ENHANCING PATIENT OUTCOMES AFTER STROKE: ACUTE CARE AND BEYOND · 2016-02-16 · ENHANCING PATIENT...
94
ENHANCING PATIENT OUTCOMES AFTER STROKE: ACUTE CARE AND BEYOND Combined Sections Meeting 2017, San Antonio, TX February 16, 2016 Presenters: Allison Lieberman PT, MSPT, GCS Gina Dubuisson PT JFK Medical Center- Johnson Rehabilitation Institute, Edison NJ
Transcript of ENHANCING PATIENT OUTCOMES AFTER STROKE: ACUTE CARE AND BEYOND · 2016-02-16 · ENHANCING PATIENT...

ENHANCING PATIENT
OUTCOMES AFTER STROKE:
ACUTE CARE AND BEYOND
Combined Sections Meeting 2017, San Antonio, TX
February 16, 2016
Presenters:
Allison Lieberman PT, MSPT, GCS
Gina Dubuisson PT
JFK Medical Center- Johnson Rehabilitation Institute,
Edison NJ

Learning Objectives
1. Identify guidelines and best practices for comprehensive stroke care in the Acute Care setting.
2. Identify Physical Therapy functional outcomes appropriate for use in the Acute Care setting for patients post stroke.
3. List evidence-based practices in the Acute Care setting that may improve patient outcomes and prevent secondary complications for patients following stroke.
4. Describe the benefits of coordinate stroke care and recall process improvement strategies that will assist clinicians in better managing patients after stroke across the continuum of care.

Disclosure
The speakers do not present with any
conflicts of interest in regards to the
content of the presentation and have
no relevant financial relationships to
disclose.

Stroke Statistics
• Leading cause of disability and one of the highest causes of death in the US1
• Recent decline from 4th to 5th leading cause of death in US; 2nd worldwide2
• Almost 800,000 individuals in the US suffer a stroke annually and 600,000 of them experience life long disability3,4
• In 2010, the worldwide prevalence of stroke was 33 million, with 16.9 million having a first stroke3

Stroke Statistics After tPA5
• Mortality from stroke has declined since the use of intravenous tissue plasminogen activator (tPA) and improvements in multidisciplinary inpatient stroke care

Rates of Disability After Stroke
• 25-74% of the 50 million stroke survivors worldwide are fully or partially dependent in ADLs and mobility5,6
• 40% of stroke survivors are left with moderate functional impairments and 15-30% experience severe disability1,7
• Early rehabilitaion in the first month after stroke leads to better recovery of body function and reduced disability8

Stroke Statistics9
• Recurrent stroke is frequent- 25% of people who have a CVA will experience a second CVA within 5 years
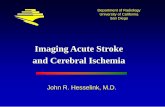
• The country's highest death rates from stroke are in the southeastern United States

Stroke Mortality Rates10

Demographic Differences
• 5th leading cause of death for Americans, but the risk varies with race and ethnicity9
– The risk of having a first stroke is nearly twice as high for blacks than for whites; blacks are more likely to die following a stroke than are whites
– Rate of strokes in the Hispanic population falls between the rate of strokes for whites and blacks
– American Indians, Alaska Natives and blacks are more likely to have had a stroke than other groups11
• In 2009, 34% of people hospitalized for stroke were younger than 65 years12

Costs and Statistics
• Annual economic burden of stroke care is 34 billion dollars; this includes direct expenses and indirect costs9
• According to 2010, CDC data, the average length of stay in the hospital for a patient post-stroke is 6.1 days13

Stroke Awareness
• In a 2005 survey, most respondents recognized sudden numbness on one side as a symptom of stroke– Only 38% were aware of all major symptoms of stroke
and knew to call 9-1-1 when someone was having a stroke14
• Patients who arrive at the emergency room within 3 hours of their first symptoms tend to have less disability 3 months after a stroke than those who received delayed care15

Stroke Research6
• An increase in stroke research over the last decade may be responsible for the decade-long decline in stroke incidence and mortality
• There are not many clinical trial or randomized control trials (RCTs) in the US
• Largest area of growth in research has been in the specialty of Physical Medicine and Rehabilitation

Northeast Cerebrovascular Consortium16
• An independent organization established in 2006• Comprised of 8 states in the Northeastern US• Develops recommendations based on the Stroke
Systems of Care Model to:– Improve care and decrease disparity– Improve collaboration and coordination – Share best practices
• Focus on stroke prevention and community education– EMS notification and response– Acute and subacute treatment and rehabilitation

• Helsingborg Declaration on stroke management recommendations:– Patient rehab needs should be assessed by a
multidisciplinary team– Early rehabilitation within first few days after stroke and
the creation of patient-centered rehab goals– Dedicated stroke units/beds – An understanding of the role of each team member– Cardiovascular conditioning– Continuum of care with stroke team on discharge and the
use of community stroke liaisons– Long term follow-up to allow easy referral to rehab if
functional changes are noted– Caregiver education
Helsingborg Declaration 200617,18

Rehabilitation Recommendations19
• Severity of stroke is the biggest predictor of outcome
• Age negatively impact outcomes
• Patients need to be able to learn and tolerate therapy to benefit from acute inpatient stroke rehabilitation
• Patients with moderately to severe deficits benefit most from comprehensive inpatient specialized rehabilitation settings
• Treatment on an organized inpatient stroke unit:
– Increases survival rates, possibility of returning home, possibility of achieving independence
– Decreases chance of medical complications
• Early admission to rehab as soon as medically stable is also associated with improved patient outcomes up to 1 year

Level of Evidence for Stroke Care20
• Level 1a evidence that patients treated on a multidisciplinary inpatient stroke unit have decreased:
– Death, dependency, need for institutionalization
– Length of stay
• Care on acute rehabilitation stroke units are associated with improved functional outcomes

Evidence for Efficiency of Stroke Care
• Very few studies have considered the cost of care provided by family, loss of income, long-term disability and general societal burden related to stroke
• Costs were not significantly lower for home-based versus in-patient therapy21,22
– Multiple regression analysis showed that the cost of a home-based program was related to level of disability after adjustment for age, comorbidity and presence/absence of a care-giver
• For patients with severe deficits, the initial cost may be greater for acute/subacute stroke specific programs, but there is reduced death and mortality versus home-based programs20

