Endometrial carcinoma with choriocarcinomatous differentiation: A case report and review of the...
4
Case Report Endometrial carcinoma with choriocarcinomatous differentiation: A case report and review of the literature Takashi Yamada a, ⁎, Hiroshi Mori b , Masanori Kanemura c , Masahide Ohmichi c , Yuro Shibayama a a Department of Pathology, Osaka Medical College, 2-7 Daigaku-machi, Takatsuki, Osaka 569-8686, Japan b Department of Clinical Pathology, Minoh City Hospital, 5-7-1 Kayano, Minoh, Osaka 562-8562, Japan c Department of Obstetrics and Gynecology, Osaka Medical College, 2-7 Daigaku-machi, Takatsuki, Osaka 569-8686, Japan abstract article info Article history: Received 30 October 2008 Available online 20 February 2009 Keywords: Endometrial cancer Adenocarcinoma Choriocarcinoma Trophoblastic tumor Choriocarcinomatous differentiation hCG Background. Choriocarcinomas unrelated to pregnancy, teratomas, or germ cell tumors have been found in the stomach, lungs, colon, esophagus, bladder, breast, renal pelvis and other sites. Case. We present a case of a 58-year-old woman with endometrial carcinoma with choriocarcinomatous differentiation. She received surgery and chemotherapy for endometrial adenocarcinoma. However, a metastatic tumor of choriocarcinomatous element appeared at the vaginal cuff 9 months after surgery. Additional chemotherapy for choriocarcinoma resulted in a decrease in the serum hCG and the tumor regressed. Fifty months following surgery, she is alive without disease. Conclusion. Treatment and follow-up must be performed not only for the adenocarcinoma element but also for the choriocarcinoma element in patients presenting with endometrial carcinoma with choriocarci- nomatous differentiation. © 2009 Elsevier Inc. All rights reserved. Introduction Choriocarcinomas unrelated to pregnancy, teratomas, or germ cell tumors have been found in the stomach [1], lung [2], colon [3], esophagus [4], bladder [5], breast [6], renal pelvis [7] and other sites. They are believed to arise from poorly differentiated carcinoma or develop as carcinoma with choriocarcinomatous differentiation. They invariably contain and produce human chorionic gonadotropin (hCG) peptide hormone. We report a case of endometrial carcinoma with choriocarcinomatous differentiation, and reviewed the literature with regard to malignant uterine tumor with choriocarcinomatous differentiation. Case report A 58-year-old gravida 1, para 1 with menopausal status for 6 years presented with postmenopausal bleeding. She had uneventful surgical and gynecological histories with no history of hormonal replacement therapy. Her height was 143 cm and her weight was 45 kg. The gynecological examination revealed a painless enlargement of the uterus with thick endometrium. Magnetic resonance imaging showed that a bulky mass, measuring about 5 cm in diameter, existed in the uterine cavity involving the anterior wall of the uterine body. The tumor in the endometrial biopsy specimen was diagnosed as poorly differentiated endometrioid adenocarcinoma with bizarre giant cells. Chest X-ray and abdominal computed tomography showed no signs of metastatic lesion. Under the diagnosis of endometrial cancer, an abdominal hysterectomy with bilateral salpingo-oophorectomy and pelvic lymphadenectomy were performed. The hysterectomy specimen, measuring 95×75 mm, showed a partially necrotic and hemorrhagic polypoid mass of approximately 45 × 45 mm in the endometrial cavity. Tumor grew with infiltration, as well as lymphovascular and blood vessel involvements, into the inner third region of the myometrium. The resected vaginal cuff as well as both adnexa and the resected lymph nodes were free of tumor (FIGO stage 1b). The pathological examination revealed 2 distinct tumor types. Approximately half of the tumor showed a well differentiated endometrioid adenocarcinoma, without psammoma bodies (Fig. 1a). The remaining parts of the tumor showed a biphasic morphology, containing mononuclear cells and syncytial-like giant cells resembling choriocarcinoma (Fig. 1c). There was a close transition from the endometrioid to the choriocarcinomatous areas on several slides (Fig. 1b). Immunohistochemical analysis for CA125 (Dako, clone OC125) and vimentin (Dako, clone V9) were positive in the adenocarcinomatous part, and human chorionic gonadotropin (Dako, polyclonal) was positive in the choriocarcinomatous part, especially in the syncytial- like cells. Keratin (Dako, clone AE1, AE3) was positive in both elements. Syncytial-like cells in the lymphovascular involvement were stained intensely with hCG. The preoperative serum β-hCG value was not measured because choriocarcinoma was not suspected before surgery. The Gynecologic Oncology 113 (2009) 291–294 ⁎ Corresponding author. Fax: +8172 684 6513. E-mail address: [email protected] (T. Yamada). 0090-8258/$ – see front matter © 2009 Elsevier Inc. All rights reserved. doi:10.1016/j.ygyno.2009.01.005 Contents lists available at ScienceDirect Gynecologic Oncology journal homepage: www.elsevier.com/locate/ygyno
-
Upload
takashi-yamada -
Category
Documents
-
view
213 -
download
1
Transcript of Endometrial carcinoma with choriocarcinomatous differentiation: A case report and review of the...

