Roadmapsbahc.org.sa/ISCIC_Sessions_2014/ISCIC_Workshops/3_Workshop edelle.pdf · Conforto et al. J...
38
1 Advanced rehabilitation strategies to optimize neurological recovery after SCI Edelle C. Field-Fote, PhD, PT, FAPTA Professor, Physical Therapy & Neurological Surgery Principal Investigator, The Miami Project to Cure Paralysis Roadmap: neuroplasticity and motor learning 1. What neural mechanisms underlie neuroplasticity ? 2. How does training influence neuroplasticity? 3. What is important about the type and amount of training? Contemporary Concepts in Neuroplasticity Old Views: • You are born with all the neurons you will ever have • The nervous system is a hardwired New Views: • New neurons are generated even in adults • There are new connections made between neurons • The new connections rely on training and practice Neuroplasticity • The capacity of the CNS to undergo changes in function and structure in response to use and motor learning • May be favorable or unfavorable
Transcript of Roadmapsbahc.org.sa/ISCIC_Sessions_2014/ISCIC_Workshops/3_Workshop edelle.pdf · Conforto et al. J...
1
Advanced rehabilitation strategies to optimize neurological recovery after SCI
Edelle C. Field-Fote, PhD, PT, FAPTAProfessor, Physical Therapy & Neurological Surgery
Principal Investigator, The Miami Project to Cure Paralysis
Roadmap: neuroplasticity and motor learning
1. What neural mechanisms underlie neuroplasticity ?
2. How does training influence neuroplasticity?
3. What is important about the type and amount of training?
Contemporary Concepts in Neuroplasticity
Old Views:• You are born with all the neurons you will
ever have• The nervous system is a hardwired
New Views:• New neurons are generated even in adults• There are new connections made between
neurons• The new connections rely on training and
practice
Neuroplasticity
• The capacity of the CNS to undergo changes in function and structure in response to use and motor learning
• May be favorable or unfavorable

2
Possible Mechanisms Underlying Neuroplasticity
• Altered Synaptic Efficacy– Increased/decreased excitability– Unmasking of Latent Connections
• New Connections– sprouting– synaptogenesis
• Neurogenesis
Rapid Mechanisms of Plasticity • Altered synaptic efficacy
– Changing the balance of excitatory and inhibitory connections
+
-
+
-
+ ++ ++
Rapid Mechanisms of Plasticity • Unmasking of latent connections
(silent synapses)
Telephone operators circa 1932
3
Roadmap: neuroplasticity and motor learning
1. What neural mechanisms underlie neuroplasticity ?
2. How does training influence neuroplasticity?
3. What is important about the type and amount of training?
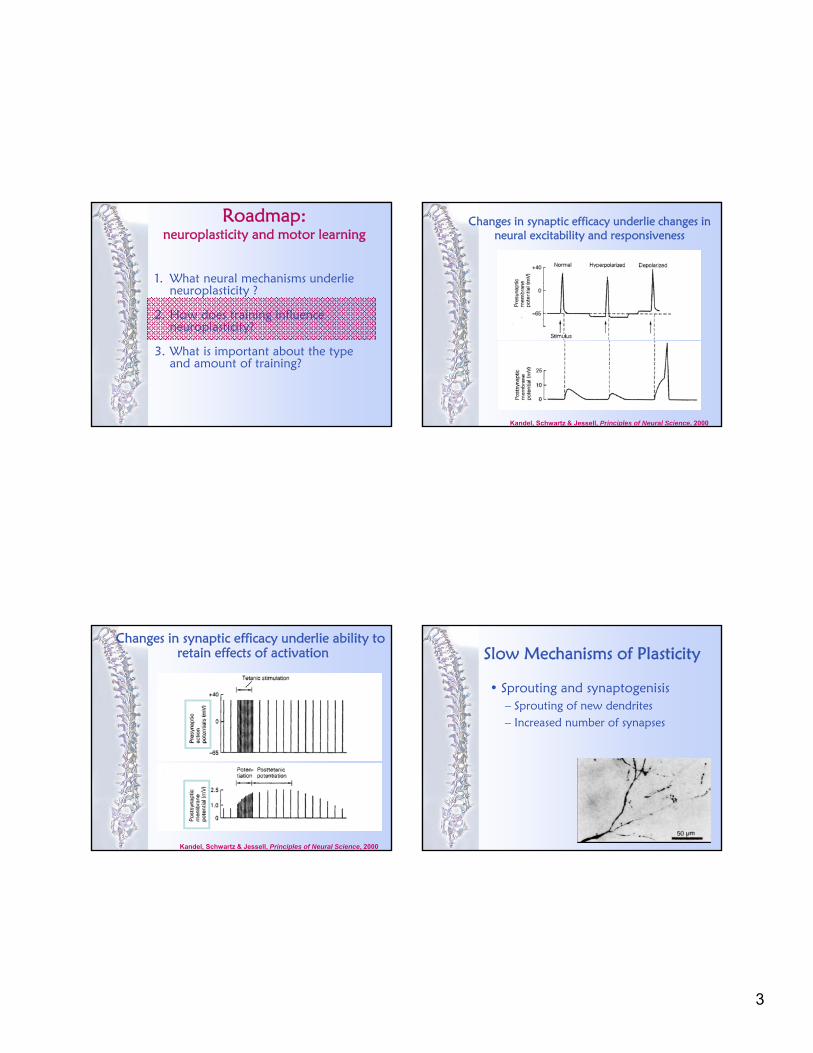
Changes in synaptic efficacy underlie changes in neural excitability and responsiveness
Kandel, Schwartz & Jessell, Principles of Neural Science, 2000
Changes in synaptic efficacy underlie ability to
Kandel, Schwartz & Jessell, Principles of Neural Science, 2000
retain effects of activation Slow Mechanisms of Plasticity
• Sprouting and synaptogenisis– Sprouting of new dendrites– Increased number of synapses

4
Neurogenesis in Humans
•Neurogenesis postnatally in:
•Hippocampus
•Subventricular Zone
•Olfactory Bulb
Running / exercise increase hippocampal neurogenesis in adult mice
van Praag, Kempermann G, and Gage. Nat Neurosci. 1999
After 12 days After 4 weeks
Walking associated with hippocampalneurogenesis in older adults
Erickson et al. PNAS. 2011
Stimulation Speaks the Language of the Nervous System
Field-Fote. Exerc Sport Sci Rev, 2004

