Effectiveness of HPV 16 viral load and the E2/E6 ratio for the prediction of cervical cancer risk...
9
Journal of Medical Virology 85:646–654 (2013) Effectiveness of HPV 16 Viral Load and the E2/E6 Ratio for the Prediction of Cervical Cancer Risk Among Chinese Women Lihong Chang, 1 Xiaoxiao He, 1 Guifang Yu, 2 and Yuping Wu 1 * 1 State Key Laboratory of Biocontrol, School of Life Sciences, Sun Yat-Sen University, Guangzhou, China 2 Department of Gynecology, People Hospital of Zhuhai, Guangdong Province, China The effectiveness of the E2/E6 ratio, the state of viral genome integration and the viral load of human papillomavirus 16 (HPV 16) in predicting the risk of cervical cancer among Chinese wom- en was investigated. Quantitative PCRs for the E2/E6 ratio and the viral load were performed on 85 cervical cancer samples and 55 HPV 16 positive healthy controls. The integrated form of the viral genome was found in 10.9% control samples and in 26.4% cervical cancer samples (P ¼ 0.02). The majority of the cervical cancer (63.2%) and control samples (60%) were mixed forms. The E2/E6 ratio was associated with a high risk of cervical cancer (OR ¼ 7.29, P ¼ 9.55E6). The integrated form (OR ¼ 6.54, P ¼ 0.005) and mixed form (OR ¼ 2.93, P ¼ 0.042) increased the risk of cervical cancer. The mean viral load in cervical cancer samples (37,371 227,135) was higher than that in the controls (4,619 27,079; P ¼ 0.011). Additional- ly, the viral load increased along with the cervical cancer progression from the Interna- tional Federation of Gynecology and Obstetrics (FIGO) stage I (12,337 25,604) to stage II (67,453 319,821). Compared with the state of viral genome integration (area under the receiv- er operating characteristic curve (AUC) ¼ 0.743) or the viral load (AUC ¼ 0.694), the E2/E6 ratio improved the effectiveness of the risk predic- tion of cervical cancer (AUC ¼ 0.777), with the sensitivity (specificity) 81.2% (71.7%). The state of viral genome integration and the viral load of HPV 16 were important factors for the risk prediction of cervical cancer among Chinese women, and the E2/E6 ratio had a better cervi- cal cancer risk prediction with age adjustment. J. Med. Virol. 85:646–654, 2013. ß 2013 Wiley Periodicals, Inc. KEY WORDS: human papillomavirus; HPV 16; viral load; E2/E6 ratio; risk prediction INTRODUCTION Cervical cancer is the third most commonly diag- nosed cancer [Arbyn et al., 2011], which was the fourth leading cause of cancer death among females worldwide (incidence 529,800 and 275,100 deaths) and resulted in the death of 40,000 women in China in 2008 [Arbyn et al., 2010, 2011]. It is a preventable cancer. Effective screening strategies that identify the precursor lesions would reduce the incidence and mor- tality of this disease. Common economical screening methods include vi- sual inspection using acetic acid solution wash and Pap smear in poor areas [Arbyn et al., 2008]. Howev- er, the low sensitivity and poor reproducibility of these two methods limit their effectiveness [Nanda et al., 2000; Stoler and Schiffman, 2001]. Since human papillomavirus (HPV) is the primary cause of cervical cancer [Walboomers et al., 1999], screening for this virus is a sensitive method when compared with liq- uid based cytology and could extend the screening in- terval to 6 years [Kitchener et al., 2011]. One caveat is that despite a high prevalence of HPV infection, most subjects that tested positive with HPV were asymptomatic and only a small proportion progressed to persistent infection or cervical cancer [Mao et al., 2003; Stanley, 2010; Insinga et al., 2011]. Thus, HPV DNA detection in the absence of additional informa- tion would lead to over-screening, added cost, and un- desirable pressure among HPV positive population. Additional supporting information may be found in the online version of this article. Grant sponsor: National Natural Science Foundation of China; Grant number: 30772333; Grant sponsor: Science & Technology Project of Zhuhai, Guangdong, China; Grant num- bers: PC20071077. 200901017. *Correspondence to: Yuping Wu, PhD, School of Life Sciences, Sun Yat-Sen University, Guangzhou 510275, China. E-mail: exwyp@163.com Accepted 6 November 2012 DOI 10.1002/jmv.23490 Published online 30 January 2013 in Wiley Online Library (wileyonlinelibrary.com). ß 2013 WILEY PERIODICALS, INC.
Transcript of Effectiveness of HPV 16 viral load and the E2/E6 ratio for the prediction of cervical cancer risk...

Journal of Medical Virology 85:646–654 (2013)
Effectiveness of HPV 16 Viral Load and theE2/E6 Ratio for the Prediction of CervicalCancer Risk Among Chinese Women
Lihong Chang,1 Xiaoxiao He,1 Guifang Yu,2 and Yuping Wu1*1State Key Laboratory of Biocontrol, School of Life Sciences, Sun Yat-Sen University, Guangzhou, China2Department of Gynecology, People Hospital of Zhuhai, Guangdong Province, China
The effectiveness of the E2/E6 ratio, the state ofviral genome integration and the viral load ofhuman papillomavirus 16 (HPV 16) in predictingthe risk of cervical cancer among Chinese wom-en was investigated. Quantitative PCRs for theE2/E6 ratio and the viral load were performedon 85 cervical cancer samples and 55 HPV 16positive healthy controls. The integrated formof the viral genome was found in 10.9% controlsamples and in 26.4% cervical cancer samples(P ¼ 0.02). The majority of the cervical cancer(63.2%) and control samples (60%) were mixedforms. The E2/E6 ratio was associated with ahigh risk of cervical cancer (OR ¼ 7.29,P ¼ 9.55E�6). The integrated form (OR ¼ 6.54,P ¼ 0.005) and mixed form (OR ¼ 2.93,P ¼ 0.042) increased the risk of cervical cancer.The mean viral load in cervical cancer samples(37,371 � 227,135) was higher than that in thecontrols (4,619 � 27,079; P ¼ 0.011). Additional-ly, the viral load increased along with thecervical cancer progression from the Interna-tional Federation of Gynecology and Obstetrics(FIGO) stage I (12,337 � 25,604) to stage II(67,453 � 319,821). Compared with the state ofviral genome integration (area under the receiv-er operating characteristic curve (AUC) ¼ 0.743)or the viral load (AUC ¼ 0.694), the E2/E6 ratioimproved the effectiveness of the risk predic-tion of cervical cancer (AUC ¼ 0.777), with thesensitivity (specificity) 81.2% (71.7%). The stateof viral genome integration and the viral loadof HPV 16 were important factors for the riskprediction of cervical cancer among Chinesewomen, and the E2/E6 ratio had a better cervi-cal cancer risk prediction with age adjustment.J. Med. Virol. 85:646–654, 2013.� 2013 Wiley Periodicals, Inc.
