Ellen M. Brown M.D. - med-surg.org
43
Hospice Approach to Caring Ellen M. Brown M.D.
Transcript of Ellen M. Brown M.D. - med-surg.org

Hospice Approach to Caring Ellen M. Brown M.D.

Objectives
By the conclusion of this session, attendees
will be able to:
O Explain the hospice philosophy and goals
O Understand what is covered by the hospice benefit
O Understand guidelines for hospice eligibility for
common non-cancer diagnoses


“The only problem with hospice is that you have to be dying to get it.” ―Dr. Michael Levy

Patient #1 O 88 yo woman with Stage 4 adenocarcinoma of the lung and
malignant pleural effusion, diagnosed September 2015 after
hospitalization in May 2015 and September 2015 for
pneumonia
O PMH: Hypertension, degenerative joint disease
O Discharge care needs: care and drainage of pleurex catheter
O Patient previously lived independently with her independence,
art classes and time with friends of primary importance
O Admitted to hospice in October 2015 with increasing weakness
and a 22 pound weight loss
O Daughter lives abroad and there is family conflict between
patient and local son

Patient #1 – Hospice Course O Decreased drainage from Pleurex catheter to every other day to twice a
week to weekly to no drainage
O Patient asks for pleural catheter removal due to increasing pain at the
site
O Increasing chest pain and shortness of breath relieved by oral morphine
solution 10mg, 2-3 times a day
O Increasing weakness and requires more help with showering.
O Ambulates slowly with a walker;otherwise independent with ADLS.
O With MSW assistance, hires caregivers
O Increases her use of oxygen and using ativan for anxiety
O March 2016: Patient has lost 15 pounds since admission
O Sleeping most of the day; has minimal po intake; Dies comfortably after
5 months on hospice

Patient #2
O 87yo man with end stage renal disease
O Had been receiving dialysis 3x/week for 2 1/2
years
O Decides to stop dialysis due to no longer being
able to do it as an outpatient because of
hypotension
O He is ambulatory, independent
in all ADLs and mentally clear.
Patient #2 – Hospice Course
O Although ambulatory on admission, he had a rapid decline
O By day #5, he was bedbound, and somnolent, but easily rousable
O He had minimal po intake
O He was receiving methadone 5mg q12h for pain and dyspnea, minimizing the need for other breakthrough opioids
O All non-comfort meds were discontinued
O He had haloperidol for hallucinations/delirium
O Supportive family was vigiling
O MSW and chaplain provided support to wife and children
O Patient died comfortably, with son stating, death couldn’t have been more peaceful.

Hospice Philosophy
O Death is a natural part of the life cycle
O Hospice enhances and optimizes quality of life
O Hospice supports palliation, rather than curative
treatment
O Psychosocial and spiritual pain as significant as
physical pain

Hospice Philosophy
O Patient, family, loved ones = “unit of care”
O Hospice emphasizes importance of relationship
between patient / family and primary care
physician
O Aggressive pain and symptom management

Goals of Hospice
O Continue life with as little disruption as possible
O Live fully in final months, weeks, days
O Be as comfortable as possible
O Attain patient’s personal goals

Living Longer with Hospice O 2007 study: 4,493 patients lived an average 29
days longer with hospice (heart failure: 81 days longer)*
O Authors: “with earlier referral to a hospice program, patients may receive care that results in better management of symptoms, leading to stabilization of their condition and prolonged survival.”
*Journal of Pain & Symptom Management, March 2007

Hospice Facts
O Modern hospice movement began in London in 1967 by Dame Cicely Saunders
O First hospice in the U.S. in 1974
O Hospice as we know it: Medicare Hospice benefit established in 1982 by Congress
O Approx. 6100 hospices in the U.S. today
O Only 36.5% of hospice patients have cancer
O Top 3 non-cancer diagnoses: dementia, heart disease, and lung disease

Eligibility
O Probable life expectancy of 6 months or less
O No longer seeking curative treatment
O Any diagnosis

Medicare Hospice Benefit
Four Levels of Care
O Routine Home Care: 93.8% pt. days
O General Inpatient Care: 4.8%
O Continuous Care: 1%
O Respite Care: 0.4%

Medicare Hospice Benefit
O Recertification
O Medicare benefit periods
1st: 90 days
2nd:90 days
3rd: 60 days
4th: Unlimited period (recert every +60
days)

