plans and Advance Care Directives
Stakeholders identified that once an advance care directive was in place it
was important to revisit a person’s wishes:
regularly – the frequency depended on the person’s health status and
health care setting (at least annually in a RACF)
when a change in health status occurs, either deterioration or
improvement
when a change in health setting occurs
at the request of the individual.
25 Department of Health, Chronic Disease Management Questions and Answers, http://www.health.gov.au/internet/main/publishing.nsf/Content/030C0CED16935261CA257BF0001D39DB/$File/CDM-qandas-feb4.pdf

Department of Health and Human Services grosvenor management consulting 42
It was emphasised that advance care planning does not stop once an
advance care directive is prepared. Individual’s views can change when
events become real rather than hypothetical, as a result of their
accumulated experiences, or due to a change in family situation.
The LWDW approach promotes regular review of advance care planning.
6.2.8 Use of the LWDW approach and tools
RACFs reported using different aspects of the LWDW approach and tools with
differing levels of consistency (i.e ad hoc to routine). Specific details of the
various approaches and tools used in the LWDW approach are included in
Attachment F.
Identify residents in their last year of life
Of the four RACFs consulted as part of the evaluation:
one indicated that the coding and illness trajectories had been well
received and were continuing to be used by staff
one noted that while they no longer routinely code residents, some
staff still discuss the coding at meetings
one noted that the coding is less helpful as it is often hard to predict
an individual’s prognosis until they reach the final stages of life. The
RACF commented that they had trialled displaying the coding but
found that the resident’s deteriorations and death did not align with
the anticipated timeframes/prognosis. The approach was ceased due
to the constant need to change the coding.
Differences in the perceived use and appropriateness of these tools may
further reflect variable understanding and ability to apply the approach and
tools between the participating RACFs.
There was a also perception among staff at one of the RACFs that the coding
was mostly conducted for the benefit of GPs. Coding was believed to enable
GPs to easily identify when a change in one of their patients has occurred
which may require a change in care. Despite the perceived benefits of
coding, the RACF staff noted that the GPs at their facility had not received
training about coding and, as such, could not utilise or apply it. It is unclear
why the GPs at this facility reportedly did not receive the training about
coding.
Advance care planning
LWDW teaches participating RACFs to utilise the DPAG approach to advance
care planning.
Only one of the consulted RACFs has incorporated advance care planning as
a routine practice. Some of the others consistently provide information about
advance care directives (or similar) but do not routinely engage in an
advance care planning discussion with all residents, record the outcomes
and regularly follow up with residents (and families).

Department of Health and Human Services grosvenor management consulting 43
One RACF noted that only a small proportion of its residents had a current
advance care directive. No RACFs were able to provide exact information
about the proportion of residents with an advance care directive.
The variable uptake of advance care planning and creation of advance care
directives may be attributed to a range of factors, such as, but not limited
to:
resident willingness to participate in advance care planning
discussions
the capacity of residents to actively participate in advance care
planning discussions
time and effort for staff to hold discussions and document outcomes.
The RACFs identified some residents are not willing to participate in
discussions about end of life care and their wishes or values. There was no
indication of how often advance care planning is revisited with residents who
have expressed a reluctance to participate. One RACF highlighted that there
can be variability in a resident’s level of comfort with advance care planning
discussions, noting that different residents may wish to:
discuss and document their wishes and preferences
only document their wishes and preferences
only discuss their wishes and preferences (but not document them).
Despite this, RACFs with low proportions of residents with an advance care
directives still considered the LWDW approach to be successful and
beneficial.
It was identified that improvements to care were able to be identified even
where the resident lacked capacity. For example, one RACF was able to
identify that a resident with severe dementia had enjoyed a particular drink
every afternoon prior to entering the RACF. This was previously unknown to
the RACF staff and identified during an advance care planning discussion
involving the resident and a family member. Following the advance care
planning discussion, the provision of the drink was incorporated into their
care.
During consultations a number of RACFs referred to particular successes
using the DPAG process. This included one RACF which discharged a resident
so that they were able to spend their final weeks of life at home with their
family. Spending their final weeks together in the home environment was a
particular preference identified by the resident and their family. The RACF
was pleased to have been able to enable this and attributed this to
successful and appropriate advance care planning.
All RACFs involved noted that they endeavour to provide a copy of any
advance care directive (and other relevant information) when a resident is
transferred to hospital.

Department of Health and Human Services grosvenor management consulting 44
A number of barriers to advance care planning were still experienced by the
participating RACFs during and after the LWDW project:
Time - As part of the implementation of LWDW, the two project leads
attended each of the RACFs to develop DPAGs for some patients.
Stakeholders reported that, at times, the project team members
spent up to five hours with a single resident conducting the DPAG.
RACF staff do not have capacity to spend this amount of time with a
single resident.
Format and content of DPAG - It was reported that the advance
care planning document the project leads developed could be up to
six or seven pages in length. Lengthy documents were not considered
to be usable for the RACF staff or GPs, who prefer short and concise
documents. While LWDW provided the RACFs with the DPAG model to
structure advance care plans, it did not provide a consistent
template. As a result, the advance care plans/directives being
produced by the participating RACFs may vary considerably.
Recognition in other settings - Stakeholders reported that the
advance care planning documents which are being produced may not
be recognised in different health settings. One stakeholder noted that
hospitals commonly require specific features in a document. Without
being produced in the particular format, provided documents may not
be used to inform decisions about care. For example, it was identified
that hospitals will only read/use documents which are presented in
the official format, including having a hospital barcode. Recognition of
document validity was also a problem experienced when using
ambulance services26.
Awareness/communication - A number of stakeholders identified
that problems had been encountered where an individual (including
those in the community) had an advance care directive that was not
known of by family members or health care professionals and thus
not complied with. The reasons for lack of awareness varied.
Clinical action plans (CAPs)
Under the LWDW approach, CAPs are used to enable prior planning for
expected or likely deteriorations. A range of CAPs were developed and
promoted as part of the LWDW program to assist GPs and other health
professionals in making decisions about a resident’s end of life care. An
example CAP is included in Attachment F.
Following the completion of the DPAG process, a GP can select and authorise
the appropriate CAP in alignment with the resident’s preferences and wishes.
The authorised CAPs can then be activated when appropriate by the RACF
staff27.
26 Note: Ambulance services were not directly engaged with during this evaluation. It was evident from consultations that they are an important future stakeholder for state-wide advance care planning. 27 ehospice, Living Well and Dying Well, http://www.ehospice.com/australia/Default/tabid/10688/ArticleId/1187
Department of Health and Human Services grosvenor management consulting 45
Use of the CAPs also enables GPs to undertake anticipatory prescribing. GPs
are able to identify and pre-approve the specific medications which would be
appropriate for the resident as they deteriorate. The RACF is then able to
enact this anticipatory prescribing as required to provide the most
appropriate care for each event.
RACFs were supportive of anticipatory prescribing. However, the CAPs as
represented in the 4CEHR system were reported to be underdeveloped and
unsuitable for use. It was suggested by some that GPs may find the CAPs
overly prescriptive and it was questioned whether the content was
appropriately supported by current literature and how it would be
maintained into the future.
Specific issues about the current format of the CAPs are identified in the
document “Tasmanian Health Organisation – North West 4C System Change
Requests” (page 7). These include:
names of the CAPs are inconsistent and confusing
there are inconsistencies in the description of options within the CAPs
it is difficult to identify some required options without knowledge of
which problem (deterioration) to select.
General feedback suggested that the dying phase CAPs should be the
highest priority for further development as they are the most relevant and
useful to support the dying.
Other projects in which DHHS are involved also focus upon the development
of guidance and tools to support and ensure consistency in clinical decision
making. Notably this includes the Tasmanian HealthPathways project (see
section 8.1.10) and Better Access to Palliative Care – Palliative Care
Formulary Project28. As these projects should result in regularly maintained
information to assist health professionals in making clinical decisions and
prescribing medications, it is unclear whether the CAPs developed as part of
LWDW (and included in the 4CEHR system) are necessary.
After Death Audits
After death audits were considered to be useful for staff debriefing and for
identifying areas in which future care could be improved. An example after
death audit is included in Attachment G.
There was evidence of ongoing ad hoc use of after death audits; however,
the approach has been modified by some of the participating RACFs. For
example, despite not conducting formal after death audits, one of the
participating RACFs holds regular ‘tool-box’ discussions with staff during
which recent deaths are discussed.
28 Department of Health and Human Services, Better Access to Palliative Care in Tasmania – Palliative Care Forumlary Project Business Plan, Version 1.0 10 June 2014

Department of Health and Human Services grosvenor management consulting 46
6.2.9 Feedback from residents and family members
Residents and families who were interviewed as part of the evaluation
expressed that they are comfortable engaging in end of life care planning
discussions. Identified benefits included:
the discussion and documentation of residents wishes provides
reassurance for some residents and their families
some residents welcome the ability to document their end of life
wishes to relieve pressure on their families to make difficult decisions
the use of advance care directives and documented advance care
plans has been used as a tool to avoid family conflict in decision
making. For example, during the consultations, one participant
indicated that accessing the documented advance care plan had
enabled the family to recognise and share the resident’s wishes,
avoiding disagreements on the best course of action and care.
While there were many reported instances of families benefiting from the
advance care planning discussions, it should be noted that indirect feedback
was received indicating that residents had varying levels of comfort and
wishes about who should be present at advance care planning discussions.
In some instances it was noted that the resident may prefer a friend, rather
than a family member. LWDW supports the inclusion of any person with
whom the resident is comfortable in advance care planning discussions.
6.2.10 Overall RACF view of the LWDW project
RACFs views were divided about the overall experience of the project.
Two of the RACFs consulted with viewed the project in a positive light, and
two negatively. While the two who view it negatively acknowledged they
have realised some benefits, overall they believed they had been required to
invest a lot of effort without fully realising the benefits that were promised.
The two RACFs who had a negative perception of the program specifically
did not like the following:
perception of discontinuing/inadequate support (4CEHR)29
uncertainty surrounding the project
lack of clear communication from the project team/ lack of
clarity/disjointed project management
training (one of the two)
having to pay for the GSF licence
29 Note: Ongoing support to the 4CEHR system was provided by a systems administrator. The two RACFs with a negative perception of the system did not reference or identify the availability of this support.

Department of Health and Human Services grosvenor management consulting 47
order of training – GP training was too late, hospital engagement was
not visible to them.
6.3 Outcomes of LWDW
The LWDW pilot sought to achieve a number of key outcomes within the
participating RACFs:
culture change and staff empowerment, including increasing staff
confidence in undertaking advance care planning
recognition of suffering, death and dying, including the identification
of deteriorations and resident pain/discomfort
delivery of person centred care which is appropriately tailored to the
needs, preferences and wishes of residents
cost savings through a reduction in hospitalisations.
6.3.1 Ongoing use of the LWDW approach
All of the RACFs consulted with as part of this evaluation noted that they had
experienced benefits as a result of the LWDW project. As discussed in
section 6.2.8, each consulted RACF has adopted elements of the LWDW
approach. Despite the uptake of particular aspects of LWDW, the content
and tools have not been used consistently, with each RACF adopting only
those elements they feel add value. Within the participating RACFs, selected
LWDW content and tools are taught to new staff within all roles (including
nurses and GPs). The fact that the RACFs are taking time to teach the
approach to new staff demonstrates that the LWDW approach is considered
to be valuable.
6.3.2 Culture change and staff empowerment
Throughout the consultations, stakeholders identified that a culture change
has been evident within the RACFs as a result of LWDW. This has included
the following:
Normalised discussions about death and dying
Death has now been accepted as a natural part of life and is openly
discussed by RACF staff. The ability to provide quality end of life care is now
seen as a ‘privilege’ by one RACF.
Empowered all staff to participate in care planning
The RACFs reported that all staff are now more willing, and able, to have
these discussions with residents and families and record information about
residents preferences and wishes.
Increased the understanding of the care which is being provided
All staff (including those in non-clinical positions) now have a better
understanding why particular care is being provided. For example, kitchen
staff have a better understanding of why residents need to have particular

Department of Health and Human Services grosvenor management consulting 48
food, or, why someone in their final weeks/days may no longer adhere to a
set diet (such as diabetic).
Increased staff confidence in undertaking more complex care
Nurses are reportedly adopting greater responsibility in the care of
residents, including using the information contained in the CAPs to discuss
the care that is being provided with GPs.
Increased the confidence of some RACFs to manage more conditions
One RACF identified that the facility as a whole is now more confident about
the conditions which it is able to manage. They have been working with the
local hospitals to provide care to residents with a wider range of needs. In
some cases the hospital has worked with the RACF to train nursing staff to
enable residents to be discharged back to the RACF. While the RACF
attributed this to the greater confidence of its staff, it is unclear whether this
is a result of the LWDW program.
6.3.3 Recognition of suffering, death and dying
Prior to the LWDW program, stakeholders believed that the RACFs were
often not expecting and were not prepared for the death of a resident. The
focus of LWDW on the recognition of death has enabled staff to become
more prepared for the death of a resident, reducing the overall level of staff
distress following a resident’s death.
It was also reported that the earlier recognition of the dying phase has
allowed residents families to be engaged, allowing them time to prepare.
Death is now considered to be less of a surprise for families. Despite this,
only one RACF reported conducting specific bereavement activities.
The LWDW program also taught RACF staff about recognising the suffering
of residents. Staff have reportedly responded well to this aspect of LWDW
and are now more aware of, and responsive to, resident’s pain symptoms.
The LWDW project team believe that the training has allowed all staff to
appropriately manage care in a way which acknowledges and minimises the
pain of residents. This has assisted in the achievement of person-centred
care which is tailored to the needs and requirements of the resident.
6.3.4 Impact on hospitalisations
While each of the RACFs noted during the consultations that they felt the
hospitalisation rate had been reduced as a result of LWDW, none have
actively collected quantitative data to support this.
The rationale for the reduction of hospital admissions under LWDW is
premised on research that shows a much higher proportion of people die in
hospital, compared to expressed preferences for place of death. LWDW aims
to reduce hospitalisations by acknowledging dying and death and complying
with preferences for place of death.
Preliminary analysis in the 2012 4C Final Report suggested that LWDW may
have resulted in some cost savings through reduced hospitalisations. This
analysis only included data for the participating RACFs over a three month

Department of Health and Human Services grosvenor management consulting 49
period (January to March) from 2010 to 2012, with the report noting that
additional analysis would be required.
As part of this evaluation, THO-North West provided data about the
emergency attendance and hospital admissions of RACF residents in North
West Tasmania from January 2010 to September 2014. A number of data
constraints were identified which may impact on the data’s accuracy. The
following constraints should be considered when interpreting the data:
the data does not include admissions to rural hospitals such as
Smithton District Hospital
RACFs are identified based on a free-text data field. Any variations in
the entered address may impact on the identification of the
participating RACFs
the emergency data system only captures the patient’s postcode and
suburb, not their full address. Where an individual attends the
emergency department, but is not admitted, the postcode and suburb
are matched against the RACF addresses to identify RACF residents.
This may result in some non-admitted patients being incorrectly
recorded as RACF residents.
Analysis of THO-North West data revealed that the number of emergency
attendances (Figure 3) decreased for both the participating RACFs and non-
participating RACFs between 2010 and 2013. Despite an overall decrease,
there was a slight increase in attendances from the participating RACFs
between 2011 and 2012.
Figure 3 Emergency attendances by year
While hospital admissions decreased for non-participating RACFs between
2010 and 2013, limited change was observed in the participating RACFs
(Figure 4).
0
100
200
300
400
500
600
700
800
900
2010 2011 2012 2013
Emergency attendance by year
Participating Other RACF

Department of Health and Human Services grosvenor management consulting 50
Figure 4 Hospital admissions by year
The average length of stay in the hospitals for RACF residents from both the
participating and other RACFs decreased between 2010 and 2013.
0
100
200
300
400
500
600
2010 2011 2012 2013
Hospital admissions by year
Participating RACF Other RACF

Department of Health and Human Services grosvenor management consulting 51
7 4CEHR
7.1 Background and purpose
In 2011 funding of $3,278,707.26 was provided by DoHA under the Wave 2
Sites for the Personally Controlled eHealth Record (PCEHR) to develop and
pilot an electronic health record to facilitate advance care planning in RACFs
across five pilot sites in North West Tasmania.
The successful funding bid united two projects which had both commenced
in 2009 – the implementation of the Gold Standards Framework in RACFs
(later known as the Living Well Dying Well Project) and the Cradle Cost
Electronic Health Information Exchange Project.
The Electronic Health Exchange Project was a consortium of the:
Cradle Coast Authority
University of Tasmania Rural Clinical School
TML
Tasmanian Health Organisation – North West (THO- North West).
The 4C system was intended to both support the development of advance
care plans and facilitate the communication of such plans between health
care professionals. The system also incorporates information and tools to
assist relevant health professionals in planning care to align with the wishes
of residents30.
7.2 Development and design
7.2.1 Timeframes
The 4C project was originally to be delivered over 18 months; however, by
the time the successful Wave 2 projects were announced the timeframes
had been reduced to 12 months from 1 July 2011 – 30 June 2012.
The timeframes for development of the 4C system were further impacted by
the delay to contract execution with Alcidion, the service provider engaged
to build the system. Planned for July 2011, the contract was not executed
until December 2011, leaving only six months for the project.
The restricted timeframes for the development of the 4C system negatively
impacted the project’s ability to deliver on its original aims. As it was
important for the project team to meet the prescribed timeframes, not all
activities associated with the development of the 4C system had been
appropriately finalised and tested prior to the initial roll-out.
30 Cradle Coast Connected Care (4C) Clinical Repository Final Report, v1.0 13 May 2013

Department of Health and Human Services grosvenor management consulting 52
The short project implementation timeframes limited the ability of the
project team to undertake appropriate system testing and review. This
contributed to system limitations and barriers in the current product. Details
of system limitations and barriers to use are discussed in section 7.3.2.
7.2.2 Scope and functionality
Table 10 compares the intended elements of the 4C system with what was
actually achieved. This includes discussion of the integration and design of
the system, as well as its key features/components.
Table 10 Comparison of the intended and actual scope of the 4CEHR
system
Scope Intended Actual
Integration
Integration between a
DHHS Shared Electronic
Health Record and 4C was
planned.
Integration with existing
GP and nurse software was
excluded from the scope.
The Shared Electronic Health
Record project did not go
ahead. As a result this
functionality was not delivered.
The 4C system has its own
infrastructure separate from
the broader DHHS ICT
environment.
NeHTA
compliant
standards
4CEHR was to be
compliant with NeHTA
standards to be a PCEHR
conformant repository. The
4C repository was to
become the foundation for
the Tasmanian PCEHR
conformant repository,
integrating with the
Tasmanian Shared
Electronic Heath Record
(SEHR).
The Tasmanian SEHR project
did not occur as planned.
The interface with the PCEHR
was not implemented as it was
not available within the
timeframes.
Users
RACFs Yes – limited use
General Practices No – ability to use, but no
actual use
Acute hospital facilities No – ability to use, but no
actual use
After hours GP services No – ability to use, but no
actual use

Department of Health and Human Services grosvenor management consulting 53
Scope Intended Actual
Allied Health providers (eg.
pharmacy)
No – ability to use, but no
actual use
Available
views
Different views relevant to
the various health
professions:
GPs
RACF nurses
GP Assist
Delivered with some
delays/barriers
End
beneficiaries
Residents of RACFs
4C’s scope did not include
residents of the
community living at home
Delivered
Interface
with
eReferrals
Send, receive and
acknowledge31 No
Consumer
portal
Access to education
content only.
7.3 4C’s scope did not include
the delivery of a consumer
portal which provided
access to health
information.
Consumer educational content
was delivered on both the
4CEHR project webpage and
DHHS webpages32.
Dashboard
Screen providing an
overview of the status of
each RACF resident,
including trajectory and
prognostic code,
completed elements of the
care plan and any
current/active
deteriorations
Delivered
Advance
Care
Directive
Records and displays
Enduring Guardian or
Person Responsible
Prompts initiation of an
Delivered with some design
limitations
31 Cradle Coast Electronic Health Information Exchange, Annex A – Project Context and Scope, v1.1 27 May 2011, page 11 32 The consumer educational content is available at: http://www.cradle-coast-ehealth.org.au/research/the-4c-project/4c-project-consumer-information.
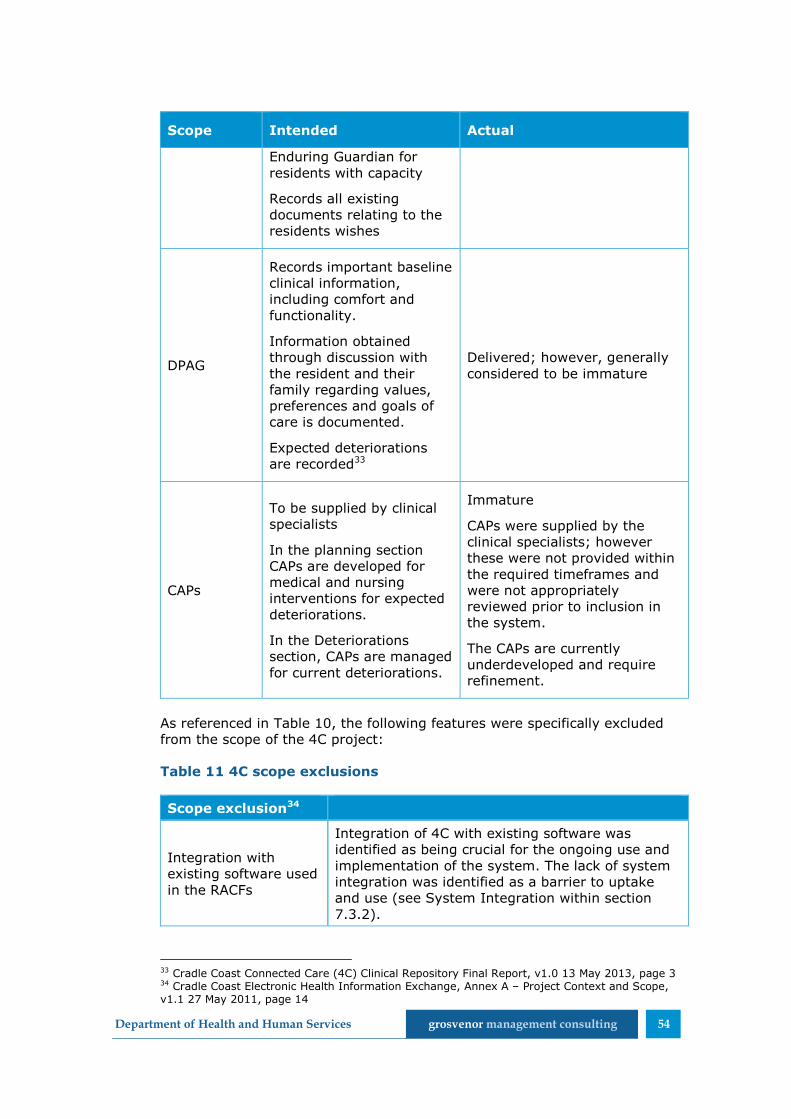
Department of Health and Human Services grosvenor management consulting 54
Scope Intended Actual
Enduring Guardian for
residents with capacity
Records all existing
documents relating to the
residents wishes
DPAG
Records important baseline
clinical information,
including comfort and
functionality.
Information obtained
through discussion with
the resident and their
family regarding values,
preferences and goals of
care is documented.
Expected deteriorations
are recorded33
Delivered; however, generally
considered to be immature
CAPs
To be supplied by clinical
specialists
In the planning section
CAPs are developed for
medical and nursing
interventions for expected
deteriorations.
In the Deteriorations
section, CAPs are managed
for current deteriorations.
Immature
CAPs were supplied by the
clinical specialists; however
these were not provided within
the required timeframes and
were not appropriately
reviewed prior to inclusion in
the system.
The CAPs are currently
underdeveloped and require
refinement.
As referenced in Table 10, the following features were specifically excluded
from the scope of the 4C project:
Table 11 4C scope exclusions
Scope exclusion34
Integration with
existing software used
in the RACFs
Integration of 4C with existing software was
identified as being crucial for the ongoing use and
implementation of the system. The lack of system
integration was identified as a barrier to uptake
and use (see System Integration within section
7.3.2).
33 Cradle Coast Connected Care (4C) Clinical Repository Final Report, v1.0 13 May 2013, page 3 34 Cradle Coast Electronic Health Information Exchange, Annex A – Project Context and Scope, v1.1 27 May 2011, page 14
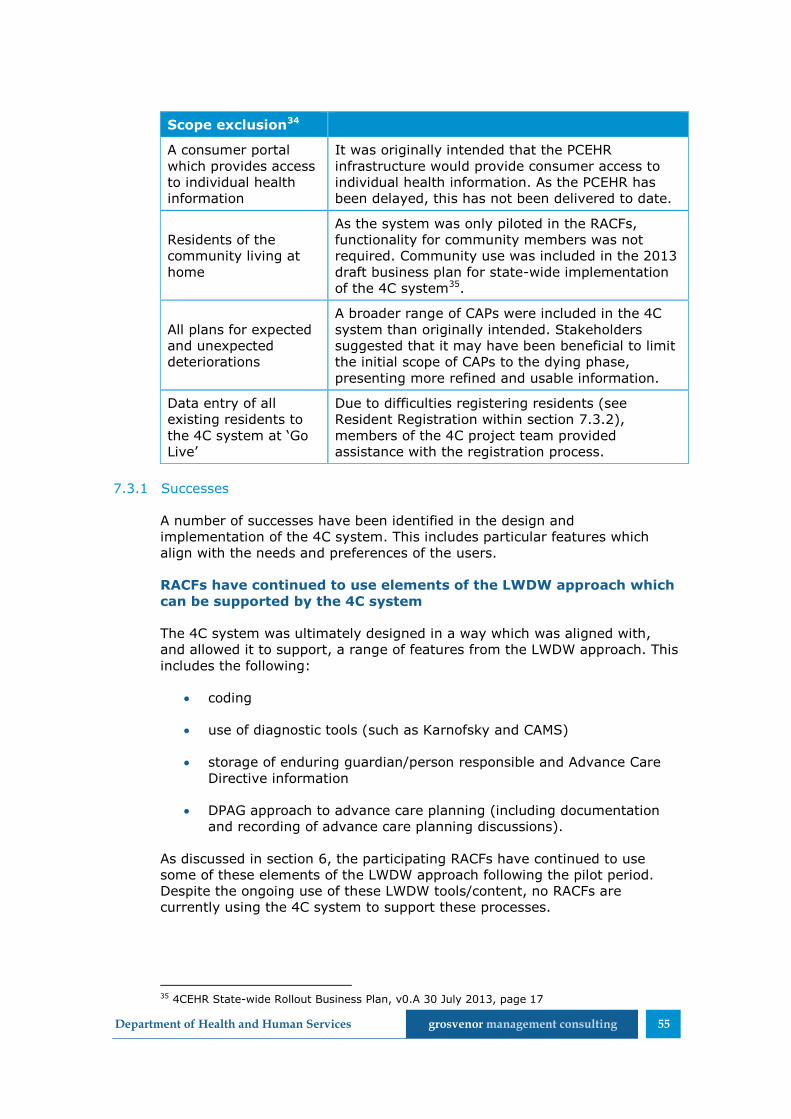
Department of Health and Human Services grosvenor management consulting 55
Scope exclusion34
A consumer portal
which provides access
to individual health
information
It was originally intended that the PCEHR
infrastructure would provide consumer access to
individual health information. As the PCEHR has
been delayed, this has not been delivered to date.
Residents of the
community living at
home
As the system was only piloted in the RACFs,
functionality for community members was not
required. Community use was included in the 2013
draft business plan for state-wide implementation
of the 4C system35.
All plans for expected
and unexpected
deteriorations
A broader range of CAPs were included in the 4C
system than originally intended. Stakeholders
suggested that it may have been beneficial to limit
the initial scope of CAPs to the dying phase,
presenting more refined and usable information.
Data entry of all
existing residents to
the 4C system at ‘Go
Live’
Due to difficulties registering residents (see
Resident Registration within section 7.3.2),
members of the 4C project team provided
assistance with the registration process.
7.3.1 Successes
A number of successes have been identified in the design and
implementation of the 4C system. This includes particular features which
align with the needs and preferences of the users.
RACFs have continued to use elements of the LWDW approach which
can be supported by the 4C system
The 4C system was ultimately designed in a way which was aligned with,
and allowed it to support, a range of features from the LWDW approach. This
includes the following:
coding
use of diagnostic tools (such as Karnofsky and CAMS)
storage of enduring guardian/person responsible and Advance Care
Directive information
DPAG approach to advance care planning (including documentation
and recording of advance care planning discussions).
As discussed in section 6, the participating RACFs have continued to use
some of these elements of the LWDW approach following the pilot period.
Despite the ongoing use of these LWDW tools/content, no RACFs are
currently using the 4C system to support these processes.
35 4CEHR State-wide Rollout Business Plan, v0.A 30 July 2013, page 17