Efficiency of Stroke Care23
• Large percent of costs are for incidental/informal costs (ie caregiver cost/time)
– Long-term disability and complication costs are a burden on our health care system
• Study in the UK on stroke care cost reported:
– 49% of costs were direct, 24% were indirect and 27% were informal
• Healthcare dollars are best if used on:
– Primary prevention and treatment of vascular risk factors related to stroke
– Admission of patients to multidisciplinary, stroke units
– Adherence to stroke guidelines for patients in the acute phase of stroke
– Early rehabilitation and availability of acute medical interventions

JFK Medical Center
• JFK Medical Center is a private, not-for-profit suburban hospital with 498 licensed bed
• Largest Emergency Department in the state• Designated as a Comprehensive Stroke Center by the
Joint Commission- recertified in 2016• American Heart Association(AHA)/American Stroke
Association (ASA) certified– Recipient of the AHA/ASA Get With the Guidelines for
Stroke Gold+ Performance Achievement Award• Healthgrades Stroke Care Excellence Award• Ranked #1 in NJ for the last 10 years and in the top 5% of
the country as per the Joint Commission

Johnson Rehabilitation Institute
• An onsite, 94 bed acute rehabilitation center – Accredited by the Joint Commission and
Committee on Accreditation of Rehabilitation Facilities (CARF)
– Inpatient rehabilitation unit: orthopedic cases, neurological cases, general medical cases
– Specialized brain trauma unit: traumatic brain injury, brain tumors, stroke
• Both units receive patients following stroke

JFK Stroke Order Set
• Physical Therapy is an automatic consult for physicians using the stroke order set
• Allows therapists to quickly follow-up with referrals for patients after stroke
• Patients are often evaluated in the Emergency Department (ED) or Intensive Care Unit (ICU)

Management of Patients in the Emergency Department (ED)
• PT works with the nursing and medical staff to ensure medical stability
– Special consideration for patients who have a neurosurgical consult or have received intravenous tPA
• A recent study which analyzed physician’s impressions of PT practice in the ED revealed:24
– Physicians had positive perceptions of PT practice in the ED
– PTs were considered a “valuable asset” to the interprofessional team
• Lebec and colleagues concluded that PTs working in the ED improve quality of care, patient education and patient satisfaction25

Management of Patients in Neurocritical Care (NCC)
• PT in the NCC Unit is specialized and requires therapists to understand both medical and surgical interventions for patients with hemorrhagic or ischemic strokes– Must possess a knowledge of craniotomies,
craniectomies, burr hole procedures, aneurysm coilings and clippings
– Familiarity with patients on ventilators or external ventriculostomy devices (EVDs)26

Use of Functional Outcome Measures27-29
• Functional outcome measure (OM) use is:
– Influenced by time, comfort, evidence, resources
– Mostly associated with practice setting instead of years of practice
• APTA membership or specialty certification

Use of OMs in Practice29,30
• Evidence Database to Guide Effectiveness (EDGE) template developed by APTA Section on Research was modified to assess utility and merit of use for evaluating a patient with stroke
• “Stroke EDGE” completed by the Neurology Section; 56 OMs were reviewed in a final compilation based on initial screening for appropriateness; Each scored from 4 (highly recommended) to 1 (not recommended)
• OMs can be used to: Monitor progress and identify at risk individuals
– Contribute to an improved development of a care and discharge plan
– Improve communication between care givers and facilities
– Increase efficiency of practice
– Compare patient outcomes between different clinicians and different facilities
• Use of OMs may facilitate compliance with CMS requirements
• Study showed training programs are effective in improving the use of OMs

Using Tools to Predict Outcomes7
• For stroke trials, the Barthel Index (BI) and Modified Rankin Scale (mRS) are most commonly used
• FIM is not well used in cohort studies beginning from stroke onset
• OMs performed early during a patient’s acute stay are often underestimated because patients are still bedridden
• If BI is done too early, it is not a good predictor of long-term function

StrokeEDGE Highly Recommended OMs in the Acute Setting31,32
6 MWT 1 minute for instruction, 6 minutes for test30 meters (100’) of uninterrupted walk areaStopwatch and measuring tape
Timed Up and Go Measures fall risk, mobility, balance, walking capacityLess than 5 minutesStopwatch and arm chairAble to use assistive device, but must do without assist Cut –off score >13 sec
5 Times Sit to Stand
Less than 5 minutesArm chair and stopwatchCan use device, but if unable to complete without assistance, it is a failureAllows contact guard, (close) supervision and (modified) independent ratings
10 Meter Walk Test(10 MWT)
Walking speedLess than 5 minutes14 meters of unobstructed walking pathStopwatchCan use device, but cannot have assistanceIncreased speed indicative of increased ability to walk independently

Modified Rankin Scale (mRS)33,34
• Scored from 0 to 6
– Describes clinically distinct functional levels
– Responds well to patient reported outcomes and disability levels
– Less detectable changes noted at lower scores (from 0-2)
– Has a ceiling effect
• mRS scores are often reported in research studies
• Scores may be completed by physicians, nurses, therapists or researchers

Barthel Index (BI)• 10 items with varying weight31,33,34
– Point scale of 0, 5, 10, 15– Higher score indicates increasing independence – Has a ceiling effect– Good for minimal detectable change in long
term studies– 2-5 minutes to complete self-report and 20
minutes of direct clinician observation• When BI scores are compared with FIM scores
they show similar results34,35
– On higher functional levels both the BI and mRS had fairly equivalent scores

Predicting Outcomes in the Upper Extremity (UE)8
• Many evidence-based (EB) treatments are dependent on appropriate patient selection
• For 80 % of patient’s who suffered from their first stroke, recovery follows the same sequence of activity progression as BI items
• Studies demonstrate that the greatest gains are within 3-6 months, but improvements can continue for over a year
• The Copenhagen study of 1,179 patients showed 95% of patients reached their maximum on the BI at 4 months– 4-10% of all patients will show further improvement in UE
and lower extremity (LE) function and ADL– 15-25% show a significant decline in function at 6 months

Patient Goals After Stroke• The rehabilitation of stroke patients is a continuum, which may begin with
preventative measures and passive interventions36
• Goals of early rehab for PT:– Encouraging proper positioning– Prevent contractures and pressure ulcers – Chest PT to improve secretion clearance and airway management– Passive stretching to maintain muscle length, prevent contractures,
reduce motor neuron excitability and spasticity37
– Cardiovascular training and progressive mobility as tolerated– Patient and caregiver education– Goal setting and discharge planning
• Goal is to improve functional outcomes for patients, which also contributes to:– Increased Patient/caregiver satisfaction – A potential reduction for readmission and long-term financial
expenditures38