KEY WORDS: humanpapillomavirus;HPV16;viral load; E2/E6 ratio; riskprediction
INTRODUCTION
Cervical cancer is the third most commonly diag-nosed cancer [Arbyn et al., 2011], which was thefourth leading cause of cancer death among femalesworldwide (incidence 529,800 and 275,100 deaths)and resulted in the death of 40,000 women in Chinain 2008 [Arbyn et al., 2010, 2011]. It is a preventablecancer. Effective screening strategies that identify theprecursor lesions would reduce the incidence and mor-tality of this disease.
Common economical screening methods include vi-sual inspection using acetic acid solution wash andPap smear in poor areas [Arbyn et al., 2008]. Howev-er, the low sensitivity and poor reproducibility ofthese two methods limit their effectiveness [Nandaet al., 2000; Stoler and Schiffman, 2001]. Since humanpapillomavirus (HPV) is the primary cause of cervicalcancer [Walboomers et al., 1999], screening for thisvirus is a sensitive method when compared with liq-uid based cytology and could extend the screening in-terval to 6 years [Kitchener et al., 2011]. One caveatis that despite a high prevalence of HPV infection,most subjects that tested positive with HPV wereasymptomatic and only a small proportion progressedto persistent infection or cervical cancer [Mao et al.,2003; Stanley, 2010; Insinga et al., 2011]. Thus, HPVDNA detection in the absence of additional informa-tion would lead to over-screening, added cost, and un-desirable pressure among HPV positive population.
Additional supporting information may be found in the onlineversion of this article.
Grant sponsor: National Natural Science Foundation ofChina; Grant number: 30772333; Grant sponsor: Science &Technology Project of Zhuhai, Guangdong, China; Grant num-bers: PC20071077. 200901017.
*Correspondence to: Yuping Wu, PhD, School of Life Sciences,Sun Yat-Sen University, Guangzhou 510275, China.E-mail: [email protected]
Accepted 6 November 2012
DOI 10.1002/jmv.23490Published online 30 January 2013 in Wiley Online Library(wileyonlinelibrary.com).
� 2013 WILEY PERIODICALS, INC.

Therefore, additional predictive markers are neededto make up these drawbacks.
Currently, potential epigenetic changes are beingevaluated as cervical cancer biomarkers. Methylationof the E2 binding site and CpG methylation of theHPV 16 long control region (LCR) and E6 gene werepreviously shown to be related to cervical cancer orprecursor lesions [Badal et al., 2003; Bhattacharjeeand Sengupta, 2006]. The methylation frequencies ofhas-miR-124-1 and/or has-miR-12-2, SOX1, HOXA11,and CADM1 were found to show different betweencervical lesions and the controls [Apostolidou et al.,2009; Wilting et al., 2010]. In addition, the overex-pressions of Kallikrein 7, p16INK4a, and ProEx Chave been reported to be associated with metastasis,cell proliferation, and the detections of cervical intra-epithelial neoplasia 2þ/3þ [Fay et al., 2009; Terminiet al., 2010; Guo et al., 2011]. However, gene methyla-tion and protein expression in cervical cancer are of-ten inconsistent across different studies and clinicalscenarios. Furthermore, these markers are not morespecific for HPV-related carcinogenesis [Wentzensenet al., 2009], but would assist in the detection of cervi-cal cancer with HPV.
Recently, measurement of HPV integration hasbeen proposed to improve the clinical assessment ofcervical intraepithelial neoplasia 2/3 in conjunctionwith HPV genotyping. Viral genome integration,which leads to the upregulation of E6 and E7 onco-gene expression in cervical cancer and disrupts ex-pression of the HPV early gene E2, is a major step incervical carcinogenesis [Jeon et al., 1995; Collinset al., 2009]. Besides, an increased viral load wasfound to be associated with an increase in cervicallesions and a decrease time to the development of per-sistent infection [Mutirangura, 2001; Anderson et al.,2006]. However, the effectiveness of these markers onpredicting the risk of cervical cancer among Chinesewomen was unknown.
As the most common high-risk HPV type, HPV 16 isresponsible for approximately 50% of invasive cancercases and accounts for 79.6% of cervical cancer casesamong Chinese women [Wu et al., 2006, 2007; Smithet al., 2007]. It was suggested that the state of viralgenome integration and the viral load of HPV 16 con-tribute to improve the effectiveness on the prognosisof cervical lesions among Chinese women.
To assess predictive effictiveness of certain factors,the sensitivity, specificity and accuracy of a predic-tion, diagnosis or discrimination should be considered.Receiver operating characteristic (ROC) curve analy-sis is an important measure for these parameters, andhelps to identify the optimal cutoff value from therange of possible values using quantitative tests [Tri-pepi et al., 2009]. ROC curve is a graphical techniquethat is carried out by plotting the sensitivity of a teston the y axis against 1-specificity on the x axis. Thearea under the ROC curve provides a measure of theoverall performance of a diagnostic test [Akobeng,2007]. This approach has been widely used in
predictive value assessment of many tumor markers,including assessment of serum melanoma inhibitoryactivity levels as the predictor for melanoma metasta-sis [Klingenstein et al., 2011], and urine levels of thenoncoding RNA transcript PCA3 for the prediction ofprostate cancer [Laxman et al., 2008].
The aim of this study was to determine the effec-tiveness of the E2/E6 ratio, the state of viral genomeintegration and the viral load of HPV 16 in predictingthe risk of cervical cancer among Chinese womenusing a ROC analysis. The strategies used for themeasurement of HPV 16 viral load and the state ofviral genome integration were based on the relativequantification of the E6 gene and the E2/E6 ratio, re-spectively, as E2 and E6 are present at similar levelsin episomes, whereas integration induces a loss of E2.