Department of Health and Human Services grosvenor management consulting 56
The system has the potential to support processes which are being
undertaken within the RACFs.
There is support for the ability to communicate Advance Care
Directives
Originally, the 4C system was intended to support the communication of
Advance Care Directives both within and between healthcare settings. It was
widely accepted that advance care planning information needs to be shared
with a variety of health professionals. As identified in the RACF survey, this
may include a range of professionals including GPs, GP Assist, nurses in
RACFs and the community, hospital staff, ambulance staff and specialists.
During consultations, stakeholders expressed support for a system or
approach which would enable and assist the communication and sharing of
this information among relevant professionals. However, the existence of an
electronic system does not achieve this simply by existing – it also needs to
be used. Achieving uptake and use of any communication mechanism,
including electronic systems was an acknowledged barrier. The same issues
currently exist with the PCEHR.
There is support for functionality in relation to clinical care planning,
in particular anticipatory prescribing
The participating RACFs were very supportive of undertaking clinical care
planning and anticipatory prescribing to support the delivery of care,
especially out of hours and during the dying phase. While it was possible for
both of these activities to be supported by/undertaken within the 4C system,
this functionality was not widely used during the pilot. Despite this, RACFs
indicate that care planning has been enhanced through the LWDW approach
and is beneficial.
As clinical care planning and anticipatory prescribing are highly valued by
RACF staff, the inclusion of these features in the 4C system is considered to
be relevant and appropriate.
7.3.2 Barriers
A number of system limitations and other barriers were identified which
limited the implementation and uptake of the 4C system. The consequences
of these issues were considered to be quite significant by the participating
RACFs and ultimately became barriers to the use of the 4C system.
System limitations and security concerns
During the consultations a number of system limitations and security
concerns were identified which impacted upon stakeholder willingness and
ability to use the 4C system. These are detailed in Table 12.
Table 12 4C system limitations and security concerns
Limitation Impact
Structural issues within the
system including: Inconsistencies in the layout of the various
4C screens and other technical issues

Department of Health and Human Services grosvenor management consulting 57
Limitation Impact
inconsistent placement
of buttons between
screens
cursor moving while
correcting typos
decrease the usability of the 4C system.
Key terminology is not
consistent, defined and
appropriate for all
healthcare settings
Different RACF staff may have different
understandings/definitions of the data
recorded in the 4C system. This may result
in:
residents being rated inconsistently by
different RACF staff
RACF staff interpreting information about
residents differently, for example, their
functional ability
Inconsistent ratings and understandings
may further limit the ability of the RACF
staff to provide person-centred care.
Documents are grouped by
type of document rather
than date
Where a resident has multiple versions of
each document type, it may be difficult for
the RACF staff to determine what
information (document types) is available.
This may limit their ability to access and use
recorded information in a crisis situation /
when decisions need to be made quickly.
Changes to a GPs default
medication preferences will
retroactively be applied to
all of the GPs residents
without warning
Retroactive updates to resident’s
medications may result in inaccuracies
within the 4C records. The system will not
record information about the medication
and doses which the resident actually
received.
Inaccuracies in medication
charts as a result of:
automatic population
from the CAPs
errors in the opioid
calculator
4C users are unable to rely on printed
medication charts due a number of known
inaccuracies.
The 4C system automatically populates the
name of the CAP for prescription from the
CAPs documents. This may not accurately
reflect the reason a resident has been
prescribed a particular medication,
potentially resulting in errors and
inaccuracies within the resident’s record.
The opioid calculator currently does not
calculate correct dosages.
GPs were able to approve
medications which can only
be authorised by palliative
care specialists (eg.
Ketamine)
Potential to generate non-compliance and
inappropriate prescriptions. This has been
corrected.
All 4C users were able to RACF staff will be able to inappropriately

Department of Health and Human Services grosvenor management consulting 58
Limitation Impact
access and print the
medications chart
access and update information about
prescribed medications. This was considered
to be particularly problematic by the
participating RACFs who refused to use the
system until this had been rectified. This
has been corrected.
Resident registration
The registration of residents within the 4C system relies upon the Healthcare
Identifiers (HI) Service. Specifically, the RACF is required to enter basic
information about the resident (such as name, date of birth and Medicare
number) which is matched against the resident’s Individual Healthcare
Identifier (IHI).
This process resulted in some difficulties for the participating RACFs. Where
a resident (or their family) were unsure about exactly what information was
recorded in Medicare, it was difficult to match the IHI and register the
resident. For example, the participating RACFs reported that some residents
used a name on a daily basis which is different to that recorded by Medicare
(and thus, against their IHI).
Medicare requires a person to attend a Medicare office to confirm or update
their information. As many RACF residents were physically unable to do this,
it was not possible to determine what was in the Medicare record to assist in
matching an IHI. These residents could therefore not be registered within
the system.
Use of the Tasmanian Health Client Index (THCI) has also been identified as
a system enhancement in the 4CEHR Draft Project Business Plan for state-
wide rollout of the 4C system36. This plan suggested that the 4C system
could be enhanced by linking the THCI to the IHI to simplify the registration
process.
System integration
A range of medical software is currently used within Australian RACFs. This
includes pieces of software which are specifically designed for either RACF
nursing staff or GPs. GPs tend to have a preference to use the same
software which is being used in their practice within the RACF setting.
Table 13 details the software which is commonly used within the
participating RACFs. ThisTable 13 should not be considered to be an
exhaustive list of all software used by Tasmanian RACFs and GPs.
36 4CEHR Draft Project Business Plan, 30 July 2013, page 18

Department of Health and Human Services grosvenor management consulting 59
Table 13 Software commonly used in RACFs by nurses and GPs
Nurse GP
Autumn Care Medical Director
iCare Best Practice
The 4C system was introduced in addition to the main software which was
already being used within the participating RACFs. No integration with the
existing software was included in the final version of 4C, nor was it in scope.
However, the lack of integration created a number of key challenges for the
RACF staff:
duplication of data entry
risk of inconsistent records.
Additionally, it was reported that GPs would generally be unwilling to use
different software in addition to their practice software.
Simultaneous development of the 4C system and LWDW was
problematic
While the 4C project was intended to be developed in a way which supported
the LWDW approach, the two projects were delivered in relative isolation.
During consultations it was identified that there was limited communication
and interaction between the two project teams, with key team members
feeling isolated from each other’s project. This lack of communication
prevented appropriate collaboration from being undertaken and was a
barrier to development of a 4C system which could fully support the
requirements of the LWDW approach.
Further, the LWDW approach was not fully developed or embedded within
the participating RACFs when the 4CEHR system was developed and
implemented. This created some confusion for the participating RACFs who
were unclear about the changing project scope. Stakeholders noted that the
changes and developments to the project were highly confusing as:
RACFs first agreed to participate in the NWAHS GSF project
the project then changed to become the NWAHS LWDW project
finally, the project expanded to include the implementation of an ICT
system (4CEHR).
Stakeholders noted that these changes to the project resulted in significant
differences between the final project scope and what was originally intended
and agreed to.
The parallel development of the LWDW approach also impinged on the
timeliness and quality of the current 4CEHR system. For example,
stakeholders noted that the CAPs were still being drafted the day prior to
system release and, as such, had not been appropriately reviewed.

Department of Health and Human Services grosvenor management consulting 60
It was suggested that it would be more beneficial to ensure that the
approach was fully developed, piloted and refined prior to the commissioning
of a supporting system.
Lack of sufficient testing and uptake impacted on the quality of the
final deliverable
Due to the short 4C project timeframes, limited user testing was
undertaken. This restricted the ability of the project team to identify system
and content flaws, inconsistencies and other issues which ultimately became
barriers to system use and uptake.
RACFs still commonly use paper based records
RACFs generally have a preference for the use of paper based records. This
was identified through consultations with the participating RACFs and the
RACF survey.
Sixty-four percent of the 11 respondents to the RACF survey only use paper
based records to store Advance Care Directives and advance care planning
information. A further 27% use both electronic and paper records while 9%
use only electronic records. Despite this, the majority of respondents
indicated that an electronic system to support advance care planning would
be of value.
The implementation of the 4C system therefore requires some cultural
change within the participating RACFs, moving away from the existing
system of paper based records. It is possible that RACF staff will be unwilling
to change their practice in this manner, creating a barrier to the ongoing use
of a system such as 4C.
RACF staff have relatively low computer literacy
Throughout the stakeholder consultations it was suggested that RACF staff
have relatively low computer literacy. This may impact upon the users
understanding of how to appropriately navigate and use the system, as well
as potentially limiting their confidence in its use. This has the potential to
become a barrier to the ongoing use of the system. RACF staff who are
uncomfortable with, or unable to appropriately use, the system will be
unlikely to support its ongoing use.
‘Help’ section immature
There is a lack of ‘help’ information in the current system. This may prevent
users from accessing the necessary information to assist them in proper use
of the system.

Department of Health and Human Services grosvenor management consulting 61
7.4 Uptake and use
Following conclusion of the project 30 June 2012, and after the target date
for the go-live release (14 June 201237) had elapsed, the current version of
the system was released 29 November 201238.
The 4CEHR system is not currently used by RACFs who participated in the
pilot.
Due to problems primarily related to permissions for prescriptions approvals
and IHI matching issues (described in section 7.3.2) the system was not
significantly used after go-live. However, work was undertaken by the
system administrator (and some RACFs) to register and load relevant
documentation for residents that had completed advance care planning
activities and provided consent for the information to be loaded and shared
via 4CEHR.
The key barriers that prevented initial and ongoing use of the system were:
1. The project concluded prior to release of a system version that was
suitable for use. (Opportunity for improved functionality)
2. End-users were not resourced sufficiently for system implementation.
(Implementation support requirements)
3. The conclusion of the project led to the withdrawal of personnel and
funding. End-user stakeholders doubted that the system would be
supported or adopted by others, and therefore were no longer willing
to commit resources to pilot its use. (Project certainty and
stakeholder engagement)
7.4.1 Functionality
Since conclusion of the 4CEHR project a number of reviews have been
undertaken and documents have been produced outlining opportunities to
improve the functionality of the system. These have been prepared based on
the experiences and feedback of users to date. Documents of this nature
that were made available during this evaluation are detailed in Table 14
below. Further feedback was collected as part of this evaluation including
from RACFs and future stakeholders.
Table 14 Documents detailing future improvement opportunities
Title Description Date
Cradle Coast
Connected Care (4C)
Clinical Repository
Final Report
Details the status, risks, issues
and lessons learnt.
13 May
2013
4CEHR State-wide Business plan to achieve state
wide rollout of 4CEHR (and 30 July
37 4C Annex D Project Implementation Approach V2.0 27 May 2011, page 10 38 4C Clinical Repository Final Report v1.0 13 May 2013, page 3

Department of Health and Human Services grosvenor management consulting 62
Title Description Date
Rollout Business Plan LWDW) 2013
Tasmania Health
Organisation – North
West 4C System
Change Requests
Details:
urgent system fixes (4)
urgent improvement requests
(30)
May 2014
While the above documents detail a number of fixes required to improve the
usability of the 4C system, they do not address the key concern of uptake
across settings.
Only one of the participating RACFs indicated that 4C would have value as a
standalone system. Despite expressing this view, the RACF is not currently
utilising the system. All other RACFs and GPs felt that the system would only
have value if it was integrated with existing RACF software and enabled the
communication of advance care planning information between health
settings. Without the inclusion of this functionality, it is unlikely that there
would be widespread use of the 4C system.
7.4.2 Implementation support
Support was provided to each of the participating RACFs during the
implementation of the 4C system. This support was provided in addition to
the formal 4C training and included project team members registering
residents at each participating RACF.
Such additional assistance was considered to be highly valuable by the
participating RACFs. As the registration of residents was considered to be
time consuming and difficult, additional assistance to complete this was well
received.
Upload of resident records
The 4C project had a target of having 500 RACF residents ready for
enrolment in the system. As shown in Table 15, the project did not meet this
target.
It should be noted that the target of 500 registrations was developed when
Umina Park was still included in the project. As the capacity of Umina Park is
greater than that of Emmerton Park it was unlikely that this target would be
achieved following the withdrawal of Umina Park from the project39.
39 The capacity of both RACFs is available on the following websites: Umina Park - http://www.agedcareguide.com.au/facility_details.asp?facilityid=15435; Emmerton Park - http://www.emmertonpark.com.au/history.html

Department of Health and Human Services grosvenor management consulting 63
Table 15 Target and actual registration of RACF residents in the 4C
system
Target of RACF residents ready
to be enrolled40
Actual (1 July 2012 - 1 May
2013)41
500 73% - 366
While an information booklet and consent form for RACF residents was
developed as part of the 4C project, this was generally considered to be
overly complex and difficult to use.
Stakeholders reported that the information booklet was not written in a
manner which could be easily understood by residents, and may have
become a barrier to participation. It was generally believed that residents
who did not understand the content of the booklet and consequently the
nature of the 4C system may have been unwilling to consent to registration.
These residents reportedly found it too difficult to participate or attempt to
understand the system. This highlights the importance of communicating
details of any system or health initiative to the target audience in a way
which can be understood.
The overly complex nature of the 4C information booklet does not align with
the approach of LWDW which seeks to communicate information in an
appropriate manner that can be easily understood by residents and families.
The detail and content of the consent booklet were driven by the PCEHR
project.
7.4.3 Project certainty and stakeholder engagement
The system name, Cradle Coast Connected Care Electronic Health Record
(4CEHR), carries negative perceptions for some past RACF stakeholders due
to the failure of the system to become operationalised, in combination with
the resources, effort and support required by them throughout the project.
The disappointment and negativity also speaks to the need to clearly set
expectations for stakeholders and engage regularly with them to ensure
there is a shared understanding.
Despite being a pilot, there was a strong belief that the project would be
continued beyond the initial period. This belief was shared by the project
team and participating RACFs. While we do not have specific details of how
or what was communicated to stakeholders with regard to the project’s
continued support, it is believed that there was no communication to
suggest the project may not continue until late in the project. . During
interviews undertaken as part of this evaluation, no RACF stakeholders
indicated understanding that, as a pilot, the outcome could be to discontinue
support for the 4CEHR system.
40 Cradle Coast Electronic Health Information Exchange, Annex A – Project Context and Scope, v1.1 27 May 2011, page 12 41 Cradle Coast Connected Care (4C) Clinical Repository Final Report, v1.0 13 May 2013

