Arbres à Palabres avril 2016 - journal interne de Prêt à Partir par François Piot



Editorial Team:Rachel Crane (GSSHealth) Michele Merkel, MS (GSSHealth)Tsehaynesh Messele, PhD (ASLM)Laurel Oldach (GSSHealth)Corey White, MPA (ASLM)Jessica Fried, MPH (GSSHealth) Caroline DeLuca (GSSHealth)
Lead Editor: Paula Fernandes, MBA, PhD (GSSHealth)For submissions and inquiries please contact: [email protected].
Disclaimer: Adverts that appear in this newsletter are paid supplements and do not represent endorsements by the African Society for Laboratory Medicine.


Letter from the ASLM CEO
Looking Ahead to the ASLM2014 CommencementIt is with great enthusiasm that I invite you to participate in the ASLM2014 international conference, which opens in a little less than one month in Cape Town, South Africa. Our committed staff and partners have designed a highly interactive conference that promises to be rich with scientific innovation. The conference theme, “Innovation and Integration of Laboratory and Clinical Systems:
Reshaping the Future of HIV, TB, Malaria, Flu, Neglected Tropical Diseases and Emerging Pathogens in Africa,’’ is especially timely as our world community continues to combat the current Ebola outbreak. This meeting, convening from 28 November through 4 December, will create an empowering environment for experts to deliberate effective preparedness and emergency responses for emerging pathogens, advancing our recent efforts to prepare technical and training documentation to guide laboratories through outbreak response, particularly for Ebola. With a line-up of exemplary plenary speakers and programmes, including lunch-and-learn sessions, roundtable discussions and a young professionals track, ASLM2014 is not to be missed!
We are still propelled by the momentum gained from our first international conference, ASLM2012, in which six African government representatives signed a Ministerial Call for Action, pledging their commitment to advancing laboratory medicine and diagnostics in the region. Within the past few months, we have seen a number of new signatories join this important Ministerial Call for Action, reinforcing their countries’ commitment to robust laboratory systems.
In alignment with the Diagnostics Access Initiative (DAI), launched earlier this year, ASLM has hosted several key meetings and workshops, engaging expert participants in topics such as HIV viral load testing, the implementation of national laboratory plans, and workforce development, amongst others. Currently, ASLM is in the process of creating a detailed Roadmap to guide governments, multilateral agencies and other stakeholders in achieving laboratory strengthening initiatives set forth by international priorities.
Additionally, ASLM has embarked on an important partnership with the European and Developing Countries Clinical Trials Partnership (EDCTP), in which ASLM will support the implementation of quality management systems in EDCTP-funded laboratories.
This issue’s Feature article on infectious disease surveillance, “Infectious Disease Surveillance in Times of Calm and in Times of Storm”, available on page 18, discusses different surveillance approaches for optimal disease tracking, proving especially timely in light of the current Ebola outbreak.
Additional in-depth information on the above-mentioned ASLM activities can be found in this issue of Lab Culture. We hope you enjoy reading and sincerely hope to see you at ASLM2014. Please visit www.ASLM2014.org for more information.
Dr. Tsehaynesh Messele, CEO, ASLM
1 November 2014: ASLM Newsletter

At ASLM2014 attend:
• Plenarysessions• Oralpresentations• Lunch&learnsessions• Roundtablediscussions
2
ASLM2014 Special Section
Pre-ConferenceSeminarsBegin 29-Nov-2014
ASLM2014OpeningCeremony 01-Dec-2014
Learn more about the conference at www.ASLM2014.org
KEY DATES
November 2014: ASLM Newsletter
Malaria EIDS
TB
Innovation&
Integration
HIV
NTDs
Flu

3
A Profile of Virologist Dr. Peter Piot, Ebola Co-Discoverer, AIDS Expert and ASLM2014 Plenary Speaker Dr. Peter Piot is the Director and Professor of Global Health at the London School of Hygiene and Tropical Medicine (LSTHM), as well as a Plenary Keynote Speaker for the ASLM2014 international conference.
In September 1976, at age 27, the young virologist Dr. Peter Piot was working in a laboratory in Antwerp, Belgium, when a sample arrived from Yambuku, Zaire, containing a blood sample from a Belgian nun who had fallen sick from a mysterious illness.1,2
Yellow fever virus was suspected, but test results came back negative. The blood also tested negative for Lassa fever, Marburg, dengue and typhoid, causing the laboratory team to suspect destruction of the pathogen during sample transport.3,4 But after laboratory mice injected with the blood began dying, Dr. Piot and his colleagues realised the infectious agent had not been destroyed, and that the blood contained something potentially very dangerous.5,6 When the laboratory team was finally able to isolate and examine the pathogen under an electron microscope, they found an entirely new virus that Dr. Piot described as “very big, very long and worm-like.”7 Dr. Piot would go on to join an international team of scientists in Yambuku, Zaire, embarking on an epidemiological investigation to determine how the new virus spread.8 The virus would come to be known as Ebola.
Member News
1 Dr. Peter Piot made history with ’76 Ebola discovery. (2014, October 7). Retrieved from http://www.sfgate.com/health/article/Dr-Peter-Piot-made-history-with-76-Ebola-5805431.php
2 Von Bredow, R., & Hackenbroch, V. (2014, October 4). ‘In 1976 I discovered Ebola - now I fear an unimaginable tragedy’. Retrieved from http://www.theguardian.com/world/2014/oct/04/ebola-zaire-peter-piot-outbreak
3 Dr. Peter Piot made history with ’76 Ebola discovery. (2014, October 7). Retrieved from http://www.sfgate.com/health/article/Dr-Peter-Piot-made-history-with-76-Ebola-5805431.php
4 Von Bredow, R., & Hackenbroch, V. (2014, October 4). ‘In 1976 I discovered Ebola - now I fear an unimaginable tragedy’. Retrieved from http://www.theguardian.com/world/2014/oct/04/ebola-zaire-peter-piot-outbreak
5 Dr. Peter Piot made history with ’76 Ebola discovery. (2014, October 7). Retrieved from http://www.sfgate.com/health/article/Dr-Peter-Piot-made-history-with-76-Ebola-5805431.php
6 Von Bredow, R., & Hackenbroch, V. (2014, October 4). ‘In 1976 I discovered Ebola - now I fear an unimaginable tragedy’. Retrieved from http://www.theguardian.com/world/2014/oct/04/ebola-zaire-peter-piot-outbreak
7 Von Bredow, R., & Hackenbroch, V. (2014, October 4). ‘In 1976 I discovered Ebola - now I fear an unimaginable tragedy’. Retrieved from http://www.theguardian.com/world/2014/oct/04/ebola-zaire-peter-piot-outbreak
8 Dr. Peter Piot made history with ’76 Ebola discovery. (2014, October 7). Retrieved from http://www.sfgate.com/health/article/Dr-Peter-Piot-made-history-with-76-Ebola-5805431.php
Dr. Peter Piot is the Director and Professor of Global Health at the London School of Hygiene and Tropical Medicine (LSTHM), as well as a Plenary Keynote Speaker for the ASLM2014 international conference.
November 2014: ASLM Newsletter

4
In the 1980s, following his work in Yambuku, Dr. Piot became one of the first scientists to study HIV/AIDS,9 and went on to dedicate the next three decades of his professional life to combatting AIDS.10 He has served as the founding Executive Director of the Joint United Nations Programme on HIV/AIDS (UNAIDS), as Under Secretary-General of the United Nations, and as the Associate Director of the World Health Organization’s Global Programme on AIDS.11
Given the current Ebola outbreak in West Africa and on-going battle against HIV/AIDS, the importance of assembling international experts like Dr. Piot at ASLM2014 cannot be overstated. The ASLM2014 international conference aims to address critical public health issues, serving as a forum where great minds in public health can exchange ideas, advocate for issues, share innovations, and discuss challenges and successes in emerging disease detection, treatment, monitoring and surveillance.
Travel Scholarships Allow Young Professionals to Attend ASLM2014 ASLM is excited to announce the beneficiaries of the ASLM2014 Travel Scholarship Programme. The programme provides financial assistance, on a competitive basis, for students and professionals to travel to Cape Town for ASLM’s second international conference. Each scholarship award includes the cost of conference registration, airfare, hotel stay and daily per diem. Recipients were chosen from hundreds of applicants, based on the quality and relevance of their scholarship applications and scientific abstract submissions.
Member News
9 Former UNAIDS director Peter Piot recounts his role in discovery of Ebola, AIDS. (2013, March 14). Retrieved from http://www.hsph.harvard.edu/news/features/former-unaids-director-peter-piot-recounts-his-role-in-discovery-of-ebola-aids/
10 Von Bredow, R., & Hackenbroch, V. (2014, October 4). ‘In 1976 I discovered Ebola - now I fear an unimaginable tragedy’. Retrieved from http://www.theguardian.com/world/2014/oct/04/ebola-zaire-peter-piot-outbreak
11 Plenary Keynote Speakers. (n.d.). Retrieved from http://www.aslm2014.org/ehome/65245/Keynote Speakers/
By: Rachel Crane (Editorial Team); Editor: Michele Merkel, MS (Editorial Team)
November 2014: ASLM Newsletter

