understanding traumatic stressChildren - Homepage...
28
ELLEN L. BASSUK, M.D. KRISTINA KONNATH, LICSW KATHERINE T. VOLK, MA February 2006 understanding traumatic stress Children in
Transcript of understanding traumatic stressChildren - Homepage...

ELLEN L. BASSUK, M.D.
KRISTINA KONNATH, LICSW
KATHERINE T. VOLK, MA
February 2006
understandingtraumaticstress
Childrenin
We are grateful to our colleagues for their
willingness to share their expertise on
traumatic stress and children.We would like to
thank the National Child Traumatic Stress
Network,The Trauma Center, and the National
Health Care for the Homeless Council for their
contributions.We want to specially thank the
W.K. Kellogg Foundation for its generous
support of this project. Finally, this booklet is
dedicated to all of the women and children
who have informed and improved our work.
Their generosity and willingness to share their
experiences with us are a testament to their
courage, strength, and resilience.
Supported by a grant from W.K. Kellogg Foundation.
Photo attributions:George CeollaMelody Ko/University Photographer,Tufts UniversityNational Center on Family Homelessness
Copyright 2006:The National Center on Family Homelessness

ELLEN L. BASSUK, M.D.
KRISTINA KONNATH, LICSW
KATHERINE T. VOLK, MA
February 2006
understandingtraumaticstress
Childrenin

UNDERSTANDING TRAUMATIC STRESS IN CHILDRENINTRODUCTION
The unexpected loss of a loved one, a car accident, or exposure to a violentexperience is familiar to many of us. Everyone reacts to such events, but theresponses vary widely, ranging from numbness and withdrawal, to crying,nervousness, and agitation.
There is no “right” way to respond to or recover from a traumatic event. Over time,some people are able to integrate these experiences and begin to heal. For others,this is considerably more difficult. Some responses to trauma are prolonged,intense, and interfere with a person’s ability to function.
Because traumatic events are prevalent, cause profound suffering, and may lead tolife altering responses, it is imperative that caregivers have the knowledge andunderstanding to respond skillfully and compassionately to children who have beenexposed to traumatic stress.
The National Center on Family Homelessness has compiled this booklet as aresource for caregivers working with children who have experienced traumaticstress. The booklet opens by defining trauma, then looks more closely at acutetraumatic stress and complex trauma. For each aspect of trauma, we describe themost common developmental effects on children and ways for caregivers torespond to help children heal. To support caregivers, we highlight the importanceof self-care and provide a list of resources.
We use the term “caregiver” in this booklet to refer to anyone who cares forchildren. This may include teachers, child care providers, health care professionals,guidance counselors, social workers, parents, neighbors, friends and family.Primary caregivers are considered those assuming a parental role (e.g., mother,father, grandparent, aunt/uncle).
Introduction
UNDERSTANDING TRAUMATIC STRESS IN CHILDREN TABLE OF CONTENTS
I What Is Trauma? 2
II Effects of Trauma 3
III Acute Traumatic Stress 7
A. The Body’s Response to Acute Trauma
B. Children’s Developmental Issues
C. Tips for Caregivers
IV Complex Trauma 13
A. The Body’s Response to Complex Trauma
B. Children’s Developmental Issues
C. Attachment and Complex Trauma
D. Tips for Caregivers
V Self-Care 20
References and Resources 22
Table of Contents

2
UNDERSTANDING TRAUMATIC STRESS IN CHILDRENI.WHAT IS TRAUMA?
Atraumatic event is sudden andunexpected, and perceived as dangerous. It may involve a
threat of physical harm or actualphysical harm, leading to intense fear.It overwhelms our immediate ability to cope.
Traumatic experiences have severalkey components:• Intense feelings of helplessness,
terror, and lack of control• Threat to one’s physical or mental
well-being through violence or threatof violence
• Catastrophic responses
Traumatic experiences come in manyforms, and can leave survivors withoverwhelming feelings of loss, danger,and helplessness. They include:• Unexpected loss of a loved one• Accidents
• School violence• Community violence• Domestic violence• Neglect• Physical abuse• Sexual abuse• Man-made and natural disasters• Terrorism
Trauma generally falls into two categories:
Acute traumatic stress typicallyinvolves a one-time experience (e.g., natural disaster or car accident).
Complex trauma involves prolonged ormultiple traumatic events that typicallyoccur within a caregiving relationship (e.g., neglect, physical or sexualabuse).
What is Trauma?
Definitions ofTrauma
“Overwhelming demands
placed upon the
physiological system that
result in a profound felt
sense of vulnerability
and/or loss of control.”
– Robert D. Macy
“Traumatic events
overwhelm the ordinary
systems of care that give
people a sense of
control, connection,
and meaning.”
– Judith Herman
3
T raumatic experiences are oftenshattering and life-altering forchildren. These experiences may
effect all levels of functioning and resultin an array of distressing symptoms:• Physical: nervousness, tiredness,
headaches, stomach aches, nausea,palpitations, pain, difficulty sleeping,nightmares, worsening of existingmedical problems.
• Emotional: fear, anxiety, panic,irritability, anger, withdrawal,numbness, depression, confusion,hopelessness, helplessness.
• Academic: inability to concentrate orremember, missing school, pooracademic performance.
• Relational: emotional barriers betweencaregivers and children, distrust andfeelings of betrayal, attachmentproblems (see Section IV-C).
Nearly all trauma survivors have acutesymptoms following a traumatic event,but these generally decrease over time.Various factors can make recoverymore difficult:• Previous exposure to trauma: This
may include neglect, physical abuse,sexual abuse, or abrupt separationfrom a caregiver.
• Duration of exposure to trauma:A one-time exposure, such as a caraccident, results in very different
responses than exposure over severalyears, such as domestic violence. Thelonger the exposure, the moredifficult the healing process.
• Severity of exposure: An incident thathappens directly to a child or in frontof a child will have different impactsthan an incident that happened tosomeone else or one a child was toldabout later. The more severe theexposure, the more difficult it will be to heal.
• Prior emotional and behavioralproblems: Pre-existing problems withbeing able to pay attention, beinghyperactive, fighting or not followingrules, or a prior history of depressionor anxiety may complicate a child’sresponse to a traumatic event.
• Caregiver’s response after theexposure: It matters whether acaregiver validates the child’sexperience or blames the child, or ifthe caregiver is able to providecomfort and reassurance instead ofhaving difficulty responding to thechild. When a caregiver experiences ahigh level of distress, a child oftenresponds similarly. Caregiver’ssupport is one of the most importantfactors in a child’s recovery from trauma.
Effects of Trauma
UNDERSTANDING TRAUMATIC STRESS IN CHILDREN II. EFFECTS OF TRAUMA
Thinking about…Responses toTrauma
Eva is seven years old.Last month, her school buswas in a bad accident andalthough she wasn’tseriously injured, otherstudents were. Ever sincethe accident, Eva has been fighting with herclassmates and has hadtrouble listening in school.You’ve tried to contact herfamily, but have had noluck.You know that Eva’smother has a history ofdepression. How wouldyou respond to Eva? What additionalinformation would helpyou better respond to the situation?