Progressive Mobility
• For lower level patients, increase: – Mobility with and without assistive device use– Activity tolerance and time out of bed– Patient and family education: orientation, positioning, cognitive
awareness
• With higher level patients:– Increase ability to multi-task and higher level cognitive tasks– Introduce higher level balance training and coordination
activities– Promote improved endurance and introduce fall recovery
strategies– Initiate community re-entry and education on return to
work/driving

JFK Program Improvement
• Emphasize clear communication across providers and patients/caregivers, concise documentation and more thorough handoffs
• Therapy department assisted:– Nursing staff on our stroke service with revising their
nursing handoff form
– Nursing leadership with improving unit-to-unit and shift-to-shift communication
– With trials of a written handoff of each patient’s mobility status in the NCC unit

JFK Program Improvement
• New NCC Intensivist started at JFK with a mission to improve mobility, communication and patient outcomes– Prioritizing NCC patients in the AM – White board handoffs– Improved communication of therapy staff and NCC
team
• Timeframe for bedrest was 24 hours after tPA– Suggested a reduction in the tPA window from 24
hours of bedrest to 6 hours of bedrest with physician consent

Mobilizing Patients After tPA• Studies demonstrated the safety of early
mobilization of patients with acute ischemic stroke between 12 and 24 hours after receiving intravenous tPA and 90% of patients experienced no adverse events– 1 patient experienced asymptomatic orthostatic
hypotension39
– 73% were mobilized without adverse events and 89% tolerated all mobilization activities • One patient had transient hemiparesis
• Patients require neurologic and vital sign monitoring40

Mobilizing Patients After tPA
• Patients received PT with early mobility 13-24 hours after receiving intravenous tPA41
– 76% of patients had no complications with mobility
– 87% of mobility activities were tolerated without any adverse response • No sustained neurological deficit noted or bleeding from an
invasive line
• AVERT Phase III included 500 patients who had tPA and focused on rehabilitation treatment and timing during a patient’s hospital stay42

Mobilizing Patients After tPA
• At JFK, over 20 cases where patients have received tPA and been mobilized in under 12 hours
• No adverse events reported

Mobilizing Patients After Stroke• Many guidelines have advocated for early patient
mobility, but the timing and type of mobility has not been addressed in research42,43
• Body of evidence on the potential negative effects of mobility within 24 hours of stroke for patients with intracerebral hemorrhage44,45
• Smaller study found that earlier mobility, defined as mobilization within 24 hours of stroke onset, was not a positive predictor of function at 3 months46

Mobilizing Patients After Stroke• Early mobilization within 24 hours of stroke onset was feasible
and did not increase 3 month mortality47
– Patients returned to walking 2.5 days faster48
– Improved functional outcomes noted at 3 months49
– Reduced cost of care50
• Rehabilitation intensity was a significant predictor of function after adjusting for initial stroke severity and age51
– Patients with severe stroke benefited more than those with moderate stroke from increased rehabilitation intensity
• It costs less to care for patients receiving early mobilization compared to standard care52

Mobilizing Patients After Stroke
• Limitation of research: Early mobilization group had a higher intensity of activity with more frequent doses53
– Future research should look at the dose response relationship of mobility and assess different mobility activities

Mobilizing Patients After Stroke54
• Authors hypothesized that PT would be different between treatment group versus standard care group and that immobility-related events would be associated with therapy dose
– Single blind, multicenter, RCT
– Timing, amount of therapy and therapy type was recorded and analyzed for 71 patients
– Frequency of therapy and percentage of out of bed activities were different between groups
– Mobilization was earlier, occurred an average of 3 times/day, with more patients receiving out-of-bed activities
• Conclusion: The therapy schedule was different in the intervention group, but there was no difference in immobility-related events in 3 months post-stroke between groups

Mobilizing Patients After Stroke• Early mobility was found to be safe for patients after aneurysmal
subarachnoid hemorrhage (SAH) in a small, retrospective analysis55
– 25 patients received early mobility by PT/OT following SAH
– Patients were mobilized 3.2 days after aneurysmal SAH
– No mortalities 30 days after mobility and adverse events occurred in under 6% of cases
• Early mobilization and rehabilitation increased the chance of good functional outcome in patients with poor grade aneurysmal SAH56
– Prospective study that assessed the impact of early mobility and rehab on global function one year after the hemorrhage
– Regression analysis did not reveal a significant effect for most patients; however in poor grade patients, early rehab more than doubled the chance of a favorable outcome
– Early rehabilitation was not harmful

Mobilizing Patients After Stroke57
• AVERT Phase III:– Trial took place in 5 countries and included 56 stroke units– 2,014 patients were enrolled over 8 years including those
with intracerebral hemorrhage and those that received tPA– Patients after stroke received either usual care or were in
the early mobilization group– Primary outcomes was functional independence on the
mRS score at 3 months – Conclusion: Those that received early mobilization had a
less favorable mRS outcome compared to the usual care group and there was no difference in mortality or immobility-related complications between the 2 groups • No differences found for patients who received tPA

Mobilizing Patients After Stroke57
• Authors recommend:
– Early, lower-dose out-of-bed activity regimen is preferable to very early, frequent, higher-dose intervention
– Refining present stroke care guidelines to reflect results
– Further research should look at analyses of dose-response associations

External Ventricular Devices (EVD)
• EVDs should be clamped for safe mobility58
• PTs mobilize patients with EVDs based on:59
– Patient current medical status, clinical findings and patient safety concerns
– Intensity level of patient mobilization is related to the experience level of the therapist
• Prospective case series:60
– 90 patients with 185 patient encounters were recorded over a 1 year period
– In 81% of encounters, patients were at least standing and 54% were walking with assistance or better
– Four adverse events were recorded

Mobilizing Patients After Stroke
• Early mobility can decrease:61
– Number of patient days in restraints
– Pneumonia and infection rates
– Overall cost of care
– Hospital readmission rates and morbidity
• Safety always comes first! – Follow systolic pressure guidelines as physicians may
induce HTN to improve cerebral perfusion62
• This may minimize brain damage and improve functional outcomes after stroke