5
Roadmap: neuroplasticity and motor learning
1. What neural mechanisms underlie neuroplasticity ?
2. How does training influence neuroplasticity?
3. What is important about the type and amount of training?
Operational premise:
The goal of therapy is to:
engage specific neural circuits in order to…
enhance the activity of those circuitsin order to…
facilitate the related motor function
Requirements for Proficient Motor Performance
–Relevant movement experience–Repetition–Neuroplasticity
6
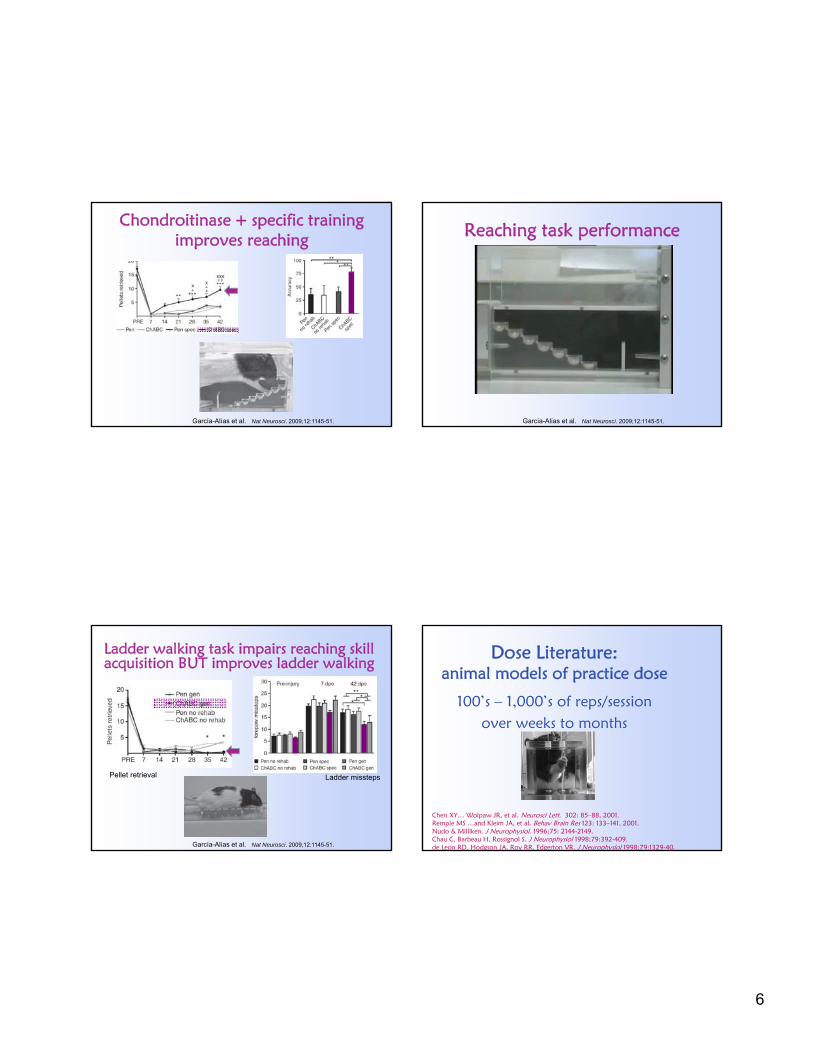
Chondroitinase + specific training improves reaching
García-Alías et al. Nat Neurosci. 2009;12:1145-51.
Reaching task performance
García-Alías et al. Nat Neurosci. 2009;12:1145-51.
Ladder walking task impairs reaching skill acquisition BUT improves ladder walking
García-Alías et al. Nat Neurosci. 2009;12:1145-51.
Pellet retrieval Ladder missteps
100’s – 1,000’s of reps/session over weeks to months
Chen XY… Wolpaw JR, et al. Neurosci Lett. 302: 85–88, 2001. Remple MS …and Kleim JA, et al. Behav Brain Res 123: 133–141, 2001.Nudo & Milliken. J Neurophysiol. 1996;75: 2144-2149.Chau C, Barbeau H, Rossignol S. J Neurophysiol 1998;79:392-409.de Leon RD, Hodgson JA, Roy RR, Edgerton VR. J Neurophysiol 1998;79:1329-40.
Dose Literature: animal models of practice dose
7
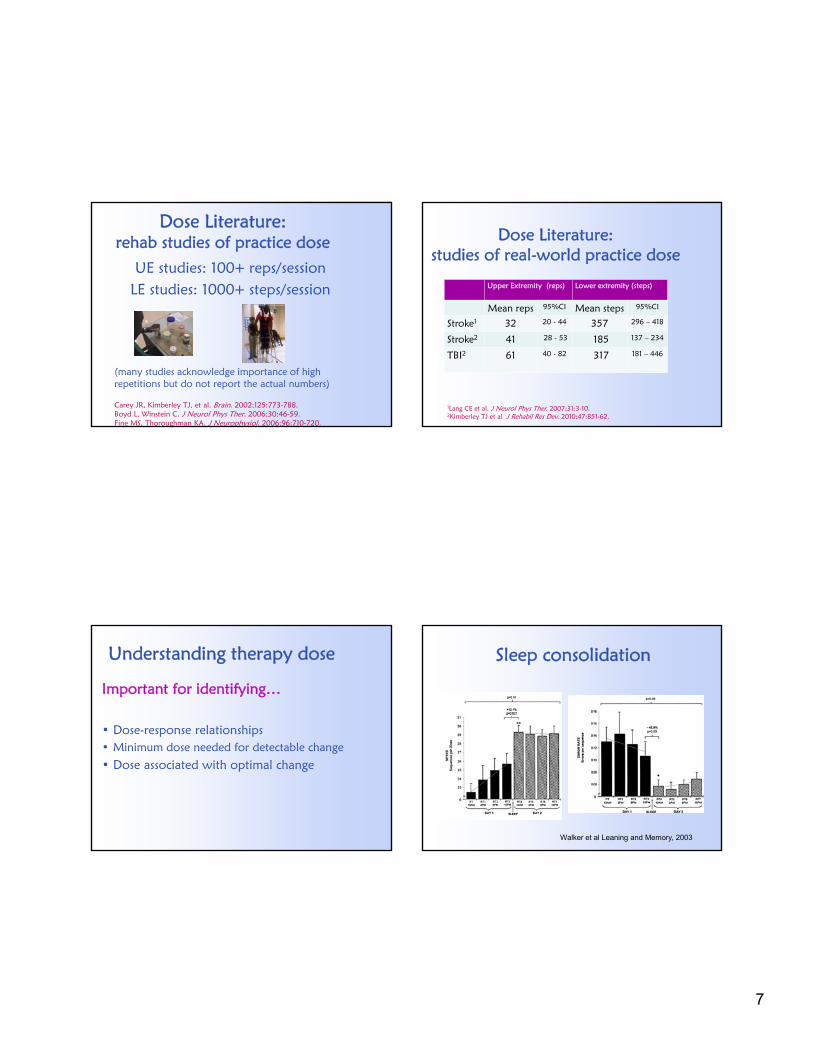
Dose Literature: rehab studies of practice dose
UE studies: 100+ reps/sessionLE studies: 1000+ steps/session
(many studies acknowledge importance of high repetitions but do not report the actual numbers)
Carey JR, Kimberley TJ, et al. Brain. 2002;125:773-788.Boyd L, Winstein C. J Neurol Phys Ther. 2006;30:46-59.Fine MS, Thoroughman KA. J Neurophysiol. 2006;96:710-720.
Dose Literature: studies of real-world practice dose
1Lang CE et al. J Neurol Phys Ther. 2007;31:3-10.2Kimberley TJ et al J Rehabil Res Dev. 2010;47:851-62.
Upper Extremity (reps) Lower extremity (steps)
Mean reps 95%CI Mean steps 95%CI
Stroke1 32 20 - 44 357 296 – 418
Stroke2 41 28 - 53 185 137 – 234
TBI2 61 40 - 82 317 181 – 446
Understanding therapy dose
Important for identifying…
• Dose-response relationships• Minimum dose needed for detectable change
• Dose associated with optimal change
Sleep consolidation
Walker et al Leaning and Memory, 2003

