
Endocarditis
31
Infective Infective Endocarditis Endocarditis
-
Upload
husnawaty-dayu -
Category
Documents
-
view
12 -
download
0
description
endocarditis
Transcript of Endocarditis
Infective EndocarditisInfective Endocarditis

ObjectivesObjectives
Describe the incidence of IE in various Describe the incidence of IE in various heart conditions.heart conditions.Review the Duke criteria of infective Review the Duke criteria of infective endocarditisendocarditisReview the indications for prophylaxis and Review the indications for prophylaxis and current recommendations for antimicrobial current recommendations for antimicrobial therapy.therapy.Review the efficacy and controversies in Review the efficacy and controversies in IE prophylaxis.IE prophylaxis.

BackgroundBackground
Relatively rare in childrenRelatively rare in children
Pre-antibiotic era: mortality was nearly Pre-antibiotic era: mortality was nearly 100%100%
Mortality approaches 15-25%Mortality approaches 15-25%
EpidemiologyEpidemiology
Increasing incidence beginning in the ‘80sIncreasing incidence beginning in the ‘80s– Increasing number of surgical patientsIncreasing number of surgical patients– Increasing number of complex congenital Increasing number of complex congenital
heart diseaseheart disease– Increased use of prosthetic materialsIncreased use of prosthetic materials– NICUs and PICUs NICUs and PICUs
Pathogenesis, Part 1Pathogenesis, Part 1
Damaged endotheliumDamaged endothelium– undamaged endothelium not conducive to undamaged endothelium not conducive to
bacterial colonizationbacterial colonization– endothelium can be damaged by high-velocity endothelium can be damaged by high-velocity
flowsflows– trauma to endothelium can induce trauma to endothelium can induce
thrombogenesis, leading to nonbacterial thrombogenesis, leading to nonbacterial thrombotic endocarditis (NBTE). NBTE is thrombotic endocarditis (NBTE). NBTE is more receptive to colonizationmore receptive to colonization

Heart disease and IEDisease No. %
Acyanotic Heart DiseaseVSD 194 21.8Aortic stenosis 89 10.0PDA 25 2.8Coarctation of the aorta 25 2.8Pulmonary stenosis 21 2.4VSD with other defects 18 2.0Atrioventricular septal defect 16 1.8Mitral valve abnormality 16 1.8Atrial septal defect 11 1.2Mitral valve prolapse 8 0.9
Cyanotic Heart DiseaseTetralogy of Fallot 143 16.0Transposition of Great Vessels 35 3.9Tricuspid Atresia 9 1.0
Rheumatic Heart Disease 86 9.7No Heart Disease 75 8.4
Berkowitz, FE: Infective endocarditis. IN Nichols EG, Cameron DE, Greeley WJ, et al (eds):Critical Heart Disease in Infants and Children. St. Louis, Mosby-Year Book, 1995.

Pathogenesis, Part 2Pathogenesis, Part 2Microorganism No. %
Streptococcus viridans 289 31.3
Staphylococcus aureus 225 24.4
Negative cultures 152 16.4
Other streptoccal species (e.g. enterococci) 55 5.9
HACEK and diphtheroids 50 5.4
Gram negative bacilli 45 4.8
Strept pneumoniae 18 1.9
Fungi 14 1.5
Others 28 3.0
Berkowitz, FE: Infective endocarditis. IN Nichols EG, Cameron DE, Greeley WJ, et al (eds):Critical Heart Disease in Infants and Children. St. Louis, Mosby-Year Book, 1995.

MicrobiologyMicrobiology
S. ViridansS. Viridans– Most common causative organismMost common causative organism
Gram negative bacilliGram negative bacilli– Neonates and immunocompromised patientsNeonates and immunocompromised patients
Prosthetic valvesProsthetic valves– Within first year of surgery: Coag-negative staphWithin first year of surgery: Coag-negative staph– After first year: similar to native valve endocarditisAfter first year: similar to native valve endocarditis
HACEK organismsHACEK organisms– Hemophilus, Actinobacillus, Cardiobacterium, Eikenella, Hemophilus, Actinobacillus, Cardiobacterium, Eikenella,
KingellaKingella– Frequently affect damaged valves and can cause emboliFrequently affect damaged valves and can cause emboli

