ENDOCRINE SYSTEM Chapter 16. Endocrine vs Nervous System NERVOUSENDOCRINE Uses action potentials...
72
ENDOCRINE SYSTEM Chapter 16
-
Upload
jayson-gaines -
Category
Documents
-
view
227 -
download
2
Transcript of ENDOCRINE SYSTEM Chapter 16. Endocrine vs Nervous System NERVOUSENDOCRINE Uses action potentials...

ENDOCRINE SYSTEM
Chapter 16

Endocrine vs Nervous System
NERVOUS ENDOCRINE• Uses action potentials along axons & chemical neurotransmitters at synapses
• Uses chemical hormones released from glands into the blood
• Receptors are on post-synaptic membrane
• Receptors are on the plasma membranes of target cells or intercellular
• Signals are very fast (milliseconds)
• Signals are slower (seconds to days)
• Response is immediate but short-lived
• Response is delayed but more sustained

HORMONES
• Hormones – chemical substances secreted by cells into blood stream–Regulate metabolic function of other cells
–Are either peptides or steroids

Hormone - Target Cell Specificity
•circulate to all tissues but affect activity of only certain cells, these are their target cells
•specificity of effect governed by hormone receptors

Characteristics of Hormones
• Hormones:– exert effects some distance from where
produced– active at very low (pg to ng) concentrations in
the blood– have short half-life in body - secs to mins

Characteristics of Hormones
• their effect is to alter cell activity. The precise response depends on the target cell type. Typical cellular effects include:–Altering plasma membrane permeability
–Stimulating protein synthesis–Activating enzymes–Inducing secretory activity–Stimulating mitosis

Control of Hormone Release
•Synthesis & release of most hormones are regulated by negative feedback. –As hormone levels rise, they cause target organ effects that inhibit hormone release.

Chemical Classes of Hormones
• Amines - Derived from tyrosine or tryptophan. Includes: epinephrine, T4, & melatonin.
• Proteins & peptides - Made from amino acid chains. Includes: antidiuretic hormone, growth hormone, & insulin.
• Glycoproteins - A polypeptide chain bound to one or more carbohydrates. Includes: follicle-stimulating hormone & luteinizing hormone.
• Steroids - Lipids derived from cholesterol. Includes: testosterone, estradiol, & cortisol.

