Effects of Norepinephrine on Coronary Circulation...
13
Effects of Norepinephrine on Coronary Circulation and Left Ventricular Dynamics in the Conscious Dog By Stephen F. Vatner, Charles B. Higgins. and Eugene Braunwald ABSTRACT The effects of norepinephrine (0.1 and 1.0 Mg/kg, iv) on coronary blood flow and resistance, left ventricular pressure and diameter, dP/dt, (dP/dt)/P, and the velocity (V lso ) of myocardial fiber shortening were studied in conscious dogs. When the heart rate was held constant, norepinephrine caused an initial reduction in coronary vascular resistance which was associated with increases in mean arterial blood pressure, systolic left ventricular pressure, end-diastolic diameter, dP/dt, (dP/dt)/P, and V iso . After this brief coronary vasodilator response, a sustained increase occurred in mean coronary vascular resistance (+0.55 ± 0.07 mm Hg/ml min"'), and increases persisted in mean arterial blood pressure (+67 ± 7 mm Hg), left ventricular systolic pressure (+74 ± 6 mm Hg), left ventricular end-diastolic pressure (+4 ± 1 mm Hg), left ventricular internal diameter ( + 1.3 ± 0.3 mm), peak dP/dt ( + 1660 mm Hg/sec), (dP/dt)/P ( + 15 ± 2 sec"), and V iso ( + 11 ± 2 mm/sec); coronary sinus Po 2 decreased. Beta-receptor blockade pre- vented the inotropic effects of norepinephrine, attenuated the early coronary vasodilator effects, and increased the late vasoconstrictor effects. Alpha-receptor blockade abolished the late coronary vasoconstrictor effects of norepinephrine; only dilatation occurred. In contrast to the effects of norepinephrine in conscious dogs without autonomic blockade, norepinephrine (1.0 ^g/kg, iv) failed to produce late coronary vasoconstriction in anesthe- tized, open-chest dogs; only dilatation occurred. Thus, in the normal, conscious dog, nor- epinephrine exerts an important coronary vasoconstrictor effect which is sufficiently in- tense to counteract completely the simultaneous tendency toward metabolic vasodilata- tion. KEY WORDS catecholamines alpha receptors beta receptors coronary vasoconstriction myocardial contractility left ventricular diameter • Norepinephrine exerts a direct constricting ef- fect on coronary vessels mediated by activation of alpha receptors (1-6) and a direct dilating effect mediated by activation of beta receptors (4-9). It is widely held that these direct effects are overshad- owed in the beating heart by the metabolic coro- nary vasodilatation induced by norepinephrine's powerful stimulation of myocardial oxygen con- sumption, which results from increases in ventricu- lar pressure and contractility (1-6, 8). However, this concept is based largely on studies in anesthe- From the Departments of Medicine, Harvard Medical School and Peter Bent Brigham Hospital, and the Department of Cardiology, Children's Hospital Medical Center, Boston, Mas- sachusetts 02115. This study was supported in part by U. S. Public Health Service Grant HL 15416 from the National Heart and Lung Institute. Dr. Vatner is an Established Investigator of the American Heart Association. Parts of this investigation were presented at the 45th Scientific Sessions of the American Heart Association, Novem- ber 18, 1972. Received April 26, 1973. Accepted for publication March 13, 1974. 812 tized animal preparations (1, 2, 4-8); norepineph- rine's action could be altered by the effects of the anesthetic agent and the open chest. Other cardio- active agents have substantially different actions in conscious and anesthetized animals (10-14), and the effects of norepinephrine on the left ventricle and the coronary vessels in normal, unanesthetized animals could differ from those observed in anes- thetized, open-chest preparations. In a previous study in conscious dogs (3), only coronary vaso- dilatation was observed when norepinephrine was administered; however, that study only reported peak responses. Therefore, responses occurring later, when inotropic stimulation has subsided and alpha-adrenergic effects are not overshadowed to such a great extent by increases in ventricular pressure and contractility, should also be studied. Accordingly, in this investigation, we adminis- tered norepinephrine to healthy, conscious dogs instrumented for direct, continuous measurement of left circumflex coronary blood flow, left ventricu- lar and systemic arterial pressures, left ventricular diameter, dP/dt, and the velocity of myocardial Circulation Research. Vol. XXXIV. June 1974 by guest on May 20, 2018 http://circres.ahajournals.org/ Downloaded from
Transcript of Effects of Norepinephrine on Coronary Circulation...

Effects of Norepinephrine on Coronary Circulation and LeftVentricular Dynamics in the Conscious Dog
By Stephen F. Vatner, Charles B. Higgins. and Eugene Braunwald
ABSTRACTThe effects of norepinephrine (0.1 and 1.0 Mg/kg, iv) on coronary blood flow and
resistance, left ventricular pressure and diameter, dP/dt, (dP/dt)/P, and the velocity(Vlso) of myocardial fiber shortening were studied in conscious dogs. When the heart ratewas held constant, norepinephrine caused an initial reduction in coronary vascularresistance which was associated with increases in mean arterial blood pressure, systolicleft ventricular pressure, end-diastolic diameter, dP/dt, (dP/dt)/P, and Viso . After thisbrief coronary vasodilator response, a sustained increase occurred in mean coronaryvascular resistance (+0.55 ± 0.07 mm Hg/ml min"'), and increases persisted in meanarterial blood pressure (+67 ± 7 mm Hg), left ventricular systolic pressure (+74 ± 6 mmHg), left ventricular end-diastolic pressure (+4 ± 1 mm Hg), left ventricular internaldiameter ( + 1.3 ± 0.3 mm), peak dP/dt ( + 1660 mm Hg/sec), (dP/dt)/P ( + 15 ± 2 sec"),and Viso ( + 11 ± 2 mm/sec); coronary sinus Po2 decreased. Beta-receptor blockade pre-vented the inotropic effects of norepinephrine, attenuated the early coronary vasodilatoreffects, and increased the late vasoconstrictor effects. Alpha-receptor blockade abolishedthe late coronary vasoconstrictor effects of norepinephrine; only dilatation occurred. Incontrast to the effects of norepinephrine in conscious dogs without autonomic blockade,norepinephrine (1.0 ^g/kg, iv) failed to produce late coronary vasoconstriction in anesthe-tized, open-chest dogs; only dilatation occurred. Thus, in the normal, conscious dog, nor-epinephrine exerts an important coronary vasoconstrictor effect which is sufficiently in-tense to counteract completely the simultaneous tendency toward metabolic vasodilata-tion.
KEY WORDS catecholamines alpha receptors beta receptorscoronary vasoconstriction myocardial contractility left ventricular diameter
• Norepinephrine exerts a direct constricting ef-fect on coronary vessels mediated by activation ofalpha receptors (1-6) and a direct dilating effectmediated by activation of beta receptors (4-9). It iswidely held that these direct effects are overshad-owed in the beating heart by the metabolic coro-nary vasodilatation induced by norepinephrine'spowerful stimulation of myocardial oxygen con-sumption, which results from increases in ventricu-lar pressure and contractility (1-6, 8). However,this concept is based largely on studies in anesthe-
From the Departments of Medicine, Harvard Medical Schooland Peter Bent Brigham Hospital, and the Department ofCardiology, Children's Hospital Medical Center, Boston, Mas-sachusetts 02115.
This study was supported in part by U. S. Public HealthService Grant HL 15416 from the National Heart and LungInstitute.
Dr. Vatner is an Established Investigator of the AmericanHeart Association.
Parts of this investigation were presented at the 45thScientific Sessions of the American Heart Association, Novem-ber 18, 1972.
Received April 26, 1973. Accepted for publication March 13,1974.
812
tized animal preparations (1, 2, 4-8); norepineph-rine's action could be altered by the effects of theanesthetic agent and the open chest. Other cardio-active agents have substantially different actionsin conscious and anesthetized animals (10-14), andthe effects of norepinephrine on the left ventricleand the coronary vessels in normal, unanesthetizedanimals could differ from those observed in anes-thetized, open-chest preparations. In a previousstudy in conscious dogs (3), only coronary vaso-dilatation was observed when norepinephrine wasadministered; however, that study only reportedpeak responses. Therefore, responses occurringlater, when inotropic stimulation has subsided andalpha-adrenergic effects are not overshadowed tosuch a great extent by increases in ventricularpressure and contractility, should also be studied.
