Ecuador - who.int · Mental Healthatlas© 2005 World Health Organization 174 E – I Ecuador...
80
174 E – I Ecuador GENERAL INFORMATION Ecuador is a country with an approximate area of 284 thousand sq. km. (UNO, 2001). Its population is 13.193 million, and the sex ratio (men per hundred women) is 101 (UNO, 2004). The proportion of population under the age of 15 years is 32% (UNO, 2004), and the proportion of population above the age of 60 years is 7% (WHO, 2004). The literacy rate is 92.3% for men and 89.7% for women (UNESCO/MoH, 2004). The country is a lower middle income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 4.5%. The per capita total expenditure on health is 177 international $, and the per capita government expenditure on health is 89 international $ (WHO, 2004). The main language(s) used in the country is (are) Spanish and Quichua. The largest ethnic group(s) is (are) Indian and Mestizo, and the other ethnic group(s) are (is) European. The largest religious group(s) is (are) Roman Catholic. The life expectancy at birth is 67.9 years for males and 73.5 years for females (WHO, 2004). The healthy life expectancy at birth is 60 years for males and 64 years for females (WHO, 2004). EPIDEMIOLOGY Aguilar (1989, 1990) conducted a study on a probabilistic random sample of 6000 individuals, representative of the country’s entire population, between the ages of 10 and 65, using questionnaires to assess the prevalence of alcohol, smoking and other illegal substance use and misuse. The rates of lifetime use reported were as follows: alcohol (75%), tobacco (54%), tranquilizers (16%), marijuana (4%), inhalants (2%), native plant drugs (1%), cocaine (1%) and cocaine base (1%). The highest prevalence of substance misuse corresponded to the consumption of alcohol and tobacco (13%), followed by tranquilizers (0.8%), opiates (0.4%), barbiturates and marijuana (0.2%) and cocaine base (0.11%). Ockene et al (1996) evaluated 800 subjects who were representative of the adult population of two cities and reported that one-third of the population smoked. Smoking was more common in males and in younger and educated subjects. Women smoked lesser number of cigarettes. Padgett et al (1998) assessed more than 2600 students from 40 communities spread across rural and urban settings. They found that 9% were current smokers and 61.1% had never smoked. Older boys and those with smokers in their families were more likely to smoke. Morillo et al (2002) conducted a population based study in Ecuador, Columbia and Venezuela to study the prevalence of erectile dysfunction (ED) in men aged 40 years and above. A 49-item questionnaire was completed by 1946 men and the age-adjusted combined prevalence of minimal, moderate and complete ED for all three countries was 53.4%, with 19.8% of all men reporting moderate to complete ED. People above 70 years and those with comorbid medical conditions suffered more compared to those below 50 years of age. Lima et al (1989, 1992) interviewed 150 patients attending a primary care centre 2 months after the 1987 earth- quake. They found emotional disturbances in 40% of the population. The risk factors were – not being married, reporting poor physical or emotional health and having ill-defined physical complaints. In a gold-mining area, Counter et al (1998 a, b) found neurocognitive deficits in village children with chronic exposure to lead because of the ceramics industry. Gorenc et al (1999) found that suicides tended to be under-reported in Mexico (42 per 100 000) and Ecuador (3.6 per 100 000), especially in men using passive or soft methods. MENTAL HEALTH RESOURCES Mental Health Policy A mental health policy is present. The policy was initially formulated in 1980. The components of the policy are promotion, prevention, treatment and rehabilitation. It was revised in 1999 by mental health pro- fessionals, civil servants and NGOs. There are no regular funds for its implementation and less than 10% of its original content was put into practice. Substance Abuse Policy A substance abuse policy is present. Details about the year of formulation are not available. There is also specific legislation for substance abuse from 1997. National Mental Health Programme A national mental health programme is present. The programme was formulated in 1980. It was revised in 1999. It was implemented less than 10.0% by regional and national authorities, probably because there was no specific budget for its implementation. Its main components are strategy of services reform, integration of mental health services at primary health care and development of specialized services. National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. It was formulated in 1977. Mental Health Legislation The Mental Health Act was revised in 2001. There are no regular funds for its implementation, and it has been implemented to the extent of 10 to 25 %. It focuses on promotion and prevention, human rights and regulation of mental health services, but there is no reference to regulation of involuntary treatment. The latest legislation was enacted in 2000. Mental Health Financing There are no budget allocations for mental health. Details about expenditure on mental health are not available. The primary source of mental health financing is out of pocket expenditure by the patient or family. The country has disability benefits for persons with mental disorders. Mental disabilities are considered disabilities under Law 180. The evaluation is done by a psychiatrist and reviewed by the National Disability Council. Chronic psychosis, mental retardation, dementia and certain epilepsies are considered for disability benefits.
Transcript of Ecuador - who.int · Mental Healthatlas© 2005 World Health Organization 174 E – I Ecuador...
© 2005 World Health OrganizationMental Healthatlas
174
E –
I
EcuadorGENERAL INFORMATIONEcuador is a country with an approximate area of 284 thousand sq. km. (UNO, 2001). Its population is 13.193 million, and the sex ratio (men per hundred women) is 101 (UNO, 2004). The proportion of population under the age of 15 years is 32% (UNO, 2004), and the proportion of population above the age of 60 years is 7% (WHO, 2004). The literacy rate is 92.3% for men and 89.7% for women (UNESCO/MoH, 2004).The country is a lower middle income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 4.5%. The per capita total expenditure on health is 177 international $, and the per capita government expenditure on health is 89 international $ (WHO, 2004).The main language(s) used in the country is (are) Spanish and Quichua. The largest ethnic group(s) is (are) Indian and Mestizo, and the other ethnic group(s) are (is) European. The largest religious group(s) is (are) Roman Catholic.The life expectancy at birth is 67.9 years for males and 73.5 years for females (WHO, 2004). The healthy life expectancy at birth is 60 years for males and 64 years for females (WHO, 2004).
EPIDEMIOLOGYAguilar (1989, 1990) conducted a study on a probabilistic random sample of 6000 individuals, representative of the country’s entire population, between the ages of 10 and 65, using questionnaires to assess the prevalence of alcohol, smoking and other illegal substance use and misuse. The rates of lifetime use reported were as follows: alcohol (75%), tobacco (54%), tranquilizers (16%), marijuana (4%), inhalants (2%), native plant drugs (1%), cocaine (1%) and cocaine base (1%). The highest prevalence of substance misuse corresponded to the consumption of alcohol and tobacco (13%), followed by tranquilizers (0.8%), opiates (0.4%), barbiturates and marijuana (0.2%) and cocaine base (0.11%). Ockene et al (1996) evaluated 800 subjects who were representative of the adult population of two cities and reported that one-third of the population smoked. Smoking was more common in males and in younger and educated subjects. Women smoked lesser number of cigarettes. Padgett et al (1998) assessed more than 2600 students from 40 communities spread across rural and urban settings. They found that 9% were current smokers and 61.1% had never smoked. Older boys and those with smokers in their families were more likely to smoke. Morillo et al (2002) conducted a population based study in Ecuador, Columbia and Venezuela to study the prevalence of erectile dysfunction (ED) in men aged 40 years and above. A 49-item questionnaire was completed by 1946 men and the age-adjusted combined prevalence of minimal, moderate and complete ED for all three countries was 53.4%, with 19.8% of all men reporting moderate to complete ED. People above 70 years and those with comorbid medical conditions suffered more compared to those below 50 years of age. Lima et al (1989, 1992) interviewed 150 patients attending a primary care centre 2 months after the 1987 earth-quake. They found emotional disturbances in 40% of the population. The risk factors were – not being married, reporting poor physical or emotional health and having ill-defined physical complaints. In a gold-mining area, Counter et al (1998 a, b) found neurocognitive deficits in village children with chronic exposure to lead because of the ceramics industry. Gorenc et al (1999) found that suicides tended to be under-reported in Mexico (42 per 100 000) and Ecuador (3.6 per 100 000), especially in men using passive or soft methods.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is present. The policy was initially formulated in 1980.The components of the policy are promotion, prevention, treatment and rehabilitation. It was revised in 1999 by mental health pro-fessionals, civil servants and NGOs. There are no regular funds for its implementation and less than 10% of its original content was put into practice.
Substance Abuse Policy A substance abuse policy is present. Details about the year of formulation are not available. There is also specific legislation for substance abuse from 1997.
National Mental Health Programme A national mental health programme is present. The programme was formulated in 1980.It was revised in 1999. It was implemented less than 10.0% by regional and national authorities, probably because there was no specific budget for its implementation. Its main components are strategy of services reform, integration of mental health services at primary health care and development of specialized services.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. It was formulated in 1977.
Mental Health Legislation The Mental Health Act was revised in 2001. There are no regular funds for its implementation, and it has been implemented to the extent of 10 to 25 %. It focuses on promotion and prevention, human rights and regulation of mental health services, but there is no reference to regulation of involuntary treatment.The latest legislation was enacted in 2000.
Mental Health Financing There are no budget allocations for mental health.Details about expenditure on mental health are not available.The primary source of mental health financing is out of pocket expenditure by the patient or family.The country has disability benefits for persons with mental disorders. Mental disabilities are considered disabilities under Law 180. The evaluation is done by a psychiatrist and reviewed by the National Disability Council. Chronic psychosis, mental retardation, dementia and certain epilepsies are considered for disability benefits.

© 2005 World Health OrganizationMental Healthatlas
175
E –
I
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is not available at the primary level. Less than 25% of the population is covered by this kind of service. Mental health care is provided by Primary Health Care doctors. A referral system is in place.Regular training of primary care professionals is carried out in the field of mental health. In the last two years, about 250 personnel were provided training. General physicians, nurses, social workers and educators are provided a 30 hour training in mental health.There are no community care facilities for patients with mental disorders. The community care system covers for one-fourth of the intended patient group. It includes preventive/promotion, home interventions and family interventions. Nurses are responsible for taking care of patients with mental disorders in the community.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 1.69Psychiatric beds in mental hospitals per 10 000 population 1.53Psychiatric beds in general hospitals per 10 000 population 0.16Psychiatric beds in other settings per 10 000 population 0Number of psychiatrists per 100 000 population 2.1Number of neurosurgeons per 100 000 population Number of psychiatric nurses per 100 000 population 0.5Number of neurologists per 100 000 population Number of psychologists per 100 000 population 29.1Number of social workers per 100 000 population 0.04
The personnel refer to those in the public sector only. Almost 50% of nurses, 80% of psychiatrists and 95% of psychologists work in the private sector.
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in prevention, treatment and rehabilitation. These organizations participate in mental health activities related to women, children and domestic violence.
Information Gathering System There is mental health reporting system in the country. Information is recorded utilizing ICD-10. The mental health components reported are morbidity, admission and discharge. Depression, suicide, psychosis, drug abuse and dependence, epilepsy, mental retardation, violence and child abuse are the conditions covered.The country has data collection system or epidemiological study on mental health. The ‘Departamento Nacional de Estatísticas’ (National Department of Statistics) is in charge of the data collection system for mental disorders. It is stated that the main psychiat-ric problems are alcohol abuse and dependence (7.4 %), affective disorders, particularly depression (approximately 16 %), psycho-social problems like domestic violence and child abuse.
Programmes for Special Population The country has specific programmes for mental health for disaster affected population, indigenous population, elderly and children. Also, there are programmes for victims of domestic violence.
Therapeutic Drugs The therapeutic drug policy was revised in 1996. An essential drug list was created in 1976 and revised in 1996. Prices of medication are subsidized.
Other Information
Additional Sources of InformationAguilar, E. (1989) Prevalence of the improper use of alcohol, tobacco and drugs in the Ecuadorian population. Boletin de la Oficina Sanitaria Panamericana, 107, 510-513.
Aguilar, E. (1990) Prevalence of the improper use of alcohol, tobacco, and drugs in the Ecuadorian population. Bulletin of the Pan American Health Organization, 24, 35-38.
Bouwen, R., Craps, M., Santos, E. (1999) Multi-party collaboration: building generative knowledge and developing relationships among unequal partners in local community projects in Ecuador. Concepts & Transformation, 4, 133-51.
Counter, S. A., Buchanan, L. H., Laurell, G., et al (1998a) Blood mercury and auditory neuro-sensory responses in children and adults in the nambija gold mining area of Ecuador. Source Neurotoxicology, 19, 185-196.
Counter, S. A., Buchanan, L. H., Rosas, H. D., et al (1998b) Neurocognitive effects of chronic lead intoxication in Andean children. Journal of the Neurological Sciences, 160, 47-53.
Gorenc, K.-D., Flores, J. A., Peredo, S., et al (1999) Unregistered suicides in Mexico and Ecuador: a comparative study. Revista Mexicana de Sociologia, 61, 123-149.
Lima, B. R., Chavez, H., Samaniego, N., et al (1989) Disaster severity and emotional disturbance: implications for primary mental health care in developing countries. Acta Psychiatrica Scandinavica, 79, 74-82.
Lima, B. R., Chavez, H., Samaniego, N., et al (1992) Psychiatric disorders among emotionally distressed disaster victims attending primary mental health clinics in Ecuador. Bulletin of the Pan American Health Organization, 26, 60-66.
Morillo, L. E., Diaz, J., Estevez, E., et al (2002) Prevalence of erectile dysfunction in Colombia, Ecuador, and Venezuela: a population-based study (DENSA). International Journal of Impotence Research, 14 (Suppl. 2), 10-18.
Ockene, J. K., Chiriboga, D. E., Zevallos, J. C. (1996) Smoking in Ecuador: prevalence, knowledge, and attitudes. Tobacco Control, 5, 121-126.
Padgett, D. I., Selwyn, B. J., Kelder, S. H. (1998) Ecuadorian adolescents and cigarette smoking: a cross-sectional survey. Pan American Journal of Public Health, 4, 87-93.
ECUADOR

© 2005 World Health OrganizationMental Healthatlas
176
E –
I
EgyptGENERAL INFORMATIONEgypt is a country with an approximate area of 1001 thousand sq. km. (UNO, 2001). Its population is 73.389 million, and the sex ratio (men per hundred women) is 100 (UNO, 2004). The proportion of population under the age of 15 years is 34% (UNO, 2004), and the proportion of population above the age of 60 years is 7% (WHO, 2004). The literacy rate is 67.2% for men and 43.6% for women (UNESCO/MoH, 2004).The country is a lower middle income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 3.9%. The per capita total expenditure on health is 153 international $, and the per capita government expenditure on health is 75 international $ (WHO, 2004).The main language(s) used in the country is (are) Arabic. The largest ethnic group(s) is (are) Arab. The largest religious group(s) is (are) Sunni Muslim (nine-tenths), and the other religious group(s) are (is) Coptic Christian.The life expectancy at birth is 65.3 years for males and 69 years for females (WHO, 2004). The healthy life expectancy at birth is 58 years for males and 60 years for females (WHO, 2004).
EPIDEMIOLOGYGhanem et al (2004) conducted a national household survey of prevalence of mental disorders in 5 governorates, using the Mini International Neuropsychiatric Interview-Plus (MINI-Plus). Almost 17% (11% to 25.4% in different governorates) of adults had mental disorders, with the common ones being mood disorders (6.4%), anxiety disorders (4.9%) and somatoform disorders (0.6%). Psychoses were seen in 0.3% of the population. Mental disorders were associated with gender (female), marital status (widow, divorced), occupation (housewife, unemployed), education (illiteracy), housing (overcrowding) and physical illnesses. Okasha et al (2001) assessed a sample of students, selected through multistage stratified random sampling with the General Health Questionnaire, the Arabic Obsessive Scale for obsessive traits and the Yale Brown Obsessive Compulsive Scale. They found that psychiatric morbidity was present in 51.7% and obsessive compulsive disorder (ICD 10) in 19.6%. Girls, younger adolescents and first-borns were likely to be affected to a greater extent. In a study on University students, Okasha et al (1985) found that almost 14% of students faced academic difficulties. Psychiatric disorders were diagnosed in 42% of male students with academic problems, compared to 9% of students with no such problems, with neuroses accounting for nearly half of the cases and schizophrenia for a quarter. Farrag et al (1988) examined 2000 elderly (above 60 years) subjects from a region in a 3-phase population-based study using a modified version of the MMSE and a standardized protocol for those who screened positive (MMSE score of 21 or below). The prevalence of dementia was 4.5% with Alzheimer in 2.2%, multi-infarct dementia in 0.9%, dementia of mixed type in 0.55% and secondary dementia in 0.45%. Age-specific prevalence tended to double every 5 years. Soueif et al (1982, 1990) reported on psychoactive drug use in a nationally representative sample (n=14 656) of male secondary school students, using standardized ques-tionnaires. They found that between 8% (for alcohol) and 21.4% (for synthetic drugs) of experimenters continued their drug use and that the age of onset was between 12-16 years. A greater proportion of urban students used tobacco, alcohol and cannabis, and delinquency was associated with drug use. In another sample (n=5530), they noted that consistently more arts stream students in comparison to science stream students were immersed in the drug culture. In similar studies, Soueif et al (1986, 1987) examined the non-medical use of drugs among university students (n=2711), using standardized tools. They found that university students were more likely to use stimulants and continue with drug use (10%-31% for different drugs) compared to male secondary school students, but the age of starting drug use was later in this sample. In comparison to male university students using drugs, female university student (n=2366) who used drugs came from a higher socioeconomic background. They were less likely to use stimulants and narcotics or to smoke, and they started drug use later (usually after 16 years). Their preferred drugs were hypnotics, tranquiliz-ers and alcohol. Nasser (1986, 1994) found lower rates of abnormal eating attitudes in college students in Cairo (12%) in compari-son to those in London (22%). In the earlier study, no Arab student fulfilled criteria for an eating disorder, but in the later studies he found a prevalence rate of 1.2% for bulimia and 3.4% for partial syndrome of bulimia (Russel’s criteria). Okasha and Lotaif (1979) estimated the rate of suicide attempts in Cairo to be 38.5/100 000 population based on their assessment of admissions for attempt-ed suicide in one hospital. Among suicide attempters, those in the age group of 15-44 years and students were overrepresented. Depression, hysterical reactions and situational reactions were common psychiatric conditions associated with suicide. Overdosing was the commonest method (80%) used. Temtamy et al (1994) administered the Stanford-Binet test to 3000 randomly selected community subjects. The prevalence of mental retardation was 3.9% (higher rates were reported in rural areas). Parental consan-guinity was established in 65%. Farrag et al (1998) assessed 2878 children from the 2nd and 3rd grades in elementary schools for their reading ability by means of standardized tests for linguistic ability and rate of letter identification. The 84 children (3%) with IQ 90 or more and no evidence of sensory or motor impairment identified as backward in their reading ability at this stage were reassessed after 3 years. Thirty seven (1%) children, who did not attain satisfactory reading skills even at this stage, were diagnosed to have specific reading disability. The male to female ratio was 2.7 to 1. Abou et al (1991) administered the Arabic version of the Children’s Depression Inventory to 1561 preparatory school children selected through stratified random sampling and found the rate of depression to be 10.3%. Further testing in sub-samples revealed that depression scores were predicted by neuroticism, introver-sion, relationship with fathers, sibs and peers, scholastic performance and mothers’ depression scores.

© 2005 World Health OrganizationMental Healthatlas
177
E –
I
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is present. The policy was initially formulated in 1978.The components of the policy are promotion, prevention and treatment. The objectives of the policy are to provide a basis for improving mental health and well-being of the population through provision of services to the population at risk, community care and family support.
Substance Abuse Policy A substance abuse policy is present. The policy was initially formulated in 1986. A President’s Decree has established a National Fund for the Control of Drug Addiction and Abuse. The supreme Council for the Control of Drug Addiction and Abuse is chaired by the Prime Minister. Laboratories for detection of addictive substances in biological secretions have been established in most regions. The policy direction is towards harm reduction policy.
National Mental Health Programme A national mental health programme is present. The programme was formulated in 1986.A new mental health programme was adopted in 2002. The programme aims to integrate mental health into community care, develop health recording and information gathering system, provide essential drugs and develop human resources. The other areas earmarked for development are quality assurance, development of intermediate and alternative systems of proving mental health care, developing child and adolescent psychiatry services, analysing the role of NGOs, increasing awareness about mental health problems among the population and promoting mental health and preventing mental disorders.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. Details about the year of formulation are not available.
Mental Health Legislation There is a Mental Health Act from 1940’s, that is being revised. There is also a more recent law on nar-cotics which was formulated in 1989. Currently, efforts are made to upgrade the law.The latest legislation was enacted in 1944.
Mental Health Financing There are budget allocations for mental health.The country spends 9% of the total health budget on mental health.The primary sources of mental health financing in descending order are tax based, out of pocket expenditure by the patient or fam-ily, social insurance and private insurances.The country has disability benefits for persons with mental disorders.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is not available at the primary level. Psychiatry has been integrated in the primary health care services in line with the Health Reform adopt-ed by the Ministry of Health. A system for referral between the different levels of care has been established.Regular training of primary care professionals is carried out in the field of mental health. In the last two years, about 639 personnel were provided training. Manuals for mental health care for primary care physicians and basic health care units are available. Training facilities are present. Training courses have been organized for general practitioners, maternal child health physicians, social workers and nursing staff working at basic health units. Training courses have also been held for trainers. Evaluation of training programmes for general practitioners showed significant improvement in attitudes, knowledge and skills regarding mental disorders and drug mis-use and their management.There are community care facilities for patients with mental disorders. Intermediate services were started for both patients with chronic mental disorders and drug use disorders. Large mental hospitals are trying to place long-stay patients in and follow them up in the community.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 1.3Psychiatric beds in mental hospitals per 10 000 population 1.1Psychiatric beds in general hospitals per 10 000 population 0.1Psychiatric beds in other settings per 10 000 population 0.1Number of psychiatrists per 100 000 population 0.9Number of neurosurgeons per 100 000 population 0.2Number of psychiatric nurses per 100 000 population 2Number of neurologists per 100 000 population 0.5Number of psychologists per 100 000 population 0.4Number of social workers per 100 000 population 0.1
There are few occupational therapists. Almost four-fifths of psychiatric beds are in Cairo. Beds for treatment of drug abusers and forensic patients are available. Specific allocations of beds have not been made for child and adolescent mental health. In an effort to provide quality assurance in big mental hospitals, standards have been developed and quality assurance teams have been deployed. Most psychiatrists have their own private clinics. There is a permanent training centre for continuous in- service training of mental health professionals, particularly nurses, psychologist and social workers employed in mental health facilities.
EGYPT