8
Roadmap: functional recovery in the upper extremity
1. What neuroplastic changes occur in the brain after CNS injury.
2. What is the evidence that training and stimulation can promote adaptive neuroplasticity?
3. What functional changes are observed with combined training and stimulation?
Unfavorable Neuroplasticity Occurs after CNS Injury
Maladaptive plasticity of the motor cortex after stroke
Nudo et al. J Neurosci, 1996
What is the source motor impairment after SCI?
Damage to descending tracts
Detrimental spinal reorganizationDamage to ascending tractsDetrimental cortical reorganization
9
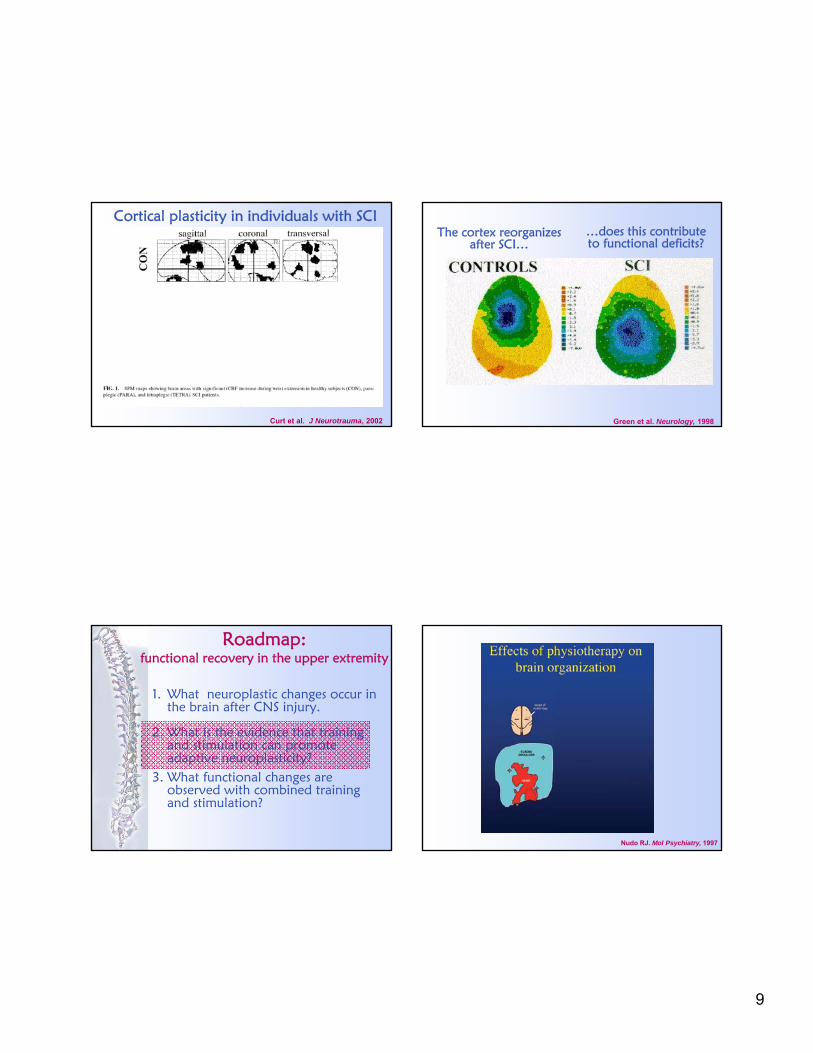
Curt et al. J Neurotrauma, 2002
Cortical plasticity in individuals with SCIThe cortex reorganizes
after SCI…
Green et al. Neurology, 1998
…does this contribute to functional deficits?
Roadmap: functional recovery in the upper extremity
1. What neuroplastic changes occur in the brain after CNS injury.
2. What is the evidence that training and stimulation can promote adaptive neuroplasticity?
3. What functional changes are observed with combined training and stimulation?
Nudo RJ. Mol Psychiatry, 1997
10
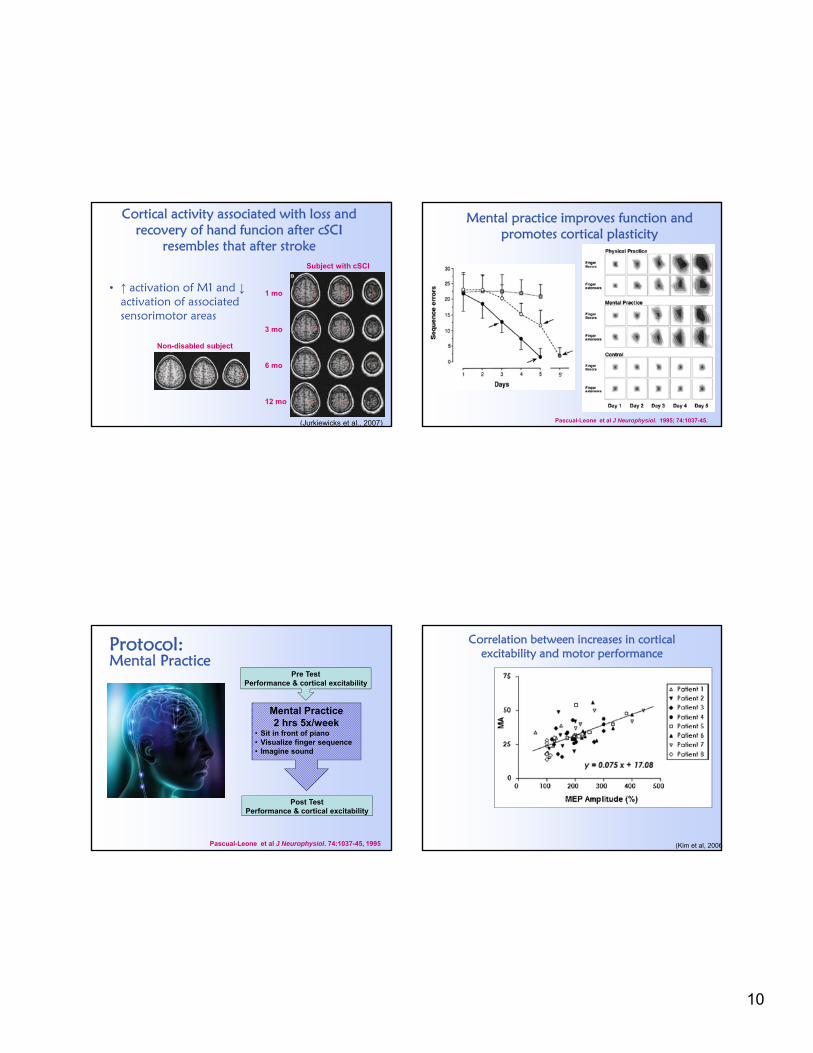
Cortical activity associated with loss and recovery of hand funcion after cSCI
resembles that after stroke
• ↑ activation of M1 and ↓activation of associated sensorimotor areas
(Jurkiewicks et al., 2007)
Non-disabled subject
Subject with cSCI
1 mo
3 mo
6 mo
12 mo
Mental practice improves function and promotes cortical plasticity
Pascual-Leone et al J Neurophysiol. 1995; 74:1037-45.
Protocol: Mental Practice
Pre TestPerformance & cortical excitability
Mental Practice2 hrs 5x/week
• Sit in front of piano• Visualize finger sequence• Imagine sound
Post TestPerformance & cortical excitability
Pascual-Leone et al J Neurophysiol. 74:1037-45, 1995
Correlation between increases in cortical excitability and motor performance
(Kim et al, 2006
11
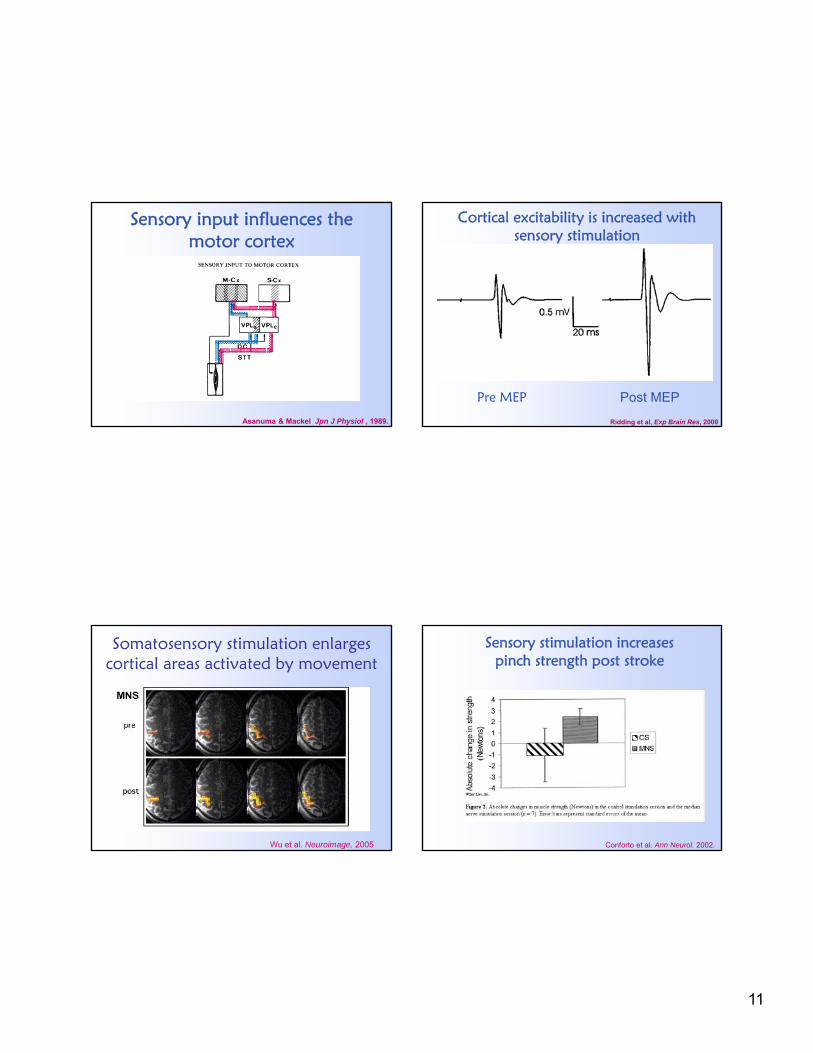