Department of Health and Human Services grosvenor management consulting 64
Future stakeholders may also be put off by the system name due to its
‘ownership’ by North-West Tasmania. This is within context of historically
strained relationships between the three areas of Tasmania. As Tasmania
adopts a single health area model it may also be inappropriate to use
regionally based names.
7.4.4 Cost to enhance and roll-out
As detailed throughout this section, a number of improvements to the
functionality and capability of the 4C system would be required to support
and encourage the future use of the system.
DHHS and THO-North West provided an estimation of the costs associated
with the ongoing implementation and maintenance of the 4C system (Table
16).
Table 16 Estimated implementation and maintenance costs for the
4C system42, 43
Purpose Estimated cost
Ongoing licences, support and
maintenance $500,000 (per annum)
System enhancements,
implementation and state-wide roll-
out
$3,800,000
Project management $950,000
42 Note: These costs were provided by DHHS and THO-North West and have not been validated by Grosvenor. 43 Note: The cost estimate excludes the change management component.
Department of Health and Human Services grosvenor management consulting 65
8 Approaches to advance care planning
A number of different approaches and tools for conducting advance care
planning are currently used throughout Australia. This includes specific
approaches and tools which are used and promoted by:
Medicare Locals
State and Commonwealth Government Departments
health care providers (including hospitals and RACFs)
peak bodies such as Palliative Care Australia and Alzheimer’s
Australia.
National guidance has been provided through the 2011 ‘National Framework
for Advance Care Directives’ which aims to encourage consistency between
the different approaches to end of life care planning. The framework was
developed to be an aspirational document which describes goals for policy
and practice, rather than presenting the current law and practice across
Australia.
As identified in the framework, different legislation in each state and
territory has contributed to the development of different Advance Care
Directives. Further, the framework identifies that the ‘high level of variability
makes it difficult for one jurisdiction to legally recognise an ACD [Advance
Care Directive] from elsewhere’44. The framework seeks to address the
challenges presented by the different laws as well as concerns about the use
of and application of Advance Care Directives] throughout Australia.
The Commonwealth Government has provided funding and support for a
number of national palliative care projects which relate to advance care
planning. This includes:
funding for Austin Health’s Respecting Patients Choices program
(section 8.1.1)
support for the Residential Aged Care Palliative Approach and funding
for the development of the Residential Aged Care Facility End of Life
Care Pathway (section 8.1.2)
establishment of the Specialist Palliative Care and Advance Care
Planning Advisory Service (Decision Assist – section 8.1.3).
This section discusses some of the major approaches to advance care
planning which are currently used in Australia. Each of the approaches which
have received either Commonwealth funding or support are discussed, along
with some of the other approaches used within Tasmania or referenced by
the LWDW pilot RACFs.
44 A National Framework for Advance Care Directives, http://www.ahmac.gov.au/cms_documents/AdvanceCareDirectives2011.pdf, page 1
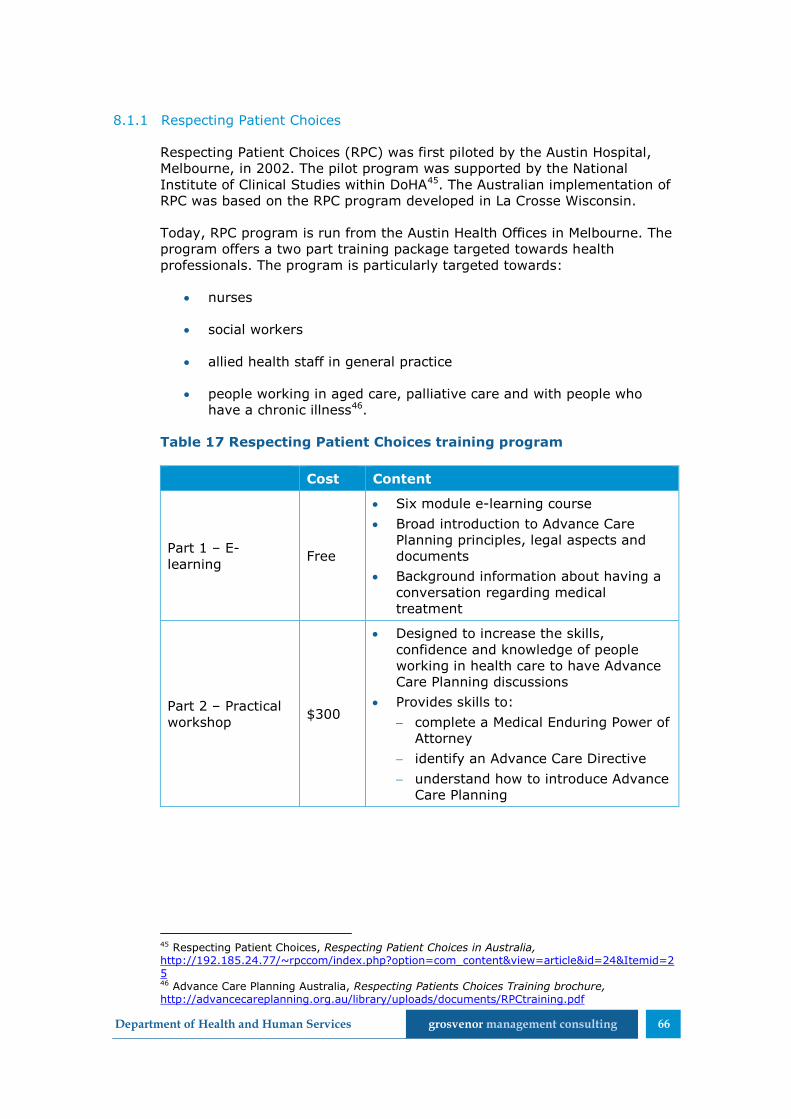
Department of Health and Human Services grosvenor management consulting 66
8.1.1 Respecting Patient Choices
Respecting Patient Choices (RPC) was first piloted by the Austin Hospital,
Melbourne, in 2002. The pilot program was supported by the National
Institute of Clinical Studies within DoHA45. The Australian implementation of
RPC was based on the RPC program developed in La Crosse Wisconsin.
Today, RPC program is run from the Austin Health Offices in Melbourne. The
program offers a two part training package targeted towards health
professionals. The program is particularly targeted towards:
nurses
social workers
allied health staff in general practice
people working in aged care, palliative care and with people who
have a chronic illness46.
Table 17 Respecting Patient Choices training program
Cost Content
Part 1 – E-
learning Free
Six module e-learning course
Broad introduction to Advance Care
Planning principles, legal aspects and
documents
Background information about having a
conversation regarding medical
treatment
Part 2 – Practical
workshop $300
Designed to increase the skills,
confidence and knowledge of people
working in health care to have Advance
Care Planning discussions
Provides skills to:
complete a Medical Enduring Power of
Attorney
identify an Advance Care Directive
understand how to introduce Advance
Care Planning
45 Respecting Patient Choices, Respecting Patient Choices in Australia, http://192.185.24.77/~rpccom/index.php?option=com_content&view=article&id=24&Itemid=25 46 Advance Care Planning Australia, Respecting Patients Choices Training brochure, http://advancecareplanning.org.au/library/uploads/documents/RPCtraining.pdf
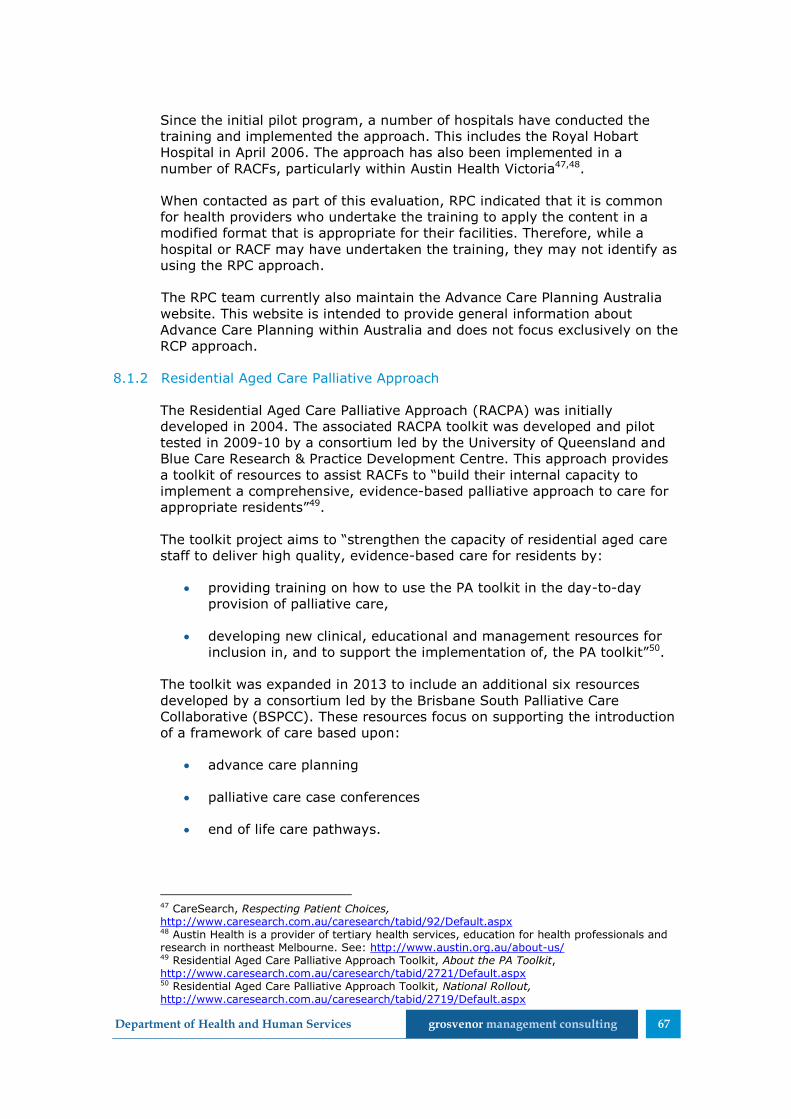
Department of Health and Human Services grosvenor management consulting 67
Since the initial pilot program, a number of hospitals have conducted the
training and implemented the approach. This includes the Royal Hobart
Hospital in April 2006. The approach has also been implemented in a
number of RACFs, particularly within Austin Health Victoria47,48.
When contacted as part of this evaluation, RPC indicated that it is common
for health providers who undertake the training to apply the content in a
modified format that is appropriate for their facilities. Therefore, while a
hospital or RACF may have undertaken the training, they may not identify as
using the RPC approach.
The RPC team currently also maintain the Advance Care Planning Australia
website. This website is intended to provide general information about
Advance Care Planning within Australia and does not focus exclusively on the
RCP approach.
8.1.2 Residential Aged Care Palliative Approach
The Residential Aged Care Palliative Approach (RACPA) was initially
developed in 2004. The associated RACPA toolkit was developed and pilot
tested in 2009-10 by a consortium led by the University of Queensland and
Blue Care Research & Practice Development Centre. This approach provides
a toolkit of resources to assist RACFs to “build their internal capacity to
implement a comprehensive, evidence-based palliative approach to care for
appropriate residents”49.
The toolkit project aims to “strengthen the capacity of residential aged care
staff to deliver high quality, evidence-based care for residents by:
providing training on how to use the PA toolkit in the day-to-day
provision of palliative care,
developing new clinical, educational and management resources for
inclusion in, and to support the implementation of, the PA toolkit”50.
The toolkit was expanded in 2013 to include an additional six resources
developed by a consortium led by the Brisbane South Palliative Care
Collaborative (BSPCC). These resources focus on supporting the introduction
of a framework of care based upon:
advance care planning
palliative care case conferences
end of life care pathways.
47 CareSearch, Respecting Patient Choices, http://www.caresearch.com.au/caresearch/tabid/92/Default.aspx 48 Austin Health is a provider of tertiary health services, education for health professionals and research in northeast Melbourne. See: http://www.austin.org.au/about-us/ 49 Residential Aged Care Palliative Approach Toolkit, About the PA Toolkit, http://www.caresearch.com.au/caresearch/tabid/2721/Default.aspx 50 Residential Aged Care Palliative Approach Toolkit, National Rollout, http://www.caresearch.com.au/caresearch/tabid/2719/Default.aspx
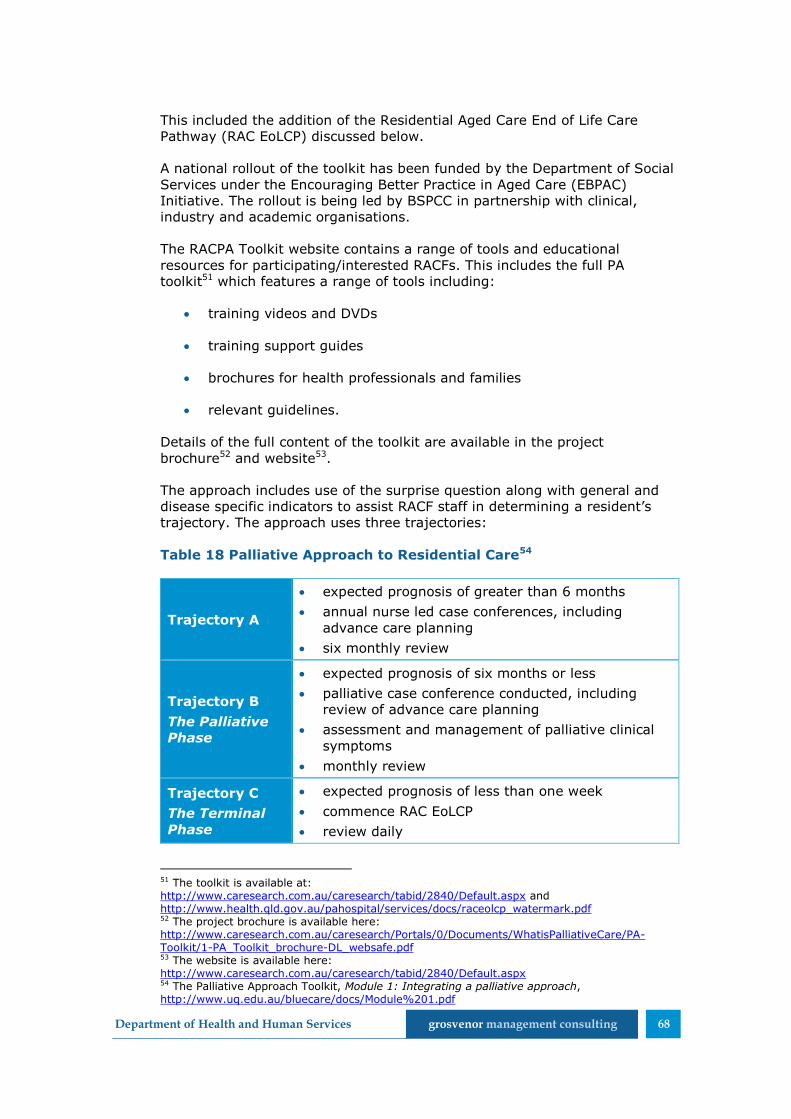
Department of Health and Human Services grosvenor management consulting 68
This included the addition of the Residential Aged Care End of Life Care
Pathway (RAC EoLCP) discussed below.
A national rollout of the toolkit has been funded by the Department of Social
Services under the Encouraging Better Practice in Aged Care (EBPAC)
Initiative. The rollout is being led by BSPCC in partnership with clinical,
industry and academic organisations.
The RACPA Toolkit website contains a range of tools and educational
resources for participating/interested RACFs. This includes the full PA
toolkit51 which features a range of tools including:
training videos and DVDs
training support guides
brochures for health professionals and families
relevant guidelines.
Details of the full content of the toolkit are available in the project
brochure52 and website53.
The approach includes use of the surprise question along with general and
disease specific indicators to assist RACF staff in determining a resident’s
trajectory. The approach uses three trajectories:
Table 18 Palliative Approach to Residential Care54
Trajectory A
expected prognosis of greater than 6 months
annual nurse led case conferences, including
advance care planning
six monthly review
Trajectory B
The Palliative
Phase
expected prognosis of six months or less
palliative case conference conducted, including
review of advance care planning
assessment and management of palliative clinical
symptoms
monthly review
Trajectory C
The Terminal
Phase
expected prognosis of less than one week
commence RAC EoLCP
review daily
51 The toolkit is available at: http://www.caresearch.com.au/caresearch/tabid/2840/Default.aspx and http://www.health.qld.gov.au/pahospital/services/docs/raceolcp_watermark.pdf 52 The project brochure is available here: http://www.caresearch.com.au/caresearch/Portals/0/Documents/WhatisPalliativeCare/PA-Toolkit/1-PA_Toolkit_brochure-DL_websafe.pdf 53 The website is available here: http://www.caresearch.com.au/caresearch/tabid/2840/Default.aspx 54 The Palliative Approach Toolkit, Module 1: Integrating a palliative approach, http://www.uq.edu.au/bluecare/docs/Module%201.pdf

Department of Health and Human Services grosvenor management consulting 69
Free workshops (funded by the Department of Social Services (DSS)) are
being conducted for RACF managers, clinical leaders and educators. Up to
two representatives were able to attend the workshops from each RACF. As
the workshops focus on introducing the toolkit and training staff how to use
the resources and specifically target managerial and clinical staff,
recommended attendees include:
the RACF Manager (Care Director or Director of Nursing)
a Registered Nurse or Enrolled Nurse employed in a clinical area who
is able to become the RACFs ‘Link Nurse’55.
Workshops were scheduled to be held throughout Australia from October
2013 to December 2014. In Tasmania, these workshops were held in Hobart
and Launceston in March 2014. No further funding has been provided to
extend the training beyond these dates.
A total of 96 individuals from 44 RACFs in Tasmania participated in the
training sessions. This included at least one of the five LWDW pilot RACFs.
Material from the RACPA is to be included in the Department of Health’s
Decision Assist Program. To avoid duplication, with Decision Assist, the
RACPA project team advised that no further broad workshop programs will
be conducted. Despite this, fee for service education may be available in the
future.
It is expected that all material associated with the RACPA (including
additional factsheets and podcasts) will be made available online by
December 2014.
An evaluation of the RACPA is currently being conducted, with the findings to
be presented to DSS in May 2015.
Residential Aged Care Facility End of Life Care Pathway
In 2013, BSPCC received funding from DoHA to ‘develop, implement and
evaluate an End of Life Care Pathway specifically for use in… RACFs’56. This
resulted in the development of the Residential Aged Care End of Life Care
Pathway (RAC EoLCP) which was designed to guide the provision of end of
life care in RACFs57.
As part of DoHA funding, the RAC EoLCP was evaluated against Palliative
Care Australia’s best practice standards across 299 deaths. The results of
this evaluation showed that:
when the RAC EoLCP was implemented with a supportive framework,
dying residents were significantly less likely to be transferred to
hospital
55 The Link Nurse has a range of specific duties within the RACF to promote and implement a palliative approach. 56 Queensland Government, Department of Health, End of Life Care Pathways, http://www.health.qld.gov.au/cpcre/eol_pthwys.asp 57 The RAC EoLCP is available here: http://www.caresearch.com.au/Caresearch/Portals/0/PA-Tookit/2%20RAC%20EoLCP%20Form%20%28the%20Pathway%20Document%29.pdf

Department of Health and Human Services grosvenor management consulting 70
there were improvements in the quality of palliative care provided by
RACFs
the RAC EOLCP increased the confidence of RACF clinical staff to
deliver palliative care.
The RAC EoLCP has been further evaluated against the EBPAC project. From
this project it was recommended that the RAC EoLCP document be made
widely available to RACFs. It is now available with a supporting webinar on
the RACPA Toolkit website58.
Under the RAC EoLCP approach, training should be made available to all
staff within the RACF involved in end of life care. Specifically, the following
elements of the implementation framework have been identified:
“establishment of dedicated Palliative Care Link Nurses within each
RACF
creation of palliative care educational resources
establishment of a RACF Medication Imprest System that allows for
timely access to drugs commonly used at end of life
mechanisms to link RACF staff with Specialist Palliative Care
colleagues to improve complex case management
mechanisms to facilitate GP support to provide end of life (terminal)
care ‘in place’”59.
At this stage, the RACPA and RAC EoLCP only focus upon RACFs.
8.1.3 Specialist Palliative Care and Advance Care Planning Advisory Service
(Decision Assist)
The Australian Government has funded the Specialist Palliative Care and
Advance Care Planning Advisory Service (Decision Assist) Project to enhance
the national provision of palliative care and advance care planning
services60.
There are several key aspects to Decision Assist, as outlined on the care
search website. The project includes:
the establishment of a national advice based telephone service for
GPs and aged care providers
development of standard clinical practice guidance for specialist
palliative care and advance care planning.
58 Residential Aged Care Palliative Approach Toolkit, Webinar, http://www.caresearch.com.au/caresearch/tabid/3087/Default.aspx 59 Queensland Government, Queensland Health, Residential Aged Care End of Life Care Pathway, http://www.health.qld.gov.au/pahospital/services/raceolcp.asp 60 Decision Assist, About Decision Assist, http://www.caresearch.com.au/caresearch/tabid/3104/Default.aspx

Department of Health and Human Services grosvenor management consulting 71
focus on up skilling and educating GPs and aged care providers
increasing the linkages between aged care and palliative care
services61.
Respecting Patient Choices is the lead agency for Decision Assist. The
project also involves:
Palliative Care Australia
Care Search
The University of Queensland
Queensland University of Technology
The Australian and New Zealand Society of Palliative Medicine
Leading Age Services Australia
Aged and Community Services Australia.
A range of educational activities have been designed as part of Decision
Assist for GPs and Aged Care Providers.
The ‘Decision Assist Aged Care Training Package – Residential’ will combine
e-learning modules and face to face workshops to provide training about
palliative care and advance care planning. The two workshops are designed
as follow on training from the Palliative Approach Toolkit62.
While only two face to face workshops will be conducted, these are
scheduled two months apart to enable participants to implement the content
of the first session. This is similar to the LWDW approach. Attendance at the
workshops will cost $150 per attendee63.
8.1.4 Enhancing Aged Care through better Palliative Care
Enhancing Aged Care through better Palliative Care seeks to provide
intensive community-based palliative care services for aged care clients
living in the community and in RACFs. The project specifically aims to:
“enhance client choice in their end-of-life care
reduce client admissions to emergency departments, where possible
increase client satisfaction and quality of life, through reduced delays
to receive specialist palliative care services, the availability of a 24/7
61 Full details of Decision Assist are available at: http://www.caresearch.com.au/caresearch/tabid/3104/Default.aspx 62 Decision Assist, Decision Assist Aged Care Training Package – Residential, http://www.caresearch.com.au/caresearch/tabid/3301/Default.aspx 63 Decision Assist, Aged Care Workshops http://www.caresearch.com.au/caresearch/tabid/3207/Default.aspx
Department of Health and Human Services grosvenor management consulting 72
home service and the ability of the NP [nurse practitioner] to liaise
with hospital care services and GPs on the client’s behalf”64.
A pilot of the project is currently being undertaken and is expected to
conclude on 31 December 2014. This project is funded by the Better Health
Care Connections grant program65.
8.1.5 Peak bodies and area specific programs
A number of peak bodies within Australia and individual Medicare Locals
provide information about advance care planning through their websites.
Examples of these programs include:
Alzheimer’s Australia’s Start2Talk Program66
the My Wishes program managed by Sydney South West Area Health
Service67
MyChoice, NSW North Coast68.
Depending upon the organisation, the information may be targeted towards
health professionals or individual members of the community. The content of
these websites is often similar, aiming to provide the skills and knowledge
required to complete an advance care directive.
Additionally, some health care providers and RACFs have established or
adopted their own approaches to advance care planning. This includes
Southern Cross Care in South Australia which has implemented LWDW under
the support of Dr Robyn Brogan69.
8.1.6 Healthy Dying Framework
At the time of this evaluation, DHHS was developing the Tasmanian Healthy
Dying Framework. This framework has been designed to
“support and guide community-wide efforts towards making Tasmania
a place where the idea of healthy dying is familiar and unexceptional,
and the prospect of natural death is recognised, acknowledged and
supported by all parts of the Tasmanian community and its services”70
64 University of Queensland, Evaluation of the Enhancing Aged Care through Better Palliative
Care, http://www.uq.edu.au/bluecare/evaluation-of-the-enhancing-aged-care-through-better-palliative-care 65 Australian College of Nurse Practitioners, Queensland Chapter Newsletter, Volume 1, Issue 4 December 2013, In the Spot Light – Prviate Sector Emerging Models of Care, http://acnp.org.au/sites/default/files/33/acnp_qld_newsletter_dec_2013.pdf 66 Alzheimers Australia, Start2Talk, https://www.start2talk.org.au/ 67 NSW South Western Sydney Local Health District, My Wishes Advance Care Planning Program, www.mywishes.org.au 68 North Coast NSW Medicare Local, Advance Care Planning, http://www.ncml.org.au/index.php/resource-centre/advance-care-planning 69 Southern Cross Care, Living Well Dying Well Project, http://www.southerncrosscare.org.au/?p=254 70 Department of Health and Human Services, An approach to healthy dying in Tasmania: a policy framework, October 2014 Draft v0.D

Department of Health and Human Services grosvenor management consulting 73
The framework is structured around three essential components referred to
as ‘pillars’:
Having the Conversation - Building capacity to talk about death and
dying and engage in advance care planning for end of life care
Delivering End of Life Care - Building a Tasmanian community and a
service system network that supports and provides person-centred,
timely and appropriate end of life care
Bereavement Care - Building capacity to access and deliver
bereavement support71.
A number of key elements are identified throughout the framework to
ensure its successful delivery and implementation. This focuses upon actions
required and targeted towards the Tasmanian Government, health
professionals and the community.
The framework acknowledges and builds upon the range of end of life care
initiatives which are currently used within Tasmania. This includes references
to:
the 4CEHR and LWDW pilot and evaluation
the healthy dying initiative and Medical Goals of Care Plan (see
section 8.1.7)
activities undertaken by TAHPC.
8.1.7 Medical Goals of Care Plan
The Medical Goals of Care Plan is a component of the Tasmanian Healthy
Dying Initiative. This plan aims to:
“ensure that patients who are unlikely to benefit from medical
treatment aimed at cure, receive care appropriate to their condition
and are not subjected to burdensome or futile treatments.”72
This aim is underlined by seven principles73. The plan provides a tool to
assess any patients being admitted to hospital to identify their goals of care.
The Medical Goals of Care Plan was initially implemented by the Royal
Hobart Hospital and has recently been made available for use throughout
Tasmania.
While the original Medical Goals of Care Plan was developed for use in the
acute setting, an adapted version of the plan is available for use in the
71 Department of Health and Human Services, An approach to healthy dying in Tasmania: a policy framework, October 2014, Draft V0.D, page 15 72 Department of Health and Human Services, Medical Goals of Care Plan, http://www.dhhs.tas.gov.au/palliativecare/health_professionals/goals_of_care 73 Note: The Principles of the Goals of Care Plan are available at http://www.dhhs.tas.gov.au/__data/assets/pdf_file/0019/100765/Web_GOC_Principles.pdf
Department of Health and Human Services grosvenor management consulting 74
community and RACFs. The community and RACF form is considered to be a
template which may be updated and modified as required.
A Medical Goals of Care Plan developed in the acute setting may be
endorsed for use out of hospital following the transfer or discharge of a
patient. The plan must be endorsed by the Consultant, Specialist responsible
or delegate as remaining active and provided to the ambulance crew
transferring the patient for palliative or terminal care74.
During consultations it was identified that the plan is being used by some
RACFs within Tasmania; however, it was noted that the manner in which it is
used is likely to be inconsistent. Stakeholders suggested that the form could
be used by RACFs in multiple ways, including:
incorporating a form which was previously completed in another
healthcare setting into end of life care planning for a newly admitted
(or readmitted) resident
completing the form as part of end of life care planning for residents
who have not previously undertaken advance care planning.
The BAPC project intends to increase the uptake of the form within the
public health services. The identification and documentation of medical goals
of care is also referenced throughout the draft Healthy Dying Framework.
8.1.8 COMPAC Guidelines
In 2013, the Australian Healthcare and Hospitals Association (AHHA)
commenced training in Tasmania about the implementation of the Guidelines
for a Palliative Approach for Aged Care in the Community Setting (known as
the COMPAC Guidelines). This was funded as part of the Tasmanian Health
Assistance Package75 and has sought to encourage uptake and use of the
COMPAC Guidelines76.
The Tasmanian face-to-face training has been offered in addition to online
training available across Australia77. The face-to-face training is delivered
through two streams which are combined into one session:
professional stream (including paid health workers, unregistered care
workers, nurses, allied health professionals and GPs)
volunteer/family carer stream78.
74 Department of Health and Human Services, Medical Goals of Care Plan, http://www.dhhs.tas.gov.au/palliativecare/health_professionals/goals_of_care 75 Australian Healthcare and Hospitals Association, Palliative Care Training to Launch in Tasmania, http://ahha.asn.au/news/palliative-care-training-launch-tasmania 76 Australian Healthcare and Hospitals Association, Palliative Care Workshop – Burnie – 14 November, http://ahha.asn.au/events/palliative-care-workshop-burnie-14-november 77 Department of Health, Palliative Care Online Training, http://www.palliativecareonline.com.au/ 78 Australian Healthcare and Hospitals Association, Palliative Care Workshop – Burnie – 14 November, http://ahha.asn.au/events/palliative-care-workshop-burnie-14-november

Department of Health and Human Services grosvenor management consulting 75
8.1.9 TAHPC training
The Tasmanian Association for Hospice and Palliative Care (TAHPC) provides
a number of training programs and tools for health professionals and
community members interested in advance care planning and end of life
care.
TAHPC is currently conducting advance care planning workshops for health
professionals involved in care coordination or case management. These
workshops seek to educate attendees about the principles of advance care
planning and how this can be introduced to a client.
TAHPC is also operates a program of peer education to improve advance
care planning and advance care directives. The role of these educators is to:
provide information to aged and health care service providers,
volunteer groups and the wider community about advance car
planning
to explain the advance care directive document
to explain the role and responsibilities of substitute decision makers
encourage conversations about end of life care79.
8.1.10 Tasmanian HealthPathways
The Tasmanian HealthPathways project has developed and implemented a
range of specific health pathways for use within Tasmania. This project is
based on the approach used in New Zealand’s Canterbury Initiative which
has been adopted in various areas of New Zealand and Australia.
The health pathways provide agreed approaches for the management of
medical conditions in Tasmania and will ultimately address both palliative
care and advance care planning. This should align the management of
medical conditions across various health care professionals (including those
in hospitals and the community)80.
All health pathways are accessible to health professionals through an online
portal. Specifically, the portal provides ‘information on how to assess and
manage a wide range of medical conditions, and how to refer patients to
local specialists and services in the most timely and efficient way’81.
A broad range of health professionals (including GPs, specialist and allied
health providers) will be involved in the ongoing development and review of
the health pathways.
79 TAHPC, Education, http://www.tahpc.org.au/education.html 80 Tasmanian HealthPathways, http://www.tasmedicarelocal.com.au/sites/default/files/Health%20Pathways%20fact%20sheet.pdf 81 Tasmanian HealthPathways, http://www.tasmedicarelocal.com.au/sites/default/files/Health%20Pathways%20fact%20sheet.pdf

Department of Health and Human Services grosvenor management consulting 76
9 ICT support for advance care planning
A high-level desktop analysis was conducted to identify if there are
alternative ICT approaches to support the development and communication
of advance care planning documentation across health care settings.
The following alternative ICT solutions were identified:
My Health Care Wishes - Advance Care Plan app (US)
HSA Global - Collaborative Care Management Solution (NZ).
In addition the current status of the PCEHR and DHHS ICT platform were
explored.
9.1.1 Alternative ICT solutions
Table 19 Existing software and systems
Solution Description Use and reach
My Health Care
Wishes -
Advance Care
Plan app
Smartphone app that
allows you to store and
share an advance
directive. Lite version of
the app is free.
Pro app with additional
functionality costs
AU$4.33
Origin: US
Developed by: American Bar
Association
Commission On Law And
Aging
Android (Lite)
Installs: 1,000-5,000
Rated: 4.4 by 9 users
iTunes does not provide a
rating due to the low
number
Collaborative
Care
Management
Solution
(CCMS)82,83
CCMS is a purpose built
connected software
platform which is
designed with to work
existing IT systems.
Advance Care Planning
functionality has been
included in this
software.
Origin: NZ
Developed by: HSAGlobal
The system is reportedly
widely used within NZ,
including:
Auckland’s National
Shared Care Project
Canterbury’s
Collaborative Care
Program
South Eastern Sydney
Medicare Local currently
82 Pulse+IT Magazine, HAS Global Adds Advance Care Planning Functionality to CCMS, http://www.pulseitmagazine.com.au/index.php?option=com_content&view=article&id=1539:hsaglobal-adds-advance-care-planning-functionality-to-ccms&catid=67:aged-care&Itemid=332, 14 August 2013 83 HSA Global Connecting Care, Connected Care Management System, http://www.hsaglobal.net/products-services/connected-care-management-system