© 2005 World Health OrganizationMental Healthatlas
178
E –
I
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in advocacy, promotion, prevention and rehabilitation. The Child Mental Health Prevention Association, an NGO, was established in 1995, to spread the concept of mental health among families. There are also guidance and counselling centres at different governorates.
Information Gathering System There is mental health reporting system in the country. The country has no data collection system or epidemiological study on mental health. A new National Health Information System for Mental Health was developed by the Ministry of Health and Population. The General Secretariat of Mental Health is piloting a data collection system.
Programmes for Special Population The country has specific programmes for mental health for disaster affected population, eld-erly and children. Outpatient clinics and day care centres for children and adolescents are present in some mental hospitals. Clinics for school and university students are available in 4 centres. Eight special schools for education and rehabilitation of mentally retarded children are available. Of these, one caters to girls. Under the aegis of the school mental health programme, training programmes for school teachers, school physicians and school supervisors are undertaken, orientation courses for adolescents are held and special clinics at district levels are conducted in the area of mental health and drug misuse.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: pheno-barbital, amitriptyline, diazepam.Imipramine is available in primary health care (commonest strength: 25 mg, approximate cost for 100 tablets: 9.45 USD).
Other Information Finland has provided support to the mental health programme in Egypt since 2002. The Programme addresses five main components: human resource development, functional development, structural development, community development and mental health prevention and promotion. UNODP supports some activities for improving treatment services and rehabilitation of drug abusers.
Additional Sources of InformationAbou Nazel, M. W., Fahmy, S. I., Younis, I. A., et al (1991) A study of depression among Alexandria preparatory school adolescents. Journal of the Egyptian Public Health Association, 66, 649-674.
Daoud, R., Atallah, S., Loza, N. (2002). Psychiatric services in Egypt – an update. International Psychiatry, 2, 12-14.
Farrag, A. F., el Behary, A. A., Kandil, M. R. (1988) Prevalence of specific reading disability in Egypt. Lancet, 2, 837-839.
Farrag, A., Farwiz, H. M., Khedr, E. H., et al (1998) Prevalence of Alzheimer’s disease and other dementing disorders: Assiut-Upper Egypt study. Dementia & Geriatric Cognitive Disorders, 9, 323-328.
Ghanem, M., Gadallah, M., Mourad, S., et al (2004) National Survey of Prevalence of Mental Disorders in Egypt. WHO sponsored study (under publication).
Mental Health Programme in Egypt (2003) Country profile for mental health services. Mental Health programme in Egypt : [email protected].
Mental Health Programme in Egypt (2003) Master plan for provision of mental health services in Egypt. Mental Health programme in Egypt : [email protected].
Nasser, M. (1986) Comparative study of the prevalence of abnormal eating attitudes among Arab female students of both London and Cairo universities. Psychological Medicine, 16, 621-625.
Nasser, M. (1994) Screening for abnormal eating attitudes in a population of Egyptian secondary school girls. Social Psychiatry & Psychiatric Epidemiology, 29, 25-30.
Okasha, A. (1999) Mental Health in the Middle East: An Egyptian Perspective. Clinical Psychology Review, 19, 917-33.
Okasha, A., Fahmy, M., Haggag, W. et al. (2002) A psychiatric training programme for general practitioners in primary heatlh care in Egypt. Primary Care Psychiatry, 8, 9-16.
Okasha, A., Kamel, M., Khalil, A. H., et al (1985) Academic difficulty among male Egyptian university students. I. Association with psychiatric morbidity. British Journal of Psychiatry, 146, 140-144.
Okasha, A., Lotaif, F. (1979) Attempted suicide. An Egyptian investigation. Acta Psychiatrica Scandinavica, 60, 69-75.
Okasha, A., Ragheb, K., Attia, A. H., et al (2001) Prevalence of obsessive compulsive symptoms (OCS) in a sample of Egyptian adolescents. Encephale, 27, 8-14.
Soueif, M. I., Darweesh, Z. A., Hannourah, M. A., et al (1986) The extent of drug use among Egyptian male university students. Drug & Alcohol Dependence, 18, 389-403.
Soueif, M. I., el Sayed, A. M., Darweesh, Z. A., et al (1982) The extent of nonmedical use of psychoactive substances among secondary school students in Greater Cairo. Drug & Alcohol Dependence, 9, 15-41.
Soueif, M. I., Hannourah, M. A., Darweesh, Z. A., et al (1987) The use of psychoactive substances by female Egyptian university students, compared with their male colleagues on selected items. Drug & Alcohol Dependence, 19, 233-247.
Soueif, M. I., Youssuf, G. S., Taha, H. S., et al (1990) Use of psychoactive substances among male secondary school pupils in Egypt: a study on a nation-wide representative sample. Drug & Alcohol Dependence, 26, 63-79.
Temtamy, S. A., Kandil, M. R., Demerdash, A. M., et al (1994) An epidemiological/genetic study of mental subnormality in Assiut Governorate, Egypt. Clinical Genetics, 46, 347-351.
WHO, EMRO (1995) Intercountry Meeting on the Evaluation of the Progress of National Mental Health Programmes in the Eastern Mediterranean Region. World Health Organization, Regional Office for the Eastern Mediterranean.
WHO, EMRO (1997) Intercountry Consultation on Mental Health Legislation in Different Law Traditions. World Health Organization, Regional Office for the Eastern Mediterranean.
WHO, EMRO (1997) Intercountry Meeting on the Mental Health Needs Assessment at the Community, Health Services and Policy Levels in the Countries of the Eastern Mediterranean Region. World Health Organization, Regional Office for the Eastern Mediterranean.
EGYPT

© 2005 World Health OrganizationMental Healthatlas
179
E –
I
El SalvadorGENERAL INFORMATIONEl Salvador is a country with an approximate area of 21 thousand sq. km. (UNO, 2001). Its population is 6.614 million, and the sex ratio (men per hundred women) is 96 (UNO, 2004). The proportion of population under the age of 15 years is 34% (UNO, 2004), and the proportion of population above the age of 60 years is 8% (WHO, 2004). The literacy rate is 82.4% for men and 77.1% for women (UNESCO/MoH, 2004).The country is a lower middle income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 8%. The per capita total expenditure on health is 376 international $, and the per capita government expenditure on health is 175 international $ (WHO, 2004).The main language(s) used in the country is (are) Spanish. The largest ethnic group(s) is (are) Mestizo. The largest religious group(s) is (are) Roman Catholic (five-sixths).The life expectancy at birth is 66.5 years for males and 72.8 years for females (WHO, 2004). The healthy life expectancy at birth is 57 years for males and 62 years for females (WHO, 2004).
EPIDEMIOLOGYChocron et al (1995) conducted a two-phase study in a systematically selected primary care center sample (n=400) using the GHQ-28 (cut-off point 5/6) and Clinical Interview Schedule. The overall prevalence of psychopathology was 38.8%. Depression was found in 10.3% (major depression 6% and dysthymia 4.3%), anxiety in 13.8% (generalized 7.3%, panic 3% and obsessive/compulsive 3%) and adjustment disorder in 9.5% of the sample. Barthauer and Leventhal (1999) have reported on the psychologi-cal effects of child sexual abuse on 83 rural women interviewed using Hopkins Symptom Checklist. Abused women showed more depressive pathology in comparison to non-abused women. After controlling for the number of relatives killed in the war, however, that difference failed to reach statistical significance. The lack of difference in psychological symptoms between abused and non-abused women may be related to the different characteristics of the abuse and perpetrators. It also may be secondary to adverse social conditions, e.g. poverty and war, which could obscure the long-term effects of childhood sexual abuse. Walton et al (1997) conducted an ecologically conceptualized study to assess the mental health impact of the Salvadoran Civil War on 12-year-olds (n=54) who were born during the war and had been exposed to different levels of war violence. Half of the students came from a repopulated country village and half from an industrial neighbourhood near the capital city. Interviews and some instruments were administered to children, mothers/caretakers and teachers. Children from the repopulated village reported higher war experience and lower mental health. The personal/social impact of the war was more important than family togetherness or war intensity in determining the mental health of the children. Children’s intelligence was highly related to surviving with higher mental health. Higher socioeconomic status (SES) and education of parents was related to better mental health. Controlling for intelligence, children who experienced the highest personal-social impact of war showed the poorest mental health. Children with high war experience were most likely to have difficulty in imagining the future.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is present. The policy was initially formulated in 2000.The components of the policy are advocacy, promotion, prevention, treatment and rehabilitation. The policy was drafted through a process that involved professionals, NGOs and public servants. Between 10 to 25% of its original content have been put into prac-tice. Mental health is included in the Government Programme 1999-2004 called ‘the New Alliance’, within the Solidarity Alliance, as one of its strategic areas of action and sets limits for the strategic borders. This structured programme includes six elements or ‘alli-ances’- consolidation of economic stability, work alliance, solidarity alliance, security alliance, future alliance, participating and effec-tive Government.
Substance Abuse Policy A substance abuse policy is present. The policy was initially formulated in 2001. The Ministry of Public Health and Welfare is responsible for it. Drug addiction is considered a priority area in mental health. There is the Salvadorean Anti-Drug Commission, which is made of four governmental and non-governmental institutions. Its purpose is to reduce drug demand. There is also a Commission against Drug-related Activities, which is made of four governmental institutions. Its aim is to reduce drugs offer. The National Plan Against Drugs, 2000-2005, is functional. The substance abuse policy has a specific budget for its implementation and has been implemented to the extent of 10 to 255 as yet. El Salvador also has a law on Substance Abuse estab-lished in 1998.
National Mental Health Programme A national mental health programme is present. The programme was formulated in 2000.It was revised in 2001 and has been implemented 10 to 25% by national authorities. There are no funds for its implementation. Its main components are strategy of services reform, promotion and prevention, integration of mental health care in primary care and development of specialized specialized services.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. It was formulated in 1997.Currently, the seventh version of the essential drugs list is being used. The newly approved drugs list includes a lot of psychotropics for the first and second health care levels.

© 2005 World Health OrganizationMental Healthatlas
180
E –
I
Mental Health Legislation There is no mental health legislation. During 1998, a proposal to modify the Health Code was made. It focuses on promotion, prevention and advocacy, but it makes no reference to human rights of patients or regulation of mental health services.Details about the year of enactment of the mental health legislation are not available.
Mental Health Financing There are no budget allocations for mental health.Details about expenditure on mental health are not available.The primary sources of mental health financing in descending order are tax based, social insurance, out of pocket expenditure by the patient or family and private insurances.The country has disability benefits for persons with mental disorders. Less than 10% of the population is entitled for receiving ben-efits as it applies only to those who are covered by social security.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is available at the primary level. Primary care is carried out by the social security and is included in the proposal of the mental health programme. Less than 25% of the population is covered by this kind of service.Regular training of primary care professionals is not carried out in the field of mental health. There are no community care facilities for patients with mental disorders.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 0.65Psychiatric beds in mental hospitals per 10 000 population 0.65Psychiatric beds in general hospitals per 10 000 population 0Psychiatric beds in other settings per 10 000 population 0Number of psychiatrists per 100 000 population 0.5Number of neurosurgeons per 100 000 population Number of psychiatric nurses per 100 000 population 0Number of neurologists per 100 000 population Number of psychologists per 100 000 population 31.2Number of social workers per 100 000 population
Three-fifths of the beds are occupied by long stay patients. Three mental health units in general hospitals are proposed in three dif-ferent regions.
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in prevention and treatment. These organizations participate in mental health activities related to women, children, domestic violence and con-sumers.
Information Gathering System There is mental health reporting system in the country. The country has data collection system or epidemiological study on mental health. Some figures related to mental health, such as drug addiction, physical violence, etc. are reported in the weekly epidemiological report.
Programmes for Special Population The country has specific programmes for mental health for disaster affected population, eld-erly and children. The Ministry of Health is working to include the mental health component in different programmes of comprehen-sive health care (children, adolescents, women, elderly).Also there are programmes for women and children in vulnerable situations and for victims of domestic violence. Several of these activities are carried out with assistance of institutions like the Red Cross Federation, UNICEF and CICAD/OAS.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, phenobarbital, phenytoin sodium, diazepam, haloperidol.Some other drugs are also available but not at primary level.
Other Information The mental health team in the Health Ministry was created after the earthquake.
Additional Sources of InformationBarthauer, L. M., Leventhal, J. M. (1999) Prevalence and effects of child sexual abuse in a poor, rural community in El Salvador: a retrospective study of women after 12 years of civil war. Child Abuse & Neglect, 23, 1117-1126.
Chocron, B. L., Vilalta, F. J., Legazpi, R. I., et al (1995) Prevalence of psychopathology at a primary care center. Atencion Primaria, 16, 586-590.
Fernandes, J. D., Hurst, I. H., Oliveira, M. R., et al (1998) Psychiatric nursing research: concepts and expectations of nurses in psychiatric institutions. Revista Latinoamerica de Enfermagem, 6, 89-98.
Walton, J. R., Nuttall, R. L., Nuttall, E. V. (1997) The impact of war on the mental health of children: a Salvadoran study. Child Abuse & Neglect, 21, 737-749.
EL SALVADOR

© 2005 World Health OrganizationMental Healthatlas
181
E –
I
Equatorial GuineaGENERAL INFORMATIONEquatorial Guinea is a country with an approximate area of 28 thousand sq. km. (UNO, 2001). The country consists of the mainland (Rio Muni) and several islands, the largest of which is Bioko. Its population is 0.507 million, and the sex ratio (men per hundred women) is 98 (UNO, 2004). The proportion of population under the age of 15 years is 44% (UNO, 2004), and the proportion of population above the age of 60 years is 6% (WHO, 2004). The literacy rate is 92.1% for men and 74.5% for women (UNESCO/MoH, 2004).The country is a low income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 2%. The per capita total expenditure on health is 106 international $, and the per capita government expenditure on health is 64 inter-national $ (WHO, 2004).The main language(s) used in the country is (are) Spanish, French, Ndowe, Bisio and Annobonés. The largest ethnic group(s) is (are) Fang, and the other ethnic group(s) are (is) Buby, Ndowe, Bisio and Annobonés. The largest religious group(s) is (are) Roman Catholic, and the other religious group(s) are (is) Protestant and indigenous groups.The life expectancy at birth is 51.9 years for males and 54.8 years for females (WHO, 2004). The healthy life expectancy at birth is 45 years for males and 46 years for females (WHO, 2004).
EPIDEMIOLOGYThere is a paucity of epidemiological data on mental illnesses in Equatorial Guinea in internationally accessible literature.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is absent.
Substance Abuse Policy A substance abuse policy is absent.
National Mental Health Programme A national mental health programme is present. The programme was formulated in 1997.The programme exists in a preliminary form.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. It was formulated in 1996.
Mental Health Legislation There is no mental health legislation.
Mental Health Financing There are budget allocations for mental health.Details about expenditure on mental health are not available.The primary sources of mental health financing in descending order are out of pocket expenditure by the patient or family, social insurance, private insurances and tax based.Details about disability benefits for mental health are not available.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is not available at the primary level. While mental health care is expected to cover for mental health, very limited care is actually available.Regular training of primary care professionals is not carried out in the field of mental health. There are no community care facilities for patients with mental disorders. Only traditional healers offer treatment at community level.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 0Psychiatric beds in mental hospitals per 10 000 population 0Psychiatric beds in general hospitals per 10 000 population 0Psychiatric beds in other settings per 10 000 population 0Number of psychiatrists per 100 000 population 0Number of neurosurgeons per 100 000 population 0Number of psychiatric nurses per 100 000 population 0Number of neurologists per 100 000 population 0Number of psychologists per 100 000 population 0Number of social workers per 100 000 population 0.2
Non-Governmental Organizations NGOs are not involved with mental health in the country.
Information Gathering System There is no mental health reporting system in the country. The country has no data collection system or epidemiological study on mental health.
Programmes for Special Population There are no specific programmes.

© 2005 World Health OrganizationMental Healthatlas
182
E –
I
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, phenobarbital, phenytoin sodium, sodium valproate, chlorpromazine, diazepam, haloperidol, levodopa.The essential drug list was revised in the year 2000.
Other Information The appointment of a Focal Point for mental health in the Ministry of Health is under consideration.
Additional Sources of Information
EQUATORIAL GUINEA

© 2005 World Health OrganizationMental Healthatlas
183
E –
I
EritreaGENERAL INFORMATIONEritrea is a country with an approximate area of 118 thousand sq. km. (UNO, 2001). Its population is 4.296 million, and the sex ratio (men per hundred women) is 99 (UNO, 2004). The proportion of population under the age of 15 years is 45% (UNO, 2004), and the proportion of population above the age of 60 years is 4% (WHO, 2004). The literacy rate is 67.3% for men and 44.5% for women (UNESCO/MoH, 2004).The country is a low income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 5.7%. The per capita total expenditure on health is 36 international $, and the per capita government expenditure on health is 23 interna-tional $ (WHO, 2004).The main language(s) used in the country is (are) Tigrigna, Tigre, Saho, Afar, Bilen, Kunama, Nara, Hidarib and Arabic. The larg-est ethnic group(s) is (are) Tigrinya and Tigre. The largest religious group(s) is (are) Muslim, and the other religious group(s) are (is) Eritrean Orthodox Christian.The life expectancy at birth is 55.8 years for males and 59.3 years for females (WHO, 2004). The healthy life expectancy at birth is 49 years for males and 51 years for females (WHO, 2004).
EPIDEMIOLOGYThere is a paucity of epidemiological data on mental illnesses in Eritrea in internationally accessible literature. Wolff and Fesseha (1998, 1999) followed a group of 4-7 year old war orphans and compared them to a group of refugee children living in a nearby camp with one or both parents. Behavioural problems were significantly more common among the orphans compared to the refu-gee children, but their cognitive performance was better. Though their behavioural manifestations had diminished at 5-years follow-up they continued to exhibit emotional distress. Their cognitive performance was at least as good as comparison groups from other residential settings (these children were not exposed to war). Orphans who lived in a setting where the entire staff participated in decisions affecting the children, and where the children were encouraged to become self-reliant through personal interactions with staff members, showed significantly fewer behavioural symptoms of emotional distress than orphans who lived in a setting where the director made decisions, daily routines were determined by explicit rules and schedules and interactions between staff members and the children were impersonal.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is present. The policy was initially formulated in 1997.The components of the policy are advocacy, promotion, prevention, treatment and rehabilitation.
Substance Abuse Policy A substance abuse policy is absent. The Government has issued a proclamation to provide for Tobacco Control in the Gazette of Eritrean Laws (Proclamation 143/2004, Vol. 13/2004 No. 7, August 23) in 2004.
National Mental Health Programme A national mental health programme is absent.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. It was formulated in 1997.
Mental Health Legislation The country has no mental health legislation except those mentioned in the penal code.Details about the year of enactment of the mental health legislation are not available.
Mental Health Financing There are no budget allocations for mental health.Details about expenditure on mental health are not available.Details about sources of financing are not available.The country does not have disability benefits for persons with mental disorders.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is available at the primary level. Severe mental disorders are primarily treated at the tertiary level (at St. Mary’s Psychiatric Hospital). However, limited care is available at secondary and primary levels.Regular training of primary care professionals is carried out in the field of mental health. In the last two years, about 50 personnel were provided training. Training of primary care clinicians (physicians and nurses) started in 2004.There are community care facilities for patients with mental disorders. The community-based rehabilitation programme run by the Ministry of Labour and Human Welfare gives the opportunity for priority rehabilitation and also referral for those severely ill patients who need active treatment.

© 2005 World Health OrganizationMental Healthatlas
184
E –
I
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 0.64Psychiatric beds in mental hospitals per 10 000 population 0.64Psychiatric beds in general hospitals per 10 000 population 0Psychiatric beds in other settings per 10 000 population 0Number of psychiatrists per 100 000 population 0.03Number of neurosurgeons per 100 000 population 0.03Number of psychiatric nurses per 100 000 population 0.18Number of neurologists per 100 000 population 0Number of psychologists per 100 000 population 0Number of social workers per 100 000 population 0
There are 2 psychiatrists (1 Dutch and 1 Eritrean). Both neurosurgeons are expatriates. Post basic training for psychiatric nursing (14 months full time) has started. Sixteen students are undergoing training.
Non-Governmental Organizations NGOs are not involved with mental health in the country.
Information Gathering System There is mental health reporting system in the country. The Health Management Information System collects data routinely from all health facilities.The country has no data collection system or epidemiological study on mental health.
Programmes for Special Population There are no programmes for special populations.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: pheno-barbital, chlorpromazine, diazepam.The essential drug list is revised every 3 years. The next revision is due in January 2005.
Other Information
Additional Sources of InformationWolff, P. H., Fesseha, G. (1998) The orphans of Eritrea: are orphanages part of the problem or part of the solution? American Journal of Psychiatry, 155, 1319-1324.
Wolff, P. H., Fesseha, G. (1999) The orphans of Eritrea: a five-year follow-up study. Journal of Child Psychology & Psychiatry & Allied Disciplines, 40, 1231-1237.
ERITREA

© 2005 World Health OrganizationMental Healthatlas
185
E –
I
EstoniaGENERAL INFORMATIONEstonia is a country with an approximate area of 45 thousand sq. km. (UNO, 2001). Its population is 1.308 million, and the sex ratio (men per hundred women) is 85 (UNO, 2004). The proportion of population under the age of 15 years is 15% (UNO, 2004), and the proportion of population above the age of 60 years is 22% (WHO, 2004). The literacy rate is 99.8% for men and 99.8% for women (UNESCO/MoH, 2004).The country is a higher middle income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 5.5%. The per capita total expenditure on health is 562 international $, and the per capita government expenditure on health is 438 international $ (WHO, 2004).The main language(s) used in the country is (are) Estonian. The largest ethnic group(s) is (are) Estonian (two-thirds), and the other ethnic group(s) are (is) Russian (one-fourth). The largest religious group(s) is (are) Lutheran Christian (four-fifths), and the other reli-gious group(s) are (is) Orthodox Christian.The life expectancy at birth is 65.1 years for males and 77.1 years for females (WHO, 2004). The healthy life expectancy at birth is 59 years for males and 69 years for females (WHO, 2004).
EPIDEMIOLOGYA group of general practitioners used medical records and interviews using the Geriatric Depression Scale and MMSE to find the prevalence of physical and psychiatric disorders (especially depression and cognitive disorders) among a randomly selected elderly (65+ years) population in their practice. Psychiatric disorders were present in 5.7% with depression in 40.3% and cognitive disorders in 22.5% of the total respondents numbering 1000 (Saks et al, 2001). Parna et al (2002) did a nation wide cross-sectional survey to assess the prevalence of smoking. A stratified random sample of 2086 adults aged 30-59 was taken. The prevalence of current smoking was 57.9% among men and 25.7% among women. For both genders, smoking rates were lowest in the age group 50-59 years and highest in the age group 30-39 years. Smoking was significantly more common among divorced and widowed people. Education was associated with smoking among men but not among women. Pakriev et al (2001) evaluated a rural sample consisting of 232 respondents with unipolar depression. In this sample, 21.1% had single episodes, 62.5% had recurrent episodes and 16.4% had a chronic course. Being of local ethnicity and unmarried status were significantly associated with both recurrent and chronic course of depression. Comorbid dysthymia and poor family relationships were associated with chronic depression. Suicide attempts were associated with recurrent depression. Varnik et al (1994) presented their data on changing trends of suicide in the 3 Baltic states of Estonia, Latvia and Lithuania during the period 1968-90. Since 1986, the mean male suicide rate in Estonia fell by 26.6% from a high of 55.7 per 100 000 in the period 1968-84. Female suicide rates remained constant in both those periods (nearly 14.3 per 10 000). The male female ratio dropped to 3.1 from an earlier value of 3.9. In an earlier study by Varnik (1991) it was reported that suicide rates rose gradually since independence in 1922 till 1986 and then started to fall from 1986 onwards. Wasserman et al (1998) found that alcohol related suicides among women drinkers reduced by 19% in the period 1984-1990 in 8 republics (includ-ing Estonia) of the erstwhile USSR. This was attributed to the restrictions (in the form of increased prices) imposed on alcohol by the Government during that period.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is present. The policy was initially formulated in 2002.The mental health policy is contained in the Mental Health Basic Document. A mental health strategy document is under develop-ment.
Substance Abuse Policy A substance abuse policy is present. The policy was initially formulated in 1997. Details can be obtained about the drug policy from the website: www.narko.sm.ee
National Mental Health Programme A national mental health programme is absent.Estonia does not have a comprehensive mental health plan but it has a national strategy on suicide prevention and a draft national programme.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. It was formulated in 1996.Details can be obtained from the website: www.sam.ee
Mental Health Legislation There is a Mental Health Act. The main principles are: (1) Criteria are given for involuntary treatment (dangerousness to self or others due to mental disorder, other means of treatment not being effective); (2) Supervision over involun-tary treatment is carried out both by the county medical officer and the administrative court; (3) The Mental Health Act also deter-mines the basic requirements for psychiatric treatment, including responsibilities for the provision of services by the community and the state, the rights of patients and the basic regulations for forensic psychiatry.The latest legislation was enacted in 1997.