Sensory input influences the motor cortex
Asanuma & Mackel Jpn J Physiol , 1989.
Cortical excitability is increased with sensory stimulation
Pre MEP Post MEP
Ridding et al, Exp Brain Res, 2000
Somatosensory stimulation enlarges cortical areas activated by movement
Wu et al. Neuroimage, 2005
Sensory stimulation increases pinch strength post stroke
Conforto et al. Ann Neurol. 2002.
12
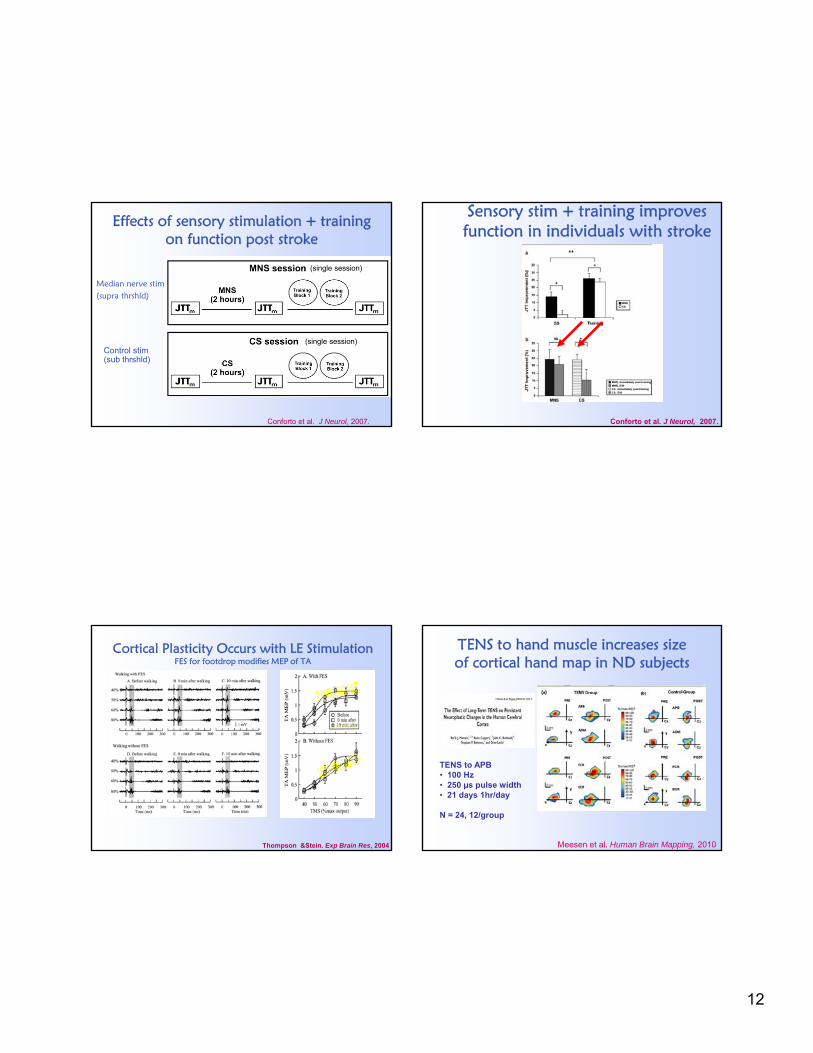
Effects of sensory stimulation + training on function post stroke
Conforto et al. J Neurol, 2007.
(single session)
(single session)
Median nerve stim (supra thrshld)
Control stim (sub thrshld)
Sensory stim + training improves function in individuals with stroke
Conforto et al. J Neurol, 2007.
Cortical Plasticity Occurs with LE StimulationFES for footdrop modifies MEP of TA
Thompson &Stein. Exp Brain Res, 2004
TENS to hand muscle increases size of cortical hand map in ND subjects
Meesen et al. Human Brain Mapping, 2010
TENS to APB • 100 Hz• 250 µs pulse width• 21 days 1hr/day
N = 24, 12/group
13
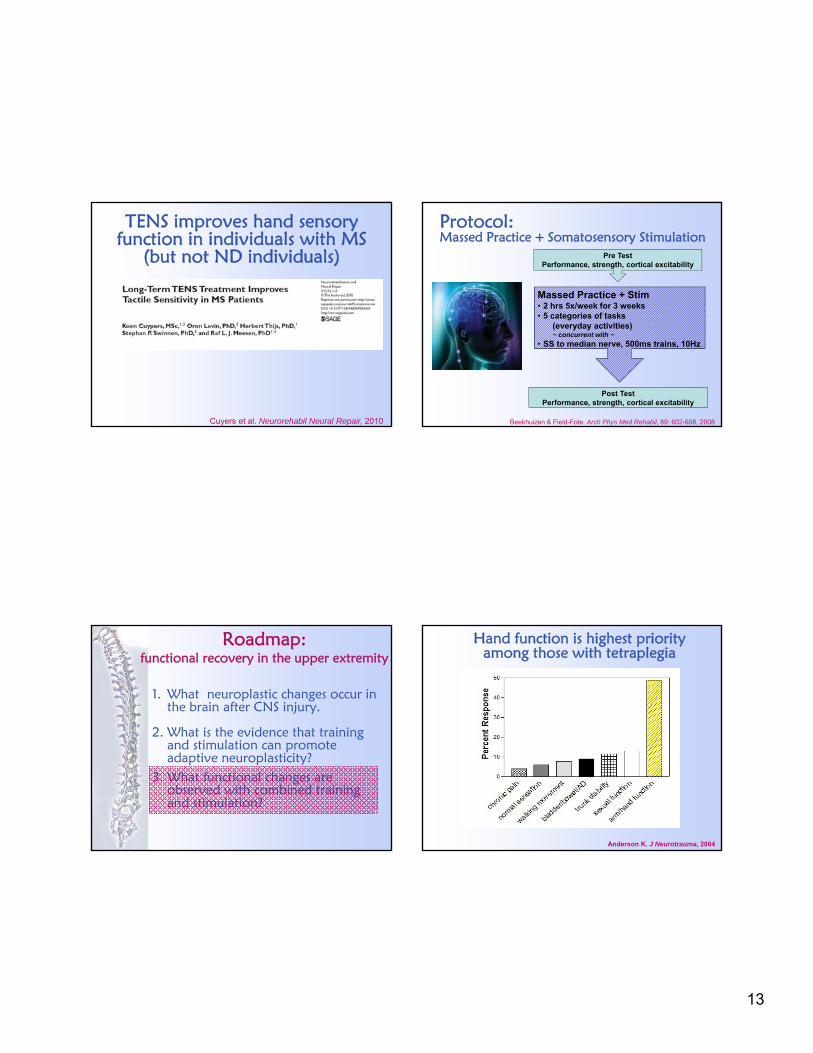
TENS improves hand sensory function in individuals with MS
(but not ND individuals)
Cuyers et al. Neurorehabil Neural Repair, 2010
Protocol: Massed Practice + Somatosensory Stimulation
Pre TestPerformance, strength, cortical excitability
Massed Practice + Stim• 2 hrs 5x/week for 3 weeks• 5 categories of tasks
(everyday activities)~ concurrent with ~
• SS to median nerve, 500ms trains, 10Hz
Post TestPerformance, strength, cortical excitability
Beekhuizen & Field-Fote. Arch Phys Med Rehabil, 89: 602-608, 2008
Roadmap: functional recovery in the upper extremity
1. What neuroplastic changes occur in the brain after CNS injury.
2. What is the evidence that training and stimulation can promote adaptive neuroplasticity?
3. What functional changes are observed with combined training and stimulation?
Hand function is highest priority among those with tetraplegia
Anderson K. J Neurotrauma, 2004