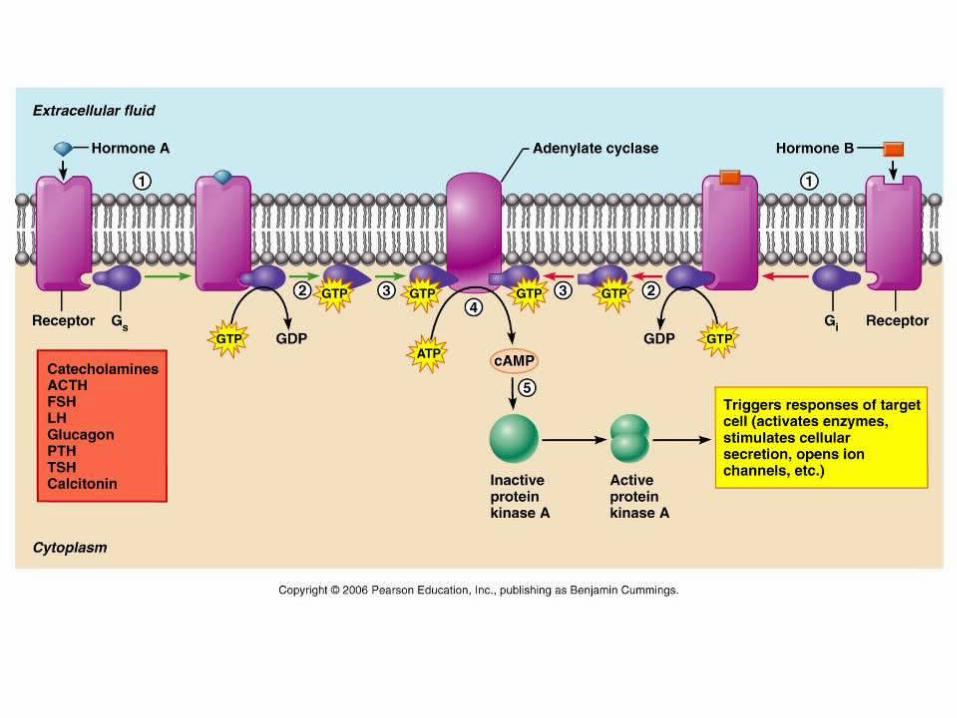
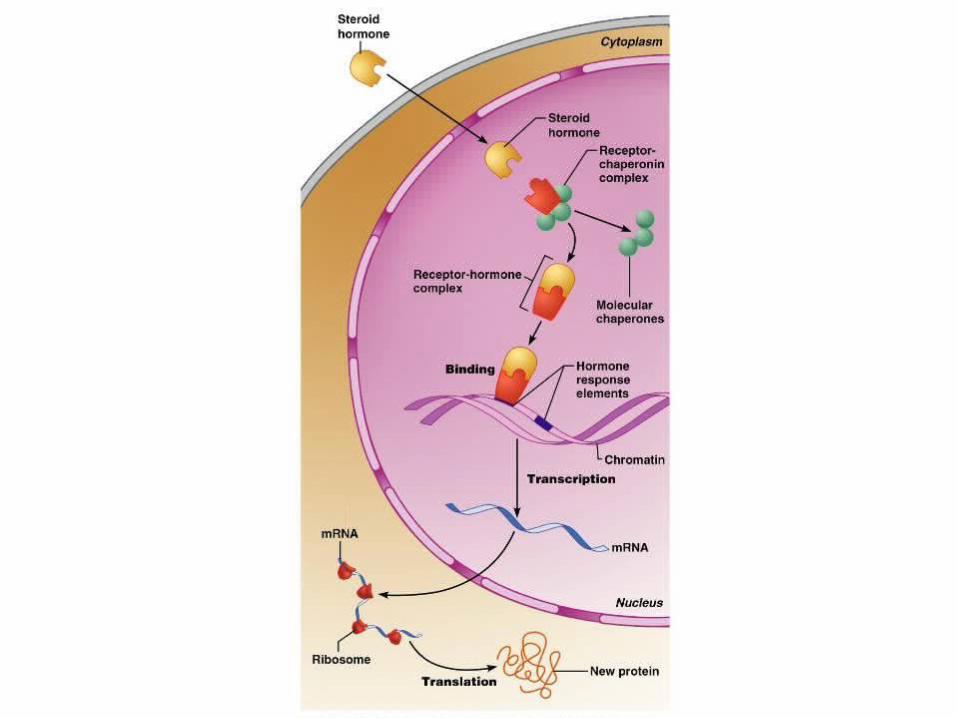
Mechanisms of Hormone Action
•Hormones:–Diffuse through the cell membrane & bind to intracellular receptors (steroid hormones & T4) or bind to receptors on the membrane of distant cells (amino-acid based hormones).
–Carry out their effects by direct gene activation (steroids) or through signal transduction systems (amino-acid based).


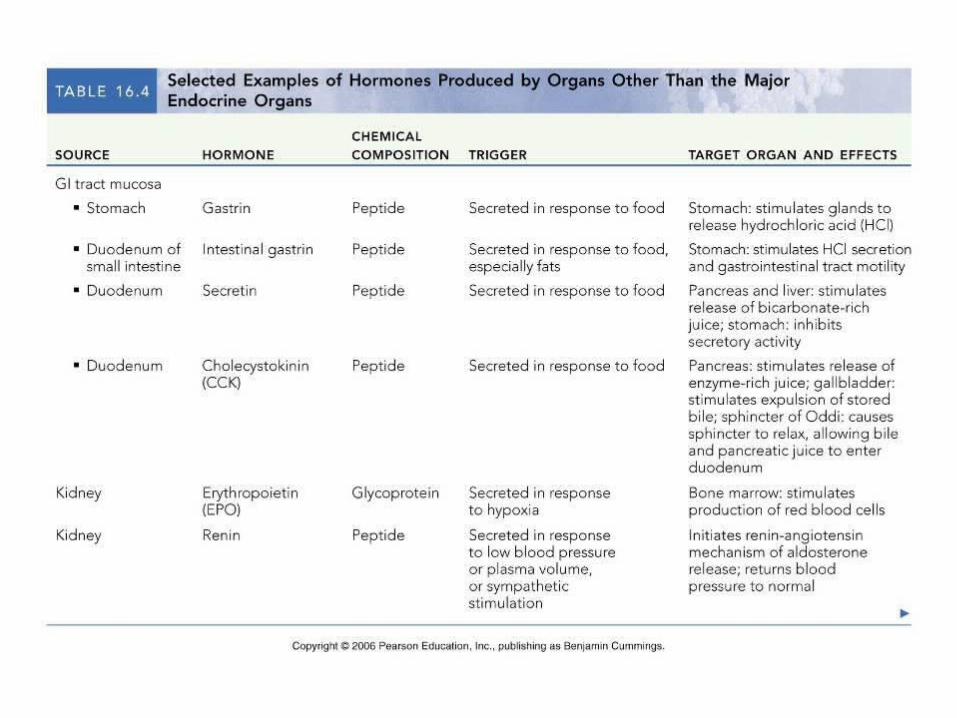
Distribution of Endocrine Tissue
•Specialized organs (pituitary, adrenal, thyroid)
•Discrete clusters within other organs (pancreas, gonads)
•Cells dispersed singly within other tissues (enteroendocrine cells)