© 2005 World Health OrganizationMental Healthatlas
186
E –
I
Mental Health Financing There are no budget allocations for mental health.Details about expenditure on mental health are not available.The primary sources of mental health financing in descending order are social insurance, out of pocket expenditure by the patient or family and private insurances.The country has disability benefits for persons with mental disorders.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is available at the primary level. Regular training of primary care professionals is carried out in the field of mental health. There are community care facilities for patients with mental disorders. Community care training for nurses has begun. The Estonian Psychiatric Association has developed several proposals for the development of community services. It is expected that with the introduction of the Hospital Masterplan (www.sm.ee/develop.html) for the development of secondary health care services, the Government will develop more community-orientated services including services for the long-term mentally ill (see the development of special care: www.sm.ee/devspecialcare.html).
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 10.2Psychiatric beds in mental hospitals per 10 000 population 8Psychiatric beds in general hospitals per 10 000 population 2.1Psychiatric beds in other settings per 10 000 population 0Number of psychiatrists per 100 000 population 13Number of neurosurgeons per 100 000 population 1Number of psychiatric nurses per 100 000 population 0Number of neurologists per 100 000 population 13Number of psychologists per 100 000 population Number of social workers per 100 000 population
Psychiatric hospitals and wards provide acute inpatient treatment, but the majority of long-term institutionalized patients are cared for in the psychiatric nursing homes of the social welfare system. The outpatient services are linked either to a psychiatric hospital or to the local general hospital. The Swedish East European Committee is supporting training of nurses.
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in advocacy, prevention and rehabilitation. There are several NGOs that are active in the field of mental health. Among them are organizations for consumers of the services or their families, professional societies and groups for the protection of consumer rights. At the level of local Government, the mental health services are mainly represented by day centres for psychiatric patients, crisis centres and tel-ephone hotlines.
Information Gathering System There is mental health reporting system in the country. The country has no data collection system or epidemiological study on mental health.
Programmes for Special Population There are no facilities for special population groups.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, ethosuximide, phenobarbital, phenytoin sodium, sodium valproate, amitriptyline, chlorpromazine, diazepam, fluphena-zine, haloperidol, lithium, biperiden, carbidopa, levodopa.Details can be obtained about the drug policy from the website: www.narko.sm.ee
Other Information In Estonia, mental health services are provided by the medical facilities and practitioners, as well as by insti-tutions from the social welfare sector. The state, the local level of services and private agencies are all represented in this field. Although cooperation between the different sectors is improving, there are still many steps to be taken to provide society with a well functioning network of services. Before the last decade, mental health services were characterized by: centralized provision, large institutions with poor material conditions, underdeveloped outpatient services, weak connections with primary health care, underdeveloped community care services for long-term severely ill patients, split between social and health care services, lack of relevant legislation, medical model dominating over psychosocial understanding of illness, lack of trained personnel (nurses, social workers) and the absence of psychotherapy training. The strategy of the Estonian Psychiatric Association are to: maintain and improve the links with the rest of the health care system, define responsibilities with the social welfare system, develop more com-munity services for the long-term mentally ill, link the social services with health care, focus on legislation in order to meet European standards, improve training of mental health specialists and develop new structures for the provision of services like psychiatric wards in general hospitals and outpatient units with multidisciplinary teams.
ESTONIA

© 2005 World Health OrganizationMental Healthatlas
187
E –
I
Additional Sources of InformationPakriev, S., Shlik, J., Vasar, V. (2001) Course of depression: findings from cross-sectional survey in rural Udmurtia. Nordic Journal of Psychiatry, 55, 185-189.
Parna, K., Rahu, K., Rahu, M. (2002) Patterns of smoking in Estonia. Addiction, 97, 871-876.
Saks, K., Kolk, H., Allev, R., et al (2001) Health status of the older population in Estonia. Croatian Medical Journal, 42, 663-668.
The provisional development plan of mental health services (in Estonian only): www.sm.ee/arengukavad/Psuhhiaatria.htm
Varnik, A. (1991) Suicide in Estonia. Acta Psychiatrica Scandinavica, 84, 229-232.
Varnik, A., Wasserman, D., Eklund, G. (1994) Suicides in the Baltic countries, 1968-1990. Scandinavian Journal of Social Medicine, 22, 166-169.
Wasserman, D., Varnik, A., Eklund, G. (1998) Female suicides and alcohol consumption during perestroika in the former USSR. Acta Psychiatrica Scandinavica, Supplementum 394, 26-33.
ESTONIA

© 2005 World Health OrganizationMental Healthatlas
188
E –
I
EthiopiaGENERAL INFORMATIONEthiopia is a country with an approximate area of 1104 thousand sq. km. (UNO, 2001). Its population is 72.42 million, and the sex ratio (men per hundred women) is 99 (UNO, 2004). The proportion of population under the age of 15 years is 45% (UNO, 2004), and the proportion of population above the age of 60 years is 5% (WHO, 2004). The literacy rate is 49.2% for men and 33.8% for women (UNESCO/MoH, 2004).The country is a low income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 3.6%. The per capita total expenditure on health is 14 international $, and the per capita government expenditure on health is 6 interna-tional $ (WHO, 2004).The main language(s) used in the country is (are) Amharic, Oromo and Tigrinya. The largest ethnic group(s) is (are) Oromo and Amhara, and the other ethnic group(s) are (is) Tigre, Somale and Walayta. The largest religious group(s) is (are) Muslim, and the other religious group(s) are (is) Ethiopian Orthodox Christian.The life expectancy at birth is 46.8 years for males and 49.4 years for females (WHO, 2004). The healthy life expectancy at birth is 41 years for males and 42 years for females (WHO, 2004).
EPIDEMIOLOGYAlem et al (1999d) assessed 10 468 subjects from a rural and semi-urban community with the Self Reporting Questionnaire (SRQ). Psychiatric morbidity was found in 17% of the respondents (cut-off – 10/11). The rate was higher among women probably because they were more likely to be older, illiterate and widowed/divorced. Tafari et al (1991) used the SRQ (cut-off – 10/11, for psychotic symptoms – 2/3) and the Holmes-Rahe Social Readjustment Scale in another rural sample (n=2000) and found the prevalence of mental illness to be 17.2% (neurotic: 11.2% and psychotic: 6.0%). Prevalence of mental disorders was significantly associated with stress, family history of mental illness and with marital status (divorced, separated or widowed). Awas et al (1999) used the Ahmaric version of the CIDI (ICD-10 criteria) for assessing 501 respondents selected from a predominantly rural district by stratified ran-dom sampling. They found a lifetime prevalence rate of 31.8% (26.7% when substance dependence was not included). The most frequent specific diagnoses were: dissociative disorders (6.3%), mood disorders (6.2%), somatoform disorders (5.9%) and anxiety disorders (5.7%). Female gender was associated with increased risk of mood disorders and somatoform disorders. Cognitive and mood disorders were more common among the elderly. Kebede et al (1999) examined a sample from an urban community (n=10 203). They reported a probable diagnosis of psychosis in 5% of the sample (positive response to 2 out of 4 items of the SRQ) and of common mental disorders in 11.7% (using a cut-off of 6 out of 20 SRQ items). Age, female sex, lower educational level, unemployment, small family size and family history of mental illness were associated with high prevalence rates. Kebede and Alem (1999c, d, e) conducted a survey on a randomly selected urban community sample of 1420 individuals using the Ahmaric version of CIDI. Lifetime prevalence for severe cognitive deficits, schizophrenia, schizoaffective disorder, affective disorders, neurotic and somatoform disorders were 2.6%, 0.4%, 0.5%, 5.0% (overall: women 7.7% and men 3.2%, bipolar disorders: 0.3%, depressive episodes: 2.7%, recurrent depressive episodes: 0.2% and persistent mood disorders: 1.6%), 10.8% (phobic disorder: 4.8%, somato-form disorders: 2.7%, dissociative disorders: 0.8% and other anxiety disorders: 2.7%). The one month prevalence of schizophrenia, schizoaffective disorder, affective disorders, phobic anxiety disorders, other anxiety disorders, dissociative disorders, and somatoform disorders were 0.3%, 0.4%, 3.8% (women 5.9% and men 2.3%), 4.4%, 1.2%, 0.4% and 2.5%, respectively. Alem et al (1999b) and Kebede and Alem (1999b) reported that the overall prevalence of problem drinking (meeting 2 criteria on the CAGE question-naire) was 3.7% in a rural (n=10 468) and 2.7% in an urban (n=10 203) sample. Age, gender (male), education (low), employment status (low), religion (Christian), ethnicity (non-Gurage) and smoking were associated with problem drinking in both sexes. Marital status, mental distress and income were associated with problem drinking only in men. Kebede et al (1999) reported that use of CIDI yielded a lifetime and one-month prevalence of alcohol dependence in 1.0% and 0.8% of the urban sample, respectively. Alcohol dependence was reported almost exclusively in males. Almost one third of the Ethiopean adult population uses or has used Khat. Alem et al (1999a) reported that 17.4% of subjects from a rural sample (n=19 468) used it daily. Habitual use was associated with gender (male), age (15-34 years), religion (Muslim), smoking, educational level (high), family functioning (better) and mental distress. De Jong et al (2001) assessed randomly selected post-conflict survivors in four countries – Algeria, Cambodia, Ethiopia (n=1200) and Gaza using the CIDI and Life Events and Social History Questionnaire. The prevalence rate of PTSD was 15.8% in Ethiopia. Conflict-related trauma after age 12 years, torture, psychiatric history and current illness were associated with PTSD in Ethiopia. Alem et al (1999c) and Kebede and Alem (1999a) reported the rate of suicide attempts to be 3.2% and 0.95% in rural (n=10 468) and urban (n=10 203) samples, respectively. In both studies hanging (among men) and poisoning (among women) were the preferred methods of attempting suicide. Suicide attempts were associated with young age (15-24 years), religion (Christianity), psychiatric morbidity and problem drinking. Kebede and Ketsela (1993) evaluated a representative sample of all high-school students in a city. Almost 14.3% of the adolescents reported having attempted suicide. Suicide attempts were strongly and linearly associ-ated with hopelessness, grade and heavy alcohol intake. Mulatu (1995) interviewed mothers using the Child Behavior Problem Questionnaire to assess 611 randomly selected children from an urban community. They found that 21.5% of boys and 25.2% of girls had some behavioural problems. Tadesse et al (1999) used the Amharic version of the Reporting Questionnaire for Children in a community survey and found behavioural disorders in 17.7% of children. Childhood mental disorder was significantly associated with the subjects’ own age (higher), gender, and parents’ age (younger), marital status (not currently married) and psychopathol-

© 2005 World Health OrganizationMental Healthatlas
189
E –
I
ogy (neurosis in mothers). Ashenafi et al (2001) used an Amharic version of a Diagnostic Instrument for Children and Adolescents to interview parents in a rural community (n=1477) and found that 3.5% had at least one mental or behavioral disorder. The most frequent diagnoses were anxiety disorders (1.6%), attention deficit hyperactivity disorder (1.5%), disruptive behaviour disorders (1.5%), mood disorders (1%) and elimination disorders (0.8%).
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is absent.A team of mental health professionals was assigned the task of drafting a mental health policy in 2004. The draft is expected to be submitted for approval in the same year.
Substance Abuse Policy A substance abuse policy is absent.
National Mental Health Programme A national mental health programme is absent.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. Details about the year of formulation are not available.Shortage of essential drugs is a problem.
Mental Health Legislation There is no mental health legislation in the country. Currently, individual rights are seen in unison with the family. Involuntary treatment only requires informed consent from the escorts. Though a draft legislation was submitted for approval several years back, it has not yet been enacted. In 2004, the team working on mental health policy is also reviewing the draft legislation for re-submission.
Mental Health Financing There are budget allocations for mental health.Details about expenditure on mental health are not available.The primary sources of mental health financing in descending order are tax based, out of pocket expenditure by the patient or fam-ily, private insurances and grants.The country has disability benefits for persons with mental disorders. Pension and transfer are allowed on the basis of psychiatric certification.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is available at the primary level. Mental health has become part of primary health care in 42 units spread throughout the country. The number is gradually increasing as trained professionals are assigned to new sites every year. Thus, actual treatment of severe mental disorders at the primary level is steadily expanding.Regular training of primary care professionals is carried out in the field of mental health. In the last two years, about 277 personnel were provided training. In the last two years, about 45 personnel were provided basic training, 160 primary mental health profes-sionals participated in yearly refresher seminars and 72 on-the-job training programmes were conducted for those working at the different units in the country.There are no community care facilities for patients with mental disorders.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 0.07Psychiatric beds in mental hospitals per 10 000 population 0.06Psychiatric beds in general hospitals per 10 000 population 0.01Psychiatric beds in other settings per 10 000 population 0Number of psychiatrists per 100 000 population 0.02Number of neurosurgeons per 100 000 population 0.003Number of psychiatric nurses per 100 000 population 0.3Number of neurologists per 100 000 population 0.006Number of psychologists per 100 000 population 0.08Number of social workers per 100 000 population 0.08
There are different medical assistants for other fields, around 10 000, but not for psychiatry. There are 36 regional and district men-tal health units besides the mental hospital in Addis Ababa. These hospitals are each staffed by at least 2 psychiatric nurses who are supervised by psychiatrists periodically. A system of referral and back-referral has been established. In some regional hospitals the psychiatric nurses admit and provide inpatient service to their cases in the medical wards when it is necessary. A postgraduate pro-gramme in psychiatry was started in Addis Ababa University with an initial intake of 7 residents in 2003.
Non-Governmental Organizations NGOs are not involved with mental health in the country. One indigenous NGO named ‘Mental Health Society of Ethiopia’ was established in 2004. The association is currently working on building up its membership but is already involved in supporting the only rehabilitation centre for mental health near Addis Ababa.
ETHIOPIA

© 2005 World Health OrganizationMental Healthatlas
190
E –
I
Information Gathering System There is mental health reporting system in the country. Hospitals send annual report to the Ministry of Health.The country has data collection system or epidemiological study on mental health. The training and research division of the Amanvel Mental hospital has been established recently for this purpose.
Programmes for Special Population There are no programmes for special population.Psychiatric services have been introduced to some police and army hospitals, one prison clinic, and some university and school clin-ics. Two substance abuse treatment units were opened in the capital city in 2004.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, ethosuximide, phenobarbital, phenytoin sodium, sodium valproate, amitriptyline, chlorpromazine, diazepam, fluphena-zine, haloperidol, lithium, carbidopa, levodopa.The essential list of drugs was revised recently. Some other medicines like cloimipramine and fluoxetine are also a part of the list. All drugs in the essential list are available in major cities of the country but not in all areas at the primary health care level.
Other Information Traditional healers play a major role in the treatment of mental health; in one study (Alem et al 1999) it was found that 85% of emotionally disturbed people sought help from traditional healers.
Additional Sources of InformationAlem, A. (2000) Human rights and psychiatric care in Africa with particular reference to the Ethiopian situation. Acta Psychiatrica Scandinavica, Supplementum 399, 93-96.
Alem, A. (2001) Mental health services and epidemiology of mental health problems in Ethiopia. Ethiopean Medical Journal, 39, 153-165.
Alem, A. (2002) Community-based vs. hospital-based mental health care: the case of Africa. World Psychiatry, 1, 98-99.
Alem, A., Araya, M., Jacobsson, L., et al (1999) How are mental disorders seen and where is help sought in a rural Ethiopian community? A key informant study in Butajira, Ethiopia. Acta Psychiatrica Scandinavica, Supplementum 397, 40-47.
Alem, A., Kebede, D., Jacobsson, L., et al (1999c) Suicide attempts among adults in Butajira, Ethiopia. Acta Psychiatrica Scandinavica, Supplementum, 397, 70-76.
Alem, A., Kebede, D., Kullgren, G. (1999a) The prevalence and socio-demographic correlates of khat chewing in Butajira, Ethiopia. Acta Psychiatrica Scandinavica, Supplementum, 397, 84-91.
Alem, A., Kebede, D., Kullgren, G. (1999b) The epidemiology of problem drinking in Butajira, Ethiopia. Acta Psychiatrica Scandinavica, Supplementum, 397, 77-83.
Alem, A., Kebede, D., Woldesemiat, G., et al (1999d) The prevalence and socio-demographic correlates of mental distress in Butajira, Ethiopia. Acta Psychiatrica Scandinavica, Supplementum, 397, 48-55.
Ashenafi, Y., Kebede, D., Desta, M., et al (2001) Prevalence of mental and behavioural disorders in Ethiopian children. East African Medical Journal, 78, 308-311.
Awas, M., Kebede, D., Alem, A. (1999) Major mental disorders in Butajira, southern Ethiopia. Acta Psychiatrica Scandinavica, Supplementum, 397, 56-64.
de Jong, J. T., Komproe, I. H., Van Ommeren, M., et al (2001) Lifetime events and posttraumatic stress disorder in 4 postconflict settings. JAMA, 286, 555-562.
Giel, R. (1999). The prehistory of psychiatry in Ethiopia. Acta Psychiatrica Scandinavica. Supplementum 397, 2-4.
Kebede, D., Alem, A. (1999a) Suicide attempts and ideation among adults in Addis Ababa, Ethiopia. Acta Psychiatrica Scandinavica, Supplementum, 397, 35-39.
Kebede, D., Alem, A. (1999b) The epidemiology of alcohol dependence and problem drinking in Addis Ababa, Ethiopia. Acta Psychiatrica Scandinavica, Supplementum, 397, 30-34.
Kebede, D., Alem, A. (1999c) Major mental disorders in Addis Ababa, Ethiopia. III. Neurotic and somatoform disorders. Acta Psychiatrica Scandinavica, Supplementum, 397, 24-29.
Kebede, D., Alem, A. (1999d) Major mental disorders in Addis Ababa, Ethiopia. II. Affective disorders. Acta Psychiatrica Scandinavica, Supplementum, 397, 18-23.
Kebede, D., Alem, A. (1999e) Major mental disorders in Addis Ababa, Ethiopia. I. Schizophrenia, schizoaffective and cognitive disorders. Acta Psychiatrica Scandinavica, Supplementum, 397, 11-17.
Kebede, D., Alem, A., Rashid, E. (1999) The prevalence and socio-demographic correlates of mental distress in Addis Ababa, Ethiopia. Acta Psychiatrica Scandinavica, Supplementum, 99, 5-10.
Kebede, D., Ketsela, T. (1993) Suicide attempts in Ethiopian adolescents in Addis Abeba high schools. Ethiopian Medical Journal, 31, 83-90.
Mulatu, M. S. (1995) Prevalence and risk factors of psychopathology in Ethiopian children. Journal of the American Academy of Child & Adolescent Psychiatry, 34, 100-109.
Tadesse, B., Kebede, D., Tegegne, T., et al (1999) Childhood behavioural disorders in Ambo district, western Ethiopia. I. Prevalence estimates. Acta Psychiatrica Scandinavica, Supplementum, 397, 92-97.
Tafari, S., Aboud, F. E., Larson, C. P. (1991) Determinants of mental illness in a rural Ethiopian adult population. Social Science & Medicine, 32, 197-201.
ETHIOPIA

© 2005 World Health OrganizationMental Healthatlas
191
E –
I
FijiGENERAL INFORMATIONFiji is a country with an approximate area of 18 thousand sq. km. (UNO, 2001). The country consists of more than 300 islands. Its population is 0.847 million, and the sex ratio (men per hundred women) is 104 (UNO, 2004). The proportion of population under the age of 15 years is 32% (UNO, 2004), and the proportion of population above the age of 60 years is 6% (WHO, 2004). The literacy rate is 94.5% for men and 91.4% for women (UNESCO/MoH, 2004).The country is a lower middle income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 4%. The per capita total expenditure on health is 224 international $, and the per capita government expenditure on health is 150 international $ (WHO, 2004).The main language(s) used in the country is (are) Fijian, Hindi, English and Rotuman. The largest ethnic group(s) is (are) Fijian (more than half of the population), and the other ethnic group(s) are (is) Indian (two-fifths). The largest religious group(s) is (are) Christian, and the other religious group(s) are (is) Hindu and Muslim.The life expectancy at birth is 64.6 years for males and 70.3 years for females (WHO, 2004). The healthy life expectancy at birth is 57 years for males and 61 years for females (WHO, 2004).
EPIDEMIOLOGYBecker (1998) assessed the frequency of ‘na tadoka ni vasucu’, a somatic syndrome occurring among ethnic Fijian women. The authors assessed 85 consecutive newly delivered ethnic Fijian women within the first few postpartum days and then again after 2-5 months with translated structured interviews, the Kellner Symptom Questionnaire and visual analogy scales to assess social supports and occurrence of mood symptoms or an episode of ‘na tadoka ni vasucu.’ Semistructured ethnographic interviews were conducted with subjects who reported an episode of the latter. ‘Na tadoka ni vasucu’ occurred in 9% (n=7) of the sample. Both quantitative and narrative data demonstrated that this syndrome is associated with perceived inferior social supports. Aghanwa (2001a) com-pared characteristics of 51 unipolar mania patients with 31 bipolar patients in a hospital-based study. Diagnosis was confirmed using SCAN and ICD-10. Though the frequency of episodes, duration of affective illness, mean age at onset, gender distribution, marital status, employment status and race were not significantly different between the two groups, family history of major psychiatric mor-bidity was significantly more in the bipolar group (9.8% for the unipolar manic patients and 22.6% for the manic-depressive group). In other studies, Aghanwa (2000, 2001b) estimated the prevalence of attempted suicide to be 34.8 per 100 000 population based on a sample of 39 consecutive cases referred to psychiatric services at the main general hospital. Suicide formed 36.8% of all the cases referred to the psychiatric service. Social problems and/or psychiatric comorbidity were present in over 60% of cases. Suicide attempters were significantly more likely to be younger, single and unemployed. When 31 consecutive patients attending a hospital, with deliberate drug-overdose and 27 others with non-overdosed self-poisoning were compared, those with overdose were found to be older and to have a history of psychiatric disorder. Alcohol use was significantly more common in the other group, which also had a greater proportion of males. Pridmore et al (1995) assessed the prevalence of suicide and self-harm based on an unidentified data source. They reported that self-harm had become more common particularly among those of Indian ethnicity (in both males and females). Non-fatal injury by self was reported to be 8 times more common than suicide and it had a female preponderance. Disproportionately high rates of completed suicide was reported among Fijian Indians (women under 30 years and males above 30 years) based on police and medical records by Haynes (1984). Pridmore et al (1996) examined the hanging and poisoning autopsy reports from two distinct regions. The rate of autopsy (per 100 000 population per year) among Indians was significantly greater than among Fijians. Regional variation with respect to gender and method of attempting suicide were noted. Hanging remains the preferred option for all groups. Booth (1999) reported high suicide rates among 13 Pacific islands. Young women outnumbered men among Fiji Indians and Western Samoans. They noted that pesticides were a common method of attempting suicide. Fiji was one of the participating countries in the Global Youth Tobacco Survey (GYTS) project developed by the World Health Organization and the US Centers for Disease Control and Prevention to track tobacco use among youth in countries across the world (Warren et al, 2000).
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is present. The policy was initially formulated in 1994.The components of the policy are advocacy, promotion, prevention, treatment and rehabilitation. The National Advisory Council in Mental Health is in the process of reviewing the National Mental Health Policy (National Mental Health Plan 2005-2008). NGOs are being consulted on this project. The draft policy focuses on development of community mental health services, development of mental health action volunteers to assist in rehabilitation, expansion of the mental health workforce, revision of the mental health legislation and mental health promotion.
Substance Abuse Policy A substance abuse policy is present. The policy was initially formulated in 1998.
National Mental Health Programme A national mental health programme is present. The programme was formulated in 1999.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. It was formulated in 1994.