Accordingly, in this investigation, we adminis-tered norepinephrine to healthy, conscious dogsinstrumented for direct, continuous measurementof left circumflex coronary blood flow, left ventricu-lar and systemic arterial pressures, left ventriculardiameter, dP/dt, and the velocity of myocardial
Circulation Research. Vol. XXXIV. June 1974
by guest on May 20, 2018
http://circres.ahajournals.org/D
ownloaded from

NOREPINEPHRINE-INDUCED CORONARY VASOCONSTRICTION 813
fiber shortening. The goal of the present study wasto clarify norepinephrine's normal action by com-paring its effects when it was administered (1)intravenously in a bolus or an infusion, (2) beforeand after administration of selecti%'e alpha- andbeta-receptor blocking agents, and (3) before andafter induction of hypoxia. Results following ad-ministration of norepinephrine to intact, consciousanimals were also compared with those followingadministration to anesthetized animals with anopen chest.
MethodsTwelve mongrel dogs (24-34 kg) were anesthetized
with sodium pentobarbital (30 mg/kg, iv) and a thoracot-omy was performed in the fifth left intercostal space.Miniature Konigsberg P22 pressure gauges were im-planted within the left ventricle through a stab wound inthe apex (10 dogs). Opposing ultrasonic diametertransducers1 were sutured to the epicardium of theanterior and posterior walls of the left ventricle (6 dogs)or implanted on opposing endocardial surfaces of the leftventricle (4 dogs), and Doppler ultrasonic transducers(10 dogs) or Statham SP2200 electromagnetic transduc-ers (2 dogs) were placed around the left circumflexcoronary artery. Stimulating electrodes were sutured tothe left ventricle (10 dogs), and heparin-filled Tygoncatheters were chronically implanted in the thoracicaorta (12 dogs). During a subsequent operation, 4 dogswere anesthetized with sodium pentobarbital (30 mg/kg,iv) and a right thoractomy was performed; heparin-filledTygon catheters were implanted in the coronary sinus.Five additional dogs were anesthetized with sodiumpentobarbital (30 mg/kg, iv) and studied with theirchests open immediately after placement of StathamSP2200 electromagnetic flow transducers on the leftcircumflex coronary artery, Konigsberg P22 miniaturepressure gauges in the left ventricle, and catheters in theaorta.
The miniature pressure gauges were calibrated in vivoagainst a calibrated Statham P23Db strain-gauge ma-nometer. At autopsy the position of the ventriculargauges within the ventricular cavity was confirmed.Arterial blood pressure was sampled with the previouslyimplanted heparin-filled Tygon catheter and measuredwith a Statham P23Db strain-gauge manometer. Leftcircumflex coronary blood flow was measured with anultrasonic Doppler flowmeter in eight dogs. This system,which has been described in detail previously, has areliable zero reference (15, 16). In the present experi-ments, the electrical zero blood flow was determinedrepeatedly and was confirmed by calibration terminally.The relationship between velocity, as measured by theDoppler flowmeter. and volume flow is linear as long asthe cross-sectional area of the blood vessel within thetransducer remains constant. This linear relationshipbetween velocity and volume flow has been demonstratedrepeatedly and confirmed by time collections of bloodflow (16). At the time of autopsy, the vessels were firmly
attached to the flow transducers by a fibrous scar whichminimized changes in the cross-sectional area of the ves-sel within the flow transducers. In two conscious dogsand five anesthetized open-chest dogs, a Statham SP2200electromagnetic flowmeter was used to measure coronary-blood flow. In these experiments, zero blood flow was de-termined by inflating a previously implanted, hydraulicocclusive cuff.
An improved ultrasonic transit time dimension gauge2
was used to measure left ventricular diameter (17); itsprinciple of operation is similar to that of other ultra-sonic gauges described previously (18, 19). It measuredthe transit time of acoustic impulses traveling at thesonic velocity of approximately 1.5 x 106 mm/sec be-tween the 5- or 3-MHz piezoelectric crystals that weresutured at opposing sites to the left ventricular epicar-dium or endocardium. This gauge was calibrated bysubstituting signals of a known time duration from acalibrated pulse generator. A voltage proportional totransit time was recorded and calibrated in terms ofcrystal separation. Thus, a measure of the external or theinternal diameter of the left ventricle was continuouslyrecorded. At a constant temperature, the drift of theinstrument was less than 0.15 mm/hour, and its fre-quency response was flat to 60 Hz.
The experiments were conducted 3 weeks to 2 monthsafter surgery when the dogs had recovered from theoperation and were vigorous and healthy. While theunsedated dogs were resting quietly, control records ofleft ventricular pressure and diameter, the time rate ofchange of diameter (dD/dt), i.e., the velocity of myocar-dial shortening, the rate of change of pressure, (dP/dt),left circumflex coronary blood flow, arterial blood pres-sure, and heart rate were obtained. These variables werecontinuously recorded during all interventions. In 12conscious dogs, norepinephrine (0.1 and 1.0 Mg/kg) wasadministered intravenously as a bolus via a peripheralvein; it was administered as an infusion at the rate of 0.5Mg/kg min"' in 5 dogs and 0.2 Mg/kg min~' in 3 dogs by aHarvard model 940 drug infusion pump.
All dogs were studied while their heart rate wascontrolled by electrical stimulation of the ventricles at afrequency slightly higher than the spontaneous rhythm.Heart rate was again controlled while eight dogs werestudied on a separate day after beta-receptor blockadewith propranolol3 (1.0-2.0 mg/kg, iv) and six dogs werestudied after alpha-receptor blockade withphentolamine4 (0.2-1.0 mg/kg, iv). The adequacy ofbeta-receptor blockade was tested with isoproterenol (1Mg/kg, iv). Alpha-receptor blockade was assessed withnorepinephrine (1.0 Mg/kg> iv); 0.1 Mg/kg of norepineph-rine was the smallest dose that consistently causedperceptible changes in systemic and coronary dynamics,and 1.0 Mg/kg was the largest dose that the consciousdogs could consistently tolerate without adverse sideeffects. Norepinephrine (1.0 Mg/kg, iv) was administeredto five conscious dogs made hypoxic by breathing 10% O2through a face mask. In these experiments as well asthose in anesthetized open-chest dogs and those in whichthe O2 content of coronary sinus blood was tested,
1 Construction details available upon request to the authors.Circulation Research. Vol. XXXIV. June 1974
2 Circuit diagrams available upon request to the authors.3 Generously supplied by Ayerst Co.* Generously, supplied by Ciba Co.
by guest on May 20, 2018
http://circres.ahajournals.org/D
ownloaded from

814 VATNER, HIGGINS. BRAUNWALD
arterial Po2 was measured with a Copenhagen radiome-ter (model PHM-72) blood-gas analyzer.
Data were recorded on a multichannel tape recorderand played back on a direct-writing oscillograph at apaper speed of 100 mm/sec. A cardiotachometer trig-gered by the signal from the pressure pulse providedinstantaneous, continuous records of heart rate. Elec-tronic resistance-capacitance filters with 2-second timeconstants were used to derive mean arterial bloodpressure and mean left circumflex coronary blood flow.Mean and late diastolic coronary vascular resistanceswere calculated as the quotients of the mean and the latediastolic arterial blood pressures and coronary bloodflows, respectively. Continuous records of dP/dt anddD/dt were derived from the left ventricular pressure anddiameter signals by using Philbrick operational amplifi-ers connected as differentiators having frequency re-sponses of 60 or 30 Hz, respectively. A triangular wavesignal with a known slope (rate of change) was substi-tuted for pressure and diameter signals to calibrate thedP/dt and dD/dt channels directly.