MATERIALS AND METHODS
Clinical Samples
A total of 140 subjects from Gansu and Guangdongprovince were used in this study. First, cervical tissuesamples (n ¼ 39) and cervical cell samples (n ¼ 46)from pathologically proven cervical cancer patientswere collected. All samples were confirmed to be HPV16 positive using general primer PCR and sequence-based typing genotype (GP PCR-SBT method) [Wuet al., 2006]. Additionally, 26 women from similar eth-nic origin served as healthy volunteers, with cervicalcell samples collected, all the cell samples were cy-tological normal. Finally, 29 formalin-fixed tissuessamples from genital warts patients with single HPV16 infection were also used in this study.
The study protocol was reviewed and approved bythe local review committee, and all subjects under-went a short standardized interview and signed awritten informed consent.
DNA Extraction
The total genomes were extracted from all tissuesamples, including formalin-fixed samples, using astandard phenol:chloroform extraction and ethanolprecipitation procedure [Sambrook and Russell, 2001].Genome DNAs from cervical cells were digested incell lysis solution, and then followed the extractionprocedure above.
Gene Cloning
The amplifications of E2, E6 and the normalizedsamples b-globin were performed in the reaction mix-ture containing DNA 100 ng, with the following proto-col: 958C pre-denaturation for 5 min, with 45 cycles ofdenaturation at 958C for 20 sec, annealing at 608C for15 sec, extension at 728C for 30 sec, and finial 728Cextension for 4 min. All primers were listed inTable I. The PCR products of HPV 16 E2 and E6, aswell as the human b-globin were separated using elec-trophoresis on a 3% agarose gel, and the products ofthe three target genes were all approximately 80 bp.
HPV 16 Status in Predicting Cervical Cancer 647
J. Med. Virol. DOI 10.1002/jmv

The fragments were then purified and inserted intoTakara PMD19-T vectors (Dalian, China). Theresponding ligation products were used to transformDH5a E. coli. After incubation at 48C for 30 min anda heat-shock at 428C for 1 min, LB liquid mediumwas added and cells were maintained at 378C for60 min with shaking. The cells were then plated onLB agarose medium containing 100 mg/ml Amp. Allthree plasmids were purified from the correspondingcells using a Takara MiniBEST Plasmid PurificationKit (Dalian, China). The products of the colony PCRsof E2, E6, and b-globin were conducted separatelyand the PCR products were analyzed using gelelectrophoresis.
Optimization of Real-Time PCR
Real-time PCRs for E2 and E6 amplifications wereperformed on a Roche LightCycler 480 using Taq-man probes according to the original report [Peitsaroet al., 2002; Depuydt et al., 2007]. Each sample wasnormalized by b-globin (as shown in Table I). Theamplifications of E2, E6, and b-globin were per-formed separately in a 10 ml volume containing 1�Premix Ex Taq (Takara, Dalian, China), 0.3 mM ofeach primer and probe, and 30–50 ng genomic DNAwith the following protocol for 40 cycles: 3 secdenaturation at 958C, annealing and extension at608C for 30 min, with the initial denaturation at958C for 30 sec.
External standard curves for E2, E6, and b-globinwere constructed to calculate the amplification effi-ciencies of these genes by averaging three replicatestandard curves to minimize the effect of interrunvariation. It was indicated that the amplification effi-ciencies of E2, E6, and b-globin were nearly 100%.The final calibrated E2/E6 and E6/b-globin valueswere calculated by averaging the E2/E6 or E6/b-globinvalues of replicate calibrators in different runs to min-imize the effect of intrarun variation. The curve ofeach gene amplification for each sample was obtainedby averaging the replicates in a run and discardingthe run that deviated from the remaining two curvesif there was a significant deviation among the threereplicates. The equation for the calculation of the
relative quantity for each sample was as follow:
RQ ðSÞ ¼ average ðRQCÞ� ðECpT ðCÞ�CpT ðSÞ
T � ECpR ðCÞ�CpR ðSÞR Þ
In the equation, RQ represents relative quantity; Crepresents calibrator, S represents tested sample; ET
and ER represent the amplification efficiency of targetand reference gene in a run; and CpT and CpR repre-sent the Cp value of the target and reference gene ina run. For the E2/E6 ratio calculation, the target andreference genes in the equation above were E2 andE6, respectively. For the viral load relative quantifica-tion, the target and reference genes in the equationwere E6 and b-globin, respectively.
HPV 16 E2/E6 Ratio and HPV 16 Viral Load Test
The standard curves for HPV 16 E6 and E2 wereconstructed based on a 10-fold dilution series to calcu-late the amplification efficiencies of HPV 16 E6 andE2. Each dilution was completed with the same con-centration of healthy female human DNA to mimicthe complex nucleic acid environment. The standardcurve of b-globin was constructed based on a fivefolddilution series of normal female genomic DNA to cal-culate its amplification efficiency. The same concen-trations of HPV 16 E2 and E6 plasmids were added toeach reaction. For each test, three no-template controlreaction mixtures and three positive control (E2, E6,and b-globin plasmids) reaction mixtures were addedfor each gene amplification. All samples underwentthe gene amplifications, which were performed tri-plexed in duplicate. The advanced relative quantifica-tion analysis was performed for each sample usingthe abs Quant/fit point method on the Roche LightCy-cler 480 software version 1.5. The E2/E6 and E6/b-globin comparative quantifications were calculatedusing the external standard curve.
Definition of the Threshold for Episomal andIntegrated Form
Viral genome integration was defined by the absenceof E2 or an E2/E6 ratio that was less than 0.001. An
TABLE I. HPV 16 Primers and Probes for the E2/E6 Ratio and the Viral Load Calculation
Primers and probes Sequence 50–30 Refs.
E2 F AACGAAGTATCCTCTCCTGAAATTATTAG Peitsaro et al. [2002]E2 R CCAAGGCGACGGCTTTG Peitsaro et al. [2002]E2 probe (FAM)-CACCCCGCCGCGACCCATA-(BHQ) Peitsaro et al. [2002]E6 F GAGAACTGCAATGTTTCAGGACC Peitsaro et al. [2002]E6 R TGTATAGTTGTTTGCAGCTCTGTGC Peitsaro et al. [2002]E6 probe (JOE)-CAGGAGCGACCCAGAAAGTTACCACAGTT-(BHQ) Peitsaro et al. [2002]b-Globin F TGCATTTGACTCCTGAGGAGAA Depuydt et al. [2007]b-Globin R GGGCCTCACCACCAACTTC Depuydt et al. [2007]b-Globin probe (FAM)-CTGCCGTTACTGCCCT-(BHQ) Depuydt et al. [2007]
648 Chang et al.
J. Med. Virol. DOI 10.1002/jmv

E2/E6 ratio less than 1 (0.001–0.900) was defined as amixture of episomal and integrated forms. That a ratiowas larger than 0.900 indicated that the episomal formwas predominant. The E6/b-globin ratio representedthe relative HPV 16 viral load.