Group Discussion & Break
• Identify areas of improvement in your organization:
– Therapy referral process
– Staff education
– Patient & caregiver education

Evidence-Based Intervention5
• Reviewed 467 RCTs involving 25,372 patients post-stroke at varying levels
• Many interventions are not generalized or transferable• Early mobility within 24 hours:
– No significant benefits for decreasing complications or neurological deterioration
– Did not significantly affect fatigue, independence in ADLs at 3 months or discharge home
• High intensity exercise therapy-mean of 17 hours more than control group over 4 weeks:– Beneficial for UE/LE motor function, gait speed, tone, quality
of life, ADL, anxiety, muscle strength• Sit to stand training- no significant benefit for body weight
distribution, sit to stand and balance• Standing balance training without biofeedback- no significant
benefit for postural sway, sit to stand, balance or walking

Evidence-Based Intervention5,19
• Standing balance with biofeedback (with use of force platforms)- used to improve postural sway
– No significant benefit for paretic LE function, gait speed, cadence, step length, balance, functional ambulation and ADLs
• Balance training during functional activities- positive benefit for increased independence with ADLs and balance during mobility
• Partial Weight Body Support (PWBS) Training- meta-analysis showed positive effect for comfortable gait speed and walking distance, but none for max speed, motor function, aerobic capacity, quality of life
• Electromechanical-assisted gait training:
– Without functional electrical stimulation (FES)- improved gait speed, walking distance, peak heart rate and basic ADLs; best in early phase
– With FES- positive for walking and balance only in early rehab phase
• Speed-dependent treadmill (no PWBS)- good for maximum walking speed and step length and beneficial at all phases

Evidence-Based Intervention5,19
• Over ground walking- beneficial for decreasing anxiety and balance in independently walking patients, particularly in chronic phase– Encourages more walking
• Circuit training class with different stations- very beneficial for increased walking speed, balance, walking ability and physical activity
• Neuromuscular Electrical Stimulation (NMES) for paretic LE- beneficial for increased motor function, muscle strength, tone
• Transcutaneous Electrical Stimulation- good results for strength, walking ability
• Constraint-induced movement therapy (CIMT)- original protocol has level 1 evidence also, positive results with multiple protocols– Modified CIMT (mCIMT)- some as little as 3 hours constraint time – Improved UE motor function, synergy, daily functional use and ADLs
• UE splinting/supportive devices- not beneficial for motor function or pain
• NMES for paretic UE- showed best results with use for wrist and finger extension

PT Performance Improvement Projects• Goal is for PT to initiate an evaluation for all patients
diagnosed with a CVA/TIA within 24 hours of electronic order placement
– Percentage in the high 90s
– Improve weekday/weekend communication; provide more staff feedback & education
• Decrease the window of PT care provided and actual documentation completed
– 90 minutes after completion of treatment
– Goal: Decrease patient LOS & improve communication with other multidisciplinary team members

Other Program Changes• Improved communication about stroke orders to stroke coordinator
– Private physicians may not order OT or Physiatry/Rehab Medicine
– New residents may inadvertently not use the Stroke protocol
• Code strokes are called in to the hospital while patient is in transit
• Flag patients with strokes for other members of the interdisciplinary team63
– One study looked at the rate that patients with acute ischemic stroke were missed by looking at ICD-9 codes
– Of 2,027 cases, 14% were missed in the ED
– Hospital stay was longer in those patients with missed diagnosis
– Younger age and decreased levels of consciousness were associated with a higher odd of being missed
– Altered mental status was the most common diagnosis that was missed

Rehabilitation Recommendations19
• Severity of stroke is the biggest predictor of outcome• Screening for rehabilitation:
– Medical status, functional status, social and environmental factors
– Capacity for improvement and assessment of needs • Family training, equipment, vocation and leisure
activities38
• Age negatively impacts outcomes:64
– For more elderly patients, factors such as cognition, family support and pre-morbid function highly impact the potential for discharge home
• Patients with moderate to severe deficits benefit most from comprehensive acute rehabilitation stroke care

Timing for Rehabilitation Transfer• Transfer should be as soon as the patient is medically
stable enough to participate in therapy65,66
• One retrospective study looked at short, moderate or long onset admission intervals for patients with stroke who were admitted into an acute rehabilitation setting67
– FIM scores at admission and discharge for 418 patients after first stroke were recorded
– Time of admission did not affect rehab outcomes of patients referred from acute care facilities where rehabilitation services were provided early and throughout the patient’s acute care stay

Decreasing Secondary Complications68
• Energy expenditure during walking can be up to 2 times greater in patients with hemiplegia
• Multiple RCTs with a variety of cardiovascular exercise program models ranging from 2 to 3x/week for 10 to 12 weeks with from 20 to 60 minutes of continuous exercise, yielded improvement in:
– Peak oxygen consumption, blood pressure response, exercise tolerance and aerobic capacity
• Aerobic programs can improve cardiovascular risk factors and improve medical management in stroke survivors

Decreasing Secondary Complications68
• Depression and fatigue have been shown to be barriers to participation in stroke rehabilitation
• Neurological deficits and comorbidities may impact participation– Study found if a physician recommended exercise, patients
were 2 times more likely to follow through
• Aggressive rehabilitation beyond 6 months post-stroke has been shown to increase aerobic capacity and sensorimotor function
• If a patient is unable to tolerate a higher intensity program, they should have more frequent training at a lower intensity

Discharge Dispositions• Options include:
– Acute inpatient rehabilitation or subacute rehabilitation
– Long term acute care or long term care/skilled nursing facility
– Home with:
• No services
• Homecare services or outpatient services
• Recommendations for community resources-medical fitness centers, local gym membership

Discharge Recommendations• Retrospective study of 311,910 patients over 65 year old, post-
stroke69
– Average admission FIM was 60 and discharge was 84.8– More than 75% were discharged home after acute hospital stay– Patients were more likely to be discharged to another inpatient
facility if:• FIM scores worse than 60 • They were older than 77• Unmarried
– FIM score, age and marital status were good predictors of discharge status
• Data collected from 481 patient records found a positive correlation between FIM scores and discharge to the community70
– FIM found to be a reliable prediction of discharge to the community from the acute hospital among patients with stroke