The effects of norepinephrine on myocardial force-velocity relationships were assessed by determining thevelocity of shortening and the intraventricular pressureat an identical ventricular diameter (isolength point),i.e., Vls(,; this technique has been described previously(11, 13, 14, 20-22). All isolength points were obtainedduring the first one-third of ejection. In addition, theeffects of norepinephrine on peak dP/dt and the quotientof dP/dt and developed pressure (left ventricular isovo-lumic pressure minus end-diastolic pressure), i.e., (dP/dt)/P, were examined. The same level of pressure thatoccurred during isometric contraction, before and aftereach intervention, was used for the calculation, anddP/dt and developed pressure were determined at thatlevel of pressure. This technique for evaluating themyocardial contractile state has also been describedpreviously (11, 13, 14, 21-23).
Results
Norepinephrine administered intravenously as abolus produced two distinct phases of action. First,the peak increase in coronary blood flow and themaximal reduction in coronary resistance occurred20-30 seconds after injection. This point, desig-nated A in Figure 1 and in the following discussion,was used to describe the early effect. Later, asustained rise in coronary resistance above controllevels occurred while pressures and contractilityremained elevated (Fig. 2). This point, designatedB in Figure 1 and in the following discussion wasrecorded 60 seconds after injection. The resultswith the larger dose of norepinephrine (1.0 Mg/kg)will be discussed in detail, but the results with thesmaller dose (0.1 Mg/kg) are simply presented inTables 1 and 2 and illustrated in Figures 1, 3, and4. The paired £-test was used to compare the resultsat points A and B with the control results and tocompare the changes from control at points A and
NE I.Ojig/Kg
ARTERIALPRESSURE(mmHg)
MEAN PRESSURE(mmHg}
CORONARYFLOW VELOCITY(cm/sec)
MEAN FLOW(ml/min)
CALCULATEDMEAN CORONARYRESISTANCE ~
ml/mHEART RATE(beols/min)
200
100
0
200
100
0
120 "
60 -
0 .
150 "
75 -
0 .
30
20
"jOO "I
150 -I0 -
FIGURE 1
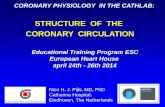
Typical responses to intravenously administered norepineph-rine (NE), 1.0 iiglkg (left) and 0.1 uglkg (right), when the heartrate was held constant. Responses for phasic and mean arterialblood pressure, phasic and mean left circumflex coronary flowvelocity, calculated mean coronary resistance, and heart rateare shown. Both doses of norepinephrine decreased coronaryresistance initially (A) and then produced a later, sustainedperiod of uasoconstriction (B).
B in the different states for the same dog. Thegroup i-test was used to compare the changes in theanesthetized open-chest dogs. Significance wasdetermined at the 0.05 level (24).
NORMAL CONSCIOUS DOGS: BOLUS INJECTION
Pressures.—Norepinephrine (1.0 ^g/kg) in-creased mean arterial blood pressure from 97 ± 3(SE) mm Hg to 172 ± 7 mm Hg at point A; pressureremained elevated at 165 ± 6 mm Hg at point B(Table 2). Late diastolic pressure increased bysimilar amounts (Fig. 3). Left ventricular peaksystolic and isolength systolic pressures increasedsimilarly; the latter rose from a control value of121 ± 2 mm Hg to 193 ± 7 mm Hg at point A andremained elevated at 195 ± 6 mm Hg at point B.Left ventricular end-diastolic pressure increasedfrom a control of 6 ± 1 mm Hg to 10 ± 1 mm Hg atpoint A and remained elevated at 10 ± 1 mm Hg atpoint B.
Diameters.—Norepinephrine (1.0 Mg/kg) in-creased left ventricular end-diastolic external andinternal diameters by 1.3 ± 0.3 (SE) mm and 1.2 ±0.1 mm, respectively, at point A from controlvalues of 61.7 ± 1.1 mm and 35.6 ± 0.9 mm,respectively (Table 1). End-diastolic diametersremained at the same level at point B (Fig. 4). Leftventricular end-systolic diameters increased bysmall amounts (Table 1).
Contractility.—Norepinephrine (1.0 /xg/kg) in-creased peak dP/dt from 3350 ± 210 (SE) mm
Circulation Research. Vol. XXXIV. June 1974
by guest on May 20, 2018
http://circres.ahajournals.org/D
ownloaded from

NOREPINEPHRINE-INDUCED CORONARY VASOCONSTRICTION 815
CONTROL NOREPINEPHRINE
LV DIAMETER(mm)
LV VELOCITY(mm/sec)
LV PRESSURE(mmHg)
LV PRESSURE(mmHg)
dP/dt(mmHg/sec)
HEART RATE(beots/min)
26 J-100 •
o -+45 .200 •
100 -0 .
30
0 J+7.000.
0-3,000
250
125
0
SPONTANEOUSRHYTHM PACED
V----H-"- 1 ^ . . A_UI I i
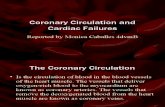
FIGURE 2
Typical response to norepinephrine. 1.0 fig/kg, for phasic wave forms of left ventricular (LV) internaldiameter, velocity, and systolic and diastolic pressures. dP/dt. and heart rate. Left: Controlrecordings in spontaneous rhythm and during ventricular pacing. Right: early responses (A) associ-ated with coronary dilatation and late responses (B) associated with coronary vasoconstriction.
Hg/sec to 9620 ± 350 mm Hg/sec at point A (Table1); this variable remained elevated above thecontrol level and was 5010 ± 290 mm Hg/sec atpoint B. (dP/dt)/P increased from 38 ± 2 sec"1 to66 ± 2 sec"1 at point A and remained elevatedabove the control level at a value of 53 ± 2 sec"' atpoint B. Left ventricular isolength velocity in-creased from 61 ± 4 mm/sec to 76 ± 6 mm/sec atpoint A and remained elevated above the controllevel at a value of 72 ± 5 mm/sec at point B.
Coronary Dynamics.—Norepinephrine (1.0 \iglkg) dilated the coronary vascular bed at point A. Atthis point, mean coronary blood flow rose from acontrol of 48 ± 3 (SE) ml/min to a maximal level of112 ± 5 ml/min; late diastolic flow rose similarly(Table 2). Mean coronary vascular resistance fellfrom 2.05 ± 0.11 mm Hg/ml min"1 to 1.56 ± 0.10mm Hg/ml min"1; late diastolic coronary resist-ance decreased similarly (Fig. 3). However, meanand late diastolic coronary blood flows began toreturn to the control level, but left ventricularpressures, dimensions, and contractility remainedelevated and a sustained increase in mean and latediastolic resistance ensued (Figs. 1, 4). At point B,mean and late diastolic coronary blood flows wereonly 16 ± 2 ml/min and 18 ± 3 ml/min above thecontrol level, whereas calculated mean and latediastolic coronary resistances had increased by0.55 ± 0.07 mm Hg/ml min"' and 0.50 ± 0.05 mmCirculation Research. Vol. XXXIV. June 1974
Hg/ml min \ respectively, above the control lev-els. The effect of the smaller dose of norepinephrine(0.1 ngfkg) was slightly different in that coronaryblood flow was not significantly elevated at point B(Table 2); in fact, in several experiments it actuallyfell below the control level at point B despiteelevated pressures and contractility. After fallingbelow the control level at point A, mean and latediastolic coronary resistances rose by 0.29 ± 0.05mm Hg/ml min"1 and 0.28 ± 0.06 mm Hg/mlmin"1, respectively, above the control levels atpoint B.
Thus, when norepinephrine was administeredintravenously as a bolus in the conscious dog, abrief early period of coronary dilatation occurredand was followed by a sustained period of coronaryvasoconstriction despite elevated left ventricularpressures, dimensions, and contractility.
Arterial and Coronary Sinus Oxygen.—Duringthe period of coronary vasoconstriction that oc-curred after the injection of norepinephrine (1.0^g/kg), i.e., at point B, arterial Po2 remained atcontrol levels of 84 ± 3 (SE) mm Hg, but in fourconscious dogs coronary sinus Po2 fell from 16 ± 1mm Hg to 13 ± 1 mm Hg (P < 0.01).