Data Analysis
The means for the descriptive statistical, the stan-dard error of means for HPV 16 viral load and thepercentage of HPV 16 viral integration for each groupwere calculated based on clinical diagnosis. TheMann–Whitney test was used to compare pair-wisethe clinical diagnosis groups and the different statesof viral genome integration. The mean viral loadswere compared between the two different clinical di-agnosis groups using a t-test after logarithmic trans-formation to close normal distribution. ROC analysiswas used to test the diagnosis potential of the HPV 16E2/E6 ratio, the state of viral genome integration, andthe viral load. Non-parametric estimate of standarderror means of the AUC (area under the ROC curve)were performed to evaluate the prediction effective-ness. The maximum Youden index was used to obtainthe best cutoff value.
A binary logistic regression model was conducted tofit the three markers to predict the risk of cervicalcancer, adjusted with age. A risk probability from thelogistic regression equation was obtained for each sub-ject. A non-parametric estimate of standard errormean of the AUC of each ROC curve was performedto evaluate the goodness-of-fit of the equation, and theprediction efficiency of the combination markers. Themaximum Youden index was used to obtain the bestcutoff value. All of the statistical analyses above wereperformed using the SPSS 16.0 for Windows. A two-tailed P-value less than 0.05 was considered statisti-cally significant.
RESULTS
In this study, 85 HPV 16 positive cervical cancerand 55 HPV 16 positive control subjects were validat-ed. Among the cervical cancer subjects, 32 were theInternational Federation of Gynecology and Obstet-rics (FIGO) stage I and 43 were FIGO stage II, whilean additional 10 had an unknown FIGO stage. Thebasic characteristics of the subjects were shown inTable II.
Association Between HPV 16 Integration andCervical Cancer
A lower percentage (10.3%) of the episomal form ofthe viral genome was found in the samples from thewomen with cervical cancer when compared with thecontrol samples from the women without cervicallesions (29.1%, P ¼ 0.004). The integrated form wasfound in 26.4% cervical cancer samples and in 10.9%controls (P ¼ 0.02). Both cervical cancer and the con-trol samples showed a high percent of mixed form ofHPV 16 genome (Table III). An increased integratedform with a concurrent decreased episomal form wasfound as the lesion grade increased. It was demon-strated that the E2/E6 ratio and the state of viralgenome integration between cervical cancer samplesand the controls were significantly different(P ¼ 3.077E�6 and 0.001, respectively). However,the state of viral genome integration and the E2/E6ratio did not show a significant difference between
TABLE II. Demographics and Characteristics ofthe Subjects
Group N
Age
Mean Range Median
CCIa 32 46.3 � 13.1 25–64 46.0IIa 43 47.4 � 10.6 27–76 47.0Unknowna 10 48.7 � 12.1 28–65 47.5Total 85 47.2 � 10.4 25–76 46.0
ControlGW 26 29.7 � 9.5 19–54 26.7Health 29 45.7 � 9.8 22–65 50.0Total 55 37.9 � 12.6 19–65 38.0
N: the number of the subjects of each group.aFIGO stage.
TABLE III. HPV 16 Integration and the Viral Load in Controls and Cases
N
State of viral integration Viral loada
Integrated Mixed Episomal Mean Median Range
CCIb 32 11 (34.4%) 19 (59.4%) 2 (6.2%) 12,337 � 25,604 237.7 1.60–1.04E5IIb 43 12 (27.9%) 27 (62.8%) 4 (9.3) 67,453 � 319,821 51.3 0.00–1.93E6Unknownb 10 0 7 (70.0%) 3 (30.0%) 122 � 210 30.8 4.90–613.24Total 85 23 (26.4%) 55 (63.2%) 9 (10.3%) 38,329 � 227,135 205.2 0.00–1.93E6Control 55 6 (10.9%) 33 (60.0%) 16 (29.1%) 4,619 � 27,079 45.4 0.80–1.92E5
N: the number of the subjects of each group.aThe viral load was the relative quantification that was the ratio of E6/b-globin.bFIGO stage.
HPV 16 Status in Predicting Cervical Cancer 649
J. Med. Virol. DOI 10.1002/jmv

the two FIGO stages (P ¼ 0.38 and 0.490,respectively).
An increased E2/E6 ratio was correlated with a de-creased risk of cervical cancer (OR ¼ 0.137,P ¼ 9.55E�6). The integrated form and mixed formwere correlated with an increased risk of cervical can-cer (OR ¼ 6.54, P ¼ 0.005; OR ¼ 2.93, P ¼ 0.042, re-spectively), as shown in Table IV. The E2/E6 ratio,integrated form and mixed form were not associatedwith the risk from FIGO stage I to FIGO stage II(P > 0.05 for all).
Association Between the HPV 16 Viral Loadand Cervical Cancer
The mean viral loads of cervical cancer and the con-trol samples were summarized in Table III. HPV 16viral load increased with disease progression, and thedifference between cervical cancer samples and thecontrols was significant (P ¼ 0.011; Mann–Whitneytest). The mean viral load of cervical cancer sampleswas higher (38,329 � 227,135) than that of the con-trols (4,619 � 27,079; P ¼ 0.294), and the median vi-ral load of cervical cancer samples (205.21) was alsohigher than that of the controls (45.39). The mean vi-ral load of FIGO stage I was lower than that of FIGOstage II (12,337 � 25,604 and 67,453 � 319,821, re-spectively); however, although the difference of meanvial load was not significant (P ¼ 0.616), the FIGOstage II had higher median viral load than FIGOstage I.
