Essential Endocrinology - media control - Startseite€¦ · How to get the best out of your...
30
Transcript of Essential Endocrinology - media control - Startseite€¦ · How to get the best out of your...



Essential Endocrinology and Diabetes


Essential Endocrinology and Diabetes
Richard IG HoltProfessor in Diabetes and Endocrinology
Faculty of MedicineUniversity of Southampton
Neil A HanleyProfessor of Medicine
Faculty of Medical & Human SciencesUniversity of Manchester
Sixth edition
A John Wiley & Sons, Ltd., Publication

This edition first published 2012 © 2012 by Richard IG Holt and Neil A HanleyFifth edition © 2007 Richard Holt and Neil Hanley
Blackwell Publishing was acquired by John Wiley & Sons in February 2007. Blackwell’s publishing program has been merged with Wiley’s global Scientific, Technical and Medical business to form Wiley-Blackwell.
Registered office: John Wiley & Sons, Ltd, The Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK
Editorial offices: 9600 Garsington Road, Oxford, OX4 2DQ, UK The Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK 111 River Street, Hoboken, NJ 07030-5774, USA
For details of our global editorial offices, for customer services and for information about how to apply for permission to reuse the copyright material in this book please see our website at www.wiley.com/wiley-blackwell
The right of the author to be identified as the author of this work has been asserted in accordance with the UK Copyright, Designs and Patents Act 1988.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, except as permitted by the UK Copyright, Designs and Patents Act 1988, without the prior permission of the publisher.
Designations used by companies to distinguish their products are often claimed as trademarks. All brand names and product names used in this book are trade names, service marks, trademarks or registered trademarks of their respective owners. The publisher is not associated with any product or vendor mentioned in this book. This publication is designed to provide accurate and authoritative information in regard to the subject matter covered. It is sold on the understanding that the publisher is not engaged in rendering professional services. If professional advice or other expert assistance is required, the services of a competent professional should be sought.
The contents of this work are intended to further general scientific research, understanding, and discussion only and are not intended and should not be relied upon as recommending or promoting a specific method, diagnosis, or treatment by physicians for any particular patient. The publisher and the author make no representations or warranties with respect to the accuracy or completeness of the contents of this work and specifically disclaim all warranties, including without limitation any implied warranties of fitness for a particular purpose. In view of ongoing research, equipment modifications, changes in governmental regulations, and the constant flow of information relating to the use of medicines, equipment, and devices, the reader is urged to review and evaluate the information provided in the package insert or instructions for each medicine, equipment, or device for, among other things, any changes in the instructions or indication of usage and for added warnings and precautions. Readers should consult with a specialist where appropriate. The fact that an organization or Website is referred to in this work as a citation and/or a potential source of further information does not mean that the author or the publisher endorses the information the organization or Website may provide or recommendations it may make. Further, readers should be aware that Internet Websites listed in this work may have changed or disappeared between when this work was written and when it is read. No warranty may be created or extended by any promotional statements for this work. Neither the publisher nor the author shall be liable for any damages arising herefrom.
Library of Congress Cataloging-in-Publication Data
Holt, Richard I. G. Essential endocrinology and diabetes. – 6th ed. / Richard I.G. Holt, Neil A. Hanley. p. ; cm. – (Essentials) Includes bibliographical references and index. ISBN-13: 978-1-4443-3004-5 (pbk. : alk. paper) ISBN-10: 1-4443-3004-7 (pbk. : alk. paper) 1. Endocrinology–Case studies. 2. Diabetes–Case studies. I. Hanley, Neil A. II. Title. III. Series: Essentials (Wiley-Blackwell) [DNLM: 1. Endocrine Glands–physiology. 2. Diabetes Mellitus. 3. Endocrine System Diseases. 4. Hormones–physiology. WK 100] RC648.H65 2012 616.4–dc23 2011024249
A catalogue record for this book is available from the British Library.
Set in 10 on 12 pt Adobe Garamond Pro by Toppan Best-set Premedia Limited
1 2012

Contents
Preface viiListofabbreviations xHowtogetthebestoutofyourtextbook xii
PART 1: Foundations of Endocrinology 1
1 Overviewofendocrinology 32 Cellbiologyandhormonesynthesis 143 Molecularbasisofhormoneaction 274 Investigationsinendocrinologyanddiabetes 48
PART 2: Endocrinology – Biology to Clinical Practice 63
5 Thehypothalamusandpituitarygland 656 Theadrenalgland 997 Reproductiveendocrinology 1278 Thethyroidgland 1659 Calciumandmetabolicbonedisorders 190
10 Pancreaticandgastrointestinalendocrinologyandendocrineneoplasia 213
PART 3: Diabetes and Obesity 233
11 Overviewofdiabetes 23512 Type1diabetes 25713 Type2diabetes 28514 Complicationsofdiabetes 31115 Obesity 343
Index 360


Preface
There have been significant advances and developments in the 4 years since we wrote the last edition. Consequently, many areas of the book have required substantial updating and extensive re-writing. Nevertheless, the structure of the book has remained similar to the last edition, which seemed popular around the world.
The first part strives to create a knowledgeable reader prepared for the clinical sec-tions. Recognizing that many students now come to medicine from non-scientific backgrounds, we have tried to limit assumptions on prior knowledge. For instance, the concept of negative feedback regulation, covered in Chapter 1, is mandatory for under-standing almost all endocrine physiology and is vital for the interpretation of many clinical tests. Similarly, molecular diagnostics has advanced far beyond the historical development of immunoassays. New modalities, such as molecular genetics, mass spec-trometry and sophisticated imaging, are already standard practice and it is important that aspiring clinicians, as well as scientists, appreciate their methodology, application and limitations. The second part retains a largely organ-based approach. The introduc-tory basic science in these chapters aims to be concise yet sufficient to understand, diagnose and manage the associated clinical disorders. The chapter on endocrine neo-plasia, including hormone-secreting tumours of the gut, has been expanded in recogni-tion of the increasing array of hormones discovered from the pancreas and gastrointestinal tract. In previous editions these hormones have lacked attention. However, many of them are now emerging as key regulators that are exploited in new therapies. For instance, augmentation of glucagon-like peptide 1 signalling is an effective treatment for diabetes. The third part on diabetes and obesity was entirely new in the last edition and these chapters have undergone the greatest change here. Over the last 4 years we have seen significant advances in the treatment of type 2 diabetes such as the new incretin-based therapies and the withdrawal of other treatments due to safety concerns. Clinical algorithms have also changed and these have been updated.
The textbook aims to bridge the gap from basic science training, through clinical train-ing, to the knowledge required for the early postgraduate years and specialist training. The text goes beyond core undergraduate medical education. Learning objectives, boxes, and concluding ‘key points’ aim to emphasize the major topics. There is hopefully useful detail for more advanced clinicians who, like the authors, enjoy trying to interpret clinical medi-cine scientifically, but for whom memory occasionally fails. Although the structure of the book is largely unchanged from the previous edition, readers of the old edition will recog-nize welcome developments. For the first time, the book is in full colour, which has allowed us to include colour photographs in the relevant chapter. We have introduced recap and cross-reference guides at the beginning of each of the clinical chapters to help the reader find important information in other parts of the book more easily. The case histories that were introduced in the last edition proved to be a success and these have been expanded to provide greater opportunity to put theory into practice.
We have brought our clinical and research experiences together to create this book. While it has been a truly collaborative venture and the book is designed to read as a whole, inevitably one of us has taken a lead with each chapter depending on our own interests. As such, NAH was responsible for writing Part 1 and Part 2, while RIGH was responsible for Part 3.