Department of Health and Human Services grosvenor management consulting 77
Solution Description Use and reach
uses CCMS to manage two
mental health programs84.
HSAGlobal has engaged DoH
and NEHTA on how Advance
Care Plans in CCMS could be
published to the PCEHR.
Operates using a licensing
model.
9.1.2 PCEHR
The PCEHR provides a potential mechanism for the storage and sharing of
advance care directives. There is intent to include capture of advance care
directives within the PCEHR85. There is no current agreement for the
functionality of this component of the PCEHR. Nor is there a current
timeframe for the inclusion of advance care directive functionality. Currently
the PCEHR includes an Advance Care Directive Custodian component86. This
allows for the custodian of an individual’s advance care directive to be
recorded, but does not allow for the advance care directive itself to be
captured.
9.1.3 iPM
iPM is the patient administration system used in Tasmania. There is a clinical
alert within iPM called ‘Advance Care Directive’.
9.1.4 DHHS ICT platform
The Connected Care Strategy “seeks to deliver an information services
platform, offering a single, longitudinal view of patient / client
information.”87
There is potential for this platform to provide the ability to interface with:
4CEHR and/or
a community targeted mobile app for advance care directives and/or
advance care planning.
The Connected Care Strategy sets out that “all ICT systems within
Tasmanian Health will continue to use THCI as their primary identifier,
mapping to the IHI as required for PCEHR related activity. Nevertheless,
front-line staff will be empowered and encouraged to collect and update
84 Pulse+IT Magazine, HSAGlobal signs first Medicare Local for Mental Health Plan, http://www.pulseitmagazine.com.au/index.php?option=com_content&view=article&id=1434:hsaglobal-signs-first-medicare-local-for-mental-health-management&catid=16:australian-ehealth&Itemid=328 85 Written advice received from Department of Health, 29/08/2014 86 NeHTA, Advance Care Directive custodian v1.0.1, http://www.nehta.gov.au/implementation-resources/clinical-documents/EP-1745-2014 87 Connected Care Strategy v1.3 FINAL 29 November 2013, page 34

Department of Health and Human Services grosvenor management consulting 78
Medicare numbers to enable increased rates of matching with the IHI and
enable online billing processes.”88
As a result if the 4CEHR system was to be adopted it would need to use the
THCI (which it currently does not) to interface with the future DHHS
platform. It should be noted that the 4CEHR system has been built on the
same platform and is compatible with the systems proposed under the
Connected Care Strategy. It would therefore be possible to interface 4CEHR
with the portal in the future, potentially avoiding the duplication of data
entry and facilitating the communication of advance care directives across
health settings.
9.1.5 Comparison to 4CEHR
With the exception of the Collaborative Care Management Solution all of the
identified ICT solutions relate to enabling the communication of advance
care directives between individuals and their health care providers, rather
than supporting the process of advance care planning.
The PCEHR and DHHS Connected Care platform may both provide alternative
options to local interfaces between 4CEHR and other health management
information systems89.
88 Connected Care Strategy v1.3 FINAL 29 November 2013, page 44 89 Note: The PCEHR is currently an opt-in system which does not provide this functionality. It is unclear when this functionality will be introduced.
Department of Health and Human Services grosvenor management consulting 79
10 A consistent approach for Tasmania
Throughout this evaluation it was widely acknowledged that many palliative
care activities (including different approaches and training programs) are
currently being conducted within Tasmania. Stakeholders from both within
the State and other areas of Australia noted that this is often quite
confusing, with health professionals being presented with a range of
different approaches and tools.
Stakeholders were generally supportive of the development of a state-wide
approach to advance care planning. Throughout the consultations, a variety
of views were expressed regarding the development and implementation of
a consistent advance care planning approach or system in Tasmania.
Specific feedback was sought from stakeholders about what would be
required in a state-wide system, as well as how this should be implemented.
This section of the report considers what would be required to develop and
implement a state-wide approach to advance care planning. This will
address:
the design of a state-wide approach, including scope, stakeholders
and outcomes sought (section 9.1)
how a state-wide approach could best be implemented (section 9.2).
10.1 Developing a state-wide approach
During the consultations, stakeholders expressed a range of suggestions and
requirements for what a state-wide approach would need to include. These
have been broadly grouped into:
involvement of health professionals
required personal skills of health professionals
applicability and documents access across settings
content and detail
community education and promotion
systems.
Involvement of health professionals
As individuals are remaining in their own homes for longer, it was generally
agreed that a state-wide approach to advance care planning would need to
target all levels of the health system, including primary care. Engaging a
variety of health professionals within the community may support more
recent models for palliative care. During consultations, stakeholders referred
to changes in the palliative model as shown in Figure 5.

Department of Health and Human Services grosvenor management consulting 80
Figure 5 Approaches to palliative care90
Stakeholders suggested that there has been (or needs to be) a shift in
palliative care from a model where curative and palliative care are conducted
in isolation (A) to one where the two forms of care overlap (B). The inclusion
of advance care planning in the community setting may assist in developing
an environment where this can occur.
Despite common acceptance that advance care planning should occur in the
community, there was no consensus on the most appropriate time, or
setting, for this to occur. No health professional identified their profession as
being the most appropriate point to commence advance care planning.
Professions which were identified as potentially being appropriate to conduct
advance care planning in the community included:
GPs
Practice Nurses
Care Coordinators
Community Nurses
Allied Health Professionals (such as Social Workers)
Aged Care Assessment Teams.
Time and resource constraints were generally cited as reasons it would be
inappropriate to conduct advance care planning within particular health care
settings. Advance care planning discussions reportedly vary in time, ranging
from 10 to 15 minutes to several hours across multiple days/sessions (as
experienced using the LWDW approach). This time requirement was
considered to be a particular barrier to the completion of advance care
90 Murray, S., Kendall, M., Boyd, K., Sheikh, A. (2005) Illness trajectories and palliative care, http://www.cphs.mvm.ed.ac.uk/groups/ppcrg/images/pdf/Murray%20SA%202007%20Scot%20Prim%20Care%2066%2017-19.pdf
Curative CarePalliative
Care
Disease modifying or potentially curative
Supportive and palliative care
Bereavement care
A
B
Time

Department of Health and Human Services grosvenor management consulting 81
planning by those professions who only have short consultations with their
patients (such as GPs).
Additionally, it was identified that current billing arrangements may be a
barrier to the completion of advance care planning in some health care
settings. Health professionals will be unlikely to spend time conducting
advance care planning discussions if this is not something that they can
easily claim/bill for.
Required personal skills of health professionals
A range of skills were identified as being necessary for health professionals
involved in advance care planning and end of life care discussions.
Stakeholders believed that these skills should be introduced and promoted
as part of any state-wide training. It was emphasised that advance care
planning should not be undertaken by health professionals who do not have
the required personal skills.
Identifying suitable times to conduct advance care planning
Stakeholders suggested that it may not always be appropriate to discuss a
patient’s or resident’s preferences for end of life care. This conversation
should not be forced onto the person, instead, health professionals should be
educated to identify when the patient or resident is ready to have this
discussion and/or introduce it sensitively.
Appropriate, sympathetic and simple communication
Stakeholders suggested that health professionals need to be able to
communicate in a sympathetic manner which is easily understood by the
patient and their family. Avoiding the use of medical jargon was identified as
being particularly important in Tasmania due to the low level of health
literacy within the community. Communicating in an appropriate manner will
assist in ensuring that all parties understand and are comfortable with the
outcomes of the discussion. It will also assist in minimising the distress of
advance care planning discussions on individuals and their families.
Applicability and document access across settings
As discussed in section 6.2.8, different forms are accepted and recognised in
different health settings. This may result in a lack of transferability of
advance care planning information between the health settings.
To overcome this lack of transferability and recognition, it would be
beneficial for a state-wide approach to use consistent forms in all health care
settings. This would ensure that health professionals were familiar with the
format of the information and were easily able to identify such information in
a paper (or digital) file.
As multiple health professionals may be involved in the care of one person,
any advance care planning information also needs to be accessible. For
example, ambulances attending an emergency situation should be easily
able to determine whether someone has an advance care directive in place.
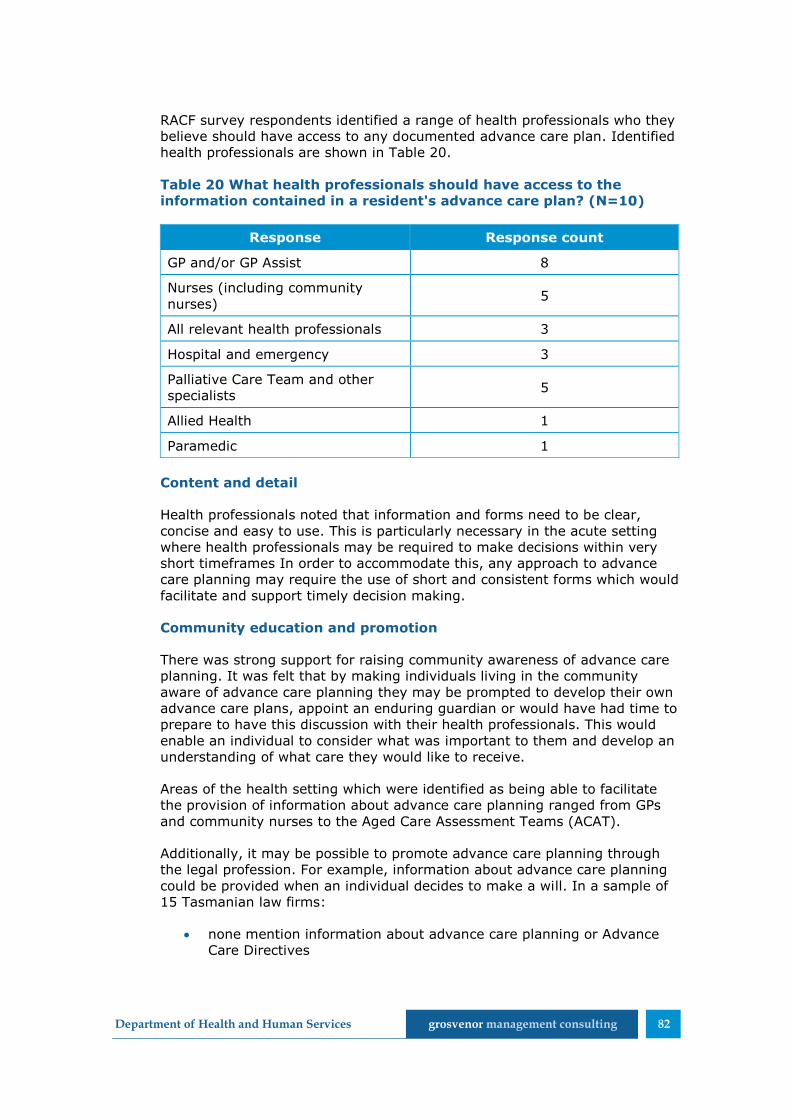
Department of Health and Human Services grosvenor management consulting 82
RACF survey respondents identified a range of health professionals who they
believe should have access to any documented advance care plan. Identified
health professionals are shown in Table 20.
Table 20 What health professionals should have access to the
information contained in a resident's advance care plan? (N=10)
Response Response count
GP and/or GP Assist 8
Nurses (including community
nurses) 5
All relevant health professionals 3
Hospital and emergency 3
Palliative Care Team and other
specialists 5
Allied Health 1
Paramedic 1
Content and detail
Health professionals noted that information and forms need to be clear,
concise and easy to use. This is particularly necessary in the acute setting
where health professionals may be required to make decisions within very
short timeframes In order to accommodate this, any approach to advance
care planning may require the use of short and consistent forms which would
facilitate and support timely decision making.
Community education and promotion
There was strong support for raising community awareness of advance care
planning. It was felt that by making individuals living in the community
aware of advance care planning they may be prompted to develop their own
advance care plans, appoint an enduring guardian or would have had time to
prepare to have this discussion with their health professionals. This would
enable an individual to consider what was important to them and develop an
understanding of what care they would like to receive.
Areas of the health setting which were identified as being able to facilitate
the provision of information about advance care planning ranged from GPs
and community nurses to the Aged Care Assessment Teams (ACAT).
Additionally, it may be possible to promote advance care planning through
the legal profession. For example, information about advance care planning
could be provided when an individual decides to make a will. In a sample of
15 Tasmanian law firms:
none mention information about advance care planning or Advance
Care Directives

Department of Health and Human Services grosvenor management consulting 83
seven (47%) mention enduring guardians, however, none provided
an explanation
14 (93%) mentioned wills.
Systems
Some stakeholders felt that benefits may be experienced through the use of
a state-wide system. Specific system requirements were identified which
may encourage its use:
designed in a way which is simple, practical and easy to use
should assist GPs and other staff in making complex decisions (for
example, calculating dose and providing transparency around the
prescription of opioids)
integrate with other systems to avoid duplication of data entry or
multiple sources of truth.
While there was broad support for simplifying the communication of advance
care planning information, there was not universal support for the use of a
system to achieve this. Stakeholders provided a number of examples of why
a system may not be used/ideal. This included:
lack of alignment with existing DHHS tools and systems
lack of consistency with the broader ICT work being undertaken by
DHHS
a reluctance to use multiple systems to complete a task (especially if
multiple log-ins are required)
concerns around the duplication of data which may result in
conflicting patient records.
It should be noted that the barriers above are general in nature and are not
specifically targeted at 4CEHR. As discussed in section 9.1.4, it is
acknowledged that the 4CEHR system has been built to be compatible and
integrate with other DHHS systems to be established under the Connected
Care Strategy.
Learnings from the review of the Liverpool Care Pathway
Similar to LWDW and the other advance care planning approaches, the
Liverpool Care Pathway was designed to improve end of life care for all
patients. The pathway specifically targets the final days of life and can be
used regardless of care setting91. Following numerous criticisms of the
approach in the media, a major review of this pathway was undertaken.
91 Independent Review of the Liverpool Care Pathway, More Care, Less Pathway, A Review of the Liverpool Care Pathway, https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/212450/Liverpool_Care_Pathway.pdf, page 5

Department of Health and Human Services grosvenor management consulting 84
Learnings from this review should be considered in the development and
implementation of any state-wide approaches in Tasmania. Some of the
relevant learnings/recommendations include:
variable definitions and understanding of the term ‘end-of–life’ (from
last year of life to last days of life) lead to incorrect use of the
pathway
the term ‘pathway’ should not be used in relation to care in the last
year of life as it can carry connotations of assisted death
the use of a dying pathway should not be financially incentivised
evidence gaps exist for care provision in the last year of life
honest communication was fundamental to providing appropriate care
– acknowledging death and dying, futility of medical intervention and
uncertainty
the need to plan for and support ‘out of hours’ care to avoid crisis
the importance of documentation
that staff competence and resourcing level were a serious concern.
Duplication and communication
While it was suggested that all health professionals should be educated and
able to undertake advance care planning, potential barriers were identified
to the practical use of this approach. The involvement of multiple individuals
in advance care planning may result in confusion around which is the latest
(and most accurate) version of a patient’s advance care directive.
Additionally, it is possible that some health professionals engaged with a
patient may be unaware that an advance care directive exists, preventing its
appropriate use.
To overcome this, the importance of regular communication with the patient,
and if relevant, substitute decision maker was emphasised.
Current practice in RACFs
As part of this evaluation an online survey was made available to all RACFs
within Tasmania. The RACF survey sought to identify existing and preferred
approaches to advance care planning within each of the RACFs.
All RACF survey respondents (100%, N=15) indicated that their RACF
engaged residents in conversations about their end of life care. Despite this,
the RACF survey responses showed inconsistencies in the way that advance
care planning is conducted in RACFs.
The proportion of residents at each RACF engaged in these discussions
varied (Figure 6). Additional consultation and analysis would be required to
determine why some of the facilities only engaged ‘some’ or ‘few’ residents
in these discussions.
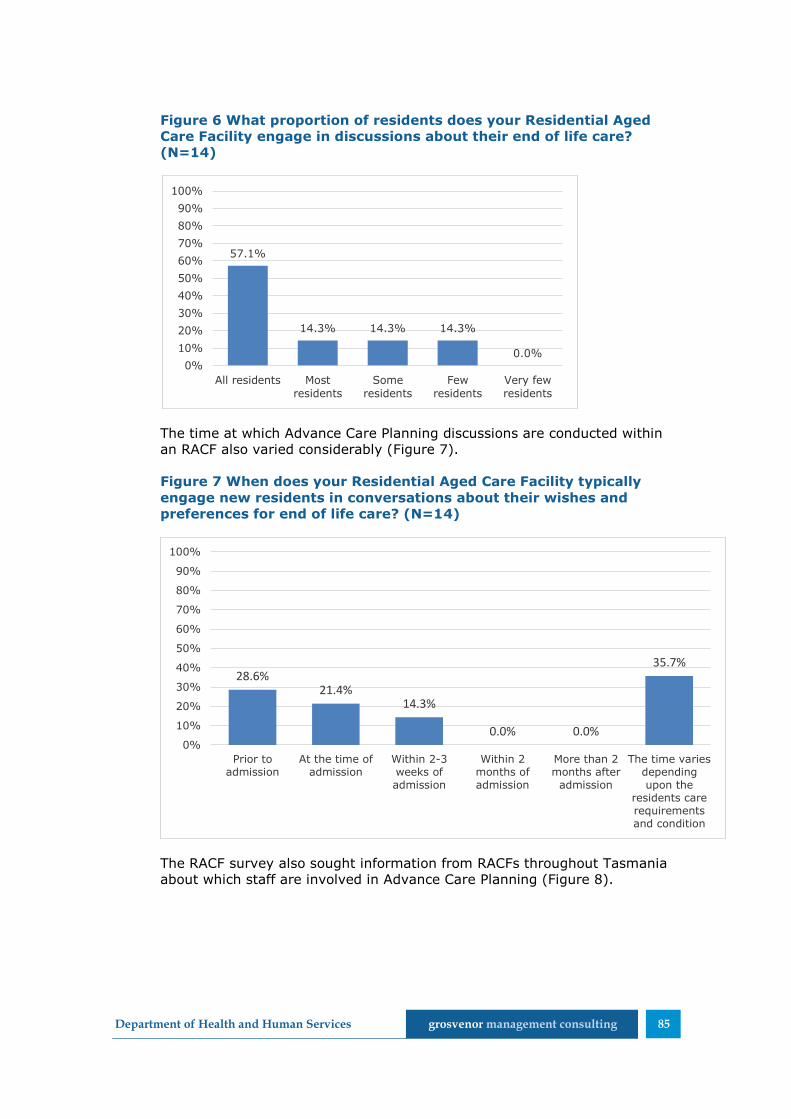
Department of Health and Human Services grosvenor management consulting 85
Figure 6 What proportion of residents does your Residential Aged
Care Facility engage in discussions about their end of life care?
(N=14)
The time at which Advance Care Planning discussions are conducted within
an RACF also varied considerably (Figure 7).
Figure 7 When does your Residential Aged Care Facility typically
engage new residents in conversations about their wishes and
preferences for end of life care? (N=14)
The RACF survey also sought information from RACFs throughout Tasmania
about which staff are involved in Advance Care Planning (Figure 8).
57.1%
14.3% 14.3% 14.3%
0.0%0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
All residents Mostresidents
Someresidents
Fewresidents
Very fewresidents
28.6%21.4%
14.3%
0.0% 0.0%
35.7%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Prior toadmission
At the time ofadmission
Within 2-3weeks ofadmission
Within 2months ofadmission
More than 2months after
admission
The time variesdependingupon the
residents carerequirementsand condition

Department of Health and Human Services grosvenor management consulting 86
Figure 8 Who is commonly involved in discussions about patient’s
wishes and preferences for end of life care? (N=14)
As shown in the above figure, advance care planning discussions at the
respondent’s facilities commonly involve the Resident, Family and a
Registered Nurse. However, a broader range of staff may be involved,
including the GP (85.7%), Enrolled Nurses (50%) and care staff (35.7%).
RACF survey results suggest that the formal documentation of advance care
plans is a common practice throughout the state with 92.9% (13)
respondents currently completing this. Of the respondents formally
documenting advance care plans, 91.7% (11) do this in an internally
consistent format.
RACFs within Tasmania are still largely reliant upon paper based records to
store advance care planning information (Figure 9). This was also identified
through the consultations conducted with LWDW participants.
Figure 9 How are the documented advance care plans generally
stored? (N=11)
Despite currently relying on paper based records, seven (87.5%) of eight
RACF survey respondents felt that the implementation of an electronic end
100.0% 100.0% 100.0%
85.7%
50.0%
35.7%
28.6%
21.4%
14.3%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Resident Family RegisteredNurse
GP EnrolledNurse
Care staff Other(pleasespecify)
Friends Palliativecare
specialist
9%
64%
27%
0%
Electronically
In a paper record
Both electronically andon a paper record
Other (please specify)

Department of Health and Human Services grosvenor management consulting 87
of life care planning system would be of value for their RACF. Respondents
noted that such a system would be of value providing it was consistent and
recognised by all stakeholders. One respondent also noted that it would be
of value if such a system could be applied both in the community and RACF
settings.
10.2 Implementing a state-wide approach
A range of factors were identified as being crucial to achieving consensus for
and successfully implementing a state-wide approach. These factors are
discussed below and have been broadly grouped into:
authority and management
communication, engagement and consultation
clarity of purpose
certainty
understanding of benefits
meeting the specific needs of health professionals
systems.
Authority and management
In order to successfully implement a state-wide approach, it is important to
have a well-managed project. Stakeholders highlighted that it would be
particularly beneficial to have both an appropriate steering committee and
project team while implementing a state-wide advance care planning system
or approach.
Stakeholders suggested that it would be necessary to establish one steering
group which has the appropriate authority to drive the project’s
development and/or implementation.
The different health professions and regions within Tasmania each have
different needs and requirements. In order to ensure that a system
appropriately meets the needs of all health professionals and stakeholder
groups, they would require appropriate representation on the steering
committee.
Stakeholders highlighted the importance of ensuring that a diverse range of
individuals were included in the steering group. It was identified that this
should include not only representatives from each health profession
impacted by the state-wide approach, but also representatives from each of
the different regions and consumers.
By ensuring diverse membership to the steering group, it is possible each
health profession within each region will feel that their particular needs and
requirements have been heard and incorporated. This may assist in
increasing the uptake and ongoing use of any state-wide approach or
system.