CONSCIOUS DOGS WITH ADRENERGIC BLOCKADES
Beta-Receptor Blockade.—Following the admin-istration of propranolol (1.0-2.0 mg/kg, iv) and
by guest on May 20, 2018
http://circres.ahajournals.org/D
ownloaded from

816 VATNER. HIGGINS. BRAUNWALD
DCO
Qw:
O
coQ
g
Ic0)cC-cD&
1
fect
s
-̂_o"3
<1
CQ
<1
<̂
"o
coO
CD _
o Jjp
H ^Z —
O l
d
—d
d-H
CO
d
CM—*
-H
—;
-Hco.CMCD
CM
d-H
l ~ ;
d
q—
'55.9
CM
•H[ - ;
CMCD
O
—
CM
l Oi O
—
—
61.7
±
o
mm
)
O
iam
e
CO
c
1
d
o— •
d
CO
CM_ '
41CM
*£d4 j
q
CO
4—CM
d-H
t -
d' M
CO
-
-H
/55.
9
d•H
oCOCD
O—
-H
2——
61.7
±
o—
"o
d-sy
s
ccu
"5
dia
73
rMd41
—
d4 —
d-II
COd
—-H
"^
9/2'
d•H
%
H—CM
d-H
CO
dCO
d-H
^^
—
-H
'29.
9
o
+1
COCO
—
—
CM
d
35.6
±
o
'i
<u
amet
=5cc
c«c
d
a;d
d
CO
-Ho
CO
—
41
d-H
d
d+1
CM
—'
O
CD
d
CO
CDCO
—
—
-H
aiCM
cnd
35.6
±
o
—
CJ
tol
d-sv
s
c~5i"o
en
dia
ld-
—
41
- T
-t—
^ - .
+)00CO
—
»O
-H
CO
CO
o
COm41
„o
o>
*
-H
4|
O^
•
' ^
- ^
[ ^
CD
-H
CO
CM
T f
COm+1
to
o—
COcu
41
CN!
-«
j :<M
-HCM
4)
137
„-H
CO
41
724
CO
aCO
^ -
-H
-H
:5/l
41—^
!
-nCO
CM\
125
±:
o
"SB
s
IT3
a,
CO
"H
5:i ^
•H
—
-HO
CO41
2^;
J I
200
#
-H
*
41
CO
41( ^CO
-
o
-H
9/li
-HO )
CM
—
+1CO
CM\
125
± 2
o
ED
P)
• ^
• e .
olen
g
a
a.
*o
o
300
s
*41
370
41o
472
o
CM
o
»C
CO
__,
o
?/se
c)
*T"
C
IP/C
099
—
o
l O
oCO
-H
o
CD
4)o
i
oCM
41
O
CO
o—
4 -
TI
41
^
CM
M
0 0
CO
41
"^
CM
0 0CO
^ -
C J
(sec
(ip
3
CM
41
in
#CM
41O OO l
41CO
CM
410 0CO
o
03
and
<;
"SO
• ^
cCD
-ao
CO
CDCU
™CUr!
neph
rii
' acu
nor
!!
z
SE.
-H
lean
s
E
IB S31
"I><
0.01
05
V °V
. a.
ican
tca
nt.
• •— t ^
& E•S .5!» •»cu a
f 1O O* 4—
with heart rate maintained constant at 106 ± 4beats/min, norepinephrine (1.0 ^g/kg) producedincreases in systolic left ventricular and arterialblood pressures that were similar to those in theunblocked dog. Mean arterial blood pressure in-creased by 67 ± 4 (SE) mm Hg at point A andremained 61 ± 4 mm Hg above the control level atpoint B (Table 2). Similar increases occurred inlate diastolic arterial pressures. However, after theadministration of propranolol, norepinephrinecaused greater increases (P < 0.01) in end-systolic(1.8 ± 0.4 mm) and end-diastolic (2.2 ± 0.5 mm)diameters and in left ventricular end-diastolicpressure (7 ± 1 mm Hg) and prevented theincreases in contractility, as shown by the valuesof peak dP/dt, (dP/dt)/P, and Vjso. When the re-sponses in the coronary vascular bed of the pro-pranolol-treated dogs were compared with those ofthe normal dogs, the increases in mean and latediastolic coronary blood flows (35 ± 3 ml/min and40 ± 3 ml/min, respectively) and the reductions inmean and late diastolic coronary vascular resist-ances (-0.22 iO.OemmHg/mlmin-'and -0.12 ±0.04 mm Hg/ml min~', respectively) were less (P <0.01) at point A than those observed in the un-blocked dogs. However, the increases at point B inmean and late diastolic coronary resistances (0.81± 0.09 mm Hg/ml min~' and 0.60 ± 0.05 mmHg/ml min"1, respectively) were slightly greaterthan those observed in the unblocked dogs (P <0.05) (Table 2).
Thus, beta-receptor blockade modified the re-sponse to norepinephrine by preventing the in-creases in contractility and by attenuating theearly coronary vasodilatation.
Alpha-Receptor Blockade.—Following the ad-ministration of phentolamine (0.5-1.0 mg/kg, iv)and with heart rate maintained constant at 144 ± 9beats/min, norepinephrine (1.0 Mg/kg) only slightlyincreased left ventricular systolic pressure andmean and late diastolic arterial blood pressures atboth points A and B, although mean and latediastolic coronary blood flows increased at bothpoints A and B (Table 2). At point A mean and latediastolic coronary resistances had decreased fromthe control value by 0.36 ± 0.09 (SE) mm Hg/mlmin"1 and 0.23 ± 0.07 mm Hg/ml min"1, respec-tively; at point B they remained depressed by0.29 ± 0.10 mm Hg/ml min"1 and 0.18 ± 0.08 mmHg/ml min"1, respectively, below the control level.The responses in the coronary vascular bed afteralpha-receptor blockade were significantly differ-ent from those before blockade in the following
Circulation Research. Vol. XXXIV, June 1974
by guest on May 20, 2018
http://circres.ahajournals.org/D
ownloaded from

irculat %'
ft:
^search . Vol. .•5 June
Cor
onar
y D
ynam
ic E
ffec
ts o
f N
orep
inep
hrin
e
Sta
te
I
Con
scio
us,
unbl
ocke
dC
onsc
ious
, un
bloc
ked
Con
scio
us,
beta
-re
cept
or b
lock
ade
Con
scio
us,
alph
a-re
cept
or b
lock
ade
Ane
sthe
tize
d, o
pen-
ches
t
Con
scio
us,
unbl
ocke
dC
onsc
ious
, un
bloc
ked
Con
scio
us,
beta
-re
cept
or b
lock
ade
Con
scio
us,
alph
a-re
cept
or b
lock
ade
Ane
sthe
tize
d, o
pen-
ches
t
Con
scio
us,
unbl
ocke
dC
onsc
ious
, un
bloc
ked
Con
scio
us,
beta
-re
cept
or b
lock
ade
Con
scio
us,
alph
a-re
cept
or b
lock
ade
Ane
sthe
tize
d, o
pen-
ches
t
NE
dose
iA<g
/kg)
0.1
1.0
1.0
1.0
1.0
0.1
1.0
1.0
1.0
1.0
0.1
1.0
1.0
1.0
1.0
N 10 12 8 6 5 10 12 8 6 5 10 12 8 6 5
Con
trol
TABL
E 2
A
Art
eria
l P
ress
ure
(mm
Hg)
(M
ean/
Lat
e99
± 3
/83
± 6
97 ±
3/8
1±
510
3 ±
3/8
6 ±
3
90 ±
3/7
2 ±
3
109
± 1
0/90
± 9
122
± 4
/105
± 3
172
± 7
/150
± 6
170
± 6
/145
± 7
99 ±
4/8
1 ±
3
160
± 1
6/14
2 ±
13
Cor
onar
y F
low
(m
l/m
in)
(Mea
n/L
ate
i
50 ±
3/5
6 ±
348
± 3
/54
± 3
45 i
4/
51 ±
5
52 ±
4/5
6 ±
4
51 ±
4/5
6 ±
4
68 ±
4/7
8 ±
511
2 ±
5/1
23 ±
580
± 5
/90
± 5
70 ±
5/1
5 ±
5
125
± 1
8/13
4 ±
20
A
Dia
stol
ic) 23
± 3
*/22
± 3
*75
± 6
*/69
± 6
*67
± 4
*/59
± 6
*
9±
l*t/
9 =t
1*"
51 ±
9*/
52±
9*
Dia
stol
ic) 18
± 2
*/22
± 3
*64
± 3
V69
± 3
*35
±
3*t/
40
18 ±
3*t
/19
74 ±
19*
/78
Cor
onar
y R
esis
tanc
e (m
m
Hg/
ml
min
~')
(M
ean/
Lat
e D
iast
olic
)
2.03
x 0
.13/
1.52
± 0
.09
2.05
± 0
.11/
1.54
± 0
.08
2.31
± 0
.20/
1.75
± 0
.14
1.80
x 0
.16/
1.32
i
0.12
2.17
± 0
.58/
1.60
± 0
.44
1.83
± 0
.10/
1.40
± 0
.09
1.56
± 0
.10/
1.24
± 0
.09
2.09
± 0
.17/
1.63
± 0
.15
1.44
± 0
.09/
1.09
± 0
.07
1.33
± 0
.11/
0.95
±0
.33
-0.2
0 ±
0.0
5V
-0.