DiagnosisDiagnosis
Traditionally based upon “positive blood Traditionally based upon “positive blood cultures in the presence of a new or cultures in the presence of a new or changing heart murmur”, or persistent changing heart murmur”, or persistent fever in the presence of heart disease.fever in the presence of heart disease.
Shortcomings include culture-negative Shortcomings include culture-negative endocarditis, lack of typical endocarditis, lack of typical echocardiographic findings, etc.echocardiographic findings, etc.
Duke CriteriaDuke Criteria
Based on pathological and clinical criteria.Based on pathological and clinical criteria.
Utilizes microbiological data, evidence of Utilizes microbiological data, evidence of endocardial involvement, and other phenomenon endocardial involvement, and other phenomenon associated with infective endocarditis to estimate associated with infective endocarditis to estimate the probability of infective endocarditis in a given the probability of infective endocarditis in a given patient.patient.
Has been shown to be valid and reproducible in Has been shown to be valid and reproducible in childrenchildren
Durack DT, Lukes AS, Bright DK. New criteria for diagnosis of infective endocarditis: utilization of specific echocardiographic findings. AM J Med 96:200, 1994
Stockheim JA, Chadwick EG, Kessler S, et al. Are the Duke Criteria superior to the Beth Israel criteria for the diagnosis of infective endocarditis in children? Clin Infect Dis 27:1451, 1998

Duke criteriaDuke criteriaDefinitiveDefinitive– Pathological criteriaPathological criteria
Microorganisms, Microorganisms, oror
Pathologic lesionsPathologic lesions– Clinical criteriaClinical criteria
2 major criteria, 2 major criteria, oror
1 major and 3 minor criteria, 1 major and 3 minor criteria, oror
5 minor5 minor
PossiblePossible
– Findings consistent with infective endocarditis that fall short of “definitive” but are not Findings consistent with infective endocarditis that fall short of “definitive” but are not “rejected”“rejected”
RejectedRejected– Firm alternative diagnosis, Firm alternative diagnosis, oror– Resolution of manifestations of endocarditis with antibiotic therapy of 4 days or less, Resolution of manifestations of endocarditis with antibiotic therapy of 4 days or less, oror– No pathological evidence of endocarditis at surgery or autopsy with antibiotic therapy No pathological evidence of endocarditis at surgery or autopsy with antibiotic therapy
of 4 days or lessof 4 days or less
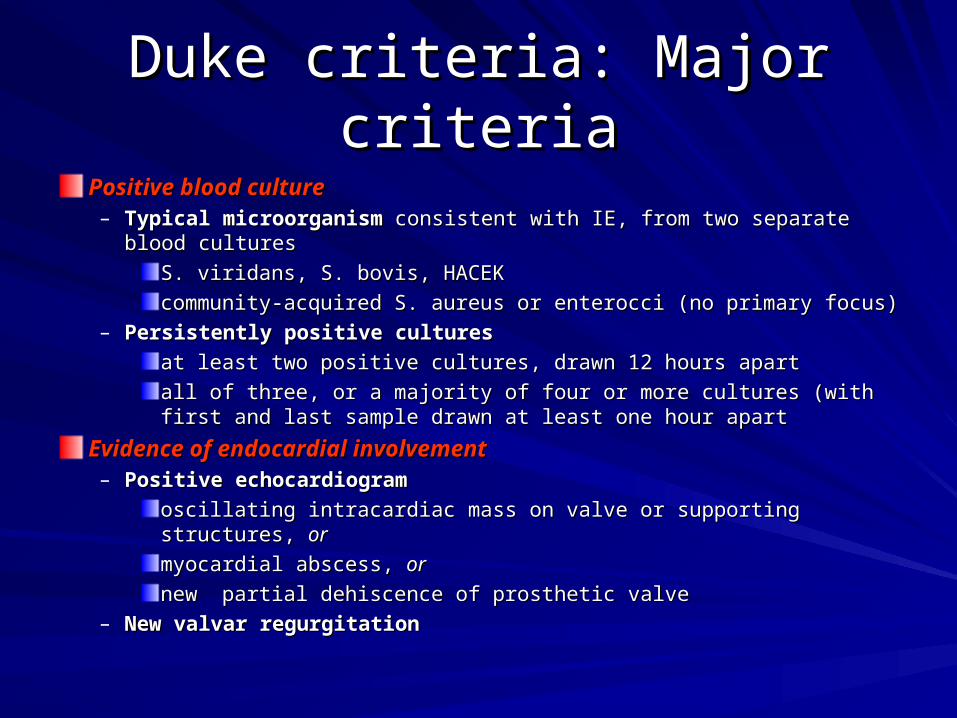
Duke criteria: Major criteriaDuke criteria: Major criteria
Positive blood culturePositive blood culture– Typical microorganismTypical microorganism consistent with IE, from two separate blood consistent with IE, from two separate blood
culturescultures
S. viridans, S. bovis, HACEKS. viridans, S. bovis, HACEK
community-acquired S. aureus or enterocci (no primary focus)community-acquired S. aureus or enterocci (no primary focus)– Persistently positive culturesPersistently positive cultures
at least two positive cultures, drawn 12 hours apartat least two positive cultures, drawn 12 hours apart
all of three, or a majority of four or more cultures (with first and last all of three, or a majority of four or more cultures (with first and last sample drawn at least one hour apartsample drawn at least one hour apart
Evidence of endocardial involvementEvidence of endocardial involvement– Positive echocardiogramPositive echocardiogram
oscillating intracardiac mass on valve or supporting structures, oscillating intracardiac mass on valve or supporting structures, oror
myocardial abscess, myocardial abscess, oror
new partial dehiscence of prosthetic valvenew partial dehiscence of prosthetic valve– New valvar regurgitationNew valvar regurgitation