Discharge Recommendations71
• Prospective study using NIHSS, mRS, Short Portable Mental Status Questionnaire, and BI
• Higher BI was the only factor found to be associated with a return home versus another inpatient facility
• More likely to be discharged to rehab with moderate to severe ADL impairment (BI score 25-60)
• Factors affecting discharge home versus inpatient facility:
– Sociodemographics, premorbid function and ADL impairment
• Selection of rehab versus subacute rehab influenced by nonclinical factors such as:
– Cost, geography, referral relationship or bed availability

Discharge Recommendations72
• The National Quality Forum reports that:– Clinical stroke rehabilitation guidelines and
national standards of care suggest assessment of patients for rehabilitation after stroke
– Place of discharge is associated with rate of functional gains and readmission rates to acute care
– Endorse ordering rehabilitation services for all patients and assessment for further rehabilitation in acute care

Staff Education & Training
• Hospital-wide staff education and training
– BE: Balance decreased & Eyes impaired
– FAST: Face drooping, Arm weakness, Speech difficulties, Time to call 9-1-1
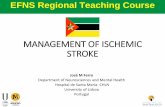
• Patient/Caregiver handouts:
– ROM handouts
– Improved NCC Unit education

Improved Education: ICU

Role of Acute PT• PTs play an active role in multidisciplinary committees
• Why is this important?
– Educate other practitioners/disciplines about PT role in the Acute setting
– Improve programs and patient outcomes
– One study found that factors that positively influenced Acute PT staff’s experiences and clinical decision making was:73
• Communication/relationships and professional identity/role
• Strategies to improve these areas in the Acute Care setting include:
– Promoting interprofessional relationships
– Clearly defining the role of PT in the work setting
– Conducting multidisciplinary team member education

Improving Patient Mobility
• Work with nursing department to write a proposal for ceiling lifts– Improve staff and patient safety– Decrease patient and therapist exertion
• Case report of PT treatment of a patient with stroke while using a ceiling mounted lift for transfers/gait training:74
– With lift use, the patient’s rate of perceived exertion (RPE) was an average of 6
– RPE for the PT was a 2 when the ceiling lift was used and 5 when it was not used

Certified Stroke Rehab Specialist Committee
• Comprised of PTs and OTs who are stroke-certified
• Mission/Goals are to:
– Provide a standardized level of excellent care across the rehabilitation continuum at JFK for patients with stroke
– Organize a uniform system of assessments for stroke used across the continuum of care
– Participate in stroke research to support evidence-based practice and sustain our JFK values of perfect performance and visionary spirit
– Promote interdepartmental communication amongst the disciplines and departments to improve the care of patients with stroke across the rehabilitation continuum
– Promote and enhance patient and family education regarding stroke management, recovery and prevention

Case Study• 68 year-old female was found confused and wandering
• Diagnosed with a right frontal hematoma; treated and discharged
• No improvement after a few days, family brought her to JFK for further workup which revealed:
– Large right frontal intracranial hemorrhage with edema and mass effect
• PT/OT evaluation revealed: mRS score of 4
– 3+ bilateral LE muscle strength
– Completed bed mobility and transfers with close supervision
– Ambulated 50 feet with contact guard assistance, with no assistive device
– Decreased right eye vision and scanning to the left side
– Poor attention to task, decreased memory, decreased cognition, decreased insight and orientation
– Decreased independence with activities of daily living: dressing, grooming, bathing

Case Study• Therapy plan: balance training, labeling of objects, visual scanning
and improving attention to the left side, patient and family education
• Discharge disposition was initially home
– Objective PT/OT findings, functional status, safety, social support were discussed extensively with patient, caregivers and with multidisciplinary team members
– Team decided that the patient would benefit from a Physiatry consult for safe and appropriate discharge planning based on findings
• Following the Physiatrist’s evaluation it was determined that the patient was a good acute rehabilitation candidate
– Insurance authorization was obtained and patient was transferred to the brain trauma unit of the Johnson Rehabilitation Institute

Case Study• She received 3 hours of skilled PT, OT and speech language
services, 5 days a week• Plan of care in inpatient rehabilitation was similar to that on
the acute care service, but more intense• The patient was followed by her cardiologist and neurologist
while in acute rehabilitation• Upon discharge from inpatient rehabilitation, the patient was:
– Independent with feeding– Required supervision for washing/drying clothes and
completing toilet/shower transfers– Required close supervision for ambulation and stair
climbing– Was not cleared for return to work or to driving

JFK Stroke Recovery Program• Compares outcomes of patients with stroke who
received specialized, multidisciplinary outpatient follow-up with patients receiving traditional rehab
• Why is this important?– Hospital readmission among stroke survivors with
disability is common; follow-up intervention after discharge can prevent readmissions, especially for patients with greater impairments75
– Physical activity, muscle strengthening and exercise should be incorporated into the management of stroke survivors76
– Research shows that patients with stroke do better with an organized, interprofessional approach to post-acute rehabilitation77

Dissemination of Stroke Information• In-service on stroke continuum and 4 hours of stroke education
• Journal club:
– Individuals with chronic right middle cerebral artery (MCA) territory lesions exhibit slower, asymmetrical gait compared to those with left MCA lesions78
• For these patients, larger amounts of gray matter may help preserve locomotor control
– Aquatic treadmill training yields better cardiovascular responses than land training for patients with subacute stroke79
– TENS, electrostimulation, optokinetic stimulation, mirror therapy and virtual reality training are effective in treating unilateral neglect syndrome in patients with stroke80
– Early assessment of and management of trunk control for patients with stroke can predict and potential improve long term ADL function81

Dissemination of Stroke Information
• Staff education: American Heart Association/American Stroke Association released updated guidelines on preventing recurrent stroke in patients who have had a previous stroke/TIA
– Guidelines address risk factors for stroke: modifiable vascular risk factors and behavioral risk factors1

Additional Resources
• National Stroke Association82 – Information for stroke survivors, patients, families and healthcare professonals
• American Heart Association/American Stroke Association American83- Information for patients and families on life after stroke, warning signs
• Center for Disease Control and Prevention84- Quick stroke facts and educational materials for patients/families
• National Institute of Neurological Disorders and Stroke85-Information on general stroke facts, post-stroke brochures for patients and caregivers, rehabilitation and research initiatives

Additional Resources
• National Institute of Health86- Information on stroke for families via a stroke toolkit, available in English and Spanish
• Academy of Neurologic Physical Therapy87- Consumer information and stroke PT information
• Rehabilitation Measures Database88- List of different rehabilitation measures with valuable information
• Move Forward. Physical Therapy Brings Motion to Life89-List of stroke warning signs and symptoms and information for patients following stroke
• Booklet on Stroke Recovery90- Describes the stroke recovery process for patients and families