-0.4
9 ±
0.0
7V
0.0.
22 ±
0.0
6*t/
0.
± 3
:
± 3
*
± 2
1
12 ±
30 ±
12 -
i
-0.3
6 ±
0.0
9V
0.23
±
-0.8
4 ±
0.3
0V
0.65
±
1- *t t * 0.02
*0.
06*
0.04
ft
0.07
*
0.22
*
116
165
164 96 148 51 64 52 65 71
2.32
±2.
60 ±
3.12
±
1.51
i
2.10
±
B
± 3
/101
± 3
± 6
/144
± 5
± 6
/139
± 5
± 3
/78
±
± 1
8/13
1
± 3
/57
±±
3/7
2 ±
± 4
/59
±
± 4
/70
±
± 6
/79
±
0.04
/1.8
00.
14/2
.04
0.25
/2.3
5
0.09
/1.1
4
0.26
/1.5
4
3 ± 15
3 3 5 4 7 i 0.
09i
0.10
i 0.
22
±0.
08
-i 0.
23
0.29 0.55
0.81
•0.2
9 =
0.07
17 68 61 6 39
1 16 7 13 20 i ± i: t C ±
A
± 2
V1
8 ±
± 6
V63
±±
4V
53 ±
± lf
t/6
±
±
10*§
/41
±
1/1
± 1
± 2*
/I8
±
± r/
9 ±
:
± 3
*/14
i
± 4
*/23
-i
0.05
V0.
280.
07*/
0.50
0.09
5/0.
60
3* 6* 5* 2tt
±
10*§
3* 1 * 3* 5* ±
0.06
*±
0.05
± 0.
05 §
).10*
t/ 0.
18 i
0.0
8*t
0.07
t/-0
.06
i 0.
07t
Z o X TO
TJ Z m TJ X X z m z o c o mO O O O z X o o z (A X o H o z
All
valu
es a
re m
eans
±
SB
. NE
no
repi
neph
rine
: se
e te
xt f
or d
efin
itio
n of
A a
nd B
.*
Cha
nge
from
con
trol
sig
nifi
cant
, P
< 0
.01.
t C
hang
e si
gnif
ican
tly
diff
eren
t fr
om c
onsc
ious
dog
s w
itho
ut b
lock
ade
(1.0
Mg/
kg).
P <
0.0
1.$
Cha
nge
from
con
trol
sig
nifi
cant
. P
< 0
.05.
§ C
hang
e si
gnif
ican
tly
diff
eren
t fr
om c
onsc
ious
dog
s w
itho
ut b
lock
ade
(1.0
jig
/kg)
. P
< 0
.05.
00
by guest on May 20, 2018http://circres.ahajournals.org/Downloaded from

8 1 8 VATNER.HIGGINS, BRAUNWALD
I Ojug/ kg 0 l / jg /kg
ARTERIAL
PRESSURE
CORONARY
FLOW
CORONARY
RESISTANCE
EARLY(A) LATE(B) EARLY(Al LATE (Bl
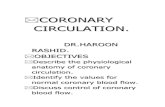
FIGURE 3
Average changes ± SE in response to norepinephrine, 1.0 \iglkg(left) and O.I ng/kg (right), in ten conscious dogs for mean andlate diastolic values of arterial pressure, coronary flow, andcoronary' resistance.
ways. (1) The rise in arterial blood pressure wassignificantly less at both points A and B. (2) Therise in coronary blood flow was less at point A butnot at point B. (3) The early coronary vasodilata-tion was similar, but the late coronary vasocon-striction did not occur and was actually reversed(Table 2). Thus, alpha-receptor blockade at-tenuated the pressor action of norepinephrine and
NE I.Ojug/kg
IV end DIASTOLICDIAMETER A%
LV VELOCITY,SO
A%
LV PRESSURE|S0
A%
• 1.50 -,
•0.75 -
LV A %
MEAN CORONARYRESISTANCE A%
-20 -
CONTROL EARLY (A) LATE (B)
FIGURE 4
Average changes ± SE in response to norepinephrine (NE), 1.0Hg/kg, in ten conscious dogs for left ventricular (LV) end-dia-stolic diameter, isolength (iso) velocity, and systolic pressure,(dPldt)IP, and mean coronary resistance. The early response(A) is associated with a decrease in coronary' resistance, and thelate response (B) is associated with an increase in coronaryresistance.
prevented the striking later increase in coronaryresistance.
After partial alpha-receptor blockade with phen-tolamine (0.2 mg/kg, iv), norepinephrine (1.0 fig/kg, iv) was administered to three dogs with heartrate maintained constant at 126 beats/min. Inthese dogs mean arterial blood pressure rose from107 mm Hg to 146 mm Hg at point A and remainedabove the control level at 114 mm Hg at the lateresponse. Mean coronary blood flow rose from 42ml/min to 108 ml/min (point A) and remainedabove the control level at 55 ml/min at the lateresponse. Mean coronary resistance fell in all threedogs from an average of 2.54 mm Hg/ml min"1 to1.34 mm Hg/ml min"1 at point A and remaineddepressed at an average of 2.09 mm Hg/ml min"1
at point B (Fig. 5). Thus, the late increase incoronary resistance was not observed after partialalpha-receptor blockade. During this blockade,norepinephrine stimulated alpha receptors suf-ficiently to elevate arterial blood pressure; how-ever, coronary alpha receptors were blocked suf-ficiently to reverse the late coronary vasocon-strictor response to a vasodilator response.
CONSCIOUS DOGS WITH HYPOXIA
After hypoxia had been induced in five dogs bybreathing 10% O2, norepinephrine (1.0 Mg/kg, iv)was administered as a bolus. Arterial Po2 fell from
MEANARTERIAL
PRESSURE(mmHg)
L.CIRCUMFLEXCORONARY
FLOW(ml/min)
MEANCORONARY
FLOW(ml/min)
MEANCORONARYRESISTANCE(mmHg/ml/min)
200n
160
1.00I-.
FIGURE 5
(—30 SEC—|
Typical response to intravenously administered norepinephrine(NE), 1.0 tig/kg, after partial alpha-receptor blockade withphentolamine, 0.2 mg/kg, iv. with the heart rate held constant.Responses for mean arterial blood pressure, phasic and meanleft circumflex coronary flow, and computed mean coronaryresistance are shown. Norepinephrine still caused pressure toincrease, but coronary vasconstriction was no longer observed incontrast to the normal response illustrated in Figure 1.
