Effective Investigations and Corrective Actions(CAPA)ipapharma.org/events/reports/Anisfield -...
31
© Copyright, Globepharm Consulting, 2008 1 Effective Investigations and Corrective Actions (CAPA) P I i i f Q li E Proper Investigation of Quality Events Michael H. Anisfeld Globepharm Consulting What Do You Do When The Bad Stuff Happens? I It Pretend It Never Happened Ignore It Advise Boss Curse Walk Away It’s a One-Off Advise Your Buddy Pretend It Never Happened !#&*!$%... 2 Fix It Blame Someone Else Investigate + Fix Investigate, Fix + Document Investigate
Transcript of Effective Investigations and Corrective Actions(CAPA)ipapharma.org/events/reports/Anisfield -...

© Copyright, Globepharm Consulting, 2008 1
Effective Investigations and
Corrective Actions (CAPA)
P I i i f Q li EProper Investigation of Quality Events
Michael H. AnisfeldGlobepharm Consulting
What Do You Do When The Bad Stuff Happens?
I It Pretend It Never HappenedIgnore It
Advise Boss Curse
Walk AwayIt’s a One-Off
Advise Your Buddy
Pretend It Never Happened
!#&*!$%...
2
Fix It
Blame Someone Else
Investigate + Fix
Investigate, Fix + Document
Investigate

© Copyright, Globepharm Consulting, 2008 2
Failure/Deviation System
Th f f il /d i i i The purpose of a failure/deviation system is to assure that each failure/deviation does not adversely impact product quality and that effective corrective action is taken to reduce the probability of such failure in the future
4

© Copyright, Globepharm Consulting, 2008 3
Contributors to Failure
MaterialsFacilitiesEquipmentInstrumentationPeople
5
PeopleProcessesProcedures
Failure / DeviationDefinition
F ilFailureProduct does not meet specification.Failure may be detected in/by
ProductionLaboratory
6
DeviationChange in procedures, equipment, materials, personnel related to product manufacture having an impact on product quality

© Copyright, Globepharm Consulting, 2008 4
Definitions
Immediate CauseSituation directly causing the problem
Root CauseBasic Causal Factor, which if corrected or removed prevents a repeat of the problem
Intermediate CauseReason for problem at more fundamental level than the
7
Reason for problem at more fundamental level than the immediate cause, but not the root cause [why-2, why-3]
Root Cause AnalysisStructured questioning process enabling identification of underlying beliefs and practices that result in poor quality
Causes of Failure
C mm n C [End mi S t m ti ] (V i ti n)Common Cause [Endemic – Systematic] (Variation)Originates from the basic elements of the process:
MachinesMaterialsMethodsManpowerMeasurement
8
Assignable Cause [Special] (Variation)An unplanned variation originating outside expected
operating process conditions [special cause variation]

© Copyright, Globepharm Consulting, 2008 5
Failure/DeviationsMeasures
There are three key steps in this process and each of these should There are three key steps in this process and each of these should be monitored regularly
Recording the failures and deviationsTotal numberNumber by department
Action on product batch(es) involved
9
Audit by sampling to verify that corrective action was taken
Corrective action on root causesThere should be an elimination of failures/deviations due to causes for which corrective actions have been implemented
Regulators Expectations
C h i H A h T Comprehensive, Honest Approach To Investigate OOS Results/Failures
Evaluation Using Scientifically Valid Principles
Learning From Experiences
10
Permanent Solutions To Problem
Authorities Not The Ones To Find The Problem

© Copyright, Globepharm Consulting, 2008 6
11
What to Do When the Unexpected Happens
UNEXPECTED?UNEXPECTED?OOS
LaboratoryManufacturing
Water SystemOOTOOEOOY
12
Reconciliation – Yield CheckReconciliation – Packaging Material
DeviationDiscrepancyUnusual Event

© Copyright, Globepharm Consulting, 2008 7
13
What Do The US Regulations Say?
“In ti ti n” p ifi ll t t d in th GMP :Investigation specifically stated in the cGMPs:
§211.22 - Responsibilities of quality control unit. §211.125 - Labeling issuance. §211.170 - Reserve samples. §211.180 - General requirements. §211.186 - Master production and control records.
14
p§211.188 - Batch production and control records. §211.192 - Production record review. §211.198 - Complaint files. §211.204 - Returned drug products.

