Ern Mrcs Bk1

of 21
Transcript of Ern Mrcs Bk1
-
7/28/2019 Ern Mrcs Bk1
1/21
Essential Revision Notes
for Intercollegiate MRCS
Book 1
-
7/28/2019 Ern Mrcs Bk1
2/21
Contents
Acknowledgements vi
Preface vii
Contributors viii
Introduction x
CHAPTER
1. Basic surgical knowledge and skills 1Claire Ritchie Chalmers
2. Infection and inflammation 89Catherine Sargent and Claire Ritchie Chalmers
3. Neoplasia 193Amer Aldouri and Claire Ritchie Chalmers
4. Haematology 265
Sheila Fraser and Claire Ritchie Chalmers5. Trauma 329
Claire Ritchie Chalmers
6. Peri-operative care 437Sally Nicholson and Catherine Parchment Smith
7. Critical care 577Sam Andrews and Claire Ritchie Chalmers
8. Surgical outcomes, research, ethics and the law 753Shireen MacKenzie and Nerys Forester
9. Vascular surgery 801Sam Andrews and Nerys Forester
10. Paediatric surgery 897Susan Picton and David Crabbe
11. Urology and transplantation 973Sunjay Jain and Kilian Mellon
Abbreviations 1113
Picture permissions 1119
Bibliography 1121
Index 1124
-
7/28/2019 Ern Mrcs Bk1
3/21
1 Physiology of wound healing
1.1 Skin anatomy and physiology1.2 Pathophysiology of wound healing1.3 Healing in specialised tissues1.4 Delayed wound healing1.5 Wound dehiscence and incisional
hernias
2 Creation and care of the surgicalwound
2.1 Classification of wounds2.2 Incisions and closures
2.3 Needles and sutures2.4 Surgical drains2.5 Dressings2.6 Scars and contractures
3 Basic surgical techniques
3.1 Anastomosis3.2 Biopsy3.3 Basic plastic surgery3.4 Abscess drainage3.5 Minimal access surgery
4 Tumours and lesions of the skin andsubcutaneous tissues
4.1 Benign skin lesions4.2 Excision of benign skin lesions4.3 Curettage and cryosurgery
4.4 Pre-malignant skin lesions4.5 Basal cell carcinoma4.6 Squamous cell carcinoma4.7 Malignant melanoma
Claire Ritchie Chalmers
Physiology of wound healing
1
Chapter 1
Basic Surgical Knowledgeand Skills
-
7/28/2019 Ern Mrcs Bk1
4/21
Basic Surgical Knowledge and Skills
2
-
7/28/2019 Ern Mrcs Bk1
5/21
Section 1
Physiology of wound healing1.1 SKIN ANATOMY AND PHYSIOLOGY
All skin has the same basic structure, although it varies in thickness, colour and the pres-ence of hairs and glands in different regions of the body. The external surface of the skinconsists of a keratinised squamous epithelium called the epidermis. The epidermis issupported and nourished by a thick underlying layer of dense, fibroelastic connectivetissue called the dermis which is highly vascular and contains many sensory receptors. Thedermis is attached to underlying tissues by a layer of loose connective tissue called the
hypodermis or subcutaneous layer which contains adipose tissue. Hair follicles, sweatglands, sebaceous glands and nails are epithelial structures called epidermal appendagesthat extend down into the dermis and hypodermis.
Physiology of wound healing
3
In a nutshell
A core knowledge of skin anatomy and physiology is essential to understand fullythe processes involved in wound healing.
The skin is an enormously complex organ acting both as a highly efficient mechani-cal barrier and also as a complex immunological membrane. It is constantly regen-erating with a generous nervous, vascular and lymphatic supply, and has specialiststructural and functional properties in different parts of the body.
