
Esophagectomy in aquired tof(tracheoesophageal fistula)
15
25 yrs old patient took sulphos accidentally 9 months back and developed stricture and tracheoesophageal fistula just above the Carina.He was treated with a covered self expanding metallic esophageal stent (SEMS).His pneumonia improved but fistula did not close and he started having disphagia (difficulty in swallowing).He was taken up for surgery. Esophagectomy stent removal & closure of tracheal defect and gastric pull up forming neo esophagus was done.
-
Upload
doctorarindamghosh -
Category
Healthcare
-
view
126 -
download
2
Transcript of Esophagectomy in aquired tof(tracheoesophageal fistula)

25 yrs old patient took sulphos accidentally 9 months back and developed stricture and tracheoesophageal fistula just above the Carina.He was treated with a covered self expanding metallic esophageal stent (SEMS).His pneumonia improved but fistula did not close and he started having disphagia (difficulty in swallowing).He was taken up for surgery. Esophagectomy stent removal & closure of tracheal defect and gastric pull up forming neo esophagus was done.
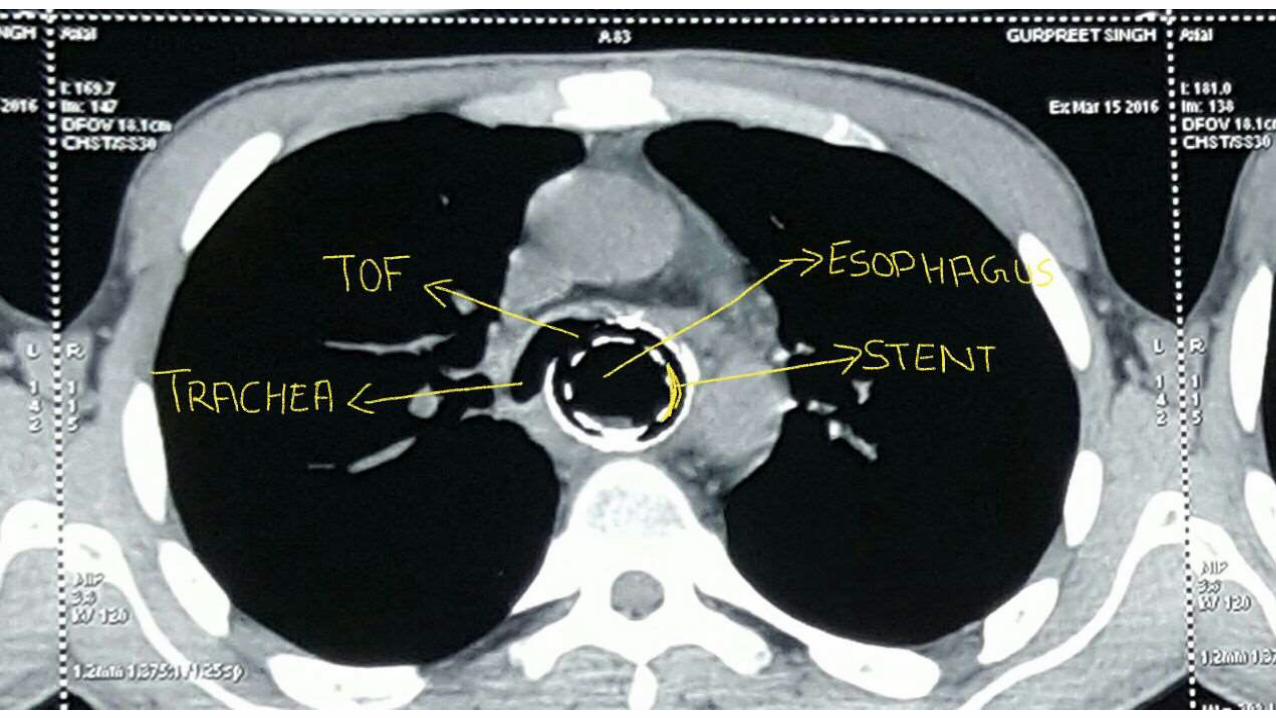

Tracheoesophageal fistula with stent in situ

• Stomach mobilized on right gastro epiploic vessels. Complete Kocherisation done along with pyloric dilatation to pull the stomach tube at the apex of chest.