5
Member News
Scholarship recipients come from a variety of countries (Ethiopia, Ghana, Guinea, Kenya, Nigeria and Senegal) and professional backgrounds, including education, research, medicine, and programme coordination. When asked about his expectations for ASLM2014, Dr. Kenneth Onyedibe, scholarship recipient and Medical Microbiologist at Jos University Hospital, Nigeria, said, “The ASLM2014 conference will bring together all the great minds in the laboratory profession, from technologists to physicians, to share ideas on topical laboratory issues as it concerns healthcare delivery. These professionals will then serve as ambassadors of positive change when they return back to their home bases.”
By attending the ASLM2014 international conference, Travel Scholarship recipients will be able to showcase their scientific findings in poster presentations or oral presentations, network with leaders in laboratory medicine, and broaden their understanding of current issues in emerging infectious diseases and diagnostics therefore.
Dr. Onyedibe went on to say that he anticipates that ASLM will improve healthcare in Africa “by encouraging unity of purpose amongst laboratorians working in the health sector and ensuring that international standards of laboratory practice becomes the order of the day in laboratories across Africa. If all laboratory medicine professionals come together and consistently deliver quality laboratory services in their various health facilities, we will inch very close to achieving most of our health targets in Africa.”
The ASLM2014 Scholarship Programme underscores the Society’s commitment to supporting African scientists, who will carry the torch for the next generation of medical laboratory services across Africa.
Ministerial Call for Action Gains Momentum ASLM2012, the Society’s first international conference, hosted in December 2012 in Cape Town, South Africa, made healthcare history when six African health ministers conducted an ministerial roundtable event and delivered a Ministerial Call for Action pledging their countries’ commitment to the advancement of laboratory medicine and diagnostics.
The roundtable participants unveiled the Call for Action following a discussion about the present situation and future goals of African laboratory services. The Ministerial Call for Action included the commitment of Minister of Health signatories to promote policy development in: 1) laboratory workforce expansion and quality improvement, 2) standardisation of regulations on diagnostics and medical devices, 3) advancement of laboratory quality management and accreditation, and 4) harmonisation of laboratory strengthening efforts across different regions and partners, including ASLM, the World Health Organization (WHO), the US President’s Emergency Plan for AIDS Relief
By: Rachel Crane (Editorial Team); Contributors: Menyeshu Hailu (ASLM) and Brooke Chateauneuf (Daktari Diagnostics); Editor: Michele Merkel, MS (Editorial Team)
November 2014: ASLM Newsletter

6
Member News
(PEPFAR), and others. The Call for Action also included a pledge to support ASLM in implementing its ASLM2020 Strategic Vision of Equity and Quality Laboratory Results for Better Disease Management for All by 2020.
Africa is currently experiencing a human resources crisis in healthcare, particularly in the laboratory field, where there is estimated to be less than one laboratory professional per 10,000 people.12 Strategies to address this human resources deficiency may include pre-service and in-service training, career development opportunities, employment incentives and retention strategies. In addition to lacking adequate numbers of trained professionals, many medical laboratories lack quality systems to ensure accurate and timely diagnosis, which may be combatted through investment in accreditation programmes. Concurrently, the rise of new diagnostic technologies at or near the point-of-care necessitates the development of policy and regulatory guidelines, as well as harmonisation approaches across the continent.
Since the ASLM2012 conference, a number of new signatories have joined the Ministerial Call for Action, including the Honourable Ministers of Health of Burkina Faso, Cameroon, Ethiopia, Malawi, Sudan, Uganda, and Zimbabwe. In signing the Ministerial Call for Action, the Honourable Ministers have attested to the importance of the medical laboratory profession, brought to light the pressing issues of laboratory systems, prioritised their engagement of laboratory systems improvement, and helped direct efforts to strengthen health systems through quality laboratory services across Africa.
For more information on the ASLM Ministerial Call for Action, please visit: http://www.aslm.org/what-we-do/ministerial-call-for-action/
.
.
By: Rachel Crane (Editorial Team); Contributor: Corey White, MPA (Editorial Team); Editor: Michele Merkel, MS (Editorial Team)
Commitments set forth in the ASLM2012 Ministerial Call for Action.
. ASLM2020 Vision: Strengthen laboratory workforce by training and certifying laboratory professionals and clinicians through standardised frameworks; transform laboratory testing quality by enrolling laboratories in quality improvement programmes to achieve accreditation by international standards; develop strong, harmonised regulatory systems for diagnostic products as defined by the Global Harmonization Taskforce; build a network of national public health reference laboratories to improve early disease detection and collaborative research.
12 SA has 90% of Africa’s internationally accredited laboratories: Expert. (2014, April 3). Retrieved October 26, 2014, from http://www.timeslive.co.za/scitech/2014/04/03/sa-has-90-of-africa-s-internationally-accredited-laboratories-expert
November 2014: ASLM Newsletter

7
Member News
ASLM Continues Commitment to Expanded HIV Viral Load Testing Though viral load testing is a powerful tool, recommended by the World Health Organization (WHO) for improving the long-term success of antiretroviral treatment (ART) for HIV, less than 20% of ART patients in Africa receive regular viral load monitoring.13 At the AIDS 2014 International Conference in Melbourne, Australia, in partnership with UNAIDS, ASLM helped to launch the Diagnostics Access Initiative, which, through plans for improved laboratory capacity, specifically set the aim of ensuring that 90% of all people living with HIV know their HIV status, that 90% of those diagnosed with HIV receive sustained antiretroviral therapy, and that 90% of all people receiving antiretroviral therapy have achieved lasting viral suppression. The assertion is that these goals can be made possible, in part, through regular viral load testing.
As a step to set priorities for increasing access to HIV viral load testing, in April 2013 ASLM hosted the Expert Consultation on Viral Load Monitoring in African HIV Treatment Programmes in Cape Town, South Africa, in partnership with the WHO Regional Office for Africa, UNAIDS, the Society for AIDS in Africa, and the Southern African HIV Clinicians Society. Participants established priorities for providing clear guidance on WHO guidelines, by which the Viral Load Monitoring in African HIV Treatment Programmes report was generated (please visit: www.aslm.org/viralload).
Recently, ASLM, in partnership with UNAIDS, WHO, the Global Fund, the Clinton Health Access Initiative (CHAI), the US President’s Emergency Plan for AIDS Relief (PEPFAR), and Cheikh Anta Diop University hosted a workshop to actualise the priorities previously set forth. In Addis Ababa, Ethiopia from 15-17 September, participants assembled to develop country-specific plans
The Diagnostic Access Initiative strives to attain the 90-90-90 targets, which were first introduced by the Joint United Nations Programme on HIV/AIDS (UNAIDS) in May 2014. Adapted from: 90-90-90 Targets. (2014). Adapted from
http://www.avert.org/90-90-90-targets.htm.
13 World Health Organization [in partnership with UNAIDS and UNICEF]. Global update on HIV treatment 2013: Results, impact and opportunities. June 2013; Retrieved from: http://www.unaids.org/en/media/unaids/contentassets/documents/unaidspublication/2013/20130630_treatment_report_en.pdf
November 2014: ASLM Newsletter

8
Member News
implementing the expansion and enhancement of viral load testing using a network model. Regional HIV treatment providers, laboratory scientists, Ministries of Health, policy makers, programme managers and implementing agencies attended the workshop and heard presentations from field experts on subjects such as: maximising efficiency of viral load testing on the structural level; improving patient care; the experiences of Uganda and South Africa in crafting strategies for expanding access to viral load testing; sample transport; WHO guidelines; and measuring the impact of strategy implementation. Participants also identified the crucial components of a sustainable viral load programme and the essential tools to be developed and shared, such as a monitoring and evaluation framework, cost frameworks, training for clinicians and nurses, and guidelines for referral systems. Each day, after the presentations, the participants broke into groups to discuss and formulate country-specific plans, and later presented them to the workshop as a whole.
At the conclusion of the workshop, participants left with a clearer sense of the technology and resources available to expand access to viral load testing programmes, and more specifically developed strategies for eventually achieving the UNAIDS 90-90-90 goals.
Participants of the September Viral Load Meeting in Addis Ababa, Ethiopia.
By: Caroline DeLuca (Editorial Team); Contributors: Ruth Girma (ASLM) and Rediet Argaw (ASLM); Editor: Rachel Crane (Editorial Team)
November 2014: ASLM Newsletter