Duke criteria: Minor criteriaDuke criteria: Minor criteriaPredispositionPredisposition– Predisposing heart condition or IV Predisposing heart condition or IV
drug abuserdrug abuserFeverFever– > 38.0º C > 38.0º C
Vascular phenomenaVascular phenomena– arterial emboli, septic pulmonary arterial emboli, septic pulmonary
infarct, mycotic aneurysm, infarct, mycotic aneurysm, intracranial hemorrhage, conjunctival intracranial hemorrhage, conjunctival hemorrhage, Janeway’s lesionhemorrhage, Janeway’s lesion
Immunologic phenomenaImmunologic phenomena– glomerulonephritis, Osler’s nodes, glomerulonephritis, Osler’s nodes,
Roth’s spots, rheumatoid factors Roth’s spots, rheumatoid factors Microbiologic evidenceMicrobiologic evidence– positive blood culture but does not positive blood culture but does not
meet major criteria as noted meet major criteria as noted Echocardiographic evidenceEchocardiographic evidence– consistent with IE but does not meet consistent with IE but does not meet
major criteria as notedmajor criteria as noted
SequelaeSequelae
Neurologic manifestations, 20%Neurologic manifestations, 20%– Cerebral emboli, mycotic aneurysms, Cerebral emboli, mycotic aneurysms,
cerebritis, brain abscess, hemorrhage, etc.cerebritis, brain abscess, hemorrhage, etc.
Peripheral embolizationPeripheral embolization– Ischemia, infarction, mycotic aneurysms, etcIschemia, infarction, mycotic aneurysms, etc
Pulmonary infarctionPulmonary infarction
Renal insufficiencyRenal insufficiency
Congestive heart failureCongestive heart failure

Treatment of infective Treatment of infective
endocarditisendocarditis GENERAL CONSIDERATIONSGENERAL CONSIDERATIONS
Antimicrobial therapy should be Antimicrobial therapy should be administered in a dose designed to give administered in a dose designed to give sustained bactericidal serum sustained bactericidal serum concentrations throughout much or all concentrations throughout much or all of the dosing intervalof the dosing interval
In vitro determination of the minimum In vitro determination of the minimum inhibitory concentration of the etiologic inhibitory concentration of the etiologic cause of the endocarditis should be cause of the endocarditis should be performed in all patientsperformed in all patients
Treatment of infective Treatment of infective endocarditisendocarditis
GENERAL CONSIDERATIONSGENERAL CONSIDERATIONS The duration of therapy has to be The duration of therapy has to be
sufficient to eradicate microorganisms sufficient to eradicate microorganisms growing within the valvular vegetationsgrowing within the valvular vegetations
The need for prolonged therapy in The need for prolonged therapy in treating endocarditis has stimulated treating endocarditis has stimulated interest in using combination therapy to interest in using combination therapy to treat endocarditistreat endocarditis