14
Gross UE Movement
Pinch
Pinch with rotation Grip with rotation
Grip
Massed practice for task-specific training effects
Beekhuizen & Field-Fote. Arch Phys Med Rehabil, 89: 602-608, 2008
Massed practice categories and sample tasks
Beekhuizen & Field-Fote. Arch Phys Med Rehabil, 89: 602-608, 2008
Task Modification for Success / Challenge
Somatosensory Stimulation Parameters• 2 hrs/day • median nerve stimulation (at wrist) • Either:
– in conjunction with MP training (MP +SS)– or alone (SS)
• Parameters: trains of stimulation– 10 Hz (500ms on / 500 ms off) – 1 msec pulse duration – Submotor threshold intensity
• (no visible thumb contraction)
• Goal: – Preferentially activate large proprioceptive
and cutaneous sensory fibers
stimulating electrode placement over the median nerve
recording electrodes over thenar eminence
Ridding et al. Exp Brain Res, 2000 (ND) Conforto et al. Ann Neurol, 2002 (Stroke)

15
Protocol: Massed Practice + Somatosensory Stimulation
Pre TestPerformance, strength, cortical excitability
Massed Practice + Stim• 2 hrs 5x/week for 3 weeks• 5 categories of tasks
(everyday activities)• SS to median nerve 500ms trains, 10Hz
Post TestPerformance, strength, cortical excitability
Beekhuizen & Field-Fote. Arch Phys Med Rehabil, 89: 602-608, 2008
Functional hand use
Beekhuizen &Field-Fote . Arch Phys Med Rehabil, 2008
Jebsen -Taylor Hand Function test
Strength
Beekhuizen &Field-Fote . Arch Phys Med Rehabil, 2008
Sensory Function
Beekhuizen &Field-Fote . Arch Phys Med Rehabil, 2008
16
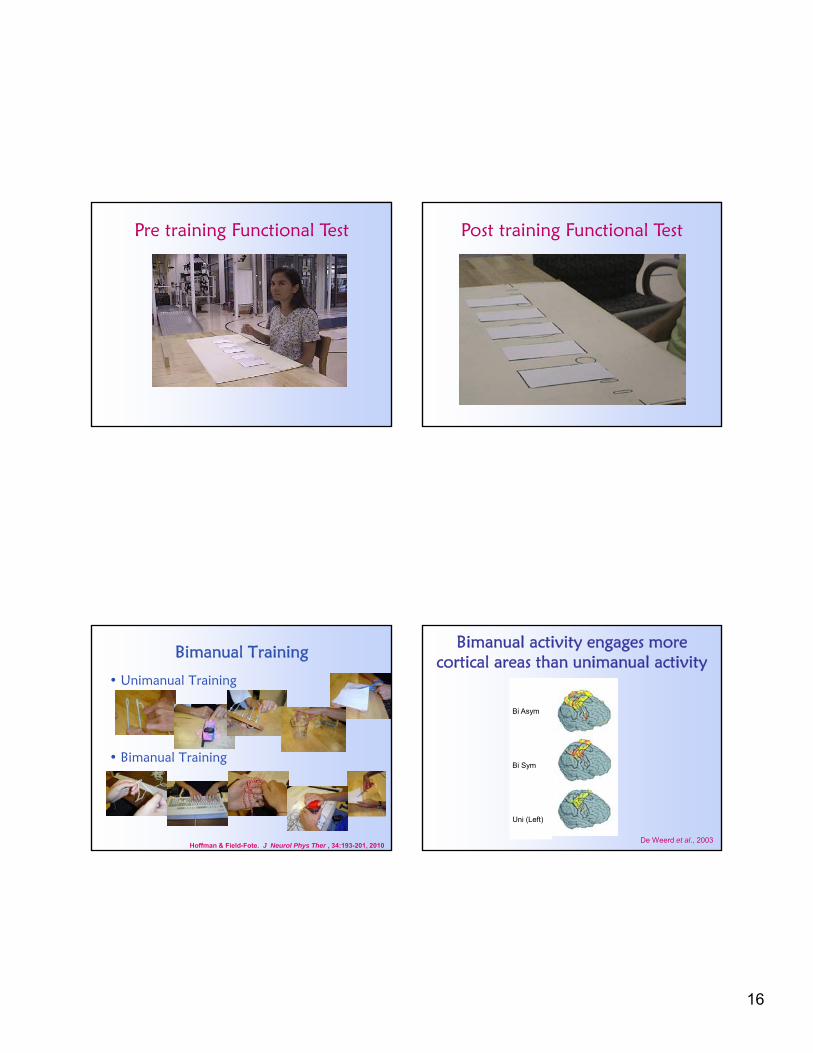
Pre training Functional Test Post training Functional Test
• Unimanual Training
• Bimanual Training
Bimanual Training
Hoffman & Field-Fote. J Neurol Phys Ther , 34:193-201, 2010
Bimanual activity engages more cortical areas than unimanual activity
De Weerd et al., 2003
Bi Asym
Bi Sym
Uni (Left)

17
Rationale: unilateral arm use is associated
with inhibition of the inactive cortex
INHIBITION↓EXCITATION↑
(Mc Combe & Waller, 2008)
ACTIVECORTEX
(UNI)
INACTIVECORTEX
(UNI)
BILATERALBASELINE
but…
bilateral arm use is associated with bihemispheric excitation
(Mc Combe & Waller, 2008)
BILATERALBASELINE ACTIVECORTEX
(UNI)
INACTIVECORTEX
(UNI)
EXCITATION↑ EXCITATION↑
Unimanual hand function outcomes
Hoffman & Field-Fote. J Neurol Phys Ther , 34:193-201, 2010
bimanual hand function outcomes
Hoffman & Field-Fote. J Neurol Phys Ther , 34:193-201, 2010

18
TMS cortical mapping to assess cortical plasticity Cortically Evoked Potentials after SCI
11 2233 11 2233
2
1
0
-1
-2
VA
DC
1
2
10
5
0
-5
-10
VA
DC
7
8
Keyboard9
-0.02 -0.01 0.00 0.01 0.02 0.03 0.04 0.05 0.06 0.07s
MEP at 60%MSO in ND individual
11 2211 22
2
1
0
-1
-2
V
AD
C 0
1
10.0
7.5
5.0
2.5
0.0
-2.5
-5.0
V
AD
C 7
8
-0.04 -0.03 -0.02 -0.01 0.00 0.01 0.02 0.03 0.04 0.05 0.06 0.07 0.08 0.09 0.10
MEP at 90% MSO in individual witincomplete cervical SCI
Sample Thenar MEP at 88% MSOPre-training
Post-training
The cortex reorganizes after SCI…
Green et al. Neurology, 1998
…does this contribute to functional deficits?