Additional Resources
• The Northeast Cerebrovascular Consortium16-Dedicated to improving stroke systems of care across the Northeast
• Evidence Based Research on Stroke Rehabilitation (EBRSR)91: The Canadian Partnership for Stroke Recovery- Provides in depth reviews on stroke-related research
• Stroke Engine92- The Canadian Partnership for Stroke Recovery patient education website

Questions

References1. Mozaffarian D, Benjamin EJ, Go AS et al. Heart Disease and Stroke Statistics. Circulation. http://circ.ahajournals.org/content/circulationaha/131/4/e29.full.pdf. Published 2016. Accessed on October 1, 2016.2. Kochanek KD, Murphy SL, Xu J, et al. National Vital Statistics Report, Deaths: Final Data for 2014. http://www.cdc.gov/nchs/data/nvsr/nvsr65/nvsr65_04.pdf. 65(4). Uploaded June 30, 2016. Accessed 10/20/2016.3. Mozaffarian D, Benjamin EJ, Go AS. Heart Disease, Stroke and Research Statistics at-a-Glance. http://www.heart.org/idc/groups/ahamah-public/@wcm/@sop/@smd/documents/downloadable/ucm_480086.pdf. Published December 5, 2016. Accessed on October 4, 2016.4. Stroke Facts. Centers for Disease Control and Prevention. http://www.cdc.gov/stroke/facts.htm. Updated on March 24, 2015. Accessed on October 14, 2016.5. Veerbeek JM, van Wegen E, van Peppen R, et al. What is the Evidence for Physical Therapy Poststroke? A Systematic Review and Meta-Analysis. PLoS ONE. 2014;9(2):e87987.

References
6. Chow D, Hauptman J, Wong T, et al. Changes in stroke research productivity: a global perspective. Surg Neurol Int. 2012;3:2.7. Veerbeek JM, Kwakkel GK, Van Wegen EEH, Ket JC, Heymens MW. Early Prediction of Outcomes of Activities of Daily Living After Stroke: A Systematic Review. Stroke. 2011;42:1482-1488.8. Kwakkel G, Kollen B. Predicting activities after stroke: what is clinically relevant? Int J Stroke. 2013;8:25-32.9. Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics—2015 update: A report from the American Heart Association. Circulation. 2015;e29-322.10. Stroke Facts. Centers for Disease Control and Prevention. http://www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_stroke.htm . Published 2015. Updated on June 16, 2016. Accessed on November 4, 2016.

References11. CDC. Prevalence of stroke -United States, 2006–2010. MMWR. 2012;61(20):379–382.12. Hall MJ, Levant S, DeFrances CJ. Hospitalization for stroke in U.S. hospitals, 1989–2009. NCHS data brief, No. 95. Hyattsville, MD: National Center for Health Statistics; 2012.13. National Hospital Discharge Survey: 2010 table. Average length of stay and days of care-Number and rate of discharges by first-listed diagnostic categories. CDC. http://www.cdc.gov/nchs/data/nhds/2average/2010ave2_firstlist.pdf. Published 2011. Accessed on October 11, 2016.14. Fang J, Keenan NL, Ayala C, et al. Awareness of stroke warning symptoms-13 states and the District of Columbia, 2005. MMWR. 2008;57(18):481-485. 15. The ATLANTIS, ECASS, and NINDS tPA Study Group Investigators. Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS tPA stroke trials. Lancet. 2004;363:768–774.

References16. Northeast Cerebrovascular Consortium (NECC). http://www.thenecc.org. Accessed on November 21, 2016.17. Kjellström T, Norrving B, Shatchkute A. Helsingborg Declaration 2006 on European stroke strategies. Cerebrovasc Dis. 2007;23:231-241.18. Schwamm LH, Pancioli A, Acker JE. Recommendations for the Establishment of stroke systems of care: Recommendations from the American Stroke Association’s Task Force on the Development of Stroke Systems. Circulation. 2005;111:1078-1091.19. Teasell R, McClure A, Salter K, et al. Managing the stroke rehabilitation triage process. Evidence Based Review of Stroke Rehabilitation website. http://www.ebrsr.com/sites/default/files/H_Clinical_Assessment_Tools.pdf. Uploaded April 9, 2014. Accessed on November 23, 2016.20. Teasell R, Foley N, Hussein M, Cotoi A. Evidence Based Review of Stroke Rehabilitation: The Efficacy of Stroke Rehabilitation.2016: Chapter 5. http://www.ebrsr.com/evidence-review/5-efficacy-stroke-rehabilitation. Accessed November 16, 2016.

References21. Evers SM, Struijs JN, Ament AJ, et al. International comparison of stroke cost studies. Stroke. 2004;35(5):1209-15. 22. Anderson C, Mhurchu CN, Rubenach S, et al. Home or hospital for stroke rehabilitation? Results of a randomized controlled trial II: cost minimization analysis at 6 months. Stroke;31(5):1032-7.23. Di Carlo A. Human and economic burden of stroke. Age and Aging. 2009;38:4-5.24. Fruth SJ, Wiley S. Physician impressions of Physical Therapist practice in the emergency department: Descriptive, comparative analysis over time. Phys Ther. 2016;96(9):1333-1340.25. Lebec MT, Cernohous S, Tenbarge L, et al. Emergency department physical therapist service: A pilot study examining physician perceptions. Internet J Allied Health Sci Pract. 2010:8:1-12.26. Sprenkle KJ, Pechulis M. Early mobility of patients poststroke in the neuroscience intensive care unit. JACPT. 2013;4(3):101-109.

References27. Duncan PW, Jorgensen HS, Wade DT. Outcome measures in acute stroke trials a systematic review and some recommendations to improve practice. Stroke. 2000;31(6):1429-1438.
28. Anderson HD, Sullivan JE. Outcome measures for persons with acute stroke: A survey of Physical Therapists practicing in acute care and acute rehabilitation settings. JACPT. 2016;7(2):76-83.
29. Sullivan JE, Crowner BE, Kluding PM, et al. Outcome measures for individuals with stroke: Process and recommendations from the American Physical Therapy Association Neurology Section Task Force. Phys Ther. 2013;93:1383–1396.
30. van Peppen R, Schuurmans M, Stutterheim E, et al. Promoting the use of outcome measures by an educational programme for physiotherapists in stroke rehabilitation: A pilot randomized controlled trial. Clin Rehabil. 2009;23:1005–1017.
31. American Physical Therapy Association (APTA). Tests and Measures. PTNow website. Available at: http://www.ptnow.org/tests-measures. Accessed on December 14, 2016.