© 2005 World Health OrganizationMental Healthatlas
192
E –
I
Mental Health Legislation There are the Laws of Fiji – Chapter 113 – Mental Treatment Act. The Act was initially formulated in the 1940’s and partly revised in 1978, but it is considered to be too narrow as it deals only with treatment issues. Based on a cabinet paper that was prepared with the assistance of WHO, the Cabinet has approved of review for MTA. Fiji Law Reform will draft the law and then consultations with various stakeholders will be held.The latest legislation was enacted in 1978.
Mental Health Financing There are budget allocations for mental health.The country spends 1.7% of the total health budget on mental health.The primary sources of mental health financing in descending order are tax based, out of pocket expenditure by the patient or fam-ily and private insurances.The entire mental health budget is spent on curative services.The country has disability benefits for persons with mental disorders. They are able to apply for social welfare assistance.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is not available at the primary level. There is a lack of sufficiently trained doctors or facilities to treat severely ill patients in the primary health centres.Regular training of primary care professionals is carried out in the field of mental health. In the last two years, about 140 personnel were provided training. Training to primary health care workers is through workshops that are being held regularly since the last two years.There are no community care facilities for patients with mental disorders. There are no community-based care facilities for the men-tally ill. Discussions on establishing regional (in all 4 divisions) mental health units are under way. St. Giles Hospital has day care and occupational therapy facilities and the hospital staff provide limited community services in the greater Suva area. A community psy-chiatric nursing team has been established. The community service provided is largely a pre-discharge contact with the appropriate zone nurse and the sub-divisional medical officer to whom the details of the patient is provided. Medication required for the patients are sent every month to the nurse. A community team comprising of a doctor and nurses also make domiciliary visits and conduct counselling and education. This operates within a radius of about 10 km from the hospital.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 2.34Psychiatric beds in mental hospitals per 10 000 population 2.34Psychiatric beds in general hospitals per 10 000 population 0Psychiatric beds in other settings per 10 000 population 0Number of psychiatrists per 100 000 population 0.25Number of neurosurgeons per 100 000 population 0.1Number of psychiatric nurses per 100 000 population 0Number of neurologists per 100 000 population 0Number of psychologists per 100 000 population 0.25Number of social workers per 100 000 population 0
There is one occupational therapist. There are 23 nurses working in mental health care settings. The clinical psychologists are in pri-vate practice and other psychologists work in the university (academic psychology) setting. There are about 10 000 social workers, but they are not trained in mental health.
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in advocacy, promotion, prevention and rehabilitation.
Information Gathering System There is mental health reporting system in the country. The main source of information collection is through annual reports of the St. Giles Hospital at Suva (these are submitted to the MOH). A patient Information System (PATIS) is being established in the general health sector. The mental health services are yet to be linked to the PATIS.The country has data collection system or epidemiological study on mental health. The Statistics Department collects information from hospitals.
Programmes for Special Population The Fiji Council for Social Services attends to the needs of the elderly in the community.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, ethosuximide, phenobarbital, phenytoin sodium, sodium valproate, amitriptyline, chlorpromazine, diazepam, fluphena-zine, haloperidol, lithium, carbidopa, levodopa.Olanzapine has been added to the essential list. The supply is limited to 1000 (10 mg) tablets per month. The approximate cost of 100 tablets of a generic brand (10 mg – commonest strength) is 14.25 USD. It is, however, not available at the primary care level.
FIJI

© 2005 World Health OrganizationMental Healthatlas
193
E –
I
Other Information
Additional Sources of InformationAghanwa, H. S. (2000) The characteristics of suicide attempters admitted to the main general hospital in Fiji Islands. Journal of Psychosomatic Research, 49, 439-445.
Aghanwa, H. S. (2001a) Recurrent unipolar mania in a psychiatric hospital setting in the Fiji Islands. Psychopathology, 34, 312-317.
Aghanwa, H. S. (2001b) Attempted suicide by drug overdose and by poison-ingestion methods seen at the main general hospital in the Fiji islands: a com-parative study. General Hospital Psychiatry, 23, 266-271.
Becker, A. E. (1998) Postpartum illness in Fiji: a sociosomatic perspective. Psychosomatic Medicine, 60, 431-438.
Booth, H. (1999) Pacific Island suicide in comparative perspective. Journal of Biosocial Science, 31, 433-448.
Cruz, M. (2004) A review of existing functions and responsibilities of the Fiji Ministry of Health in relation to the care, treatment and rehabilitation of mentally ill people in Fiji (Draft).
Government document (1978) Laws of Fiji. Mental Treatment, Chapter 113.
Government document (1998) Substance Abuse Advisory Council Act.
Haynes, R. H. (1984) Suicide in Fiji: a preliminary study. British Journal of Psychiatry, 145, 433-438.
Khan, S. (1998) Community Psychiatric Nursing Annual Report.
Medical Superintendent (1998) Report on the St. Giles Staff Activities in the Western Division.
Narayan, S. (2003) Country report on mental health issues for the Regional Report on Mental Health from the Western Pacific Region.
Narayan, S., Plange, N-K. (2003) Project: Mental Health Policy project. Country Fiji (Draft).
Pridmore, S., Ryan, K., Blizzard, L. (1995) Victims of violence in Fiji. Australian & New Zealand. Journal of Psychiatry, 29, 666-670.
Pridmore, S., Lawler, A., Couper, D. (1996) Hanging and poisoning autopsies in Fiji. Australian & New Zealand Journal of Psychiatry, 30, 685-687.
St. Giles Hospital Annual Report (1999) Mental Health, Non-Communicable Diseases.
St. Giles Hospital Annual Report (1997) Community Mental Health Team.
Warren, C. W., Riley, L., Asma, S., et al (2000) Tobacco use by youth: a surveillance report from the Global Youth Tobacco Survey project. Bulletin of the World Health Organization, 78, 868-876.
FIJI

© 2005 World Health OrganizationMental Healthatlas
194
E –
I
FinlandGENERAL INFORMATIONFinland is a country with an approximate area of 338 thousand sq. km. (UNO, 2001). Its population is 5.216 million, and the sex ratio (men per hundred women) is 96 (UNO, 2004). The proportion of population under the age of 15 years is 17% (UNO, 2004), and the proportion of population above the age of 60 years is 20% (WHO, 2004). The literacy rate is 99% for men and 99% for women (UNESCO/MoH, 2004).The country is a high income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 7%. The per capita total expenditure on health is 1845 international $, and the per capita government expenditure on health is 1395 international $ (WHO, 2004).The main language(s) used in the country is (are) Finnish and Swedish. The largest ethnic group(s) is (are) Finn. The largest religious group(s) is (are) Lutheran Christian (five-sixths), and the other religious group(s) are (is) Orthodox Christian.The life expectancy at birth is 74.8 years for males and 81.5 years for females (WHO, 2004). The healthy life expectancy at birth is 69 years for males and 74 years for females (WHO, 2004).
EPIDEMIOLOGYThere is substantial epidemiological data on mental illnesses in Finland in internationally accessible literature. No attempt was made to include this information here.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is present. The policy was initially formulated in 1993.The components of the policy are advocacy, promotion, prevention, treatment and rehabilitation. Finland has a health policy docu-ment (Health 2015) where mental health is included as an integrated component (a specific mental health policy paper is not there). In health policy, the main priorities are basic services and outpatient services. The Ministry of Social Affairs and Health produced quality guidelines for mental health services in 2001 and is working on quality guidelines for supportive housing regarding people with mental health problems.
Substance Abuse Policy A substance abuse policy is present. The policy was initially formulated in 1997. The substance abuse policy is known as Drug Strategy. The Government has adopted a Drug Policy Action Programme for the period 2004-2007. An Alcohol Programme was formulated in 2004.
National Mental Health Programme A national mental health programme is present. The programme was formulated in 1999.Finland was the first country in the world to adopt a comprehensive national suicide prevention programme (in 1992).
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is absent.
Mental Health Legislation There is a Mental Health Act. An amendment was made in 1997 regarding involuntary treatment of persons with criminal records and in 2000 regarding coercive actions. The other laws are Specialized Health Care Act, Public Health Act, Social Welfare Act and The Law of Patient’s Rights. In Finland, there are two national laws that deal with the forensic psychiat-ric services: the Penal Code (1889, amended 2003) and the Mental Health Act (1990) with the Mental Health Decree (1990). While the Mental Health Act defines when and how patients can be committed into mental hospitals involuntarily, according to the Finnish Law, the courts decide if a forensic psychiatric evaluation should be conducted. In many cases of violent acts, the court asks the National Authority of Medicolegal Affairs to arrange for an evaluation.The latest legislation was enacted in 1990.
Mental Health Financing There are budget allocations for mental health.Details about expenditure on mental health are not available.The primary sources of mental health financing in descending order are tax based, social insurance, out of pocket expenditure by the patient or family and private insurances.One special feature of the Finnish health care system, since the state subsidy reform in 1993, is that its financing is much decen-tralized. The financial units are the municipalities which total 450, with an average size of 6000 people. The biggest municipality is Helsinki, with half a million people, but the smallest have only a few hundred inhabitants. Despite this, every municipality has the responsibility to provide all health care, including the most specialized, to their inhabitants, either by organizing this themselves or by buying it from health care districts, other municipalities or private providers. The municipalities have the right to collect their own taxes. The other part of the needed money comes to municipalities as a state subsidy, but without any specific earmarking for health. This has led to increasing regional and local differences in the provision of mental health care, e.g. the differences between health care districts in the annual prevalence of hospital treated patients was twofold in 2002. The differences between municipali-ties were even greater. The same is true for the numbers of outpatient personnel: the difference between the districts was three-fold in this respect in 1999.The country has disability benefits for persons with mental disorders.

© 2005 World Health OrganizationMental Healthatlas
195
E –
I
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is available at the primary level. Mainly, emergency treatment of severe mental disorders is available at the primary level.Regular training of primary care professionals is not carried out in the field of mental health. Mental health is a part of basic training for physicians and nurses, however, systematic further education is not provided to primary care workers in mental health.There are community care facilities for patients with mental disorders. Mental health services are primarily organized as community-based outpatient services. According to available data, the deinstitutionalization process was in the balance during the 1980s. The decrease in the number of psychiatric beds was compensated for by increasing outpatient resources and by developing community-based care, e.g. the personnel in outpatient care doubled from 1982 to 1992. The main problem in implementing community care is the scarcity of supporting services for long-term patients living in general communities. There is a need for more supported housing, day centres, support persons and guided leisure activities; patients’ families also need more help and support. In recent years, there has in fact been a slight increase in these services. Extramural rehabilitative facilities used to be provided mainly by the public health sector and a few semi-private foundations. In the 1990s, a large number of private complimentary services were founded, and now they provide nearly 90% of all extramural residential services. Currently, nearly as many patients stay in such facilities as in psychiat-ric hospitals. However, the standard of care in such facilities is variable as the control of authorities over such institutions is weak.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 10Psychiatric beds in mental hospitals per 10 000 population 0Psychiatric beds in general hospitals per 10 000 population 9Psychiatric beds in other settings per 10 000 population 1Number of psychiatrists per 100 000 population 22Number of neurosurgeons per 100 000 population 1Number of psychiatric nurses per 100 000 population 180Number of neurologists per 100 000 population 4Number of psychologists per 100 000 population 79Number of social workers per 100 000 population 150
Mental health services are organized around the concept of catchment areas, which are currently governed by health care districts (HCD). Roughly two-fifths of psychiatric services, mostly outpatient care, has been moved administratively to primary care in many districts. Most psychiatric wards belong to the administration of general hospitals. Other settings include state hospital beds for forensic psychiatry, prisoners, military psychiatric wards, psychiatric wards in primary care and in private hospitals. Traditionally, the mental health care system has been hospital-centred, and the deinstitutionalization process started later than in many other developed countries. At the beginning of the 1980s, Finland still had about 20 000 psychiatric beds, almost all situated in separate psychiatric hospitals. A specific feature of the Finnish situation, however, was that there never were really big hospitals; beds are spread between 60 hospitals located all over the country, and no hospital has more than 300 beds. During the last two decades, a substantial (75%) reduction in the number of beds in psychiatric institutions has occurred. The 1990 Mental Health Act forbade the treatment of minors in the same wards as adults, so the Health Care districts had to build separate units for adolescents run by ado-lescent psychiatrists. Hospital services for adolescents and children are separated, though they may be provided together with out-patient services. The Finnish mental health care system is characterized by teamwork (usual outpatient team comprises of psychia-trist, psychologist, psychiatric nurses and social worker). One prerequisite for this cooperation is the high standard of training among all personnel, so that all staff groups can participate in this cooperation on an equal basis. For instance, many nurses have received formal training in psychotherapy, especially family therapy. At the municipality level, local mental health work is often organized on a multidisciplinary basis. Currently there is a shortfall of psychiatrists by about one-third of the requirement, despite the intensified programme for training of psychiatrists since 1980s. Four psychiatric specialities are recognized: general psychiatry, child psychiatry, adolescent psychiatry and forensic psychiatry. About one-fifth of psychiatrists work as private practitioners only and one-third of psychiatrists working in the public sector have part-time private practice.
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in advocacy, promotion, prevention, treatment and rehabilitation. The Finnish Mental Health Association is the world’s oldest NGO in the mental health field.
Information Gathering System There is mental health reporting system in the country. The Ministry of Social Affairs and Health biannually sends a social and health report to the parliament and mental health is incorporated in it.The country has data collection system or epidemiological study on mental health. A large national epidemiological health examina-tion study (Health 2000) was conducted in 2000. A central finding was that the prevalence of mental disorders is at present the same as twenty years before. Finland has a care register for institutional social and health care, including mental health, for service data collection.
FINLAND

© 2005 World Health OrganizationMental Healthatlas
196
E –
I
Programmes for Special Population The country has specific programmes for mental health for refugees, disaster affected popu-lation, elderly and children. The Finnish National Schizophrenia Project, which was carried out in the 1980s, recommended that ‘acute psychosis’ teams should be established in every catchment area. Their task would be to take care of new psychotic patients in the area by active initial inter-vention which, whenever possible, includes family participation. The 10-year follow-up of the Project, focusing on the year 1992, verified that most of the catchment areas had established these multi-disciplinary teams. In the last few years, the Government has allocated special resources for the development of services for children and adolescents. Financing of psychotherapy for children and adolescents has also increased. Specialized outpatient departments and a few wards in mental hospitals have been created for substance abuse patients. In the last few years, the Government has allocated funds for expanding such services and extending it also to primary care. There is still, however, a shortage of rehabilitative services for chronic drug users. For forensic patients, who are judged to be not criminally responsible and in need of treatment, hospitalization usually starts at either of the two state mental hospitals. After discharge the patient is under supervision for the initial 6 months and is assessed regularly at a municipal psychiatric centre, since there are no specific forensic psychiatric outpatient treatment facilities in Finland. After this period he has no other obli-gations to the judicial system and can continue treatment, if required, as any other psychiatric patient.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, ethosuximide, phenytoin sodium, sodium valproate, amitriptyline, chlorpromazine, diazepam, fluphenazine, haloperidol, lithium, biperiden, carbidopa, levodopa.Fluphenazine is available only as a decanoate injection. Medicines for outpatients are dispensed from private pharmacies and not by the Government or institutions.
Other Information Social welfare and health care are integrated at the national and provincial levels. At the national level, the Ministry of Social Affairs and Health has the highest administrative responsibility, and STAKES (National Research and Development Centre for Welfare and Health) is the active agent in the field of research and development activities. In every provincial administra-tion, there is a Department for Social Affairs and Health. At municipal level, the models and degree of cooperation vary. In some, the social welfare and primary health care services are joined both at the administrative as well as at the practical level. In others, they still work separately from each other, although there has been, especially during the 1990s, an increasing tendency to achieve stronger integration. One practical example of increasing multi-sectoral cooperation in the area of mental health work has been the development programme called ‘Meaningful Life’. This nation-wide programme from 1998-2002, the aim of which was to improve the quality of life for people suffering from mental disorders or their consequences, operated at national, regional and local levels. It has a genuinely multi-sectoral approach, as almost all ministries are participating in its steering group. The main target areas in the field of mental health promotion have been: enhancement of the value and visibility of mental health; development of mental health indicators; promotion of mental health in children and adolescents; in old age; in relation to working life and employment policy and the use of telematics in mental health promotion and substance abuse prevention. Mental health and its promotion have been stressed both in the new health strategy ‘Health for 2015’, as well in the governmental Goal and Action Plan for Social Welfare and Health Care 2004-2007. A national project to secure the future of health care services started in 2002 and a national development project for social services started in 2003. Both projects are financed and coordinated by the Ministry of Social Affairs and Health. The main priority is regional development of mental health work.
Additional Sources of InformationEronen, M. Repo, E., Vartiainen, H., et al (2000) Forensic psychiatric organization in Finland. International Journal of Law and Psychiatry, 23, 541-546.
Korkeila, J. (1998) Perspectives on the Public Psychiatric Services in Finland – Evaluating the Deinstitutionalization Process. National Research and Development Centre for Welfare and Health – Finland.
Lahtinen, E., Lehtinen, V., Riikonen, E., et al (1999) Framework for Promoting Mental Health in Europe. National Research and Development Centre for Welfare and Health – Finland.
Lavikainen J, Lahtinen E, Lehtinen V. (2000) Public Health Approach to Mental Health in Europe – A Report Prepared Within the EU-Funded Project on Putting Mental Health on the European Agenda. Ministry of Social Affairs and Health.
Ministry of Social Affairs and Health (1987) Health for All by the Year 2000 – The Finnish National Strategy.
Ministry of Social Affairs and Health (1993) Health for All by the Year 2000 – Revised Strategy for Cooperation.
Ministry of Social Affairs and Health (1997) Finnish Drug Policy Committee.
Ministry of Social Affairs and Health (1998) Third Evaluation of Progress Towards Health for All – Finland.
Ministry of Social Affairs and Health (2001) Government Resolution on the Health 2015 Public Health Programme
Ministry of Social Affairs and Health (2004) Government Resolution on a drug Policy Action Program in Finland 2004-2007.
National Board of Medicolegal Affairs (1997) Amending the Mental Health Act.
Quality Recommendations for Mental Health Services (2001) Ministry of Social Affairs and Health.
Salokangas, R. K. R. (2004) Psychiatric specialist care in Finland-achievements and challenges. Journal of Mental Health, 13, 47-54.
FINLAND

© 2005 World Health OrganizationMental Healthatlas
197
E –
I
FranceGENERAL INFORMATIONFrance is a country with an approximate area of 552 thousand sq. km. (UNO, 2001). Its population is 60.434 million, and the sex ratio (men per hundred women) is 95 (UNO, 2004). The proportion of population under the age of 15 years is 18% (UNO, 2004), and the proportion of population above the age of 60 years is 20% (WHO, 2004). The literacy rate is 99% for men and 99% for women (UNESCO/MoH, 2004).The country is a high income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 9.6%. The per capita total expenditure on health is 2567 international $, and the per capita government expenditure on health is 1951 international $ (WHO, 2004).The main language(s) used in the country is (are) French. The largest ethnic group(s) is (are) Celtic, Latin and Teutonic., and the other ethnic group(s) are (is) Slavic, North African and Southeast Asian. The largest religious group(s) is (are) Roman Catholic.The life expectancy at birth is 76 years for males and 83.6 years for females (WHO, 2004). The healthy life expectancy at birth is 69 years for males and 75 years for females (WHO, 2004).
EPIDEMIOLOGYThere is substantial epidemiological data on mental illnesses in France in internationally accessible literature. No attempt was made to include this information here.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is present. The policy was initially formulated in 1960.The components of the policy are advocacy, promotion, prevention, treatment and rehabilitation. Details can be obtained from the circulars of 1960, 1990 and 1992.
Substance Abuse Policy A substance abuse policy is present. The policy was initially formulated in 1970.
National Mental Health Programme A national mental health programme is present. The programme was formulated in 1985.France has a comprehensive national suicide prevention programme and more recently a programme titled ‘Actions against Depression.’
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. Details about the year of formulation are not available.
Mental Health Legislation The latest legislation deals with admission under constraints in psychiatric hospitals. The law is due for modification in 2005 following a thorough evaluation.The latest legislation was enacted in 1990.
Mental Health Financing There are budget allocations for mental health.The country spends 8% of the total health budget on mental health.The primary sources of mental health financing in descending order are social insurance and tax based.Much of mental health care including psychotherapy of long duration is financed by social security system. Patients have free access to private or public mental health professionals of their choice. The cost of private treatment is partly financed by the social security system (fully for severe mentally ill and severely deprived patients) and partly through private insurance. However, psychotherapy by psychologists and many psychoanalysts working in the private sector are not financed by social security.The country has disability benefits for persons with mental disorders. There are allowances for handicapped people under the law from 1975. There are also some housing benefits for them.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is available at the primary level. Regular training of primary care professionals is carried out in the field of mental health. There are community care facilities for patients with mental disorders.