4
UNDERSTANDING TRAUMATIC STRESS IN CHILDRENII. EFFECTS OF TRAUMA
Factors That May Increase The Likelihood Of Children’s Recovery From Traumau
Individual Level • Easy temperament• Feeling of control over one’s life• High self-esteem/self-confidence• Sense of humor• Optimism• Sociable• Intelligent
Family Level • Safe, warm, caring, supportive environment• High expectations for achievement• Good communication• Strong family cohesion• Reasonable structure and limits• Strong relationship with at least one caregiver
School-Based • Safe place to be• Warm, caring, supportive environment• High expectations for achievement• Significant adult committed to child• Academic achievement• Models from peers of developmentally
appropriate behavior• Good relationships with peers• Involvement and participation in school
community/activities
Community Level • Safe community (or safe places to go)• Access to resources and supports
(e.g., church, mentor, clubs)• Involved in community activities

5
UNDERSTANDING TRAUMATIC STRESS IN CHILDREN II. EFFECTS OF TRAUMA
Factors That May Interfere With Children’s Recovery From Traumau
Individual Level • Difficult temperament (e.g., fussy, irritable, sensitive)• Sense of a lack of control over life events• Dependency beyond what is age-appropriate• Low self-esteem/self-confidence• Feeling of uncertain or poor future outcomes• Shy/difficulty making friends
Family Level • Physical or sexual abuse, neglect, domestic violence• High levels of parental distress• Lack of parental support• Expectation that child will fail or act out• Lack of structure, limit-setting• Negative relationships with caregivers
School-Based • Exposure to school violence• Lack of support from adults at school• Poor academic performance• Difficulty with peer relationships• Lack of participation in school community/activities
Community Level • Violence in the community• Unable to identify a safe place to go• Unable to identify resources or supports in the community• Disconnected from the community

6
UNDERSTANDING TRAUMATIC STRESS IN CHILDRENII. EFFECTS OF TRAUMA
What is Posttraumatic Stress Disorder (PTSD)?
PTSD is an anxiety disorder thatmay develop months or even yearsafter experiencing or witnessing atraumatic event. Examples of suchevents include unexpected loss of aloved one, accidents, interpersonalviolence, and military combat.Themajor symptoms of PTSD include:• Re-experiencing of the traumatic
event (e.g., nightmares orflashbacks)
• Hyperarousal (e.g., difficulty fallingor staying asleep, angry outbursts,difficulty concentrating,hypervigilance).
• Avoiding reminders of the event,along with constricted behaviorand numbing (e.g., diminishedinterest or participation insignificant activities, feelingdetached or estranged from others).
PTSD is also characterized bydissociation.We all dissociate fromtime to time to cope with stress.For example, many of us havemissed our exit on the highwaybecause we were preoccupied and
driving automatically. A person withPTSD experiences more persistentdissociation. Behaviors, feelings,physical sensations, and thoughtsassociated with the traumatic eventmay be fragmented and walled offfrom other memories.Thedissociated material tends to behighly emotional and not adequatelyprocessed. Inevitably, the dissociatedparts intrude, creating distress andsymptoms such as the onespreviously described.
Who Does It Impact?Not everyone who experiences atraumatic event develops PTSD.Only nine percent of men and 20percent of women who areexposed to traumatic experiencesdevelop PTSD. Factors such asduration and severity exposure tothe traumatic event, and previoustraumatic exposure, can makerecovery more difficult. Overall,seven to 14 percent of the generalpopulation experience PTSD atsome point in their lives.
Sources: American Psychiatric Association (2000); Yehuda (2002); Yehuda (2003).

7
UNDERSTANDING TRAUMATIC STRESS IN CHILDREN III.ACUTE TRAUMATIC STRESS
Acute trauma is generally a one-time event, such as a car accidentor a natural disaster. Because
children’s responses to acute traumavary, awareness of the wide array ofpossible responses allows caregivers to
provide a sense of safety and security,and support healing. This section looksat the effects of acute traumatic stresson children and offers tips for caregiversabout how to support children who haveexperienced an acutely traumatic event.
Acute Traumatic Stress
Imagine you are driving on thehighway. A car suddenly swerves at fullspeed into your lane, then veers awaybarely missing your vehicle. How do youfeel? Scared? Jittery? Numb? Frozen?Now imagine you are in that sameemotional state and someone asks youfor directions to your house. Are youdistracted? Can you think or evenconcentrate? Do you fumble or make mistakes?
We each have an “alarm system” inour brain that signals us when we mightbe in danger. When our brain perceivesdanger, it prepares our body to respond.Our response often depends on thenature of the danger, but we are likely toreact in one of three ways:
• Fight• Flight• Freeze
If a small bug is biting your arm, youmight choose to fight by slapping itbecause you are bigger and strongerthan the bug. If a car comes careeningat you in the street, you might try to fleebecause you can’t fight the car and, ifyou stand still, you will be hit. If a large,fierce dog attacks you, you might freezebecause you’re not strong enough tofight off the dog and you’re not fastenough to outrun it. Our responses willalso vary according to our perception ofthe danger. A person terrified of bugs,for example, might freeze or run when being bitten.
Two parts of our brain respond todanger. The “doing brain” signals theneed for action, while the “thinkingbrain” tries to solve the problem andmake a plan. When the brain perceivesdanger, the “thinking brain” makes anassessment. If it’s a false alarm becausethere is no real danger, the “thinkingbrain” shuts the alarm off and we moveon. If there is actual danger, the “doingbrain” signals the body to releasechemicals, like fuel for a car, to provideenergy to respond. When this happens,the “thinking brain” shuts off to allowthe “doing brain” to take over.
As a result of this alarm system,people often experience intenseemotional responses after a traumaticevent. These responses are generallyshort-lived and most people eventuallyreturn to their usual level of functioningafter the event. To cope with traumaticexposure, people often need time andsupport to process the event. Duringthis time, any reminder of the event maylead to a reactivation or increase in their responses.
Some people are unable to recoverfrom acute trauma in a timely way. As aresult, they are more likely to develop anAcute Stress Disorder or PosttraumaticStress Disorder. The type, severity, andduration of exposure to traumatic stresswill influence the course of recovery.The situation is compounded forchildren by their developmental stages.
A. The Body’s Response to Acute Trauma