GLAND HORMONEREGULATION OF RELEASE
TARGET ORGAN
NORMAL EFFECTS OF HORMONE
EFFECTS OF HYPER- & HYPOSECRETION




Adenohypophysis(anterior pituitary)
Neurohypophysis(posterior pituitary)





GROWTH HORMONE
• Gigantism - a hypersecretion of growth hormone during infancy, childhood or adolescence, while epiphyseal growth plates remain open.
12 year-old with mother

GROWTH HORMONE
• Acromegaly - GH hypersecretion in adulthood, when epiphyseal plates are closed.
Large, spade-like hands of acromegaly

GROWTH HORMONE
• Dwarfism - GH deficiency in childhood, leading to a maximum height of 4 feet with normal body proportions.
Dwarfed brothers with researcher in India




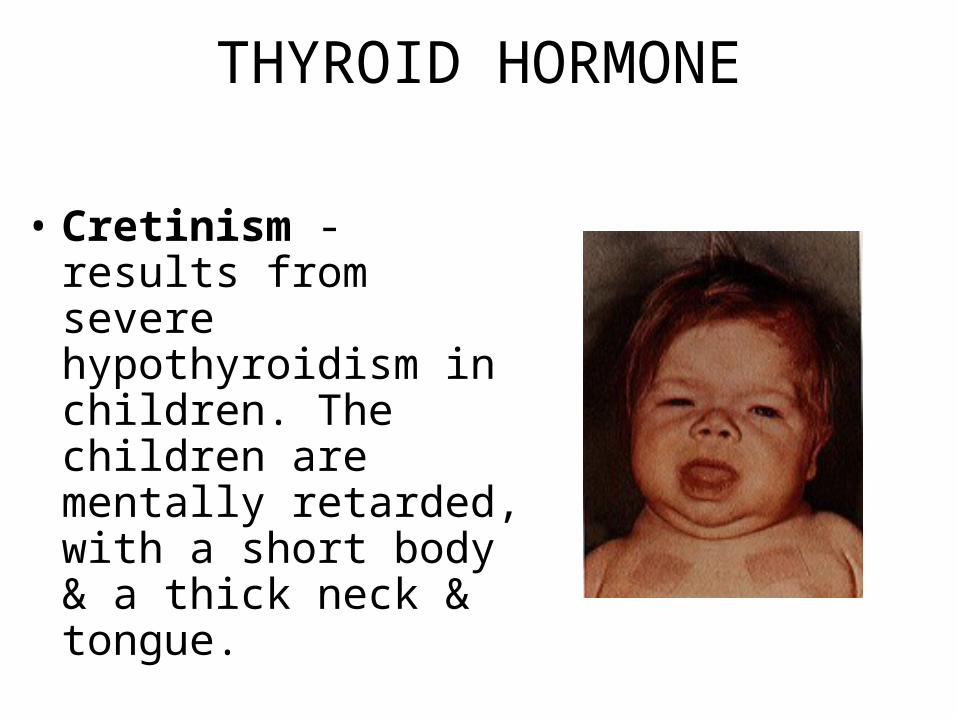
THYROID HORMONE
• Cretinism - results from severe hypothyroidism in children. The children are mentally retarded, with a short body & a thick neck & tongue.