viii / Preface
Finally, we must thank a number of people without whom this book would not have come to fruition. We are grateful for the skilled help of Wiley-Blackwell Publishing and remain indebted to our predecessors up to and including the 4th edition, Charles Brook and Nicholas Marshall, for their excellent starting point. We are also grateful to our families without whose support this book would not have been possible and to whom we dedicate this edition.
The authors
Richard Holt is Professor in Diabetes and Endocrinology at the University of Southampton School of Medicine and Honorary Consultant in Endocrinology at Southampton University Hospitals NHS Trust. His research interests are broadly focused around clinical diabetes with particular interests in diabetes in pregnancy and young adults, and the relation between diabetes and mental illness. He also has a long-standing interest in growth hormone.
Neil Hanley is Professor of Medicine and Wellcome Trust Senior Fellow in Clinical Science at the University of Manchester. He is Honorary Consultant in Endocrinology at the Central Manchester University Hospitals NHS Foundation Trust where he provides tertiary referral endocrine care. His main research interests are human developmental endocrinology and stem cell biology.
Both authors play a keen role in the teaching of undergraduate medical students and doctors. RIGH is a Fellow of the Higher Education Academy. NAH is Director of the Academy for Training & Education at the Manchester Biomedical Research Centre.
R.I.G. HoltUniversity of Southampton
N.A. HanleyUniversity of Manchester

Preface / ix
Further reading
The following major international textbooks make an excellent source of secondary reading:Melmed S, Polonsky KS, Reed Larsen P, Kronenberg HM, eds. Williams Textbook of
Endocrinology, 12th edn. Saunders, 2011.Holt RIG, Cockram C, Flyvbjerg A, Goldstein BJ. Textbook of Diabetes, 4th edn. Wiley-
Blackwell, 2010.In addition, the following textbooks cover topics, relevant to some chapters, in greater detail:Delves PJ, Martin SJ, Burton DR, Roitt IM. Roitt’s Essential Immunology, 12th edn.
Wiley-Blackwell, 2011.Johnson M. Essential Reproduction, 6th edn. Wiley-Blackwell, 2007.Nelson DL, Cox MM. Lehninger Principles of Biochemistry, 5th edn. W.H. Freeman, 2008.

List of abbreviations
5-HIAA 5-hydroxyindoleaceticacid5-HT 5-hydroxytryptophanαMSH α-melanocytestimulatinghormoneACTH adrenocorticotrophichormoneADH vasopressin/antidiuretichormoneAFP α-fetoproteinAGE advancedglycationend-productAGRP Agouti-relatedproteinAI angiotensinIAII angiotensinIIALS acidlabilesubunitAMH anti-MüllerianhormoneAR androgenreceptorAPS-1 type1autoimmunepolyglandular
syndromeAPS-2 type2autoimmunepolyglandular
syndromeCAH congenitaladrenalhyperplasiacAMP cyclicadenosinemonophosphateCBG cortisolbindingglobulincGMP guanosinemonophosphateCRE cAMPresponseelementCREB cAMPresponseelement-binding
proteinCNS centralnervoussystemCRH corticotrophin-releasinghormoneCSF cerebrospinalfluidCT computedtomographyCVD cardiovasculardiseaseDAG diacylglycerolDEXA dualenergyX-rayabsorptiometryDHEA dehydroepiandrosteroneDHT 5α-dihydrotestosteroneDI diabetesinsipidusEGF epidermalgrowthfactorEPO erythropoietinER oestrogenreceptorFFA freefattyacidFGF fibroblastgrowthfactorFIA fluoroimmunoassayFISH fluorescencein situhybridizationFSH follicle-stimulatinghormonefT3 freetri-iodothyroninefT4 freethyroxine
GC gaschromatographyGDM gestationaldiabetesGFR glomerularfiltrationrateGH growthhormone(somatotrophin)GHR GHreceptorGHRH growthhormone-releasinghormoneGI glycaemicindexGIP glucose-dependentinsulinotrophic
peptide(gastricinhibitorypeptide)GLUT glucosetransporterGnRH gonadotrophin-releasinghormoneGPCR guanine-proteincoupledreceptorGR glucocorticoidreceptorGrb2 type2growthfactorreceptor-bound
proteinhCG humanchorionicgonadotrophinhMG humanmenopausalgonadotrophinHMGCoA hydroxymethylglutarylcoenzymeAHNF hepatocytenuclearfactorHPLC highperformanceliquid
chromatographyHRE hormoneresponseelementHRT hormonereplacementtherapyICSI intracytoplasmicsperminjectionIDDM insulin-dependentdiabetesmellitusIFG impairedfastingglycaemiaIFMA immunofluorometricassayIGF insulin-likegrowthfactorIGFBP IGF-bindingproteinIGT impairedglucosetoleranceIP inositolphosphateIPF insulinpromoterfactorIR insulinreceptorIRMA intraretinalmicrovascular
abnormalities(Chapter14)IRMA immunoradiometricassay
(Chapter4)IRS insulinreceptorsubstrateIVF in vitrofertilizationJAK Janus-associatedkinaseLDL low-densitylipoproteinLH luteinizinghormoneMAO monoamineoxidaseMAPK mitogen-activatedproteinkinase

List of abbreviations / xi
MEN multipleendocrineneoplasiaMIS MüllerianinhibitingsubstanceMODY maturity-onsetdiabetesoftheyoungMR mineralocorticoidreceptorMRI magneticresonanceimagingMS massspectrometryMSH melanocyte-stimulatinghormoneNEFA non-esterifiedfattyacidNICTH non-isletcelltumourhypoglycaemiaNIDDM non–insulin-dependentdiabetes
mellitusNPY neuropeptideYNVD newvesselsatthediscNVE newvesselselsewhereOGTT oralglucosetolerancetestPCOS polycysticovariansyndromePCR polymerasechainreactionPDE phosphodiesterasePGE2 prostaglandinE2
PI phosphatidylinositolPIT1 pituitary-specifictranscription
factor1PKA proteinkinaseAPKC proteinkinaseCPLC phospholipaseCPNMT phenylethanolamineN-methyl
transferasePOMC pro-opiomelanocortinPPAR peroxisomeproliferator-activated
receptorPRL prolactinPTH parathyroidhormonePTHrP parathyroidhormone-relatedpeptidePTU propylthiouracil
RANK receptoractivatorofnuclearfactor-kappaB
RER roughendoplasmicreticulumRIA radioimmunoassayrT3 reversetri-iodothyronineRXR retinoidXreceptorSERM selectiveERmodulatorSHBG sexhormone-bindingglobulinSIADH syndromeofinappropriate
antidiuretichormoneSoS sonofsevenlessproteinSRE serumresponseelementSS somatostatinStAR steroidacuteregulatoryproteinSTAT signaltransductionandactivationof
transcriptionproteinT1DM type1diabetesT2DM type2diabetest1/2 half-lifeT3 tri-iodothyronineT4 thyroxineTGFβ transforminggrowthfactorβTK tyrosinekinaseTPO thyroidperoxidaseTR thyroidhormonereceptorTRE thyroidhormoneresponseelementTRH thyrotrophin-releasinghormoneTSH thyroid-stimulatinghormoneUFC urinaryfreecortisolV vasopressin/antidiuretichormone
(previouslyalsoknownasargininevasopressin)
VEGF vascularendothelialgrowthfactorVIP vasoactiveintestinalpeptide