Effectiveness of the HPV 16 E2/E6 Ratio and theState of Viral Genome Integration in Predicting
the Risk of Cervical Cancer
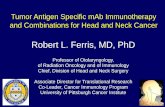
It was demonstrated that the ROC analysis of theE2/E6 ratio and the state of viral genome integrationcould play an important role in discriminating cervi-cal cancer patients from the controls (Fig. 1A),Table V lists the detailed information of ROC analysisstatistics. The E2/E6 ratio had a relative higher dis-crimination accuracy, with a larger AUC value (0.734)than that of the state of viral genome integration(AUC ¼ 0.640). The accuracies of both discriminationswere significant (E2/E6 ratio: P ¼ 3.10E�6; the stateof viral genome integration: P ¼ 0.05). In Table V, theE2/E6 ratio had a higher sensitivity (60.0%) and lower
specificity (84.7%) than those of the state of viral ge-nome integration (sensitivity: 29.1%, specificity:89.4%). The cutoff for the E2/E6 ratio was 0.484, andthe state of viral genome integration should be dichot-omized as integrated versus mixed plus episomalforms. After adjustment with age, a higher predictiveeffectiveness was obtained. As demonstrated inFigure 1B, after combining age and the E2/E6 ratiointo the logistic regression equation, the effectivenessof the risk prediction of cervical cancer was improved(AUC ¼ 0.777, P ¼ 7.90E�8). The cutoff of the proba-bility was 0.54, which was able to discriminate cervi-cal cancer patients from the controls, and thesensitivity and specificity were 82.05% and 71.7%, re-spectively. Furthermore, the predictive effectivenessof the state of viral genome integration was also im-proved (AUC ¼ 0.743, P ¼ 2.36E�6). The cutoff of theprobability was 0.462, which was able to predict therisk of cervical cancer, and the sensitivity and speci-ficity were 94.8% and 71.7%, respectively.
Predictive Effectiveness of HPV 16 Viral Load
It was indicated that the HPV viral load also had asignificant, but not higher, accuracy in discriminatingcervical cancer patients from the controls(AUC ¼ 0.632, P ¼ 0.01; Fig. 1B). The relative viralload of 1846.6 was the cutoff in differentiating cervicalcancer patients from the controls, and the sensitivityand specificity were 26.8% and 96.1%, respectively(Table V). After adjustment with age, the predictiveeffectiveness (AUC ¼ 0.694, P ¼ 1.63E�4) was higherthan that without age adjustment (AUC ¼ 0.632). Thecutoff of probability was 0.49, which was able to dis-criminate cervical cancer patients from the controls,and the sensitivity and specificity were 91.0% and47.2%.
Predictive Effectiveness of Combinations ofthe Factors
It was indicated that both the state of viral genomeintegration and the viral load were not in the logisticregression equation, the E2/E6 ratio was associatedwith a higher risk of cervical cancer, and contributedto the effectiveness of risk prediction of cervical can-cer by logistic regression analyses adjusted with age,as shown in Figure 2.
TABLE IV. Risk of Cervical Cancer of the HPV 16 E2/E6 Ratio and the State of Viral Genome Integration AdjustedWith Age
E2/E6 ratio
State of viral genome integration
Integrated form Mixed form
OR 95% CI P-value OR 95% CI P-value OR 95% CI P-value
CC versus control 0.137 0.05–0.371 9.55 � 10�5 6.543 1.770–24.194 0.005 2.934 1.04–8.273 0.042FIGO I versus II 1.496 0.351–6.375 0.59 0.545 0.083–3.590 0.528 0.711 0.118–4.281 0.709
650 Chang et al.
J. Med. Virol. DOI 10.1002/jmv

DISCUSSION
Cervical cancer is preventable by effective screen-ing. Well-organized screening programs implementingbetter screening strategies and methods would de-crease the burden of this disease [Davies et al., 2006].
Currently, although HPV DNA detection, cytologytest, and colposcopy are the common methods for
cervical cancer screening, these methods require re-peated clinic visits and place undesirable psychologi-cal and financial burdens on women. More rapid testswith increased specificity are needed to reduce thenumber of regular screenings that are currently re-quired and extend the intervals between tests.
Previously, it was confirmed that HPV integrationand E2 gene disruption represent the common and
Fig. 1. The ROC analysis of the HPV 16 E2/E6 ratio, the state of viral genome integration and theviral load in discriminating CC and the controls. A: The E2/E6 ratio and the state of viral genomeintegration in predicting CC. B: The E2/E6 ratio and the state of viral genome integration in predictingCC after adjusting with age using logistic regression. C: The viral load in predicting CC. D: The viralload in predicting CC after adjusting with age using logistic regression.
TABLE V. Sensitivity, Specificity, and Cutoff of the E2/E6 Ratio, the State of Viral Genome Integration and the Viral Loadof HPV 16 in Predicting CC
Variables AUC 95% CI P-value CutoffSensitivity
(%)Specificity
(%)
E2/E6 ratio 0.734 � 0.044 0.647–0.821 3.10E�6 0.484 60.0 84.7State of viral genome integration 0.640 � 0.05 0.546–0.733 0.05 Non-episomal
versus episomal29.1 89.4
Viral loada 0.632 � 0.050 0.535–0.730 0.01 1846.6 26.8 96.1Adjusted with ageb
E2/E6 ratio 0.777 � 0.045 0.686–0.866 7.90E�8 0.540 81.2 71.7State of viral genome integration 0.743 � 0.045 0.645–0.833 2.360E�6 0.462 94.8 52.8Viral loada 0.694 � 0.049 0.600–0.792 1.630E�4 0.490 91.0 47.2
aThe viral load was the relative quantification that was the ratio of E6/b-globin.bThe E2/E6 ratio, the state of viral genome integration and the viral load adjusted with age using logistic regression analysis.
HPV 16 Status in Predicting Cervical Cancer 651
J. Med. Virol. DOI 10.1002/jmv

important events in the HPV-infected lesions [DeMarco et al., 2007; Collins et al., 2009]. In the currentstudy, it was tested whether faster and more sensitivecervical cancer prediction was possible based on thestate of viral genome integration of the most preva-lent HPV type in China, HPV 16. It was found thatintegration occurred in 10.9% of the controls and26.4% of the cervical cancer samples (P < 0.05), andlower E2/E6 ratio and the integrated viral form wereassociated with a higher risk of cervical cancer(OR ¼ 7.300, 6.453 and P ¼ 9.55E�5, 0.042, respec-tively). Further analysis of risk predictions of cervicalcancer revealed that the low E2/E6 ratio exhibits rela-tively high accuracy with the sensitivity and specifici-ty of 81.2% and 71.7%, respectively. The AUC of theE2/E6 ratio was 0.777. The three states of the viralgenome determined by the E2/E6 ratio had evenhigher sensitivity (94.8%) but lower specificity (52.8%)compared with the sensitivity and specificity of theE2/E6 ratio. Consistent with these results, a study byCricca et al. [2007] found that the prediction was im-proved by replacing the state of viral genome integra-tion with the E2/E6 ratio to predict the risk of cervicalcancer. In that study, the sensitivity was improved to100% from 81.8%, the accuracy was improved to 0.962from 0.898 upon replacement of the viral genome inte-gration state with the E2/E6 ratio [Cricca et al.,2007].