9
New ASLM Ambassador Champions Laboratory Medicine in Central AfricaASLM recently welcomed Prof. Francois-Xavier Mbopi-Keou to the ASLM Ambassador Programme. Prof. Mbopi-Keou joins ASLM as Ambassador for Cameroon, the Central African Republic, Chad, Congo and the Democratic Republic of Congo. With over 25 years of experience in research, public health, and microbiology/virology, and as an author of more than 100 scientific papers, abstracts and book chapters, he is an expert in laboratory medicine and HIV/AIDS in Africa. More recently, Prof. Mbopi-Keou has focused his efforts on capacity building for research and public health laboratories in Africa, with the hope of equipping the region against the threat of emerging epidemics.
As an ASLM Country Ambassador, Prof. Mbopi-Keou aims to advance the ASLM2020 Vision through advocacy and facilitation of ASLM programmes in-country, promoting Society goals and activities (e.g. training and accreditation programmes) in Central Africa in partnership with regional health officials and organisations.
Prof. Mbopi-Keou serves as Professor of Laboratory Medicine, Microbiology and Infectious Diseases at the University of Yaoundé in Cameroon, and is also Head of the Division of Laboratory and Blood Safety at the Cameroon Ministry of Public Health. He is a member of several national and international professional and academic societies, and serves on technical advisory committees on laboratory medicine and HIV/AIDS. Previously, Prof. Mbopi-Keou was a Research Fellow at the London School of Hygiene and Tropical Medicine, UK, a Senior Scientist and Senior Research Fellow at the University College of London, UK, and a Fellow at Harvard University, USA.
Member News
Prof. Mbopi-Keou
By: Rachel Crane (Editorial Team); Contributors: Francois-Xavier Mbopi-Keou, PhD (University of Yaoundé) and Corey White, MPA (Editorial Team); Editor: Michele Merkel, MS (Editorial Team)
November 2014: ASLM Newsletter

Abbott RealTime mSystems
AM
D-0
0002
531
– 10
/201
4
Abbott GmbH & Co. KG Max-Planck-Ring 2 65205 Wiesbaden, Germany Tel. (+49) 61 22 58 0 Fax (+49) 61 22 58 12 44 www.abbottmolecular.com
The right solutions for your growing lab• Broad Menu
• Increased Flexibility
• High Confidence
• High Efficiency
The performance you need. Now.

11
Member News
ASLM Laboratory Strengthening Roadmap to Fulfill National Health Priorities Laboratory test results are a cornerstone for informing clinical decisions about a patient’s diagnosis, treatment and outcomes. According to estimates from the World Health Organization Regional Office for Africa (WHO-AFRO), in Africa there is approximately one microscopy laboratory per 93,000 people, and one (bacterial) culture laboratory per 7.2 million people (2010)14 for such decision-making. With so much at stake, especially during this time of emerging zoonotic disease epidemics and increased drug resistance, it would be hazardous to allow deficiencies in the laboratory healthcare system to misdiagnose illnesses, denying patients of critical life-saving treatment.
Ensuring that medical decisions regarding the combat of infectious diseases, non-communicable diseases, and healthcare-associated infections are fully informed not only leads to better patient health, but for better citizen health – culminating in better community health.
ASLM, in alignment with its mission to push forward laboratory medicine, and in collaboration with its partners, is currently involved in creating a roadmap for improving patient outcomes through robust and accurate diagnostics and laboratory processes. Such a roadmap is intended to guide governments, stakeholders and partners on the path towards realising global health priorities by providing a strategic framework and proposed action steps to meet such goals. This initiative, incorporates the commitments set forth by the International Health Regulations15, and declarations such as those formed in Abuja16 and Maputo17 and aims to provide the “how” for moving forward critical multilateral health priorities.
14 WHO AFRO Strategic Plan for Control of TB, 2013-17
15 World Health Organization, 2008. International Health Regulations (2005) Second Edition
16 http://www.unaids.org/en/media/unaids/contentassets/documents/unaidspublication/2013/JC2524_Abuja_report_en.pdf
17 http://www.who.int/diagnostics_laboratory/Maputo-Declaration_2008.pdf
November 2014: ASLM Newsletter

12
Member News
As a foundation for laying the framework are the core pillars of the ASLM2020 vision: Strengthening the workforce in laboratory diagnostic capacity; transforming the quality of diagnostic testing to achieve accreditation by international standards; raising regulatory standards for diagnostic products to international levels; and building a network of laboratories to improve disease detection and collaborative research. ASLM has engaged numerous stakeholders, collaborating centre leaders, and ministry officials for planning and strategic working meetings as part of the roadmap development process. In September in Addis Ababa, ASLM hosted a laboratory human resources for health (LHRH) meeting, in which key country and regional partners came together for a consultation on laboratory workforce strengthening and harmonisation. Additionally, twenty experts from key areas met to discuss the roadmap framework. ASLM will continue to convene stakeholders to review and develop this plan. As a result of these activities, a clear, prioritised roadmap of strategic and actionable items will be produced.
For those attending the ASLM2014 conference, please be sure to participate in the roadmap discussions.
WHO laboratory strengthening is guided by six IHR goals. Adapted from: WHO IHR (2005). Retrieved from: http://www.who.int/ihr/about/en/
By: Michele Merkel, MS (Editorial Team); Editor: Caroline DeLuca (Editorial Team)
November 2014: ASLM Newsletter

13
Member News
ASLM and EDCTP Partner to Support Laboratory AccreditationIn sub-Saharan Africa, with the exception of South Africa, fewer than 50 medical laboratories are accredited according to international standards, almost none of which are public laboratories. In 2009, the World Health Organization, Regional Office for Africa (WHO-AFRO) established the Stepwise Laboratory Quality Improvement Process Towards Accreditation (SLIPTA), a guide for gradually achieving the criteria for regional and international accreditation. To aid more laboratories in following SLIPTA to improve quality of care and get on track for accreditation, ASLM is forging a partnership with the European and Developing Countries Clinical Trials Partnership (EDCTP).
Europe launched EDCTP in 2003 as an attempt to help tackle the three major poverty-related diseases of HIV/AIDS, tuberculosis, and malaria, which together claim 3.5 million lives each year18, disproportionately affecting sub-Saharan Africa. EDCTP supports projects in sub-Saharan Africa that combine clinical trials, capacity building, and networking in order to advance the development of new or better drugs, vaccines, microbicides and diagnostics against the aforementioned diseases. ASLM plans to support 16 EDCTP-funded laboratories in the building and applied use of quality management systems (QMS), so as to bolster their efforts in following the WHO-AFRO SLIPTA. These efforts will improve efficiency and competence in laboratory structure, as well as enhance participating laboratories’ ability to meet client needs through high-quality services.
ASLM provides partnership opportunities in strengthening laboratory programming due to its access to regular technical assistance and programme reviews from partners; support from international organisations like the US Centers for Disease Control and Prevention (CDC), the US President’s Emergency Plan for AIDS Relief (PEPFAR), the United Nations (UN), and WHO, as well as from African Ministers of Health, many of whom signed the ASLM2012 Ministerial Call for Action in Cape Town, South Africa. ASLM has also trained 123 auditors from eight African countries over the past two years, who are now available to assess the QMS of African laboratories and assist them in the accreditation process.
ASLM plans to support the EDCTP-funded laboratories through mentorship and continuous technical support, and to address crucial deficiencies in capacity to prepare laboratories for future accreditation. For the mentorship component, ASLM will train embedded mentors – quality officers already working in laboratories – as well as four project officers, or external professionals who ASLM will hire to oversee the work of four laboratories each. The mentors will all be trained together so as to ensure collaboration and shared vision. Mentorship training will include education in biosafety, biosecurity, laboratory management and QMS.
Project officers will be based in-country, and will spend two weeks at each assigned laboratory three times per year, otherwise communicating with laboratory management remotely. An ASLM Senior
18 The Organisation - EDCTP. (2003, January 1). Retrieved October 14, 2014.
November 2014: ASLM Newsletter