How to get the best out of your textbook
Welcome to the new edition of Essential Endocrinology and Diabetes. Over the next few pages you will be shown how to make the most of the learning features included in the textbook.
The anytime, anywhere textbook
For the first time, your textbook comes with free access to a Wiley Desktop Edition – a digital, interactive version of this textbook which you own as soon as you download it. Your Wiley Desktop Edition allows you to:
Search: Save time by finding terms and topics instantly in your book, your notes, even your whole library (once you’ve downloaded more textbooks)Note and Highlight: Colour code highlights and make digital notes right in the text so you can find them quickly and easilyOrganize: Keep books, notes and class materials organized in folders inside the applicationShare: Exchange notes and highlights with friends, classmates and study groupsUpgrade: Your textbook can be transferred when you need to change or upgrade computers
To access your Wiley Desktop Edition:
• Find the redemption code on the inside front cover of this book and carefully scratch away the top coating of the label.
• Visit www.vitalsource.com/software/bookshelf/downloads to download the Bookshelf application to your computer, laptop or mobile device
• Open the Bookshelf application on your computer and register for an account.
• Follow the registration process and enter your redemption code to download your digital book.

Chapter 7: / xiiiHow to get the best out of your textbook / xiii
CourseSmart gives you instant access (via computer or mobile device) to this Wiley-Blackwell eTextbook and its extra electronic functionality, at 40% off the recommended retail print price. See all the benefits at: www.coursesmart.com/students.
Instructors . . . receive your own digital desk copies!
It also offers you an immediate, efficient, and environmentally-friendly way to review this textbook for your course. For more information visit:www.coursesmart.com/instructors.With CourseSmart, you can create lecture notes quickly with copy and paste, and share pages and notes with your students. Access your Wiley CourseSmart digital textbook from your computer or mobile device instantly for evaluation, class prepara-tion, and as a teaching tool in the classroom.
Simply sign in at:http://instructors.coursesmart.com/bookshelf to download your Bookshelf and get started. To request your desk copy, hit ‘Request Online Copy’ on your search results or book product page.
CourseSmart®
Throughout your textbook you will find this icon which points you to cases with self-test questions. You will find the answers at the end of each chapter.
You will also find a helpful list of key points at the end of each chapter which give a quick summary of important principles.
Features contained within your textbook
Every chapter has its own chapter-opening page that offers a list of key topics and learning objectives pertaining to the chapter
RE
VI S
ED
311
Essential Endocrinology and Diabetes, Sixth Edition. Richard IG Holt, Neil A Hanley. © 2012 Richard IG Holt and Neil A Hanley. Publlished 2012 by Blackwell Publishing Ltd.
CHAPTER 14
Complications of diabetes
Key topics
� Microvascular complications 312
� Macrovascular disease 330
� Cancer 334
� Psychological complications 334
� How diabetes care can reduce complications 335
� Diabetes and pregnancy 336
� Social aspects of diabetes 339
� Key points 340
� Answers to case histories 340
Learning objectives
� To discuss the causes of microvascular and macrovascular complications
� To understand the importance of screening for complications
� To understand the strategies to prevent and treat complications
� To discuss diabetes in pregnancy
� To understand the psychosocial aspects of diabetes
This chapter discusses the microvascular and macrovascular complications of diabetes, diabetes in pregnancy and psychosocial aspects of diabetes
onsonssss
RE
VI S
ED
3
Essential Endocrinology and Diabetes, Sixth Edition. Richard IG Holt, Neil A Hanley. © 2012 Richard IG Holt and Neil A Hanley. Publlished 2012 by Blackwell Publishing Ltd.
CHAPTER 1
Overview of endocrinology
Key topics
� A brief history of endocrinology and diabetes 4
� The role of hormones 5
� Classification of hormones 8
� Organization and control of endocrine organs 9
� Endocrine disorders 13
� Key points 13
Learning objectives
� To be able to define endocrinology
� To understand what endocrinology is as a basic science and a clinical specialty
� To appreciate the history of endocrinology
� To understand the classification of hormones into peptides, steroids and amino acid derivatives
� To understand the principle of feedback mechanisms that regulate hormone production
This chapter details some of the history to endocrinology and diabetes, and introduces basic principles that underpin the subsequent chapters
d dd