© Copyright, Globepharm Consulting, 2008 8
What Does The EU Guide Say?
“I ti ti ” ifi ll t t d i th GMP“Investigation” specifically stated in the GMPs:
1.3 Quality Assurance1.4 Quality Control2.7 Production/QC Responsibilities5 39 Production
15
5.39 Production5.56 Packaging Operations6.2 Quality Control8.1 Complaints
Future Regulations
i i l h i d An international harmonized approach to
Risk Management
16
ICH-Q9

© Copyright, Globepharm Consulting, 2008 9
initiate risk management process
risk identification
srisk assessment
ICH-Q9Risk Management
risk analysis
risk evaluation
risk reduction
i k tnage
men
t to
ols
risk control unacceptable
17
risk acceptance
risk communication
Ris
k m
an
review event
risk communicationrisk acceptance
output/results of the risk management process
OK

© Copyright, Globepharm Consulting, 2008 10
CAPA
19
How do you know what’s happening?
R i h h i blRecognize that there is a problem:Capture The DataAnalyze The DataTrend The Data
Then Fix the problem:
20
hen Fix the problemInvestigate the CauseAttempt to Get to “Root Cause”Implement Effective FixesMonitor the Fix

© Copyright, Globepharm Consulting, 2008 11
21CFR820.100 - CAPA
§820.100 Corrective and preventive action(a) Each manufacturer shall establish and maintain procedures for implementing corrective and preventive action. The procedures shall include requirements for:
(1) Analyzing processes, work operations, concessions, quality audit reports, quality records, service records, complaints, returned product, and other sources of quality data to identify existing and potential causes of nonconforming product, or other quality problems.
21
g p , q y pAppropriate statistical methodology shall be employed where necessary to detect recurring quality problems;
(2) Investigating the cause of nonconformities relating to product, processes, and the quality system;
(3) Identifying the action(s) needed to correct and prevent recurrence of nonconforming product and other quality problems;
21CFR820.100 - CAPA
§820.100 Corrective and preventive action (continued)(4) Verifying or validating the corrective and preventive action to ensure that such action is effective and does not adversely affect the finished device;(5) Implementing and recording changes in methods and procedures needed to correct and prevent identified quality problems;(6) Ensuring that information related to quality problems or
f mi d t i di mi t d t th di tl
22
nonconforming product is disseminated to those directly responsible for assuring the quality of such product or the prevention of such problems; and(7) Submitting relevant information on identified quality problems, as well as corrective and preventive actions, for management review.
(b) All activities required under this section, and their results, shall be documented

© Copyright, Globepharm Consulting, 2008 12
CAPA – Analyzing Sources of Quality Data
E i l
CAPA
Complaints/Returns
Repairs/Ser icing
ProcessDeviationsor Failures
Acceptance Activities
Environmental Monitoring
23
CAPAServicing
Calibration/Maintenance
StabilityData
Audits Yields/Scrap
What To Track
T k BTrack By:
Product In-process, release, stability, validation
Event Reason for investigation
Operator/Analyst If cause is operator/analyst error
Instrument/Equipment If cause instrument related
24
Cause Investigation conclusion
Corrective Action Remedy and prevention
Timeliness Time to complete investigations

© Copyright, Globepharm Consulting, 2008 13
Incidents Reported - 2003
CAPA Data Collection
186 178
210
165 171
143132 130
119150
200
250
Incidents
Question:Are we Getting Better as a Company?Or Dropping Off in Capturing Incidents?
25
9885 92
0
50
100
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Run Charts: Trend ChartsEnvironmental Data – Purified Water System
SpecificationSpecificationUpper Limit
OOT? / OOE?
26
SpecificationLower Limit

© Copyright, Globepharm Consulting, 2008 14
Tracking / Trending
Paper/PenPaper/Pen
Spreadsheet (Excel, Oracle)
Dedicated Computer SystemsTrackwise
(Sparta Systems: http://www.sparta-systems.com) CATSweb
(AssurX: http://www.assurx.com/catsweb.html)
27
pMetricStream
(Metric Stream: http://www.metricstream.com) SmartCAPA
(SmartCAPA: http://www.pilgrimsoftware.com)
Others …..
SmartCAPA®(www.pilgrimsoftware.com)
28