Circulation Research. Vol. XXXIV. June 1974
by guest on May 20, 2018
http://circres.ahajournals.org/D
ownloaded from

NOREPINEPHRINE-INDUCED CORONARY VASOCONSTRICTION 819
84 (SE) mm Hg to 40 mm Hg. With heart rate heldconstant by pacing at 132 ± 6 beats/min, norepi-nephrine increased mean arterial blood pressurefrom a control of 109 ± 5 mm Hg to 141 ± 6 mm Hgat point A and to 135 ± 6 mm Hg at point B;(dP/dt)/P rose from a control of 43 ± 3 sec"1 to75 ± 5 sec"1 at point A and remained elevated at59 =t 4 sec'1 at point B. Mean coronary blood flowrose from a control of 72 ± 5 ml/min to 142 ± 10ml/min at point A and remained elevated at 78 ± 6ml/min at point B. Mean coronary resistance fellfrom 1.55 ± 0.10 mm Hg/ml min"1 to 1.00 ± 0.08mm Hg/ml min"1 at point A and then increasedabove the control level to 1.74 ± 0.09 mm Hg/mlmin"1 at point B. Thus, the early period of coro-nary vasodilatation and the later period of coro-nary vasoconstriction were observed in hypoxicdogs as well as in normal, conscious, eupneic dogs.
NORMAL CONSCIOUS DOGS NOREPINEPHRINE INFUSION
Infusion of norepinephrine (0.5
creases in coronary blood flow. Accordingly, coro-nary' vascular resistance rose (Fig. 6). Mean arterialblood pressure increased from 99 ± 4 (SE) mm Hgto 154 ± 5 mm Hg, mean coronary blood flow rosefrom 44 ± 3 ml/min to 61 ± 5 ml/min, andcalculated mean coronary resistance increasedfrom 2.28 ± 0.12 mm Hg/ml min"1 to 2.59 ± 0.19mm Hg/ml min"1 (P < 0.05). Similar changesoccurred in late diastolic arterial pressure, coro-nary blood flow, and coronary vascular resistance.
Infusion of norepinephrine (0.2 j/g/kg min"1) tothree conscious dogs whose heart rates were heldconstant did not affect mean arterial blood pres-sure (98 mm Hg) but did reduce mean and latediastolic coronary blood flows from averages of 39ml/min and 42 ml/min to 34 ml/min and 35ml/min, respectively. Mean and late diastolic coro-nary resistances rose in all three dogs from averagesof 2.53 mm Hg/ml min" ' and 1.99 mm Hg/ml min" 'to 2.89 mm Hg/ml min"1 and 2.37 mm Hg/ml
min"1) to min"1, respectively. Thus, norepinephrine infusionfive dogs whose heart rates were held constantcaused a transient coronary vasodilatation (Fig. 6)followed by steady-state increases in arterial bloodpressures that were associated with smaller in-
constricted the coronary vessels; however, at lowerdoses of norepinephrine coronary constriction wasobserved without a concomitant elevation in arte-rial blood pressure (Fig. 7).
ARTERIALPRESSURE(mmHq)
MEAN PRESSURE(mmHg)
CORONARYFLOW VELOCITY(cm/sec)
MEAN FLOW(ml/min)
CALCULATEDMEAN CORONARYRESISTANCE - ™ml/mi
HEART RATE(beats/min)
200 ~
100 -0 _
200 ~100 -
0 _120 "
60 -0 -
100 "50 -
0 _3.0 "
2.0 -1.0 _
300 ~
150 -
0 _
; •: r i g
-Am
! Hi .
•rr! !''+:•:—
FIGURE 6
Typical response to infusion of norepinephrine (NE), 0.5 uglkg min~\ for phasic and mean arterialpressure, phasic and mean coronary flow velocity, calculated mean coronary resistance, and heartrate. With the heart rate held constant, norepinephnne produced a brief initial decrease in coronaryresistance and then a sustained increase during the steady state. The capability of the coronary'vessels to dilate markedly is shown by the response to an injection of 1 mg of nitroglycerin (NTG).
Cimilalion Ramrch. Vol. XXXIV. Junr 1974
by guest on May 20, 2018
http://circres.ahajournals.org/D
ownloaded from

820 VATNER. HIGGINS. BRAUNWALD
NO SLOCK
CONTROL (C) NE
ALPHA BLOCK
(C) NE
MEANARTERIAL
PRESSURE
L.CIRCUMFLEXCORONARY
FLOW(ml/min)
MEANCORONARY
FLOW(ml/min)
MEANCORONARYRESISTANCE(mmHg/ml/min)
200
1.00-k. n(H h»iic-l h »wc -I
HR-120/min.
FIGURE 7
HR-150/min.
Response to infusion of norepinephrine (NE) 0.2 uglkg min'',/or mean arterial blood pressure, phasic and mean coronaryflow, and computed mean coronary resistance. Left: With theheart rate (HR) held constant, norepinephrine produced areduction in coronary flow without a rise in arterial bloodpressure, i.e., coronary vasoconstriction took place. Right: Afteradministration of phentolamine, 1 mg/kg, iu, norepinephrineinfusion, 0.5 tiglkg min~', caused only coronary dilatation witha substantial increase in coronary' flow.
Infusion of norepinephrine (0.5 Mg/kg min"1)after administration of phentolamine (1 mg/kg, iv)caused only coronary dilatation. Although meanarterial blood pressure fell slightly from 99 mm Hgto 94 mm Hg, mean and late diastolic coronaryblood flows rose from 46 ml/min and 51 ml/min to61 ml/min and 66 ml/min, respectively, and meanand late diastolic coronary resistances fell from2.15 mm Hg/ml min"1 and 1.69 mm Hg/ml min"1
to 1.56 mm Hg/ml min"1 and 1.25 mm Hg/mlmin"1, respectively.
ANESTHETIZED. OPEN-CHEST DOGS
With heart rate held constant at 186 ± 8 beats/min, norepinephrine (1.0 fig/kg, iv) increased meanarterial blood pressure by 51 ± 9 (SE) mm Hg froma control value of 109 ± 10 mm Hg at point A; thepressure remained 39 ± 10 mm Hg above controllevels at point B (Table 2). Late diastolic arterialblood pressure and left ventricular systolic pressureincreased similarly. Arterial Po2 remained at thecontrol level, 82 ± 3 mm Hg. Peak dP/dt increasedby 7130 ± 670 mm Hg/sec at point A from a controlof 2080 ± 210 mm Hg/sec and remained elevated atpoint B. (dP/dt)/P increased by 39 ± 5 sec"' from acontrol of 21 ± 4 sec"1 at point A and remainedelevated at point B. Mean left circumflex coronaryblood flow increased by 74 ± 19 ml/min from acontrol of 51 ± 4 ml/min at point A and remained
elevated by 20 ± 4 ml/min above control at pointB. These increases in coronary blood flow wereslightly, although not significantly, greater thanthose observed in the conscious dog. Calculatedmean coronary resistance decreased by 0.84 ± 0.30mm Hg/ml min"1 from a control of 2.17 ± 0.58 mmHg/ml min"1 at point A. In contrast to the experi-ments in the normal, conscious dogs, calculatedmean coronary resistance did not rise at point Bbut returned to 2.10 ± 0.26 mm Hg/ml min"1, alevel very close to control (Table 2).
In two anesthetized dogs treated with pro-pranolol, norepinephrine caused only coronary vas-oconstriction; at point B coronary resistance roseby 0.79 mm Hg/ml min"1 and 0.61 mm Hg/mlmin"' from controls of 2.39 mm Hg/ml m i n 1 and2.24 mm Hg/ml min"1, respectively.
Thus, general anesthesia and the open-cheststate modified the normal response to norepineph-rine in that the later prominent elevation of coro-nary resistance was not observed.