THYROID HORMONE
• Myxedema - Due to hypothyroidism in adults. Symptoms of low metabolic rate, chills, lethargy, mental sluggishness, & swelling of body tissues.
Swelling associated with myxedema

THYROID HORMONE
• If myxedema results from a lack of iodine, the thyroid enlarges & protrudes into a condition called goiter.
THYROID HORMONE
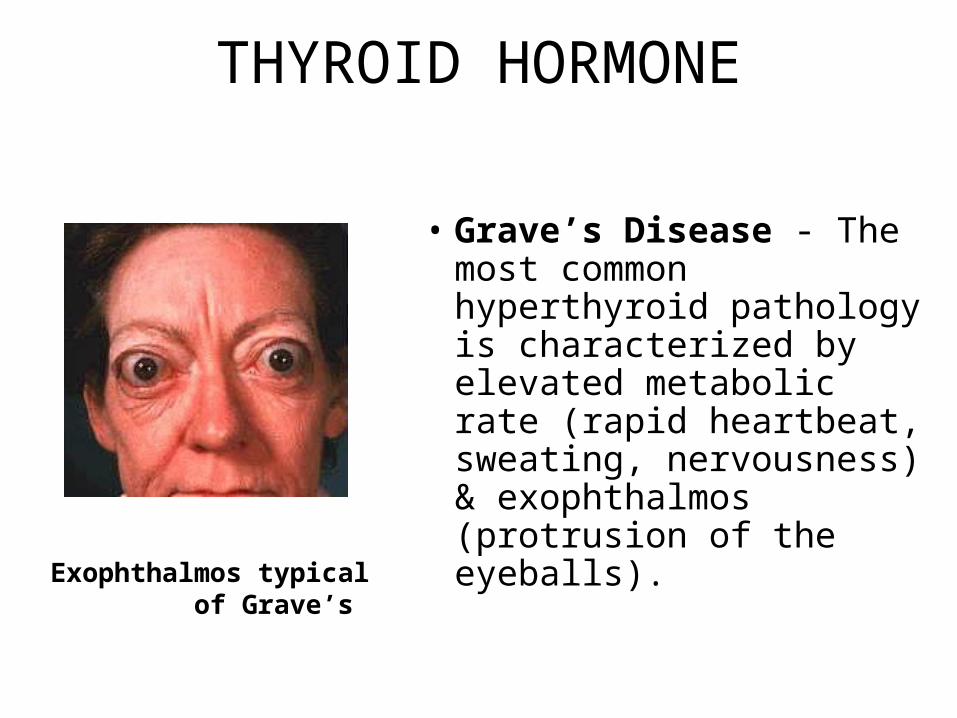
• Grave’s Disease - The most common hyperthyroid pathology is characterized by elevated metabolic rate (rapid heartbeat, sweating, nervousness) & exophthalmos (protrusion of the eyeballs).Exophthalmos typical
of Grave’s