© 2014 Alere. All rights reserved. The Alere Logo and Alere are trademarks of the Alere group of companies. 120001501-01 10/14
Alere™ q HIV-1/2 Detect for Early Infant Diagnosis is a revolutionary point of care nucleic acid amplification test for the detection of HIV-1 and HIV-2.To learn more from Key Opinion Leaders on their experiences evaluating Alere™ q, visit alerehiv.com.
Alere™ q HIV-1/2 Detect available for Investigational Use Only (IUO). Product availability varies by region.
14
Member News
Specialist will visit each laboratory twice a year, running SLIPTA assessments, identifying shortcomings and making recommendations for addressing gaps, and helping to create implementation plans. In turn, the laboratory management will periodically evaluate the mentors and project officers. Together, based on the results of SLIPTA checklists, the mentors and officers will create plans of action for each laboratory, taking each one closer to stronger infrastructures, more effective services for patients, and international standards of practice.
By: Caroline DeLuca (Editorial Team); Contributor: Corey White, MPA (Editorial Team); Editor: Michele Merkel, MS (Editorial Team)
November 2014: ASLM Newsletter

15
Industry Focus
Smartphone Technology to Bolster Infectious Disease Surveillance A patient presents to the healthcare facility with prolonged fever and chills. Within moments of diagnosis using a rapid-test for malaria, the results are disseminated to health officials 200 kilometres away who are able to track the prevalence of malaria in real-time. This, made possible with a smartphone and cloud-based programming, is an initiative that researchers have been developing in order to maximise disease management in resource-limited settings.
Such a system could prove especially important for enhancing quality and timeliness of surveillance methods. For example, as data accumulates into the electronic system, they can be monitored for suspicious activity (high rates of positive test results) in order to detect disease outbreaks. This data can also be used to inform evidence-based decision making at the policy level.
In the last decade, scientists have invented rapid-result diagnostic tests (RDTs) for infections including HIV, malaria, dengue, and hepatitis B. However, even with the use of RDTs, there are still problems in regards to reporting and aggregating result data. Excessive paperwork is time-consuming and inefficient. Possible solutions to these problems include using diagnostic methods
that conform to WHO’s ASSURED criteria; enforcing adequate QA systems; providing better training; and utilising information technology.
In response to these needs, GSID, working with the University of Washington (Seattle, WA, USA) and the social enterprise Dimagi (Boston, USA), has created ground-breaking new software for Android smartphones to read, digitise and transmit point-of-care (POC) diagnostic results for significant infectious diseases. Workers in healthcare worldwide will have quick and accurate diagnoses for their patients, and public health officials will be able to view real-time results and analysis compiled data using a secure, cloud-based database. The system will be a crucial step for patient care, health system evaluation, and global disease surveillance and control efforts.
Along with being easy to utilise, the system allows healthcare workers to capture the results of various POC tests with an Android phone camera, and submit it instantaneously to a central web database for public health officials, which is secured or accessed according to national regulations and guidelines.
Ian Francis of Global Solutions for Infectious Diseases (GSID) and Dr. Haynes Sheppard, GSID consultant, describe a proof-of-concept study conducted in late 2013: In partnership with Zimbabwe Ministry of Health and Child Care and funded by Econet Wireless Zimbabwe, GSID trained over 60 healthcare
Smart phones can be used to capture and report data from the point-of-care, which can help improve patient care, surveillance and monitoring, logistics
and supply chain management, programme management and market opportunities. Adapted
from: “The GSID System: Real-Time Data From the Point of Care,” Haynes Sheppard, Ian Francis.
November 2014: ASLM Newsletter

16
Industry Focus
workers in the Manicaland province – at a provincial hospital, two district hospitals, and two rural health centres – to use the GSID System for HIV and malaria RDT tests, providing a phone for each department in hospitals performing tests. After two months, the GSID system had collected demographic data and images for 2,500 test results, and officials were able to identify and correct any inaccurate readings. One of the primary goals of the study was to determine the equivalency between reading tests with the software and trained healthcare workers reading the test without software. Sheppard states, “There was excellent agreement between the visual interpretations by the nurses versus the RDT reader.” Programme training for healthcare workers took less than an hour, and data entry took about 90 seconds per result. Those trained reported that the smartphone RDT reader was easy to learn, user-friendly, beneficial, and non-disruptive to their work flow.
A benefit specific to the GSID system is that it has a universal approach to reading RDTs from multiple manufacturers, so healthcare providers can pick tests that suit their needs and budgets. This flexibility will also allow the system to expand as new tests are developed, including RDTs Ebola that are currently in accelerated development. The reader software will establish a standardised interpretation of results to guide the diagnostic and treatment path for patients, also helping to monitor disease outbreaks or new health threats. Eventually, GSID will incorporate already-existent test results from diagnostic devices and POC laboratory management systems. GSID will also help local healthcare workers and caregivers to incorporate this new database system into local healthcare systems and record-keeping.
The next steps GSID has planned are to ameliorate any issues discovered in the test data, to run a bigger, province-wide study, and to determine how to link the data with national systems and solve data transfer issues. “Our reader stands out in a number of ways,” Sheppard says, “…next, we plan to demonstrate both scale and value within Zimbabwe ... and then our goal is to implement our system in other countries around Africa.” GSID is also working to garner interest and support from international public health organisations for broader implementation.
By: Caroline DeLuca (Editorial Team); Contributors: Sheppard Haynes, PhD (GSID) and Ian Francis (GSID); Editor: Rachel Crane (Editorial Team)
November 2014: ASLM Newsletter

17

18
Feature Article
Infectious Disease Surveillance in Times of Calm and in Times of Storm
No individual doctor, nurse, clinical laboratory professional, or healthcare worker, no matter how dedicated, can single-handedly stop an epidemic. Solving the problem of disease at a population level requires coordinated, population-wide understanding of and response to the disease. To build this broader understanding, countries rely on surveillance systems. Surveillance programmes are designed to detect, verify, report and respond to new cases of diseases of concern, on the principle that the more thoroughly we understand a disease, the more effectively it can be combated.
As the key agents that confirm diagnoses and transfer this information from the point of patient care to the Ministry of Health (MOH), laboratories play a central role in many surveillance activities. To find out more about how surveillance works outside the laboratory, Lab Culture spoke to three epidemiologists who are national coordinators of surveillance programmes for established and emerging infectious diseases (EIDs). Dr. Akin Oyemakinde of Nigeria is the Chief Consulting Epidemiologist at Nigeria’s Center for Disease Control and a Programme Director at the MOH. Ms. Semá Baltazar is the Head of the Surveillance Department at the Mozambique National Institute of Health. Mr. Zephania Irura of Kenya is the Focal Laboratory Person in the Department of Disease Surveillance and Response at the Kenya MOH. Lab Culture also spoke to Dr. Angela Amayo, Associate Professor Department of Human Pathology (Clinical Chemistry Unit), University of Nairobi, who is also an Honorary Consultant in Laboratory Medicine at Kenyatta National Hospital.
It is imperative to know as much as possible about the disease burden and how it changes over time. However, if every laboratory technician and doctor filed a separate report for every case of every disease they diagnosed and treated, resource-limited healthcare systems would collapse under mountains of data, not to mention expense. In order to be productive rather than overwhelming, surveillance systems have to be designed with care: clear about a country’s disease priorities, clear about the case definition for a disease, and efficient in analysing the information gathered and directing resources to respond.
There are many approaches to gathering diagnostic and epidemiological information. Diagnoses of a specific disease may be reported in the aggregate over a set time period, or immediately each time they are confirmed; reporting parties may include clinics, hospital laboratories, community health workers; and reporting may be practiced either country-wide or at selected “sentinel sites,” among other strategies. MOHs use this information to create and revise policies aimed at bringing the disease burden down to an acceptable level.
November 2014: ASLM Newsletter

19
Feature Article
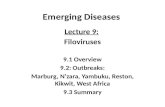
Active Data is forwarded routinely, without a data request
Someone reviews records to identify suspected cases, then requests data
Compiles data from as many sites as possible
A few selected sites report on a disease
Cases are self-reported or reported by community sources of information
Health care providers, programme managers of specific services types (ie pathology) provide data
Data from laboratory tests is obtained (e.g., diagnostic blood smears, pathogen-specific IgM antibodies)
Relies on reporting specific information (ie symptoms, demographics, risk factors, travel) for cases of illnesses
Goal is to identify illnesses early. Use existing medical data as it is obtained by the clinicians and analyse it immediatley
Community-based
Comprehensive
Laboratory-based
Passive
Health facility-based
Sentinel
Case-based
Syndromic
Description of different surveillance types
Oftentimes, in addition to passing information about disease forward to more central levels, laboratories and healthcare facilities also receive feedback reports that can help improve case management. For example, combining antimicrobial susceptibility data from many facilities in a district can help guide clinicians’ decisions about an appropriate course of treatment for cases in that region. Furthermore, knowing what diseases are at work in a given region at a given time can heighten doctors’ awareness of possible diagnoses.
Disease-specific surveillance: Many goals, many approaches
All surveillance networks share the overarching goal of situational awareness, or knowing the health status of a population over time, especially as outbreaks evolve and responses go into effect. What is to be done with surveillance data on specific diseases depends on the goals for disease control. Insights gained from surveillance for an entrenched epidemic such as tuberculosis (TB) may be used to direct funds to reduce the disease burden, whereas surveillance for an EID may be intended to detect and halt an outbreak.
November 2014: ASLM Newsletter