Gynecologic Oncology 113 (2009) 291–294
Contents lists available at ScienceDirect
Gynecologic Oncology
j ourna l homepage: www.e lsev ie r.com/ locate /ygyno
Case Report
Endometrial carcinoma with choriocarcinomatous differentiation:A case report and review of the literature
Takashi Yamada a,⁎, Hiroshi Mori b, Masanori Kanemura c, Masahide Ohmichi c, Yuro Shibayama a
a Department of Pathology, Osaka Medical College, 2-7 Daigaku-machi, Takatsuki, Osaka 569-8686, Japanb Department of Clinical Pathology, Minoh City Hospital, 5-7-1 Kayano, Minoh, Osaka 562-8562, Japanc Department of Obstetrics and Gynecology, Osaka Medical College, 2-7 Daigaku-machi, Takatsuki, Osaka 569-8686, Japan
⁎ Corresponding author. Fax: +81 72 684 6513.E-mail address: [email protected] (T.
0090-8258/$ – see front matter © 2009 Elsevier Inc. Adoi:10.1016/j.ygyno.2009.01.005
a b s t r a c t
a r t i c l e i n f oArticle history:
Background. Choriocarci Received 30 October 2008Available online 20 February 2009Keywords:Endometrial cancerAdenocarcinomaChoriocarcinomaTrophoblastic tumorChoriocarcinomatous differentiationhCG
nomas unrelated to pregnancy, teratomas, or germ cell tumors have been foundin the stomach, lungs, colon, esophagus, bladder, breast, renal pelvis and other sites.
Case. We present a case of a 58-year-old woman with endometrial carcinoma with choriocarcinomatousdifferentiation. She received surgery and chemotherapy for endometrial adenocarcinoma. However, ametastatic tumor of choriocarcinomatous element appeared at the vaginal cuff 9 months after surgery.Additional chemotherapy for choriocarcinoma resulted in a decrease in the serum hCG and the tumorregressed. Fifty months following surgery, she is alive without disease.
Conclusion. Treatment and follow-up must be performed not only for the adenocarcinoma element butalso for the choriocarcinoma element in patients presenting with endometrial carcinoma with choriocarci-nomatous differentiation.
© 2009 Elsevier Inc. All rights reserved.
Introduction
Choriocarcinomas unrelated to pregnancy, teratomas, or germ celltumors have been found in the stomach [1], lung [2], colon [3],esophagus [4], bladder [5], breast [6], renal pelvis [7] and other sites.They are believed to arise from poorly differentiated carcinoma ordevelop as carcinoma with choriocarcinomatous differentiation. Theyinvariably contain and produce human chorionic gonadotropin (hCG)peptide hormone. We report a case of endometrial carcinoma withchoriocarcinomatous differentiation, and reviewed the literaturewith regard to malignant uterine tumor with choriocarcinomatousdifferentiation.
Case report
A 58-year-old gravida 1, para 1 with menopausal status for 6 yearspresentedwith postmenopausal bleeding. She had uneventful surgicaland gynecological histories with no history of hormonal replacementtherapy. Her height was 143 cm and her weight was 45 kg. Thegynecological examination revealed a painless enlargement of theuterus with thick endometrium. Magnetic resonance imaging showedthat a bulky mass, measuring about 5 cm in diameter, existed in theuterine cavity involving the anterior wall of the uterine body. Thetumor in the endometrial biopsy specimen was diagnosed as poorlydifferentiated endometrioid adenocarcinoma with bizarre giant cells.