O Discharge: when patient is no longer “appropriate”
(i.e., doesn’t meet criteria)
O Revocation: patient or family decide to return to
non-palliative care
Medicare Hospice Benefit

O Discharge: when patient is no longer “appropriate”
(i.e., doesn’t meet criteria)
O Revocation: patient or family decide to return to
non-palliative care
Medicare Hospice Benefit

Included in Hospice
O Intermittent visits
O Medications
O Equipment
O Supplies
O Respite stays
O Bereavement support

Hospice Statistics
O Hospice cares for approximately 41.6% of all dying patients in US
O 2014: estimated 1.6 million received services from hospice (NHPCO 2015 report)
O Gallup poll: 88% of people asked preferred to be cared for at home at the end of life

Length of Stay
O 2014 median length of stay: 14 days
O Down from 18.5 days in 2013
O 2014: 35.5% of hospice patients died in
7 days or less; and 50.3% die within 14
days of admission
O 10.3% remained on hospice for
longer than 180 days
NHPCO Facts and Figures on Hospice Care 2015
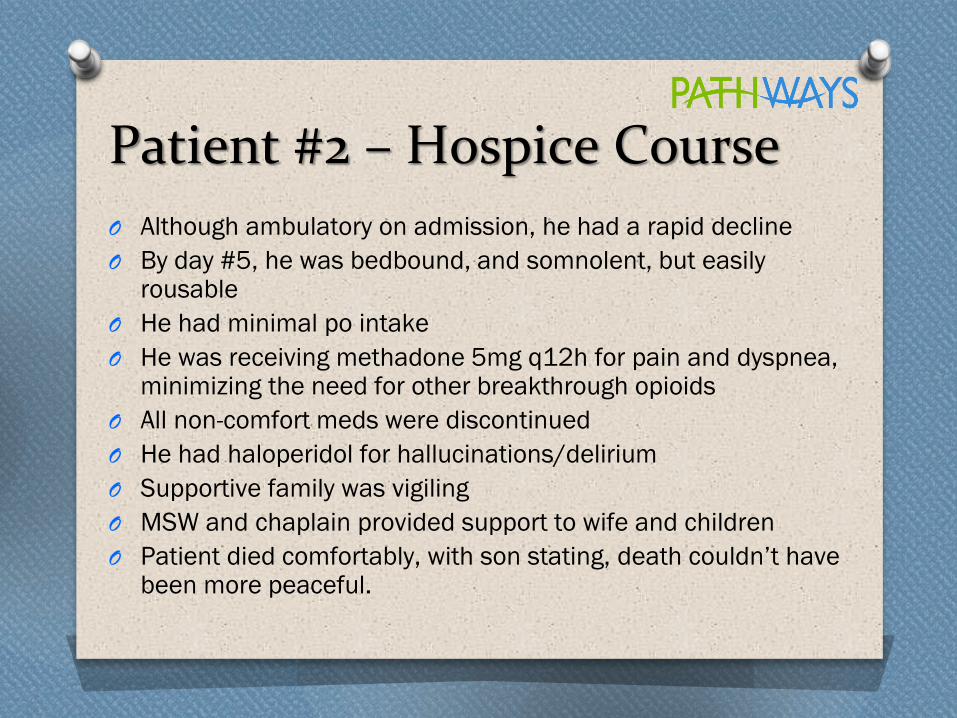
Location of Death
Location of Death 2013 2014
Patient’s Place of Residence 66.6% 58.9%
Private Residence 41.7% 35.7%
Nursing Home 17.9% 14.5%
Residential Facility 7.0% 8.7%
Hospice Inpatient Facility 26.4% 31.8%
Acute Care Hospital 7.0% 9.3%
NHPCO 2014 National Data set

Debunking Myths
Hospice is NOT:
O Giving up hope
O One-way street
O Hastening or delaying death
O Death sentence
O Just for final few days
O Giving up medications

Team Approach
O May not see, but on
the case: ● Pharmacist
● Medical director
O Available as needed: ● Dietitian
● Physical therapist
O Patient, family, primary care physician
O Intermittent visits from ● Nurse
● Hospice aide
● Social worker
● Volunteer (5% patient hrs mandated by Medicare)
● Spiritual counselor