VIRIDANS STREPTOCOCCI AND STREP. BOVISAntibiotic Antibiotic Dosage and routeDosage and route Duration Duration CommentsComments
Aqueous crystallineAqueous crystalline 12-18 million U/24 h12-18 million U/24 h 4 wks 4 wks preferred in most patients older than 65 yrspreferred in most patients older than 65 yrs
penicillin G sodiumpenicillin G sodium IV either continuouslyIV either continuously and in those with impairment of the and in those with impairment of the eightheighth
or in 6 = divided doses or in 6 = divided doses nerve or renal function nerve or renal function
oror
Ceftriaxone sodiumCeftriaxone sodium 2g once daily IV or IM2g once daily IV or IM 2 wks 2 wks
Aqueous crystallineAqueous crystalline 12-18 million U/24 h12-18 million U/24 h 2 wks 2 wks when obtained 1h after a 20-30 min. when obtained 1h after a 20-30 min.
penicillin G sodiumpenicillin G sodium IV either continuously IV either continuously IV infusion or IM injection, serumIV infusion or IM injection, serum
or in six equallyor in six equally concentration of gentamicin of concentration of gentamicin of
divided dosesdivided doses approximately 3 mcg/mL is desirable; approximately 3 mcg/mL is desirable;
with gentamicinwith gentamicin 1 g IM or IV every 8 h1 g IM or IV every 8 h 2 wks 2 wks trough concentration should be < 1 trough concentration should be < 1 pg/mLpg/mL
sulfatesulfate
VancomycinVancomycin 30 mg/kg per 24 h IV30 mg/kg per 24 h IV 4 wks 4 wks vancomycin therapy is recommended forvancomycin therapy is recommended for
hydrochloridehydrochloride in two equally dividedin two equally divided patients allergic to beta lactams; patients allergic to beta lactams; peak peak doses, not to exceed 2doses, not to exceed 2 serum concentrations of serum concentrations of vancomycin shouldvancomycin should
gram/24h unless serumgram/24h unless serum be obtained one h after completion be obtained one h after completion of theof the
levels are monitoredlevels are monitored infusion and should be in the range of infusion and should be in the range of
30-45 mcg/mL for twice-daily dosing30-45 mcg/mL for twice-daily dosing
JAMA 1995; 274:1706

Indications for surgery in Indications for surgery in IEIE
The indications for surgery in patients with native-The indications for surgery in patients with native-valve IE and prosthetic-valve IE are essentially the valve IE and prosthetic-valve IE are essentially the same same
Surgery is warranted for patients with active IE who Surgery is warranted for patients with active IE who have one or more of the following complications:have one or more of the following complications: CHF CHF that is directly related to valve dysfunctionthat is directly related to valve dysfunction Persistent or uncontrolled infectionPersistent or uncontrolled infection while receiving while receiving
appropriate antimicrobial therapy, including appropriate antimicrobial therapy, including evidence of perivalvular extensionevidence of perivalvular extension
Recurrent emboliRecurrent emboli, particularly in the presence of , particularly in the presence of large vegetationslarge vegetations

Indications for surgery in Indications for surgery in IEIE
Relative indications for surgeryRelative indications for surgery Evidence of perivalvular infection, such as Evidence of perivalvular infection, such as
intracardiac abscess or fistula formationintracardiac abscess or fistula formation Rupture of a sinus of Valsalva aneurysmRupture of a sinus of Valsalva aneurysm Fungal endocarditisFungal endocarditis Endocarditis due to highly resistant Endocarditis due to highly resistant
microorganismmicroorganism Relapse after a course of adequate antimicrobial Relapse after a course of adequate antimicrobial
therapy, particularly in prosthetic valve therapy, particularly in prosthetic valve endocarditisendocarditis
Culture-negative IE with fever more than 10 days Culture-negative IE with fever more than 10 days after starting empirical therapyafter starting empirical therapy