Cross-reference
The development of the parathyroid and parafollicular C-cells is described alongside the thyroid in Chapter 8
Tumours of the parathyroid glands are an important component of multiple endocrine neoplasia, covered in Chapter 10
Other hormones such as cortisol (see Chapter 6) and sex hormones (see Chapter 7) affect mineralization of the bones
Your textbook is full of useful photographs, illustrations and tables. The Desktop Edition version of your textbook will allow you to copy and paste any photograph or illustration into assignments, presentations and your own notes.
102 / Chapter 6: The adrenal gland Chapter 6: The adrenal gland / 103
Figure 6.2 Section through the adrenal cortex. (a) The blood vessels run from outer capsule to medullary venule. (b) A zona fasciculata cell with large lipid droplets, extensive smooth endoplasmic reticulum and mitochondria.
Smooth endoplasmic reticulum
Lipid droplets Mitochondria
Capsule
Zonaglomerulosa
Zonafasciculata
Zonareticularis
Medulla
(a) (b)
Capillary
Venule
Box 6.2 Zones of the adult adrenal cortex and their steroid hormone secretion
• Zona glomerulosa, nests of closely packed small cells creating the thinnest, outermost layer; secretes aldosterone
• Zona fasciculata, larger cells in columns making up ∼three-quarters of the cortex; secretes cortisol and some sex steroid precursors
• Zona reticularis, ‘net-like’ arrangements of innermost cells, formed at 6–8 years to herald a poorly understood change called ‘adrenarche’; secretes sex steroid precursors and some cortisol
cortisol measurement; an important clinical issue. Like thyroid hormones, it is only the free compo-nent that enters target cells. �e free component also passes into urine – ‘urinary free cortisol’ (UFC) – where its collection and assay over 24 h has been
used as a test of glucocorticoid excess (UFC is ∼1% of cortisol production by the adrenal glands). Measuring salivary cortisol similarly avoids issues with �uctuating serum CBG.
Regulation of cortisol biosynthesis and secretion – the hypothalamic–pituitary–adrenal axis�e major regulation of the adrenal cortex comes from the anterior pituitary, via the produc-tion and circulation of adrenocorticotrophic hor-mone (ACTH), a cleavage product of the pro-opiomelanocortin (POMC) gene (review Chapter 5). In turn, ACTH is regulated by corticotrophin-releasing hormone (CRH) from the hypothalamus (Figure 6.4). By binding to cell-surface receptors and activating cAMP second messenger pathways, ACTH increases �ux through the pathway from cholesterol to cortisol, particularly at the rate-limiting step catalyzed by CYP11A1. �is happens acutely such that a rise in ACTH increases cortisol levels within 5 min. Cortisol provides feedback to the anterior pituitary and hypothalamus to
17α-hydroxylase(CYP17A1)
21-hydroxylase(CYP21A2)
11β-hydroxylase(CYP11B1)
21-hydroxylase(CYP21A2)
11β-hydroxylase(CYP11B2)
3β-hydroxysteroiddehydrogenase(HSD3B2)
18-hydroxylase(CYP11B2)
Aldosterone synthase(CYP11B2)
Cholesterol side chaincleavage (CYP11A1)
17,20-lyase(CYP17A1)
Sulphotransferase(SULT2A1)
Cholesterol
Pregnenolone
Progesterone
Deoxy-corticosterone
Corticosterone
18-hydroxy-corticosterone
Cortisol
11-deoxycortisol
17a-hydroxy-progesterone
17a-hydroxy-pregnenolone
Dehydroepi-androsterone (DHEA)
(DHEAS)
DHEAsulphate
Androstenedione
Aldosterone
Figure 6.3 Biosynthesis of adrenocortical steroid hormones. HSD3B activity in the adrenal cortex arises from the type 2 isoform. The three steps from deoxycorticosterone to aldosterone are catalyzed by the same enzyme, CYP11B2 (also see Figure 2.6).
Box 6.3 Adrenocortical steroidogenesis can be summarized into a few key steps
• Transport of cholesterol into the mitochondrion by the steroid acute regulatory (StAR) protein
• The rate-limiting removal of the cholesterol side chain by CYP11A1
• Shuttling intermediaries between mitochondria and endoplasmic reticulum for further enzymatic modification
• Action of two key enzymes at branch points:
° CYP17A1 prevents the biosynthesis of aldosterone and commits a steroid to
cortisol or sex steroid precursor. Hence, CYP17A1 is absent from the zona glomerulosa
° Early action of HSD3B2 steers steroid precursors away from the sex steroid precursors towards aldosterone or cortisol
• The presence and activity of CYP11B2 in the zona glomerulosa permitting aldosterone synthesis
• The presence and activity of CYP11B1 in the fasciculata (and less so the reticularis) zone allowing cortisol production
252 / Chapter 11: Overview of diabetes Chapter 11: Overview of diabetes / 253
Table 11.6 Insulin actions on carbohydrate metabolism
Action Mechanism
Increases glucose uptake into cells
Translocation of glucose transporter (GLUT)-4 to the cell surface
Increases glycogen synthesis Activates glycogen synthase by dephosphorylation
Inhibits glycogen breakdown Inactivates glycogen phosphorylase and its activating kinase by dephosphorylation
Inhibits gluconeogenesis Dephosphorylation of pyruvate kinase and 2,6-biphosphate kinase
Increases glycolysis Dephosphorylation of pyruvate kinase and 2,6-biphosphate kinase
Converts pyruvate to acetyl CoA
Activates the intramitochondrial enzyme complex pyruvate dehydrogenase
phosphorylation and dephosphorylation of the enzymes controlling glycogenolysis and glycogen synthesis (Figure 11.12). �e rate-limiting enzymes are the catabolic enzyme glycogen phosphorylase and the anabolic enzyme glycogen synthase. Insulin increases glycogen synthesis by activating glycogen synthase, while inhibiting glycogenolysis by dephosphorylating glycogen phosphorylase kinase. Glycolysis is stimulated and gluconeogenesis inhib-ited by dephosphorylation of pyruvate kinase (PK) and 2,6-biphosphate kinase. Insulin also enhances the irreversible conversion of pyruvate to acetyl CoA by activation of the intramitochondrial enzyme complex pyruvate dehydrogenase. Acetyl CoA may then be directly oxidized via the tricarboxylic acid (Krebs’) cycle, or used for fatty acid synthesis (Figure 11.13).
Lipid metabolismInsulin increases the rate of lipogenesis in several ways in adipose tissue and liver, and controls the formation and storage of triglyceride. �e critical step in lipogenesis is the activation of the insulin-sensitive lipoprotein lipase in the capillaries. Fatty acids are then released from circulating chylomicrons or very low-density lipoproteins and taken up into the adipose tissue. Fatty acid synthesis is increased by activation and increased phosphorylation of acetyl CoA carboxylase, while fat oxidation is suppressed by inhibition of carnitine acyltransferase (Table 11.7). Lipogenesis is also facilitated by glucose uptake, because its metabo-
lism by the pentose phosphate pathway provides nicotinamide adenine dinucleotide phosphate (NADPH), which is needed for fatty acid synthesis.
Triglyceride synthesis is stimulated by ester-i�cation of glycerol phosphate, while triglyceride breakdown is suppressed by dephosphorylation of hormone-sensitive lipase.
Cholesterol synthesis is increased by activation and dephosphorylation of hydroxymethylglutaryl co-enzyme A (HMGCoA) reductase, while choles-terol ester breakdown appears to be inhibited by dephosphorylation of cholesterol esterase. Phospholipid metabolism is also in�uenced by insulin.
Protein metabolismInsulin stimulates the uptake of amino acid into cells and promotes protein synthesis in a range of tissues. �ere are e�ects on the transcription of speci�c mRNA, as well as their translation into proteins on the ribosomes (review Chapter 2 and Figure 2.2). Examples of enhanced mRNA tran-scription include glucokinase and fatty acid syn-thase. By contrast, insulin decreases mRNA encoding liver enzymes such as carbamoyl phos-phate synthetase, which is a key enzyme in the urea cycle. However, the major action of insulin on protein metabolism is to inhibit the breakdown of proteins (Figure 11.14). In this way it acts synergis-tically with GH and insulin-like growth factor I (IGF-I) to increase protein anabolism.
Figure 11.12 Inter-relationships among alternative routes of glucose metabolism. The central role of glucose in carbohydrate, fat and protein metabolism is summarized. The principal metabolic pathways are shown enclosed in boxes in order to simplify the diagram; some key intermediates and products of metabolic interconversions are shown. The
reversibility of certain reaction sequences implied by double-headed arrows is not necessarily intended to suggest that the same enzymes are involved in both the forward and reverse reactions. The principal reversible pathways that are activated during fasting are marked with heavy arrows.
Glucose
Glycolytic-gluconeogenicpathways
Pentosephosphatepathway
Glucuronate-xylulosepathway
Tricarboxylicacid cycle
Proteindegradation
Lipidsynthesis
Ureacycle
Sorbitol route
Glucose-6- P Glucose-1- P
UDP-Glucose
Ribose-5- P
α-Glycero- P
α-Glycero- P
NH3
NADPH NADP+Lactate Pyruvate
AcetylCoA
ATPAmino acids
Fructose
Glycogen
GlycoproteinMucopoly-saccharide
NucleotidesRNA and DNA
Triglycerides
Urea
Table 11.7 Insulin actions on fatty acid metabolism
Action Mechanism
Releases fatty acids from circulatingchylomicrons or very low-density lipoproteins
Activates lipoprotein lipase
Increases fatty acid synthesis Activates acetyl CoA carboxylase
Suppresses fatty acid oxidation Inhibits carnitine acyltransferase
Increases triglyceride synthesis Stimulates esterification of glycerol phosphate
Inhibits triglyceride breakdown Dephosphorylates hormone-sensitive lipase
Increases cholesterol synthesis Activates and dephosphorylates HMGCoA reductase
Inhibits cholesterol ester breakdown Dephosphorylates cholesterol esterase
We hope you enjoy using your new textbook. Good luck with your studies!
xiv / How to get the best out of your textbook
At the beginning of some chapters you will also find cross-references which make it easy to locate related information quickly and efficiently.