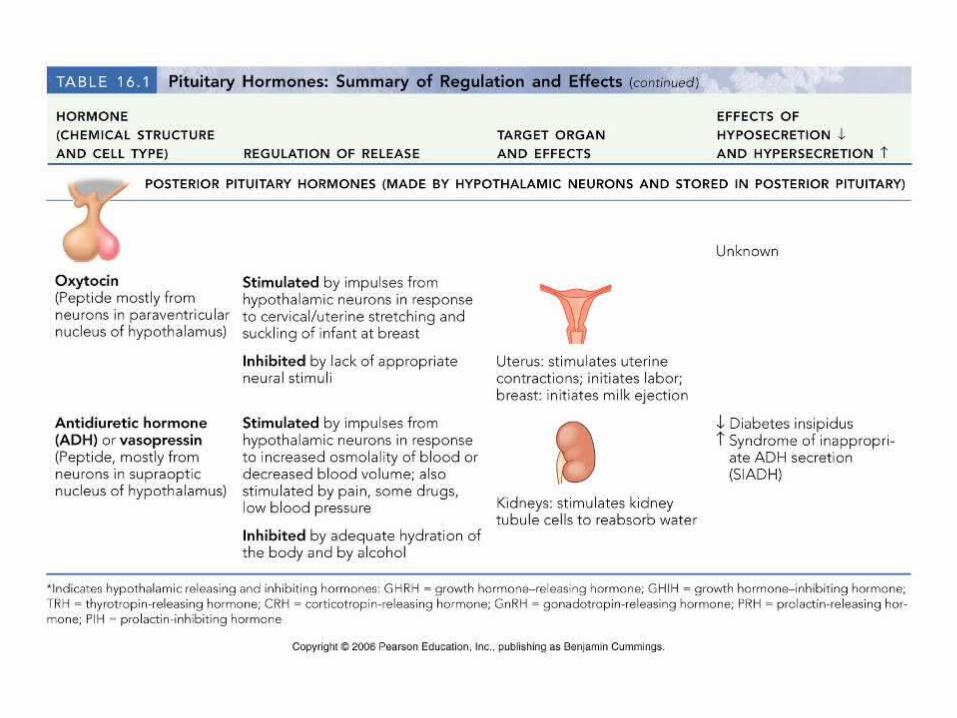

ANTIDIURETIC HORMONE
• Diabetes insipidus is a result of ADH deficiency, a syndrome marked by intense thirst & very high urine output