8
UNDERSTANDING TRAUMATIC STRESS IN CHILDRENIII.ACUTE TRAUMATIC STRESS
As children grow and mature, they arefaced with age-specific challenges theymust master before moving along to thenext stage. At each developmental stage,a child is faced with different tasks thatbuild upon one another: a toddler learnsto explore his world; school-agedchildren are interested in making friends;an adolescent tries to separate andbecome more independent. When facedwith traumatic stress, a child’s energy isdiverted and she has less capacity tomaster developmental challenges.
Most children rebound from traumaticexperiences and continue to achieveexpected developmental milestones.One of the crucial ways children areable to heal is with support fromcaregivers to make them feel safe,secure, and protected. The level ofsupport a child receives from acaregiver is the most significant factorin how well a child fares after atraumatic event.
B. Children’s Developmental Stages
Early Childhood (0 – 5 years)u
The tables below outline primarydevelopmental tasks and how they maybe impacted by exposure to an acutetraumatic stressor. These tables include
developmental tasks from birth to agetwelve, and are not inclusive of everydevelopmental task that may occur.
Effect of Acute Trauma on Developmental Tasks
Developmental Milestones Effect of Acute Trauma
Physical Sit up Sleep disturbancesCrawl Eating problemsStand Going back to earlier, younger behaviors Walk/run (e.g., baby talk or bedwetting)Talk/writeSleep gradually gets organized
into a day-night schedulePotty Training
Cognitive 0 – 1: Develop knowledge that Cognitive regression (e.g., poor impulse something continues to exist, even control, problem solving)when it is out of sight (Object Permanence)
3 – 6: Beginning to develop skills to problem solve, work with others, and manage impulses
continued
9
UNDERSTANDING TRAUMATIC STRESS IN CHILDREN III.ACUTE TRAUMATIC STRESS
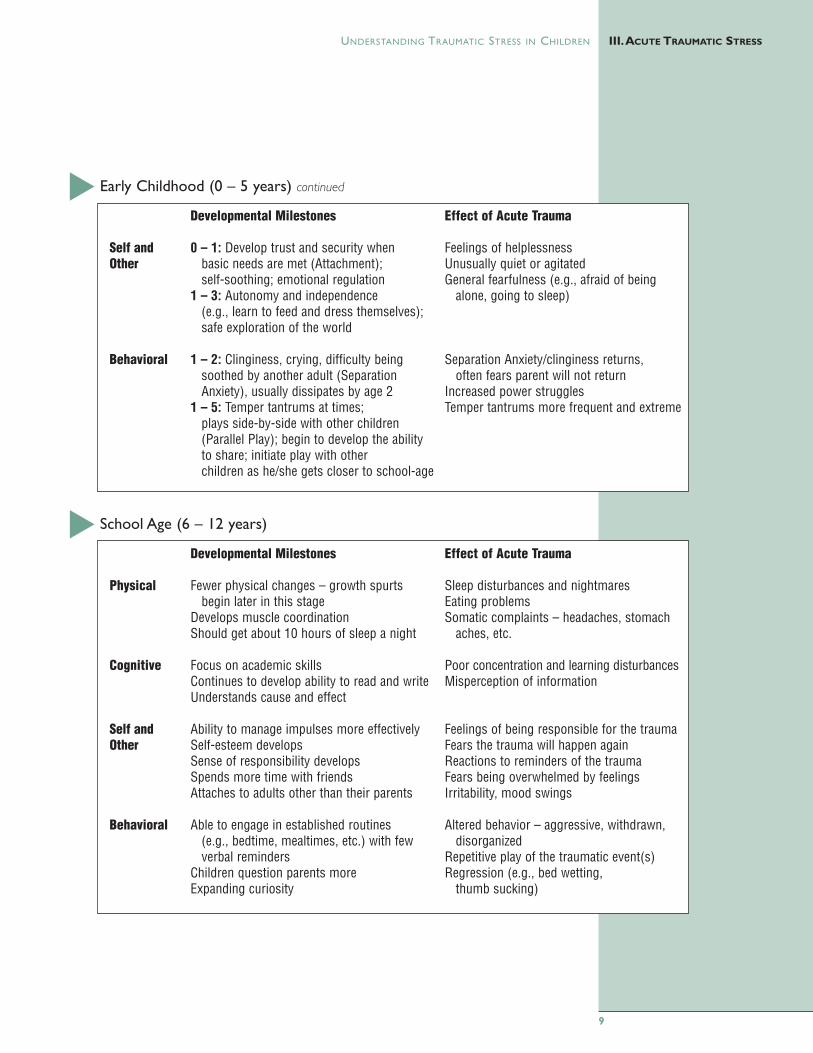
Early Childhood (0 – 5 years) continueduDevelopmental Milestones Effect of Acute Trauma
Self and 0 – 1: Develop trust and security when Feelings of helplessnessOther basic needs are met (Attachment); Unusually quiet or agitated
self-soothing; emotional regulation General fearfulness (e.g., afraid of being 1 – 3: Autonomy and independence alone, going to sleep)
(e.g., learn to feed and dress themselves); safe exploration of the world
Behavioral 1 – 2: Clinginess, crying, difficulty being Separation Anxiety/clinginess returns, soothed by another adult (Separation often fears parent will not returnAnxiety), usually dissipates by age 2 Increased power struggles
1 – 5: Temper tantrums at times; Temper tantrums more frequent and extremeplays side-by-side with other children (Parallel Play); begin to develop the ability to share; initiate play with other children as he/she gets closer to school-age
School Age (6 – 12 years)uDevelopmental Milestones Effect of Acute Trauma
Physical Fewer physical changes – growth spurts Sleep disturbances and nightmaresbegin later in this stage Eating problems
Develops muscle coordination Somatic complaints – headaches, stomach Should get about 10 hours of sleep a night aches, etc.
Cognitive Focus on academic skills Poor concentration and learning disturbancesContinues to develop ability to read and write Misperception of informationUnderstands cause and effect
Self and Ability to manage impulses more effectively Feelings of being responsible for the trauma Other Self-esteem develops Fears the trauma will happen again
Sense of responsibility develops Reactions to reminders of the traumaSpends more time with friends Fears being overwhelmed by feelingsAttaches to adults other than their parents Irritability, mood swings
Behavioral Able to engage in established routines Altered behavior – aggressive, withdrawn, (e.g., bedtime, mealtimes, etc.) with few disorganizedverbal reminders Repetitive play of the traumatic event(s)
Children question parents more Regression (e.g., bed wetting, Expanding curiosity thumb sucking)