Part 1Foundations of Endocrinology


3
Essential Endocrinology and Diabetes, Sixth Edition. Richard IG Holt, Neil A Hanley. © 2012 Richard IG Holt and Neil A Hanley. Publlished 2012 by Blackwell Publishing Ltd.
CHAPTER 1
Overview of endocrinology
Key topics
■ A brief history of endocrinology and diabetes 4
■ The role of hormones 5
■ Classification of hormones 8
■ Organization and control of endocrine organs 9
■ Endocrine disorders 13
■ Key points 13
Learning objectives
■ To be able to define endocrinology
■ To understand what endocrinology is as a basic science and a clinical specialty
■ To appreciate the history of endocrinology
■ To understand the classification of hormones into peptides, steroids and amino acid derivatives
■ To understand the principle of feedback mechanisms that regulate hormone production
This chapter details some of the history to endocrinology and diabetes, and introduces basic principles that underpin the subsequent chapters

4 / Chapter 1: Overview of endocrinology
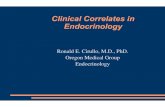
Figure 1.1 Cells that secrete regulatory substances to communicate with their target cells and organs. (a) Endocrine. Cells secrete hormone into the blood vessel, where it is carried, potentially over large distances, to its target cell. (b) Autocrine (A): hormones such as insulin-like growth factors can act on the cell that produces them, representing autocrine control. Paracrine (P): cells secrete hormone that acts on nearby cells (e.g. glucagon and somatostatin act on adjacent β-cells within the pancreatic islet to influence insulin secretion). (c) Stimulated neuroendocrine cells secrete hormone (e.g. the hypothalamic hormones that regulate the anterior pituitary) from axonic terminals into the bloodstream. (d) Neurotransmitter cells secrete substances from axonic terminals to activate adjacent neurones.
Neurotransmitter
Neurone
Neurone
Target cellBlood vessel
Axon
Axonterminal
Nerve cell
Blood vessel
Hormone Target cell
Local hormone
Target cell
A P
(a) Endocrine (b) Autocrine (A) and Paracrine (P)
(c) Neuroendocrine (d) Neurotransmitter
An organism comprised of a single or a few cells analyzes and responds to its external environment with relative ease. No cell is more than a short dif-fusion distance from the outside world or its neigh-bours, allowing a constancy of internal environment (‘homeostasis’). This simplicity has been lost with the evolution of more complex, larger, multicellular organisms. Simple diffusion has become inadequate in larger animal species where functions localize to specific organs. In humans, there are ∼1014 cells of 200 or more different types. With this compart-mentalized division of purpose comes the need for effective communication to disseminate informa-tion throughout the whole organism – only a few cells face the outside world, yet all respond to it. Two communication systems facilitate this: the endocrine and nervous systems (Box 1.1).
The specialized ductless glands and tissues of the endocrine system release chemical messengers – hormones – into the extracellular space, from where they enter the bloodstream. It is this blood-borne transit that defines endocrinology; however, the principles are similar for hormone action on a neighbouring cell (‘paracrinology’) or, indeed, itself (‘auto- or intra-crinology’) (Figure 1.1).
The nervous and endocrine systems interact. Endocrine glands are under both nervous and hor-monal control, while the central nervous system is affected by multiple hormonal stimuli – features reflected by the composite science of neuroendo-crinology (Figure 1.1).
A brief history of endocrinology and diabetes
The term ‘hormone’, derived from the Greek word ‘hormaein’ meaning ‘to arouse’ or ‘to excite’, was first used in 1905 by Sir Ernest Starling in his Croonian Lecture to the Royal College of Physicians;
Box 1.1 Functions of the endocrine and nervous systems, the two main communication systems
• To monitor internal and external environments
maintain homeostasis• To allow appropriate
adaptive changes• To communicate via
chemical messengers}

Chapter 1: Overview of endocrinology / 5
however, the specialty is built on foundations that are far older. Aristotle described the pituitary, while the associated condition, gigantism, due to excess growth hormone (GH), was referred to in the Old Testament, two millennia or so before the 19th century recognition of the gland’s anterior and pos-terior components by Rathke, and Pierre Marie’s connection of GH-secreting pituitary tumours to acromegaly.
Diabetes was recognized by the ancient Egyptians. Areteus later described the disorder in the second century ad as ‘a melting down of flesh and limbs into urine’ – diabetes comes from the Greek word meaning siphon. The pancreas was only implicated relatively recently when Minkowski real-ized in 1889 that the organ’s removal in dogs mim-icked diabetes in humans.
The roots of reproductive endocrinology are equally long. The Bible refers to eunuchs and Hippocrates recognized that mumps could result in sterility. Oophorectomy in sows and camels was used to increase strength and growth in ancient Egypt. The association with technology is also long-standing. For instance, it took the microscope in the 17th century for Leeuwenhoek to visualize sperma-tozoa and later, in the 19th century, for the mam-malian ovum to be discovered in the Graafian follicle.
During the last 500 years, other endocrine organs and axes have been identified and character-ized. In 1564, Bartolommeo Eustacio noted the presence of the adrenal glands. Almost 300 years later (1855), Thomas Addison, one of the forefa-thers of clinical endocrinology, described the con-sequences of their inadequacy. Catecholamines were identified at the turn of the 19th century, in parallel with Oliver and Schaffer’s discovery that these adrenomedullary substances raise blood pressure. This followed shortly after the clinical features of myxoedema were linked to the thyroid gland, when, in 1891, physicians in Newcastle treated hypothy-roidism with sheep thyroid extract. This was an important landmark, but long after the ancient Chinese recognized that seaweed, as a source of iodine, held valuable properties in treating ‘goitre’, swelling of the thyroid gland.
Early clinical endocrinology and diabetes tended to recognize and describe the features of the endo-
crine syndromes. Since then, our understanding has advanced through:
• Successful quantification of circulating hormones• Pathophysiological identification of endocrine dysfunction• Molecular genetic diagnoses• Molecular unravelling of complex hormone action.
Some of the landmarks from the last 100 years are shown in Box 1.2, and those researchers who have been awarded the Nobel Prize for Medicine, Physiology or Chemistry for discoveries that have advanced endocrinology and diabetes are listed in Table 1.1.
Traditionally, endocrinology has centred on spe-cialized hormone-secreting organs (Figure 1.2), largely built on the ‘endocrine postulates’ of Edward Doisy (Box 1.3). While the focus of this textbook remains with these organs, many tissues display appreciable degrees of hormone biosynthesis, and, equally relevant, modulate hormone action. All aspects are important for a complete appreciation of endocrinology and its significance.
The role of hormones
Hormones are synthesized by specialized cells (Table 1.2), which may exist as distinct endocrine glands or be located as single cells within other organs, such as the gastrointestinal tract. The chap-ters in Part 2 are largely organized on this anatomi-cal basis.
Endocrinology is defined by the secretion of hormones into the bloodstream; however, autocrine or paracrine actions are also important, often mod-ulating the hormone-secreting cell type. Hormones act by binding to specific receptors, either on the surface of or inside the target cell, to initiate a cascade of intracellular reactions, which frequently amplifies the original stimulus and generates a final response. These responses are altered in hormone deficiency and excess: for instance, GH deficiency leads to short stature in children, while excess causes over-growth (either gigantism or acromegaly; Chapter 5).