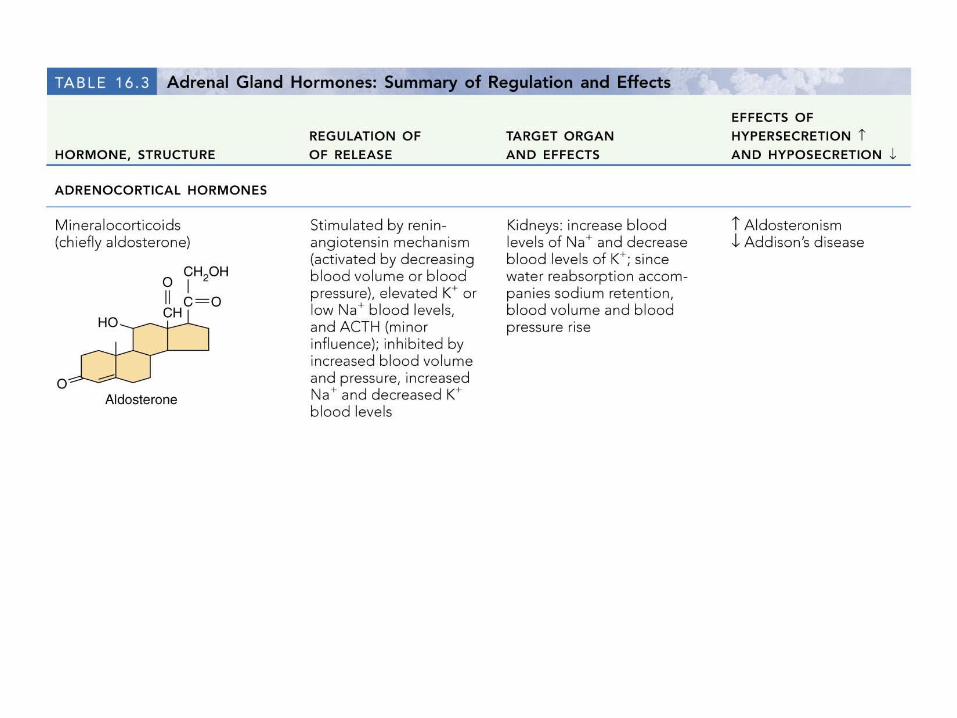

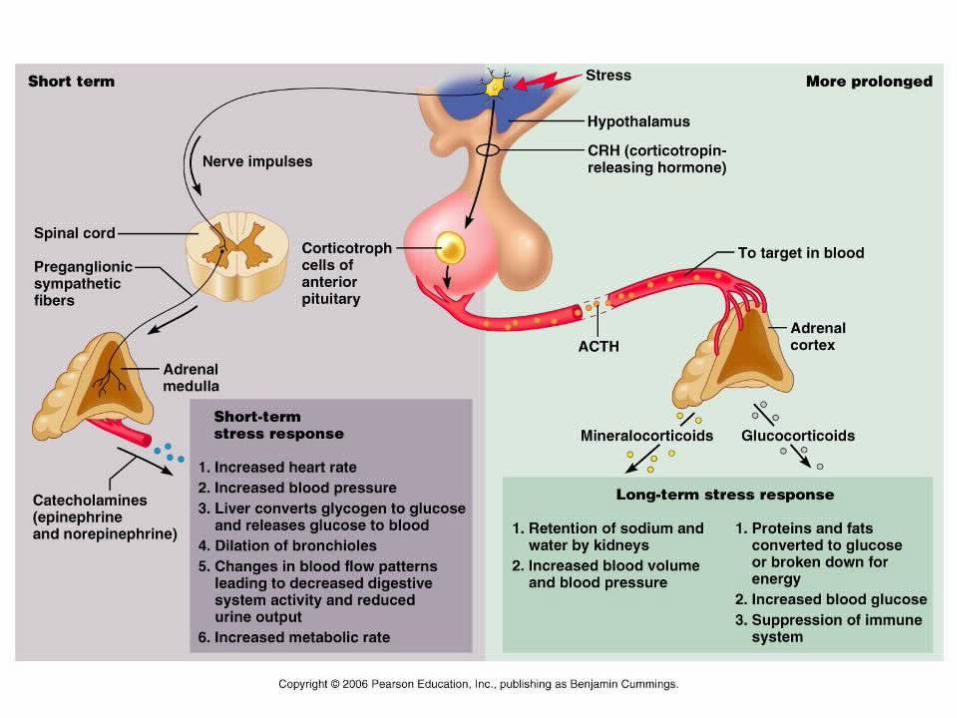
Routes of Aldosterone Stimulation

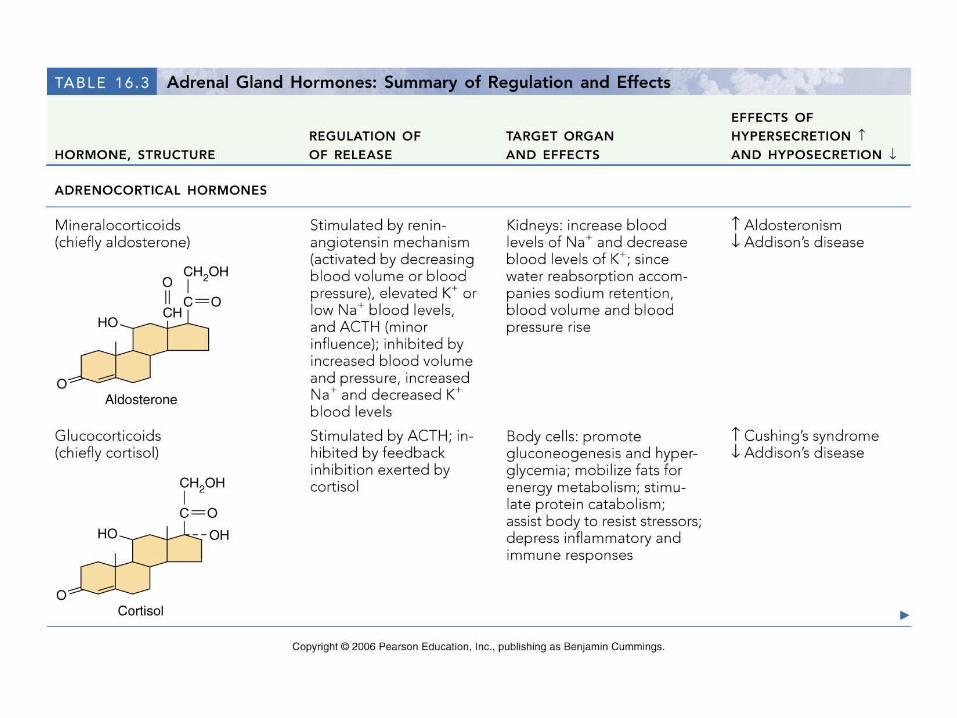
GLUCOCORTICOIDS• At high concentrations, cortisol has pronounced anti-inflammatory & anti-immune effects including:–Depressing cartilage & bone formation
–Inhibiting inflammation by stabilizing lysosomal membranes