© 2005 World Health OrganizationMental Healthatlas
198
E –
I
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 12Psychiatric beds in mental hospitals per 10 000 population 7Psychiatric beds in general hospitals per 10 000 population 3Psychiatric beds in other settings per 10 000 population 2Number of psychiatrists per 100 000 population 22Number of neurosurgeons per 100 000 population Number of psychiatric nurses per 100 000 population 98Number of neurologists per 100 000 population Number of psychologists per 100 000 population 5Number of social workers per 100 000 population
The public sector is responsible for sectorization and includes more than 80% of the inpatient facilities. However, there is a 5-10 fold variation in the manpower and structural resources between sectors. The private sector is also involved in sectorization but to a much smaller degree. Bed reduction is proceeding. In the 1990s, 20% of beds were reduced. General physicians manage most of the minor psychiatric illnesses, with psychiatrists providing expert opinions whenever consulted. Though psychiatrists work in close cooperation with other doctors a true liaison service involving multidisciplinary treatment approach is not yet fully developed. More than half of the psychiatrists have a private practice or are working in private institutions. A large proportion of private psychiatrists are exclusively practicing psychotherapy. Psychiatrists are concentrated in big cities, with posts lying vacant in rural areas and in northern regions. There is likely to be reduction in the number of psychiatrists due to a decrease in the number of medical students allowed to train in psychiatry. Most psychologists work in the private sector.
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in advocacy, promotion, prevention, treatment and rehabilitation. Families began to take an active role in psychiatric management and pro-gramme development since 1970 and are involved in advocacy, prevention and promotion and participation in different boards as representatives of consumers.
Information Gathering System There is mental health reporting system in the country. The country has data collection system or epidemiological study on mental health. A new information system collecting data on hospital activity is currently being implemented (PMSI, Programme de Médicalisation des Systèmes d’Information). Psychiatric diagnoses of adult patients are made according to ICD-10 criteria, but patients younger than 20 years are still categorized according to French classification of child psychiatry.
Programmes for Special Population The country has specific programmes for mental health for disaster affected population, eld-erly and children. A national programme ‘Mental health: the user at the core of an organization in need of renovation’ was launched in 2001 to pro-mote campaigns against stigma, reinforce patients’ rights, improve professional practices, prevention and rehabilitation programmes and community psychiatry.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, ethosuximide, phenobarbital, sodium valproate, amitriptyline, chlorpromazine, diazepam, fluphenazine, haloperidol, lithium, biperiden, carbidopa, levodopa.
Other Information Psychiatric services in France have been defined according to the legislation of 1838, when it was decided to have one hospital per Département. The first open unit was set up in 1920 and the first outpatient unit in 1930. The concept of sectorization, where one team would be responsible for both inpatient and outpatient care of persons within its parameters, was conceptualized during the second world war, but was fully implemented only after necessary laws were passed in 1986. Each sector (there are about 1000 sectors in France) consists of inpatient, outpatient, community care and sheltered workshops. There are differ-ent sectors for adult psychiatry, child and adolescent psychiatry and forensic psychiatry.
Additional Sources of InformationJaeger, M. (1995) Inflections in France’s Mental Health Policy. Santé Mentale au Quebec, 20, 77-87.
Provost, D., Bauer, A. (2001) Trends and developments in public psychiatry in France since 1975. Acta Psychiatrica Scandinavica, 104 (suppl. 410), 63-68.
Verdoux, H. (2003) Psychiatry in France. International Journal of Social Psychiatry, 49, 83-86.
FRANCE
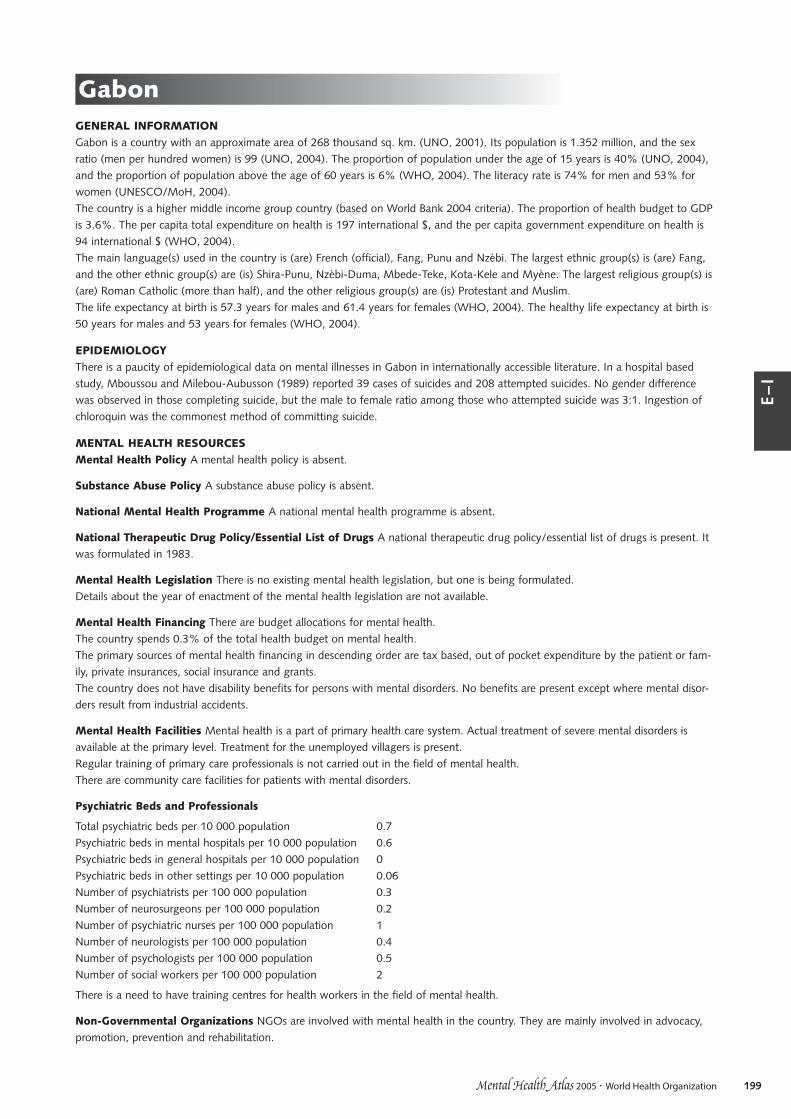
© 2005 World Health OrganizationMental Healthatlas
199
E –
I
GabonGENERAL INFORMATIONGabon is a country with an approximate area of 268 thousand sq. km. (UNO, 2001). Its population is 1.352 million, and the sex ratio (men per hundred women) is 99 (UNO, 2004). The proportion of population under the age of 15 years is 40% (UNO, 2004), and the proportion of population above the age of 60 years is 6% (WHO, 2004). The literacy rate is 74% for men and 53% for women (UNESCO/MoH, 2004).The country is a higher middle income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 3.6%. The per capita total expenditure on health is 197 international $, and the per capita government expenditure on health is 94 international $ (WHO, 2004).The main language(s) used in the country is (are) French (official), Fang, Punu and Nzèbi. The largest ethnic group(s) is (are) Fang, and the other ethnic group(s) are (is) Shira-Punu, Nzèbi-Duma, Mbede-Teke, Kota-Kele and Myène. The largest religious group(s) is (are) Roman Catholic (more than half), and the other religious group(s) are (is) Protestant and Muslim.The life expectancy at birth is 57.3 years for males and 61.4 years for females (WHO, 2004). The healthy life expectancy at birth is 50 years for males and 53 years for females (WHO, 2004).
EPIDEMIOLOGYThere is a paucity of epidemiological data on mental illnesses in Gabon in internationally accessible literature. In a hospital based study, Mboussou and Milebou-Aubusson (1989) reported 39 cases of suicides and 208 attempted suicides. No gender difference was observed in those completing suicide, but the male to female ratio among those who attempted suicide was 3:1. Ingestion of chloroquin was the commonest method of committing suicide.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is absent.
Substance Abuse Policy A substance abuse policy is absent.
National Mental Health Programme A national mental health programme is absent.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. It was formulated in 1983.
Mental Health Legislation There is no existing mental health legislation, but one is being formulated.Details about the year of enactment of the mental health legislation are not available.
Mental Health Financing There are budget allocations for mental health.The country spends 0.3% of the total health budget on mental health.The primary sources of mental health financing in descending order are tax based, out of pocket expenditure by the patient or fam-ily, private insurances, social insurance and grants.The country does not have disability benefits for persons with mental disorders. No benefits are present except where mental disor-ders result from industrial accidents.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is available at the primary level. Treatment for the unemployed villagers is present.Regular training of primary care professionals is not carried out in the field of mental health. There are community care facilities for patients with mental disorders.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 0.7Psychiatric beds in mental hospitals per 10 000 population 0.6Psychiatric beds in general hospitals per 10 000 population 0Psychiatric beds in other settings per 10 000 population 0.06Number of psychiatrists per 100 000 population 0.3Number of neurosurgeons per 100 000 population 0.2Number of psychiatric nurses per 100 000 population 1Number of neurologists per 100 000 population 0.4Number of psychologists per 100 000 population 0.5Number of social workers per 100 000 population 2
There is a need to have training centres for health workers in the field of mental health.
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in advocacy, promotion, prevention and rehabilitation.

© 2005 World Health OrganizationMental Healthatlas
200
E –
I
Information Gathering System There is no mental health reporting system in the country. The national health reporting system is being finalized.The country has no data collection system or epidemiological study on mental health. There is a lack of logistics to allow such data collection.
Programmes for Special Population The country has specific programmes for mental health for indigenous population. Due to a lack of technical people and resources it is not possible to have services for all special groups of population.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, phenobarbital, phenytoin sodium, amitriptyline, chlorpromazine, diazepam, fluphenazine, haloperidol.
Other Information
Additional Sources of InformationMboussou, M., Milebou-Aubusson, L. (1989) Suicides and attempted suicides at the Jeanne Ebori Foundation, Libreville (Gabon). Médecine Tropicale, 49, 259-264.
GABON

© 2005 World Health OrganizationMental Healthatlas
201
E –
I
GambiaGENERAL INFORMATIONGambia is a country with an approximate area of 11 thousand sq. km. (UNO, 2001). Its population is 1.462 million, and the sex ratio (men per hundred women) is 98 (UNO, 2004). The proportion of population under the age of 15 years is 40% (UNO, 2004), and the proportion of population above the age of 60 years is 6% (WHO, 2004). The literacy rate is 43.7% for men and 29.7% for women (UNESCO/MoH, 2004).The country is a low income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 6.4%. The per capita total expenditure on health is 78 international $, and the per capita government expenditure on health is 39 interna-tional $ (WHO, 2004).The main language(s) used in the country is (are) English. The largest religious group(s) is (are) Muslim, and the other religious group(s) are (is) Christian.The life expectancy at birth is 55.4 years for males and 58.9 years for females (WHO, 2004). The healthy life expectancy at birth is 48 years for males and 50 years for females (WHO, 2004).
EPIDEMIOLOGYThere is a paucity of epidemiological data on mental illnesses in Gambia in internationally accessible literature. There are two studies on Sierra Leonean (Fox & Tang, 2000) and Senegalese (Tang & Fox, 2001) refugees living in Gambian refugee camps. The Harvard Trauma Questionnaire and the Hopkins Symptom Checklist-25 were used as survey instruments. High prevalence of anxiety, depres-sion and PTSD was found among the exposed population.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is absent.The Department of State for Health and Social Welfare in collaboration with the WHO is in the process of developing a national mental health policy. The draft of the policy document is now ready for a final review by an expert committee, prior to its final sub-mission for approval of the cabinet.
Substance Abuse Policy A substance abuse policy is absent.
National Mental Health Programme A national mental health programme is present. The programme was formulated in 1992.The national mental health programme was developed with the technical assistance of the Voluntary Services Overseas (Country Office) through the support of the British Government.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. It was formulated in 1996.
Mental Health Legislation There is a Mental Health Act. It was last amended in 1964. There is a need for an updated legislation.The latest legislation was enacted in 1924.
Mental Health Financing There are no budget allocations for mental health.Details about expenditure on mental health are not available.The primary source of mental health financing is grants.The country has disability benefits for persons with mental disorders.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is available at the primary level. Treatment is available and mental health is being integrated into the primary health system.Regular training of primary care professionals is carried out in the field of mental health. A good number of doctors and nurses were trained on the diagnosis, treatment and management of mental health disorders through WHO support last year. Some traditional healers have also been trained.There are community care facilities for patients with mental disorders. There is a community mental health service that conducts country wide mental health promotional activities.

© 2005 World Health OrganizationMental Healthatlas
202
E –
I
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 0.78Psychiatric beds in mental hospitals per 10 000 population 0.78Psychiatric beds in general hospitals per 10 000 population 0Psychiatric beds in other settings per 10 000 population 0Number of psychiatrists per 100 000 population 0.08Number of neurosurgeons per 100 000 population 0.06Number of psychiatric nurses per 100 000 population 0Number of neurologists per 100 000 population 0Number of psychologists per 100 000 population 0Number of social workers per 100 000 population 0.08
There are 2 assistant occupational therapists.
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in promotion and prevention.
Information Gathering System There is no mental health reporting system in the country. The country has no data collection system or epidemiological study on mental health.
Programmes for Special Population The country has specific programmes for mental health for children.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, phenobarbital, phenytoin sodium, amitriptyline, chlorpromazine, diazepam, fluphenazine, haloperidol, biperiden.The essential drug list was formulated in 2001, and it will be reviewed again in 2004-2005. Some of the drugs are not always avail-able at primary level, but these are always available at the secondary and tertiary levels.
Other Information
Additional Sources of InformationFox, S. H., Tang, S. S. (2000) The Sierra Leonean refugee experience: traumatic events and psychiatric sequelae. Journal of Nervous & Mental Disease, 188, 490-495.
Tang, S. S., Fox, S. H. (2001) Traumatic experiences and the mental health of Senegalese refugees. Journal of Nervous & Mental Disease 189, 507-512.
GAMBIA

© 2005 World Health OrganizationMental Healthatlas
203
E –
I
GeorgiaGENERAL INFORMATIONGeorgia is a country with an approximate area of 70 thousand sq. km. (UNO, 2001). Its population is 5.074 million, and the sex ratio (men per hundred women) is 91 (UNO, 2004). The proportion of population under the age of 15 years is 14% (UNO, 2004), and the proportion of population above the age of 60 years is 19% (WHO, 2004). The literacy rate is 100% for men and 98% for women (UNESCO/MoH, 2004).The country is a lower middle income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 3.6%. The per capita total expenditure on health is 108 international $, and the per capita government expenditure on health is 41 international $ (WHO, 2004).The main language(s) used in the country is (are) Georgian. The largest ethnic group(s) is (are) Georgian (seven-tenths), and the other ethnic group(s) are (is) Armenian and Russian. The largest religious group(s) is (are) Georgian Orthodox Christian (two-thirds), and the other religious group(s) are (is) Russian Orthodox Christian and Muslim.The life expectancy at birth is 68.4 years for males and 75 years for females (WHO, 2004). The healthy life expectancy at birth is 62 years for males and 67 years for females (WHO, 2004).
EPIDEMIOLOGYThere is a paucity of epidemiological data on mental illnesses in Georgia in internationally accessible literature. Tchanturia et al (2002) held focus groups of various health professionals to establish how eating disorders present in Georgia and to identify groups perceived to be at high risk of having an eating disorder. They assessed 245 women from these identified high risk groups with translated versions of a number of standardized questionnaires (measuring eating and general psychopathology) and a sub-sample with a structured clinical interview. They estimated from the responses to the questionnaires that as many as 5% of the sample may have clinically significant bulimia nervosa, 7% fell in the weight range for anorexia nervosa with a further 7% in the weight range for obesity. Interviews with the high scoring group confirmed the presence of clinically significant eating pathology in the majority of those identified as possible cases. Georgia was one of the countries included in the study to assess changing patterns of suicide in different countries of erstwhile USSR during the period 1984-90 (Wasserman et al, 1998). There was wide variation in suicide rates across the countries with a decrease in rate after 1986. The suicide rates in the Caucasus (Georgia, Azerbaijan and Armenia) region was 3.5 cases per 100 000 inhabitants during 1984-1990 with the rates for men and women being 4.9 and 2.1 per 100 000 inhab-itants, respectively. Chubarovskii and Loginova (1986) did a comparative clinico-epidemiological study to assess borderline mental disorders in adolescents living in Moscow and Batumi. Borderline disorders were correlated with maladaptive schooling. Cultural fac-tors were found to affect the severity and direction of adolescent reactions.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is present. The policy was initially formulated in 1999.The components of the policy are prevention, treatment and rehabilitation. Mental health is one of the priorities of Georgia’s National Health Policy document of 1999. Various issues pertinent to mental health policy are discussed in other documents like the 1999 presidential decree ‘Improving Psychiatric Services in Georgia’.
Substance Abuse Policy A substance abuse policy is present. The policy was initially formulated in 1996.
National Mental Health Programme A national mental health programme is present. The programme was formulated in 1995.The Strategic Health Plan for 2000-2009 outlined specific measures for mental health care development. Georgia also has a national suicide prevention initiative. The implementation of the Strategic Plan was limited by the lack of resources.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. It was formulated in 1995.
Mental Health Legislation The mental health legislation is known as Law on Mental Health Assistance. Enforcement of the law is impeded at times due to funding shortfalls. Georgia has elected to enforce participation in continuing medical education pro-grammes on the part of physicians through law to help speed up the implementation process.The latest legislation was enacted in 1995.
Mental Health Financing There are budget allocations for mental health.Details about expenditure on mental health are not available.The primary source of mental health financing is tax based.Psychiatric services are jointly financed by the health insurance programme and central budget transfers. State funding is supposed to provide for the inpatient treatment of mentally ill offenders, acute psychotics, patients with posttraumatic stress disorders and those without a family, for the outpatient treatment of psychotic patients and those with chronic disorders prone to frequent exac-erbations. In reality, state funding is limited and provides for a few cheap medicines from the essential drug list. Limited funding has impeded the provision of even the inpatient services, where shortage of food is also known to occur. Between 1991 and 1995 about

© 2005 World Health OrganizationMental Healthatlas
204
E –
I
800 psychiatric patients died in mental hospitals due to lack of food, medication and/or care as a result of the civil war and the eco-nomic crisis. Even now the premature death rate of inpatients is as high as in other low income countries.The country has disability benefits for persons with mental disorders.
Mental Health Facilities Mental health is not a part of primary health care system. Actual treatment of severe mental disorders is not available at the primary level. Actual treatment is carried out in hospitals and outpatient clinics.Regular training of primary care professionals is not carried out in the field of mental health. Primary care is mainly provided by spe-cialists. An integrated model of family medicine is not operational.There are no community care facilities for patients with mental disorders.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 2.1Psychiatric beds in mental hospitals per 10 000 population 2Psychiatric beds in general hospitals per 10 000 population 0Psychiatric beds in other settings per 10 000 population 0.1Number of psychiatrists per 100 000 population 6Number of neurosurgeons per 100 000 population 0.6Number of psychiatric nurses per 100 000 population 24Number of neurologists per 100 000 population 13Number of psychologists per 100 000 population Number of social workers per 100 000 population 0
There are no institutions for training of social workers. Between 1990 and 1995, the bed strength was brought down from 5000 to about 1000 due to shortage of resources. However, even now most of the beds are housed in old asylums, often distant from fami-lies and homes. Some beds have been earmarked for drug addiction and forensic services. Staff remunerations are extremely poor (a psychiatrist’s monthly salary is the equivalent of $30-50 and a nurse’s about $17-20). About 15 child psychiatrists are available. Psychotherapists, occupational therapists and social workers are not officially recognized by the Government and are not registered. Every physician has to pass a CME course lasting 3-4 months every five years.
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in advo-cacy, promotion, prevention and rehabilitation. A few community-based services have been established by NGOs and donors from abroad. NGOs receive only occasional and very limited support from the Government. International humanitarian aid organizations provide some support through the supply of medicines (International Red Cross), food (World Food Programme) and other means (e.g. operational repairs by the Investment Fund of Georgia).
Information Gathering System There is mental health reporting system in the country. The country has no data collection system or epidemiological study on mental health. No epidemiological research has been carried out over the last 6 years due to lack of funds.
Programmes for Special Population The country has specific programmes for mental health for refugees and children.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, amitriptyline, chlorpromazine, diazepam, fluphenazine, haloperidol, lithium, biperiden. The medicines are distributed free of charge under the State Programme on Mental Health Assistance.
Other Information
Additional Sources of InformationChubarovskii, V. V., Loginova, M. S. (1986) Clinico-epidemiologic characteristics of borderline mental disorders comparison of the Moscow and Batumi populations of students of specialized educational institutions. Zhurnal Nevropatologii i Psikhiatrii Imeni S-S-Korsakova, 86, 1203-1208.
Sharashidze, M., Naneishvili, G., Silagadze, T., et al (2004) Georgia mental health profile. International Review of Psychiatry, 16, 107-116.
Tchanturia, K., Katzman, M., Troop, N. A., et al (2002) An exploration of eating disorders in a Georgian sample. International Journal of Social Psychiatry, 48, 220-230.
Wasserman, D., Varnik, A., Dankowicz, M. (1998) Regional differences in the distribution of suicide in the former Soviet Union during perestroika, 1984-1990. Acta Psychiatrica Scandinavica, Supplementum 394, 5-12.
GEORGIA