© Copyright, Globepharm Consulting, 2008 15
29
Purpose of Investigation
Th f i i i i The purpose of an investigation it to determine the cause of the failure.
Even if the batch is rejected based on the OOS result, the investigation is necessary to determine if the result is associated with other batches of
30
if the result is associated with other batches of the same drug product or other products
FDA: Draft OOS Guideline, September 1998

© Copyright, Globepharm Consulting, 2008 16
Failure / Deviation – What To Do
F il /D i ti D t t d I f QAFailure/Deviation Detected
Perform Investigation
Root Cause Analysis
Inform QA
Batch Disposition
Immediate Fix
24 hours
30 days
31
Communicate to Management
Corrective/Preventive Action
Assess Effectiveness of Fix
Investigations: You’ve Got to Be A Detective!
32

© Copyright, Globepharm Consulting, 2008 17
Investigations 101
P p f n In ti ti nPurpose of an InvestigationObtain facts as to cause
CommonSpecial - Assignable
Process of an InvestigationComplete description of problem
33
p p pValidity of inputsReview key process variablesDetermine scope of investigationDocument investigation
Learn How To Be A Detective
What Equipment What Equipment, Machine, Tool?
What Is Wrong?
What Is the
34
What Is the Complaint?
What is the Undesired Behavior?

© Copyright, Globepharm Consulting, 2008 18
Learn How To Be A Detective
Wh i I l d?Who is Involved?StaffConsultantsVendorsVisitors
35
Name names/positions!
Learn How To Be A Detective
Wh d th bl When does the problem occur?
DayDateTimeShiftPhase of operation
36
Phase of operationWhen in equipment life cycle
Are there time patterns?

© Copyright, Globepharm Consulting, 2008 19
Learn How To Be A Detective
Whi hWhich:UnitAreaDepartmentLineMachine
37
Location of defective item, or where on defective item
Learn How To Be A Detective
How is the “what” or “who” How is the what or who impacted?
Injury / DeathShut-Down /Start-UpDamageType Classification of Defects
38
How MuchHow ManyHow Big An Issue
What resources are needed to handle/resolve the issue!

© Copyright, Globepharm Consulting, 2008 20
Change Analysis
EPROBLEM? COMPARISON?
WHAT?What is the object or
process with the problem?What is wrong?
What similar object or process doesn’t have the
problem? What else could be wrong?
WHERE? Where does the problem occur
Where else could the problem occur?
39
occur problem occur?
WHEN? When did the problem happen?
When did the problem not happen?
HOW BIG? How large is the problem? How large could it be?
Investigation Documentation
40
A B C D E

© Copyright, Globepharm Consulting, 2008 21
Investigation Documentation
D t p bl m dDate problem occurredStatement of the Problem Listing of batches impactedList of personnel interviewedStatement of each person’s opinions and memory of eventDiscussion of potential causesDiscussion of potential impact
41
Discussion of potential impactDiscussion of extent of problemRecommendations for fixesStatement of actions taken to fixFinal decisions regarding batchManagement approvals
42

© Copyright, Globepharm Consulting, 2008 22
Root Cause Analysis
C ti ti t b ti ( ll t ) Corrective actions to observations (usually symptoms) have limited effect on sustained improvement or elimination of recurrence of the failure
Corrective actions need to address the underlying causes and root causes of a problem in order to
43
eliminate the situation from recurring
Root Cause Analysis
EquipmentDesign Capability
Management SystemsQualified SupervisionDesign, Capability
MaintenanceOperator Error
ProceduresNo ProcedureWrong Procedure UsedProcedure Not AvailableProcedure Difficult To Use
TrainingNone
Qualified SupervisionAuditsFeedbackPrior Corrective Actions TakenCommunicationPlanningProcess CapabilityAdequate Time To Perform TaskStandards
ManpowerInformation Available
44
NoneWhenEffectiveness
Quality ControlInspection RequiredInspection Performed
Information AvailableAdequateTimely
Personnel ProblemsTrainingFail/Safe ProcessesEnvironment
LightingNoise
Fatigue
© Copyright, Globepharm Consulting, 2008 23
Corrective Action
Wh i h l l l hi h What is the lowest level at which we can do something to prevent the problem from re-occurring?
45
46

© Copyright, Globepharm Consulting, 2008 24
Investigation Tools
B i t th iBrainstorm the issuesFlowchartingFishbone Analysis – Cause/Effect diagramsWhy-Why AnalysisPareto ChartsRun Charts
47
Run ChartsForce Field AnalysisSix-Sigma Analysis - MAICKepner-Tregoe®
Brainstorming
P ibl t t ti t th f l i t f Possible target questions to serve as the focal point of the brainstorming process:What would solve the problem?What strategy could resolve the root cause?What solutions have already been thought of?What solutions have not been thought of?
48
What solutions have not been thought of?How can we prevent the situation recurring?What different methods might work?What crazy ideas might help?