GLUCOCORTICOIDS
• Cushing’s disease - results from glucocorticoid excess. Symptoms include persistent hyperglycemia, a moon face, & a redistribution of fat to the abdomen & posterior neck (causing a “buffalo hump”).
GLUCOCORTICOIDS
• Addison’s disease - the major hyposecretory disorder of the adrenal cortex, usually involving both glucocorticoids & mineralcorticoids. Patients have low blood sugar & sodium, & Caucasians show an increase in skin pigmentation (bronzing)
JFK had Addison’s, which he kept from public knowledge
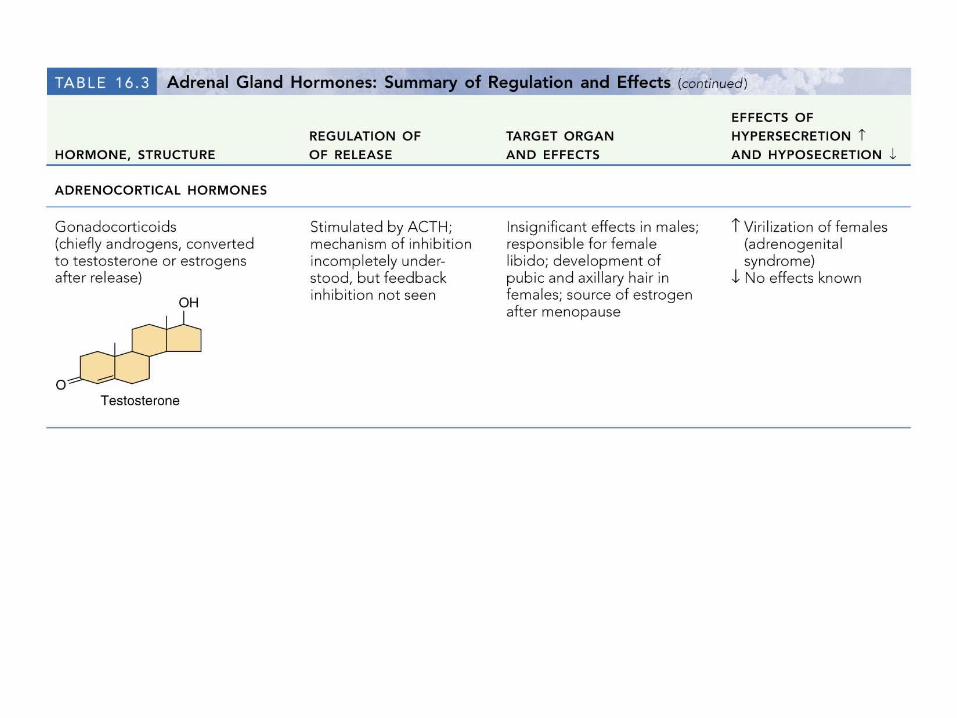

GONADOCORTICOIDS
• Androgenital syndrome is due to hypersecretion of androgens. Most often apparent in women, it manifests itself in hirsutism (including beard development).
Olga Roderick, the “Bearded Lady”


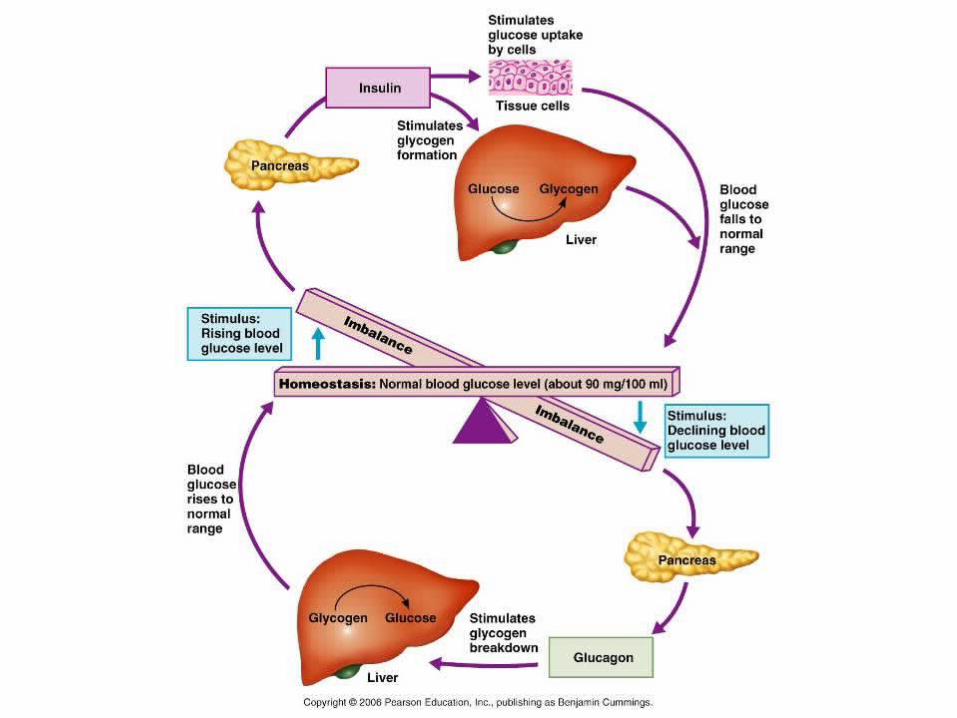
Pancreatic Hormones


INSULIN•After glucose enters a target cell, insulin binding triggers enzymatic activity that:–Catalyze the oxidation of glucose for ATP production
–Join glucose molecules together to form glycogen
–Convert excess glucose to fat