6 / Chapter 1: Overview of endocrinology
Box 1.2 Some landmarks in endocrinology over the last 100 years or so
1905 First use of the term ‘hormone’ by Starling in the Croonian Lecture at the Royal College of Physicians
1909 Cushing removed part of the pituitary and saw improvement in acromegaly1914 Kendall isolated an iodine-containing substance from the thyroid1921 Banting and Best extracted insulin from islet cells of dog pancreas and used it to
lower blood sugarEarly 1930s Pitt-Rivers and Harrington determined the structure of the thyroid hormone,
thyroxine1935–40 Crystallization of testosterone1935–40 Identification of oestrogen and progesterone1940s Harris recognized the relationship between the hypothalamus and anterior pituitary
in the ‘portal-vessel chemotransmitter hypothesis’1952 Gross and Pitt-Rivers identified tri-iodothyronine in human serum1955 The Schally and Guillemin laboratories showed that extracts of hypothalamus
stimulated adrenocorticotrophic hormone (ACTH) release1956 Doniach, Roitt and Campbell associated antithyroid antibodies with some forms of
hypothyroidism – the first description of an autoimmune phenomenon1950s Adams and Purves identified thyroid stimulatory auto-antibodies
Gonadectomy and transplantation experiments by Jost led to the discovery of the role for testosterone in rabbit sexual development
1955 Sanger reported the primary structure of insulin1957 Growth hormone was used to treat short stature in patients1966 First transplant of human pancreas to treat type 1 diabetes by Kelly, Lillehei, Goetz
and Merkel at the University of Minnesota1969 Hodgkin reported the three-dimensional crystallographic structure of insulin1969–71 Discovery of thyrotrophin-releasing hormone (TRH) and gonadotrophin-releasing
hormone (GnRH) by Schally’s and Guillemin’s groups1973 Discovery of somatostatin by the group of Guillemin1981–2 Discovery of corticotrophin-releasing hormone (CRH) and growth hormone-
releasing hormone (GHRH) by Vale1994 Identification of leptin by Friedman and colleagues1994 First transplantation of pancreatic islets to treat type 1 diabetes by Pipeleers and
colleagues in Belgium1999 Discovery of ghrelin by Kangawa and colleagues1999 Sequencing of the human genome – publication of the DNA code for
chromosome 222000 Advanced islet transplantation using modified immunosuppression by Shapiro and
colleagues to treat type 1 diabetes
Thyroid hormone acts on many, if not all, of the 200 plus cell types in the body. The basal metabolic rate increases if it is present in excess and declines if there is a deficiency (see Chapter 8). Similarly, insulin acts on most tissues, implying its receptors are widespread. Its importance is also underlined by
its role in the survival and growth of many cell types in laboratory culture. In contrast, other hormones may act only on one tissue. Thyroid-stimulating hormone (TSH), adrenocorticotrophic hormone (ACTH) and the gonadotrophins are secreted by the anterior pituitary and have specific target tissues

Chapter 1: Overview of endocrinology / 7
Table 1.1 Nobel prize winners for discoveries relevant to endocrinology and diabetes
Year Prize winner(s) For work on . . .
1909 Emil Theodor Kocher Physiology, pathology and surgery of the thyroid gland
1923 Frederick Grant Banting and John James Richard Macleod
Discovery of insulin
1928 Adolf Otto Reinhold Windhaus Constitution of the sterols and their connection with the vitamins
1939 Adolf Friedrich and Johann Butenandt Sex hormones
1943 George de Hevesy Use of isotopes as tracers in the study of chemical processes
1946 James Batcheller Summer, John Howard Northrop and Wendell Meredith Stanley
Discovery that enzymes can be crystallized and prepared in a pure form
1947 Carl Ferdinand Cori, Getty Theresa Cori (neé Radnitz) and Bernardo Alberto Houssay
Discovery of the course of the catalytic conversion of glycogen
1950 Edwin Calvin Kendall, Tadeus Reichstein and Philip Showalter Hench
Discoveries relating to the hormones of the adrenal cortex, their structure and biological effects
1955 Vincent du Vigneaud Biochemically important sulphur compounds, especially for the first synthesis of a polypeptide hormone
1958 Frederick Sanger Structures of proteins, especially that of insulin
1964 Konrad Bloch and Feodor Lynen Discoveries concerning the mechanism and regulation of cholesterol and fatty acid metabolism
1966 Charles Brenton Huggins Discoveries concerning hormonal treatment of prostatic cancer
1969 Derek HR Barton and Odd Hassel Development of the concept of conformation and its application in chemistry
1970 Bernard Katz, Ulf von Euler and Julius Axelrod
Discoveries concerning the humoral transmitters in the nerve terminals and the mechanism for their storage, release and inactivation
1971 Earl W Sutherland Jr Discoveries concerning the mechanisms of the action of hormones
1977 Roger Guillemin, Andrew V Schally and Rosalyn Yalow
Discoveries concerning peptide hormones in the production in the brain and the development of radioimmunoassay from peptide hormones
1979 Allan M Cormack and Godfrey N Hounsfield
Development of computer-assisted tomography
(Continued )