The four main functions of the skin: Protection: against UV light, and mechanical, chemical and thermal insults; it also
prevents excessive dehydration and acts as a physical barrier to micro-organisms Sensation: various receptors for touch, pressure, pain and temperature Thermoregulation: insulation, sweating and varying blood flow in dermis Metabolism: subcutaneous fat is a major store of energy, mainly triglycerides;
vitamin D synthesis occurs in the epidermis
-
7/28/2019 Ern Mrcs Bk1
6/21
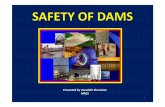
Skin has natural tension lines, and incisions placed along these lines tend to heal with anarrower and stronger scar, leading to a more favourable cosmetic result (see Fig. 1.1b).These natural tension lines lie at right angles to the direction of contraction of underlyingmuscle fibres, and parallel to the dermal collagen bundles. On the head and neck they arereadily identifiable as the wrinkle lines, and can easily be exaggerated by smiling, frown-ing and the display of other emotions. On the limbs and trunk they tend to run circumfer-entially, and can easily be found by manipulating the skin to find the natural skin creases.Near flexures these lines are parallel to the skin crease.
Basic Surgical Knowledge and Skills
4
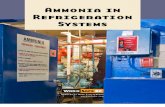
Sebaceous
gland
Hair
follicle
Hair bulb Hypodermis
Merocrine
sweat gland
Arrector
pili
Dermis
Epidermis
Dermal
papillae
Figure 1.1a Skin anatomy
-
7/28/2019 Ern Mrcs Bk1
7/21
1.2 PATHOPHYSIOLOGY OF WOUND HEALING
Physiology of wound healing
5
Figure 1.1b Langers lines. The lines correspond to relaxed skin and indicate optimalorientation of skin incisions to avoid tension across the healing wound
In a nutshell
Wound healing consists of three phases: Acute inflammatory phase (see Chapter 2 Infection and Inflammation) Proliferative phase (cell proliferation and deposition of extracellular matrix,
ECM) Maturation phase (remodelling of the ECM)
Different tissues may undergo specialised methods of repair (eg organ parenchyma,bone and nervous tissue).
-
7/28/2019 Ern Mrcs Bk1
8/21
Basic Surgical Knowledge and Skills
6
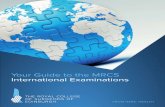
Tissue injury
Complement activationPlatelet activationClot formation
EpithelialisationAngiogenesisCollagen synthesis
ACUTE INFLAMMATORY PHASE
PROLIFERATION PHASE
Increased vascular permeabilityVasodilatation
Endothelial cellsFibroblasts
Keratinocytes
Influx of inflammatory cells of fibroblasts
Release of cytokines and growth factors
Extracellular matrix production
MATURATION PHASE
Healed wound
Matrix remodelling
Figure 1.2a Wound healing
-
7/28/2019 Ern Mrcs Bk1
9/21
All surgeons deal with wounds and it is essential to understand fully the exact pathophysi-ological mechanisms involved in wound healing, how this may be optimised, and how itmay be compromised, leading to wound dehiscence, delayed healing and incisionalhernia formation.
The aims of wound healing are a rapid restoration of tissue continuity and a rapid return tonormal function.
The inflammatory phase
Tissue damage starts a typical acute inflammatory reaction by damage to cells and bloodvessels.
The acute inflammatory response is generic to all forms of injury and noxious insult. It isdiscussed in detail in Chapter 2 Infection and Inflammation.
The proliferative phase
The proliferative phase is characterised by migration and proliferation of a number ofcell types:
Epithelial cells: within hours of injury epithelial cells at the margins of the wound
begin to proliferate and migrate across the defect; epithelial closure is usuallycomplete by 48 hours
Fibroblasts: fibroblasts migrate into the wound, proliferate and synthesise extracellularmatrix (ECM) components including collagen and ground substance (45 days)
Endothelial cells: the development of new blood vessels (angiogenesis) occurs simulta-neously with activation of fibroblasts proliferation and migration of endothelial cellsdepend on the proteolytic activity of matrix metalloproteinases (for which zinc is anessential cofactor)
Physiology of wound healing
7
The inflammatory phase of wound healing involves: Vasodilation and increased vascular permeability Influx of inflammatory cells (neutrophils) and fibroblasts Platelet activation and initiation of the coagulation and complement cascades,
leading to clot formation and haemostasis
-
7/28/2019 Ern Mrcs Bk1
10/21
Granulation tissue is a temporary structure which forms at this stage. It consists of a rich
network of capillary vessels and a heterogeneous population of cells (fibroblasts, macrophagesand endothelial cells) within the stroma of the ECM. It has a characteristic pinkish, granularappearance. Additionally the wound contracts due to the action of myofibroblasts.