Indications for surgery in Indications for surgery in prosthetic valve IEprosthetic valve IE
Same as native valve endocarditisSame as native valve endocarditis Perivalvular infectionPerivalvular infection Valve DehiscenceValve Dehiscence
excessively mobile prosthesis on echoexcessively mobile prosthesis on echo results in hemodynamic instabilityresults in hemodynamic instability

OUTCOME OF OUTCOME OF SURGERYSURGERY• The outcome of surgery in patients with IE has The outcome of surgery in patients with IE has
been good, particularly when surgical treatment is been good, particularly when surgical treatment is radical with the removal of all infected and radical with the removal of all infected and necrotic tissuenecrotic tissue
• In a recent study of 138 patients who underwent In a recent study of 138 patients who underwent valve surgery in the presence of active infection, valve surgery in the presence of active infection, the early mortality, due to heart failure or septic the early mortality, due to heart failure or septic multiorgan failure, was 11.5 %multiorgan failure, was 11.5 %
• Risk factors for early mortality were NYHA class IV Risk factors for early mortality were NYHA class IV or cardiogenic shock, advanced age, preoperative or cardiogenic shock, advanced age, preoperative acute renal failure, and staphylococcal infectionacute renal failure, and staphylococcal infectionOperation for infective endocarditis: Results after implantation of Operation for infective endocarditis: Results after implantation of mechanical valves. Ann Thorac Surg 1998; 65:359.mechanical valves. Ann Thorac Surg 1998; 65:359.
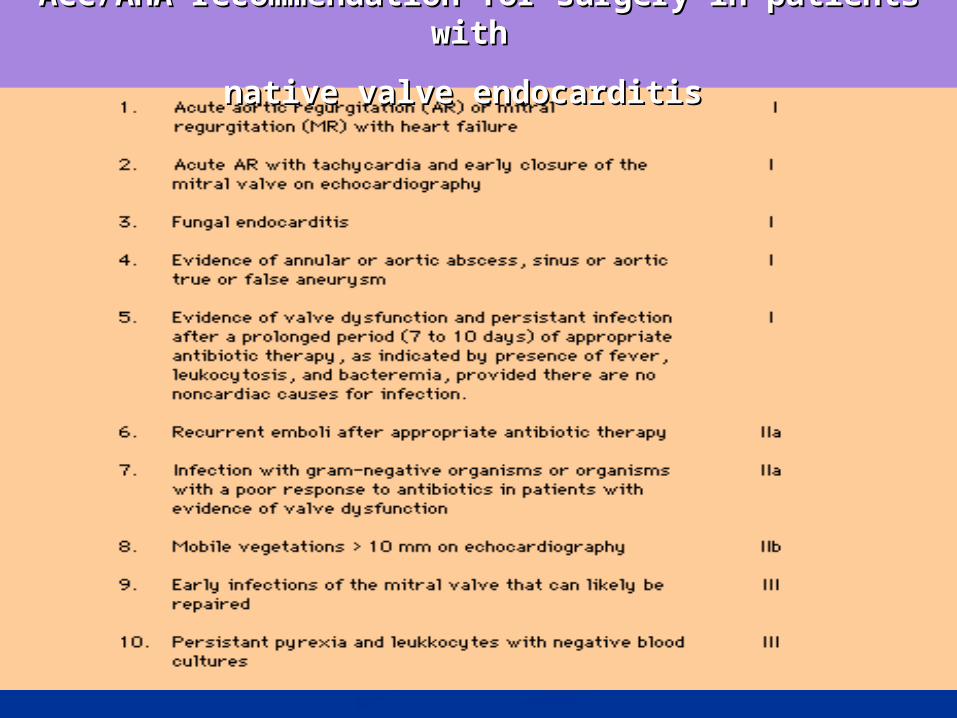
ACC/AHA recommendation for surgery in patients ACC/AHA recommendation for surgery in patients with with
native valve endocarditisnative valve endocarditis
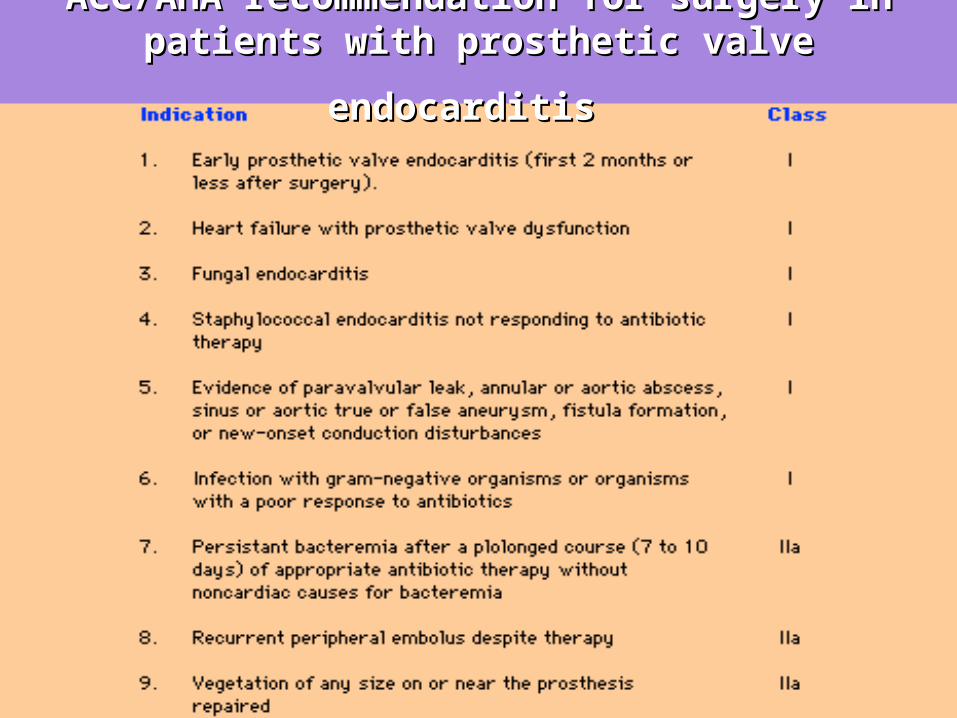
ACC/AHA recommendation for surgery in ACC/AHA recommendation for surgery in
patients with prosthetic valve endocarditispatients with prosthetic valve endocarditis