Yamada).
ll rights reserved.
Chest X-ray and abdominal computed tomography showed no signs ofmetastatic lesion. Under the diagnosis of endometrial cancer, anabdominal hysterectomy with bilateral salpingo-oophorectomy andpelvic lymphadenectomy were performed.
The hysterectomy specimen, measuring 95×75 mm, showed apartially necrotic and hemorrhagic polypoid mass of approximately45×45mm in the endometrial cavity. Tumor grewwith infiltration, aswell as lymphovascular and blood vessel involvements, into the innerthird region of the myometrium. The resected vaginal cuff as well asboth adnexa and the resected lymph nodes were free of tumor (FIGOstage 1b).
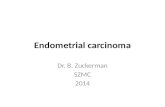
The pathological examination revealed 2 distinct tumor types.Approximately half of the tumor showed a well differentiatedendometrioid adenocarcinoma, without psammoma bodies (Fig. 1a).The remaining parts of the tumor showed a biphasic morphology,containing mononuclear cells and syncytial-like giant cells resemblingchoriocarcinoma (Fig. 1c). There was a close transition from theendometrioid to the choriocarcinomatous areas on several slides (Fig.1b).
Immunohistochemical analysis for CA125 (Dako, clone OC125) andvimentin (Dako, clone V9) were positive in the adenocarcinomatouspart, and human chorionic gonadotropin (Dako, polyclonal) waspositive in the choriocarcinomatous part, especially in the syncytial-like cells. Keratin (Dako, clone AE1, AE3) was positive in bothelements. Syncytial-like cells in the lymphovascular involvementwere stained intensely with hCG.
The preoperative serum β-hCG value was not measured becausechoriocarcinoma was not suspected before surgery. The

Fig. 1. The tumor showed a well differentiated endometrioid adenocarcinoma without psammoma bodies (a), a biphasic morphology, containing mononuclear cells and syncytial-like giant cells (c) and a close transition from the endometrioid to the choriocarcinomatous areas (b). (H&E, bar=100 μm).
292 T. Yamada et al. / Gynecologic Oncology 113 (2009) 291–294
postoperative serum β-hCG values, 19 mIU/mL (post operative day(PO) 15), 28 mIU/mL (PO 18), and 38 mIU/mL (PO 20), wereincreased as compared to before the start of the chemotherapy. Asthe lymphovascular and blood vessel involvements, the increasingserum β-hCG values and the histology (endometrioid adenocarci-noma with choriocarcinomatous differentiation), 5 courses of theCTP (carboplatin, CBDCA; therarubicin, THP; cyclophosphamide,CPA) regimen were selected as the chemotherapy for this uterineendometrial adenocarcinoma case. After the start of chemotherapy,the levels of serum β-hCG decreased to 2.3 mIU/mL (PO 53) andb0.1 mIU/mL (PO 83).
However, 9 months after the surgery, a tumor appeared at thevaginal wall near the vaginal cuff and the serum β-hCG valueincreased again to 1.7 mIU/mL. Histology of the metastatic tumor atthe vagina showed mostly mononuclear cells and syncytial-like giantcells, as choriocarcinoma without any adenocarcinoma component.Thus, chemotherapy was switched to the EMACO (etoposide, VP-16;methotrexate, MTX; actinomycin D, ACD; cyclophosphamide, CPA;vincristine, VCR) regimen, leading to a subsequent decline of the β-hCG values and complete resolution of vaginal metastatic disease after6 courses. Since then, the patient has maintained a disease-free statusand the serum β-hCG values were within normal range for 3 yearsafter the 2nd chemotherapy course. Fifty months have passed sincesurgery.
Discussion
More rarely, true choriocarcinomatous differentiation is seenhistologically in nontrophoblastic tumors, including stomach [1],lung [2], colon [3], esophagus [4], bladder [5], breast [6], and renalpelvis [7], as well as gynecologic cancers. Both syncytiotrophoblastand cytotrophoblast elements, or either one alone, may be present.
When choriocarcinomatous differentiation is seen, hCG can generallybe demonstrated immunohistochemically in the syncytiotrophoblast-like cells of these tumors, and these patients tend to have high serumor urine levels of hCG.