20
Feature Article
Surveillance can serve an important role in vaccination programmes
Surveillance is a powerful weapon in the fight to control or eradicate vaccine-preventable diseases. By identifying pockets of susceptible population that remain after an initial mass vaccination campaign, surveillance makes it possible to follow up with repeat vaccinations cost-effectively. This strategy of targeted revaccination is widely credited with the eradication of smallpox in the 1970s. More recently, the global polio eradication campaign continues to depend on case-based surveillance to prevent reintroduction. For example, in eastern Kenya, surveillance for acute flaccid paralysis detected 14 cases of polio in 2013, prompting a revaccination effort that reached one million children. The effort appears to have been successful; at the time of writing, Kenya has reported no polio cases in 2014 to date.19
Surveillance can also support vaccination programmes whose immediate aim is disease control rather than eradication. In Nigeria, which this year concludes a five-year campaign to vaccinate the population aged 1-30 using MenAfriVac, a heat-stable vaccine against Neisseria meningitidis A, case-based surveillance for meningitis is now standard. Dr. Oyemakinde describes a new system wherein “all States ensure laboratory confirmation” of suspected new cases of meningitis, and epidemiological data including attack rate and case fatality rate are collected automatically. Laboratory diagnoses have confirmed very low prevalence of N. meningitides A in Nigeria and other countries involved in the MenAfriVac vaccination programme.20
Often the most widespread epidemics are also most closely monitored. Surveillance can help public health officials identify the most pressing needs associated with diseases for which vaccines are a distant dream. Mozambique’s ministry of health uses two strategies for active, noncontinuous HIV surveillance. Antenatal clinic surveillance of pregnant women in 36 sentinel sites across the country occurs once every two years. ANC surveillance procedures in Mozambique are based on UNAIDS/WHO guidelines. At sentinel sites dried blood (DBS) spots are collected to be testes at central level with Enzyme-Linked Immunosorbent Assay (ELISA). UNAIDS’ final report on global HIV relies only on the dried blood spot results. Although rapid testing at the point of care is common especially in pregnancy, a recent analysis showed poor agreement between rapid testing and ELISAs carried out at the reference laboratory. An additional national the national prevalence survey measured HIV prevalence at community level in over 16,500 individuals aged zero to 64 years and assessed risk behaviours in youth, adolescents, and adults. This survey, was conducted with the support of many partners, first tested over sixteen thousand Mozambicans in 2009 and is underway again this year. This year, the survey also includes malaria and immunisation indicators.
19 Global Polio Eradication Initiative weekly report for 8 October 2014. Retrieved from http://www.polioeradication.org/dataandmonitoring/poliothisweek.aspx
20 World Health Organization, 2008. International Health Regulations (2005) Second Edition
November 2014: ASLM Newsletter

21
Feature Article
Like malaria, TB has significant geographical overlap and a high co-infection rate with HIV. The Stop TB strategy, a programme whose goal is to “achieve universal access to high-quality health care for all people with TB” and reduce the infection’s spread, lists as a high priority people infected with both HIV and TB.21 In many countries, new TB diagnoses are passively reported to the MOH by diagnosing facilities on a monthly or quarterly basis. For new tuberculosis cases, the World Health Organization (WHO) recommends that information including the results of sputum smear microscopy, information about HIV co-infection and antiretroviral therapy (ART) status, and case management records be collected and forwarded to the national TB programme. However, not every new case is reported; the WHO estimates that, while about six million cases were reported worldwide in 2012, three million new cases developed but went unreported owing to imperfect diagnostics, limited access to primary healthcare, and lack of consistent legal requirements to report new cases.22 It is important for a surveillance system to get a good estimate of its case detection rate, or CDR, the gap between the number of cases reported to the MOH and the true number of new cases. High CDR indicates both an accurate diagnostic strategy and an effective country reporting system. This number can not only tell the weaknesses of available data, but also illuminate gaps in the disease-control system.
The scope of a pathogen’s threat to public health affects the requirements for surveillance sensitivity. When resources are limited and a disease is widespread, a lower CDR may be acceptable; policy decisions can still be made based on statistically representative data. For example, in screening systems for diseases such as neonatal tetanus, where a large number of cases occurring in one place is a cause for concern, even with a relatively low case-detection rate the goal of identifying geographical regions of concern can still be met. On the other hand, in the context of an outbreak with the potential to spread, catching cases at the early stages of an outbreak, before it explodes into an epidemic, can save lives.
Surveillance and response to halt an outbreak: Emerging infectious diseases
For an established epidemic, “we already have the tools in place so that data is routinely collected and analysed. But with this system, we can also pick up new, concerning infections,” says Mr. Irura. If the concern is sufficiently great, such a finding may trigger an active surveillance response. According to Dr. Oyemakinde, the difference between surveillance for an established epidemic and an active outbreak of EID is that “while we wait for cases [caused by an established infectious disease] to be reported…for an emerging disease like Ebola, surveillance is active, [including a] search for contacts, suspects and cases.” When every missed case represents a new possible chain of transmission that may do devastating harm, many more resources are poured into the effort to contain the outbreak. Active surveillance of this scope can be very expensive, so there must be a significant threat to justify the set-up of a surveillance programme.
The first step in setting up surveillance for an EID, says Dr. Oyemakinde, “is to agree on the case definition (suspected, probable, confirmed), and then send out an alert which includes the case
21 World Health Organization Stop TB Strategy homepage. Retrieved from: http://www.who.int/tb/strategy/stop_tb_strategy/en/
24 World Health Organization Global Tuberculosis Report 2013, executive summary.
November 2014: ASLM Newsletter

22
Feature Article
definitions…with clear outlines for notification” to healthcare facilities and laboratories around the country. Sometimes case definitions change depending on context. For example, during an Ebola outbreak the WHO recommends that the definition of a suspected case be expanded from
Nigeria’s Emergency Operations Center for Ebola is a heartening example of how having a pre-existing surveillance infrastructure can give a country the capacity to deal with new challenges. The centre currently coordinating Nigeria’s Ebola operations was founded in 2012 as a command centre for polio eradication, and converted at the start of the current outbreak.23 Dr. Oyemakinde, who coordinates Nigeria’s surveillance programmes, has been involved in setting up Ebola surveillance in the country. New measures include thermal screening of incoming and out-going passengers at ports of entry, as well as enhanced surveillance at health facilities and thermal screening of suspected contacts of Ebola patients. This robust surveillance system is one of many factors that have contributed to Nigeria’s control of the Ebola epidemic.
Many of the previously described surveillance programmes monitor infectious diseases that are well known as public health threats, and that are familiar to the community and the doctors treating them. However, it can be difficult to differentiate an EID from its more common, less-virulent symptomatic look-alikes with similar symptomatic profiles. “People are trained to see a syndrome, but don’t have the capacity to distinguish” between aetiologies in a clinical setting, says Ms. Baltazar. She cites as an example a dengue outbreak detected this April as Mozambique’s MOH developed its new sentinel surveillance system for arboviruses. This was the first outbreak of dengue recorded in Mozambique since 1985.24 Although the prevalence of dengue has been on the rise worldwide, Ms. Baltazar points out that the long gap may not have been due to an absence of the virus, but rather an absence of laboratory testing, without which dengue is frequently misdiagnosed as malaria.
In such situations syndromic surveillance combined with a strong referral system may be an appropriate response. Syndromic surveillance takes advantage of the fact that many EIDs present as encephalitic or influenza-like illnesses of unexplained aetiology, or that fail to respond to normal treatments.25 Dr. Amayo says that although for now “the laboratory system is the weakest link in achieving the ideal surveillance system, especially for infectious conditions,” with limited capacity to identify many pathogens in many local laboratories, referring samples from such cases to a higher-tier laboratory with greater testing capacity is an effective workaround. Kenya’s own dengue surveillance system, established after a 2013 outbreak, operates on this framework.26
“Building surveillance has required a lot of investment in human resource and
laboratory capacity building.Ms. Baltazar, Instituto Nacional de Saúde, Mozambique”
23 “Nigeria’s actions seem to contain Ebola outbreak.” New York Times. 30th September 2014. Retrieved from: http://www.nytimes.com/2014/10/01/health/ebola-outbreak-in-nigeria-appears-to-be-over.html?_r=0
24 “Dengue in Africa,” Rosemary Sang. Accessed via TropIKA.net.
25 Paterson and Durrheim. “The remarkable adaptability of syndromic surveillance to meet public health needs.” Journal of Epidemiology and Global Health 2013 (3), 41-47.
26 Quarterly Bulletin of the East Africa Public Health Lab Network (Kenya chapter) newsletter- Issue 7, June 2013.
November 2014: ASLM Newsletter