INSULIN
• Diabetes mellitus - Due to hyposecretion (Type I) or hypoactivity (Type II) of insulin. When insulin is absent or deficient, blood sugar levels remain high after a meal because glucose is unable to enter most tissue cells.
DIABETES• Type I (insulin-dependent) - afflicts 1.5 million Americans.–Autoimmune disease (beta cells are attacked by immune cells).
–Insulin is not produced or secreted, requiring regular injections.

DIABETES•Type II (non-insulin-dependent) -afflicts 19 million Americans.–Insulin resistance - Insulin is usually produced but the receptors do not respond.
–Heredity & lifestyle both play roles in the disease.

DIABETES•Three clinical signs of diabetes:–Hyperglycemia -normal blood sugar should be 80 - 120 mg/dl.
–Glucosuria - glucose spills into the urine at high blood concentrations (300 mg/dl).
–Ketoacidosis & ketouria - as sugar is not available for fuel & lipolysis accelerates.

DIABETES• Three cardinal signs of diabetes (the three polys):
Polyuria - excessive urination; glucosuria leads to osmotic diuresis & dehydrationPolydipsia - excessive thirst, caused by dehydrationPolyphagia - ravenous hunger & food consumption, a sign the person is “starving in the land of plenty”
PINEAL GLAND
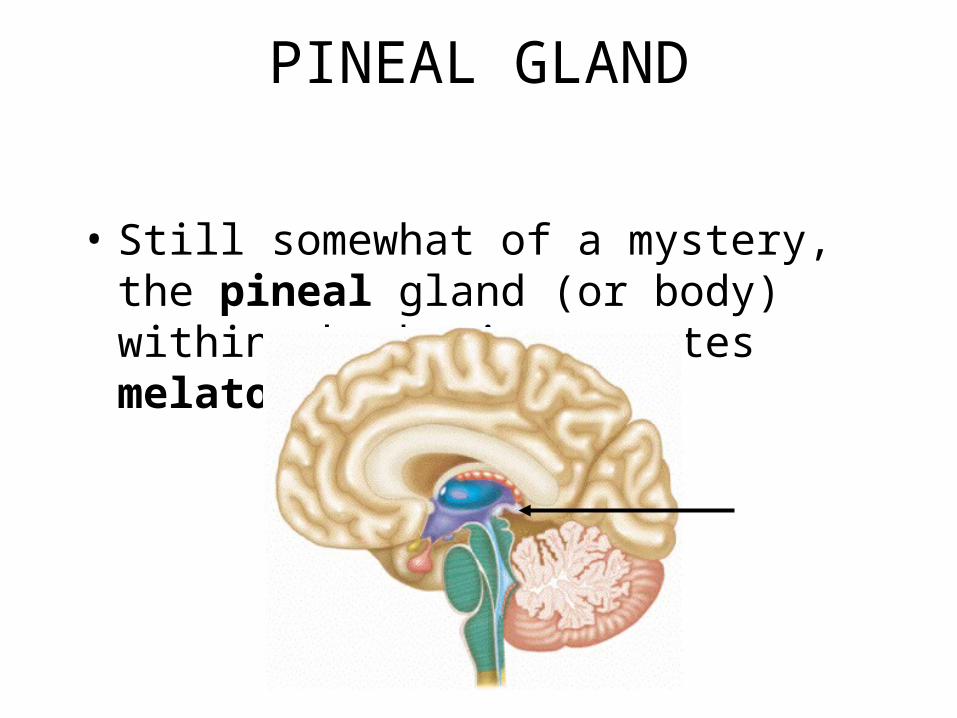
• Still somewhat of a mystery, the pineal gland (or body) within the brain secretes melatonin.

MELATONIN
• Melatonin - made from the neurotransmitter serotonin, a derivative of the amino acid tryptophan.– Levels peak at night & fall in the daytime
– Changing melatonin levels may influence physiological processes that show rhythmic variation: sleep, body temperature, & appetite
MELATONIN
• Seasonal affective disorder (SAD) has been linked to elevated melatonin levels in the winter months for people in northern latitudes like Alaska. It may lead to depression, long bouts of sleeping, & eating binges.
The Midnight Sun