Prevention of IEPrevention of IE
No randomized controlled human trials which No randomized controlled human trials which definitively establishes the efficacy of antibiotic definitively establishes the efficacy of antibiotic prophylaxis.prophylaxis.
Most cases of endocarditis are NOT attributable to Most cases of endocarditis are NOT attributable to an invasive procedurean invasive procedure
Current recommendations are based upon literature Current recommendations are based upon literature analysis of procedure-related endocarditis, analysis of procedure-related endocarditis, prophylaxis studies in experimental animal models, prophylaxis studies in experimental animal models, and retrospective analysis of human endocarditisand retrospective analysis of human endocarditis
Dajani AS, Taubert KA, Wilson W, et al. Prevention of bacterial endocarditis: Recommendations by the American Heart Association. JAMA 277;1794: 1997

Endocarditis prophylaxis Endocarditis prophylaxis recommendedrecommended
High-riskHigh-risk– Prosthestic cardiac valvesProsthestic cardiac valves– Previous bacterial endocarditisPrevious bacterial endocarditis– Complex cyanotic heart diseaseComplex cyanotic heart disease– Surgically constructed systemic-pulmonary shunts or conduitsSurgically constructed systemic-pulmonary shunts or conduits
Moderate-riskModerate-risk– Most other congenital heart diseaseMost other congenital heart disease– Acquired valvar dysfunctionAcquired valvar dysfunction– Hypertrophic cardiomyopathyHypertrophic cardiomyopathy– Mitral valve prolapse WITH regurgitation and/or thickened Mitral valve prolapse WITH regurgitation and/or thickened
leafletsleaflets