10
UNDERSTANDING TRAUMATIC STRESS IN CHILDRENIII.ACUTE TRAUMATIC STRESS
When caring for a child who hasrecently experienced an acute traumaticevent, it is helpful to think aboutmeeting the child’s needs for safety,stabilization and support.
SafetyAcute traumatic experiences challenge
children’s idea that the world is a safeand predictable place. When scarythings happen, children rely oncaregivers to keep them safe. Here aresome ways to help children feel safe.
n Identify safe places for children togo when they feel overwhelmed.At school, a safe place may be thereading corner in a classroom wherea child can sit on a warm rug, look atbooks, or listen to music onheadphones until she feels calmagain. Safe places may be a guidancecounselor’s office or an area of theplayroom separate from the mainactivities in which the class isengaged. Talk with the child to helpher determine a safe place to gowhen she feels scared, overwhelmed,or sad. Then, the next time a childshows signs of these emotions (e.g.,crying, acting out, withdrawing, etc.),take the child aside and ask her if shewould like to go to her safe placeuntil she feels calmer.
n Identify safe people for children totalk with when they feeloverwhelmed. Ask children who theyfeel comfortable being with whenthey’re upset.
n Let children know what to expectthroughout the day. Giving childreninformation about what to expectduring the day, and letting themknow when the routine will change,helps children feel more secure.
n Remember that children need tofeel safe everywhere they go.A child may feel safe in theclassroom, but may be overwhelmedin other environments. Helpingchildren throughout the day andbeyond the classroom may requirecommunicating with other school personnel about how toaccomplish this.
n Be aware of Mandated Reporterlaws. Many caregivers are requiredto report suspected abuse to childwelfare authorities. Be aware of thelaws in your state and work with yourteam to determine when you shouldfile a report to protect a child.
C. Tips for Caregivers
Thinking about…Development
Kerri is 2-years old.She and her family recentlylost their home in a firethat ravaged their entireapartment building. Kerri’sdog was lost in the fire, aswell as all of her toys.Her whole family is in ashelter and they don’tknow how long it will beuntil they find a new home.Thinking about Kerri’sdevelopmental stage, whatresponses might youexpect from her as a resultof these traumaticexperiences? Kerri also hasa 10 year old brother,Louis. How might hisresponse be similar or different?
11
UNDERSTANDING TRAUMATIC STRESS IN CHILDREN III.ACUTE TRAUMATIC STRESS
StabilizationChildren who have been traumatized
require stabilization to provide a senseof predictability, consistency, andsafety—things that are lost when atraumatic event occurs. Stabilizationallows children to process theirexperience and be able to move on.
n Create a routine. Structure andpredictability help children feel safeand secure.• Start and end each day in the
same way.• Write down a schedule to be posted
next to the child’s bed, on aclassroom bulletin board, or at the child’s desk.
n Mobilize a support system. Whenchildren are supported by the peoplearound them, their feelings ofdistress often decrease.• A support system may include a
child’s teachers, primary caregivers,other family members, guidancecounselor, friends/peers, clergy,pediatrician, and neighbors.
n Ensure the child’s physical needsare met. Traumatic experienceseffect physical health as well asemotional health.• Children may experience
headaches, stomach aches, andmuscle aches. First, find out if thereis a medical cause. If not, providecomfort and assurance that thesefeelings happen to many childrenafter a traumatic event. Be matter-of-fact with the child. Giving non-medical complaints too muchattention may increase them.
• At home, be sure children sleepnine to ten hours a night, eat well,
drink plenty of water, and getregular exercise.
• At school, be sure children drinkplenty of water, have a well-balanced lunch, and get exerciseduring the school day.
n Create opportunities to play and draw.• Young children may not have the
words to express their fears, butmay be able to process theiremotions through play anddrawing.
• School age children may retell orplay out the traumatic eventrepeatedly. Allow the child to talkand act out these reactions. Letthem know that many childrenrespond to events like this insimilar ways. Encourage positiveproblem-solving in play ordrawings.
n Be calm. Children look to theircaregivers to provide safety andsecurity. Try not to voice your ownfears in front of the child. Remind thechild that people are working to keephim safe. Help the child regainconfidence that you aren’t leavinghim and that you can protect him.
SupportChildren may need on-going support
long after the traumatic experience hasoccurred.
n Keep a routine. Children may need apredictable routine for a long period oftime in order to feel safe and secure.
n Listen empathically.• Young children may have trouble
expressing their feelings. Encourage

12
UNDERSTANDING TRAUMATIC STRESS IN CHILDRENIII.ACUTE TRAUMATIC STRESS
them to put feelings into words, suchas anger, sadness, and worry aboutthe safety of friends and family. Don’tforce them to talk, but let them knowthat they can at any time.
• School age children may haveconcerns they were to blame orshould have been able to changewhat happened. They may hesitateto voice these concerns in front ofothers. Provide a safe place forthem to express their fears, anger,sadness, etc. Allow them to cry orbe sad. Don’t expect them to bebrave or tough. Offer reassuranceand explain why it wasn’t their fault.
n Recognize “triggers.” Triggers areevents/reminders/cues that causechildren to become upset again (e.g.,rain or thunder for children whoexperienced a hurricane). Thesereminders may seem harmless toother people. Triggers will vary fromchild to child.• If a child becomes upset, it may be
helpful to explain the differencebetween the event and reminders ofthe event.
• Protect children from reminders ofthe event as much as you can,particularly media coverage.
n Give clear and honest answers.Be sure children understand thewords you use. Find out what otherexplanations children have heardabout the event and clarify inaccurateinformation. If the danger is far away,be sure to tell the child that it is notnearby. Avoid details that will scarethe child.
n Practice relaxation exercises. Deepbreathing, listening to soothing music,and muscle relaxation will helpchildren relieve some of their stress.
n Ensure regular physical exercise.Children (particularly school-age)who have experienced trauma may beunusually aggressive or restless.Exercise and other recreationalactivities provide outlets for feelingsand frustration.
n Encourage children to write ordraw. Suggest to children that theywrite about or make drawings of theirexperiences without forcing them todo so.
n Engage in positive distractingactivities. These may include sports,games, reading, and hobbies.
n Maintain a connection withchildren’s support network.Teachers and primary caregiversshould communicate consistentlywith each other.
n Recognize that children may havetrouble sleeping.• Young children may be scared to be
away from their caregivers,particularly at bed or nap times.Reassure the child that she is safe.Spend extra quiet time together atbed or nap time. Let the child sleepwith a dim light on. Some youngchildren may not understand thedifference between dreams and reallife, and will need reassurance andhelp in making this distinction.
• School age children may havesleeping problems due to baddreams. Let the child tell you aboutthe bad dreams. Explain that manychildren have bad dreams after atraumatic event and the dreams willgo away.
Self-Care
It is important that
caregivers take care of
themselves. Dealing with
traumatized children
may trigger intense and
difficult feelings in
caregivers, leaving them
feeling depleted and
exhausted. See Section V
for more information.