DiscussionThe coronary vascular bed, like other vascular
beds, responds to both direct alpha-receptor (con-strictor) and direct beta-receptor (dilator) stimula-tion (1-9). It is generally agreed, however, thatthese direct effects are minor in comparison withthe predominant metabolic effects induced by thestimulation of myocardial oxygen needs that re-sults from norepinephrine's concomitant powerfulpressor and inotropic actions (1-8). Accordingly,when norepinephrine is administered to the beat-ing heart, the major effect is thought to be thecoronary vasodilatation (1-8) which follows a tran-sient vasoconstriction. Alpha-adrenergic vasocon-striction has been observed only in the nonbeatingheart (1) or only after the beta-adrenergic effecthas been prevented in the beating heart (2-8).However, two recent studies in man have found nochange in coronary resistance with the infusion ofnorepinephrine (25, 26); this finding suggests thatnorepinephrine's alpha-adrenergic vasoconstrict-ing action might offset its secondary metabolicvasodilating effects.
In the present study conducted in healthy, con-scious dogs, the results were substantially differentand actually opposite in direction from those notedin earlier investigations conducted in experimentalanimals (1-8). When norepinephrine was adminis-tered intravenously as a bolus, two effects wereobserved. First, a transient period of coronaryvasodilatation occurred. This vasodilatation was
Circulation Research, Vol. XXXIV. June 1974
by guest on May 20, 2018
http://circres.ahajournals.org/D
ownloaded from

NOREPINEPHRINE INDUCED CORONARY VASOCONSTRICTION 821
associated with peak increases in left ventricularsystolic pressure and contractility and probablyresulted mainly from increases in myocardial oxy-gen consumption and to a lesser extent fromactivation of coronary vascular beta receptors.Then a period of sustained coronary vasoconstric-tion ensued. This coronary vasoconstrictor effectcould not have resulted from a reduction in themyocardial oxygen requirements below the controllevels, since heart rate was maintained constant.The major hemodynamic determinants of myocar-dial O2 consumption (i.e., left ventricular pres-sures, end-diastolic diameter, and myocardial con-tractility) were elevated, and the coronary arterio-venous Po2 difference was widened above controllevels. When norepinephrine was administered asan infusion, coronary, vasoconstriction occurredduring the steady state; this finding further sup-ports the importance of this action. Since a similarcoronary vasoconstrictor component was observedwhether the Doppler or the electromagnetic flow-meter was used and whether mean or late diastolicresistance was calculated, our results could not beattributed to possible errors due to reverse flowduring systole consequent to increased myocardialcompression of the coronary vessels.
Autoregulation has been observed in the coro-nary vascular bed (27, 28); the tendency for coro-nary blood flow to return toward the control leveland for coronary vasoconstriction to occur duringthe late response to norepinephrine could, in part,be explained on the basis of autoregulation. How-ever, this explanation is incomplete for the follow-ing reasons. When norepinephrine was adminis-tered as a bolus or an infusion in the presence ofphentolamine, an alpha-receptor blocking agent,the period of coronary vasoconstriction was notobserved and only a sustained vasodilatation re-sulted, presumably owing to betaradrenergic in-creases in myocardial contractility and stimulationof beta2 coronary vascular receptors (4-7). In someof the experiments in which the smaller bolus doseof norepinephrine (0.1 Mg/kg) was administered,coronary blood flow actually decreased below thecontrol level during the later period of coronaryvasoconstriction. Similarly, when the smaller doseof norepinephrine was administered as an infusion,coronary blood flow fell while arterial blood pres-sure remained at control levels* A reduction incoronary blood flow in association with an eleva-tion in arterial blood pressure certainly cannot beexplained on the basis of autoregulation. Further-more, in the anesthetized, open-chest dogs and inCirculation Research. Vol. XXXIV. June 1974
the conscious dogs with partial alpha-receptorblockade (Fig. 5), the late increase in coronaryresistance did not occur when arterial blood pres-sure rose. If autoregulation had been entirelyresponsible for the increase in coronary vascularresistance in the conscious dogs without blockade,this increase should also have occurred in theanesthetized dogs and in the conscious dogs withpartial alpha-receptor blockade in which the coro-nary vessels dilated despite arterial blood pressureelevation. Finally, after beta-receptor blockade,the increases in coronary resistance produced bynorepinephrine were greater than those producedwithout such treatment. These findings furthersupport the concept that active alpha-adrenergicvasoconstriction was primarily responsible for theincrease in resistance, but they do not completelyrule out the contribution of an autoregulatoryresponse.
Both the previous studies in which only dilata-tion occurred in response to norepinephrine (1-8)and those in which alpha-receptor activity in thecoronary vascular bed appeared to be trivial (4, 5)were conducted primarily in anesthetized, open-chest preparations (1, 2, 4, 8); the presence ofgeneral anesthesia and the open chest might ex-plain the differing results. When norepinephrinewas administered to five anesthetized, open-chestdogs in the present study, the later period ofcoronary vasoconstriction was not observed, i.e.,our results resembled those previously reported. Anumber of explanations might be invoked to ex-plain this difference in responses. (1) The coronaryvascular bed was relatively constricted in theanesthetized state even prior to the administra-tion of norepinephrine. (2) The anesthetized dogswere hypoxic and constriction might not be ob-served in hypoxia. (3) The anesthetic agent maskedthe constrictor action of norepinephrine on thecoronary vessels and perhaps acted directly as avascular depressant (29). (4) The relative increasesin myocardial oxygen requirements induced bynorepinephrine were much greater in the anes-thetized dogs than in the conscious dogs. Sincecontrol values for coronary resistance in both theconscious and the anesthetized dogs were notsignificantly different (Table 2), the first possi-bility appears to be excluded. Second, alterationsin arterial Po2 could not explain the differences be-tween the results in the conscious and anes-thetized dogs. In the anesthetized dogs ventila-tion was well maintained as evidenced by ar-terial Po2 values. Moreover, the conscious
by guest on May 20, 2018
http://circres.ahajournals.org/D
ownloaded from

822 VATNER. HIGGINS. BRAUNWALD
dogs were studied in the hypoxic state. Evenafter the coronary vascular bed was dilated byhypoxia, norepinephrine still produced the laterperiod of coronary vasoconstriction. Thus, thedifference between the results in the conscious andthe anesthetized dogs was probably due to thediffering experimental preparations. The presenceof a general anesthetic agent (1) affects highercentral nervous system control of the cardiovascu-lar system to an unknown extent, (2) alters reflexcontrol of the circulation (30), (3) substantiallydepresses the myocardial contractile state (11),and (4) exerts a direct dilating effect on theresistance vessels (29). Moreover, inotropic agentssuch as cardiac glycosides (11) and norepinephrineexert a relatively greater inotropic effect on themyocardium depressed by general anesthesia and,accordingly, can be expected to cause a relativelygreater augmentation in myocardial oxygen con-sumption and secondarily, coronary vasodilata-tion. These considerations could explain the find-ing that the effects of norepinephrine in consciousand anesthetized dogs differ strikingly. The differ-ence between our results and those of Pitt et al. (3),who reported that coronary dilatation occurredwith the administration of norepinephrine, cannotbe resolved on the same basis, since their study wasconducted in conscious dogs. However, in thatinvestigation the response to norepinephrine wasreported only at one instant (20-30 seconds afterintravenous administration of norepinephrine), apoint which corresponded to the early peak effectsof norepinephrine in the present study (point A)where coronary vasodilatation was also observed.
Thus, in normal, healthy, conscious dogs, norepi-nephrine causes a significant alpha-adrenergic con-strictor response despite increases in left ventricu-lar pressures, end-diastolic diameter, and myocar-dial contractility. Failure to demonstrate this ac-tion in open-chest, anesthetized dogs in both thisand previous studies (1, 2, 4-8) underscores theimportance of elucidating cardiovascular pharma-cological responses in normal, healthy, consciousanimals in which the anesthetic agent and recentsurgery have not produced myocardial depression(11), altered vasoactivity of the peripheral vessels,or both.
AcknowledgmentWe acknowledge the technical assistance of T. Manders. D.