Fifteen cases in the literature have reported histological chor-iocarcinomatous differentiation in malignant uterine tumors. Thirteenof these involved uterine body tumors (11 endometrial cancers [8–15]and 2 carcinosarcomas [16,17]) and 2 involved cervical cancers [18,19],as shown in Table 1. All 15 cases, including the present one,complained of abnormal genital bleeding. In all cases of choriocarci-nomatous element, hCG was demonstrated immunohistochemicallyand all, except for not measured cases, had high levels of serum orurine hCG.
In the 11 endometrial cancer cases, the mean age was 68.9 years(48–88 years), and 9 of the 11 patients were multigravida. As for thehistology of the co-existing tumors, 9 of 11 were endometrioidadenocarcinomas and 2 of these were serous adenocarcinomas. Theprimary tumors included areas of choriocarcinomatous differentia-tion, but in 5 cases of metastatic or recurrent tumors, 2 werechoriocarcinoma, 1 was serous adenocarcinoma, 1 was endometrioidadenocarcinomawithout co-existing histology, and 1was described asthe same as primary tumor. Prognosis is not good because only 2 of 11cases had no evidence of disease.
In the 2 carcinosarcoma cases, both of themwere nulligravida andthe carcinomatous elementswere endometrioid adenocarcinoma. Oneof these patients died of the disease 7 months after initial diagnosis.
In the 2 cervical cancer cases, histology of both cases showedmucinous adenocarcinoma of endocervical type, and 1 of thesepatients died of disease 4 months after surgery.
The pathogenesis of trophoblastic differentiation in nongestationaland non-germ cell tumors is not well understood. It is more difficult tounderstand mixed tumors that are categorically different. Two

Table 1Cases of malignant uterine tumor with choriocarcinomatous differentiation
Author Year Caseno.
Age (y) Gravidityand parity
Coexistingtumor
hCGstain
hCG level Histology atmetastasisor recurrence
Surgery Chemotherapy Irradiation Autopsy Metastasisand invasion
Follow-uptime (mo)
Statusat lastfollow-up
Endometrial carcinomaCivantos andRywlin [8]
1972 1 87 3/2 SPC Positive UrinaryhCG:1000 IU/24 h
ND – – + ND ND ND ND
Savageet al. [9]
1987 2 70 1/1 Well AD Positive – Chorio TAH, BSO Medroxyprogesterone,5FU, DXR, megestrolacetate
+ + Lungs, brain,peritoneum, liver,kidneys
14 DOD
Pesceet al. [10]
1991 3 78 ND/0 Poor AD Positive Serumβ-hCG:19,500 mIU/mL
ND – CDDP, BLM, VCR – – Pelvic lymph nodes 1.5 DOD
4 48 5/ND Poor AD Positive Serumβ-hCG:3050 mIU/mL
ND TAH MTX, VP-16, BLM,CDDP
– ND Lungs ND ND
5 63 Multi/multi AD Positive UrinaryhCG:10,000 IU/24 h
Same asprimary
TAH, BSO – – ND Peritoneum,lungs, liver
14 DOD
Kaliret al. [11]
1995 6 83 0/0 Mod AD Positive SerumhCG:100,000 mIU/mL
ND TAH, BSO CDDP, VP-16 – ND Lungs 1 AWD
Blacket al. [12]
1998 7 88 ND/1 Clear cell AD Positive Serum hCG: 851 IU/L – TAH, BSO – + – None 16 DOD
Bradleyet al. [13]
1998 8 68 4/4 Poor AD,clear AD, SPC
Positive Serumβ-hCG:95 mIU/mL
SPC TAH, BSO, OMT, LD Megestrol acetate,PTX, CBDCA
– – Pelvic lymph nodes 16 NED
Tuncet al. [14]
1998 9 54 6/6 Mod AD Positive Serumβ-hCG:5514 mIU/mL
AD TAH, BSO MTX, CPA, ACD,VP-16,folinik acid
– – Retroperitonealmass
24 DOD
Hornet al. [15]
2006 10 61 3/3 SPC Positive SerumhCG:225,000 IU/Lpostoperation
ND TAH, BSO, LD MTX, EMACO(VP-16,MTX,ACD, CPA, VCR)
– – Lungs 3 DOD
Present case 2008 11 58 1/1 Well AD Positive Serumβ-hCG:38 ng/mLpostoperation
Chorio TAH, BSO, LD CBDCA, THP, CPA,EMACO(VP-16, MTX,ACD, CPA, VCR)
– – Vaginal cuff 36 NED
CarcinosarcomaKhuuet al. [16]
2000 1 71 0/0 Carcinosarcoma Positive SerumhCG: 283 mIU/mLpostoperation