• Mediastinal dissection close to the esophagus to mobilize it below the fistula


• SELF EXPANDING METALLIC STENT(SEMS)
• FULLY COVERED 12CM LONG.

• Esophagotomy done to Lay open the fistula site.

• Suture(4/0 pds double arm )taken around the fistula on the tracheal ring and on the anterior esophageal flap.
• Double lumen endotracheal tube going to left bronchus.
• Tracheal baloon at the Carina is presenting.

• Fistula closed in two layers over Tachosil Patch.
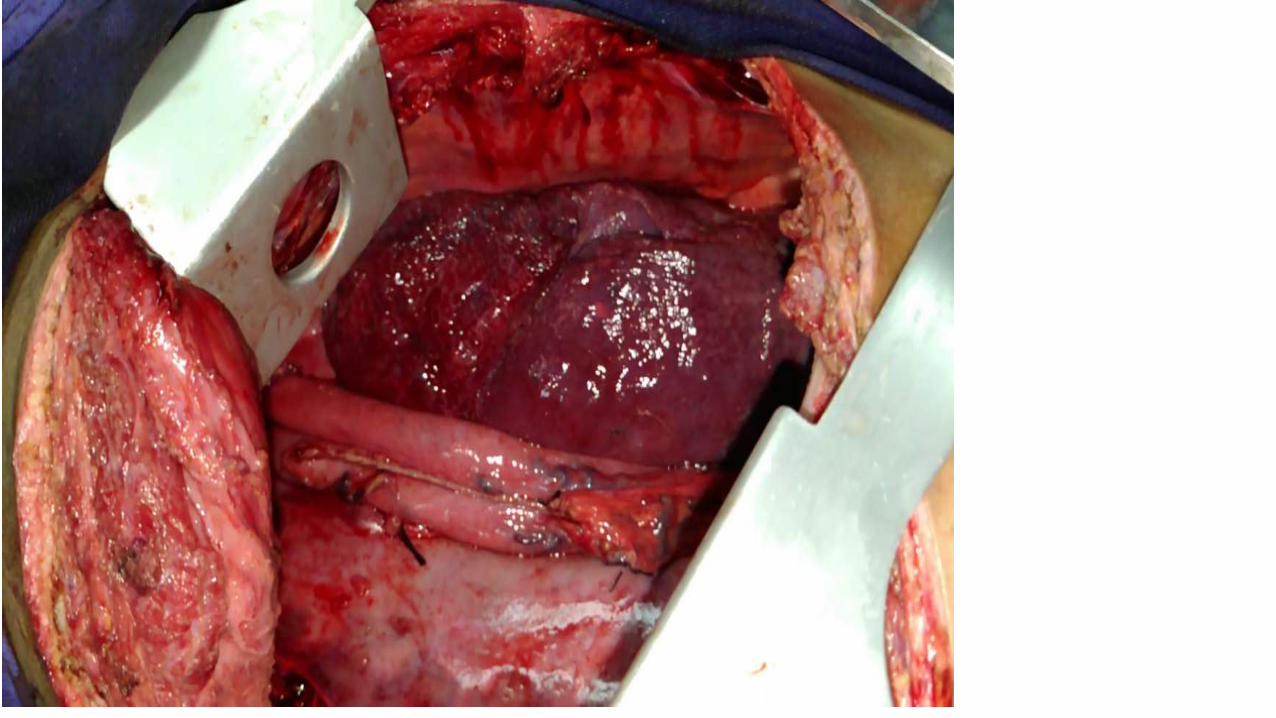

• Stomach tube taken in the chest and anastomosed with the esophagus at the apex of chest.



