Department of Health and Human Services grosvenor management consulting 88
In addition to the steering group, stakeholders highlighted the importance of
having an appropriate project team with sufficient project management
resources and skills. This team would need to have the authority and project
management skills to manage the project timeframes and deliverables,
engage with stakeholders, as well as having appropriate health and medical
knowledge.
Communication, engagement and consultation
Mutual benefits can be achieved through the ongoing engagement and
consultation of health professionals who would be required to use a new
system or process.
Stakeholders noted that they become frustrated if they are unable to
regularly access information about a project in which they are interested or
will be impacted by. This will assist in managing stakeholder expectations,
particularly if delays are encountered or changes occur.
During the consultations a number of opinions about what stakeholders
considered would be appropriate, beneficial and useful in an advance care
planning system or approach were identified (as discussed in section 10.1).
These views should be taken into account during the development (or
selection) and implementation of a state-wide approach or system.
Understanding the requirements and views of the different stakeholders will
provide a better understanding of what the end-users will demand, and
therefore what they are likely to accept. The state-wide approach or system
can then be tailored (or selected) to best fit these needs and requirements,
providing users with what they consider to be useful. Aligning the approach
with the needs and requirements of the stakeholders may assist in
encouraging uptake and use.
Clarity of purpose
In order to encourage its uptake and ongoing use, the purpose and intent of
a state-wide approach or system would need to be clearly articulated to all
relevant health care professionals. This will ensure that all health
professionals have a common understanding and expectations of the system
or approach.
Certainty
As discussed in section 7.3.2, multiple changes occurred to the LWDW
project during its development and implementation. These changes resulted
in some of the RACFs feeling uncertain about whether the training they were
receiving and system that they were using would ultimately be replaced or
changed. This feeling was exacerbated when the 4C system was not
ultimately used or further developed.
As a result of this, the RACFs expressed some reluctance to engage with
new approaches or systems until they were certain that they would be used
and supported on an ongoing basis.
Department of Health and Human Services grosvenor management consulting 89
Understanding of benefits
Health professionals are commonly driven to adopt or use a new system or
approach based on available evidence about the benefits of changing. This
often involves relying on academic and scholarly articles about the ability of
the approach or system to achieve its intended outcome and result in
benefits to users and/or patients. These health professionals are unlikely to
undertake the additional work associated with learning how to use and
implement a new approach or system if the benefits are unclear.
It would therefore be important to highlight the benefits of a state-based
approach to health professionals to encourage its uptake and ongoing use.
This may include any benefits and achievements which were realised during
a pilot program or which have been published in academic journals.
Meeting the specific needs of health professionals
The specific needs and requirements of health professionals should be
considered as part of any state-wide approach or system. For example,
consulted health professionals often highlighted that they were time poor
and may be unable to take on additional tasks. The time requirements of
using any state-wide system or approach on participating health
professionals would therefore need to be carefully considered.
Any state-wide approach or system should also be simple and easy to use,
complementing the other tools and systems currently in use.
Systems
A number of ICT projects are currently being progressed by DHHS and the
THO’s which would potentially impact upon the implementation of a state-
wide Advance Care Planning system. This includes the recently developed
Connected Care Strategy.
The Connected Care Strategy has been designed to provide a clear, well-
articulated ICT vision and strategy for DHHS. It “defines the vision, goals,
principles, architecture and plans that will be delivered by 2016, in order to
place care consumers at the centre of their own care, and to be better utilise
ICT as an important lever in delivering a more accessible, equitable and
sustainable Health and Human Services system”92.
The vision of the Connected Care Strategy is to develop a Connected Care
Platform which:
“…underpins an increasingly accessible, equitable and sustainable
Tasmanian Health and Human Services system by enabling and
supporting new and emerging models of care, based on the
provision of high quality, longitudinal care consumer centric
information
… support[s] improving care consumer access and engagement,
streamlining and standardising the care consumer journey and
92 Connected Care Strategy v1.3 FINAL 29 November 2013, page 8
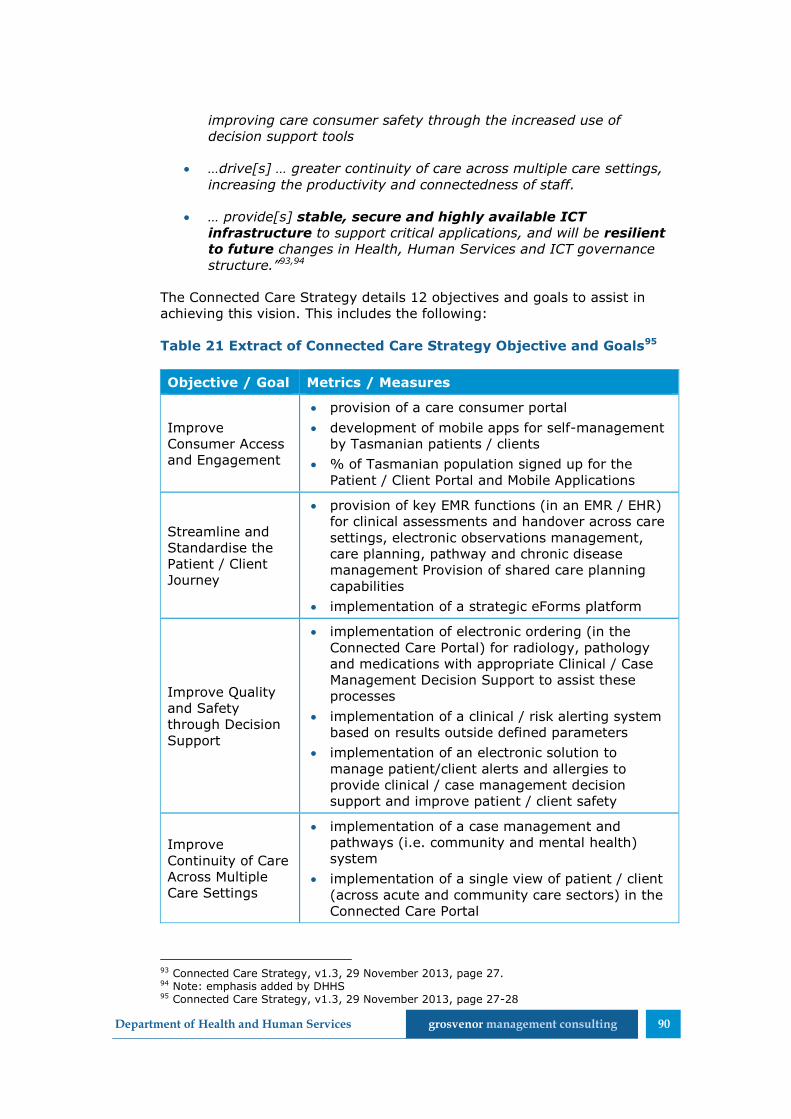
Department of Health and Human Services grosvenor management consulting 90
improving care consumer safety through the increased use of
decision support tools
…drive[s] … greater continuity of care across multiple care settings,
increasing the productivity and connectedness of staff.
… provide[s] stable, secure and highly available ICT
infrastructure to support critical applications, and will be resilient
to future changes in Health, Human Services and ICT governance
structure.”93,94
The Connected Care Strategy details 12 objectives and goals to assist in
achieving this vision. This includes the following:
Table 21 Extract of Connected Care Strategy Objective and Goals95
Objective / Goal Metrics / Measures
Improve
Consumer Access
and Engagement
provision of a care consumer portal
development of mobile apps for self-management
by Tasmanian patients / clients
% of Tasmanian population signed up for the
Patient / Client Portal and Mobile Applications
Streamline and
Standardise the
Patient / Client
Journey
provision of key EMR functions (in an EMR / EHR)
for clinical assessments and handover across care
settings, electronic observations management,
care planning, pathway and chronic disease
management Provision of shared care planning
capabilities
implementation of a strategic eForms platform
Improve Quality
and Safety
through Decision
Support
implementation of electronic ordering (in the
Connected Care Portal) for radiology, pathology
and medications with appropriate Clinical / Case
Management Decision Support to assist these
processes
implementation of a clinical / risk alerting system
based on results outside defined parameters
implementation of an electronic solution to
manage patient/client alerts and allergies to
provide clinical / case management decision
support and improve patient / client safety
Improve
Continuity of Care
Across Multiple
Care Settings
implementation of a case management and
pathways (i.e. community and mental health)
system
implementation of a single view of patient / client
(across acute and community care sectors) in the
Connected Care Portal
93 Connected Care Strategy, v1.3, 29 November 2013, page 27. 94 Note: emphasis added by DHHS 95 Connected Care Strategy, v1.3, 29 November 2013, page 27-28

Department of Health and Human Services grosvenor management consulting 91
Objective / Goal Metrics / Measures
deliver integration of patient medical records with
Ambulance Tasmania
As the Connected Care Strategy and Platform are being developed to be
used by all DHHS clinicians in both the acute and community care sectors,
they are likely to have a wide reach and impact.
Members of the DHHS IT team expressed reluctance for standalone,
independent systems to be implemented for use within the Tasmanian
Health System. There is a preference for all new ICT projects to align with
both the Connected Care Strategy and Platform where possible. The
stakeholders also commented that any systems which are built should be on
a flexible platform.
Any state-wide system to support advance care planning should be
developed and implemented in the context of the broader ICT work being
undertaken by DHHS. This will assist in ensuring that the system aligns with,
and is supported by, the broader DHHS ICT environment, potentially
increasing the robustness of the system96.
96 Note: While the 4CEHR system intended to meet these criteria this was not realised. As discussed in section 10.1, both 4CEHR and the Connected Care Platform are built on the Miya Platform and could therefore be integrated if required.
Department of Health and Human Services grosvenor management consulting 92
11 Conclusions
11.1 Is the LWDW the most appropriate approach to advance care planning in aged care for application across Tasmania? (KEQ5)
To answer this question Grosvenor canvassed other approaches to advance
care planning in residential aged care homes in Tasmania. We found that the
RACPA approach to advance care planning is very similar to LWDW, and has
a number of advantages over LWDW. Namely;
the RACPA toolkit is supported by DSS as the national approach
the RACPA tools and guidance are well developed, available online,
and are free of charge
RACPA has broader reach, in Tasmania and nationally
there is ongoing support for the RACPA toolkit via Decision Assist.
Given that RACPA appears to have a more substantial reach than LWDW in
Tasmania, and is supported as the national approach, it may be a more
appropriate choice for Tasmania.
11.2 What will it take to establish a sustainable LWDW program
state-wide in Tasmania? (KEQ4)
As we have found that RACPA appears to be a more appropriate choice for
Tasmania, we have not sought to describe how to establish LWDW as a
sustainable program. Instead we have drawn upon the information collected
in the evaluation to describe the key strengths and learnings from the
LWDW pilot and reflect how Tasmania could further support the
implementation of RACPA, or another advance care planning approach, using
these strengths and learnings.
Change management and implementation support
The implementation of a state-wide approach to advance care planning is a
major endeavour requiring engagement and change across the health care
system in Tasmania. The importance of organisational readiness for
successful implementation was particularly apparent in the LWDW pilot. For
example the changes in leadership at Umina Park during the pilot created an
organisational environment that was no longer ready to implement LWDW.
The primary strength of the LWDW approach that is not present in the
RACPA approach to the same extent is the facilitated culture change and
implementation support approach. This key strength of the LWDW program
could be utilised in conjunction with RACPAs broad use, online presence and
polished documentation to further improve advance care planning and end-
of-life care.
Recommendation 1: It is recommended that DHHS supports RACPA as the advance care planning approach for Tasmanian RACFs.
Department of Health and Human Services grosvenor management consulting 93
Advance care planning approach across health settings
It is acknowledged that the RACPA currently focuses on the RACF setting
and does not address the need for advance care planning in the community
or hospital settings.
The different health settings within Tasmania are likely to have different
requirements and resources available to conduct and support advance care
planning. The ‘how to’ guidance and support provided to healthcare
professionals as part of a sustainable state-wide approach needs to
recognise the constraints of each setting and be able to be supported within
the available resources and finances and meet the user needs.
That is, implementation design needs to consider:
when to do something
how long it will take on average
what needs to be achieved
how it will be used and by whom
cost and risk
resources and sources of knowledge available and relevant to each
health setting and how these can be accessed (including expert
support).
These may vary in each setting based on the practice and processes already
in place. For example, conduct of a DPAG process over five hours is not
practical within RACF resourcing. However, a short preliminary introduction,
followed by a detailed conversation, and then a short follow-up to conclude
and confirm the planning over two weeks may be.
Tailoring the state-wide approach to each health care setting and ensuring
its appropriateness given the available resources will assist in achieving its
sustainability. Healthcare settings are much less likely to use an approach on
an ongoing basis which is not considered to be practical and/or relevant to
their needs.
Recommendation2: It is recommended that DHHS considers investing in
a supported implementation model for RACPA to embed and improve
advance care planning in Tasmanian RACFs.
Recommendation 3: It is recommended that DHHS ensure appropriate
change management practices are utilised to support the state-wide
implementation of RACPA (or another approach). Change management
activities should focus upon ensuring organisational readiness for the
change, and draw upon the strengths of LWDW in facilitating culture change and supporting on the ground implementation.

Department of Health and Human Services grosvenor management consulting 94
A number of other projects (such as Enhancing Aged Care through better
Palliative Care) provide examples of how advance care planning can be
implemented in the community setting. Additionally, the GSF could be
utilised by DHHS as an example of how the central principles of an advance
care planning approach can be tailored to, and applied within, a range of
health care settings.
Further, the pilot identified that it is important for the outputs of an advance
care planning approach to be known and accepted across health settings to
be effective. I.e. An advance care plan developed in a RACF needs to be
used outside of this setting to be effective, including by ambulance, hospital
and after hours GP services.
Engage and seek commitment and support from all health settings
and professionals
In order to successfully implement a state-wide approach it is necessary to
engage and gain commitment from all health settings and professionals that
will be impacted by the changes.
The LWDW and 4CHER projects highlighted:
the differing needs and preferences of the various health professions
which would need to be identified and addressed during the
development and implementation of any state-wide system/approach
the importance of engaging GPs to ensure the successful adoption of
improved advance care planning within RACFs and the community.
This also extends to engagement of afterhours services such as GP
Assist to ensure advance care plans are appropriately used in crisis
situations occurring outside of business hours. Failure to engage GPs
is likely to hinder acceptance and use of any state-wide approach
Recommendation 4: In order to ensure the ongoing sustainability of a
state-wide approach, it is recommended that DHHS ensures the state-wide
approach:
is practical and appropriate for the capabilities and limitations of each
health care setting
is able to be supported from within the healthcare setting (ie. within
the available resources)
educates each health settings about the support which is available,
including from experts such as the Specialist Palliative Care Service.
It is recommended that DHHS draws upon other projects such as
Enhancing Aged Care through better Palliative Care and the GSF to inform
how advance care planning can be implemented beyond RACFs, that is, in
the community and other health settings.
Recommendation 5: It is recommended that DHHS engage sufficiently
with all health settings to overcome barriers to the recognition and use of
advance care planning outputs across health settings.

Department of Health and Human Services grosvenor management consulting 95
the criticality of securing senior management support to successfully
achieve and embed culture and practice changes
the importance of engaging senior management and senior staff with
clarity of purpose and requirements/commitments. At the outset a
clear road map of the journey should be provided as well as realistic
estimates of resource effort and costs.
It is noted that health professionals can be difficult to engage in a timely
manner. For example, both the LWDW project and this evaluation found it
problematic to appropriately engage GP Assist. Early engagement with these
groups is likely to provide the best opportunity to gain their input and views
within the required timeframes, and ensure that these can be used to inform
development and implementation.
If there are data collection requirements for evaluative purposes these
should also be made clear from the outset and along with any guidance and
tools to support data collection.
Engage with hubs
A key learning from the LWDW pilot is not to stagger roll-out by setting
type, but rather engage ‘hubs’ of relevant stakeholders concurrently. A hub
could be relatively small or large, but it would include at least:
1 RACF
each GP servicing that RACF (and potentially the entire general
practice of each relevant GP)
the pharmacy servicing the RACF
the hospital (or hospitals) primarily used by the RACF
local ambulance services
Recommendation 6: It is recommended that DHHS engages more
broadly with health professionals to implement a system wide approach to
advance care planning which includes the community and acute care
settings. DHHS should ensure all stakeholders and health care settings are
appropriately engaged and commit to the state-wide approach. Any
engagement should be undertaken with clarity of purpose and
requirements/commitments. In particular DHHS should engage:
all relevant health professionals during the development and
implementation of the approach to ensure that their unique needs are
identified and appropriately addressed
senior management within affected health organisations to seek
endorsement of the implementation and ongoing use of the approach
within their facility.
Recommendation 7: It is recommended that DHHS identify any data
collection requirements during implementation of the state-wide approach.
Department of Health and Human Services grosvenor management consulting 96
allied health professionals who work at the RACF
specialist palliative care services in the area.
Within the same localised hub other activities in the BAPC framework could
be promoted simultaneously to raise awareness in the broader local
community and allow for a system wide advance care planning approach to
be implemented. The education of community health professionals alongside
professionals from RACFs, hospitals and general practices within their local
region will ensure that all health sectors represented within the region are
aware of and using the same approach.
It makes sense to start with smaller hubs at first. Once the project is fully
established (and if there is sufficient capacity) larger sized hubs could be
engaged (i.e. multiple RACFs and by extension larger groups of other health
providers). There are benefits to be gained by involving multiple providers of
one type in capacity building/culture change sessions. The benefits are
derived primarily from the sharing of experiences and practice with each
other.
Targeting of RACFs for engagement could involve are range of factors, such
as:
willingness (including senior management support as detailed above)
quality of advance care planning (eg facilitated by state-wide use of
the National Standards Assessment Program (NSAP)), and/or
hospitalisation rates as indicators of quality).
Recommendation 8: It is recommended that DHHS implements a state-
wide approach through a ‘hub’ model which concurrently targets cross
sector health professionals in the same location at the same time as
RACFs.
Recommendation 9: It is recommended that DHHS consider how the
hub-based implementation model can support the sharing of experiences
and practices between providers in the same and across health settings to
improve practices.
Recommendation 10: It is recommended that DHHS integrates the roll-
out of a state-wide advance care planning approach with the BAPC
framework to simultaneously raise community awareness of advance care
planning.
Recommendation 11: It is recommended that DHHS targets those
RACFs which have the greatest opportunity to improve under the
approach. This should be assessed against their willingness to participate,
quality of advance care planning and hospitalisation rate.
Department of Health and Human Services grosvenor management consulting 97
11.3 Does 4CEHR have the capacity to support the goals of LWDW in Tasmania? (KEQ2)
AND Is 4CEHR the most appropriate system to support LWDW and advance
care planning in Tasmania?
The 4CEHR system does not currently have the capacity to support the goals
of LWDW (or another advance care planning approach such as RACPA) in
Tasmania. This is for a number of reasons:
the initial pilot of 4CEHR in residential aged care homes was not
completed, so there is not detailed knowledge of its suitability
substantial updates would be required to prepare the 4CEHR system
prior to the commencement of any further pilot testing.
Thus there is need for further investment prior to determining 4CEHR’s
capacity to be utilised state-wide and support the goals of an approach such
as RACPA. While there is evidence supporting the need to improve end of life
care through advance care planning approaches, this alone does not make
4CEHR the most appropriate option or necessarily worth investment.
To inform this investment decision the following should be considered:
1. How will widespread uptake of the system be achieved across
settings (eg RACF, GP, acute) sufficient to justify investment?
2. Is achievement of downstream outcomes incumbent upon (or
sufficiently promoted by) an ICT system?
These are demonstrated by the draft program logic in Figure 10.
The qualitative information provided in this evaluation indicated system
uptake/use will be difficult to achieve.
There is not sufficient information available to provide any indication on the
likely outcomes of question 2 above.
Other options for supporting or enabling the communication of advance care
directives include:
use of common forms within settings and gaining endorsement and
recognition across settings (we note that this has already
commenced)
wait for PCEHR functionality and continue to promote uptake of
PCEHR in the interim
migrate core functionality of the 4CEHR into the Connected Care
platform.
Advance care planning functionality may be further supported by
investigating the willingness of major RACF and GP software providers to
further develop their products in this area in a way that is consistent with
the RACPA approach.

Department of Health and Human Services grosvenor management consulting 98
Figure 10 Draft program logic
11.4 Is 4CEHR consistent with the approach of LWDW? (KEQ1)
A key caveat to answering this question is the fact that piloting of 4CEHR by
residential aged care facilities was not completed due to system issues and
uncertainty of future support. The conclusion to this key evaluation question
is limited by the lack of a true pilot to generate the necessary data for
evaluation.
Lack of skills, knowledge and
capability
Lack of documentation
Difficultly sharing
information across settings
Culture change driven training
and implementation
support
ICT system supports
processes and activities including
documentation and
communication
Participation in training across
settings
Uptake of ICT system across
settings
Conversations about end of
life care choices are consistently
undertaken with individuals (and families)
Individuals receive person centred care
which respects their values and is consistent with
their choices
Futile treatment is avoided
There is shared understanding
among carers and individual/family
Individuals are empowered to
make care decisions
because they understand the likely benefits, costs and risks
Individual decisions and preferences
are documented
and communicated
Care plans reflect
individuals decisions and preferences
Regular review takes place
that involves individual and
changes in circumstance
1. Not clear if widespread uptake across settings will
be achieved 2. Is achievement of downstream
outcomes incumbent upon
ICT system?
Recommendation 12: It is recommended that DHHS considers the
options for supporting communication of advance care directives in
Tasmania and make a decision on the further investment in a 4CEHR pilot.
In making this decision, DHHS should analyse the core functionality of the
4CEHR to determine whether it can be integrated into existing systems,
including the Connected Care Platform.
If further investment in 4CEHR is supported:
it should be integrated with relevant software and platforms
it should be appropriately named in a descriptive manner and have state-wide relevance (rather than a regional focus)

Department of Health and Human Services grosvenor management consulting 99
Furthermore, given conclusion 1, it appears necessary to comment upon the
capability of 4CEHR to support other advance care planning approaches,
especially RACPA. We have done so below.
At a high level the 4CEHR system appears to be consistent with the
approach of LWDW. It encompasses functionality which is likely to have the
ability to support many of the key LWDW processes and activities for
advance care planning in residential aged care facilities. Such as: coding,
use of diagnostic tools (Karnofsky, CAMS), storage of current enduring
guardian or person responsible details and advance care directives, supports
DPAG.
The similarity of RACPA and purposeful decoupling of 4CEHR from GSF, also
gives 4CEHR the potential to support other advance care planning
approaches.
However, some 4CEHR content such as the CAPs and opioid calculator is less
mature and duplicates other existing sources of information some of which
are maintained by DHHS. For example, some duplication has been identified
between:
the Tasmanian Palliative Care HealthPathways and 4CEHR CAPS
Tasmanian Palliative Care formularies and 4CEHR opioid calculator.
Where an existing information source is already available and maintained,
there may be redundancy in including this functionality in the 4CEHR
system. Instead a link could be provided to existing materials through the
4CEHR system. The inclusion of existing DHHS tools within the system would
assist in ensuring that all health professionals are accessing and utilising the
same guidance materials (consistency of care).
In comparing the LWDW approach and 4CEHR system there were also gaps
in coverage identified. It is unclear whether it would be necessary for a
state-wide system to include/support this functionality. These gaps are
detailed below:
after death audits (or other performance reporting capability for
continuous quality improvement and performance monitoring)
guidance/support within the system is limited (i.e. ‘help’ function)
there is potential for person centeredness to be further facilitated –
eg. patient able to access via PCEHR integration
care of carers and family/friends is not covered by the system
unclear how aligned/suitable it would be to a LWDW program adapted
to other settings. For example in the community would more
emphasis need to be placed on the ‘identify’ task.

Department of Health and Human Services grosvenor management consulting 100
11.5 How does 4CEHR interface with the national program to implement a PCEHR? (KEQ3)
4CEHR provides supportive functionality to undertake advance care planning
and improve end of life care based on the LWDW approach. The system is
technically able to upload information to the PCEHR, although this is not
enabled, and the PCEHR does not currently contain advance care directives.
The PCEHR has the potential to support sharing of advance care directives
between health settings in the future (with or without 4CEHR). The ability to
do this, and for it to be used, is still some time off.
11.6 How can Tasmania move beyond trials and establish a state-wide program of coordinated communication for advance care
planning? (KEQ6)
4CEHR is not ready to proceed to state-wide roll-out. It requires two key
decisions going forward:
whether to invest further in 4CEHR and run a pilot
whether to proceed to roll-out based on the pilot outcomes.
As detailed in section 11.1 RACPA appears to be a better supported, lower
cost option for Tasmania to adopt as a state-wide advance care planning
approach in RACF settings than LWDW.
There is already a range of initiatives at a State and Commonwealth level,
which are gaining traction and supporting advance care planning (e.g.
implementation of Medical Goals of Care across the acute sector with
No recommendation can be made at this time due to the uncertainty around the PCEHR.
Recommendation 13: If further investment in 4CEHR is supported it is
recommended that DHHS:
review the existing content of 4CEHR and only retain that which is
considered to be a ‘core’ requirement by stakeholders/users
analyse the 4CEHR system to identify any duplication between its
functionality/content and existing DHHS tools and materials
provide appropriate linkages to existing DHHS materials within the
system rather than further developing the 4CEHR specific content
conduct a gap analysis to identify any omissions in the system’s ability
to address the requirements of/support LWDW or the RACPA and
determine whether the inclusion of this capability is required.
Department of Health and Human Services grosvenor management consulting 101
potential adaption and adoption in RACFs and the community). The
development of a state-wide approach needs to:
take into account pre-existing programs and activities to avoid
duplication and achieve sufficient integration
address the acceptability of existing and alternative approaches
within a state-wide model
encourage and monitor uptake and implementation.
A range of resources and training materials are available in these alternative
approaches which could be leveraged as part of a state-wide approach. For
example, GP training activities were developed and approved for LWDW
which could be utilised during the implementation of the state-wide
approach. It would be necessary to review the appropriateness of these
training materials prior to use.
Some key advance care planning initiatives and approaches which are
currently being utilised were identified as part of this evaluation and have
been highlighted throughout this report. While the approaches detailed in
this report should not be considered to be exhaustive, they provide an
overview of the types of activities which are presently being conducted. It is
also evident through this evaluation that greater awareness and knowledge
of advance care planning is required within the community and across the
health sector prior to/as part of the implementation of any state-wide
approach.
Considerations for establishing a state-wide approach are detailed in section
1010.
Recommendation 14: It is recommended that DHHS actively seeks to
avoid duplication and achieve integration with other State and
Commonwealth approaches to advance care planning through the state-
wide approach.
Recommendation 15: It is recommended that DHHS review the
appropriateness of any approved LWDW training materials to the state-
wide approach. If relevant and appropriate, DHHS should refine and
utilise these materials to support state-wide implementation.
Recommendation 16: It is recommended that DHHS monitors the
uptake and implementation of the state-wide approach to advance care
planning to ensure it has been consistently adopted across the various
healthcare settings.
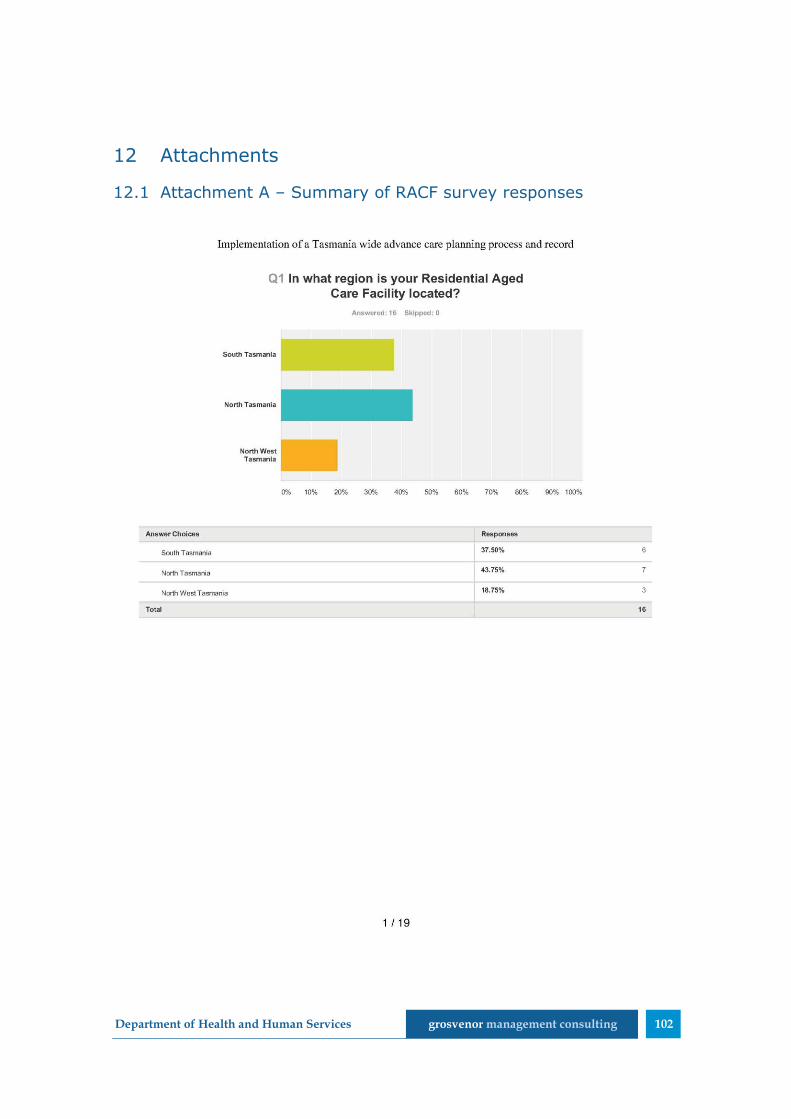
Department of Health and Human Services grosvenor management consulting 102
12 Attachments
12.1 Attachment A – Summary of RACF survey responses
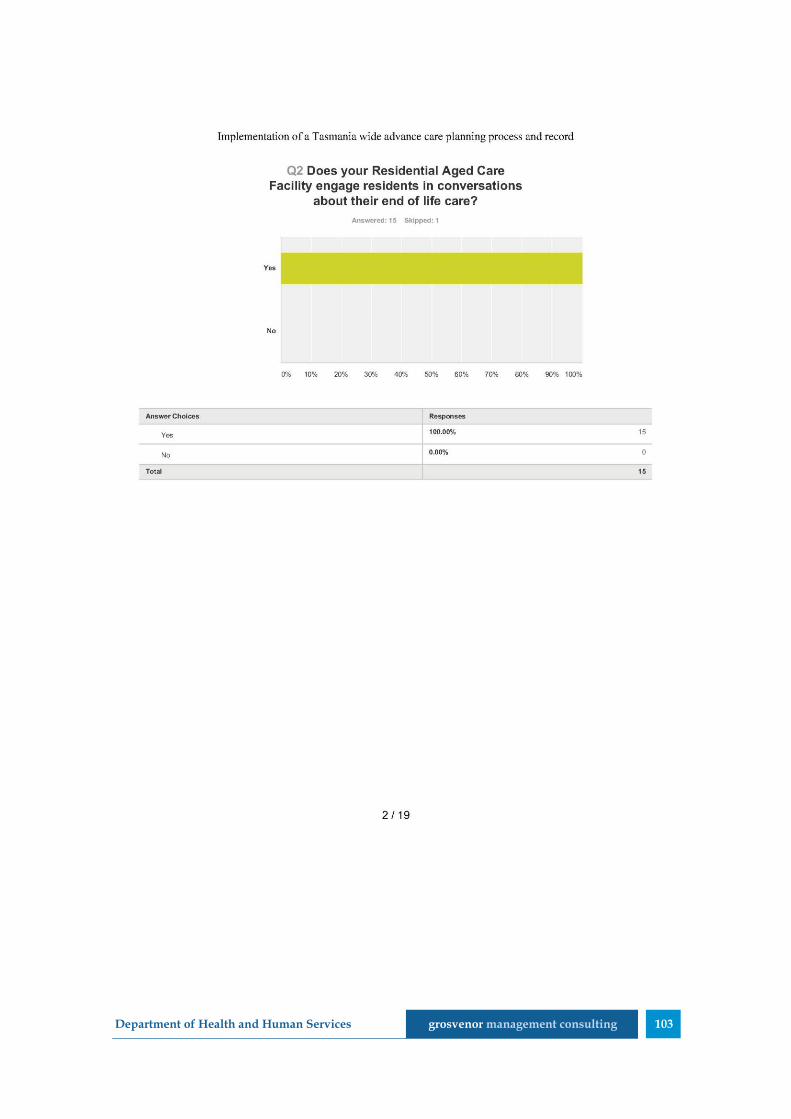
Department of Health and Human Services grosvenor management consulting 103