23
The African Cholera Surveillance Network, or Africhol, which Ms. Baltazar coordinates in Mozambique, is another programme undertaking active, syndrome-based surveillance to prevent epidemics before they begin. In zones of enhanced surveillance, where there is some history of cholera, samples and information are collected for every case of acute diarrhoea meeting the case definition.
Consolidating surveillance efforts: Integrated disease surveillance and response
Although the goals for disease control are numerous and vary by disease, many surveillance systems share the same general structure, with laboratories or healthcare facilities reporting to a more central level. Notwithstanding this similarity, the first surveillance systems established tended to focus on individual diseases. Parallel surveillance programmes, with numerous disease-specific diagnosis and reporting structures, tend to multiply the administration required and limit the resources for verification of and response to reported outbreaks.27 Furthermore, they can result in warehousing of knowledge about different infections in different offices, where important connections may be missed. Therefore, in 1998 the WHO Regional Office for Africa (WHO-AFRO) introduced the concept of Integrated Disease Surveillance, which sought to bring together disparate surveillance activity within each country. Because surveillance is only the first half of responding to and managing outbreaks and longer-lasting epidemics, the framework is now called Integrated Disease Surveillance and Response (IDSR).
Mr. Irura describes Kenya’s national IDSR programme as “a plan for dedication of resources we have in the country to complementary surveillance activities,” instead of splitting these resources between many separate, redundant activities. Likewise, WHO-AFRO’s technical guidelines for IDSR are clear that IDSR’s purpose is to streamline the existing programmes, rather than to build a whole new system. The goal is to make the system more flexible, more sensitive, and closer to real-time awareness of public health concerns as they arise.
Part of dedicating resources for integrated disease response is setting clear priorities for surveillance. There are a few conditions that under the International Health Regulations must be reported to the WHO when detected; these are smallpox, poliomyelitis, human influenza caused by a new subtype, and SARS. Otherwise, countries prioritise disease surveillance at their discretion; the WHO suggests focusing on diseases that are epidemic-prone; targeted for eradication and elimination; or otherwise important for public health.
“Integrated disease surveillance is a good strategy, but it sometimes has some challenges,” says Ms. Baltazar. Concentrating resources at the same site, she says, can dramatically improve the capacity of healthcare providers at that site. On the other hand, expanding the services provided at the same site means that “in countries with limited human resources, you concentrate a lot of work on the same person,” who must report numerous cases in addition to their normal duties.
27 Nsubuga, Brown et al. “Implementing integrated disease surveillance: four countries’ experience, 1998-2005.” Global Public Health 2009
Feature Article
November 2014: ASLM Newsletter

24
IDSR also demands substantial coordination at the district and national levels, both in the development and distribution of case definitions and in the construction of systems for reporting cases. Healthcare workers need to be trained about what is a reportable case and provided with a steady supply of materials for collecting and reporting cases as they arise, and new facilities need to be enrolled in surveillance programmes. In many countries, private laboratories are separate from the national surveillance system and may not be legally required to report cases, which can lead to important miscommunications. During the Kenyan dengue outbreak first reported in March 2013, an investigation team looking for the index case found that two private laboratories in the region had diagnosed dengue as early as two months prior to the first case confirmed at the Kenyan Medical Research Institute.28 The IDSR technical guidelines published by WHO-AFRO in 2010 include suggestions for district-level coordinators of surveillance programmes to address some of these challenges.
IDSR tends to focus on diseases with epidemic potential, but it is increasingly apparent that non-communicable diseases are also a threat to public health. “We’re dealing with a double burden,” says Dr. Amayo, warning that overlooking trends in non-communicable diseases could lead to disaster in the future. Dr. Amayo will present a report on laboratory-based surveillance in Kenya at ASLM2014 (see sidebar).
On balance, however, the experts agree that integration of disease surveillance and response systems is a move in the right direction. IDSR has made surveillance more visible to governments and other funders as an important component of disease control. Involving the public as knowledgeable health informants has expanded awareness of specific epidemics and of surveillance in general. One of the greatest positive effects is in building capacity. “Building surveillance has required a lot of investment in human resource and laboratory capacity building,” says Ms. Baltazar. The returns on this investment have been substantial; Mozambique’s reference laboratory has dramatically expanded its technical abilities, all while improving data collection about the distribution and prevalence of diseases that previously went untracked. Likewise, during implementation of IDSR in Nigeria Dr. Oyemakinde
27 Quarterly Bulletin of the East Africa Public Health Lab Network (Kenya chapter) newsletter- Issue 7, June 2013.
Feature Article
“Integrated disease surveillance is a good strategy, but it sometimes has some
challenges
“There is a “team spirit,” notes Mr. Irura (Department of Disease Surveillance and Response, Kenya), among epidemiologists,
veterinarians, clinicians and others invested in public health within the IDSR framework.
”
”
November 2014: ASLM Newsletter

25
has seen great advances in case detection and reporting at the healthcare facility level. Mr. Irura and Dr. Amayo agree about laboratory capacity building, noting also that they see more capacity for mobilizing responses to concerning findings.
Most of all IDSR facilitates what Mr. Irura calls a “team spirit” among epidemiologists, veterinarians, clinicians and others invested in public health. By building a system in which all of these parties communicate about health concerns on a regular basis, integrated surveillance and response systems facilitate relationships where they can work together when the need arises. That way no individual doctor, nurse, clinical lab professional, or healthcare worker—no matter how dedicated—has to work alone, especially in times of active infectious disease outbreaks.
Feature Article
The experts who will be participating in ASLM2014 come from different backgrounds and settings, ensuring that the diversity of laboratory systems within the continent will be adequately captured in presentations and discussions. By providing a forum to speak on emerging infections, and importantly the current Ebola outbreak, lessons learned and innovations in diagnostics will be shared. There will be oral presentation tracks that focus on surveillance of EIDs and non-communicable diseases including:
• The role of laboratories in outbreak response: Participants will discuss innovations that they have embarked upon for ensuring that laboratories play a pivotal role in emergency response, via active or passive data capture and analysis.
• Laboratory-based surveillance and epidemiology: Clinical or public health laboratories produce a large amount of rich biological and demographic data on a daily basis. Participants will discuss how this passive surveillance method has provided information for detecting patterns for disease management and control.
For more information about ASLM2014 conference, Innovation and Integration of Laboratory and Clinical Systems, please visit www.aslm2014.org.
By: Laurel Oldach (Editorial Team); Contributors: Akin Oyemakinde, PhD (Center for Disease Control, Nigeria), Semá Baltazar, MPH (Departamento de Vigilância em Saúde, Instituto Nacional de Saúde, Mozambique), Zephania Irura (Ministry of Health, Kenya), and Angela Amayo (University of Nairobi, Kenya); Editor: Michele Merkel, MS (Editorial Team) and Rachel Crane (Editorial Team)
Disclaimer: The views and perspectives expressed by this article’s contributors consist of personal opinions and do not necessarily reflect the official policy or position of any agency.
November 2014: ASLM Newsletter