The maturation phase
Matrix remodelling
This stage lasts for many months after the wound is clinically healed The scar becomes less vascular hence the change in colour The scar tensile strength increases due to modifications made to collagen. The
collagen molecule is a triple -helix. Multiple molecules orientate to form a fibril.The cross-linkage of collagen fibrils by formation of covalent bonds (aided by theaction of vitamin C) increase the tensile strength of the scar
Basic Surgical Knowledge and Skills
8
Cell types involved in wound healing and time of appearance in wound
Platelets Immediate
Neutrophils 01 day
Macrophages 12 days
Fibroblasts 24 days
Myofibroblasts 24 days
Endothelial cells 35 days
PROLIFERATIVE PHASE
Covers epithelial
defect
GRANULATION
TISSUE
Angiogenesis
and new vessel
development
Synthesis of components
of the extracellular matrix
(ECM) eg collagen
Epithelial cell
migration
Fibroblast
migration
Macrophage
migration
Endothelial
cell migration
Figure 1.2b The proliferative phase
-
7/28/2019 Ern Mrcs Bk1
11/21
Regaining strength in the wound
During matrix remodelling the scar regains its strength. The tissue types and thicknessinvolved in the scar will determine the length of time to regain strength. Bowel and muscleregains virtually full strength within 1 month and skin takes up to 6 months. Strength tends
to increase very quickly over the first 710 days although full maturation of a scar can takeup to 1218 months. Choice of wound closure materials should reflect this. Abdominalincisions through muscle layers will take many weeks to regain their strength, achievingsufficient strength at 34 months to no longer require suture support and about 80% oftheir former strength after many months. Closure is therefore performed either with loopnylon that will persist in the wound, or a strong, slowly absorbing suture material such asPDS that will support the wound. Superficial skin wounds require minimal support and socan be closed with a quickly absorbable suture material or by interrupted sutures or staplesthat can be removed within days.
1.3 HEALING IN SPECIALISED TISSUES
Classification of wound healing
First (primary) intention
This typically occurs in uncontaminated wounds with minimal tissue loss and when thewound edges can easily be approximated with sutures, staples or adhesive strips, without
Physiology of wound healing
9
In a nutshell
Wound healing can be classified into: First (primary) intention Second (secondary) intention Third (tertiary) intention
In addition different tissues have different healing properties. You should be aware
of the healing properties of:SkinBoneNerveBowelSolid organs (liver, kidney, spleen, heart)Non-regenerative organs (eg eye)
-
7/28/2019 Ern Mrcs Bk1
12/21
excessive tension. The wound usually heals by rapid epithelialisation and formation ofminimal granulation tissue and subsequent scar tissue.
Second (secondary) intention
Usually secondary intention occurs in wounds with substantial tissue loss, when the edgescannot be apposed without excessive tension. The wound is left open and allowed to healfrom the deep aspects of the wound by a combination of granulation, epithelialisation andcontraction. This inevitably takes longer, and is accompanied by a much more intenseinflammatory response. Scar quality and cosmetic result are poor.
Wounds which may be left to heal by secondary intention:
Extensive loss of epithelium
Extensive contamination Extensive tissue damage Extensive oedema leading to inability to close Wound reopened (eg infection, failure of knot)
Third (tertiary) intention
The wound is closed several days after its formation. This may well follow a period ofhealing by secondary intention, for example when infection is under control or tissue
oedema is reduced.
Healing in different tissues
Different tissues heal in a remarkably similar way, albeit at different rates the scalp and faceheal very quickly, at least in part because of increased vascularity. Healing rates are quickestearly in life, and decline with advancing years. Surgery performed on the fetus in utero leavesno scarring at all as it occurs by regeneration. Some tissues possess the ability to regenerate
their specialised cells following injury, with the result that significant tissue loss can bereplaced by regenerated specialised cells, with no or minimal loss of function (eg bone,intestine). Conversely, some tissues have little regenerative ability (eg cardiac tissue) andwounds heal by simple scar formation significant tissue loss will result in significant loss offunction. Nervous tissue possesses very limited regenerative capacity and partial functionmay be regained through slow neuronal growth in peripheral nerve injuries.