P. McKown, and F. Werner and the help of R. Bulva in thepreparation of the manuscript.
References1. BERNE, R.M.: Effect of epinephrine and norepinephrine
on coronary circulation. Circ Res 6:644-655, 1958.2. HARDIN, R.A., SCOTT, J.B., AND HADDY, F.J.: Effect of
epinephrine and norepinephrine on coronary vascular re-sistance in dogs. Am J Physiol 201:276-280, 1961.
3. PITT, B., ELLIOTT, E.C., AND GREGG, D.E.: Adrenergic re-
ceptor activity in the coronary arteries of the unanesthe-tized dog. Circ Res 21:75-84, 1967.
4. MARK, A.L., ABBOUD, F.M., SCHMID, P.G., HEISTAD,
D.D., AND MAYER, H.E.: Differences in direct effects ofadrenergic stimuli on coronary, cutaneous, and muscularvessels. J Clin Invest 51:279-287, 1972.
5. MCRAVEN, D.R., MARK, A.L., ABBOUD, F.M., AND MAYER,
H.E.: Responses of coronary vessels to adrenergic stim-uli. J Clin Invest 50:773-778, 1971.
6. MALINDZAK, G.S., JR., VAN DYKE, A.H., GREEN, H.D.,
AND MEREDITH, J.H.: Alpha and beta adrenergic recep-tors in the coronary vascular bed. Arch Int PharmacodynTher 197:112-122, 1972.
7. ZUBERBUHLER, R.C., AND BOHR, D.F.: Responses of
coronary' smooth muscle to catecholamines. Circ Res 16:431-440, 1965.
8. GAAL, P.G., KATTUS, A.A., KOLIN, A., AND ROSS, G.: Ef-
fects of adrenaline and noradrenaline on coronary bloodflow before and after beta-adrenergic blockade. Br JPharmacol 26:713-722, 1966.
9. KLOCKE, F.J., KAISER, G.A., Ross, J., JR., AND BRAUNWALD,
E.: Intrinsic adrenergic vasodilator mechanism in the cor-onary vascular bed of the dog. Circ Res 16:376-382, 1965.
10. VATNER, S.F., HIGGINS, C.B., FRANKLIN, D., AND BRAUN-
WALD, E.: Effects of a digitalis glycoside on coronary andsystemic dynamics in conscious dogs. Circ Res 28:470-479, 1971.
11. VATNER, S.F., HIGGINS, C.B., PATRICK, T., FRANKLIN, D.,
AND BRAUNWALD, E.: Effects of cardiac depression and ofanesthesia on the myocardial action of a cardiac glycoside.J Clin Invest 50:2585-2595, 1971.
12. HIGGINS, C.B., VATNER, S.F., AND BRAUNWALD, E.: Re-
gional hemodynamic effects of a digitalis glycoside in theconscious dog with and without experimental heart fail-ure. Circ Res 30:406-417, 1972.
13. VATNER, S.F., HIGGINS, C.B., MILLARD, R.W., AND FRANK-
LIN, D.: Direct and reflex effects of nitroglycerin on coro-nary and left ventricular dynamics in conscious dogs. JClin Invest 51:2872-2882, 1972.
14. VATNER, S.F., MILLARD, R.W., AND HIGGINS, C.B.: Coro-
nary and myocardial effects of dopamine in the consciousdog: Parasympatholytic augmentation of pressor and ino-tropic actions. J Pharmacol Exp Ther 187:280-295, 1973.
15. FRANKLIN, D.E., WATSON, N.W., PIERSON, K.E.. AND VAN
CITTERS, R.L.: Technique for radio telemetry of blood-flow velocity from unrestrained animals. Am J Med Elec-tron 5:24-28. 1966.
16. VATNER, S.F., FRANKLIN, D., AND VAN CITTERS, R.L.: Si-
multaneous comparison and calibration of the Dopplerand electromagnetic flowmeters. J Appl Physiol 29:907-910, 1970.
17. PATRICK, T.A., VATNER, S.F., KEMPER, W.S.. AND FRANK-
LIN, D.: Telemetry of left ventricular diameter and pres-sure measurements in unrestrained animals. J Appl Phys-iol, in press.
18. RUSHMER, R.F., FRANKLIN, D., AND ELLIS, R.M.: Left ven-
Cimilation Research. Vol. XXXIV. June 1974
by guest on May 20, 2018
http://circres.ahajournals.org/D
ownloaded from

NOREPINEPHRINE-INDUCED CORONARY VASOCONSTRICTION 823
tricular dimensions recorded by sonocardiometry. CircRes 4:684-688, 1956.
19. STEGALL, H.F., KARDON, M.B., STONE, H.L., AND BISHOP,V.S.: Portable simple sonomicrometer. J Appl Physiol23:289-293, 1967.
20. GLICK, G., SONNENBLICK, E.H., AND BRAUNWALD, E.: Myo-
cardial force-velocity relations studies in intact unanes-thetized man. J Clin Invest 44:978-988, 1965.
21. VATNER, S.F., FRANKLIN, D., HIGGINS, C.B.. PATRICK, T.,
AND BRAUNWALD, E.: Left ventricular response to severeexertion in untethered dogs. J Clin Invest 51:3052-3060.1972.
22. VATNER, S.F., HIGGINS, C.B., FRANKLIN, D., AND BRAUN-
WALD, E.: Extent of carotid sinus control of the myocar-dial contractile state in conscious dogs. J Clin Invest 51:995-1008, 1972.
23. MASON, D., BRAUNWALD, E., COVELI, J.W., SONNENBLICK,
E.H., AND Ross, J., JR.: Assessment of cardiac contrac-tility: Relation between the rate of pressure rise and ven-tricular pressure during isovolumic systole. Circulation44:47-58. 1971.
24. SNEDECOR, G.W., AND COCHRAN, W.G.: Statistical Meth-ods. Ames, Iowa, Iowa State University Press, 1969. pp91-98.
25. GREENFIELD, J.C., JR., REMBERT, J.C.. YOUNG, W.G., JR..OLDHAM, H.N., JR., ALEXANDER, J.A.. AND SABISTON.D.C.. JR.: Studies of blood flow in aorta-to-coronary ve-nous bypass grafts in man. J Clin Invest 51:2724-2735.1972.
26. MUELLER, H., AVERS, S.M., GREGORY, J.J.. GIANELLI, S..JR., AND GRACE, W.J.: Hemodynamics. coronary bloodflow, and myocardial metabolism in coronary shock: Re-sponse to /-norepinephrine and isoproterenol. J ClinInvest 49:1885-1902. 1970.
27. CROSS, C.E.: Influence of coronary' arterial pressure on cor-onary vasomotor tonus. Circ Res 15(suppl. 0:1-87-92,1964.
28. MOSHER, P., Ross, J., JR., MCFATE, P.A., AND SHAW, R.F.:
Control of coronary blood flow by an autoregulatory mech-anism. Circ Res 14:250-259. 1964.
29. HERSHEY, S.G., ZWEIFACH, B.W.. AND ROVENSTINE, E.A.:
Effects of depth of anesthesia on behavior of peripheralvascular bed. Anesthesiology 14:245-254. 1953.
30. VATNER, S.F., FRANKLIN, D., AND BRAUNWALD, E.: Effects
of anesthesia and sleep on circulatory response to carotidsinus nerve stimulation. Am J Physiol 220:1249-1255,1971.
Circulation Research. Vol. XXXIV. June 1374
by guest on May 20, 2018
http://circres.ahajournals.org/D
ownloaded from

STEPHEN F. VATNER, CHARLES B. HIGGINS and EUGENE BRAUNWALDConscious Dog
Effects of Norepinephrine on Coronary Circulation and Left Ventricular Dynamics in the
Print ISSN: 0009-7330. Online ISSN: 1524-4571 Copyright © 1974 American Heart Association, Inc. All rights reserved.is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation Research
doi: 10.1161/01.RES.34.6.8121974;34:812-823Circ Res.
http://circres.ahajournals.org/content/34/6/812World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circres.ahajournals.org//subscriptions/
is online at: Circulation Research Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further informationEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculation Research Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on May 20, 2018
http://circres.ahajournals.org/D
ownloaded from