Department of Health and Human Services grosvenor management consulting 104

Department of Health and Human Services grosvenor management consulting 105
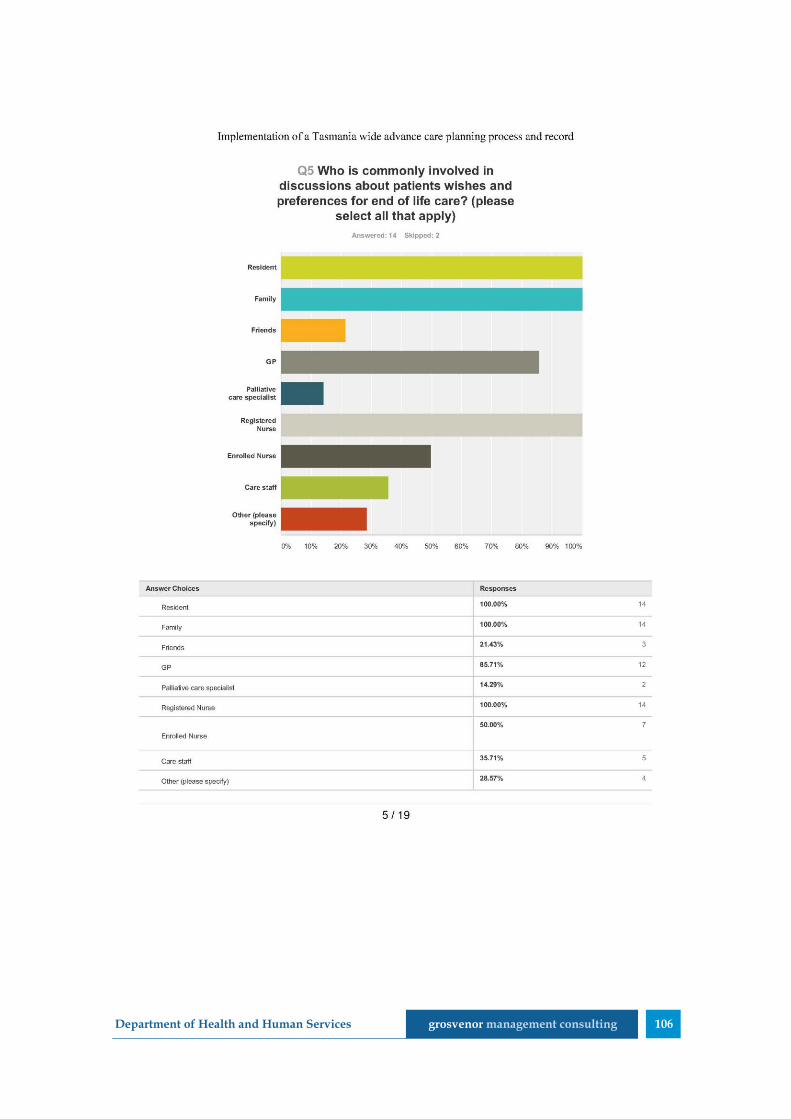
Department of Health and Human Services grosvenor management consulting 106

Department of Health and Human Services grosvenor management consulting 107
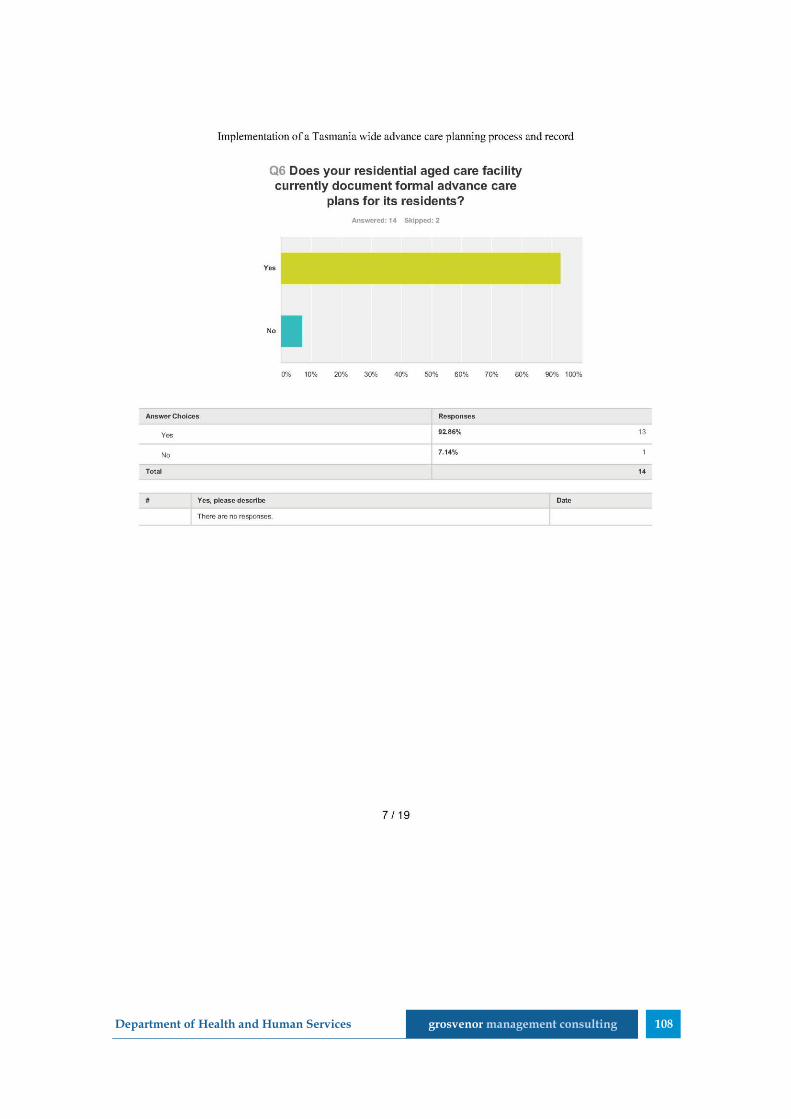
Department of Health and Human Services grosvenor management consulting 108

Department of Health and Human Services grosvenor management consulting 109
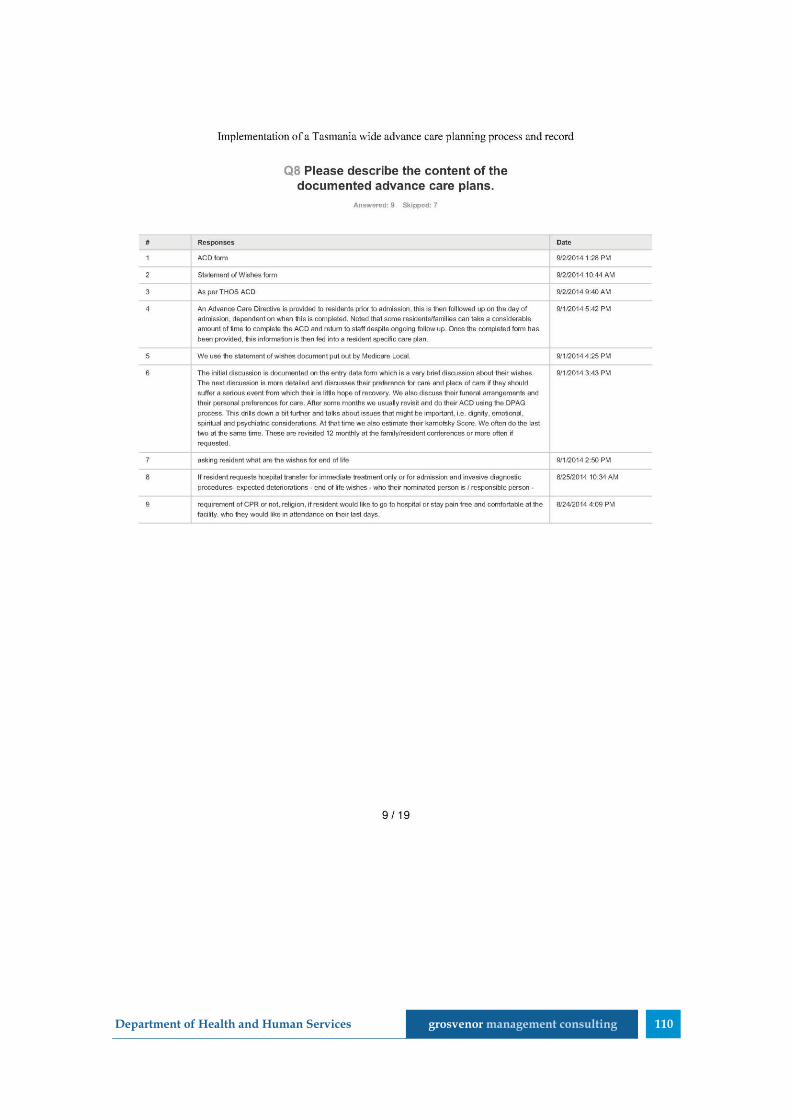
Department of Health and Human Services grosvenor management consulting 110

Department of Health and Human Services grosvenor management consulting 111

Department of Health and Human Services grosvenor management consulting 112

Department of Health and Human Services grosvenor management consulting 113

Department of Health and Human Services grosvenor management consulting 114

Department of Health and Human Services grosvenor management consulting 115
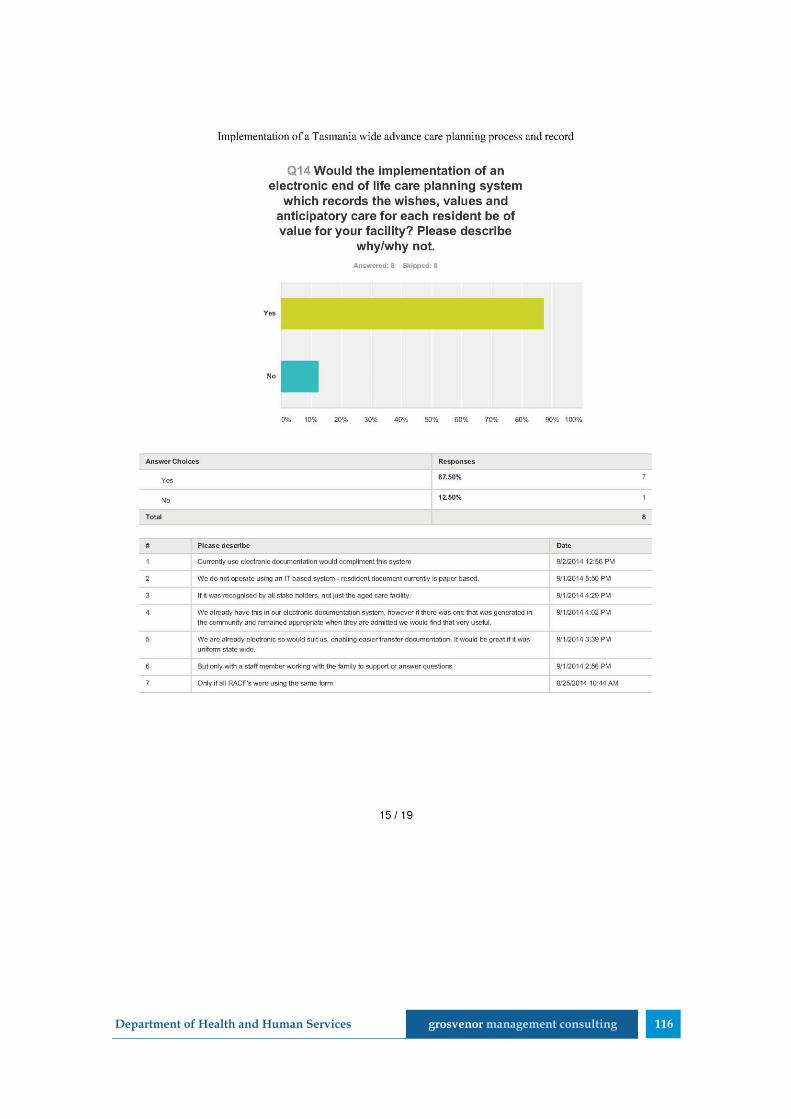
Department of Health and Human Services grosvenor management consulting 116

Department of Health and Human Services grosvenor management consulting 117
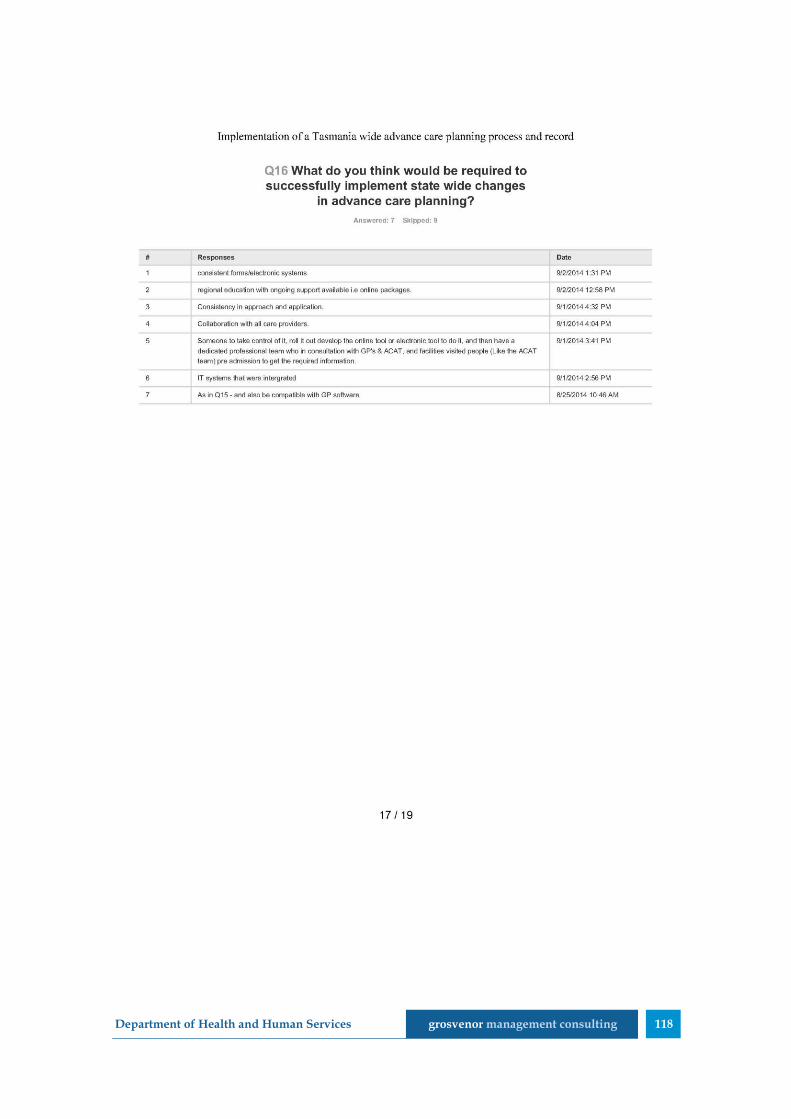
Department of Health and Human Services grosvenor management consulting 118
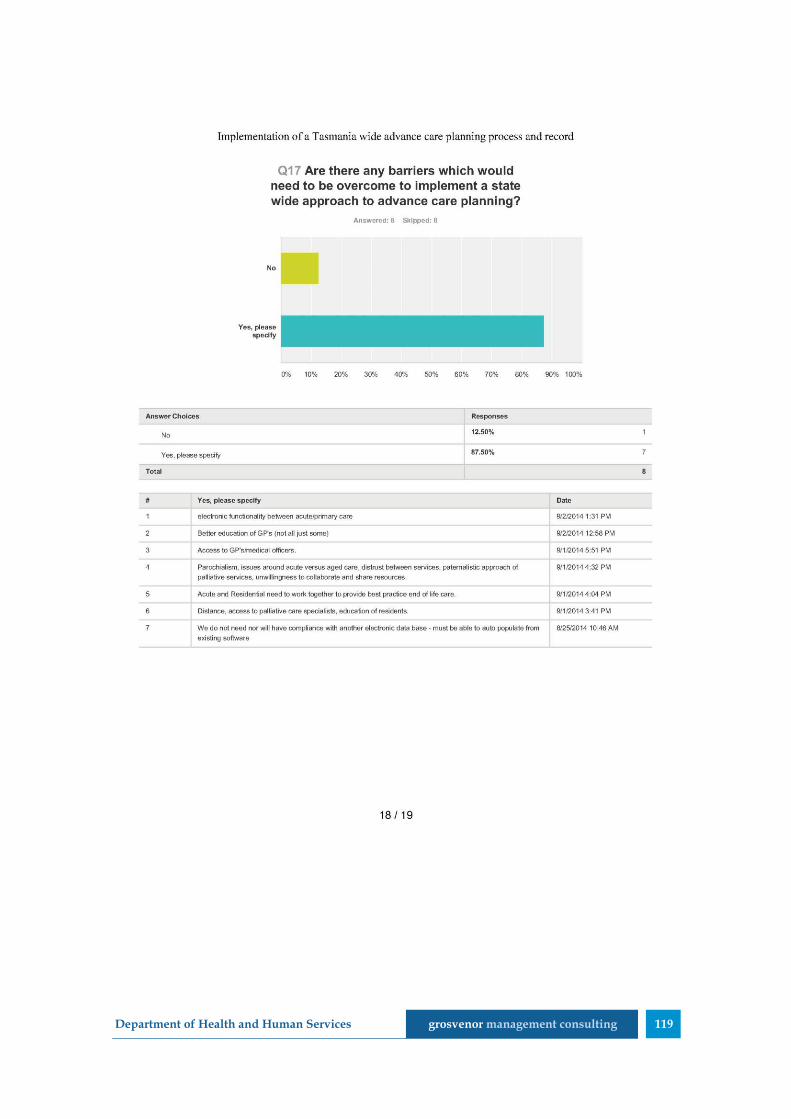
Department of Health and Human Services grosvenor management consulting 119
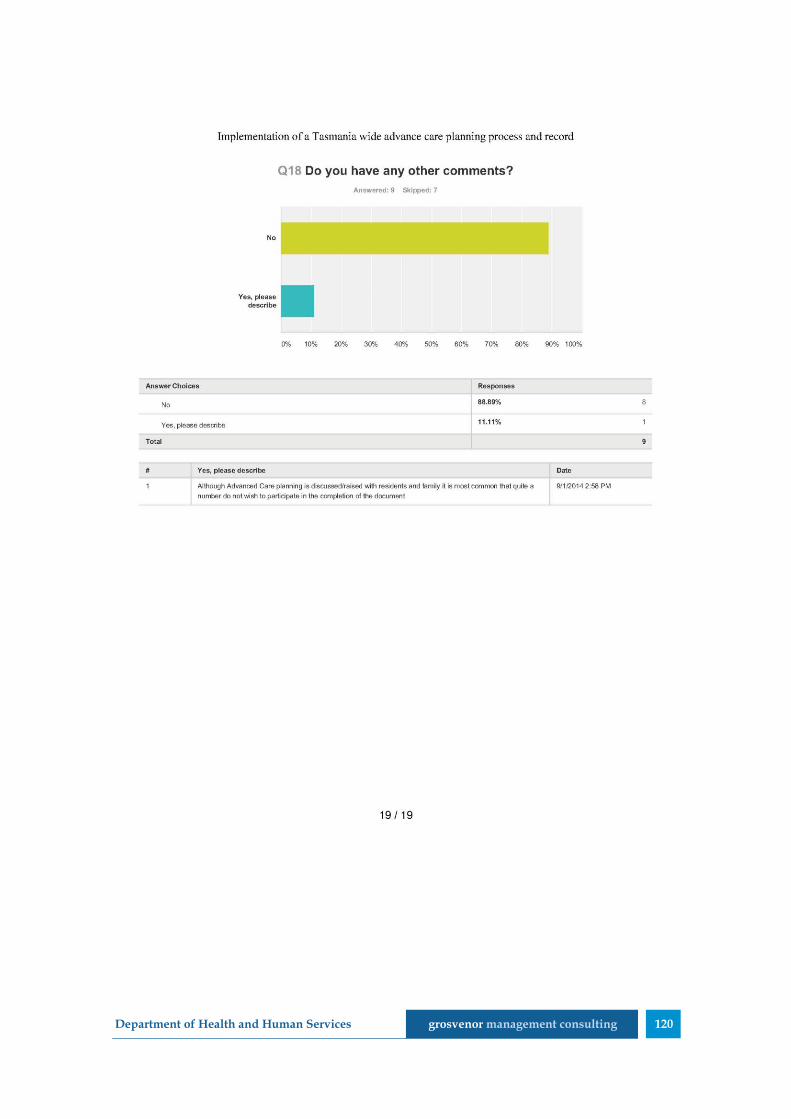
Department of Health and Human Services grosvenor management consulting 120

Department of Health and Human Services grosvenor management consulting 121
12.2 Attachment B – Consultations
A range of consultations were conducted to inform the evaluation of LWDW
and 4CHER.
Consultations
17 consultations were conducted with various stakeholders throughout the
project. An additional two stakeholders were able to provide written input
into the evaluation.
Stakeholders included:
Area Position
THO
Director, eHealth
RACF Project Officer (Nursing)
Palliative Care Medical Officer
GP Liaison Officer
Acting CEO
CO-Director of Nursing
RACFs Director of Care, Emmerton Park
UTAS 4C Project Manager
Research Assistant
TML Director Primary Health Services97
Program Support
Hospitals Staff Specialist, Director of Intensive Care
DHHS
Community Care, Transition (HACC and My Aged
Care)
eCare Strategy and Planning
Department of
Health
Director, Engagement and Education, eHealth
Change and Adoption Branch98
TAHPC BAPC Project Manager
Cradle Coast
Authority Former CEO
Other LWDW Clinical Lead (former)
All stakeholders were asked a range of questions which focused around the
questions below.
1. Your involvement with 4CEHR and LWDW. What were your
perceptions and experiences with 4CEHR and LWDW?
97 Written input was received from this stakeholder 98 Written input was received from this stakeholder

Department of Health and Human Services grosvenor management consulting 122
2. What processes and/or approaches are currently used for advance
care planning?
3. How could the communication of advanced care plans (ACPs) and
advance care directives (ACDs) be improved? What are the key
requirements to ensure adequate communication of ACPs and ACDs
across the health sector?
4. What is required to increase the quality and promote the use of ACPs
by:
health professionals?
individuals?
5. What would be required to achieve state wide implementation of an:
ACP approach or process?
ACP system?
Future stakeholders workshop
A workshop was conducted with individuals identified as being ‘future
stakeholders’ to gain an understanding of the impact any changes to
advanced care planning may have across the state.
Individuals invited to participate in this workshop included:
General Manager, THO North-West
Director of Nursing Health West
Staff Specialist, Emergency Medicine
Co-Director, UTAS Rural Clinical School
Project Manager, Streamlined Care Pathways, TML
Representatives from Community Nursing
Three individuals were available to attend this workshop.
RACF consultations
Consultations were sought with four of the five RACFs that participated in
the pilot program. These consultations were conducted with:
Mt St Vincents, Ulverstone
Emmerton Park, Smithton
Baptcare Karingal, Devonport (via telephone)
Meercroft Care, Devonport
Department of Health and Human Services grosvenor management consulting 123
The RACFs were engaged to participate in three forms of consultation:
focus group with staff involved in the implementation and/or use of
LWDW and 4CEHR
a process review with a key staff member to discuss the processes
used prior to, during and following the pilot program
individual interviews with existing residents and/or family members
of those residents that were involved in the LWDW/4CEHR pilot.
Both the focus group and process review were conducted simultaneously at
the four RACFs.
While all RACFs were asked to identify suitable residents and/or families to
participate in the interview, these interviews were only conducted at one
site. The other RACFs indicated that these consultations would not be
possible as they were no longer in communication with appropriate families,
or existing residents would not have the capacity to participate in an
interview.
A total of three consultations were conducted with family members and two
interviews with current residents. Participants in these interviews were
provided with a plain English overview of the evaluation and asked to sign
consent forms.