Skin
Skin consists of two layers the keratinised stratified epidermis and the connective tissue ofthe dermis. Following injury to the skin, healing essentially follows the pattern outlinedabove. Blood lost into the wound clots into a fibrin meshwork (the scab). Inflammatory cells,fibroblasts and capillaries invade the clot to form a contractile granulation tissue that drawsthe wound margins together. Neutrophils release cytokines and growth factors that activatefibroblasts and keratinocytes, which alter their anchorage to the surrounding cells, ECM and
Basic Surgical Knowledge and Skills
10
-
7/28/2019 Ern Mrcs Bk1
13/21
basal lamina. Protease secretion by the keratinocytes allows them to migrate through thefibrin mesh of the clot and the cut epidermal edges to move forward to cover the denudedwound surface. A new stratified epidermis with underlying basal lamina is then re-estab-lished. Epidermal appendages (eg sweat glands and hair follicles) do not regenerate.
Bone and callus
Bone is unique in its ability to repair itself as it re-activates processes that normally occurduring embryogenesis.
Primary bone healing
This occurs when the fracture gap is small (12 mm) and when there is absolute stability
between the fracture fragments. Bone remodelling units cross the small gap and Haversianremodelling occurs (without callus formation); this type of bone healing is seen when therehas been an anatomical reduction and stable internal fixation of the fracture (an intactblood supply is required).
Secondary bone healing
Haematoma formation
Formed by rupture of blood vessels within medullary cavity
Haematoma fills the fracture gap and spills out into the surrounding tissue Haematoma provides a fibrin mesh that seals off the fracture site and provides a
framework for the influx of inflammatory cells, fibroblasts, and capillary vessels
Inflammatory phase
Necrotic material at the fracture site releases inflammatory mediators, promotingchemotaxis of neutrophils
Inflammatory cells release cytokines (eg TGF- and fibroblast growth factor which
activate osteoprogenitor cells)
Repair phase
By the end of the 1st week the organised haematoma is being replaced by soft callus(it provides some anchorage but no structural rigidity)
Soft callus gradually changes from fibrinous matrix, through a cartilaginous phase,to bony callus (resembles embryonic endochondral ossification and is similar toprocess occurring at the physis)
Around the periphery, under the periosteum, osteoblasts deposit a layer of wovenbone the hard callus (process resembles embryonic intra-membranous ossification) So the fracture ends are bridged by a bony callus that gains strength as it mineralises
(giving the fracture increasing stability, and allowing early weight-bearing)
Physiology of wound healing
11
-
7/28/2019 Ern Mrcs Bk1
14/21
Remodelling phase
Remodelling occurs over the months and years following a fracture Callus and new bone (formed initially) is bulky and relatively disordered; it is
replaced with lamellar bone through Haversian remodelling
Internal architecture of any bone alters in response to loads placed on it (the sameholds true at the fracture site); this phenomenon is known as Wolffs law
Factors that impede fracture healing
Infection Diabetes mellitus Vascular insufficiency Calcium, phosphate, or vitamin D deficiency Displaced and comminuted fractures:
Large areas of periosteal stripping result in large volume of devitalised bone Devitalised bone is gradually revascularised or resorbed Increased volume of callus is produced and increases the process of remodelling
Inadequate immobilisation Normal constituents of callus dont form if there is constant significant move-
ment of the fracture site Callus mainly consists of fibrous tissue and cartilage, perpetuating instability,
resulting in delayed union and non-union Drugs: steroids and possibly NSAIDs delay fracture healing
Basic Surgical Knowledge and Skills
12
Times for healing of nerves, tendons and bone (general guide)
Tendon repair 35 weeks to protected mobilisation 612 weeks to full mobilisation > 12 weeks to full strength
Nerve repair 46 weeks of cast immobilisation of neighbouring joints > 6 weeks to free mobilisation
Fracture of upper limb 34 weeks in a cast (mobilise rest of limb)
Fracture of lower limb 68 weeks in a cast Protected weight-bearing from 34 weeks if the cast is a stable fracture May take 1216 weeks for full unprotected weight-bearing
-
7/28/2019 Ern Mrcs Bk1
15/21
Nerve injury and repair
There are many variations of nerve injury. A common classification was described bySeddon, dividing injuries into three groups: neuropraxia, axonotmesis, and neurotmesis.Sunderlands classification expands the category of neurotmesis and refers to categories ofincreasing severity.