13
UNDERSTANDING TRAUMATIC STRESS IN CHILDREN IV. COMPLEX TRAUMA
Children experience complextraumatic stress when they havehad prolonged exposure to trauma
(e.g., physical or sexual abuse),experience multiple traumatic eventsover time, or when different traumaticevents occur at the same time (e.g.,
separation from a caregiver, followed byphysical abuse, neglect, etc.). Complextrauma profoundly impacts children’sphysical, emotional, behavioral, andcognitive development. It impairs theirability to feel safe in the world and todevelop sustaining relationships.
Complex Trauma
Imagine you are back in a car the dayafter having a severe accident and thesame thing happens again. Now imaginethat every time you get into a car, youhave another accident—and this happensagain and again. How would yourespond? Would you stop driving? Wouldyou avoid the places you normally go?Would you become watchful and jittery,slamming on your brakes whenever a caris nearby?
Multiple car accidents may lead us toexpect that we will be in another caraccident. Because we are always preparingfor another accident, we may change theway we behave. We might decide to walkinstead of drive; we might avoid placeswhere we’ve had an accident (thusavoiding things we used to enjoy); if wehear a noise that sounds like an accident,we might be startled and start shaking.
Traumatic experiences change the waythe brain functions. According to JudithHerman, “Traumatic events produceprofound and lasting changes inphysiological arousal, emotion, cognition,and memory. Moreover, traumatic eventsmay sever these normally integratedfunctions from one another.”
As discussed earlier, the brain’s alarmsystem prepares the body to respond todanger. The “thinking brain” assesses thesituation to determine if there is danger ornot. For children who have experiencedmultiple traumatic events, such as physical
abuse, sexual abuse, or witnessingdomestic violence, this danger alarm goesoff too often. Faced with repeated alarms,the “thinking brain” gets tired of checkingthings out, and assumes instead the signalalways means real danger. This causes the“thinking brain” to shut down and allowsthe “doing brain” take over.
False alarms can be set off whenchildren hear, see, or feel something thatreminds them of previous traumaticevents. These reminders are called“triggers.” Their brains have learned torecognize these triggers, because in thepast when they heard, saw, or felt thatway, it meant they had to react quickly toa dangerous situation. Because thesetriggers may not seem alarming to others,they don’t always seem to make sense.Triggers can range from loud soundssuch as sirens or yelling to smells, subtlefacial expressions or hand gestures.
Whatever the trigger, it sets off thealarm and the body “fuels” itself toprepare to deal with danger. When thedanger is real, this response is helpful.When the body prepares, but there isn’tany danger, the child is left with pent upenergy and no outlet. As a result, childrenmay feel angry, want to fight, or hide in acorner to get far away from what theirbody perceives as danger. Often childrendo not understand why they are actingthis way. Triggers vary from child to childand are unique to each child’s experience.
A. The Body’s Response to Complex Trauma Thinking about…Complex Trauma
Michael was just placed infoster care and is new toyour third grade class.After talking to yourschool’s social worker, youknow he has beenphysically abused and hasmoved around a lot, livingat times in homelessshelters with his mother.You are not sure what toexpect on Michael’s firstday at school, but youknow that he has hadsome previous problems inschool (e.g., doing hiswork, getting along withother children).What aresome ways you can beprepared to work mosteffectively with Michael?

14
UNDERSTANDING TRAUMATIC STRESS IN CHILDRENIV. COMPLEX TRAUMA
As discussed in the section on acutetraumatic experiences, children arefaced at each life stage with variousage-specific tasks they must master tocontinue with their development.Generally, children rebound fromtraumatic experiences and continue tomaster these tasks. However, childrenexposed to complex trauma are likely
to experience more severe difficultiesand challenges over a longer time.Because complex traumatic experiencesoften occur within the caregivingsystem, adaptations becomeincreasingly difficult and more deeplyingrained, resulting in greater impact onchildren’s day-to-day functioning.
B. Children’s Developmental Stages
The tables below outline primarydevelopmental tasks and how they maybe impacted by exposure to complextrauma. These tables include
developmental tasks from birth to agetwelve, and are not inclusive of everydevelopmental task that may occur.
Effect of Complex Trauma on Developmental Tasks
Early Childhood (0 – 5 years)uDevelopmental Milestones Effect of Complex Trauma
Physical Sit up Slower achievement of developmental Crawl milestones or regression that may turn Stand into developmental delays.Walk/runTalk/writeSleep gradually gets organized
into a day-night schedulePotty Training
Cognitive 0 – 1: Develop knowledge that Problems with Object Permanence something continues to exist, even Difficulties with impulse controlwhen it is out of sight (Object Permanence)
3 – 6: Beginning to develop skills to problem solve, work with others, and manage impulses
continued