19
Subject with incomplete C5 injury
Green JB et al. Neurology,1999.
Plasticity of the Motor Map Accompanying Recovery of Function Following SCI
Cor
tical
Map
ping
Hoffman & Field-Fote. Phys Ther, 2007
Cortical stimulation as an intervention
Biophysics of TMS

20
rTMS in SCI and ND
• High frequency (excitatory) rTMS– Direct cortical activation – Elicits motor response
(Pascual-Leone, 1994; Beradelli et al, 1998; Butefish et al, 2004; Kim et al, 2006; Tallelli & Rothwell, 2006)
Results: functional outcomes
Dashed line indicates threshold for moderate effect size
Is direct cortical activation more beneficial than indirect (somatosensory) activation ?
Transcranial direct current stimulation (tDCS)• Electrodes applied to the scalp• Simple unidirectional direct current• 1 mA current• Session time: 20 min• Mild adverse effects (itching), non-invasive, painless
Transcranial direct current stimulation (tDCS)
ANODAL CATHODAL
(Fregni & Pascual-Leone, 2007)
Lesioned hemisphere Non-Lesioned hemisphere
Polarizing currents applied to cortex modulate neuronal excitability
– Anodal = lowers threshold– Cathodal = raises threshold
Appears effective for hemiparesis
– Increase excitability of lesioned ctx
– Decrease excitability of non-lesioned ctx

21
Uni-hemispheric tDCS in stroke
Boggio et al. Rest Neurol Neurosci, 2007
Bi-hemispheric (anodal/cathodal) more effective than uni-hemispheric (ND subjects)
Vines et al. BMC Neurosci, 2008
Protocol: Transcranial Direct Current Stimulation
Pre TestFunctional hand performance
tDCS• Electrodes applied to the scalp• M1 & contra forehead (anodal ~OR~ cathodal)~OR~ M1 & ipsi forehead (anodal + cathodal)• 1 mA current• 20 min session duration• Mild adverse effects (itching)
Post TestFunctional hand performance
Boggio et al. Rest Neurol Neurosci, 2007
tDCS
• Cervical Spinal Cord Injury- Bilateral upper extremity impairment- What about bilateral excitatory
stimulation?

22
Experimental Setup• Bilateral anodal
corticomotor tDCS (1 mA, 20 min) or sham
• Outcome Measures: BT and STM tasks
Bimanual finger-sequencing scores
Rios-Gomes & Field-Fote. In review, 2013
*
Evidence suggests that stimulation can potentiate effects of motor practice…
Is there an advantage in choosing one modality over another?
VERSUS VERSUS
tDCS Vibration TENS
Methods/Research Design
MOTOR TRAINING
30 MIN BREAK
TESTING
TESTING
TESTING
SESSION
OR OR
OUTCOME MEASURES Active MEP Threshold Pinch Grip Strength Visuomotor Tracking Task 9-hole peg test
ONE SESSION PER WEEK3 SESSIONS TOTAL
23
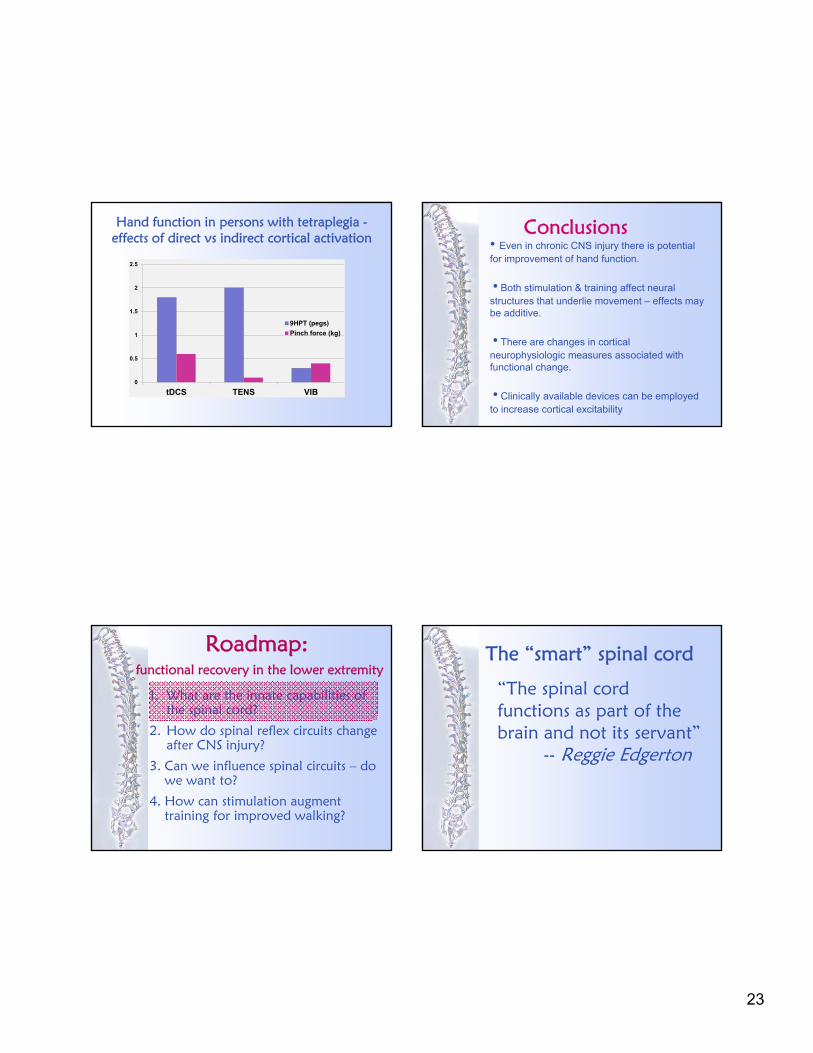
Hand function in persons with tetraplegia -effects of direct vs indirect cortical activation
0
0.5
1
1.5
2
2.5
tDCS TENS VIB
9HPT (pegs)
Pinch force (kg)
Conclusions• Even in chronic CNS injury there is potential for improvement of hand function.
• Both stimulation & training affect neural structures that underlie movement – effects may be additive.
• There are changes in cortical neurophysiologic measures associated with functional change.
• Clinically available devices can be employed to increase cortical excitability
Roadmap:functional recovery in the lower extremity
1. What are the innate capabilities of the spinal cord?
2. How do spinal reflex circuits change after CNS injury?
3. Can we influence spinal circuits – do we want to?
4. How can stimulation augment training for improved walking?
The “smart” spinal cord
“The spinal cord functions as part of the brain and not its servant”
-- Reggie Edgerton