8 / Chapter 1: Overview of endocrinology
Year Prize winner(s) For work on . . .
1982 Sune K Bergström, Bengt I Samuelson and John R Vane
Discoveries concerning prostaglandins and related biologically active substances
1985 Michael S Brown and Joseph L Goldstein Discoveries concerning the regulation of cholesterol metabolism
1986 Stanley Cohen and Rita Levi-Montalcini Discoveries of growth factors
1992 Edmond H Fischer and Edwin G Krebs Discoveries concerning reversible protein phosphorylation as a biological regulatory mechanism
1994 Alfred G Gilman and Martin Rodbell Discovery of G-proteins and the role of these proteins in signal transduction in cells
2003 Peter Agre and Roderick MacKinnon Discovery of water channels, and the structural and mechanistic studies of ion channels
2003 Paul Lauterbur and Sir Peter Mansfield Discoveries concerning magnetic resonance imaging
2010 Robert G Edwards Development of in vitro fertilization
Table 1.1 (Continued )
– the thyroid gland, the adrenal cortex and the gonads, respectively (Table 1.2).
Classification of hormones
There are three major groups of hormones accord-ing to their biochemistry (Box 1.4). Peptide or protein hormones are synthesized like any other cellular protein. Amino acid-derived and steroid hormones originate from a cascade of biochemical reactions catalyzed by a series of intracellular enzymes.
Peptide hormones
The majority of hormones are peptides and range in size from very small, only three amino acids [thyrotrophin-releasing hormone (TRH)], to small proteins of over 200 amino acids, such as TSH or luteinizing hormone (LH). Some peptide hormones are secreted directly, but most are stored in granules, the release from which is commonly controlled by another hormone, as part of a cascade, or by innervation.
Some peptide hormones have complex tertiary structures or are comprised of more than one peptide chain. Oxytocin and vasopressin, the two posterior pituitary hormones, have ring structures linked by disulphide bridges. Despite being remark-ably similar in structure, they have very different physiological roles (Figure 1.3). Insulin consists of α- and β-chains linked by disulphide bonds. Like several hormones, it is synthesized as an inactive precursor that requires modification prior to release and activity. To some extent this regulation protects the synthesizing cell from being overwhelmed by its own hormone action. The gonadotrophins, follicle-stimulating hormone (FSH) and LH, TSH and human chorionic gonadotrophin (hCG) also have two chains. However, these α- and β-subunits are synthesized quite separately, from separate genes. The α-subunit is common; the distinctive β-subunit of each confers biological specificity.
Amino acid derivatives
These hormones are small water-soluble com-pounds. Melatonin is derived from tryptophan, whereas tyrosine derivatives include thyroid hor-

Chapter 1: Overview of endocrinology / 9
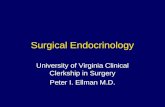
Four parathyroidglands
Stomach
Kidney
Pancreas: Islets of Langerhans
Two ovaries(o)
Two testes(o)
Duodenum
Two adrenalglands: cortex
and medulla
Pituitary gland:anterior and
posterior
Thyroidgland
Hypothalamusand medianeminence
Figure 1.2 The sites of the principal endocrine glands. The stomach, kidneys and duodenum are also shown. Not shown, scattered cells within the gastrointestinal tract secrete hormones.
stituent of the cell membrane. Produced by the adrenal cortex, gonad and placenta, steroid hor-mones are insoluble in water and largely circulate bound to plasma proteins.
Organization and control of endocrine organs
The synthesis and release of hormones is regulated by control systems, similar to those used in engineer-ing. These mechanisms ensure that hormone signals can be limited in amplitude and duration. Central to the regulation of many endocrine organs is the anterior pituitary gland, which, in turn, is controlled by a number of hormones and factors released from specialized hypothalamic neurones (see Chapter 5). Thus, major endocrine axes comprise the hypotha-lamus, anterior pituitary and end organ, such as the adrenal cortex, thyroid, testis or ovary. An under-standing of these control mechanisms is crucial for appreciating both regulation of many endocrine systems and their clinical investigation.
Simple control
An elementary control system is one in which the signal itself is limited, either in magnitude or
Box 1.3 The ‘Endocrine Postulates’: Edward Doisy, St Louis University School of Medicine, USA, 1936
• The gland must secrete something (an ‘internal secretion’)
• Methods of detecting the secretion must be available
• Purified hormone must be obtained from gland extracts
• The pure hormone must be isolated, its structure determined and synthesized
To this could be added:• The hormone must act on specific target
cells via a receptor such that excess or deficiency results in a specific phenotype
mones, catecholamines, and dopamine, which regulates prolactin secretion in the anterior pitui-tary. The catecholamines from the adrenal medulla, epinephrine (adrenaline) and norepinephrine (noradrenaline), are also sympathetic neurotrans-mitters, emphasizing the close relationship between the nervous and endocrine systems (see Figure 1.2). Like peptide hormones, they are stored in granules prior to release.
Steroid hormones
Steroid hormones are lipid-soluble molecules derived from cholesterol, which is itself a basic con-

10 / Chapter 1: Overview of endocrinology
Table 1.2 The endocrine organs and their hormones*
Gland Hormone Molecular characteristics
Hypothalamus/median eminence
Releasing and inhibiting hormones:
Thyrotrophin-releasing hormone (TRH) Peptide
Somatostatin (SS; inhibits GH)) Peptide
Gonadotrophin-releasing hormone (GnRH) Peptide
Corticotrophin-releasing hormone (CRH) Peptide
Growth hormone-releasing hormone (GHRH) Peptide
Dopamine (inhibits prolactin) Tyrosine derivative
Anterior pituitary Thyrotrophin or thyroid-stimulating hormone (TSH)
Glycoprotein
Luteinizing hormone (LH) Glycoprotein
Follicle-stimulating hormone (FSH) Glycoprotein
Growth hormone (GH) (also called somatotrophin)
Protein
Prolactin (PRL) Protein
Adrenocorticotrophic hormone (ACTH) Peptide
Posterior pituitary Vasopressin [also called antidiuretic hormone (ADH)]
Peptide
Oxytocin Peptide
Thyroid Thyroxine (T4) and tri-iodothyronine (T3) Tyrosine derivatives
Calcitonin Peptide
Parathyroid Parathyroid hormone (PTH) Peptide
Adrenal cortex Aldosterone Steroid
Cortisol Steroid
Androstenedione Steroid
Dehydroepiandrosterone (DHEA) Steroid
Adrenal medulla Epinephrine (also called adrenaline) Tyrosine derivative
Norepinephrine (also called noradrenaline) Tyrosine derivative
Stomach† Gastrin Peptide
Pancreas (islets of Langerhans)†
Insulin Protein
Glucagon Protein
Somatostatin (SS) Protein
Duodenum and jejunum†
Secretin Protein
Cholecystokinin Protein

Chapter 1: Overview of endocrinology / 11
Box 1.4 Major hormone groups
• Peptides and proteins• Amino acid derivatives• Steroids
duration, so as to induce only a transient response. Certain neural impulses are of this type. Refinement allows discrimination of a positive signal from background ‘noise’ to ensure that the target cell cannot or does not respond below a certain thresh-old level. An example is the pulsatile release of gonadotrophin-releasing hormone (GnRH) from the hypothalamus.
Negative feedback
Negative feedback is the commonest form of regula-tion used by many biological systems. For example,
in enzymology, the product frequently inhibits further progress of the catalyzed reaction. In endo-crinology, a hormone may act on its target cell to stimulate a response (often secretion of another hormone) that then inhibits production of the first hormone (Figure 1.4a). Hormone secretion may also be regulated by metabolic processes. For instance, the pancreatic β-cell makes insulin in response to high ambient glucose. The effect is to lower glucose, which, in turn, inhibits further insulin production. The hypothalamic–anterior pituitary–end organ axes are a more complex extension of this model. The hypothalamic hormone [e.g. corticotrophin-releasing hormone (CRH)] stimulates release of anterior pituitary hormone (e.g. ACTH) to increase peripheral hormone production (e.g. cortisol), which then feeds back on the anterior pituitary and hypothalamus to reduce the original secretions. Figure 1.4b illustrates the anterior pituitary and end-organ components of this model.
Figure 1.3 The structures of vasopressin and oxytocin are remarkably similar, yet the physiological effects of the two hormones differ profoundly.
Vasopressin regulates water excretion
Cys – Tyr – Phe – Gln – Asn – Cys – Pro – Arg – Gly (NH2)
Cys – Tyr – IIe – Gln – Asn – Cys – Pro – Leu – Gly (NH2)
Oxytocin
S S
S S
8
83
3
uterine contraction
Table 1.2 (Continued )
Gland Hormone Molecular characteristics
Liver Insulin-like growth factor I (IGF-I) Protein
Ovary Oestrogens Steroid
Progesterone Steroid
Testis Testosterone Steroid
* The distinction between peptide and protein is somewhat arbitrary. Shorter than 50 amino acids is termed a peptide in this table. † The list is not exhaustive for the gastrointestinal tract and the pancreas (see Chapter 11).