15
UNDERSTANDING TRAUMATIC STRESS IN CHILDREN IV. COMPLEX TRAUMA
Early Childhood (0 – 5 years) continueduDevelopmental Milestones Effect of Complex Trauma
Self and 0 – 1: Develop trust and security when Difficulty being soothedOther basic needs are met (Secure Attachment); Hyperalert, easily startled and frightened
self-soothing; emotional regulation Distrust of others1 – 3: Autonomy and independence Simultaneous clinginess and withdrawal
(e.g., learn to feed and dress themselves); from caregiverssafe exploration of the world Show no interest in caregivers
Too dependent, leads children not to developage appropriate skills (e.g., feeding and dressing self)
Behavioral 1 – 2: Clinginess, crying, difficulty being Power struggles and temper tantrums soothed by another adult (Separation beyond what is normally expectedAnxiety), usually dissipates by age 2 Severe separation anxiety that continues or
occurs after it is developmentally expected1 – 5: Temper tantrums at times; Difficulty sharing, rarely initiate play with
plays side-by-side with other children other children, and continue Parallel Play (Parallel Play); begin to develop the ability beyond when developmentally expected.to share; initiate play with other children as he/she gets closer to school-age

16
UNDERSTANDING TRAUMATIC STRESS IN CHILDRENIV. COMPLEX TRAUMA
School Age (6 – 12 years)uDevelopmental Milestones Effect of Complex Trauma
Physical Fewer physical changes – growth spurts Somatic complaints (e.g., headaches, begin later in this stage stomach aches, etc.)
Develops muscle coordination Increased medical problemsShould get about 10 hours of sleep a night Problems with coordination and balance
Sleep problems
Cognitive Focus on academic skills Impact on language development and verbal Continues to develop ability to read and write processing abilitiesUnderstanding of cause and effect develops Learning difficulties
Problems focusing on and completing tasks,may be diagnosed with ADD/ADHD
Difficulty planning and anticipating
Self and Ability to manage impulses more effectively Problems with boundaries (e.g., at times Other Self-esteem develops exhibits sexualized behaviors)
Sense of responsibility develops Lack of a sense of selfSpends more time with friends Distrust/fearfulnessAttaches to adults other than their parents Anxiety
Feelings of shame and guiltDissociationProblems with peer relationshipsDifficulty understanding how other people feelProblems taking/understanding responsibility
Behavioral Able to engage in established routines Aggression(e.g., bedtime, mealtimes, etc.) with few Self-destructive behavior (e.g., poor hygiene, verbal reminders self-injurious behavior)
Children question parents more Difficulty following rules and limitsExpanding curiosity Poor impulse control
Oppositional behavior, commonly diagnosedwith Oppositional Defiant Disorder
Reenactment of trauma in playSchool absencesExcessive compliance with others

17
UNDERSTANDING TRAUMATIC STRESS IN CHILDREN IV. COMPLEX TRAUMA
Attachment is the long-enduring,emotional bond between a child and aprimary caregiver. The caregiver servesas the child’s source of safety, providesfor the child’s needs, and guides her inunderstanding herself and others. Inturn, the child meets the caregiver’sneed to provide nourishment andguidance. This is a natural andautomatic process that begins from themoment a child is born and a caregiverlooks into the infant’s eyes.
Healthy attachments provide thebuilding blocks for later relationshipsand a child’s ability to masterdevelopmental tasks by:
n Regulating emotions and self-soothing: A child learns how to calmdown when a caregiver usessoothing techniques such as rocking,holding, and cooing. Over time, thechild learns how to calm down byhimself.
n Developing trust in others: When thecaregiver and child are attuned to eachother, the caregiver knows how torespond to the child’s needs and thechild learns that he can depend onothers. This leaves the child with asense the world is predictable and safe.
n Encouraging children to freelyexplore their environment: Becausethe child has learned that he can relyon others, he feels safe to explore theworld knowing that someone will bethere if he is in distress or needshelp. This exploration is the waychildren learn.
n Helping children understandthemselves and others: Thecaregiver-child relationship provides
the child with a model forunderstanding who she is, who thecaregiver is, and how the worldworks. Because the caregiverresponds, the world is seen as a safeplace where people can be trustedand depended upon.
n Helping children understand theycan have an impact on their world:Through interactions with thecaregiver, the child learns that he hasan impact on others. The child smilesand the caregiver smiles back; thechild laughs and the caregiver playswith her; the child cries and thecaregiver picks her up.
This natural process of attachmentmay be eroded by complex trauma invarious ways:• The caregiver may be the source of
the trauma.• The availability, reliability, or
predictability of the caregiver may be limited.
• The child may not learn to regulatehis emotions or calm himself downwhen experiencing intense emotions.
• The child’s ability to learn byexploring the world may take a backseat to the child’s need for protectionand safety.
• The child begins to perceive the worldas dangerous, leading to a sense ofvulnerability and distrust of others.
• As the child has little sense of herimpact on others, her lack of controlover her life leads to a sense ofhopelessness and helplessness.
C. Attachment and Complex Trauma
Attachment andComplex Trauma
n Complex trauma mostoften occurs within thecare giving system,which causes profounddisruptions inattachment andrelationshipdevelopment.
n Children with complextrauma often havecaregivers who haveexperienced complextrauma themselves.
n Children and caregiversmay requireconsiderable supportwhen complex traumais present.
18
UNDERSTANDING TRAUMATIC STRESS IN CHILDRENIV. COMPLEX TRAUMA
Caregivers should be aware thatmeeting the needs of children who haveexperienced complex trauma mayrequire assistance from trainedprofessionals. Nevertheless, childrenwill still require sustained support andunderstanding from caregivers atschool, child care, and at home.
Short-Term StrategiesCaregivers can help children cope
with complex trauma in the short term.Here are some suggestions:
n Establish safety. On-going traumaticexperiences leave children feeling theworld is dangerous and unpredictable.Children who have experiencedcomplex trauma have had experiencesof caregivers being unable to keepthem safe. Providing a safeenvironment can help children beginto recognize that safe places exist andcan support the healing process.• Identify safe places for children to
go when they feel overwhelmed. Atschool, a safe place may be thereading corner in a classroom,where a child can sit on a warmrug, look at books, or listen tomusic on headphones until he feelscalm again. A guidance counselor’soffice or an area of the playroomthat is removed from theclassroom’s main activity may alsobecome a safe place.
• Talk with the child to help herdetermine a safe place to go whenshe feels scared, overwhelmed, orsad. When a child shows signs ofdistress (e.g., crying, acting out,withdrawing), take the child asideand ask her if she would like to go toher safe place until she feels calmer.
• Remember that children need tofeel safe everywhere they go. Achild may feel safe in theclassroom, but may beoverwhelmed in otherenvironments. Helping childrenoutside of school involvescommunicating with other teachers,social workers, and primarycaregivers about what helps thechild feel safe.
n Create and maintain a routine.Structure and predictability helpchildren feel safe and secure:• Start and end the day in the same way.• Write down a schedule for the day
that can be posted next to thechild’s bed, on a classroom bulletinboard, or at the child’s desk.
n Recognize “triggers.” Triggers arereminders of the traumaticexperience and may cause the childto re-experience the emotionsassociated with a traumatic event.Triggers may include loud voices,hand gestures, fights, etc. Triggerswill vary from child to child.• Make a plan about how to respond
when a child is “triggered.”• This plan should involve the child
as well as the team working withthe child to ensure follow throughand support.
n Practice relaxation exercises. Deepbreathing, listening to soothingmusic, and muscle relaxation will helpchildren relieve some of their stress.
n Ensure children have a healthy dietand plenty of exercise. Traumaticexperiences effect physical health aswell as emotional health.• Children who have experienced
D. Tips for Caregivers
Self-Care
Over both the short- and
long-term, it is important
that caregivers take care of
themselves. Dealing with
traumatized children may
trigger intense and difficult
feelings in caregivers,
leaving them feeling
depleted and exhausted.
See Section V for more
information.
19
UNDERSTANDING TRAUMATIC STRESS IN CHILDREN IV. COMPLEX TRAUMA
multiple traumatic events are morelikely to get sick and experienceother health issues such as asthma,headaches, and stomach problems.Encourage children to eat well anddrink water throughout the day.
• Exercise and other recreationalactivities provide children withoutlets for distressing feelings and frustration.
n Engage in positive distractingactivities. These may include sports,games, reading, hobbies, etc.
Long-Term StrategiesChildren who have experienced
complex trauma often have seriousemotional needs that cannot be fullymet in school, child care, or homesettings. Here are some wayscaregivers can help:
n Refer children to appropriatecommunity agencies. Find acommunity agency that hasexperience working with childrenwho have experienced complextrauma. Guidance counselors and/orschool psychologists may help youconnect the child to appropriateservices.
n Use a team approach. Think of allthe people the child interacts withthroughout the day – teachers,coaches, extra-curricular activityleaders, etc. If you have concernsabout a child, talk to these people tosee if they share your concerns anddiscuss the best course of action.
n Help children identify safe peopleto talk with when they feeloverwhelmed. Ask children who theyfeel most comfortable with whenthey are upset.
n Be aware of Mandated Reporterlaws. Many caregivers are requiredto report suspected abuse to childwelfare authorities. Be aware of statelaws and work with your team todetermine when you may have tomake a report to protect a child.
n Maintain a connection with thechild’s support network. Thisnetwork may include teachers, socialworkers, case managers (throughlocal child welfare agencies), primarycaregivers, and the child’s extended family.
n Become “trauma-informed.” Thismeans having a basic understandingof how trauma effects people andusing this understanding to respondsensitively to those who have beenexposed to traumatic events. Thiswill also help you avoid re-traumatizing those who have hadtraumatic experiences. It is oftenhelpful to develop collaborativerelationships with other caregiversystems that have trauma-relatedexpertise. Becoming “trauma-informed” often begins with basictraining and technical assistanceabout traumatic stress and its effectson children.
n Be patient. Children who haveexperienced complex trauma willlikely have behavioral difficultiesranging from hyperactivity towithdrawal to frequent crying.Remember that healing from complextrauma can be a long-term process.