DNA-based HPV detection displayed sensitivitiesranging from 91.0% to 96.0% and specificities rangingfrom 38.0% to 46.0% among different studies [Ander-sson et al., 2011; Benevolo et al., 2011; Clad et al.,2011; Ratnam et al., 2011]. A high risk HPV E6/E7mRNA assay showed higher specificities (43.2–68.0%)with similar sensitivities [Andersson et al., 2011;Benevolo et al., 2011; Clad et al., 2011; Ratnam et al.,2011]. Visual inspection with acetic acid (VIA) indetecting cervical lesions demonstrated lower
sensitivities, less than 80.0% [Sritipsukho and Tha-weekul, 2010; Sauvaget et al., 2011]. The sensitivity(specificity) of HC2 also varied among different stud-ies, from 97.1% (85.6%) in the study by Qiao et al.[2008] to 91.3% (61.0%) in the study by Clad et al.[2011]. Compared with the common screening meth-ods described above, the current study demonstratesthat the E2/E6 ratio had an improved specificity(71.7%) and better sensitivity (81.2%).
While, different studies have shown that the per-centages of the HPV 16 E2/E6 ratio or the state ofviral genome integration among different cervical le-sion samples were not consistent completely. The per-centage of the non-episomal form of virus in thecontrol samples ranged from 27.8% in the study byCricca et al. [2007] to 44.5% in the study by Bouletet al. [2009] and was 60% in current study. The per-centage of the non-episomal form of virus in cervicalcancer samples ranged from 63.2% in current study to68.8% in the study by Boulet et al. [2009] and to81.8% in the study by Cricca et al. [2007]. One possi-bility is that the sample differences between cervicalcells and cervical tissues are responsible for the re-sult: cervical cells from the cervical cancer samplesinclude normal and disease cells which would impacton the value of the E2/E6 ratio. Another possibility isthat the actual E2/E6 ratio is underestimated owingto other disruptions of the E2 gene that omit this80 bp amplification region resulting this marker beingless effective as a cervical cancer predictor thanexpected. Overall, the state of viral genome integra-tion and the E2/E6 ratio were strong candidatemarkers for predicting the risk of cervical cancer andthey would be better methods with a high effective-ness if avoiding or reducing the normal cell influence.
It was demonstrated that a high viral load was as-sociated with virus-related cancer risk in previousstudies. High viral loads of Hepatitis B virus andEpstein–Barr virus DNA were found to be associatedwith hepatocellular carcinoma and nasopharyngealcancer, respectively [Tan et al., 2006; Chindavijaket al., 2010; Mendy et al., 2010]. Increased HPV viralload also correlated with an increased risk of preva-lent or incident disease, as determined by HC2 assays[Dalstein et al., 2003; Wu et al., 2006]. Q-PCR studieshave demonstrated consistently that HPV viral loadwas positively associated with the evolution of lesions[Ylitalo et al., 2000; Tan et al., 2006; Cricca et al.,2007]. As a representative of a more prevalent high-risk type, a high viral load of HPV 18 correlated withhigh-grade squamous intraepithelial lesions [Xi et al.,2009]. Based on these results, oncogenic viral load hasbeen suggested to be associated with carcinogenesisand represents a useful marker for predicting cancerrisk.
In this study, it was found that the mean viralload of HPV 16 was higher in the controls (4,619 �27,079) than that in cervical cancer samples(38,329 � 227,135; P ¼ 0.011) among Chinese women.HPV 16 viral load contributed to the risk of cervical
Fig. 2. The ROC analysis combining the HPV 16 E2/E6 ratio, thestate of viral genome integration and the viral load adjusted withage in discriminating CC from the controls with logistic regression.
652 Chang et al.
J. Med. Virol. DOI 10.1002/jmv

cancer (AUC ¼ 0.694, P ¼ 1.63E�4), although its pre-dictive effectiveness was lower than that of the HPV16 E2/E6 ratio (AUC ¼ 0.777, P ¼ 7.90E�8) and thestate of viral genome integration (AUC ¼ 0.743,P ¼ 2.36E�6). These results were inconsistent withprevious reports that HPV 16 viral load alone was astrong positive marker [Cricca et al., 2007] and thatHR-HPV viral load was not a suitable marker forhigh-grade cervical lesions [Carcopino et al., 2011].The background from the normal cells in the cervicalcancer cell samples may affect the viral load quantita-tion, resulting in underestimation the contribution ofthe viral load to cervical cancer prediction.
It was confirmed that HPV 16 integration inducedthe deregulation of E6 and E7 oncogene expression bydisrupting the E2 gene, especially in the hinge region,and that integration represents a major event in HPV16 induced cervical carcinogenesis [Collins et al.,2009]. Thus, the state of viral genome integration andthe E2/E6 ratio of the HPV 16 genome may be usefulfactors for predicting cervical cancer risk. In addition,the HPV 16 viral load that was adjusted with age hada moderate predictive effectiveness suggesting thatthis marker should be considered as a candidate forpredicting the risk of cervical cancer.
ACKNOWLEDGMENTS
We thank the following hospitals for providingthe samples: Department of Gynecology, Cancer Hos-pital of Gansu Province, Lanzhou, China; Departmentof Oncology, Maternal and Child Health Hospital ofJiangxi Province, Nanchang, China; Department ofGynecology, People Hospital of Zhuhai, GuangdongProvince, China; Department of Gynecological Oncolo-gy, 2nd Affiliated Hospital of Sun Yat-Sen (Zhong-shan) University, Guangzhou.
REFERENCES
Akobeng AK. 2007. Understanding diagnostic tests 3: Receiver oper-ating characteristic curves. Acta Paediatr 96:644–647.
Anderson JE, Hansen LL, Mooren FC, Post M, Hug H, Zuse A, LosM. 2006. Methods and biomarkers for the diagnosis and progno-sis of cancer and other diseases: Towards personalized medicine.Drug Resist Update 9:198–210.
Andersson E, Karrberg C, Radberg T, Blomqvist L, Zetterqvist BM,Ryd W, Lindh M, Horal P. 2011. Type-specific human papilloma-virus E6/E7 mRNA detection by real-time PCR improves identifi-cation of cervical neoplasia. J Clin Microbiol 49:3794–3799.