Neuropraxia (I)
This is the mildest form of nerve injury, referring to a crush, contusion or stretching injuryof the nerve without disruption of its axonal continuity. There is a reduction or block inconduction of the impulse down a segment of the nerve fibre. This may be caused by localbiochemical abnormalities. There is a temporary loss of function which is reversible within
hours to months of the injury (average 68 weeks). Motor function often suffers greaterimpairment than sensory function, and autonomic function is often retained.
Axonotmesis (II)
This is the loss of the relative continuity of the axon and its covering of myelin with preser-vation of the connective tissue framework of the nerve (epineurium and perineurium). It isa more serious injury than neuropraxia. Wallerian degeneration occurs and there is adegree of retrograde proximal degeneration of the remaining axon. Recovery occurs
through regeneration of the axons (which grow along the existing preserved framework ofthe nerve). Regeneration requires time and may take weeks or months, depending on thesize of the lesion. The proximal end of the lesion grows distally (23 mm per day) and thedistal end of the lesion grows proximally (1 mm per day).
Physiology of wound healing
13
In a nutshell
In order of increasing degree of injury: Neuropraxia (I): no axonal disruption Axonotmesis (II): axonal disruption/supportive tissue framework preserved Neurotmesis (IIIV): supportive tissue framework disrupted
Principles of surgical repair of nerves: Accurate apposition of nerve ends Healthy surrounding tissue No tension Minimal dissection
-
7/28/2019 Ern Mrcs Bk1
16/21
Neurotmesis (III, IV and V)
This is the loss of continuity of both axons and nerve structural connective tissue. It rangesin severity, with the most extreme degree of neurotmesis being transection. Most neurot-metic injuries do not produce gross loss of continuity of the nerve but rather internaldisruption of the architecture of the nerve sufficient to involve perineurium andendoneurium as well as the axons and their myelin sheath. There is a complete loss ofmotor, sensory and autonomic function. If the nerve has been completely divided, axonalregeneration causes a neuroma to form in the proximal stump.
In grade III injuries, axonal continuity is disrupted by loss of endoneurial tubes (theneurolemmal sheaths) but the perineurium is preserved. This causes intra-neural scarringand regenerating axons may re-enter the sheaths incorrectly.
In grade IV injuries, nerve fasciculi (axon, endoneurium, perineurium) are damaged, butnerve sheath continuity is preserved.
In grade V injuries, the endoneurium, perineurium, and epineurium, which make up theentire nerve trunk, are completely transected. This may be associated with perineuralhaematoma or displacement of the nerve ends.
Bowel
The layers of the bowel involved in the anastomosis heal at different rates. Optimal healingrequires good surgical technique and apposition of the layers.
The intestinal mucosa is a sheet of epithelial cells that undergoes rapid turnover and prolif-eration. It may sustain injury as a result of trauma (from luminal contents or surgery),chemicals (eg bile), ischaemia or infection. Injury to the mucosa resulting in breaches ofthe epithelial layer is though to render patients susceptible to bacterial translocation andsystemic sepsis syndromes. Minor disruption to the mucosa is thought to be repaired by a
process separate to proliferation called restitution, instigated by cytokines and growthfactors and regulated by the interaction of cellular integrins with the ECM. After uncompli-cated surgery to the GI tract, mucosal integrity is thought to have occurred by 24 hours.
The other muscular layers of the bowel undergo the general phases of inflammation, prolif-eration and maturation as outlined above. Anastomotic healing results in the formation ofcollagenous scar tissue. Scarring may eventually contract resulting in stenosis.
Solid organs
Solid organs either heal by regeneration (through a process of cell proliferation) or by hyper-trophy of existing cells. Some organs heal by a combination of the two processes. In organsin which the cells are terminally differentiated, healing occurs by scarring or fibrosis.