© 2005 World Health OrganizationMental Healthatlas
205
E –
I
GermanyGENERAL INFORMATIONGermany is a country with an approximate area of 357 thousand sq. km. (UNO, 2001). Its population is 82.526 million, and the sex ratio (men per hundred women) is 96 (UNO, 2004). The proportion of population under the age of 15 years is 15% (UNO, 2004), and the proportion of population above the age of 60 years is 24% (WHO, 2004). The literacy rate is 99% for men and 99% for women (UNESCO/MoH, 2004).The country is a high income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 10.8%. The per capita total expenditure on health is 2820 international $, and the per capita government expenditure on health is 2113 international $ (WHO, 2004).The main language(s) used in the country is (are) German and English. The largest ethnic group(s) is (are) German, and the other ethnic group(s) are (is) Turkish and Russian. The largest religious group(s) is (are) Protestant, and the other religious group(s) are (is) Roman Catholic, Muslim and Jew.The life expectancy at birth is 75.6 years for males and 81.6 years for females (WHO, 2004). The healthy life expectancy at birth is 70 years for males and 74 years for females (WHO, 2004).
EPIDEMIOLOGYThere is substantial epidemiological data on mental illnesses in Germany in internationally accessible literature. No attempt was made to include this information here.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is present. The policy was initially formulated in 1975.The components of the policy are advocacy, promotion, prevention, treatment and rehabilitation. Mental health policy in Germany is essentially based on two important documents. In 1975, a relevant Study Commission submitted to the German Parliament, the Bundestag, a report (Psychiatrie Enquête) about the situation of psychiatry in the Federal Republic of Germany, which pointed out the main targets of a psychiatry reform. In 1988, an Expert Commission reported on the first results of the reform and formulated further needs to go on with the reform process of mental health services. Coordinating psychiatric services, an orientation towards community-based care, the availability of mental health services for all those in need and policies to give mental disorders the same status as somatic illnesses were the main requirements. As a consequence, the Federal Government initiated a huge pilot programme in the field of psychiatry. Based on the results of this pilot programme, in which a host of individual projects were financed by the Federal Government until the end of 2002, mental health policy nowadays intends to provide a networked treatment which caters to the individual needs of the patient. In 2002, the Federal Ministry of Health and Social Security re-established a working group for the further development of psychiatric care in Germany. It consists of representatives of all the main players in the field of psychiatry, including physicians, professional associations, ‘users’ and family representatives as well as competent institutions and representa-tives of health insurances.
Substance Abuse Policy A substance abuse policy is present. The policy was initially formulated in 1990. In June 2003, the Federal Cabinet approved the ‘Action Plan on Drugs and Addiction’, presented by the Federal Drug Commissioner. Devised to serve as a framework for addiction policy for the next 5-10 years, it replaced the ‘Plan to combat drugs’ of 1990. It is meant to contribute ‘to changing health awareness and to avoiding harmful consumption or at least reduce it’. It is based on the four pillars of the national drug and addiction policy (prevention of drug consumption, offering advice and treatment to consumers, survival assistance and harm reduction, repression and supply reduction). Compared to the plan of 1990, legal drugs have been taken more into considera-tion and that new elements of care (internet offers, consumption rooms) have been included. Alongside a number of targets that involve influencing the consumption of illegal drugs indirectly by preventing tobacco use, the plan relates also specifically to drugs. For instance, it includes the demand to avoid, or at least reduce, the consumption of illegal drugs by referring to the special risks of infection – especially Hepatitis C – and possible damages to the brain through synthetic drugs. Moreover, individual target groups (children of addicted parents, high-risk groups, car drivers, polydrug users) are to be treated specifically.
National Mental Health Programme A national mental health programme is absent.Due to the decentralized German health system, a national mental health programme in the narrower sense does not exist. However, boards for coordinating and planning mental health services and policy are in place on the federal, state and local levels. The key players in mental health policy are the States (Länder). Most of them have formulated a central psychiatric planning docu-ment (Psychiatrie-Plan). A ‘National Programme for the Prevention of Suicide exacerbations’ was launched in 2002 by the German Society for Suicide Prevention. In addition, a national programme for the destigmatization of mental illness is currently being planned jointly by the German Ministry of Health and Social Security, the German Association for Psychiatry, Psychotherapy and Neurology and the initiative ‘Open the Doors’ of the WPA.
National Therapeutic Drug Policy/Essential List of Drugs Details about the national therapeutic drug policy/essential list of drugs are not available.

© 2005 World Health OrganizationMental Healthatlas
206
E –
I
Mental Health Legislation The Federal Government has an important frame-setting role, especially by providing the social and welfare legislation laid down in several Social Code Books. Some provisions deal with the special needs of mentally ill persons, oth-ers, while crucial for the interests of psychiatric patients interests, are of a general nature and not specific to this group (e.g. referring to rehabilitation, nursing care or welfare legislation). Special legislation as well as planning and coordinating mental health policy is mainly the responsibility of the States, and they have mental health legislations of their own. These also contain provisions on com-pulsory referral and involuntary treatment.The latest legislation was enacted in 1999.
Mental Health Financing There are budget allocations for mental health.Details about expenditure on mental health are not available.The primary sources of mental health financing in descending order are social insurance, private insurances, tax based and out of pocket expenditure by the patient or family.Specific budget allocations do not exist for the field of health in general. The health system is financed in a concerted system, in which all services that are medically necessary and are performed in a cost-effective manner are covered by the statutory or private health insurance. In this regard, the social law as the legal basis of this principle does not distinguish between the treatment of somatic diseases and mental illnesses. Rehabilitation is financed by the health insurance or the statutory pension insurance or – if necessary – by the social welfare system. Self-employed psychiatrists are paid on a fee-for-service basis in a strictly regulated market with semi-statutory professional associations exerting stringent control and negotiating fees with health insurance organizations.The country has disability benefits for persons with mental disorders. There are Disability IDs, disability compensation schemes, com-pensations for accidents, schemes for tax reductions, free transportation and other rehabilitation facilities.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is available at the primary level. Regular training of primary care professionals is not carried out in the field of mental health. There are community care facilities for patients with mental disorders. Community-based care is provided as a part of the psychiatric reforms. The crucial step towards its implementation was taken with the creation of the Expert Commission on mental health care in 1970 to 1975. This effort was encouraged further by the recommendations of the Central Institute of Mental Health of Baden-Württemberg and the expert commission for the Federal Republic of Germany. Funding came from by the Federal Government as well as States and local bodies. At present, there are almost 9000 places in nearly 360 day-clinics and more than 15 000 beds for rehabilitative services. Currently, the population of people with mental illness in sheltered homes is approximately equal to the number of beds in psychiatric inpatient services. Implementation of the programme, however, varies across different regions. The involvement of family members and ex-users, newly organized in groups to design several forms of activity, has proven extremely useful. However, there is no one agency that has overall responsibility for community mental health care in a given catchment area. Since 2000, pilot projects involving mental health services in 35 catchment areas, covering 10% of the population, have pursued the comprehensive care planning for individual patients involving local authority social services which fund approximately half of mental health care.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 7.5Psychiatric beds in mental hospitals per 10 000 population 4.5Psychiatric beds in general hospitals per 10 000 population 2.9Psychiatric beds in other settings per 10 000 population Number of psychiatrists per 100 000 population 11.8Number of neurosurgeons per 100 000 population 1.5Number of psychiatric nurses per 100 000 population 52Number of neurologists per 100 000 population 3.4Number of psychologists per 100 000 population 51.5Number of social workers per 100 000 population 477
The figure for psychiatrists includes specialists in psychosomatics and psychotherapy. The figure for psychologists is an estimate of only employees. The figure for social workers refers to all related professions, not only social workers in a narrow sense (only employees). Since the late 1960s, psychiatric hospitals have reduced their beds by about 50 % and one psychiatric hospital was closed. A 15% reduction was recorded even after 1999. More than 220 general psychiatry units have opened. There is, however, significant regional variation in the number of beds. Staffing and funding of inpatient facilities is now based on the type of patients in a given service. This system was audited in more than half of such centres and the results showed an increase in staff by 24% (doctors +43%, nurses +18%, psychologists +33%, occupational therapists +41% and social workers +84%) in such institutions. Along with increased staffing, there came the obligation to implement quality assurance. There are about 7000 beds in 65 forensic psychiatry clinics.
GERMANY

© 2005 World Health OrganizationMental Healthatlas
207
E –
I
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in advo-cacy, promotion, prevention, treatment and rehabilitation. On the federal level there is an association of family members (Familienselbsthilfe Psychiatrie) and one of the ‘users’ (Bundesverband Psychiatrie-Erfahrener). Their importance and influence has grown in the last decades, meanwhile they are involved in relevant bodies and decision-making processes.
Information Gathering System There is mental health reporting system in the country. Reporting is done under the Health Reporting and Data of Health Services.The country has data collection system or epidemiological study on mental health. There is a data analysis system with respect to services provided for chronic mental diseases.
Programmes for Special Population The country has specific programmes for mental health for minorities, refugees, disaster affected population, indigenous population, elderly and children. Due to the federal system in Germany and given responsibilities there are no specific programmes on the federal level for special populations as far as only the aspect of ‘mental health’ is affected. Within more general programmes, as for the elderly or for chil-dren the issue of mental health within those groups is taken into account. On-state level programmes for special groups as minori-ties, refugees, disaster-affected populations etc. do exist.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, ethosuximide, phenobarbital, phenytoin sodium, odium valproate, amitriptyline, chlorpromazin, diazepam, fluphena-zine, haloperidol, lithium, biperiden, carbidopa, levodopa.
Other Information Hospital treatment has been improved thanks to the Psychiatrie-Personalverordnung (1991) – a federal staffing directive which has brought an additional 6500 multidisciplinary staff members to inpatient treatment since 1991. In Germany, the trend has been to reduce the size of psychiatric hospitals without closing them down while simultaneously developing general hospi-tal services and community care.
Additional Sources of InformationAktion Psychisch Kranke. Mental Health Care in the Federal Republic of Germany – Summary of the Report Submitted by an Expert Commission to Parliament (Bundestag).
Bauer, M., Kunze, H., von Cranach, M., et al (2001) Psychiatric reform in Germany. Acta Psychiatrica Scandinavica 104 (suppl. 410), 27-34.
Bock, T. (1994) Long-term mental illness in Germany. International Journal of Social Psychiatry, 40, 276-282.
Bramesfeld A., Wismar M. (2003) The third pillar of psychiatric health care reform – structures for coordinating a planning of psychiatric health care in Germany. Psychiatrische Praxis, 30, 318-325.
Brand,U. (2001) Mental health care in Germany: carer’s perspective. Acta Psychiatrica Scandinavica, 104 (suppl. 410), 35-40.
Hafner, H. (1997) A quarter of a century of rehabilitation of psychiatric patients in Germany. Gesundheitswesen, 59, 69-78.
Kallert, T. W., Leisse, M. (1999) Occupational status of Saxony social psychiatry service clients as a result of the reunification of Germany. Psychiatrische Praxis, 26, 133-138.
Kunze, H., Becker, T., Priebe, S. (2004) Reform of psychiatric services in Germany: hospital staffing directive and commissioning of community care. Psychiatric Bulletin, 28, 218-221.
Muller-Isberner, R., Freese, R., Jockel, D., et al (2000) Forensic psychiatric assessment and treatment in Germany. International Journal of Law and Psychiatry, 23, 467-480.
Rossler, W., Salize, H.J., Reicher-Rossler, A. (1996) Changing Patterns of Mental Health Care in Germany. International Journal of Law and Psychiatry, 19, 391-411.
Wolfersdorf, M., Kukla, R. (2004) Clinics for psychiatry and psychotherapy in Germany in July 2003. An overview on numbers of beds and day-clinic places. Krankenhauspsychiatrie, 15, 12-15.
GERMANY

© 2005 World Health OrganizationMental Healthatlas
208
E –
I
GhanaGENERAL INFORMATIONGhana is a country with an approximate area of 239 thousand sq. km. (UNO, 2001). Its population is 21.377 million, and the sex ratio (men per hundred women) is 99 (UNO, 2004). The proportion of population under the age of 15 years is 39% (UNO, 2004), and the proportion of population above the age of 60 years is 5% (WHO, 2004). The literacy rate is 81.9% for men and 65.9% for women (UNESCO/MoH, 2004).The country is a low income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 4.7%. The per capita total expenditure on health is 60 international $, and the per capita government expenditure on health is 36 interna-tional $ (WHO, 2004).The main language(s) used in the country is (are) English. The largest ethnic group(s) is (are) African. The largest religious group(s) is (are) Christian, and the other religious group(s) are (is) indigenous groups and Muslim.The life expectancy at birth is 56.3 years for males and 58.8 years for females (WHO, 2004). The healthy life expectancy at birth is 49 years for males and 50 years for females (WHO, 2004).
EPIDEMIOLOGYAffinnih (1999) found that heroin and cocaine were the common drugs of abuse in a sample of 117 current and former drug users. The typical drug user was a 30-year old, who belonged to the working or lower socioeconomic class. Petty theft was common among male drug users. Community-based studies on chronic psychosis (Field, 1968) and schizophrenia (Sikanartey & Eaton, 1984) are also available. Turkson and colleagues have published a series of studies on psychiatric outpatients. In a sample of 131 depressed female outpatients, Turkson and Dua (1996) reported that the majority of patients were in the 20-40 years age group, were mar-ried with 5-8 children but with poor financial support from husbands and had limited education or employment opportunities. They often presented with somatic symptoms like headache and insomnia. Social stress was one of the causes for onset of depres-sion. Turkson (1996) reviewed 7-year (1987-94) outpatient data on adolescents (n=454). Results indicated that only 59.3% had a psychiatric illness. In the subgroup with psychiatric disorders (n= 269), 32.7% had functional psychoses (more than half of these were depression), neurotic disorders (23.4%), personality disorders (20.4%) and organic psychosis (10%) were the other common disorders. Turkson and Asamoah (1997) did a retrospective assessment of 35 elderly (more than 60 years) outpatients seen between 1989-93. The commonest presentations were depression, dementia and paranoid disorders. Dementia was associated with the his-tory of alcohol use and paranoid disorders with female sex, past history of a similar disorder and hearing and visual impairment. Turkson (1998) studied the prevalence of psychiatric disorders in patients referred to the psychiatry outpatient clinics of a teaching hospital. Out of the 96 patients referred in 1988, 62.8% were referred by physicians and 14.9% by surgeons. Nearly half of these patients suffered from affective, neurotic and stress related disorders, 13.2% from schizophrenia, schizotypal and delusional disor-ders. Behavioural disorders and drug use were common among the adolescent group. About 2/3 of the patients were treated as outpatients in the centre, whereas the remaining required admission in specialized centres or general hospitals. Turkson and Asante (1997) reviewed records of 130 criminal offenders seen as outpatients and found that the commonest diagnoses were psychotic states related to drug use, schizophrenia and drug use disorders (without psychosis).
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is present. The policy was initially formulated in 1994.The components of the policy are advocacy, promotion, prevention, treatment and rehabilitation. The mental health policy has been revised in 2000.
Substance Abuse Policy A substance abuse policy is present. The policy was initially formulated in 1990. On substance abuse there are three laws. The Narcotic Drugs (Control, Enforcement and Sanctions) Law 1990, PNDC Law 236 and Pharmacy and Drugs Act 1961.
National Mental Health Programme A national mental health programme is present. The programme was formulated in 1994.The national mental health programme was revised in 2000.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. It was formulated in 1986.Risperidone, olanzapine and fluoxetine are available in the open market but they are expensive.
Mental Health Legislation The NRC Decree (1972) is the current mental health law. Plans to revise this law to conform with changes in mental health delivery, particularly community mental care and human rights concerns are in an advanced stage.The latest legislation was enacted in 1972.
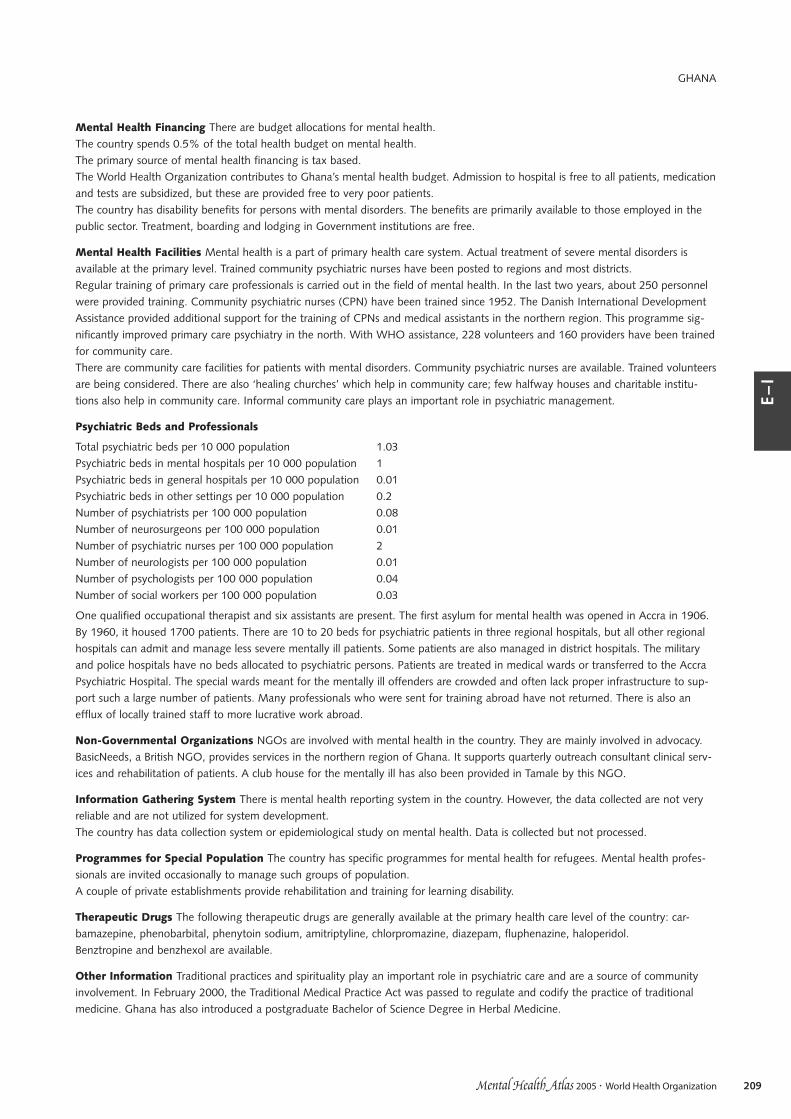
© 2005 World Health OrganizationMental Healthatlas
209
E –
I
Mental Health Financing There are budget allocations for mental health.The country spends 0.5% of the total health budget on mental health.The primary source of mental health financing is tax based.The World Health Organization contributes to Ghana’s mental health budget. Admission to hospital is free to all patients, medication and tests are subsidized, but these are provided free to very poor patients.The country has disability benefits for persons with mental disorders. The benefits are primarily available to those employed in the public sector. Treatment, boarding and lodging in Government institutions are free.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is available at the primary level. Trained community psychiatric nurses have been posted to regions and most districts.Regular training of primary care professionals is carried out in the field of mental health. In the last two years, about 250 personnel were provided training. Community psychiatric nurses (CPN) have been trained since 1952. The Danish International Development Assistance provided additional support for the training of CPNs and medical assistants in the northern region. This programme sig-nificantly improved primary care psychiatry in the north. With WHO assistance, 228 volunteers and 160 providers have been trained for community care.There are community care facilities for patients with mental disorders. Community psychiatric nurses are available. Trained volunteers are being considered. There are also ‘healing churches’ which help in community care; few halfway houses and charitable institu-tions also help in community care. Informal community care plays an important role in psychiatric management.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 1.03Psychiatric beds in mental hospitals per 10 000 population 1Psychiatric beds in general hospitals per 10 000 population 0.01Psychiatric beds in other settings per 10 000 population 0.2Number of psychiatrists per 100 000 population 0.08Number of neurosurgeons per 100 000 population 0.01Number of psychiatric nurses per 100 000 population 2Number of neurologists per 100 000 population 0.01Number of psychologists per 100 000 population 0.04Number of social workers per 100 000 population 0.03
One qualified occupational therapist and six assistants are present. The first asylum for mental health was opened in Accra in 1906. By 1960, it housed 1700 patients. There are 10 to 20 beds for psychiatric patients in three regional hospitals, but all other regional hospitals can admit and manage less severe mentally ill patients. Some patients are also managed in district hospitals. The military and police hospitals have no beds allocated to psychiatric persons. Patients are treated in medical wards or transferred to the Accra Psychiatric Hospital. The special wards meant for the mentally ill offenders are crowded and often lack proper infrastructure to sup-port such a large number of patients. Many professionals who were sent for training abroad have not returned. There is also an efflux of locally trained staff to more lucrative work abroad.
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in advocacy. BasicNeeds, a British NGO, provides services in the northern region of Ghana. It supports quarterly outreach consultant clinical serv-ices and rehabilitation of patients. A club house for the mentally ill has also been provided in Tamale by this NGO.
Information Gathering System There is mental health reporting system in the country. However, the data collected are not very reliable and are not utilized for system development.The country has data collection system or epidemiological study on mental health. Data is collected but not processed.
Programmes for Special Population The country has specific programmes for mental health for refugees. Mental health profes-sionals are invited occasionally to manage such groups of population.A couple of private establishments provide rehabilitation and training for learning disability.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, phenobarbital, phenytoin sodium, amitriptyline, chlorpromazine, diazepam, fluphenazine, haloperidol.Benztropine and benzhexol are available.
Other Information Traditional practices and spirituality play an important role in psychiatric care and are a source of community involvement. In February 2000, the Traditional Medical Practice Act was passed to regulate and codify the practice of traditional medicine. Ghana has also introduced a postgraduate Bachelor of Science Degree in Herbal Medicine.
GHANA