Advantages For Patient O Be at home
O Expert pain and symptom control
O Emotional and spiritual support
O Knowledge that family has support
O Companionship
O Extra personal care
O Comfort therapies

Advantages For Family
O Instruction in end-of-life care
O Financial relief for cost of meds, equipment,
supplies related to the illness
O Bereavement support for 13 months
O 24-hour nursing availability
O Assistance with financial
and funeral plans
O Counseling

Advantages For Facility
O Education on pain and symptom management,
other topics relevant to hospice patients
O Assistance with complicated patients
O 24-hour hospice nurse availability
O Extra patient services, e.g. animal assisted
activities, personal care
O Bereavement support

Percent of Patients Served by Payer
Payer 2013 2014
Medicare Hospice Benefit 87.2% 85.5%
Managed Care or Private Insurance 6.2% 6.9%
Medicaid Hospice Benefit 3.8% 5%
Uncompensated or Charity Care 0.9% 0.7%
Self Pay 0.8% 0.8%
Other Payment Source 1.2% 1.2%
NHPCO 2014 National Data Set

Organizational Tax Status
O Not-for-profit (charitable organization, subject to
501 (c) 3 tax provisions)
O For-profit (privately owned or publicly held)
O Government (owned or operated by federal, state,
or local municipality

Medicare-certified Hospice Providers
O 28% not-for-profit
O 68% for-profit
O 4% government owned
O Number of for-profit hospices provider has
steadily increased over past 26 years
O Number of not-for-profit decreasing over same
period

Cost Savings For Medicare
O Medicare costs for hospice patients were lower
than non-hospice Medicare beneficiaries with
similar diagnoses
O Hospice enrollment is associated with fewer 30
day hospital readmissions and hospital deaths
O Hospice enrollment is associated with fewer
hospital and ICU days

Recent Regulatory Changes
O Face to face encounter: began in 2011
O Inability to use debility or failure to thrive as
primary diagnosis
O Inability to use dementia as primary diagnosis

Hospice Criteria for Common Diagnoses

Heart Disease O CHF or angina at rest (NYHA Class IV)
O Optimal diuretic and vasodilator therapy
O Tx includes ACE inhibitors
O May include patients who do not tolerate tx
O Other factors : • Resistant arrhythmias
• History of cardiac arrest or syncope
• Cardiogenic embolic stroke
• HIV
Pulmonary Disease
O Disabling dyspnea at rest
● Poor response to bronchodilators
● Bed to chair existence
O Progressive disease
● Increasing complications
(infections, respiratory failure)
● Serial decrease
>40 ml in 1 second forced
expiratory volume (FEV1) over
last year

O Hypoxemia at rest on supplemental O2
(<55mm Hg or <88% saturation)
O Right sided failure 2° to cor pulmonale
O Hypercapnia (pCO2 >50 mmHg)
O Weight loss >10% over 6 months
O Resting tachycardia >100/min
Pulmonary Disease

End-stage Liver Disease
O Severely impaired liver function tests
● Protime > 5 seconds over control
● Albumin < 2.5 gm/dl
O Clinical parameters
● Refractory ascites
● Hepatic encephalopathy
● Hepatorenal syndrome
● Recurrent variceal bleeding

End-stage Renal Disease O Creatinine clearance < 10 cc/min
O Serum creatinine > 8 mg/dl (> 6mg/dl in diabetics)
O Clinical uremia with dialysis
O Other supporting criteria:
• Oliguria < 400cc/day
• Uremic pericarditis
• Intractable fluid overload
• Hyperkalemia
Stroke and Chronic Coma O Palliative Performance Scale < 40%
O Unable to maintain hydration and caloric intake
with one of following:
● 10% wt loss over 6 months
● Serum albumin < 2.5 gm/dl
● Aspiration not responsive to speech therapy
● Calorie counts documenting inadequate
intake
● Dysphagia preventing sufficient intake
to sustain life

Choices

Patients Have Choices
O “How does your hospice differ from others?”
O “Are you certified by the Joint Commission?”
O “What sort of bereavement follow-up programs do you have?”
O “How many of your nurses and doctors are certified hospice specialists?”
O If they get a recommendation, tell them to ask why the person recommended that organization.

Dame Cicely Saunders
“You matter until the last moment of
your life, and we will do all we can,
not only to help you die peacefully,
but to LIVE until you die.”

visit us at Pathwayshealth.org


