12 / Chapter 1: Overview of endocrinology
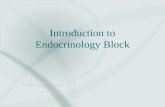
Figure 1.4 Two models of feedback regulating hormone synthesis. (a) The endocrine organ releases a hormone, which acts on the target tissue to stimulate a response. The response usually feeds back to inhibit ( – ) the endocrine organ to decrease further supply of the hormone. Occasionally, the feedback can act to enhance the hormone secretion ( + , positive feedback). (b) The endocrine organ
produces hormone 1, which acts on a second endocrine gland to release hormone 2. In turn, hormone 2 acts dually on the target tissue to induce a response and feeds back negatively onto the original endocrine organ to inhibit further release of hormone 1. This model is illustrative of the axes between the anterior pituitary and the peripheral end-organ targets.
Endocrineorgan
Target
tissue
Hormone Response
+
–
(a) (b)
Endocrineorgan
Target
endocrine
organ
Hormone 1
Response
–
Hormone 2
Target
tissue
Positive feedback
Under certain, more unusual, circumstances, hormone feedback enhances, rather than inhibits, the initial response. This is called positive feedback (an example is shown alongside the more usual negative feedback in Figure 1.4a). This is intrinsi-cally unstable. However, in some biological systems it can be transiently beneficial: for instance, the action of oestrogen on the pituitary gland to induce the ovulatory surge of LH and FSH (see Chapter 7); or during childbirth, stretch receptors in the distended vagina and nerves to the brain stimulate oxytocin release. This hormone causes the uterus to contract, further activating the stretch receptors to
establish positive feedback that is only terminated by delivery of the baby. The role of oxytocin in the suckling–milk ejection reflex is similar – a positive feedback loop that is only broken by cessation of the baby’s suckling.
Inhibitory control
The secretion of some hormones is under inhibitory as well as stimulatory control. Somatostatin, a hypothalamic hormone, prevents the secretion of GH, such that when somatostatin secretion is dim-inished, GH secretion is enhanced. Prolactin is similarly controlled, under tonic inhibition from dopamine.

Chapter 1: Overview of endocrinology / 13
Box 1.5 Endocrine cycles
Circadian = 24-h cycle• Circa = about, dies = day
Ultradian < 24-h cycle• E.g. GnRH release
Infradian > 24-h cycle• E.g. menstrual cycle
Endocrine rhythms
Many of the body’s activities show periodic or cyclical changes (Box 1.5). Control of these rhythms com-monly arises from the nervous system, e.g. the hypoth-alamus. Some appear independent of the environment, whereas others are coordinated and ‘entrained’ by external cues (e.g. the 24-h light/dark cycle that becomes temporarily disrupted in jetlag). Cortisol secretion is maximal between 0400h and 0800h as we awaken and minimal as we retire to bed. In contrast, GH and prolactin are secreted maximally ∼1 h after falling asleep. Clinically, this knowledge of endocrine rhythms is important as investigation must be refer-enced according to hour-by-hour and day-to-day vari-ability. Otherwise, such laboratory tests may be invalid or, indeed, misleading.
Endocrine disorders
The chapters in Part 2 largely focus on organ-specific endocrinology and associated endocrine disorders. Diabetes in Part 3, incorporating obesity, has now become its own specialized branch of endo-crinology. Nevertheless, it is possible to regard all endocrine abnormalities as disordered, too much or too little production of hormone. Some clinical fea-tures can occur because of compensatory over-production of hormones. For example, Addison disease is a deficiency of cortisol from the adrenal cortex (see Chapter 6), which reduces negative feed-back on ACTH production at the anterior pituitary. ACTH rises and stimulates melanocytes in the skin to increase pigmentation – a cardinal sign of Addison disease.
Imbalanced hormone production may occur when a particular enzyme is missing because of a
genetic defect. For example, in congenital adrenal hyperplasia, the lack of 21-hydroxylase causes failure to synthesize cortisol (see Chapter 6). Other pathways remain intact, leading to excess produc-tion of sex steroids that can masculinize aspects of the female body. Endocrine disorders may also arise from abnormalities in hormone receptors or down-stream signalling pathways. The commonest example is type 2 diabetes, which arises in part from resistance to insulin action in target tissues (see Chapter 13).
For those endocrine glands under regulation by the hypothalamus and anterior pituitary, disorders can also be categorized according to site. Disease in the end organ is termed ‘primary’. When the end organ is affected downstream of a problem in the anterior pituitary (either underactivity or overactiv-ity), it is secondary, while in tertiary disease, the pathology resides in the hypothalamus.
Like in other specialties, tumourigenesis impacts on clinical endocrinology. Most commonly, these tumours are sporadic and benign, but they may oversecrete hormones, and are described in the appropriate organ-specific chapters in Part 2. However, endocrine tumourigenesis may also form part of recognized multiorgan clinical syndromes. These are described in Chapter 10.
Key points
• Endocrinology is the study of hormones and forms one of the body’s major communication systems
• A hormone is a chemical messenger, commonly distributed via the circulation, that elicits specific effects by binding to a receptor on or inside target cells
• The three major types of hormones are peptides, and the derivatives of amino acids and cholesterol
• Negative and, occasionally, positive feedback, and cyclical mechanisms operate to regulate hormone production, commonly as part of complex multiorgan systems or axes
• Clinical endocrine disorders usually arise through too much, too little or disordered hormone production

14
Essential Endocrinology and Diabetes, Sixth Edition. Richard IG Holt, Neil A Hanley. © 2012 Richard IG Holt and Neil A Hanley. Publlished 2012 by Blackwell Publishing Ltd.
CHAPTER 2
Cell biology and hormone synthesis
Key topics
■ Chromosomes, mitosis and meiosis 15
■ Making a protein or peptide hormone 16
■ Making a hormone derived from amino acids or cholesterol 20
■ Hormone transport 24
■ Key points 26
Learning objectives
■ To appreciate the organization, structure and function of DNA
■ To understand mitosis and meiosis
■ To understand protein synthesis and peptide hormone production
■ To understand the function of enzymes and how enzyme cascades generate steroid and amino acid-derived hormones
This chapter aims to introduce some of the basic principles that are needed to understand later chapters