Apostolidou S, Hadwin R, Burnell M, Jones A, Baff D, Pyndiah N,Mould T, Jacobs IJ, Beddows S, Kocjan G, Widschwendter M.2009. DNA methylation analysis in liquid-based cytology for cer-vical cancer screening. Int J Cancer 125:2995–3002.
Arbyn M, Sankaranarayanan R, Muwonge R, Keita N, Dolo A, Mba-lawa CG, Nouhou H, Sakande B, Wesley R, Somanathan T,Sharma A, Shastri S, Basu P. 2008. Pooled analysis of the accu-racy of five cervical cancer screening tests assessed in elevenstudies in Africa and India. Int J Cancer 123:153–160.
Arbyn M, Walker A, Meijer C. 2010. HPV-based cervical-cancerscreening in China. Lancet Oncol 11:1112–1113.
Arbyn M, Castellsague X, de Sanjose S, Bruni L, Saraiya M, Bray F,Ferlay J. 2011. Worldwide burden of cervical cancer in 2008.Ann Oncol 22:2675–2686.
Badal V, Chuang LS, Tan EH, Badal S, Villa LL, Wheeler CM,Li BF, Bernard HU. 2003. CpG methylation of human
papillomavirus type 16 DNA in cervical cancer cell lines and inclinical specimens: Genomic hypomethylation correlates withcarcinogenic progression. J Virol 77:6227–6234.
Benevolo M, Vocaturo A, Caraceni D, French D, Rosini S, Zappa-costa R, Terrenato I, Ciccocioppo L, Frega A, Giorgi Rossi P.2011. Sensitivity, specificity, and clinical value of human papillo-mavirus (HPV) E6/E7 mRNA assay as a triage test for cervicalcytology and HPV DNA test. J Clin Microbiol 49:2643–2650.
Bhattacharjee B, Sengupta S. 2006. CpG methylation of HPV 16LCR at E2 binding site proximal to P97 is associated with cervi-cal cancer in presence of intact E2. Virology 354:280–285.
Boulet GAV, Benoy IH, Depuydt CE, Horvath CAJ, Aerts M, HensN, Vereecken AJ, Bogers JJ. 2009. Human papillomavirus 16Load and E2/E6 ratio in HPV16-positive women: Biomarkers forcervical intraepithelial neoplasia �2 in a liquid-based cytologysetting? Cancer Epidem Biomar 18:2992–2999.
Carcopino X, Bolger N, Henry M, Mancini J, Boubli L, Olive D,Cleary S, Prendiville W, Tamalet C. 2011. Evaluation of type-specific HPV persistence and high-risk HPV viral load quantita-tion in HPV positive women under 30 with normal cervical cytol-ogy. J Med Virol 83:637–643.
Chindavijak S, Tiwawech D, Sangariyavanich E. 2010. Quantitativedetection of plasma cell-free Epstein–Barr virus DNA in naso-pharyngeal carcinoma patients by real-TIME PCR. ThaiCancer J 28:13–23.
Clad A, Reuschenbach M, Weinschenk J, Grote R, Rahmsdorf J,Freudenberg N. 2011. Performance of the Aptima high-risk hu-man papillomavirus mRNA assay in a referral population in com-parison with hybrid capture 2 and cytology. J Clin Microbiol49:1071–1076.
Collins SI, Constandinou-Williams C, Wen K, Young LS, Roberts S,Murray PG, Woodman CBJ. 2009. Disruption of the E2 gene is acommon and early event in the natural history of cervical humanpapillomavirus infection: A longitudinal cohort study. CancerRes 69:3828–3832.
Cricca M, Morselli-Labate AM, Venturoli S, Ambretti S, GentilomiGA, Gallinella G, Costa S, Musiani M, Zerbini M. 2007. ViralDNA load, physical status and E2/E6 ratio as markers to gradeHPV16 positive women for high-grade cervical lesions. GynecolOncol 106:549–557.
Dalstein V, Riethmuller D, Pretet JL, Le Bail Carval K, Sautiere JL,Carbillet JP, Kantelip B, Schaal JP, Mougin C. 2003. Persistenceand load of high-risk HPV are predictors for development ofhigh-grade cervical lesions: A longitudinal French cohort study.Int J Cancer 106:396–403.
Davies P, Arbyn M, Dillner J, Kitchener HC, Meijer CJ, Ronco G,Hakama M. 2006. A report on the current status of Europeanresearch on the use of human papillomavirus testing for primarycervical cancer screening. Int J Cancer 118:791–796.
De Marco L, Gillio-Tos A, Bonello L, Ghisetti V, Ronco G, Merletti F.2007. Detection of human papillomavirus type 16 integration inpre-neoplastic cervical lesions and confirmation by DIPS-PCRand sequencing. J Clin Virol 38:7–13.
Depuydt CE, Boulet GA, Horvath CA, Benoy IH, Vereecken AJ,Bogers JJ. 2007. Comparison of MY09/11 consensus PCR andtype-specific PCRs in the detection of oncogenic HPV types.J Cell Mol Med 11:881–891.
Fay J, Kelehan P, Lambkin H, Schwartz S. 2009. Increased expres-sion of cellular RNA-binding proteins in HPV-induced neoplasiaand cervical cancer. J Med Virol 81:897–907.
Guo M, Baruch AC, Silva EG, Jan YJ, Lin E, Sneige N, DeaversMT. 2011. Efficacy of p16 and ProExC immunostaining in thedetection of high-grade cervical intraepithelial neoplasia and cer-vical carcinoma. Am J Clin Pathol 135:212–220.
Insinga RP, Perez G, Wheeler CM, Koutsky LA, Garland SM,Leodolter S, Joura EA, Ferris DG, Steben M, Hernandez-AvilaM. 2011. Incident cervical HPV Infections in young women:Transition probabilities for CIN and infection clearance. CancerEpidem Biomar 20:287–296.
Jeon S, Allen-Hoffmann BL, Lambert PF. 1995. Integration of hu-man papillomavirus type 16 into the human genome correlateswith a selective growth advantage of cells. J Virol 69:2989–2997.
Kitchener HC, Gilham C, Sargent A, Bailey A, Albrow R, Roberts C,Desai M, Mather J, Turner A, Moss S, Peto J. 2011.A comparison of HPV DNA testing and liquid based cytologyover three rounds of primary cervical screening: Extended followup in the ARTISTIC trial. Eur J Cancer 47:864–871.
HPV 16 Status in Predicting Cervical Cancer 653
J. Med. Virol. DOI 10.1002/jmv

Klingenstein A, Haritoglou I, Schaumberger MM, Markus M, Nent-wich MM, Hein R, Schaller UC. 2011. Receiver operating charac-teristic analysis: Calculation for the marker ‘melanomainhibitory activity’ in metastatic uveal melanoma patients. Mela-noma Res 21:352–356.