© Copyright, Globepharm Consulting, 2008 25
Fishbone Analysis
Manpower Management
Batch
People too busyPeople not paying attention
49
Methods Machines
RecordErrors
Why-Why Analysis
Oil D O FlOil Drops On FloorDripping EngineOil Can to CollectFunnel in Oil CanRaise Funnel
50
Raise FunnelUnless you’ve gone 5 levels of questionsyou probably have not got to root cause!

© Copyright, Globepharm Consulting, 2008 26
Pareto Analysis
Pareto: 80 – 20 rule
87
50
60
70
80
90
Batch Record Problems
51
2318
12
0
10
20
30
40
Signatures Data Errors Other
Process Shift, F-440 Particle Size

© Copyright, Globepharm Consulting, 2008 27
APR – Annual Product Review
53
Force-Field Analysis
Th P iti /N ti Wh t ld k Wh t ld k The Positive/Negative Analysis for Solutionscan stimulate thinking just as a the force-field format did in the past. Since we are looking for solutions, the two columns play “better”
What would make the problem
better?
What would make the problem
worse?1.2.3.4.
1.2.3.4.
54
columns play better against “worse”.
4.5.6.7.8.
4.5.6.7.8.
© Copyright, Globepharm Consulting, 2008 28
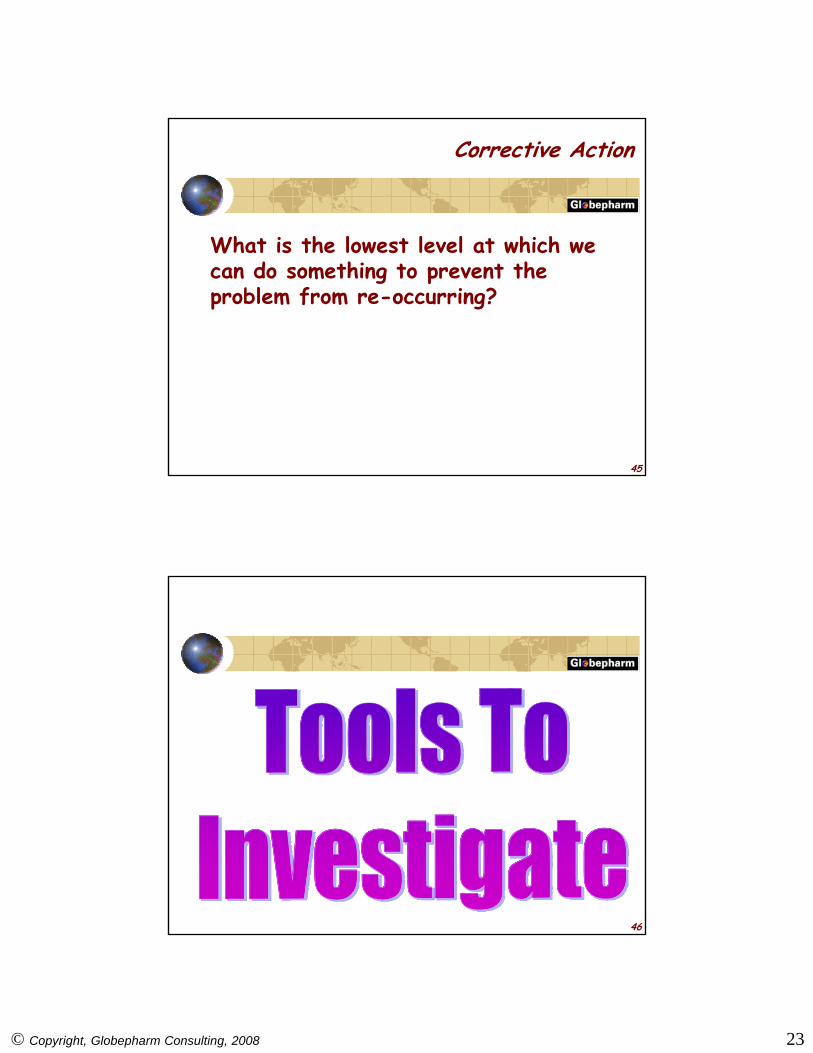
Six Sigma Problem Solving – MAICMeasure Analyze Improve Control
(12) ImplementSolution
(9) Determine Best Solution(4) Identify PotentialCauses
(1) Describe theProblem
(5) Analyze Existing Data
0 251
(10) Pilot Solution
(2) Determine WhenProblem Started
(6) Construct List ofVerified Facts
LSL USL
Item Function Failure Mode Causes Effects Control
Control Plan(2) Lid Prevents Spills Lid falls off due
to looseness
Leaks from drinking hole
Spill when removing lid
Lid diameter too large
Body diameterto small
Surfaces too slick
Hole too large
Hole has toodirect of path
Lid diameter too small
Body diameterto large
Material catches
Burn
Burn
Burn
Stain
Stain
Burn
Burn
Burn
Go-no go gauge
Go-no go gauge
Sampling Plan
Pin gauge
(above)
(above)
Sampling Plan
(7) Compare Causes to Facts
19
12.5
IS NOTIS
WhatWhereWhenExtent
(11) Verify Solution Works
1 2 3 4
T M B T M B T M B T M B
0.251
0.250
0.249
0.248
Fact
1Fa
ct 2
Fact
3Fa
ct 4
Fact
5
Cause 1 O X X O ACause 2 X O A A OC 3 O O A A O
FACTS(1) All Machines(2) Second Shift(3) Certain Codes(4) Started 8/22
55
(8) Collect Additional Data Until Root Cause Identified(3) Measure Problem
Magnitude
15 20 25 30 35
Seal Strength
2 4 6 8 10
Percent Defective
0.0
0.5Pa
1.0
0
OC Curve
© Copyright 2000, Taylor Enterprises Inc.
70
60
40
30
50
TORQUE
L36.0 37.0 38.0
K = 20
K = -20
6
Jan '87 Jul '87 Jan '88 Jul '88
Month
Subgroup
1 5 10 15 20
10.2
10.0
9.8
9.6
Radius
Upper Control Limit
Lower Control Limit
Cause 3 O O A A OCause 4 X A X O OCause 5 O O O O X
(4) Started 8/22(5) Steadily Worse(6) All Operators
A B C E HCode
Num
ber
D F G
56