– TAH, BSO, LD – – Alive None 8 NED
Nguyenet al. [17]
2000 2 34 0/0 Carcinosarcoma Positive Serumβ-hCG:32,000 mIU/mL
Chorio TAH, BSO, OMT, LD BLM, VP-16, CDDP,EMACO (VP-16, MTX,ACD, CPA, VCR),CDDP, PTX
+ – Lungs, brain,para-aortic lymphnode
7 DOD
Cervical carcinomaCollinset al. [18]
1989 1 39 5/4 Mucinous AD Positive Serumβ-hCG:30 mIU/mL
– TAH, BSO, LD – + Alive – 28 NED
Shintakuet al. [19]
2000 2 65 0/0 Mucinous AD,hepatoidcarcinoma
Positive Serumβ-hCG:113 ng/mLpostoperation
ND TAH, BSO CDDP, PTX ND – Lungs 4 DOD
ND: not described. SPC: serous papillary carcinoma. AD: adenocarcinoma. well: well differentiated. mod: moderately differentiated. poor: poorly differentiated. hCG: human chorionic gonadotropin. chorio: choriocarcinoma. TAH: totalabdominal hysterectomy. BSO: bilateral salpingo-oophorectomy. OMT: omentectomy. LD: lymphadenectomy. 5-FU: 5-fluorouracil. DXR: doxorubicin. CDDP: cisplatin. BLM: bleomycin. VP-16: etoposide. PTX: paclitaxel. CBDCA: carboplatin.MTX: methotrexate. CPA: cyclophosphamide. ACD: actinomycin D. VCR: vincristine. THP: therarubicin. DOD: dead of the disease. AWD: alive with the disease. NED: no evidence of the disease.
293T.Yam
adaet
al./Gynecologic
Oncology
113(2009)
291–294

294 T. Yamada et al. / Gynecologic Oncology 113 (2009) 291–294
popular hypotheses regarding the origin of extragenital or nongesta-tional choriocarcinoma are both based on the “embryonic rest” theory[17]. The first theory suggests that a group of germ cells, coming to restin the region of the urogenital ridge, fails to complete their migrationto the gonadal tissue, and subsequently undergo malignant transfor-mation. The second theory suggests that nests of totipotent germ cellsare left in ectopic sites outside the urogenital ridge during earlyembryonal development, fail to undergo apoptosis, and then subse-quently transform into choriocarcinoma. This would explain chor-iocarcinomas originating from organs remote from the urogenitaltract. A third theory, supported by recent molecular analyses of thetumors [1,7], suggests that a tumor consisting of adult tissue elementsmay undergo retrodifferentiation or dedifferentiation, resulting incells with different morphological features, for example, trophoblasticand nontrophoblastic differentiations.
We thought that adenocarcinoma was basic histology and chosethe regimen for endometrioid adenocarcinoma in this case. Actuallythe serum β-hCG decreased to the normal range once. Although therecurrent tumor appeared after that, the regimen for choriocarcinomalead to a complete resolution, since the histology was onlychoriocarcinoma. The prognosis depends on the sensitivity of thechemotherapy. As the histology of the recurrent tumor is bothadenocarcinoma and choriocarcinoma in previous reports, it wouldbe necessary to use the regimen which is sensitive to both of them.
Urine and serum hCG levels are not routinely used as tumormarkers in preoperative testing for malignant uterine tumors. Whenchoriocarcinoma was suspected in a biopsy or cytology of endome-trium, hCG should be measured. For uterine adenocarcinoma withchoriocarcinomatous differentiation, treatment and follow-up mustbe done not only for adenocarcinoma but also for the choriocarcinomaelement.
Conflict of interest statementThe authors declare that there are no conflicts of interest.
References
[1] Liu AY, Chan WY, Ng EK, Zhang X, Li BC, Chow JH, et al. Gastric choriocarcinomashows characteristics of adenocarcinoma and gestational choriocarcinoma: acomparative genomic hybridization and fluorescence in situ hybridization study.Diagn Mol Pathol 2001 Sep;10(3):161–5.