24
Stretch Reflex H-reflex: the electrical analogue of the stretch reflex
Spinal circuits generate innate rhythmic behaviors
Hultborn. J Rehabil Med, 2003.
The Wiping Reflex of the Spinal Frog: Target-Specific Movement Trajectory. From Fukson OI, Berkinblit MB, Feldman AG. The spinal frog takes into account the scheme of its body during the wiping reflex. Science 209: 1261- 1263, 1980
Spinal Cord Performs Sensory – Motor Transformation
25
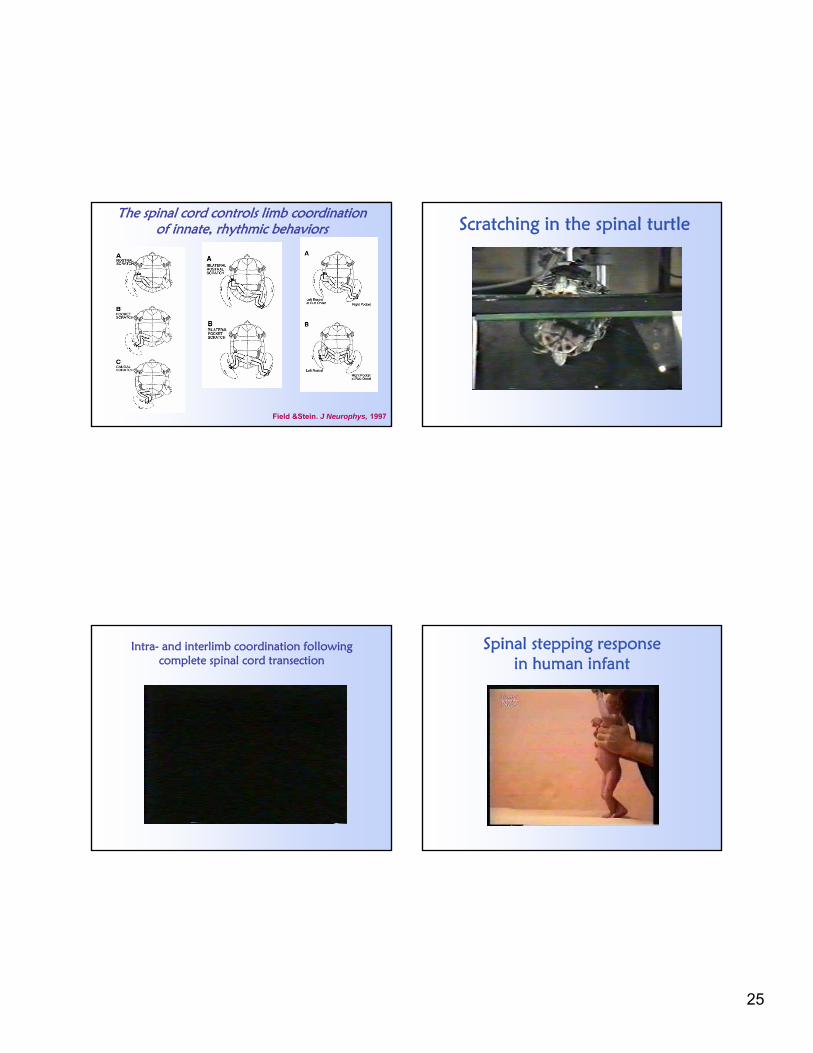
Field &Stein. J Neurophys, 1997
The spinal cord controls limb coordinationof innate, rhythmic behaviors Scratching in the spinal turtle
Intra- and interlimb coordination following complete spinal cord transection
Spinal stepping response in human infant

26
Involuntary stepping after SCI as evidence of human locomotor CPG
Similar case in: Calancie et al. Brain, 1994
Principles of motor control generalize across species
Roadmap:functional recovery in the lower extremity
1. What are the innate capabilities of the spinal cord?
2. How do spinal reflex circuits change after CNS injury?
3. Can we influence spinal circuits – do we want to?
4. How can stimulation augment training for improved walking?
Disrupted reflex modulation
27
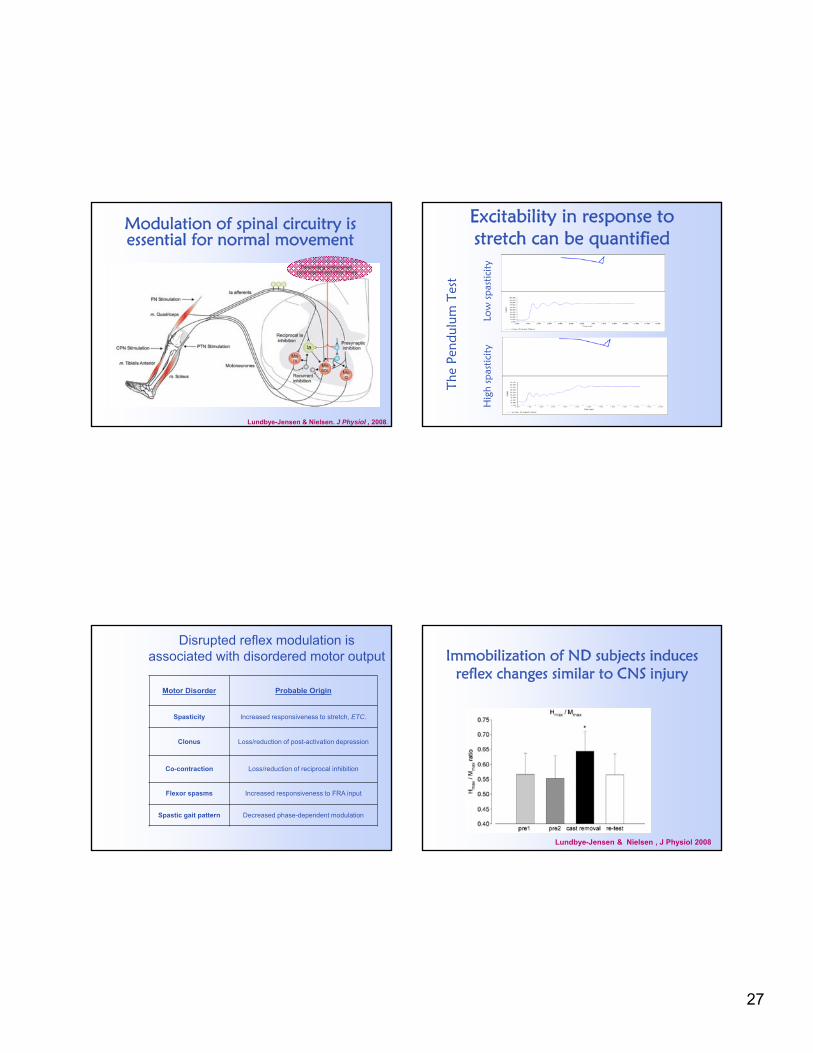
Modulation of spinal circuitry is essential for normal movement
Lundbye-Jensen & Nielsen. J Physiol , 2008.
Excitability in response to stretch can be quantified
The
Pend
ulum
Tes
t
Hig
h sp
astic
ity
L
ow
spa
stic
ity
Motor Disorder Probable Origin
Spasticity Increased responsiveness to stretch, ETC.
Clonus Loss/reduction of post-activation depression
Co-contraction Loss/reduction of reciprocal inhibition
Flexor spasms Increased responsiveness to FRA input
Spastic gait pattern Decreased phase-dependent modulation
Disrupted reflex modulation is associated with disordered motor output Immobilization of ND subjects induces
reflex changes similar to CNS injury
Lundbye-Jensen & Nielsen , J Physiol 2008

28
Spasticity during walking is correlated with severity of SCI
Fung & Barbeau J Neurophysiol, 1994
non-disabled mildly impaired moderately impaired severely impaired
Foot contact
Toe off
Roadmap:functional recovery in the lower extremity
1. What are the innate capabilities of the spinal cord?
2. How do spinal reflex circuits change after CNS injury?
3. Can we influence spinal circuits – do we want to?
4. How can stimulation augment training for improved walking?
Spinal reflexes respond to training
Wolpaw et al, Brain Res, 1983
Stimulation improves reciprocal inhibition in those with spasticity
Crone et al. Brain, 1994
● ND subjects (n =74)
o subjects with spasticity (n=39)
subjects with spasticity who used CPN stim (n=4)

29
CPN stimulation improves phase-dependent reflex modulation
Fung & Barbeau. J Neurophysiol,1994; 72: 2090-2104
■ static□ walking
Central pattern generators respond to trainingCPG plasticity
Hodgson et al Med Sci Sports Exerc, 1994
Should we train to ↓ reflexes or to ↑ voluntary control?
N =12
3 baseline sessions
12 training sessions(3/wk x 4 wks)
Manella, Roach, Field-Fote. J Neurophys. In press, 2013
Sample SOL ↓ Outcome
Manella, Roach, Field-Fote. J Neurophys. In press, 2013

30
OutcomesEMG, clinical, walking, reflexes
Manella, Roach, Field-Fote. J Neurophys. In press, 2013
Roadmap:functional recovery in the lower extremity
1. What are the innate capabilities of the spinal cord?
2. How do spinal reflex circuits change after CNS injury?
3. Can we influence spinal circuits – do we want to?
4. How can stimulation augment training for improved walking?
Approaches to locomotor training in individuals with chronic CNS injury
• Treadmill-based training with BWS• manual assisted• FES assisted• robotic assisted
• Overground training
Treadmill vs skilled overground training in chronic SCI
Musselman et al. Phys Ther, 2009
Crossover design case series: BWSTT followed by OG or BWSTT2 – 3x/week for 12 weeks
Conclusion: speed gains with skill-based OG training were greater than with BWSTT
N = 4 (8 per group)