© Copyright, Globepharm Consulting, 2008 29
initiate risk management process
risk identification
srisk assessment
ICH-Q9Risk Management
risk analysis
risk evaluation
risk reduction
i k tnage
men
t to
ols
risk control unacceptable
57
risk acceptance
risk communication
Ris
k m
an
review event
risk communicationrisk acceptance
output/results of the risk management process
OK
Tools To Prioritize Fixes and Efforts
FME F il M d Eff l iFMEA - Failure Mode Effect Analysis
FTA - Fault Tree Analysis
HACCP Hazard Analysis
58
HACCP - Hazard Analysis, Critical Control Points

© Copyright, Globepharm Consulting, 2008 30
BibliographyRoot Cause Analysis:
- Kepner and Tregoe, “The New Rational Manager”- Paradies and Unger, “Taproot: The System for Root Cause Analysis,
Problem Investigation & Proactive Improvement”- Ammerman “The Root Cause Analysis Handbook”- Ammerman, The Root Cause Analysis Handbook- Pokras, “Systematic Problem-Solving and Decision-Making”
Risk:McDermott et al., “The Basics of FMEA”
Human Error:Lorenzo, ABS Consulting, “A Manager’s Guide to Reducing Human Error”
Management’s Role:
59
gHarbour and Kieffer, “Managing the Quality System”
FDA:“Investigating Out of Specification (OOS) Test Results for Pharmaceutical Production” (Guidance), September 1998Quality Systems Approach to Pharmaceutical GMPs, September 2004
Mi h l H Ani f ld
Stay In Touch
Michael H. AnisfeldGlobepharm Consulting313 Pine StreetDeerfield IL 60015, USA
Phone: USA +1+847 914 0922
60
Fax: USA +1+847 914 0988E-mail: [email protected]: www.globepharm.org

© Copyright, Globepharm Consulting, 2008 31
61
Questions?
62