Department of Health and Human Services grosvenor management consulting 124
12.3 Attachment C - Example RACF workshop agendas
Example agendas for each of the workshops are provided below. While each
of these agendas was taken from LWDW materials, it is unknown whether
any variation occurred in the final delivery of the workshop.
Table 22 Agenda - LWDW Workshop 2
Indicative
timing Topic
0930 Introduction
0940 Appreciating your contribution
0945 Plan of day and Learning Outcomes
0955 A Good death, A Dignified death
Small groups table discussions
1005
1015
1025
Dignity - participants’ words, small groups
Film
Explore and Debrief
1045 Break
1055
3 trajectories, Q Who Dies, Nursing Homes
Indicators Coding: Approaching Death
Coding and Dying
Who Dies
Table discussion
1135 Standards
Table Discussion
1155 Coding Surprise Question
1230 Lunch
1300 Head Heart Hands
1310 Communication – 3 scenarios
1405
Debrief
How I listen to discover values, dignity
How could you promote dignity in EP
1450
The Advance Care planning process
The DPAG form,
Changing the Goals of care
Clinical Action Plans
What ACP are you using
1525 Your next steps: Starting a register, GSF coding, dignity:
values, and preferences,

Department of Health and Human Services grosvenor management consulting 125
Indicative
timing Topic
Summary of day.
Last questions Wind up
1555-
1600 evaluation and close
Table 23 Agenda - LWDW Workshop 3
Indicative
timing Topic
0900-
Register
Intro
Sharing experiences and progress. Promote Team
0930
GSF Coding. Code everyone
The Register - Supportive +Palliative Approach to care.
ABCD, Colours, mounting
1030- Short break
1040
LDW Project: Person Centred approach to Advance
Care Planning
CASE frail, aged, early dementia, PVD + gangrene, DM,
sepsis (leg and chest), delirium + pain + dsypnoea +
panic +odour
Codes Group develop Matrix of Needs: yellow and
red
Group exercise DPAG process
Communicating and documenting skills.
Using Standards.
Nurses’ and Carers’ roles: The DPAG process
Dignity in Living, Dignity in Dying
1230- 30 min lunch
1300
GSF process for Suffering: Identify+ Assess + Plan +
COMMUNICATE.
Identify common symptoms (yellow, Red) in group
EOL care: Identify +C + Assess + C +
“pepsicola” suffering, pain, delirium, dyspnoea, panic:
TOOLS (CAM, 4 pain tools)
Clinical Action Plans for EOL Clinical Action Plans in
Dying Phase.
1430 15 min break
1445 (identify and assess) + C + Plan + C
Preventing crises: planning ahead for Expected

Department of Health and Human Services grosvenor management consulting 126
Indicative
timing Topic
Deteriorations, and for Dying.
Team work: enabling the GP’s involvement in anticipatory
planning
group Discussions: Preventing avoidable hospital
admissions
1530-
1630
Allow a Natural Death: design it? Policies, forms.
Review of this day’s learning group.
Next Steps. Homework, Delegating, RACF’s needs for
support.
Staff roles: Doing the DPAG’s enables you to do ACP’s
well.
GP training plan.
Evaluation and Close
Table 24 Agenda - LWDW Workshop 4
Indicative
timing Topic
0900-
0930
Intro
Reflective practice:
Sharing experiences across sites: Advanced Care
Planning, Symptom control. Learning from each others’
progress.
Sharing experiences: Register, Coding, Coordinators,
Getting all staff engaged, management support, organising
GP meetings?
1020 Teamwork at your RACF: Sharing, notes
Lets have an open discussion: Q’s Reflective practice
1115
Recognising C’s and D’s: approaching death, then
dying
20 their experience – what are the challenges, SEA
1205
Prevention of crises by planning ahead – for Terminal
phase, LCP adaptations – GSF modified integrated care
pathway
Any Crises? SEA? Preventing avoidable hospital
admissions? SEA
Project Guideline: anticipatory planning and prescribing
1245- Break
1330
Preparing everyone
Staff – everyone
Primary health team
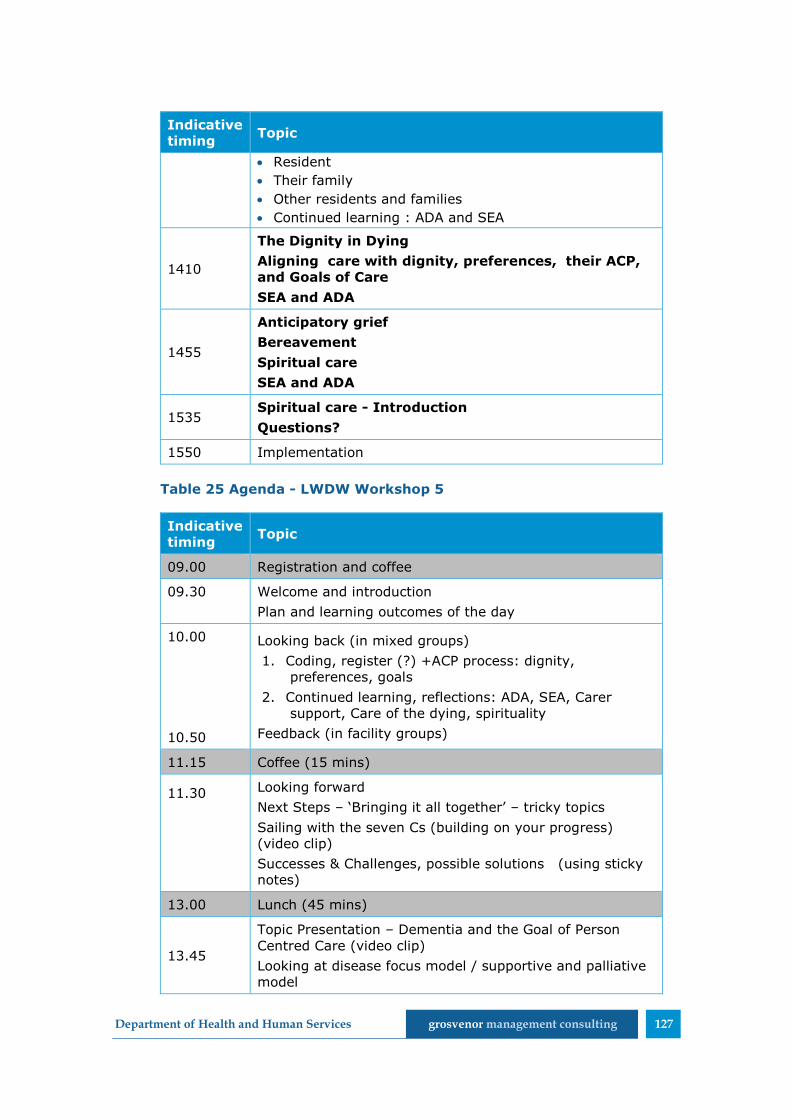
Department of Health and Human Services grosvenor management consulting 127
Indicative
timing Topic
Resident
Their family
Other residents and families
Continued learning : ADA and SEA
1410
The Dignity in Dying
Aligning care with dignity, preferences, their ACP,
and Goals of Care
SEA and ADA
1455
Anticipatory grief
Bereavement
Spiritual care
SEA and ADA
1535 Spiritual care - Introduction
Questions?
1550 Implementation
Table 25 Agenda - LWDW Workshop 5
Indicative
timing Topic
09.00 Registration and coffee
09.30
Welcome and introduction
Plan and learning outcomes of the day
10.00
10.50
Looking back (in mixed groups)
1. Coding, register (?) +ACP process: dignity,
preferences, goals
2. Continued learning, reflections: ADA, SEA, Carer
support, Care of the dying, spirituality
Feedback (in facility groups)
11.15 Coffee (15 mins)
11.30
Looking forward
Next Steps – ‘Bringing it all together’ – tricky topics
Sailing with the seven Cs (building on your progress)
(video clip)
Successes & Challenges, possible solutions (using sticky
notes)
13.00 Lunch (45 mins)
13.45
Topic Presentation – Dementia and the Goal of Person
Centred Care (video clip)
Looking at disease focus model / supportive and palliative
model

Department of Health and Human Services grosvenor management consulting 128
Indicative
timing Topic
Topic – ‘Living Well’ with Dementia – making the most of
life – How do we look after our residents with dementia?
14.45 Tea and coffee
15.10 Key tasks – Portfolios
- Next steps
15.35 Any Questions?
15.50 Reflection and – video clip – ‘Live like you are dying’
16.00 Close & Evaluations

Department of Health and Human Services grosvenor management consulting 129
12.4 Attachment D - RACF Training Schedule
The RACF training schedule was designed to allow an implementation period
of three months between each workshop.
The following table provides an overview of the originally scheduled/intended
dates for the implementation of LWDW99.
Table 26 Original RACF training schedule
LWDW
Workshop 1
LWDW
Workshop 2
LWDW
Workshop 3
LWDW
Workshop 4
LWDW
Workshop 5
Round 1 Sep-Nov 2010
December 2010
March 2011 June 2011 September 2011
Round 2 March – May 2011
June 2011 Sept 2011 Dec 2011 March 2012
Round 3 Sep-Nov 2011
December 2011
March 2012 June 2012 September 2012
Round 4 March –
May 2012 June 2012 Sept 2012 Dec 2012 March 2013
99 Note: It was intended that the pilot RACFs would participate in round 1 of the training.
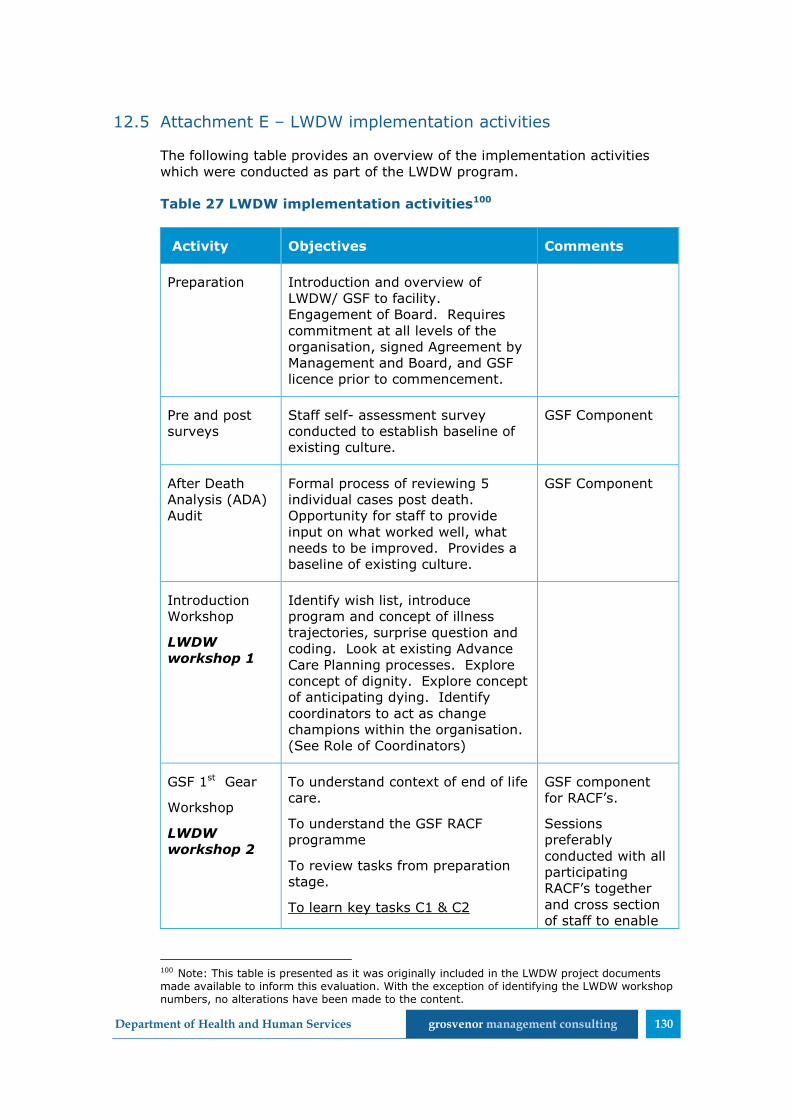
Department of Health and Human Services grosvenor management consulting 130
12.5 Attachment E – LWDW implementation activities
The following table provides an overview of the implementation activities
which were conducted as part of the LWDW program.
Table 27 LWDW implementation activities100
Activity Objectives Comments
Preparation Introduction and overview of
LWDW/ GSF to facility.
Engagement of Board. Requires
commitment at all levels of the
organisation, signed Agreement by
Management and Board, and GSF
licence prior to commencement.
Pre and post
surveys
Staff self- assessment survey
conducted to establish baseline of
existing culture.
GSF Component
After Death
Analysis (ADA)
Audit
Formal process of reviewing 5
individual cases post death.
Opportunity for staff to provide
input on what worked well, what
needs to be improved. Provides a
baseline of existing culture.
GSF Component
Introduction
Workshop
LWDW
workshop 1
Identify wish list, introduce
program and concept of illness
trajectories, surprise question and
coding. Look at existing Advance
Care Planning processes. Explore
concept of dignity. Explore concept
of anticipating dying. Identify
coordinators to act as change
champions within the organisation.
(See Role of Coordinators)
GSF 1st Gear
Workshop
LWDW
workshop 2
To understand context of end of life
care.
To understand the GSF RACF
programme
To review tasks from preparation
stage.
To learn key tasks C1 & C2
GSF component
for RACF’s.
Sessions
preferably
conducted with all
participating
RACF’s together
and cross section
of staff to enable
100 Note: This table is presented as it was originally included in the LWDW project documents made available to inform this evaluation. With the exception of identifying the LWDW workshop numbers, no alterations have been made to the content.

Department of Health and Human Services grosvenor management consulting 131
Activity Objectives Comments
Set up register and code residents
Needs support matrices, planning
meetings
Collaboration /involvement of GPs,
PCT
Role of Coordinator(s)
Involvement of other staff
To understand Dignity at end if Life
care
To understand Advanced Care
planning
shared
contribution to
learning.
Multiple
workshops may be
required to ensure
access to as many
staff as possible.
Potential for Train
the Trainer so that
information is
disseminated to all
staff in each
facility.
DPAG
Processes
Provide formal and informal
training in using the principles of
the DPAG for Advance Care
Planning, defining Goals of Care
and developing anticipatory care
plans in collaboration with GP.
Training encompasses how to have
difficult discussions and allowing a
natural death. Apply DPAG to
individual residents with facility
staff.
DPAG = LWDW
Tool to prompt
and capture
discussions with
residents and
significant others
about Dignity,
Preferences,
Advance Care Plan
and Goals of Care.
Implementation
activities in
facilities.
Facilities are expected to
commence coding of residents,
Coding is to be displayed in an area
that can be viewed by all relevant
staff but not residents/ families and
to be reviewed/ updated weekly by
the care team. Implementation of
the Summary of Care Register.
(See attached)
Facilities are expected to ensure
that Advance Care Planning occurs
for all residents (as close as
possible to admission for new
residents and especially if there is a
status change for existing
residents, plus all residents likely to
be in last days/ weeks/ months of
life. Initiate weekly Toolbox
Meetings with teams in each
facility.
Toolbox meetings provide
opportunity to raise questions,
explore issues, reflect on practice,
Coding involves
asking the
question “Would
you be surprised if
this resident died
in the next Days
(red)? Weeks
(yellow)? Months
(green)? Years
(blue)? Coloured
dots are used to
identify current
status.
Using the DPAG
process for
advance care
planning is
encouraged and
supported.

Department of Health and Human Services grosvenor management consulting 132
Activity Objectives Comments
learn specific skills and implement
Significant Event Analysis (SEA)
and ADA’s.
GP
Engagement
Preliminary engagement of GP’s
and preparation for training.
Includes overview of processes
occurring in facilities and
development of agreed training
schedule.
Engagement of pharmacists in this
process is also beneficial.
Where possible GP
training is
conducted at the
facility and
involving facility
staff (change
champions).
GSF 2nd Gear
Workshop
LWDW
workshop 3
To share and learn from others C1
C2
To understand the next stage and
learn key tasks C3, C4:
Control of symptoms – assessment
tools
Continuity- use OOH handover
forms
To understand avoidance of
admission issues.
To learn more about Advance Care
Planning, Not for CPR, and related
EOLC issues
Second Gear:
Symptom control and
Assessment C3
Advance care Planning C1
Out of hours continuity C4
Key topics:
1. Advanced Care Planning-
communication skills
2. Decreasing Hospitalisation,
DNAR (NFR)
To share learn from others
experiences of implementing C
5,6,7
To understand the importance of
embedding and sustain of GSF.
To learn the process of the next
stage – consolidation and
GSF Component
as above

Department of Health and Human Services grosvenor management consulting 133
Activity Objectives Comments
accreditation.
To understand Quality of life
issues- “living well until you die”,
To understand the detection and
management of the 4 D’s:
depression, delirium,
demoralisation and dementia.
To understand the specific issues
/challenges around EoLC for people
with Dementia.
GP Training Encompasses concepts covered in
1st and 2nd Gear workshops with
facility staff.
Includes culture
change, ADA’s and
the DPAG process.
GSF 3rd Gear
Workshop
LWDW
Workshop 4
To share and learn from others
implementation of C3&4.
To understand the next stage and
learn the key tasks C5,6,7
Continued learning
Carer support
Care of the dying
Includes staff support
To learn communication skills and
discussing dying.
To discuss aspects of spiritual care.
Third Gear
Reflective practice and
education C5
Relatives support and
bereavement C6
Care in the final days C7
Key topics
1. Discussing dying
2. Spirituality
GSF Component
as above
Consolidation Staff should be gaining confidence
in coding, identifying illness
trajectories, using DPAG process,
developing clinical action plans,
preventing unnecessary suffering
and preventing avoidable hospital

Department of Health and Human Services grosvenor management consulting 134
Activity Objectives Comments
admissions.
GP Training Using DPAG to develop clinical
action plans and anticipatory
prescribing. Look at care plans for
common symptoms.
GSF 4th Gear
Workshop
LWDW
workshop 5
To share learn from others
experiences of implementing C
5,6,7
To understand the importance of
embedding and sustain of GSF.
To learn the process of the next
stage – consolidation and
accreditation.
To understand Quality of life
issues- “living well until you die”,
To understand the detection and
management of the 4 D’s:
depression, delirium,
demoralisation and dementia.
To understand the specific issues
/challenges around EoLC for people
with Dementia.
Fourth Gear
Sustain, embed, extend
Consolidation
Introduction to the accreditation
process “going for Gold’
Key topics:
1. Quality of life/ living well/
depression/ demoralisation
/delirium
2. Dementia
GSF Component
as above
Coordinators
Action Learning
Groups
4-6 weekly workshops for
coordinators provide professional
support to ensure competence with
the DPAG and other processes and
to ensure momentum with culture
change is sustained.
Consumer and
Community
Consumers are provided
information at point of care
concerning involvement in and
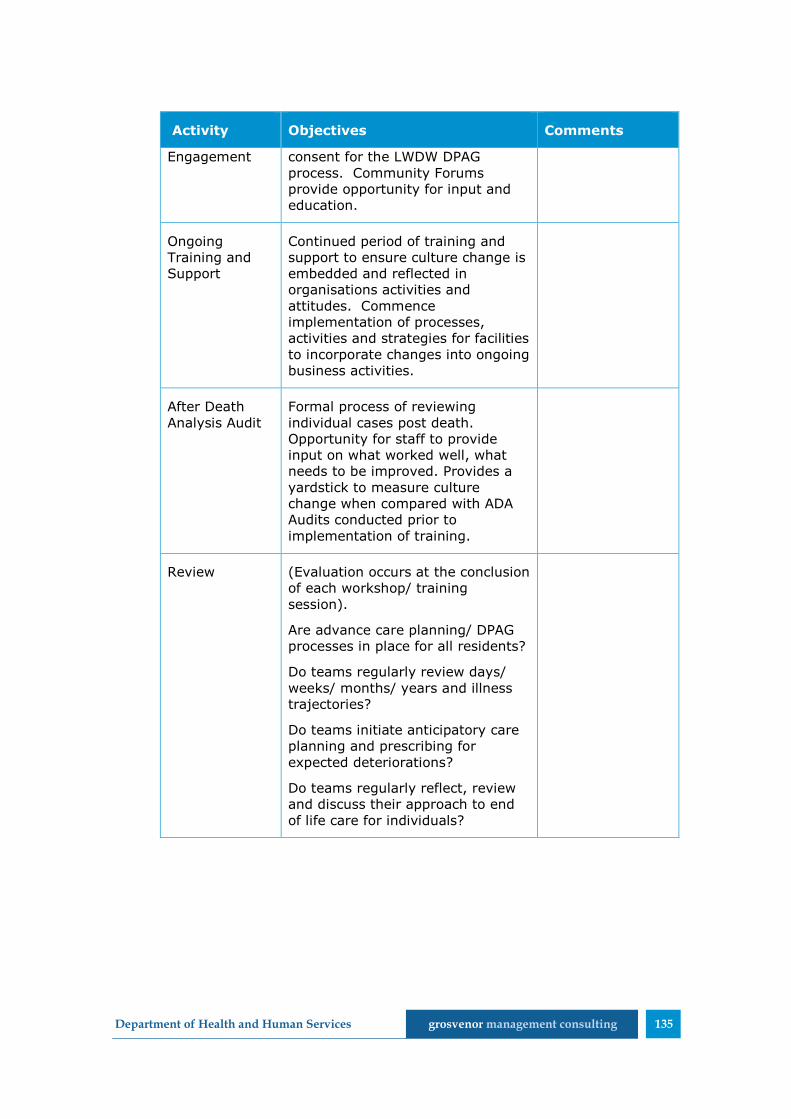
Department of Health and Human Services grosvenor management consulting 135
Activity Objectives Comments
Engagement consent for the LWDW DPAG
process. Community Forums
provide opportunity for input and
education.
Ongoing
Training and
Support
Continued period of training and
support to ensure culture change is
embedded and reflected in
organisations activities and
attitudes. Commence
implementation of processes,
activities and strategies for facilities
to incorporate changes into ongoing
business activities.
After Death
Analysis Audit
Formal process of reviewing
individual cases post death.
Opportunity for staff to provide
input on what worked well, what
needs to be improved. Provides a
yardstick to measure culture
change when compared with ADA
Audits conducted prior to
implementation of training.
Review (Evaluation occurs at the conclusion
of each workshop/ training
session).
Are advance care planning/ DPAG
processes in place for all residents?
Do teams regularly review days/
weeks/ months/ years and illness
trajectories?
Do teams initiate anticipatory care
planning and prescribing for
expected deteriorations?
Do teams regularly reflect, review
and discuss their approach to end
of life care for individuals?