Basic Surgical Knowledge and Skills
14
-
7/28/2019 Ern Mrcs Bk1
17/21
Liver
The liver has remarkable regenerative capacity. The stimulation for regeneration is reductionin the liver mass to body mass ratio (eg surgical resection) or the loss of liver functionalcapacity (eg hepatocyte necrosis by toxins or viruses). Regeneration is achieved by prolifera-tion of all the components of the mature organ hepatocytes, biliary epithelial cells, fenes-trated epithelial cells and Kupffer cells. Hepatocytes, which are normally quiescent andrarely divide, start to proliferate to restore hepatic mass and function. This occurs initially inthe areas surrounding the portal triads and then extends to the pericentral areas after 48hours. After 70% hepatectomy in animal models, the remaining hepatocytes divide once ortwice and then return to quiescence. About 24 hours after the hepatocytes start to prolifer-ate, so do all the other cell types and ECM is produced, including the structural protein,laminin. Eventually the cell types re-structure into functional lobules over 710 days. The
stimulus for hepatocyte proliferation is thought to be TNF and the IL-6 family of cytokines.Subsequently HGF and TGF- are responsible for continued cell growth. Regeneration isterminated after about 72 hours by the action of cytokines such as TGF-1.
Kidney
The cells of the kidney are highly specialised, reflecting their terminal state of differentia-tion. Healing in the kidney predominantly occurs by scarring and fibrosis.
Spleen
Splenic regeneration is controversial. Increases in size and weight of the residual splenictissue have been recognised after partial splenectomy (eg for trauma) and, hypertrophy ofmissed splenunculi after splenectomy for haematological and glycogen storage diseases(eg Gauchers) may also occur. However, there is little evidence that this increase in size ofthe residual splenic tissue results in functional regeneration and the increase in size maybe due to infiltration of the tissue with cells characteristic of the underlying haematologicalor other disorder.
Heart and lung
Cardiac tissue is commonly damaged by ischaemia and occasionally by trauma. Theinflammatory response is particularly important in the healing of cardiac tissue and is insti-gated by release of cytokines such as tumour necrosis factor-alpha (TNF- or interleukin-6(IL-6) from the damaged myocardium. These cytokines have been implicated in the regula-tion of myocyte survival or apoptosis, myocyte hypertrophy, defects in myocyte contractil-
ity, proliferation of myofibroblasts and angiogenesis/vasculogenesis and, to a limitedextent, progenitor cell proliferation. The cytokine response lasts about a week and theinfarcted myocardium is gradually replaced by scar tissue. Within this scar tissue there is adegree of regeneration of myocytes and blood vessels and current research is focused onfacilitating this process for an improvement in myocardial function post infarct.
Physiology of wound healing
15
-
7/28/2019 Ern Mrcs Bk1
18/21
Non-regenerative tissues
Non-regenerative tissues, such as the cornea of the eye, heal by collagen deposition andscarring. This is obviously accompanied by complete loss of function.
1.4 DELAYED WOUND HEALING
Factors affecting wound healing
Local risk factors
Wound infection Haematoma Excessive mobility Foreign body Dead tissue Dirty wound Surgical technique Ischaemia
Acute; damage to blood supply; sutures too tight Chronic; previous irradiation Diabetes Atherosclerosis Venous disease
Basic Surgical Knowledge and Skills
16
In a nutshell
Wound healing is affected by:
Local factors (factors specific to the wound)Wound classificationSurgical skill
General factors (factors specific to the patient)Concomitant diseaseNutrition
-
7/28/2019 Ern Mrcs Bk1
19/21
General risk factors
Elderly Cardiac disease Respiratory disease
Anaemia Obesity Renal (uraemia) or hepatic failure (jaundice) Diabetes mellitus Malnutrition (vitamins and minerals) Malignancy Irradiation Steroid or cytotoxic drugs Other immunosuppressive disease or drugs
Nutritional factors Proteins are essential for ECM formation and effective immune response Vitamin A is required for epithelial cell proliferation and differentiation Vitamin B6 is required for collagen cross-linking Vitamin C is necessary for hydroxylation of proline and lysine residues. Without
hydroxyproline, newly synthesised collagen is not transported out of fibroblasts; inthe absence of hydroxylysine, collagen fibrils are not cross-linked
Zinc is an essential trace element required for RNA and DNA synthesis and for thefunction of some 200 metalloenzymes
Copper plays a role in the cross-linking of collagen and elastin
Optimising wound healing
Wound failure may be minimised by attention to the risk factors listed above. Ensure gooddelivery of blood and oxygen to the wound (and be aware of the importance of good
hydration and respiratory function). Debride devitalised tissues and handle other tissueswith care to prevent tissue necrosis. Sutures that are tied very tightly will cause tissuehypoxia. Avoid tension on the wound. Careful aseptic technique should be used. Heavilycontaminated wounds or the abdominal cavity should be washed with copious amounts ofwarmed saline until clean. Patient nutrition is also very important and critically ill patientsmay require support either via NG feeding or parenteral nutrition.