Endocarditis prophylaxis NOT Endocarditis prophylaxis NOT recommendedrecommended
Isolated secundum ASDIsolated secundum ASD
Surgically repaired VSD, ASD, or PDA after 6 Surgically repaired VSD, ASD, or PDA after 6 months (no residua)months (no residua)
s/p CABGs/p CABG
MVP without MRMVP without MR
Previous Kawasaki disease w/o valvar dysfunctionPrevious Kawasaki disease w/o valvar dysfunction
Previous rheumatic fever w/o valvar dysfunctionPrevious rheumatic fever w/o valvar dysfunction
Pacemakers and AICDsPacemakers and AICDs
Flow murmursFlow murmurs

Dental procedures and IE Dental procedures and IE prophylaxis: Recommendedprophylaxis: Recommended
Dental extractionsDental extractions
Periodontal proceduresPeriodontal procedures
Dental implants and reimplantation of avulsed teethDental implants and reimplantation of avulsed teeth
Endodontic proceduresEndodontic procedures
Subgingival placement of antibiotic fibers and stripsSubgingival placement of antibiotic fibers and strips
Initial placement of orthodontic bands (not brackets)Initial placement of orthodontic bands (not brackets)
intraligamentary local anesthetic injectionsintraligamentary local anesthetic injections
Prophylactic cleaningProphylactic cleaning

Dental procedures and IE Dental procedures and IE prophylaxis: Not recommendedprophylaxis: Not recommended
Restorative dentistryRestorative dentistry
Non-intraligamentary local anesthetic injectionsNon-intraligamentary local anesthetic injections
Taking oral impressionsTaking oral impressions
Fluoride treatmentsFluoride treatments
Oral radiographsOral radiographs
Orthodontic appliance adjustmentOrthodontic appliance adjustment
Shedding primary teethShedding primary teeth

Other procedures and IE Other procedures and IE prophylaxis: Recommendedprophylaxis: Recommended
RespiratoryRespiratory– T&AT&A– Surgical procedures involving respiratory mucosaSurgical procedures involving respiratory mucosa– Rigid bronchoscopyRigid bronchoscopy
GastrointestinalGastrointestinal– SclerotherapySclerotherapy– Esophageal stricture dilationEsophageal stricture dilation– ERCP with biliary obstructionERCP with biliary obstruction– Surgery involving biliary tract or intestinal mucosaSurgery involving biliary tract or intestinal mucosa
Genitourinary tractGenitourinary tract– Prostatic surgery, cystoscopyProstatic surgery, cystoscopy– Urethral dilation Urethral dilation
Other procedures and IE Other procedures and IE prophylaxis: Not Recommendedprophylaxis: Not Recommended
RespiratoryRespiratory– Endotracheal intubationEndotracheal intubation– PE tubesPE tubes– Flexible bronchoscopyFlexible bronchoscopy
GastrointestinalGastrointestinal– Transesophageal echocardiographyTransesophageal echocardiography– Endoscopy (with or without biopsy)Endoscopy (with or without biopsy)
Genitourinary tractGenitourinary tract– Vaginal hysterectomy, and vaginal or Caesarean deliveriesVaginal hysterectomy, and vaginal or Caesarean deliveries– In uninfected tissues: urethral catheterization, uterine In uninfected tissues: urethral catheterization, uterine
D&C, therapeutic abortions, sterilization procedures, D&C, therapeutic abortions, sterilization procedures, insertion or removal of IUDsinsertion or removal of IUDs
– CircumcisionCircumcision
How about How about Tattoos and Body piercing?Tattoos and Body piercing?
Ear piercingEar piercing– 43% of respondents had ear piercing43% of respondents had ear piercing– Only 6% took antibioticsOnly 6% took antibiotics– 23% reported infections but no IE reported23% reported infections but no IE reported
TattoosTattoos– 5% of respondents had tattoos5% of respondents had tattoos– No antibiotics or infections reportedNo antibiotics or infections reported
PhysiciansPhysicians– Majority of physicians did not approve of piercing or tattoosMajority of physicians did not approve of piercing or tattoos– 60% felt that IE prophylaxis use was appropriate60% felt that IE prophylaxis use was appropriate
Cetta F, Graham LC, Lichtenberg RC, Warnes CA. Piercing and tattooing in patients with congenital heart disease. J Adolesc Health 1999;24:160