© 2005 World Health OrganizationMental Healthatlas
210
E –
I
Additional Sources of InformationAffinnih, Y. H. (1999) Drug use in greater Accra, Ghana: pilot study. Substance Use & Misuse, 34, 157-169.
Ewusi-Mensah. (2001) Post colonial psychiatric care in Ghana. Psychiatric Bulletin, 25, 228-229.
Field, M. J. (1968) Chronic psychosis in rural Ghana. British Journal of Psychiatry, 114, 31-33.
Kyei-Faried, S., Hermans, M. (1995) Primary health care in Ghana: no pay no cure? Nederlands Tijdschrift voor Geneeskunde, 139, 2321-2325.
Laugharne, R., Burns, T. (1999) Mental health services in Kumasi, Ghana. Psychiatric Bulletin, 23, 361-363.
Osei, Y. (1994) Psychiatric services in a developing country – the case of Ghana. Curare, 17, 39-43.
Roberts, H. (2001). A way forward for mental health care in Ghana? Lancet, 357, 1859.
Roberts, H. (2001) Mental health in Ghana. Research Report. The Ghana Mental Health Association. Accra-North.
Sikanartey, T., Eaton, W. W. (1984) Prevalence of schizophrenia in the Labadi District of Ghana. Acta Psychiatrica Scandinavica, 69, 156-161.
Tsey, K. (1997) Traditional medicine in contemprory Ghana: a public policy analysis. Social Science and Medicine, 45, 1065-1074.
Turkson, S. N. (1996) Psychiatric disorder among adolescents attending a psychiatric out-patient clinic in Accra, Ghana: a seven year review study (1987-1994). West African Journal of Medicine, 15, 31-35.
Turkson, S. N. (1998) Psychiatric diagnosis among referred patients in Ghana. East African Medical Journal, 75, 336-338.
Turkson, S. N., Asamoah, V. (1997) Common psychiatric disorders among the elderly attending a general psychiatric out patient clinic in Accra, Ghana: a five year retrospective study (1989-1993). West African Journal of Medicine, 16, 146-149.
Turkson, S. N., Asante, K. (1997) Psychiatric disorders among offender patients in the Accra Psychiatric Hospital. West African Journal of Medicine, 16, 88-92.
Turkson, S. N., Dua, A. N. (1996) A study of the social and clinical characteristics of depressive illness among Ghanaian women--(1988-1992). West African Journal of Medicine, 15, 85-90.
GHANA

© 2005 World Health OrganizationMental Healthatlas
211
E –
I
GreeceGENERAL INFORMATIONGreece is a country with an approximate area of 132 thousand sq. km. (UNO, 2001). Its population is 10.977 million, and the sex ratio (men per hundred women) is 97 (UNO, 2004). The proportion of population under the age of 15 years is 14% (UNO, 2004), and the proportion of population above the age of 60 years is 24% (WHO, 2004). The literacy rate is 98.5% for men and 95.9% for women (UNESCO/MoH, 2004).The country is a high income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 9.4%. The per capita total expenditure on health is 1522 international $, and the per capita government expenditure on health is 852 international $ (WHO, 2004).The main language(s) used in the country is (are) Greek (official). The largest ethnic group(s) is (are) Greek. The largest religious group(s) is (are) Greek Orthodox (official religion, 98% of the population), and the other religious group(s) are (is) Muslim (1.5%).The life expectancy at birth is 75.8 years for males and 81.1 years for females (WHO, 2004). The healthy life expectancy at birth is 69 years for males and 73 years for females (WHO, 2004).
EPIDEMIOLOGYThere is substantial epidemiological data on mental illnesses in Greece in internationally accessible literature. No attempt was made to include this information here.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is present. The policy was initially formulated in 1983.The components of the policy are advocacy, promotion, prevention, treatment and rehabilitation. A ten-year National Plan for Mental Health that was submitted for financial assistance to the EU in 1997 (Psychoargos). The main points of this plan were: the continuation of deinstitutionalization and di-stigmatization; sectorization of the psychiatric services throughout the country; continu-ation of the development of primary health care units and psychiatric units in general hospitals; continuation and intensification of the development of rehabilitation facilities; establishment and development of patient co-operatives in order to promote the social, economic and occupational reintegration into society of patients with severe psychiatric problems; establishment of detailed guaran-tees and procedures for the protection of patients’ rights. The ten-year National Mental Health Plan was revised in 2001 and hence-forth the revisions will be done every five years. The latest plan anticipates the closure of five out of the nine psychiatric hospitals by 2006 and the rest by 2015 (the first psychiatric hospital was closed under this plan in January 2004). During the period 2000 – 2006, there will also be a special emphasis on the areas of child psychiatry and psychogeriatrics.
Substance Abuse Policy A substance abuse policy is present. The policy was initially formulated in 1970.
National Mental Health Programme A national mental health programme is present. The programme was formulated in 1984.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. It was formulated in 1998.
Mental Health Legislation The Act 2716 deals with mental health. The new Mental Health Act (Law 2716/99) is based on and informed by the Mental Health Plan. All the essential points are included in the Act; in particular, the sectorization of mental health services is elaborated in considerable detail. The passing of the Mental Health Act constitutes a comprehensive policy document for the further development of psychiatric services in Greece, including its emphasis on the sectorization of mental health services and the priority it gives to primary health care and community-based psychiatry.The latest legislation was enacted in 1999.
Mental Health Financing There are no budget allocations for mental health.Details about expenditure on mental health are not available.The primary sources of mental health financing in descending order are tax based, social insurance, out of pocket expenditure by the patient or family and private insurances.Under current laws, it is forbidden to have separate budget for mental health. The social security system covers 95% of the popula-tion. Clients on social security can use the services of private practitioners for which part-payment is often made through private insurance. Psychological services are not included in private insurance plans.The country has disability benefits for persons with mental disorders. Special pensions, tax deductions and therapeutic benefits are provided.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is available at the primary level. Primary care is available in some areas only.Regular training of primary care professionals is not carried out in the field of mental health. General practitioners spend three months in psychiatry during their specialist training. Training of other primary care professionals is not carried out systematically in the field of mental health. However, for the last three years an annual 3-day seminar on communication and diagnostic skills has been run by psychiatrists for general physicians. There were 30 participants each year. Psychiatrists are currently visiting and provid-ing consultation in about one-third of primary care centres.

© 2005 World Health OrganizationMental Healthatlas
212
E –
I
There are community care facilities for patients with mental disorders. Community care is available through visiting psychiatrists at the health centres, through hostels, sheltered accommodation and sheltered workshops. Community care facilities changed considerably during the period 1981-1996. The developments have changed substantially the pattern of provision of psychiatric services in Greece with more emphasis on care provided through general hospitals and mental health centres. The EU, through the ‘Psychoargos’ programme, has already approved the development of many hostels and rehabilitation centres. By 1996, 388 new psychiatric settings in the community were in operation and the regional distribution was reasonably even, although there are par-ticular problems in developing services in remote mountainous and small island areas. For these areas, Act 2716/99 provides for mental health mobile units, and currently four such units are in operation in the Cyclades and the Dodecanese. The momentum of establishing community care facilities during the period 1991-1996, has been accelerated in recent years. As a result, 31 mental health centres, 60 psychiatric units in general hospitals, 12 day centres, 27 child guidance clinics, 302 rehabilitation units (hostels, boarding houses, sheltered flats) and 69 vocational rehabilitation centres were in operation by 2004.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 8.7Psychiatric beds in mental hospitals per 10 000 population 4.3Psychiatric beds in general hospitals per 10 000 population 0.3Psychiatric beds in other settings per 10 000 population 4.1Number of psychiatrists per 100 000 population 15Number of neurosurgeons per 100 000 population 2Number of psychiatric nurses per 100 000 population 3Number of neurologists per 100 000 population 4Number of psychologists per 100 000 population 14Number of social workers per 100 000 population 56
Since 1984, there has been a reduction in psychiatric beds in almost all regions. Almost all psychiatrists are working in urban areas and most are in western and central regions. Licensing/certification is required to work as a psychologist but there is no further additional legal provision to practice as a clinical psychologist. There is also no requirement for continuing education in the field of psychology. Most psychologists work in the private sector. Psychologists do not have prescription privileges.
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in advocacy, promotion, prevention, treatment and rehabilitation.
Information Gathering System There is no mental health reporting system in the country. The country has no data collection system or epidemiological study on mental health.
Programmes for Special Population The country has specific programmes for mental health for minorities, refugees, disaster affected population, elderly and children. There are extensive health programmes targeted at the use of narcotic drugs. A programme for depression, with particular emphasis on the elderly is in the initial stages. Services for children and adolescents and elderly are being expanded.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, ethosuximide, phenobarbital, phenytoin sodium, sodium valproate, amitriptyline, chlorpromazine, diazepam, haloperi-dol, lithium, biperiden, carbidopa, levodopa.
Other Information In 1983, Greece enacted the legislation aimed at the formation of a national health service and psychiatric leg-islation became a part of the NHS. There is very close cooperation between the Ministry of Health and the Ministry of Labour and Social Security concerning management and support for the National Mental Health Plan. The Ministry of Health also works closely with the Ministry of Internal Affairs and Public Administration to achieve approval of new posts within the Health Sector in general and mental health in particular. There is variable cooperation at the local level between mental health units and County authorities. Telepsychiatry in the form of internet and helpline, based on the success of similar exercises in cardiology and radiology is being developed. This e-facility is linked with the psychiatry department of the University of Athens.
Additional Sources of InformationConstantopoulos, A., Yannulatos, P. (2004) Greek psychiatric reform: difficulties, achievements and perspectives. In: J. Kyriopoulos (Ed.). Health Systems in the World: From Evidence to Policy. Athens: Papazisis Publishers.
Lambousis, E., Politis, A., Markidis, M., et al (2002) Development and use of online mental health services in Greece. Journal of Telemedicine and Telecare, 8 (suppl. 2), 51-52.
Madianos, M. G., Zacharakis, C., Tsitsa, C., et al. (1999) The mental health care delivery system in Greece: regional variation and socioeconomic corre-lates. Journal of Mental health Policy and Economics, 2, 169-176.
Macri, I. (2001) Medical psychology in Greece. Journal of Clinical Psychology in Medical Settings, 8, 27-30.
Strutti, C., Rauber, S. (1994) Leros and the Greek mental health system. International Journal of Social Psychiatry, 40, 306-312.
Yfantopoulos, J. (1994) Economic and legal aspects of mental health policies in Greece. International Journal of Social Psychiatry, 40, 296-305.
GREECE

© 2005 World Health OrganizationMental Healthatlas
213
E –
I
Grenada*GENERAL INFORMATIONGrenada is a country with an approximate area of 0.34 thousand sq. km. (UNO, 2001). Its population is 0.103 million, and the sex ratio (men per hundred women) is 98 (UNO, 2004). The proportion of population above the age of 60 years is 10% (WHO, 2004). The literacy rate is 98% for men and 98% for women (UNESCO/MoH, 2004).The country is a higher middle income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 5.3%. The per capita total expenditure on health is 445 international $, and the per capita government expenditure on health is 320 international $ (WHO, 2004).The main language(s) used in the country is (are) English. The largest ethnic group(s) is (are) African. The largest religious group(s) is (are) Roman Catholic, and the other religious group(s) are (is) Anglican and Protestant.The life expectancy at birth is 65.9 years for males and 68.8 years for females (WHO, 2004). The healthy life expectancy at birth is 58 years for males and 60 years for females (WHO, 2004).
EPIDEMIOLOGYThere is a paucity of epidemiological data on mental illnesses in Grenada in internationally accessible literature.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is absent.
Substance Abuse Policy A substance abuse policy is absent.
National Mental Health Programme A national mental health programme is present. The programme was formulated in 1985.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. Details about the year of formulation are not available.
Mental Health Legislation There is a mental health legislation which is being upgraded.Details about the year of enactment of the mental health legislation are not available.
Mental Health Financing There are budget allocations for mental health.The country spends 10% of the total health budget on mental health.The primary source of mental health financing is tax based.The country does not have disability benefits for persons with mental disorders.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is available at the primary level. Mental health care services are offered within primary care set-ups.Regular training of primary care professionals is not carried out in the field of mental health. There are community care facilities for patients with mental disorders. There are weekly community mental health clinics. Community health workers and social workers also render community care services. The community health worker pays regular visits to patients’ houses to ensure compliance to treatment. They were also trained to pick up early signs of deterioration and to inter-vene where necessary in order to prevent re-hospitalization. The public health nurse supports the community mental health worker.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 10.8Psychiatric beds in mental hospitals per 10 000 population 8.6Psychiatric beds in general hospitals per 10 000 population 2.2Psychiatric beds in other settings per 10 000 population 0Number of psychiatrists per 100 000 population 1Number of neurosurgeons per 100 000 population Number of psychiatric nurses per 100 000 population 5.4Number of neurologists per 100 000 population Number of psychologists per 100 000 population 1Number of social workers per 100 000 population 3
There is one occupational therapist. There is an urgent demand for trained psychiatric nurses and social workers to meet the demands of the increasing mental health population.
Non-Governmental Organizations NGOs are not involved with mental health in the country. There is a need for involvement of NGOs in mental health.
Information Gathering System There is mental health reporting system in the country. There is not much emphasis on collection of mental health data, and the information gathering system requires improvement.

© 2005 World Health OrganizationMental Healthatlas
214
E –
I
The country has no data collection system or epidemiological study on mental health. Only patients’ charts are available for collect-ing data related to health services.
Programmes for Special Population The country has specific programmes for mental health for elderly and children. Weekly out-patient clinics are carried out for children.Psychiatrists and the psychiatric nurses pay regular visits to the prisons to assess any psychiatric problems among the prisoners.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, phenobarbital, phenytoin sodium, amitriptyline, chlorpromazine, diazepam, haloperidol, lithium.
Other Information Since 1855, psychiatric care has largely been provided by the island’s only mental hospital. Mental health had low priority and the main patients, till the late 1950s, were the ‘wandering lunatics’. In 1970, an acute psychiatric unit was opened adjacent to the general hospital. After the US intervention, US aids facilitated the reconstruction of the destroyed psychiatric hospital and the development of psychiatry. Project HOPE was launched in 1985 to help in establishing diagnostic facilities, treatment and rehabilitation programmes and community care facilities. There is a need to establish policy and legislation for mental health and substance abuse. Additional mental health services need to be incorporated into the programme, such as day hospitals and psycho-geriatric facilities.* The verification of this country profile is still being awaited from the Ministry of Health of Grenada.
Additional Sources of InformationDeVooght, J, Walker, K. (1989) Community mental health Care in Grenada. International Nursing Review, 36, 22-24.
Fisher, F. D., Griffith, E., May, G. (1998) Recent developments in the Grenada Mental Health Program. Hospital and Community Psychiatry, 39, 980-85.
GRENADA

© 2005 World Health OrganizationMental Healthatlas
215
E –
I
GuatemalaGENERAL INFORMATIONGuatemala is a country with an approximate area of 109 thousand sq. km. (UNO, 2001). Its population is 12.661 million, and the sex ratio (men per hundred women) is 101 (UNO, 2004). The proportion of population under the age of 15 years is 42% (UNO, 2004), and the proportion of population above the age of 60 years is 5% (WHO, 2004). The literacy rate is 77.3% for men and 62.5% for women (UNESCO/MoH, 2004).The country is a lower middle income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 4.8%. The per capita total expenditure on health is 199 international $, and the per capita government expenditure on health is 96 international $ (WHO, 2004).The main language(s) used in the country is (are) Spanish and Indian (Maya). The largest ethnic group(s) is (are) indigenous (Maya, more than two-fifths of the population), and the other ethnic group(s) are (is) Mestizo. The largest religious group(s) is (are) Roman Catholic, and the other religious group(s) are (is) Protestant and Mayan.The life expectancy at birth is 63.1 years for males and 69 years for females (WHO, 2004). The healthy life expectancy at birth is 55 years for males and 60 years for females (WHO, 2004).
EPIDEMIOLOGYThere is a paucity of epidemiological data on mental illnesses in Guatemala in internationally accessible literature. In a report from the Ministry of Health from Guatemala, in Chiquimula, a province with 300 thousand habitants, the percentage of outpatient con-sultations by diagnosis was: Depression (25.5%), Chronic Psychosis (21.9%), Epilepsy(10.4%), Bipolar Disorder (5.2%), Somatoform Disorders (11.4%), Mental Retardation (4.4%) and Anxiety Disorders (8.3%) (La Salud Mental en Guatemala: Ideas y Reflexiones, 1999). Berganza and Aguilar (1992) used a modified version of the Center for Epidemiological Studies Depression Scale for Children (CES-DC-M) in 339 adolescent school children belonging to three different social strata to identify the prevalence of depression. The prevalence was 35.1%. Gender rather than social class was related to depression. Weller et al (1991) described clinical characteristics of a folk illness called ‘empacho’ which manifested as diarrhea, headache, vomiting and lack of appetite. It differed from other gas-trointestinal illnesses in that headaches were more likely and stomach-aches were less likely to be reported. Though empacho was frequently diagnosed by residents both in adults and children, folk healers were rarely consulted for it. Nevertheless, a strong asso-ciation exists between a household diagnosis of empacho and the use of folk healers by those households.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is present. The policy was initially formulated in 1997.The components of the policy are promotion, prevention, treatment and rehabilitation. It was revised in 2000 by mental health pro-fessionals and public servants. There are regular funds for its implementation Between 50 to 75% of its original content has been implemented.
Substance Abuse Policy A substance abuse policy is present. The policy was initially formulated in 1998. The substance abuse policy does not have a specific budget for its implementation and has been implemented to the extent of 25 to 50%. Guatemala also has a law on Substance Abuse from 2000, ‘Decreto Ley 50-2000 (Reformas al Código de Salud)’, aiming to control and to reduce alcohol and tobacco use. The national mental health programme has a sub-programme for the prevention of alcoholism and other addictions, which in turn is considered within the National Steering Plan prepared by the Secretariat against addictions and illicit drug trafficking.
National Mental Health Programme A national mental health programme is present. The programme was formulated in 1997.It was revised in 2000. There are regular funds for its implementation and it has been implemented 50 to 75% by local, regional and national authorities. Its main components are strategy of services reform, promotion and prevention, mental health services at primary health care and specialized services.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. It was formulated in 1984.
Mental Health Legislation The decree 50/2000 (Reforms to the Health Code) is an anti-tobacco legislation and was enacted in 2000.Details about the year of enactment of the mental health legislation are not available.
Mental Health Financing There are budget allocations for mental health.The country spends 0.9% of the total health budget on mental health.The primary sources of mental health financing in descending order are tax based, social insurance, out of pocket expenditure by the patient or family and private insurances.Psychiatric hospitals receive 85% of the budget, community care 10%. General hospitals receive 5% of the funding.The country has disability benefits for persons with mental disorders. Only 18% of the population have social security coverage, which is the portion that could be entitled to social benefit.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is available at the primary level. This is possible in some primary health units (10/22) where the national mental health programme has

© 2005 World Health OrganizationMental Healthatlas
216
E –
I
been implemented.25-50% of the population is covered by this kind of service. Mental health care is provided by Primary Health Care doctors.Regular training of primary care professionals is not carried out in the field of mental health. In the last two years, about 9980 per-sonnel were provided training. There are community care facilities for patients with mental disorders. Community care system for the mentally ill includes preven-tive/promotion interventions and covers 25 to 50% of the population. Home interventions, family interventions, vocational training and employment programmes are also available, but cover less than 25% of the treated population. The major part of community care facilities exist in the capital. The church plays a major role in providing community care services.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 0.35Psychiatric beds in mental hospitals per 10 000 population 0.32Psychiatric beds in general hospitals per 10 000 population 0.03Psychiatric beds in other settings per 10 000 population 0Number of psychiatrists per 100 000 population 0.54Number of neurosurgeons per 100 000 population Number of psychiatric nurses per 100 000 population 0.04Number of neurologists per 100 000 population 0.009Number of psychologists per 100 000 population 0.7Number of social workers per 100 000 population 0.07
These professionals include those in public services and Guatemalan Mental Health Services. No information from the private sector is available. There are 4 other workers in mental health. Two-thirds of the beds are occupied by long stay patients. All mental health professionals are employed in public institutions.
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in advocacy, promotion, prevention, treatment and rehabilitation. These organizations participate in mental health activities related to women, children, domestic violence and consumers. These activities include treatment (psychiatric care), promotion (community work with children, women and human rights), prevention (at risk populations), rehabilitation (for victims of armed conflicts and disasters) and advocacy (education and information). The Ministry is working with NGOs on psychosocial recovery of war victims.
Information Gathering System There is mental health reporting system in the country. ICD-10 is used to record information. Besides psychiatric diagnoses, the other mental health component reported is family violence.The country has data collection system or epidemiological study on mental health. An epidemiological assessment of the mental disorders is included. The department in charge of service data collection system is the National Program of Mental Health and the ‘Departamento del Sistema Único de Información’ both from the Ministry of Health. Data is collected only in the areas where the Mental Health Program is implemented. Only data coming from the public health system is available. The system is not very reliable.
Programmes for Special Population The country has specific programmes for mental health for refugees, disaster affected popu-lation, indigenous population and children. There is a school care system. Several NGOs are working in areas affected by war and Hurricane Mitch.In addition, there are programmes for women, children in vulnerable situation and for domestic violence. There is an Inter-institutional Working Group in Mental Health composed by the Ministry of Health, Guatemalan Institute of Social Security, Psychiatric Association of Guatemala, Psychologist Association of Guatemala, Neurological Association of Guatemala, Alzheimer of Guatemala with support from PAHO and UNICEF. It is not functional as yet; efforts are being made by Ministry to get the collaboration of multiple sectors.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, phenobarbital, phenytoin sodium, amitriptyline, chlorpromazine, diazepam, fluphenazine, haloperidol, lithium, biperiden.Some drugs are subsidized in state owned pharmacies and others are available only at normal prices. Free medication is provided to outpatients, but not in community centres where there are limitations. As the prices are high the Ministry of Health is establishing a network of national (popular) pharmacies which have reduced prices. Free service through primary health centres is being attempted.
Other Information Its reported that about 40% of the country has no mental health services and in the remaining part there are inadequate numbers of mental health professionals. The hospitals are in a poor state due to the lack of resources, and a large number of residents are institutionalized for a number of years.
Additional Sources of InformationBerganza, C. E., Aguilar, G. (1992) Depression in Guatemalan adolescents. Adolescence, 27, 771-782.
Republica de Guatemala Ministerio de salud publica y asistencia social (1999). Programa Nacional de salud mental memoria de labores.
Roberts, H. (2002). Mental health, truth and justice in Guatemala. Lancet, 359, 953.
Weller, S. C., Ruebush, T. K., Klein, R. E. (1991) An epidemiological description of a folk illness: a study of empacho in Guatemala. Medical Anthropology, 13, 19-31.
GUATEMALA

© 2005 World Health OrganizationMental Healthatlas
217
E –
I
GuineaGENERAL INFORMATIONGuinea is a country with an approximate area of 246 thousand sq. km. (UNO, 2001). Its population is 8.62 million, and the sex ratio (men per hundred women) is 101 (UNO, 2004). The proportion of population under the age of 15 years is 44% (UNO, 2004), and the proportion of population above the age of 60 years is 4% (WHO, 2004). The literacy rate is 50% for men and 22% for women (UNESCO/MoH, 2004).The country is a low income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 3.5%. The per capita total expenditure on health is 61 international $, and the per capita government expenditure on health is 33 interna-tional $ (WHO, 2004).The main language(s) used in the country is (are) French. The largest ethnic group(s) is (are) Peuhl, and the other ethnic group(s) are (is) Malinke and Susu. The largest religious group(s) is (are) Muslim.The life expectancy at birth is 50.9 years for males and 53.7 years for females (WHO, 2004). The healthy life expectancy at birth is 44 years for males and 46 years for females (WHO, 2004).
EPIDEMIOLOGYThere is a paucity of epidemiological data on mental illnesses in Guinea in internationally accessible literature.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is present. The policy was initially formulated in 1995.The components of the policy are advocacy, promotion, prevention, treatment and rehabilitation. Integration and decentralization are also components of the policy.
Substance Abuse Policy A substance abuse policy is present. The policy was initially formulated in 1999.
National Mental Health Programme A national mental health programme is present. The programme was formulated in 2000.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. Details about the year of formulation are not available.
Mental Health Legislation Measures related to prevention, protection and treatment have been taken (chapter 11, article 209-221 of the public health code) as part of the mental health legislation.The latest legislation was enacted in 1997.
Mental Health Financing There are no budget allocations for mental health.Details about expenditure on mental health are not available.The primary source of mental health financing is out of pocket expenditure by the patient or family.The country does not have disability benefits for persons with mental disorders.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is not available at the primary level. Mental health in primary care is to be introduced.Regular training of primary care professionals is not carried out in the field of mental health. There are no community care facilities for patients with mental disorders. Traditional medicine is available at the community level.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 0.05Psychiatric beds in mental hospitals per 10 000 population 0.05Psychiatric beds in general hospitals per 10 000 population 0Psychiatric beds in other settings per 10 000 population 0Number of psychiatrists per 100 000 population 0.04Number of neurosurgeons per 100 000 population 0.03Number of psychiatric nurses per 100 000 population 0Number of neurologists per 100 000 population 0.04Number of psychologists per 100 000 population 0Number of social workers per 100 000 population 0
Psychologists and social workers are present in the Ministry of Social Affairs.
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in advocacy, prevention, treatment and rehabilitation.