[2] Yoshimoto T, Higashino K, Hada T, Tamura S, Nakanishi K, Mitsunobu M, et al. Aprimary lung carcinoma producing alpha-fetoprotein, carcinoembryonic antigen,and human chorionic gonadotropin. Immunohistochemical and biochemicalstudies. Cancer 1987 Dec 1;60(11):2744–50.
[3] Verbeek W, Schulten HJ, Sperling M, Tiesmeier J, Stoop H, Dinjens W, et al. Rectaladenocarcinoma with choriocarcinomatous differentiation: clinical and geneticaspects. Human Pathol 2004 Nov;35(11):1427–30.
[4] McKechnie JC, Fechner RE. Choriocarcinoma and adenocarcinoma of theesophagus with gonadotropin secretion. Cancer 1971 Mar;27(3):694–702.
[5] Obe JA, Rosen N, Koss LG. Primary choriocarcinoma of the urinary bladder.Report of a case with probable epithelial origin. Cancer 1983 Oct 15;52(8):1405–9.
[6] Resetkova E, Sahin A, Ayala AG, Sneige N. Breast carcinoma with choriocarcino-matous features. Ann Diagn Pathol 2004 Apr;8(2):74–9.
[7] Zettl A, Konrad MA, Polzin S, Ehsan A, Riedmiller H, Muller-Hermelink HK,et al. Urothelial carcinoma of the renal pelvis with choriocarcinomatousfeatures: genetic evidence of clonal evolution. Human Pathol 2002 Dec;33(12):1234–7.
[8] Civantos F, Rywlin AM. Carcinomas with trophoblastic differentiation andsecretion of chorionic gonadotrophins. Cancer 1972 Mar;29(3):789–98.
[9] Savage J, Subby W, Okagaki T. Adenocarcinoma of the endometrium withtrophoblastic differentiation and metastases as choriocarcinoma: a case report.Gynecol Oncol 1987 Feb;26(2):257–62.
[10] Pesce C, Merino MJ, Chambers JT, Nogales F. Endometrial carcinoma withtrophoblastic differentiation. An aggressive form of uterine cancer. Cancer 1991Oct 15;68(8):1799–802.
[11] Kalir T, Seijo L, Deligdisch L, Cohen C. Endometrial adenocarcinoma withchoriocarcinomatous differentiation in an elderly virginal woman. Int J GynecolPathol 1995 Jul;14(3):266–9.
[12] Black K, Sykes P, Ostor AG. Trophoblastic differentiation in an endometrialcarcinoma. Aust N Z J Obstet Gynaecol 1998 Nov;38(4):472–3.
[13] Bradley CS, Benjamin I, Wheeler JE, Rubin SC. Endometrial adenocarcinoma withtrophoblastic differentiation. Gynecol Oncol 1998 Apr;69(1):74–7.
[14] Tunc M, Simsek T, Trak B, Uner M. Endometrium adenocarcinoma withchoriocarcinomatous differentiation: a case report. Eur J Gynaecol Oncol 1998;19(5):489–91.
[15] Horn LC, Hanel C, Bartholdt E, Dietel J. Serous carcinoma of the endometriumwithchoriocarcinomatous differentiation: a case report and review of the literatureindicate the existence of 2 prognostically relevant tumor types. Int J GynecolPathol 2006 Jul;25(3):247–51.
[16] Khuu HM, Crisco CP, Kilgore L, Rodgers WH, Conner MG. Carcinosarcoma of theuterus associated with a nongestational choriocarcinoma. South Med J 2000Feb;93(2):226–8.
[17] Nguyen CP, Levi AW, Montz FJ, Bristow RE. Coexistent choriocarcinoma andmalignant mixed mesodermal tumor of the uterus. Gynecol Oncol 2000 Dec;79(3):499–503.
[18] Collins RJ, Wong LC. Adenocarcinoma of the uterine cervix with beta-hCGproduction: a case report and review of the literature. Gynecol Oncol 1989Apr;33(1):99–107.
[19] Shintaku M, Kariya M, Shime H, Ishikura H. Adenocarcinoma of the uterine cervixwith choriocarcinomatous and hepatoid differentiation: report of a case. Int JGynecol Pathol 2000 Apr;19(2):174–8.