On occasions the patient may be in such a poor condition (eg be elderly, have septicshock, be on steroids) and the circumstances of the operation so hostile (emergency, faecal
contamination, disseminated malignancy) that the chance of good wound healing is verylow. Under these circumstances, there are various surgical options:
Bring out a stoma rather than perform a primary bowel anastomosis Leave the skin and subcutaneous fat open in a heavily contaminated abdomen for
delayed primary closure this wound can then be packed as required (be awarethat changing dressings on large wounds may require return visits to theatre)
Physiology of wound healing
17
-
7/28/2019 Ern Mrcs Bk1
20/21
Close the wound with additional deep tension sutures The abdominal wall itself may be left open (a laparostomy) or partially closed with
an artificial mesh to reduce intra-abdominal pressure after surgery for intra-abdomi-nal catastrophe and prevent abdominal compartment syndrome
1.5 WOUND DEHISCENCE AND INCISIONALHERNIAS
Wound dehiscence is the partial or total disruption of any or all layers of the operative
wound. Risk factors for wound dehiscence are the same as those for factors affectingwound healing
Evisceration (burst abdomen) is rupture of all layers of the abdominal wall and extru-sion of the abdominal viscera (usually preceded by the appearance of blood-stainedfluid the pink-fluid sign)
Wound dehiscence without evisceration should be repaired by immediate electivere-closure. Dehiscence of a laparotomy wound with evisceration is a surgical emer-gency with a mortality rate of > 25%. Management involves resuscitation, reassur-
ance, analgesia, protection of the organs with moist sterile towels, and immediatereoperation and closure (usually with deep tension sutures)
Incisional hernias are still common despite modern suture materials. They occur at sites ofpartial wound failure or dehiscence. Risk factors for incisional hernia are therefore thesame as those for dehiscence. Symptoms include visible protrusion of the hernia duringepisodes of raised intra-abdominal pressure and discomfort. Incisional hernias usuallycorrespond to a wide defect in the abdominal wall and so do not often incarcerate.Treatment depends on symptoms and size of defect (eg. conservative measures including a
truss/corset and surgical repair). Further details on incisional hernias and methods of repairare covered in theAbdomen chapter of Book 2.
Basic Surgical Knowledge and Skills
18
In a nutshell
The same risk factors predispose to: Failure of wound healing Wound dehiscence Incisional herniation
-
7/28/2019 Ern Mrcs Bk1
21/21
Section 2
Creation and care of thesurgical wound
2.1 CLASSIFICATION OF WOUNDS
Depth of wound
Superficial wounds
Superficial wounds involve only the epidermis and dermis and heal without formation ofgranulation tissue and true scar formation. Epithelial cells (including those from any resid-ual skin appendages such as sweat or sebaceous glands and hair follicles) proliferate and
migrate across the remaining dermal collagen.
Examples:
Superficial burn Graze Split skin graft donor site
Deep wounds
Deep wounds involve layers deep to the dermis and heal with the migration of fibroblastsfrom perivascular tissue and formation of granulation tissue and subsequent true scarformation. If a deep wound is not closed with good tissue approximation, it heals by acombination of contraction and epithelialisation, which may lead to problematic contrac-tures, especially if over a joint.
Creation and care of the surgical wound
In a nutshell
Wounds can be classified in terms of: Depth: superficial vs deep Mechanism: incised, lacerated, abrasion, degloved, burn Contamination or cleanliness: clean, clean contaminated, contaminated, dirty