References32. Teasell R, McClure A, Salter K, et al. Clinical assessment tools. Evidence-Based Review of Stroke Rehabilitation website. Available at: http://www.ebrsr. com/ebrsr/uploads/H_Clinical_Assess ment_Tools.pdf. Last Accessed November 16, 2016.33. Weimar C, Kurth T, Kraywinkel K, et al. Assessment of functioning and disability after ischemic stroke. Stroke. 2002;33(8):2053-2059. 34. Kwon S, Hartzema AG, Duncan PW, et al. Disability measures in stroke: Relationship among the Barthel Index, the Functional Independence Measure, and the Modified Rankin Scale. Stroke.2004;35:918-923.35. Lai SM, Duncan PW. Stroke recovery profile and the Modified Rankin assessment. Neuroepidemiology. 2001;20(1):26-30.36. Brandstater ME, Shutter LA. Rehabilitation interventions during acute care of stroke patients. Top Stroke Rehabil. 2002;9(2):48-56.37. Proske U, Morgan DL, Gregory E. Thixotrophy in skeletal muscle and in muscle spindles: A review. Prog Neurobiol. 1993;41:705.38. Duncan PW, Zorowitz VR, Bates, B. Management of adult stroke rehabilitation care: A clinical practice guideline. Stroke. 2005;36:e100-e143.

References39. Arnold SM, Chavez OS, Dinkins MM, et al. Outcomes of patients receiving early mobilization less than 24 hours post-IV tPA infusion for acute ischemic stroke. Poster presentation at 2011 American Physical Therapy Association Annual Conference, National Harbor, MD: American Physical Therapy Association; 2011.40. Arnold SM, Dinkins M, Mooney LH, et al. Very early mobilization in stroke patients treated with intravenous recombinant tissue plasminogen activator. J Stroke Cerebrovasc Dis. 2015;24(6):1168-1173.41. Davis O, Mooney L, Dinkins M, et al. Early mobilization of ischemic stroke patients post intravenous tissue plasminogen activator [abstract]. Stroke. 2013;44:A121.42. Bernhardt J, English C, Johnson L, et al. Early mobilization after stroke; early adoption but limited evidence. Stroke. 2015;46:1141-1146.43. Freeman WD, Chavez OS, Meschia J. Letter by Freeman et al regarding article “Very Early Mobilization after stroke fast-tracks return to walking: Further results from the Phase II AVERT randomized controlled trial”. Stroke.201142:e375.44. Olavarria VV, Arima H, Anderson CS, et al. Head position and cerebral blood flow velocity in acute ischemic stroke: A systematic review and meta-analysis. Cerebrovasc Dis.2014;37:401-408.

References
45. Skarin M, Bernhardt J, Sjoholm A, et al.” Better wear out sheets than shoes”. A survey of 202 stroke professionals’ early mobilisation practices and concerns. Int J Stroke. 2011;6(10):10-15.46. Sundseth A, Thommessen B, Ronning OM. Early mobilization after acute stroke. J Stroke Cerebrovas Dis. 2014;23(3):496-499.47. Bernhardt J, Dewey H, Thrift A, et al. A very early rehabilitation trial for stroke (AVERT): phase II safety and feasibility. Stroke. 2008;39(2):390-396.48. Cumming T, Thrift A, Collier J, et al. Very early mobilization after stroke fast-tracks return to walking: Further results from the phase II AVERT randomized control trial. Stroke. 2011;42:153-158.49. Craig LE, Berhnardt J, Langhorne P et al. Early mobilization after stroke: an example of an individual patient data meta-analysis of a complex intervention. Stroke. 2010;41:2632-2636.

References50. Tay-Teo K, Moodie M, Bernhardt J, et al. Economic evaluation alongside a phase II, multi-centre, randomized controlled trial of very early rehabilitation after stroke (AVERT). Cerebrovasc Dis. 2008;26(5):475-481. 51. Hu MH, Hsu SS, Yip PK, et al. Early and intensive rehabilitation predicts good functional outcomes in patients admitted to a stroke intensive care unit. Disabil. Rehabil. 2010;32(15):1251-1259.52. Cumming T, Collier J, Bernhardt J. The effect of very early mobilization after stroke on psychological well-being. J Rehabil Med. 2008;40(8):609-614.53. Awad AJ, Kellner CP, Mascitelli JF, et al. No early mobilization after stroke: Lessons learned from the AVERT trial. World Neurosurgery. 2016;87:474.54. Wijk R, Cumming T, Churilov L. An early mobilization protocol successfully delivers more and earlier therapy to acute stroke patients: Further results from Phase II of AVERT. Neurorehabil and Neural Repair. 2012;26(1):20-26.

References55. Olkowski BF, Devine MA, Slotnick LE. Safety and feasibility of an early mobilization program for patients with aneurysmal subarachnoid hemorrhage. Phys Ther. 2013;93(2)208-215.56. Karic T, Roe C, Nordenmark TH, et al. Impact of early mobilization and rehabilitation on global functional outcome one year after aneurysmal subarachnoid hemorrhage. J Rehabil Med. 2016;48:00-00.57. Group ATC, Bernhardt J, Langhorne P, et al. Efficacy and safety of very early mobilisation within 24 h of stroke onset (AVERT): A randomized controlled trial. Lancet. 2015;386:46-55.58. Gillen G. Pathophysiology, medical management and acute rehabilitation of stroke survivors. In: Stroke Rehabilitation: A Function Based Approach. 4th ed. Elsevier Science Health Science; 2015: 2-45.59. Hale C, Wong K, Pennings A, et al. Practice patterns of Canadians physiotherapists mobilizing patients with external ventricular drains. Physiotherapy Canada. 2013;65(4):365-373.