27
Research
ASLM2014 is a “Great Platform… to Discuss Diagnostics, Research and Capacity Building”:An Interview with Dr. Amadou Sall, Virologist and ASLM2014 Co-Chair
Amadou Sall, PhD, is a virologist and public health expert. He is the Head of the Arboviruses and Viral Haemorrhagic Fever Unit, Director of the
WHO Collaborating Centre and member of the governing board at Institut Pasteur of Dakar,
Senegal. Dr. Sall’s research focuses primarily on the ecology and evolution of arboviruses and viral
haemorrhagic fevers. He has published more than 80 papers and book chapters and has
given more than 100 scientific presentations at international meetings.
Can you tell us a little about your role at the Institut Pasteur in Dakar?
I am the Scientific Director of the Institut Pasteur, Dakar, and Director of the World Health Organization (WHO) Collaborating Centre for Arboviruses and Viral Haemorrhagic Fevers. As a WHO Collaborating Centre, nine months ago we were deployed to work on Ebola. I am currently in Guinea, where we have set up a mobile laboratory. We first arrived on 23 March to do Ebola testing, and a few days later we confirmed first case of Ebola in Conakry and also in Liberia. Currently, we are doing laboratory tests on a daily basis, and looking at samples from the different parts of the country, except for the forested areas of Guinea, where another mobile laboratory is operating. The mobile laboratory contributes to the control of the outbreak by identifying Ebola virus infected patients, and supports case management by ensuring that patients are no longer infectious before discharge. At the laboratory, I am coordinating and managing all activities in relation to the response coordinating teams. This my third term in Guinea, and the number of cases is much higher than in previous months.
In your opinion, what role should ASLM have in the Ebola outbreak?
ASLM is working to promote laboratories in Africa, which are an essential part of the health system. In Africa, there are not enough laboratory professionals, and many professionals do not have a high level of competence. ASLM can mobilise lab professionals to help fight Ebola because we need human resources. It is important to improve laboratory capacity in
the long term, and to control outbreaks at a very early stage. Helping build capacity in human resources, improving standards through accreditation, and developing laboratory tools—these are very specialised services that ASLM can offer in different parts of Africa. A more long-term goal of ASLM could be to help countries be more innovative in terms of diagnostics.
November 2014: ASLM Newsletter

28
Research
What are your principal research interests at the Institut Dakar?
My research area is arboviruses and viral haemorrhagic fevers. About half of my time is dedicated to research that focuses on understanding factors leading to virus emergence, as this is essential to better detecting and controlling viruses. Therefore, my group has projects on diagnostic tool development, virus evolution, virus vector interactions, modelling and risk assessment, and pathogen discovery. Most of our research is linked to public health actions such as surveillance and outbreak investigation, which are among the most important missions of my laboratory..
What are the major challenges to laboratory research capacity in Africa?
There are three main challenges to research in Africa. The first one is human resources, as we do not have enough qualified people to conduct research on diseases affecting our continent. The second issue is infrastructure. We need good infrastructure that adheres to international standards for research. The third issue is financial resources. Except for a few diseases, most of the research conducted in Africa is not well-funded.
These are all issues that ASLM and other pan-African organisations can help with, including mobilising countries, professionals and funding sources.
What is your role in ASLM2014, and what are your expectations for the conference?
I am the conference co-chair and speaker for ASLM2014. At the conference, I’m going to talk about Ebola and about how to use a laboratory network to build capacity and deal with this epidemic.
At the conference, I expect people to discuss how we can innovate from what is in place so far. We don’t want to do business as usual; we need to innovate and build from existing innovations that can be applied to African settings.
My expectation is to have a real integration between laboratories and clinical systems, to reshape the future of systems, and to address issues like emerging infectious diseases, malaria and neglected tropical diseases. I would like to see clinicians and laboratory professionals working hand in hand, and hope the conference will emphasize the impact of the laboratory-clinical interface. Particularly given the current Ebola outbreak, we need to promote collaboration between clinicians and the laboratory so that we can face this epidemic of unprecedented proportions.
What do you think Lab Culture readers would have to gain from attending the conference?
ASLM provides a unique opportunity and framework in Africa, gathering stakeholders from the private and public sectors of laboratory medicine to discuss diagnostics, research and capacity building.
November 2014: ASLM Newsletter

29
This year’s presentation themes are especially timely given the current Ebola outbreak. We have a fantastic schedule and scientific programme, in which high-profile experts will gather to discuss the most important topics of the moment and discuss the future. People should attend ASLM2014 and invest in future of this continent, being proactive in advancing laboratory medicine. Moreover, ASLM2014 will be hosted in Cape Town, which is a fantastic place to visit and interact with other professionals.
Is there anything else you would like to add?
There is a fantastic team that did great work to make ASLM2014 a reality. Our objective is simple: to focus on the key competencies of the laboratory, which is the weak link in the health system. ASLM is providing a great platform, but we need and encourage everyone to get involved.
Research
By: Rachel Crane (Editorial Team)
November 2014: ASLM Newsletter

30
BD Biosciences is delivering an entirely new menu of clinical products designed to precisely match the budget, throughput, and workflow requirements of clinical labs wherever they are found.
The BD FACSPresto™ Near-Patient CD4 Counter, for example, is designed to meet the needs of resource-limited settings. It weighs just under 7 kilos, can handle extreme temperature environments, can be run off AC or battery power, and is operated using graphics, making it language independent. It allows CD4 and %CD4 monitoring and hemoglobin quantification in a single test.
The BD FACSPresto performs system self-diagnosis at each startup, which takes just a few minutes. The system is designed to eliminate the need for preventive maintenance.
Our clinical solutions are designed to deliver dependable outcomes while speeding workflow, easing operation, and reducing training requirements. They reflect our commitment to live by, reach to, and measure our products and services by ever higher standards.
To learn more about the BD FACSPresto, visit bdbiosciences.com/eu/go/presto.
Solutions as unique as you.
BD, BD Logo and all other trademarks are property of Becton, Dickinson and Company. © 2014 BD23-16947-00
BD Biosciences 2350 Qume Drive San Jose, CA 95131bdbiosciences.com
BD FACSPresto™ Near-Patient CD4 CounterNow CE-IVD marked and WHO prequalified
23-16947-00b_BD-2014 Conf Ad-ASLM-halfpage.indd 1 10/16/14 4:47 PM
November 2014: ASLM Newsletter

31
Research
A comprehensive study
Through collaborative efforts, Dr. Pascale Ondoa (Amsterdam Institute for Global Health and Development), Ankie van den Broek (Royal Tropical Institute [KIT]), Christel Jansen (KIT), Constance Schultsz (AIGHD), Hilde de Bruijn (KIT/AIGHD), and with support from ASLM, analysed national health policies in 39 sub-Saharan African countries. The group performed a systematic qualitative and quantitative analysis of policies and strategies, valid as of December 2010, using 126 national documents, including ten Laboratory National Plans, 25 HRH development plans, 38 health policies and 53 disease-specific plans.31 The laboratory themes that were examined included:
• Governance• Policy, legal and regulatory frameworks• Quality assurance• Laboratory equipment and commodities• Human resources for laboratories
The national laboratory strategic plans reviewed in the study were also evaluated for adherence to the goals outlined in the Maputo Declaration32 in which governments and their partners outlined specific actions for strengthening laboratory systems in resource-limited settings.
This research culminated in an extensive report published in October 2013: Attention to Laboratory Services and Human Resources for Laboratory in Health Policies and Plans of Sub-Saharan African
This study analysed national health plans and policies from 39 sub-Saharan countries for the incorporation of laboratory-specific considerations, including human resources, with an aim to inform future laboratory policies.
29 Pre-service laboratory education strengthening enhances sustainable laboratory workforce in Ethiopia. (2013). Human Resources for Health Journal, Vol 11, No. 56. Retrieved from: http://www.human-resources-health.com/content/11/1/56
30 Governance and Human Resources for Health. (2011). Human Resources for Health Journal, Vol 9, No. 29. Retrieved from: http://www.human-resources-health.com/content/9/1/29
31 Ondoa P., Van den Broek A., Jansen C., De Bruijn H., Schultsz C. Attention to Laboratory Services and Human Resources for Health in Health Policies and Plans in Sub-Saharan African Countries. Report for the African Society of Laboratory Medicine. Amsterdam, 2013.
32 The Maputo Declaration on Strengthening of Laboratory Systems. (24 January 2008). WHO Regional Office for Africa. Retrieved from: http://www.who.int/diagnostics_laboratory/Maputo-Declaration_2008.pdf
November 2014: ASLM Newsletter
Medical Laboratories: Mapping the Landscape of National Health Policies and Plans in Sub-Saharan AfricaNational health policies and plans form a country’s strategy for moving the needle forward on progress towards improved and adequate health outcomes for the population. National commitment on health requires an understanding and examination of the current state of such programmes. Specifically, advancements in laboratory strategic planning, including laboratory human resources for health (HRH), seems to be undervalued in governance and policy making.29,30 The need for clear strategies to improve the availability and quality of the health workforce is essential for achieving the Millennium Development Goals and an AIDS-free generation.