Department of Health and Human Services grosvenor management consulting 136
12.6 Attachment F – Living Well Dying Well Content and Materials
12.6.1 Illness trajectories
Three distinct illness trajectories are presented as part of the LWDW
approach. These trajectories have been described by a range of health
professionals for people with progressive chronic illness101.
The three illness trajectories provide RACF staff with an indication of the
expected deterioration for residents with particular conditions overtime.
They may also be used to assist in determining the likely prognosis for a
resident.
1) Short period of evident decline (typically cancer)
2) Long term limitations with intermittent acute, serious episodes
(typically organ failure)
3) Prolonged dwindling (typically frail and aged with multiple
comorbidities)
Gaining an understanding of the expected illness trajectory of a resident
allows the RACF staff to plan ahead and work to prevent crises. As it
provides them with an indication of what may be expected in the future they
can be prepared to provide appropriate care. For example, if a resident is on
trajectory two, they are likely to experience frequent serious episodes.
101 Note: The three illness trajectories are described in detail in the article ‘Illness trajectories and palliative care’. This article is available at: http://www.cphs.mvm.ed.ac.uk/groups/ppcrg/images/pdf/Murray%20SA%202007%20Scot%20Prim%20Care%2066%2017-19.pdf

Department of Health and Human Services grosvenor management consulting 137
12.6.2 Prognostic indicators
LWDW teaches a range of prognostic and general indicators to assist RACF
staff and other health professionals in identifying residents in the last year of
life. A range of general and specific indicators may be taken into account, for
example:
level of activity
co-morbidity
physical decline
need for support
response to treatments
choices regarding treatment
weight loss
Sentinel events such as a serious fall or bereavement.
Specific Prognostic Indicator Guidance is available on the GSF website102.
Along with the Prognostic Indicators, this document also provides guidance
about other tools used as part of both GSF and LWDW which are used to
identify and assess residents in their last year of life.
12.6.3 Coding and the ‘surprise question’
LWDW seeks to enable participants to code residents based on their likely
prognosis. In order to identify residents in their final year of life, participants
are taught to ask the ‘surprise’ question. This question asks:
Would you be surprised if the resident died in days/hours, weeks,
months or years?
It is expected that experienced health professionals will be able to
instinctively respond to this question based on their knowledge of illness
trajectories and the resident. Considerations from the application of the
illness trajectories and prognostic indicators are also applied.
The implementation of coding activities is used to prepare everyone involved
in the residents care for periods of decline and ultimately death, including
doctors, staff, carers and the family. It provides a sense of how long the
resident can reasonably be expected to live, and allows plans to be made
accordingly for their care.
102 The GSF Prognostic Indicator Guidance is available at: http://www.goldstandardsframework.org.uk/cd-content/uploads/files/General%20Files/Prognostic%20Indicator%20Guidance%20October%202011.pdf

Department of Health and Human Services grosvenor management consulting 138
Figure 11 Needs based coding
Code Description
A - Years
Team would be surprised if the resident died within
the next six to 12 months.
Adjusting to Living Well in a new environment
Regular review of care
B - Months Team would not be surprised if the resident died
within the next six to 12 months.
Regular proactive review of patient needs and care.
Would be advisable to consider a Supportive and
Palliative pathway now- if not on it already
C - Weeks Team would not be surprised if the resident only had
weeks of life left. Reasonably expect death within six
weeks.
Prepare for final stage.
D - Days
Reasonably expect death within hours or a few days.
Preparation for death in preferred place – resist
transfers at this time
Only a palliative pathway
Residents who are considered to have weeks remaining (yellow) are
considered to be ‘Approaching the Dying Phase’ while those with days/hours
remaining (red) are in the ‘Dying Phase’. No specific terminology was
identified to describe the phase of residents with years (blue) or months
(green) remaining.
12.6.4 DPAG tool
The DPAG tool was designed to assist in conducting advance care planning
and is used to prompt and record discussions with residents about their
care. This allows RACF staff to ensure that care is appropriately tailored to
the condition, needs and wishes of each individual resident.
LWDW encourages RACFs to conduct DPAG discussions with all residents.
There is also a particular emphasis on conducting and revisiting these
discussions with residents who are expected to only have weeks or
days/hours of life remaining. This was particularly evident in the GSF
materials.
The four elements/aspects of the DPAG are detailed in the table below.
Table 28 DPAG
DPAG
Element Description/purpose
Dignity
Understanding the resident’s views on dignity, including
what dignity means to them and how this can be achieved
and maintained.

Department of Health and Human Services grosvenor management consulting 139
DPAG
Element Description/purpose
This may include the identification of actions which can be
undertaken to ensure that the resident maintains a sense
of dignity throughout their care, and that the resident’s
values are respected.
Assessing dignity will involve taking into account and
having respect for the resident’s values. A range of values
should be considered such as:
Freedom, autonomy, independence, choice
Comfort, pleasure, enjoyment
Safety, certainty, security
Preferences
Identification of the residents preferences for care, such
as:
Receiving information about their condition and
prognosis
Being involved in decisions and discussions about their
care
Particular requirements for their care, including where
they would prefer to receive treatment and the extent
of medical interventions they would like to occur
Information collected about the preferences of a resident
can be used to directly inform their advance care plan.
Advance Care
Directives
Identify and clarify the meaning of any existing ACDs. This
should explore:
Enduring Guardian/Person Responsible,
Extent and type of medical treatment wanted and/or
not wanted
Specific personal requests
Clinical Goals
of Care
Identify realistic and achievable outcomes for the four
main clinical goals:
1) Length of life (may range from prolonging life at all
costs to allowing a natural death)
2) Function (whether failing function will be
treated/restored or accepted)
3) Comfort (to what extent symptoms will be treated
and/or relieved)
4) Prevention of avoidable crises (the degree to which
any complications will be treated)
LWDW encourages the use of a variety of tools to develop
an understanding of what would goals of care would be
realistic for each resident. The following tools are taught
as part of LWDW to support decisions about the Clinical
Goals of Care:
Karnofsky Performance Scale - used to measure a
residents day to day level of function on a scale from 0

Department of Health and Human Services grosvenor management consulting 140
DPAG
Element Description/purpose
(“Comatose or barely rousable”) to 100 (“Normal, no
complaints, no evidence of disease”)103,104. The score
can also be used to assist in validating a resident’s
likely prognostic code or category (see ‘Coding and the
‘surprise’ question’ below).
Confusion Assessment Method (CAM) - a bedside
tool used by carers to assess delirium. The CAM
provides a structured format to identify the key
features of delirium (fluctuating symptoms, an acute
onset and a change in cognition)105. The CAM tool
recognises that the presence of delirium within a
resident may change overtime106.
LWDW teaches RACF staff to undertake a baseline
Karnofsky and CAMs assessment for each resident. By
comparing the results of further assessments to the
baseline, the RACF staff are able to monitor and track
deteriorations and adjust care.
12.6.5 Clinical Pathways
LWDW utilises three categories of Clinical Pathways:
aggressive diseased focused pathways
less aggressive disease focused emphasising supporting care pathways
supportive and palliative pathways.
The goals of care identified as part of the DPAG process are used to inform
the selection of the most appropriate clinical pathway for the resident. The
clinical pathway is then used to assist in the planning for an individual’s end
of life care. Each pathway is described in the Table 29.
103 Department of Health and Human Services, Clinical Assessment Scales, http://www.dhhs.tas.gov.au/__data/assets/pdf_file/0008/37538/PCS20Protocol203.1.520Comprehensive20Assessment20Appendix2071.pdf 104 University of Wollongong, The Australia-modified Karnofsky Performance Scale (AKPS), http://ahsri.uow.edu.au/content/groups/public/@web/@chsd/@pcoc/documents/doc/uow129188.pdf 105 Department of Health, Delirium in older people, http://www.health.gov.au/internet/main/publishing.nsf/Content/ageing-publicat-dementia-delirium.htm 106 Note: More detailed information about the CAMs, including an example assessment tool is available at: http://www.dementia-assessment.com.au/delirium/The_Confusion_Assessment_Method.pdf, page 25
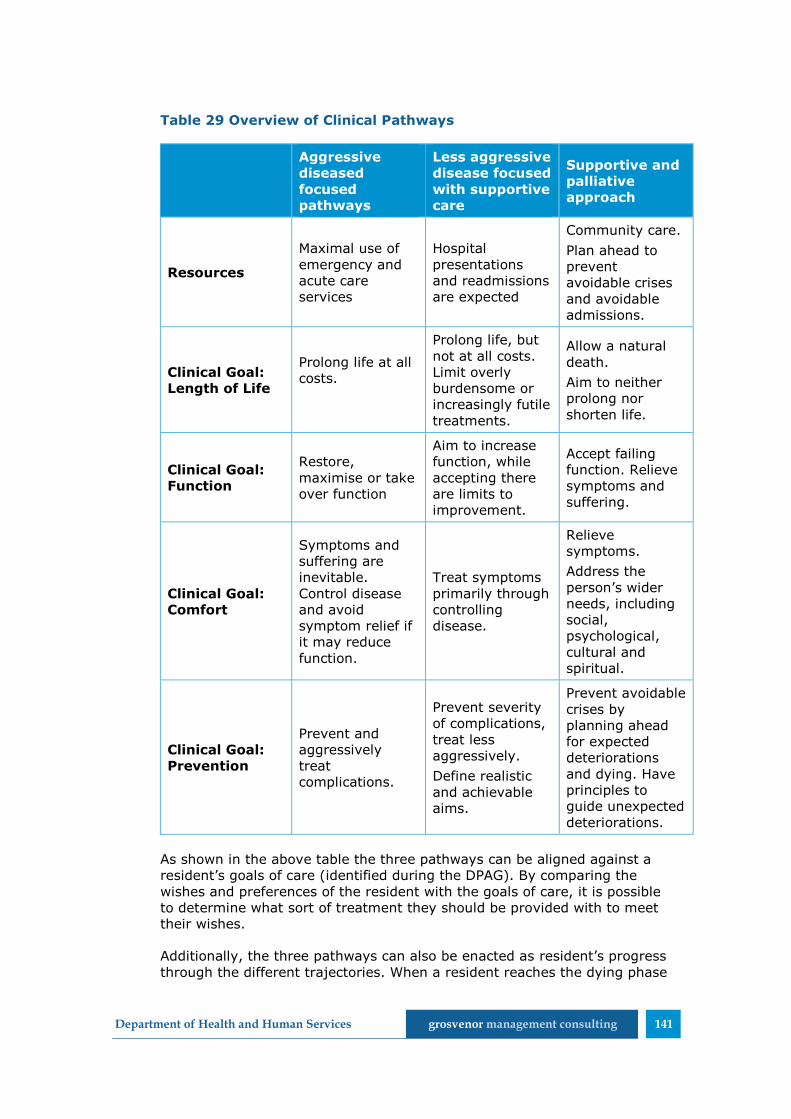
Department of Health and Human Services grosvenor management consulting 141
Table 29 Overview of Clinical Pathways
Aggressive
diseased
focused
pathways
Less aggressive
disease focused
with supportive
care
Supportive and
palliative
approach
Resources
Maximal use of
emergency and
acute care
services
Hospital
presentations
and readmissions
are expected
Community care.
Plan ahead to
prevent
avoidable crises
and avoidable
admissions.
Clinical Goal:
Length of Life
Prolong life at all
costs.
Prolong life, but
not at all costs.
Limit overly
burdensome or
increasingly futile
treatments.
Allow a natural
death.
Aim to neither
prolong nor
shorten life.
Clinical Goal:
Function
Restore,
maximise or take
over function
Aim to increase
function, while
accepting there
are limits to
improvement.
Accept failing
function. Relieve
symptoms and
suffering.
Clinical Goal:
Comfort
Symptoms and
suffering are
inevitable.
Control disease
and avoid
symptom relief if
it may reduce
function.
Treat symptoms
primarily through
controlling
disease.
Relieve
symptoms.
Address the
person’s wider
needs, including
social,
psychological,
cultural and
spiritual.
Clinical Goal:
Prevention
Prevent and
aggressively
treat
complications.
Prevent severity
of complications,
treat less
aggressively.
Define realistic
and achievable
aims.
Prevent avoidable
crises by
planning ahead
for expected
deteriorations
and dying. Have
principles to
guide unexpected
deteriorations.
As shown in the above table the three pathways can be aligned against a
resident’s goals of care (identified during the DPAG). By comparing the
wishes and preferences of the resident with the goals of care, it is possible
to determine what sort of treatment they should be provided with to meet
their wishes.
Additionally, the three pathways can also be enacted as resident’s progress
through the different trajectories. When a resident reaches the dying phase
Department of Health and Human Services grosvenor management consulting 142
it would be appropriate for them to be moved on to the supportive and
palliative approach.
12.6.6 Clinical Action Plans
An example Clinical Action Plan (CAP) is provided overleaf.

Department of Health and Human Services grosvenor management consulting 143

Department of Health and Human Services grosvenor management consulting 144
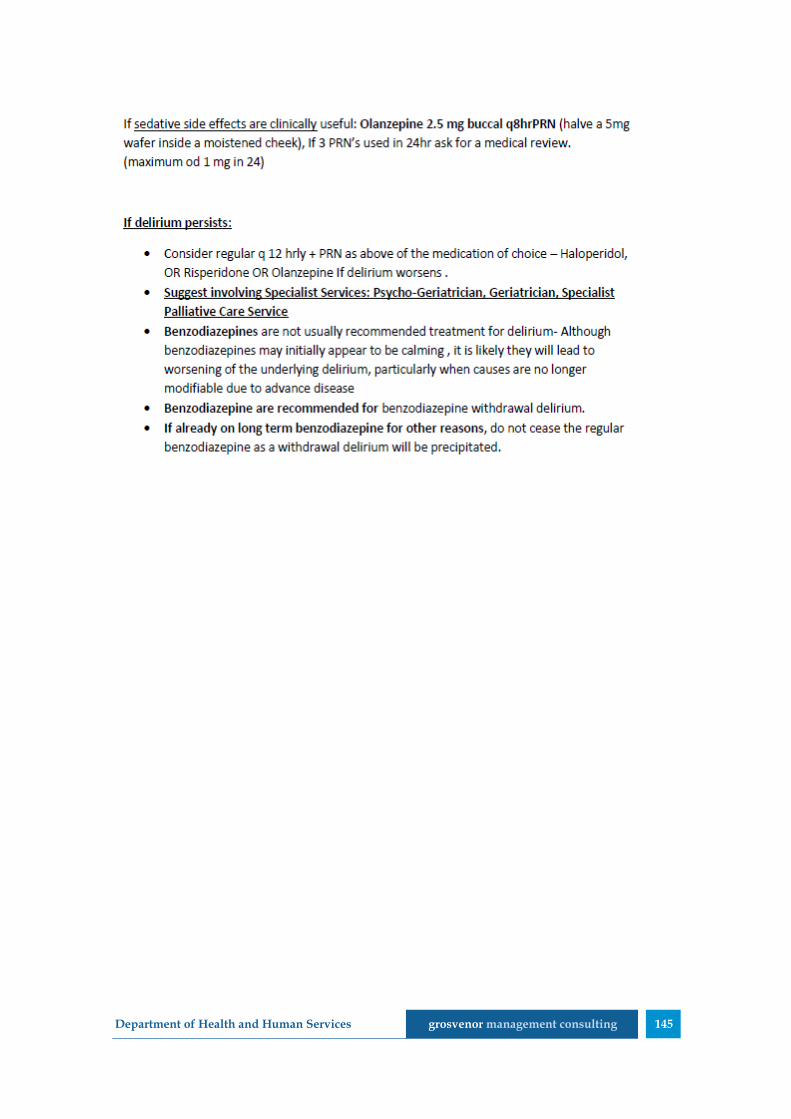
Department of Health and Human Services grosvenor management consulting 145

Department of Health and Human Services grosvenor management consulting 146
12.7 Attachment G – Evaluation activities
12.7.1 Before and after staff confidence assessment surveys
As part of the LWDW training program, all RACFs were expected to complete
before and after staff confidence assessment surveys. This survey is
designed to self-assess the competence and confidence level of staff in
completing tasks associated with each of the seven C’s.
An example survey tool is included overleaf.

Department of Health and Human Services grosvenor management consulting 147

Department of Health and Human Services grosvenor management consulting 148
12.7.2 After death Audits
LWDW encourages after death audits within each of the RACFs. These are
used to review recent deaths and are a tool for continued learning.
The after death audit process provides staff with the opportunity to consider
and discuss the death, including whether the care that was provided aligned
with the wishes and needs of the resident.
During after death audits, the RACF staff will review the death to identify:
what went well?
what didn’t go so well?
what could have done better?
how can we do better?
In considering ‘how can we do better?’ the staff identify specific
improvement opportunities for each of the 7C’s. This is then used to develop
an action plan for future improvements within the RACF.
As part of the LWDW program, each of the participating RACFs were
expected to conduct five baseline after death audits prior to the training and
an additional five following the completion of the pilot program.
The completion of these pre- and post-training audits was intended to assist
the participating RACFs in measuring the extent to which cultural and
practice change had been achieved.
An example after death audit tool is provided overleaf107.
107 Note: The example after death audit form has not been formatted. It is presented as it
appears in the LWDW project documentation which was reviewed to inform this evaluation.
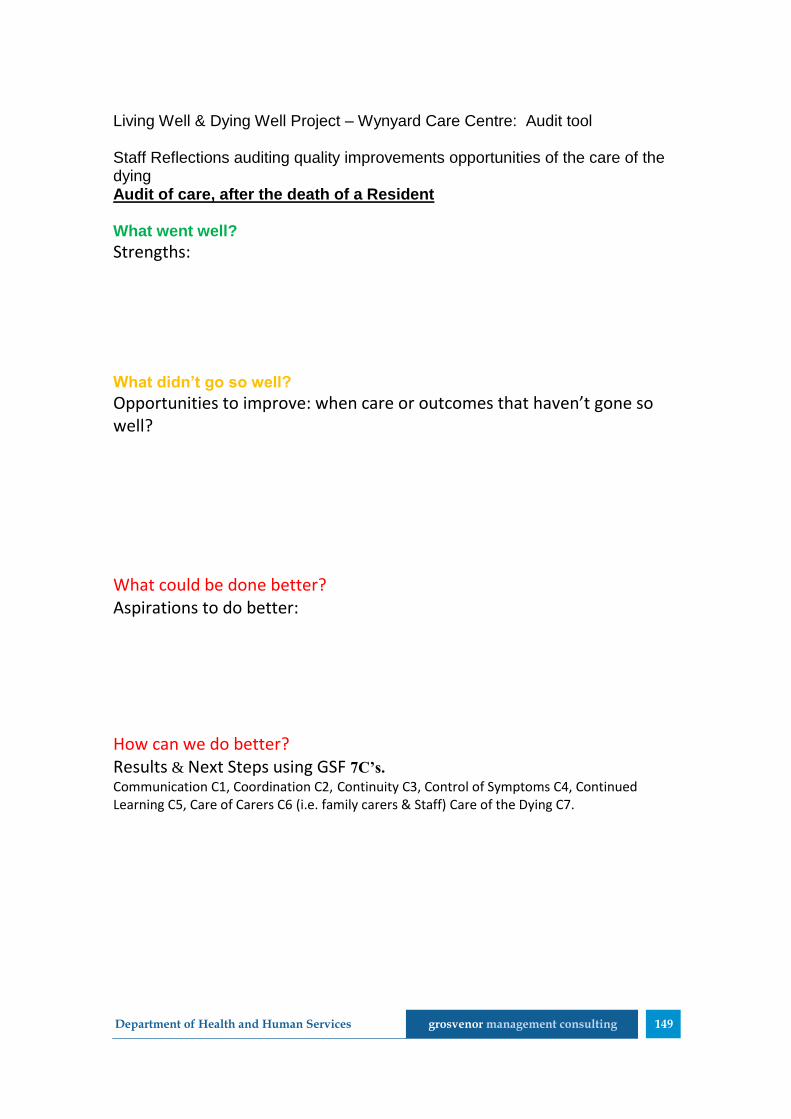
Department of Health and Human Services grosvenor management consulting 149
Living Well & Dying Well Project – Wynyard Care Centre: Audit tool Staff Reflections auditing quality improvements opportunities of the care of the dying Audit of care, after the death of a Resident What went well?
Strengths: What didn’t go so well?
Opportunities to improve: when care or outcomes that haven’t gone so well? What could be done better? Aspirations to do better: How can we do better? Results & Next Steps using GSF 7C’s. Communication C1, Coordination C2, Continuity C3, Control of Symptoms C4, Continued Learning C5, Care of Carers C6 (i.e. family carers & Staff) Care of the Dying C7.
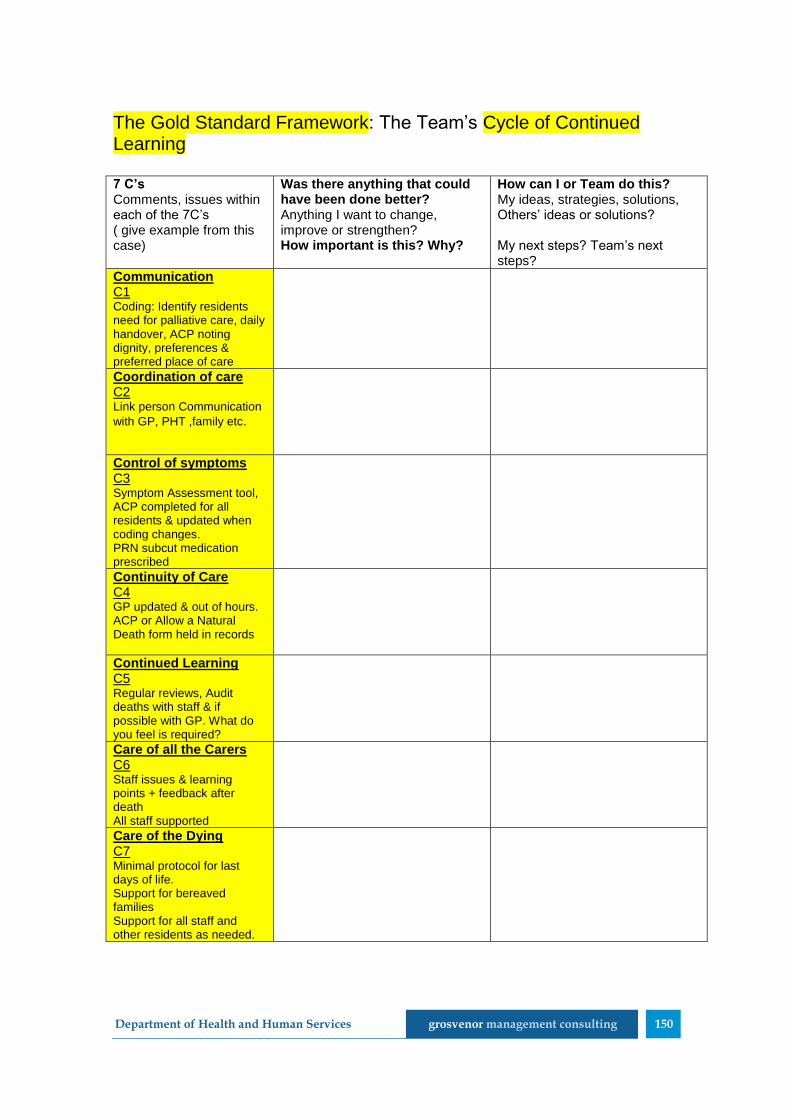
Department of Health and Human Services grosvenor management consulting 150
The Gold Standard Framework: The Team’s Cycle of Continued Learning 7 C’s Comments, issues within each of the 7C’s ( give example from this case)
Was there anything that could have been done better? Anything I want to change, improve or strengthen? How important is this? Why?
How can I or Team do this? My ideas, strategies, solutions, Others’ ideas or solutions? My next steps? Team’s next steps?
Communication C1 Coding: Identify residents need for palliative care, daily handover, ACP noting dignity, preferences & preferred place of care
Coordination of care C2 Link person Communication
with GP, PHT ,family etc.
Control of symptoms C3 Symptom Assessment tool, ACP completed for all residents & updated when coding changes. PRN subcut medication prescribed
Continuity of Care C4 GP updated & out of hours. ACP or Allow a Natural Death form held in records
Continued Learning C5 Regular reviews, Audit deaths with staff & if possible with GP. What do you feel is required?
Care of all the Carers C6 Staff issues & learning points + feedback after death All staff supported
Care of the Dying C7 Minimal protocol for last days of life. Support for bereaved families Support for all staff and other residents as needed.
Department of Health and Human Services grosvenor management consulting 151
Reflections and comments
Action Plan Actions Who is
responsible
Date due Date
reviewed
Date
Completed
1
2
3
Department of Health and Human Services grosvenor management consulting 152
12.8 Attachment H – GP Training
Small Group Learning Sessions were conducted to educate GPs about the
LWDW program and key concepts. The training consisted of four, two hour
sessions (total of eight hours training) conducted after business hours to
accommodate GPs working hours.
Attendance at all four sessions entitled the GP to 40 continuing professional
development (CPD) points.
GP training sessions were scheduled to occur in locations near participating
RACFs to target appropriate GPs who are providing care to residents. This
training was not delivered concurrently to the RACF training.
As detailed in the original training application to the Royal Australian College
of General Practitioners (RACGP), the GP training sessions sought to:
“examine illness trajectories for RACF residents, assist in constructing
individual clinical care plans for a number of patients in a
multidisciplinary environment and provide the GP with the tools to
audit the care of patients after their death”.
The following five learning objectives were identified for this training:
1. To understand the three main trajectories of life limiting advanced
chronic illness
2. Demonstrate competency in using prognostic indicator guidelines,
identify residents likely prognosis (years, months, weeks, days,
hours)
3. To strengthen GPs capacity within Primary Health Teams, working
together to promote supportive and palliative care pathways for
patients in their last year of life
4. To provide GPs with an opportunity to contribute to the resident’s
advance care planning process
5. To use the DPAG document and Clinical Action Plan templates that
are aligned with the resident’s preferences.