Caregivers of children worktirelessly to ensure the children’sneeds are met. This can be both
rewarding and draining. Tension oftenexists between feeling inspired by ourwork and feeling frustrated about themany things we cannot control. It isnot unusual to feel stressed andweighed down by working with childrenwho have been traumatized.
To understand self-care, it is helpfulto consider what it is not: Self-care isnot an “emergency response plan” tobe activated when stress becomesoverwhelming. Self-care is not aboutacting selfishly (“It’s all about me!”).Self-care is not about doing more oradding more tasks to an alreadyoverflowing “to-do” list.
Healthy self-care can renew ourspirits and help us to become moreresilient. Self-care is most effectivewhen approached proactively, notreactively. Think of self-care as havingthree basic aspects: awareness,balance, and connection — the “ABC’s”of self-care.
AWARENESS: Self-care begins instillness. By quieting our busy lives andentering into a space of solitude, wecan develop an awareness of our ownneeds, and then act accordingly. This isthe contemplative way of the desert,rather than the constant activity of thecity. Too often we act first, without true understanding, and then wonderwhy we feel more burdened rather than relieved.
BALANCE: Self-care is a balancing act.It includes balancing action andmindfulness. Balance guides decisions
about embracing or relinquishingcertain activities, behaviors, orattitudes. It also informs the degree towhich we give attention to the physical,emotional, psychological, spiritual, andsocial aspects of our being. In otherwords, how much time we spendworking, playing, and resting. Think ofthis healthy prescription for balanceddaily living: eight hours of work, eighthours of play, and eight hours of rest!
CONNECTION: Healthy self-care cannottake place solely within oneself. Itinvolves being connected in meaningfulways with others and to somethinglarger. We are interdependent andsocial beings. We grow and thrivethrough connections that occur infriendships, family, social groups,nature, recreational activities, spiritualpractices, therapy, and a myriad ofother ways.
There is no formula for self-care.Each of our “self-care plans” will beunique and change over time. As weseek renewal in our lives and work, wemust listen well to our own bodies,hearts, and minds as well as to trustedfriends. Caregivers should rely on otheradults and support systems (e.g.,church, mental health, etc.) to helpmeet their own emotional needs sothey will have enough energy tosupport a child who is stressed.
It may be useful for you to reflect onyour own self-care. The self-assessment checklist on the next pageis a way for you to pay attention to how(and how often) you care for yourself.
Self-Care
Adapted from: Kraybill, K. Healing Hands, Health Care for the Homeless Clinicians’ Network newsletter, Vol. 6, No. 2, February 2002.
20
UNDERSTANDING TRAUMATIC STRESS IN CHILDRENV. SELF-CARE
Thinking about…Self-Care
You are a senior teacherwho is mentoring threeyoung teachers who arestruggling with the demandsof their jobs, includingmanaging the behavior ofseveral children in theirclassrooms, and dealing withtheir overwhelming feelingsabout students withextensive trauma histories.They routinely seek you outfor advice and support.Youare concerned for them andeven though you alreadyhave many personal andprofessional demands, youprovide them with extensivesupervision every week andoften make phone calls forthem.You are beginning tonotice this is having animpact on how you feel atwork and at home.Whatsolution(s) best addresseveryone’s needs? Thinkabout this situation in termsof awareness, balance, andconnection.