32
Research
A view of progress towards the achievement of the Maputo Declaration
As a result of this research, it was noted that countries have taken steps to move the laboratory development agenda forward to meet the Maputo Declaration goals. Dr. Ondoa noted that now, in developing and executing national policies and plans, “major themes, like quality assurance and the reinforcement of the lab workforce, which were vague or unknown notions a few years ago, are, most of the time, taken into consideration. The laboratory workforce is no longer a neglected topic.” Additionally, laboratory planning that tackles major cross-cutting issues related to HIV, TB and malaria has progressed throughout the continent.
Countries.33 In the report, the authors describe how laboratories are discussed in national policies; explore possible barriers to the advancement of laboratory policy planning and the development of laboratory human resources; and, importantly, offer strategies for improving laboratory systems.
This report also includes the first comprehensive overview of laboratory policies in sub-Saharan Africa, taking specifically into account the HRH in policy planning for laboratory services. Results from the analysis of the commitment of governments to improving laboratory systems can shed light on critical issues, especially in the context of outbreak preparedness, antimicrobial resistance and the emergence of new diseases. Identifying the need for more regional collaboration and addressing the shortages of trained laboratory staff are preliminary steps toward helping governments effectively plan for future public health crises and challenges.
33 Attention to Laboratory Services and Human Resources for Health in Health Policies and Plans in Sub-Saharan African Countries. (2013). ANALABS report for the African Society of Laboratory Medicine.
Six calls of the Maputo Declaration on Strengthening of Laboratory Systems
November 2014: ASLM Newsletter

33
Research
Conversely, many areas of national policy documents fall short of meeting the goals of the Maputo Declaration. While some countries provide comprehensive strategies to address main key issues of the laboratory system, details on the costing, financing and execution of these strategies are often lacking (or unavailable on the Ministry websites). Secondly, gaps and shortages for human resources for laboratories remain poorly defined, due to the combined insufficiencies of data from the situation in the fields and the lack of clear job descriptions at each tier of the laboratory system. Thirdly, the private sector and the size of the population it serves is poorly described, compromising the realisation of a well-defined and effective public-private partnership.
The greatest challenge faced in this study was the scarcity of some policies and plans. It was unclear whether the documents did not exist or simply were not made available to the public.
Moving beyond policy plans
Based on the synthesis of data from 126 national documents, the authors outlined a key component for countries aiming to improve laboratory capacity: the formulation of national laboratory policy with sufficient details and linkages to other relevant policies such as health and human resources development, as an effort to highlights gaps in laboratory systems and facilitate the implementation of the strategies. This entails the incorporation of:
• Accurate situational analysis, or at the minimum a SWOT analysis, for laboratory services;• Practical monitoring and evaluation framework;• Preparation for subsequent national laboratory policies or the modification of timelines
so that laboratory goals can be linked to other long-term policies in various health and economic sectors;
• Budgetary and financial aspects of the plan should be firmly described and include the financial benefit of the strategy to better facilitate partner and donor support.
Despite the overall advancement of laboratory policy and planning throughout the continent more than a third of the countries studied are still lagging behind. These countries are mostly from West and Central francophone Africa, with lower prevalence of HIV, possibly reflecting the preferential directing of international aid to regions with larger HIV epidemics, reflects Dr. Ondoa. With the West African region experiencing the worst of the current Ebola outbreak, it is important that no geographic area be left behind in healthcare system strengthening.
National laboratory policy and plans address major laboratory themes more exhaustively and thoroughly, as compared to other type of national documents. Therefore, continuing to improve laboratory polices and plans and finding ways to engage least advanced countries will prove fruitful for providing optimal patient care and achieving the Millennium Development Goals for all countries in sub-Saharan Africa.
More information on this study will soon be available on the ASLM website, www.ASLM.org.
By: Michele Merkel, MS (Editorial Team); Contributors: Pascale Ondoa, MD, PhD (AIGHD); Editor: Jessica Fried, MPH (Editorial Team)
November 2014: ASLM Newsletter

25% of deaths worldwide are caused by infectious diseases.1
500,000 people die each year from Hepatitis C-related liver diseases.2
780,000 people die each year as a consequence of Hepatitis B.3
Viral and bacterial infections are among the leading causes of disease and morbidity worldwide and constitute an ever growing medical need. Developing countries are strongly affected, but the Western World and East Asia are also facing considerable healthcare challenges in this area. Roche focuses on discovery, research and development of new anti-infective agents, targeting both the pathogen as well as the host immune defenses. Roche Diagnostics builds on our industry-leading technology platform and on a rich legacy of research in this field to produce outstanding diagnostic solutions.
The Infectious Diseases portfolio from Roche: Covering all steps - from screening to patient management
Approved for use in blood banks: 1. Under development, 2. Clinical Chemistry assay (production by Sekisui, supplied by Roche Diagnostics), and 3. For Research use only. Please check with your local Roche representative on the availability of these assays and tests in your country.
References 1: Roche Diagnostics (http://www.roche.com/research_and_development/what_we_are_working_on/infectious_diseases.htm)Reference 2 & 3: WHO 2014 (http://www.who.int/mediacentre/factsheets/fs164/en/)
ASL
M_6
926
Roche Products (PTY) Ltd | 9 Will Scarlet Road, Ferndale, Randburg, 2125 | www.roche.co.za | [+27] 11 504 4600

35
Education and Training
A Partner Meeting to Review the Implementation of a National Strategic Plan in Angola
On the 10th of July 2014, ASLM conducted a seminar in Angola that brought together a number of partners to discuss the status of implementation of the National Strategic Plan. This meeting aimed to establish strategies to strengthen laboratory networks in order for laboratories to achieve international accreditation.
Over 60 participants attended the meeting in Luanda. Partners included, amongst others, Ministry of Health senior officials, CDC and PEPFAR technical teams, ASLM, African Field Epidemiology Network (AFENET), in-country WHO representatives, the Association of Public Health Laboratories (APHL) and the Angola Field Epidemiology and Laboratory Training Programme (FELTP).
A number of presentations were made to inform the meeting participants on the implementation of the national laboratory strategic plan towards accreditation. Discussions were held on the creation of mechanisms to strengthen the national network of laboratories. The meeting also highlighted the activities to be supported by CDC and PEPFAR within the National Laboratory Strategic plan. During the meeting, it was emphasised that one of the priorities of the Ministry of Health of Angola is the improvement of laboratory services. Additionally, ASLM, CDC and AFENET held a small meeting with the Minister of Health to discuss the way forward and supported needed to strengthen laboratory services in Angola.
Meeting held with the Minister of Health of Angola (fourth from the left) and members from ASLM, CDC and AFENET.
By: Ndlovu Nqobile, MPH (ASLM); Editor: Michele Merkel, MS (Editorial Team)
November 2014: ASLM Newsletter

36
Education and Training
ASLM Facilitates Joint SLIPTA Auditor Training and Quality Management System WorkshopIn collaboration with the US Centers for Disease Control and Prevention (CDC) and the Ministry of Health of Tanzania, a regional SLIPTA auditor training was conducted on 22-26 September 2014 in Dar es Salaam, Tanzania.
Facilitated by two senior programme specialists from ASLM, a total of 25 participants successfully completed the training to become auditors of the World Health Organization Regional Office for Africa (WHO-AFRO) Stepwise Laboratory Quality Improvement Process Towards Accreditation (SLIPTA) checklist. The 25 participants came from a variety of institutions, such as the Foundation for Innovative New Diagnostics and Global Health Care Public Foundation, and countries including namely Angola, Cameroon, Namibia, Swaziland, and Tanzania, among others.
Additionally, on 8-10 October, ASLM and the Clinical and Laboratory Standards Institute (CLSI) conducted a Quality Management System (QMS) workshop for Laboratory Leadership in Namibia. The objectives of the training were to sensitise managers on QMS, and provide them with the tools to implement QMS programmes such as the ISO1589 standard, Strengthening Laboratory Management Toward Accreditation (SLMTA) and SLIPTA. Twenty-five participants from the Ministry of Health and Social Services (MOHSS) Namibia, CDC and laboratory and quality managers from laboratories and universities in Namibia, participated in the training.
Such training activities, which have resulted, cumulatively, in the training of over 150 laboratory auditors, form a cornerstone of ASLM activities for advancing laboratory medicine through transforming the quality of testing. As more laboratories undergo official SLIPTA audits, laboratory staff are able to systematically track improvements, ultimately leading to better laboratory services for their clients.
Participants of the September ASLM/CDC/Ministry of Tanzania WHO-AFRO SLIPTA Auditor Training.
By: Ndlovu Nqobile, MPH (ASLM) and Michele Merkel (Editorial Team); Contributor: Talkmore Maruta, MPH (ASLM)
November 2014: ASLM Newsletter