Laxman B, Morris DS, Yu J, Siddiqui J, Cao J, Mehra R, LonigroRJ, Tsodikov A, Wei JT, Tomlins SA, Chinnaiyana AM. 2008.A first-generation multiplex biomarker analysis of urine for theearly detection of prostate cancer. Cancer Res 68:645–649.
Mao C, Hughes JP, Kiviat N, Kuypers J, Lee SK, Adam DE, Kout-sky LA. 2003. Clinical findings among young women with genitalhuman papillomavirus infection. Am J Obstet Gynecol 188:677–684.
Mendy ME, Welzel T, Lesi OA, Hainaut P, Hall AJ, Kuniholm MH,McConkey S, Goedert JJ, Kaye S, Rowland-Jones S. 2010. Hepa-titis B viral load and risk for liver cirrhosis and hepatocellularcarcinoma in The Gambia, West Africa. J Viral Hepatitis 17:115–122.
Mutirangura A. 2001. Serum/plasma viral DNA: Mechanisms anddiagnostic applications to nasopharyngeal and cervical carcino-ma. Ann N Y Acad Sci 945:59–67.
Nanda K, McCrory DC, Myers ER, Bastian LA, Hasselblad V, Hick-ey JD, Matchar DB. 2000. Accuracy of the Papanicolaou test inscreening for and follow-up of cervical cytologic abnormalities: Asystematic review. Ann Intern Med 132:810–819.
Peitsaro P, Johansson B, Syrjanen S. 2002. Integrated human papil-lomavirus type 16 is frequently found in cervical cancer precur-sors as demonstrated by a novel quantitative real-time PCRtechnique. J Clin Microbiol 40:886–891.
Qiao YL, Sellors JW, Eder PS, Bao YP, Lim JM, Zhao FH, Weigl B,Zhang WH, Peck RB, Li L, Chen F, Pan QJ, Lorincz AT. 2008.A new HPV-DNA test for cervical-cancer screening in developingregions: A cross-sectional study of clinical accuracy in ruralChina. Lancet Oncol 9:929–936.
Ratnam S, Coutlee F, Fontaine D, Bentley J, Escott N, Ghatage P,Gadag V, Holloway G, Bartellas E, Kum N, Giede C, Lear A.2011. Aptima HPV E6/E7 mRNA test is as sensitive as HybridCapture 2 Assay but more specific at detecting cervical precancerand cancer. J Clin Microbiol 49:557–564.
Sambrook J, Russell DW. 2001. Molecular cloning: A laboratorymanual. New York: CSHL Press.
Sauvaget C, Fayette JM, Muwonge R, Wesley R, SankaranarayananR. 2011. Accuracy of visual inspection with acetic acid for cervi-cal cancer screening. Int J Gynecol Obstet 113:14–24.
Smith JS, Lindsay L, Hoots B, Keys J, Franceschi S, Winer R,Clifford GM. 2007. Human papillomavirus type distribution in
invasive cervical cancer and high-grade cervical lesions: A meta-analysis update. Int J Cancer 121:621–632.
Sritipsukho P, Thaweekul Y. 2010. Accuracy of visual inspectionwith acetic acid (VIA) for cervical cancer screening: A systematicreview. J Med Assoc Thai 93:S254–S261.
Stanley M. 2010. Pathology and epidemiology of HPV infection infemales. Gynecol Oncol 117:S5–S10.
Stoler MH, Schiffman M. 2001. Interobserver reproducibility of cer-vical cytologic and histologic interpretations: Realistic estimatesfrom the ASCUS-LSIL Triage Study. JAMA 285:1500–1505.
Tan EL, Looi LM, Sam CK. 2006. Evaluation of plasma Epstein–Barr virus DNA load as a prognostic marker for nasopharyngealcarcinoma. Singapore Med J 47:803–807.
Termini L, Maciag PC, Soares FA, Nonogaki S, Pereira SM, AlvesVA, Longatto-Filho A, Villa LL. 2010. Analysis of human kalli-krein 7 expression as a potential biomarker in cervical neoplasia.Int J Cancer 127:485–490.
Tripepi G, Jager KJ, Dekker FW, Zoccali C. 2009. Diagnostic meth-ods 2: Receiver operating characteristic (ROC) curves. KidneyInt 76:252–256.
Walboomers JMM, Jacobs MV, Manos MM, Bosch FX, Kummer JA,Shah KV, Snijders PJF, Peto J, Meijer CJLM, Munoz N. 1999.Human papillomavirus is a necessary cause of invasive cervicalcancer worldwide. J Pathol 189:12–19.
Wentzensen N, Sherman ME, Schiffman M, Wang SS. 2009. Utilityof methylation markers in cervical cancer early detection:Appraisal of the state-of-the-science. Gynecol Oncol 112:293–299.
Wilting SM, van Boerdonk RA, Henken FE, Meijer CJ, Diosdado B,Meijer GA, le Sage C, Agami R, Snijders PJ, Steenbergen RD.2010. Methylation-mediated silencing and tumour suppressivefunction of hsa-miR-124 in cervical cancer. Mol cancer 9:167.
Wu Y, Chen Y, Li L, Yu G, Zhang Y, He Y. 2006. Associations ofhigh-risk HPV types and viral load with cervical cancer in China.J Clin Virol 35:264–269.
Wu Y, Liu B, Lin W, Xu Y, Li L, Zhang Y, Chen S, Xu A. 2007.HPV16 E6 variants and HLA class II polymorphism among Chi-nese women with cervical cancer. J Med Virol 79:439–446.
Xi LF, Koutsky LA, Castle PE, Wheeler CM, Galloway DA, Mao C,Ho J, Kiviat NB. 2009. Human papillomavirus type 18 DNA loadand 2-year cumulative diagnoses of cervical intraepithelial neo-plasia grades 2–3. J Natl Cancer 101:153–161.
Ylitalo N, Josefsson A, Melbye M, Sorensen P, Frisch M, AndersenPK, Sparen P, Gustafsson M, Magnusson P, Ponten J, GyllenstenU, Adami HO. 2000. A prospective study showing long-term in-fection with human papillomavirus 16 before the development ofcervical carcinoma in situ. Cancer Res 60:6027–6032.
654 Chang et al.
J. Med. Virol. DOI 10.1002/jmv