21
UNDERSTANDING TRAUMATIC STRESS IN CHILDREN V. SELF-CARE
Assess Your Self-CareuHow often do you do the following? As you read the list below, rate the items using this scale:5 = Frequently, 4 = Occasionally, 3 = Sometimes, 2 = Never, 1 = It never even occurred to me.
Physical Self Care: o Eat regularly (e.g. breakfast & lunch) and healthfullyo Exercise (go to the gym, lift weights, practice martial arts, etc.)o Get medical care when needed and for preventiono Take time off when you’re sicko Do a physical activity that is fun for youo Take time to be sexualo Get enough sleepo Take vacations, day trips, or mini-vacationso Get away from stressful technology such as pagers, faxes, telephones, and e-mail
Psychological Self Care: o Make time for self-reflectiono Go to see a psychotherapist or counselor for yourselfo Read literature unrelated to work (or re-read a favorite book)o Do something at which you are a beginnero Notice your inner experience — your dreams, thoughts, imagery, feelingso Engage your intelligence in a new area — go to an art museum, performance,
sports event, etc.o Practice receiving from otherso Say no to extra responsibilities sometimes
Emotional Self Care: o Spend time with others whose company you enjoyo Stay in contact with important people in your lifeo Treat yourself kindly (supportive inner dialogue or self -talk)o Feel proud of yourselfo Identify and seek out comforting activities, objects, people, places, etc.o Allow yourself to cryo Find things that make you laugho Express your outrage in a constructive way
Spiritual Self Care: o Make time for prayer, meditation, reflectiono Spend time in natureo Participate in a spiritual gathering, community or groupo Cherish your optimism and hopeo Be open to mystery, not knowingo Identify what is meaningful to you and notice its place in your lifeo Sing and/or listen to musico Express gratitudeo Celebrate milestones with rituals that are meaningful to youo Remember and memorialize loved ones who are dead
Workplace Self Care: o Take time to eat luncho Take time to chat with co-workerso Make time to complete taskso Identify projects or tasks that are exciting, growth-promoting, and rewarding
for youo Arrange your workspace so it is comfortable and comfortingo Get regular supervision or consultationo Negotiate for your needs (benefits, pay raise)
Now, re-read the list and put a star next to one item in each category that you would like to incorporate into your dailyroutine. Revisit this list from time to time to help stay focused on caring for yourself.
Adapted from: Kraybill, K. Healing Hands, Health Care for the Homeless Clinicians’ Network newsletter, Vol. 6, No. 2, February 2002.

22
UNDERSTANDING TRAUMATIC STRESS IN CHILDRENREFERENCES AND RESOURCES
American Psychiatric Association (2000). Diagnostic and Statistical Manual of Mental Disorders,Fourth Edition. Washington, DC: American Psychiatric Association.
Berk, L. (1996). Infants and Children: Prenatal through Middle Childhood, Second Edition. Boston: Allyn & Bacon.
Cook, A., Spinazzola, J., Ford, J., et al. (2005). Complex Trauma in Children and Adolescents.Psychiatric Annals. 35(5): 390-398.
Herman, J. Trauma and Recovery. Basic Books, 1992, p. 34.
Kinninburgh, K. & Blaustein, M. (2005). Attachment, Self-Regulation & Competency: A ComprehensiveFramework for Intervention with Complexly Traumatized Youth. The Trauma Center.
James, B. (1994). Human Attachments and Trauma. Handbook for Treatment of Attachment –Trauma Problems in Children. New York: Lexington Books.
Kessler R.C., Sonnega, A., Bromet E., et al. (1995). Posttraumatic Stress Disorder in the NationalComorbidity Survey. Archives of General Psychiatry. 52(12):1048 – 1060.
Kraybill, K. Healing Hands, Health Care for the Homeless Clinicians’ Network newsletter, Vol. 6, No. 2,February 2002.
Macy, Robert, D. (2004). Basic Training Manual for PTSM, in Macy, R. et al. Community-Based, AcutePosttraumatic Stress Management: A Description and Evaluation of a Psychosocial-InterventionContinuum. Harvard Rev Psychiatry, July-Aug 2004.
National Child Traumatic Stress Network and National Center for PTSD, Psychological First Aid,September, 2005.
National Child Traumatic Stress Network, Complex Trauma Task Force (2003). White Paper: ComplexTrauma in Children and Adolescents.
Rothbaum, B.O. and Foa, E.B. (1993). Subtypes of Posttraumatic Stress Disoder and Duration ofSymptoms. In: Posttraumatic Stress Disorder: DSM-IV and Beyond, Davidson, J.R.T., Foa, E.B., eds.Washington, D.C.: American Psychiatric Press, pp. 23 – 35.
Stubblefield-Tave, J. Kinniburgh,K. Zucker, M., et al. (October 2005). Complex Trauma in Toddlers andSchool-Aged Children. The Judges’ Page Newsletter. National CASA Association and National Councilof Juvenile and Family Court Judges. Available at www.nationalcasa.org/Judgespage.
Yehuda, R. (2002). Posttraumatic Stress Disorder. New England Journal of Medicine, 346(2): 108-114.
Yehuda, R. (2003). Changes in the Concept of PTSD and Trauma. Psychiatric Times, 20(4).
ResourcesThe National Center on Family Homelessness (www.familyhomelessness.org)The National Center on Family Homelessness has been devoted to helping homeless children and theirfamilies for almost twenty years through applied research and innovative program development.
The National Child Traumatic Stress Network (www.nctsnet.org)The National Child Traumatic Stress Network is a federally funded collaboration of over 54 sites(including the National Center on Family Homelessness) working on issues of trauma and children.
The National Health Care for the Homeless Council (www.nhchc.org)The National Health Care for the Homeless Council is a membership organization whose mission is tohelp bring about reform of the health care system to best serve the needs of people who are homeless,to work in alliance with others whose broader purpose is to eliminate homelessness, and to providesupport to Council members.
The Trauma Center (www.traumacenter.org)The Trauma Center helps individuals, families and communities impacted by trauma and adversity tore-establish a sense of safety and predictability in the world, and to provide them with state-of-the-arttherapeutic care as they reclaim, rebuild and renew their lives.
References

O U R M I S S I O N
To discover what works | To educate and inspire To take action to end family homelessness
181 Wells Avenue | Newton Centre, MA 02459 | 617-964-3834
Visit our website to learn more at www.familyhomelessness.org
u