31
Locomotor training improves walking in those with chronic incomplete SCI….
But what is the best approach
to improving walking function?
Protocol: Locomotor Training
Pre TestWalking speed & distance, reflexes, balance, etc
Randomization to 1 of 4 groups•1 hr/day •5 days/wk•12 week training
Post TestWalking speed & distance, reflexes, balance, etc
Field-Fote & Roach. Phys Ther, 91:48-60, 2011
TS
OG LR
Locomotor training improves walking in SCI – is there a “best” approach?
• Treadmill training with manual assistance (TM)
• Treadmill training with CPN stimulation assist (TS)
• Overground training with CPN stimulation assist (Walkaide II stimulator; OG)
• Treadmill training with robotic assistance (Lokomat robotic orthosis; LR)
TM
Field-Fote & Roach. Phys Ther, 91:48-60, 2011
N = 74 enrolled, 64 completed (across 4 groups)
Lokomat using passive mechanical guidance only

32
Changes in Walking Speed by Intervention Group
Sp
eed
(m
/s)
Walking speed in ND individuals is 1.2 m/s (2.7mph)
Field-Fote & Roach. Phys Ther, 91:48-60, 2011
Proportion of subjects who increased walking speed by more than .05 m/sec
Field-Fote & Roach. Phys Ther, 2011
Changes in Walking Distance by Intervention Group
Sp
ee
d (
m/s
)
Field-Fote & Roach. Phys Ther, 91:48-60, 2011
Proportion of subjects who increased walk distance by more than 2 meters
Field-Fote & Roach. Phys Ther, 91:48-60, 2011

33
Proportion of subjects who improved in distance and/or speed
Pro
po
rtio
n
What is the influence of training speed?
Training Speed
0.000.100.200.300.400.500.600.700.800.90
TM TS OG LR
Groups
Me
an
Sp
ee
d (
m/s
)
Pre Test
Post Test
Field-Fote & Lindley J Neurol Phys Ther, 2005
Pre-Intervention 2-Minute Walk Test Post-Intervention 2-Minute Walk Test
34
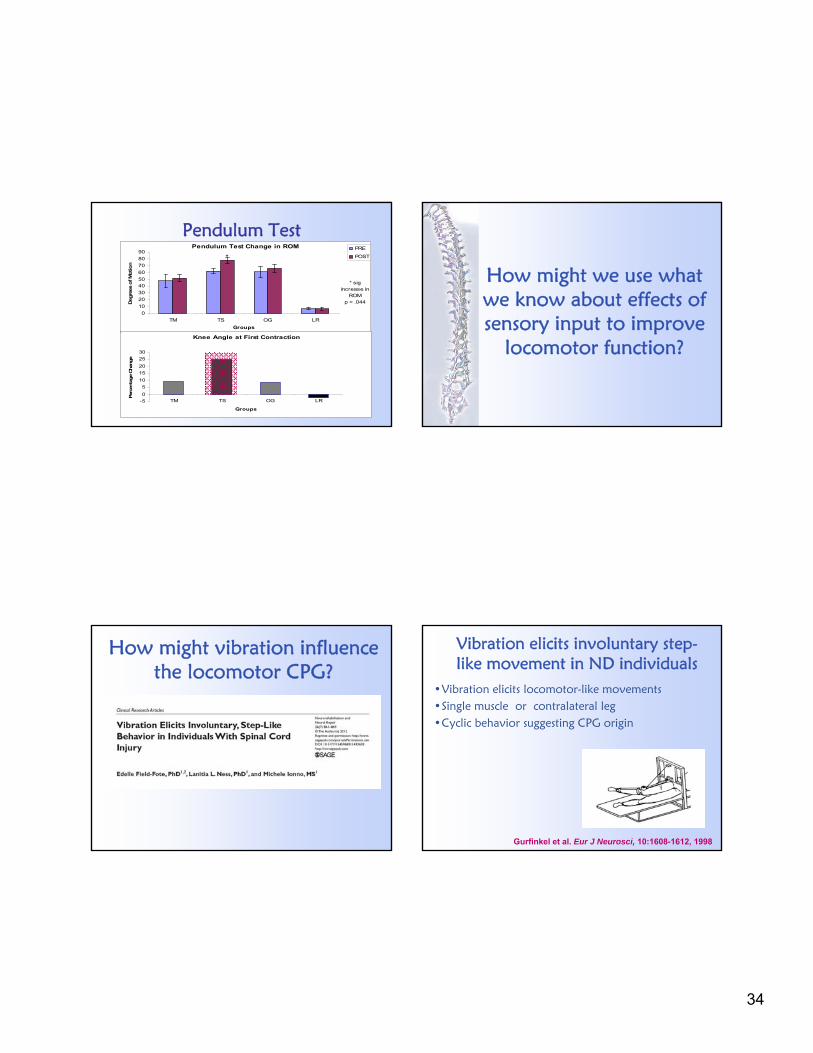
Pendulum TestPendulum Test Change in ROM
0
10
20
30
4050
60
70
80
90
TM TS OG LR
Groups
Deg
rees
of M
otion
PRE
POST *
* sig increase in
ROM p = .044
Knee Angle at First Contraction
-5
0
5
10
15
20
25
30
TM TS OG LR
Groups
Per
cen
tage
Chan
ge
How might we use what we know about effects of sensory input to improve
locomotor function?
How might vibration influence the locomotor CPG?
Vibration elicits involuntary step-like movement in ND individuals
•Vibration elicits locomotor-like movements•Single muscle or contralateral leg•Cyclic behavior suggesting CPG origin
Gurfinkel et al. Eur J Neurosci, 10:1608-1612, 1998

35
Vibration elicits involuntary stepping in individuals with SCI
Vibration: 60 Hz, ~1 mm displacement
ND Individual: Involuntary Stepping with Muscle Vibration
Field-Fote et al, Neurorehabil Neural Repair. 2012
Motor-incomplete SCI: Involuntary Stepping with Muscle Vibration
Field-Fote et al, Neurorehabil Neural Repair. 2012
Motor-complete SCI: Involuntary Stepping with Muscle Vibration
Field-Fote et al, Neurorehabil Neural Repair. 2012

36
Whole-body Vibration (WBV)
• Literature supports:– decreased spasticity in
individuals with CP (Ahlborg ‘06)
– Increased walking speed in elders and individuals with PD
(Kawanabe ‘07, Ebersbach ‘08)
– Improved balance in individuals with stroke
(van Nes, ‘04 & ‘06)
FS
E (
deg
rees
)
Ness & Field-Fote. Restor Neurol Neurosci, 2009.
WBV is associated with decreased quadriceps spasticity
WBV influences on spasticity• cumulative multi-session effects• early within-session effects • late within-session effects
FS
E (
deg
rees
)
Intervention week
Ness & Field-Fote. Restor Neurol Neurosci, 2009
WBV is associated with improved gait speed and quality
Ness & Field-Fote. Gait & Posture, 2009

37
Improved walking following 12-session course of WBV
Protocol: Whole Body Vibration
Pre TestQuad spasticity, walking speed (10m)
WBV: • Static squat• 50 Hz• low amplitude • 4x45sec – 1min rest • 3 days/week x 4 wks
Post TestQuad spasticity, walking speed (10m)
Ness & Field-Fote. Gait & Posture, 2009 (Walking function)Ness & Field-Fote. Restor Neurol Neurosci, 2009 (Spasticity)
Journey’s End1. Neural mechanisms underlying
neuroplasticity rely on changes excitability
2. Excitability is influenced by practice and by stimulation
3. Neuroplastic cortical changes appear to reflect changes in function
4. Spinal reflex and pattern-generating circuits respond training in the same way as cortical circuits
5. Combining training and stimulation may represent an optimal approach to promoting adaptive neuroplasticity
Activating the nervous system
can make a difference today

38