References
60. Kraft J, Shah SO, Ankam N, et al. Early ambulation in patients with external ventricular drains: Results of a quality improvement project. Neurology. 2016;86(16):P3.289.
61. Titsworth WL, Hester J, Correia T, et al. The effect of increased mobility on morbidity in the Neurointensive Care Unit. J Neurosurg. 2012;116:1379-1388.62. Rordorf G, Cramer SC, Efird JT, et al. Pharmacological elevation of blood pressure in acute stroke: Clinical effects and safety. Stroke. 1997;28:2133-2138.63. Madsen T, Khoury J, Cadena R, et al. Potentially missed diagnosis of ischemic stroke in the emergency department in the greater Cincinnati/northern Kentucky stroke study. Acad Emerg Med. 2016;23(10):1128-1135.

References64. Gresham GE, Duncan PS, Stason WB, et al. Clinical Practice Guideline Number 16. Post-Stroke Rehabilitation. Rockville, MD.: US Department of Health and Human Services, Agency for Health Care Policy and Research; 1995. AHCPR publication 95-0662.
65. Novack TA, Satterfield WT, Lyons K, et al. Stroke onset and rehabilitation: Time lag as a factor in treatment outcome. Arch Phys Med. 1984;65:316-319.
66. Asberg KH. Orthostatic tolerance training of stroke patients in general medical wards. Scand J Rehabil Med. 1989;21:179-185.
67. Gagnon D, Nadeau S, Tam V. Ideal timing to transfer from an acute care hospital to an interdisciplinary inpatient rehabilitation program following a stroke: An exploratory stud. BMC Health Services Research. 2006. http://www.biomedcentral.com/1472-6963/6/151. Updated on November 23, 2006. Accessed on October 21, 2016.

References
68. Gordon NF, Gulanick M, Costa F, et al. Physical activity and exercise recommendations for stroke survivors an American heart association scientific statement from the council on clinical cardiology, subcommittee on exercise, cardiac rehabilitation, and prevention; the council on cardiovascular nursing; the council on nutrition, physical activity, and metabolism; and the stroke council. Stroke.2004;35(5):1230-1240.69. Pohl PS, Billinger SA, Lentz A, et al. The role of patient demographics and clinical presentation in predicting discharge placement after inpatient stroke rehabilitation: analysis of a large, US data base. Disability and Rehabilitation. 2013;35(12):990-994.70. Roberts PS, Mix J, Rupp K, et al. Using functional status in the acute hospital to predict discharge destination for stroke patients. Am J Phys Med Rehabil. 2016; 95(6):416-424.

References
71. Stein J, Bettger JP, Sicklick A, et al. Use of standardized assessment to predict rehabilitation care after acute stroke. Arch Phys Med Rehabil. 2015;96(2):210-217.72. National Quality Foundation. http://www.qualityforum.org/News_And_Resources/Press_Releases/2012/NQF_Endorses_Neurology_Measures.aspx.Accessed on December 14, 2016. 73. Lau B, Skinner EH, Lo K, et al. Experiences of Physical Therapists working in the acute care hospital setting: Systematic review. Phys Ther. 2016;96(9):1317-1332.
74. Halbert J, Pearce R, Burgess T, et al. Advantages of using ceiling mounted lifts in acute stroke rehabilitation. JACPT. 2013;4(2):73-83.

References
75. Andersen HE, Schultz-Larsen K, Kreiner S, et al. Can readmission after stroke be prevented? Stroke. 2000;31:1038-1045.
76. Billinger S, Ross, A, Bernhardt J, et al. Physical activity and exercise recommendations for stroke survivors: A statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45:2532-2553.
77. Stroke Unit Trialists’ Collaboration. Organized inpatient (stroke unit) care for stroke. Cochrane Database Syst Review. 2002(1):CD000197.

References
78. Chen, Novak, Manor. Infarct hemisphere and noninfarcted brain volumes affect locomotor performance following stroke. Neurology. 2014;828-834.79. Lee, YK, Kim BR, Han EY. Peak cardiorespiratory responses of patients with subacute stroke during land and aquatic treadmill exercise. Am J Phys Med Rehabil. 2016;00:00-00.80. Pernet L, Jughters A, Kerckhofs E. The effectiveness of different treatment modalities for rehabilitation of unilateral neglect in stroke patients: A systematic review. NeuroRehabilitation. 2013;33(4):611-62081. Hsieh CL, Sheu CF, Hsueh IP, et al. Trunk control as an early predictor of comprehensive activities of daily living function in stroke patients. Stroke. 2002;33:2626-2630.

82. National Stroke Association: Hope After Stroke. National Stroke Association. http://www.stroke.org. Published 2016. Accessed on November 2, 2016.
83. Heart Association/American Stroke Association: Together to End Stroke. American Heart Association/American Stroke Association. http://www.strokeassociation.org. Published 2016. Accessed on November 2, 2016.
84. Center for Disease Control and Prevention: Stroke. http://www.cdc.gov/Stroke/index.htm . Published May 5, 2016. Accessed on October 21, 2016.
85. Brain Basics: Preventing Stroke. National Institute of Neurological Disorders and Stroke. http://www.ninds.nih.gov/disorders/stroke/preventing_stroke.htm. Published February 1, 2016. Accessed on October21, 2016.
86. Know Stroke: Know the Signs. Act in Time. National Institute of Health. https://stroke.nih.gov/. Accessed on November 2, 2016.
87. Academy of Neurologic Physical Therapy. http://neuropt.org/. Published 2015. Accessed on October 21, 2016.
References

References88. Rehabilitation Measures Database: The Rehabilitation Clinician's Place to Find the Best Instruments to Screen Patients and Monitor Their Progress. Rehabilitation Institute of Chicago. http://www.rehabmeasures.org/default.aspx. Published 2010. Accessed on October 21, 2016.89. Physical Therapist’s Guide to Stroke. Move Forward. Physical Therapy Brings Motion to Life. American Physical Therapy Association. http://www.moveforwardpt.com/symptomsconditionsdetail.aspx?cid=929683c9-e6ab-4b0b-ad65-1c4d69dfa269. Published May 10, 2011. Updated on February 11, 2016. Accessed on October 21, 2016.90. US Agency for HealthCare Research and Quality. Recovering After a Stroke: A Patient and Family Guide. AHCPR. 1995;16(Number 95-0664):1-17.91. The Canadian Partnership for Stroke Recovery. http://www.ebrsr.com. Published 2015. Accessed December 14, 2016. 92. The Canadian Partnership for Stroke Recovery. http://www.strokengine.ca/ Published 2016. Accessed December 14, 2016.