© 2005 World Health OrganizationMental Healthatlas
218
E –
I
Information Gathering System There is no mental health reporting system in the country. It is proposed to start a form of report-ing system for mental health.The country has no data collection system or epidemiological study on mental health. Data is collected only at the hospital level. No epidemiological survey exists.
Programmes for Special Population There are no programmes for special population.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, phenobarbital, phenytoin sodium, amitriptyline, chlorpromazine, diazepam, fluphenazine, haloperidol, lithium.Only phenobarbital, chlorpromazine and diazepam are available at the primary care level. Other drugs are on the list but are not available at the primary care level.
Other Information
Additional Sources of Information
GUINEA

© 2005 World Health OrganizationMental Healthatlas
219
E –
I
Guinea-BissauGENERAL INFORMATIONGuinea-Bissau is a country with an approximate area of 36 thousand sq. km. (UNO, 2001). Its population is 1.537 million, and the sex ratio (men per hundred women) is 98 (UNO, 2004). The proportion of population under the age of 15 years is 47% (UNO, 2004), and the proportion of population above the age of 60 years is 5% (WHO, 2004). The literacy rate is 54.1% for men and 23.5% for women (UNESCO/MoH, 2004).The country is a low income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 5.9%. The per capita total expenditure on health is 37 international $, and the per capita government expenditure on health is 20 interna-tional $ (WHO, 2004).The main language(s) used in the country is (are) Portuguese (official). The largest religious group(s) is (are) indigenous groups, and the other religious group(s) are (is) Muslim.The life expectancy at birth is 45.7 years for males and 48.7 years for females (WHO, 2004). The healthy life expectancy at birth is 40 years for males and 42 years for females (WHO, 2004).
EPIDEMIOLOGYThere is a paucity of epidemiological data on mental illnesses in Guinea-Bissau in internationally accessible literature. A study by de Jong (1996) described the community mental health programme set-up in Guinea-Bissau. An epidemiological study was a part of the programme. A two-stage design was used to screen 351 consecutive adults and 100 children attending general health care set-ups in both rural and urban areas. Psychiatric disorders were present in 12% of the adults and 13% of the children attending a primary care centre. The commonest presentations were neuroses (74%). Psychoses were also common. Residence in rural/urban or war/no war zones was not significantly associated with occurrence of disorder. Overall, the programme showed a profitable cost/benefit ratio and a high sustainability over a 10-year period.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is absent.
Substance Abuse Policy A substance abuse policy is absent.
National Mental Health Programme A national mental health programme is absent.All documents related to the national mental health programme were destroyed during the military conflict. A national mental health programme is being formulated with WHO support. It is likely to be ready for adoption in 2004-2005.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. It was formulated in 1984.After the introduction of the World Bank and International Monetary Fund Programme, the Essential Drug List Policy has suffered in more recent years.
Mental Health Legislation Details about the mental health legislation are not available.
Mental Health Financing There are budget allocations for mental health.The country spends 2.3% of the total health budget on mental health.The primary source of mental health financing is out of pocket expenditure by the patient or family.The country does not have disability benefits for persons with mental disorders. Government employees with a medical attestation issued by the National Medical Committee receive their salaries.
Mental Health Facilities Mental health is not a part of primary health care system. Actual treatment of severe mental disorders is not available at the primary level. Patients with problems are sent to the mental health centre for treatment and follow-up.Regular training of primary care professionals is carried out in the field of mental health. A nation-wide intervention programme with training of health workers and repetitive supervisory visits was initiated. In 1984 itself, 150 health workers were trained in 5-day seminars. It was followed by the evaluation of the programme. By 1985, Guinea-Bissau was the first third world country to suc-ceed in integrating a social-psychiatric programme into its basic health care services on a national level. In the next three years, 600 health workers were trained in order to compensate for transfers, deaths and emigration. Over 10 years, it sustained these efforts. In 1997, a programme was started to train primary care doctor and nurses in mental health, but it was interrupted due to the war.There are no community care facilities for patients with mental disorders. No community care exists due to lack of training and integration among workers. However, before the war, a community mental health programme was set up in 1983-84. The first part concentrated on epidemiological aspects. Subsequently, 850 primary health care workers were trained and supervised nationwide on their ability to manage mental disorders in patients.

© 2005 World Health OrganizationMental Healthatlas
220
E –
I
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 0Psychiatric beds in mental hospitals per 10 000 population 0Psychiatric beds in general hospitals per 10 000 population 0Psychiatric beds in other settings per 10 000 population 0Number of psychiatrists per 100 000 population 0Number of neurosurgeons per 100 000 population 0Number of psychiatric nurses per 100 000 population 0Number of neurologists per 100 000 population 0Number of psychologists per 100 000 population 0Number of social workers per 100 000 population 0
There are psychologists and social workers but they do not work in the area of mental health. In fact, two psychologists work in the Ministry of Health but not in the area of mental health. With support of WHO, one doctor initiated his specialization in Psychiatry in Cuba. The training will finish in October 2006. There was one mental health centre with 60 beds, but it was destroyed during the military conflict. After the Military Conflict, WHO helped in refurbishing two pavilions, which are being used for outpatient consulta-tion and for inpatient care (2 rooms with 5 beds each and 2 other rooms for acute/emergency cases). Unfortunately the hospitaliza-tion unit is not functioning fully because of the inadequate support from the Government (electricity, water and security).
Non-Governmental Organizations NGOs are not involved with mental health in the country.
Information Gathering System There is no mental health reporting system in the country. The country has no data collection system or epidemiological study on mental health. The Work Plan for 2004/05 has suggested the inclusion of mental disorders in studies on the prevalence of non-communicable diseases.
Programmes for Special Population The country has specific programmes for mental health for refugees, disaster affected popu-lation, elderly and children. The Government, international organizations and NGOs help whenever there is a crisis and the situation demands activities for a special group of population.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, phenobarbital, phenytoin sodium, amitriptyline, chlorpromazine, diazepam, fluphenazine, haloperidol, biperiden, carbi-dopa, levodopa.Hospital drugstores provide the drugs free. Other drugs are available from private pharmacies. Mental health centres obtain drugs from the central warehouse. The central drug deposit provides phenobarbital, haloperidol, amitriptylline, chlorpromazine and diazepam. Following the implementation of the Work Plan of 2002/03 and 2004/05 (supported by WHO) it is expected that the situation with regard to availability of psychotropics will improve.
Other Information
Additional Sources of Informationde Jong, J. T. (1996). A comprehensive public mental health program in Guinea-Bissau: a useful model for African, Asian and Latin-American countries. Psychological Medicine, 26, 97-108.
GUINEA-BISSAU

© 2005 World Health OrganizationMental Healthatlas
221
E –
I
GuyanaGENERAL INFORMATIONGuyana is a country with an approximate area of 215 thousand sq. km. (UNO, 2001). Its population is 0.767 million, and the sex ratio (men per hundred women) is 94 (UNO, 2004). The proportion of population under the age of 15 years is 29% (UNO, 2004), and the proportion of population above the age of 60 years is 7% (WHO, 2004). The literacy rate is 98.9% for men and 98.1% for women (UNESCO/MoH, 2004).The country is a lower middle income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 5.3%. The per capita total expenditure on health is 215 international $, and the per capita government expenditure on health is 171 international $ (WHO, 2004).The main language(s) used in the country is (are) English. The largest ethnic group(s) is (are) East Indian, and the other ethnic group(s) are (is) African. The largest religious group(s) is (are) Christian (half), and the other religious group(s) are (is) Hindu and Muslim.The life expectancy at birth is 61.5 years for males and 66.9 years for females (WHO, 2004). The healthy life expectancy at birth is 53 years for males and 57 years for females (WHO, 2004).
EPIDEMIOLOGYThere is a paucity of epidemiological data on mental illnesses in Guyana in internationally accessible literature. Affonso et al (2000) conducted a study to identify the characteristics of postpartum depression (PPDS) in almost 900 women across 9 countries. The Edinburgh Postnatal Depression Scale (EPDS) and the Beck Depression Inventory (BDI) were used to assess PPDS among a con-venience sample of primiparae with no obstetrical complications and having a healthy baby. On both the scales, European and Australian women had the lowest levels of PPDS, women from the USA were at the midpoint and women from Asia and South America had the highest levels of PPDS.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is absent.
Substance Abuse Policy A substance abuse policy is absent.
National Mental Health Programme A national mental health programme is absent.The national mental health programme is currently in development.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. It was formulated in 1997.
Mental Health Legislation Details about the mental health legislation are not available.
Mental Health Financing There are budget allocations for mental health.Details about expenditure on mental health are not available.The primary source of mental health financing is tax based.The budget allocations are mainly made for psychiatric institutions and departments.The country has disability benefits for persons with mental disorders.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is not available at the primary level. Treatment is available in hospitals and psychiatric clinics.Regular training of primary care professionals is not carried out in the field of mental health. There are no community care facilities for patients with mental disorders.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 3Psychiatric beds in mental hospitals per 10 000 population 2.6Psychiatric beds in general hospitals per 10 000 population 0.4Psychiatric beds in other settings per 10 000 population 0Number of psychiatrists per 100 000 population 0.2Number of neurosurgeons per 100 000 population 14Number of psychiatric nurses per 100 000 population 0.6Number of neurologists per 100 000 population 14Number of psychologists per 100 000 population 0Number of social workers per 100 000 population 0.4
The numbers represent those working in the public health sector.

© 2005 World Health OrganizationMental Healthatlas
222
E –
I
Non-Governmental Organizations NGOs are involved with mental health in the country. NGOs are also involved with substance abuse programmes.
Information Gathering System There is no mental health reporting system in the country. The country has no data collection system or epidemiological study on mental health.
Programmes for Special Population There are no special programmes.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, phenobarbital, phenytoin sodium, sodium valproate, amitriptyline, chlorpromazine, diazepam, fluphenazine, haloperi-dol, carbidopa, levodopa.The essential drug list was updated in 2004.
Other Information
Additional Sources of InformationAffonso, D. D., De, A. K., Horowitz, J. A., et al (2000) An international study exploring levels of postpartum depressive symptomatology. Journal of Psychosomatic Research, 49, 207-216.
Government document (1998) Essential Drug List of Guyana. Government Pharmacy Programme, 1
GUYANA

© 2005 World Health OrganizationMental Healthatlas
223
E –
I
HaitiGENERAL INFORMATIONHaiti is a country with an approximate area of 28 thousand sq. km. (UNO, 2001). Its population is 8.437 million, and the sex ratio (men per hundred women) is 98 (UNO, 2004). The proportion of population under the age of 15 years is 38% (UNO, 2004), and the proportion of population above the age of 60 years is 6% (WHO, 2004). The literacy rate is 53.8% for men and 50% for women (UNESCO/MoH, 2004).The country is a low income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 5%. The per capita total expenditure on health is 56 international $, and the per capita government expenditure on health is 30 international $ (WHO, 2004).The main language(s) used in the country is (are) French and Creole. The largest ethnic group(s) is (are) African (descent). The largest religious group(s) is (are) indigenous groups, and the other religious group(s) are (is) Roman Catholic.The life expectancy at birth is 49.1 years for males and 51.1 years for females (WHO, 2004). The healthy life expectancy at birth is 44 years for males and 44 years for females (WHO, 2004).
EPIDEMIOLOGYThere is a paucity of epidemiological data on mental illnesses in Haiti in internationally accessible literature.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is absent.Discussions between various stakeholder groups are being held on the development of a national mental health policy.
Substance Abuse Policy A substance abuse policy is absent. Discussions between various stakeholder groups are being held on the development of a substance abuse policy.
National Mental Health Programme A national mental health programme is absent.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. Details about the year of formulation are not available.
Mental Health Legislation Details about the mental health legislation are not available.
Mental Health Financing Details about disability benefits for mental health are not available.Details about expenditure on mental health are not available.Details about sources of financing are not available.Details about disability benefits for mental health are not available.
Mental Health Facilities Details about mental health facilities at the primary care level are not available. Details about training facilities are not available. Details about community care facilities in mental health are not available.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population Psychiatric beds in mental hospitals per 10 000 population Psychiatric beds in general hospitals per 10 000 population Psychiatric beds in other settings per 10 000 population Number of psychiatrists per 100 000 population Number of neurosurgeons per 100 000 population Number of psychiatric nurses per 100 000 population Number of neurologists per 100 000 population Number of psychologists per 100 000 population Number of social workers per 100 000 population
Non-Governmental Organizations Details about NGO facilities in mental health are not available.
Information Gathering System Details about mental health reporting systems are not available. Details about data collection system or epidemiological study on mental health are not available.
Programmes for Special Population Details about special programmes are not available.

© 2005 World Health OrganizationMental Healthatlas
224
E –
I
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, phenobarbital, phenytoin sodium, chlorpromazine, diazepam, haloperidol, biperiden.The PAHO/WHO list has been adapted to serve as the national essential drug list.
Other Information
Additional Sources of InformationHohner, J. A., Hughes, D. A., Jones, J. (1998) Mental health nursing support during Operation Sea Signal: Cuban/Haitian humanitarian mission. Military Medicine, 163, 353-57.
HAITI

© 2005 World Health OrganizationMental Healthatlas
225
E –
I
HondurasGENERAL INFORMATIONHonduras is a country with an approximate area of 112 thousand sq. km. (UNO, 2001). Its population is 7.1 million, and the sex ratio (men per hundred women) is 102 (UNO, 2004). The proportion of population under the age of 15 years is 40% (UNO, 2004), and the proportion of population above the age of 60 years is 5% (WHO, 2004). The literacy rate is 79.8% for men and 80.2% for women (UNESCO/MoH, 2004).The country is a lower middle income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 6.1%. The per capita total expenditure on health is 153 international $, and the per capita government expenditure on health is 81 international $ (WHO, 2004).The main language(s) used in the country is (are) Spanish. The largest ethnic group(s) is (are) Mestizo (nine-tenths). The largest reli-gious group(s) is (are) Roman Catholic.The life expectancy at birth is 64.2 years for males and 70.4 years for females (WHO, 2004). The healthy life expectancy at birth is 56 years for males and 60 years for females (WHO, 2004).
EPIDEMIOLOGYThere is a paucity of epidemiological data on mental illnesses in Honduras in internationally accessible literature. Kohn et al exam-ined 800 victims of Hurricane Mitch. They were stratified from high, medium and low class areas and high and low exposure sub-groups. Current DSM-IV major depressive episode was diagnosed in 18.3% of the population and PTSD in 11.2%. Co-morbidity between PTSD and major depressive episode was high. Prevalence of both disorders were associated with exposure. Other risk fac-tors for PTSD included lower SES, increasing age and ‘general nervousness’ before the disaster. Quirk and Casco (1994) described the effect of forced disappearance on the physical and psychological health of family members. The families of the disappeared were compared with two control groups: (1) families who lost a member due to accident or illness, and (2) families where no one had died within the past 10 years. Constellations of stress-related symptoms commonly seen in post-traumatic stress disorder and other anxiety disorders were approximately 2 times more prevalent in families of the disappeared as compared to the other two groups, indicating that families of the disappeared suffer over and above that due to normal grieving. Meza (1988) found that the presence of mental disorders in parents was associated with serious malnutrition in children. The commonest mental disorders in his sample were neurosis and alcohol use disorders. Wittig et al (1997) reported on the use of drugs by street children (n=1244) and found that family relations, length of time on the street and delinquency were associated with drug use, especially with sniffing glue.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is present. The policy was initially formulated in 2004.
Substance Abuse Policy A substance abuse policy is present. The policy was initially formulated in 1989. In 1988, the National Government created the Institute for the Prevention of Alcoholism, Drug Addiction and Pharmaceutical Dependence, with the fundamental objective to prevent the consumption of alcohol, tobacco products and other drugs especially in children and young adults. The substance abuse policy has a specific budget for its implementation. It focuses on drinking and driving, prohibition of selling alcohol to underage subjects and regulation of advertisement. More than 90% of the policy has been already implemented. There is legislation on substance abuse in place since 2001.
National Mental Health Programme A national mental health programme is present. Details about the year of formulation of the programme are not available.There is a national programme under the Secretary of Mental Health. The objective is to have community participation.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. It was formulated in 1985.
Mental Health Legislation There is no mental health legislation. Although, there is a law against domestic violence which was passed in 1998.Details about the year of enactment of the mental health legislation are not available.
Mental Health Financing There are budget allocations for mental health.The country spends 2.3% of the total health budget on mental health.Details about sources of financing are not available.More than 90% of funds for mental health services goes to the psychiatric hospitals.The country has disability benefits for persons with mental disorders. However, only a minority of the eligible population get the benefits (less than 10%).

© 2005 World Health OrganizationMental Healthatlas
226
E –
I
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is available at the primary level. Less than 25 % of the population is covered by this kind of service. Psychiatrists are responsible for treatment of mental disorders at primary care level. Medication is the only therapy available.Regular training of primary care professionals is not carried out in the field of mental health. There are no community care facilities for patients with mental disorders.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 0.6Psychiatric beds in mental hospitals per 10 000 population 0.53Psychiatric beds in general hospitals per 10 000 population 0.07Psychiatric beds in other settings per 10 000 population 0Number of psychiatrists per 100 000 population 0.76Number of neurosurgeons per 100 000 population 0.36Number of psychiatric nurses per 100 000 population 0Number of neurologists per 100 000 population 0.17Number of psychologists per 100 000 population 0.5Number of social workers per 100 000 population 0.26
90% of the beds are occupied by long stay patients. There are no psychiatric beds in general hospitals and prisons. There is one day care centre for mental health patients.
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in advocacy, promotion, prevention, treatment and rehabilitation. They participate in activities related to women, children, domestic violence and consumers.
Information Gathering System There is mental health reporting system in the country. ICD-10 is used for recording information.The country has data collection system or epidemiological study on mental health. The data is collected at regional level and sent to the Department of Statistics, but mental health data are not processed.
Programmes for Special Population The country has specific programmes for mental health for elderly. There are facilities for counselling on family violence and on HIV.Also there are programmes for domestic violence. These programmes are managed by multidisciplinary personnel and have been developed under the National Program of Mental Health. There are 15 distributed councils of family in all the country. Also, a pro-gramme of Council in VIH/SIDA exists.
Therapeutic Drugs The essential drug list was revised in 2001. There is almost no availability of the medications listed below at pri-mary health care level. Medicines in the primary health care are free and in some cases subsidized for those in need based on eco-nomic and social graph anchors and according to the availability of financing and to prices in the market for the following medica-tions: carbamazepine, phenobarbital, phenytoin sodium, diazepan, flufenazin, cloropromazin, biperiden and levodopa. Ethosuximide, chlorpromazine, biperiden and lithium carbonate are available only at the Ministry of Health.
Other Information
Additional Sources of InformationMeza, J. M. (1988) Prevalence of mental health problems in parents of children with malnutrition in one area of Tegucigalpa, Honduras. Acta Psiquiatrica y Psicologica de America Latina, 34, 145-148.
Quirk, G. J., Casco, L. (1994) Stress disorders of families of the disappeared: a controlled study in Honduras. Social Science & Medicine, 39, 1675-1679.
Wittig, M. C., Wright, J. D., Kaminsky, D. C. (1997) Substance use among street children in Honduras. Substance Use & Misuse, 32, 805-827.
HONDURAS

© 2005 World Health OrganizationMental Healthatlas
227
E –
I
HungaryGENERAL INFORMATIONHungary is a country with an approximate area of 93 thousand sq. km. (UNO, 2001). Its population is 9.831 million, and the sex ratio (men per hundred women) is 91 (UNO, 2004). The proportion of population under the age of 15 years is 16% (UNO, 2004), and the proportion of population above the age of 60 years is 20% (WHO, 2004). The literacy rate is 99.5% for men and 99.2% for women (UNESCO/MoH, 2004).The country is a higher middle income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 6.8%. The per capita total expenditure on health is 914 international $, and the per capita government expenditure on health is 686 international $ (WHO, 2004).The main language(s) used in the country is (are) Modern Hungarian. The largest ethnic group(s) is (are) Hungarian (nine-tenths), and the other ethnic group(s) are (is) Roma, German and Slovak. The largest religious group(s) is (are) Roman Catholic (three-fourths).The life expectancy at birth is 68.4 years for males and 76.8 years for females (WHO, 2004). The healthy life expectancy at birth is 62 years for males and 68 years for females (WHO, 2004).
EPIDEMIOLOGYKopp and Csoboth (2001) studied a national representative sample of 12640 people and found that just less than half of men and more than a quarter of women smoked. In a community sample of 2953 randomly selected adults, Szadoczky et al (1998, 2000) found that the lifetime prevalence of major depressive disorder (MDD), bipolar disorder (BD) and dysthymia were 15.1% (male to female ratio of 2.7), 5.1%, and 4.5%, respectively. The 1-year and 1-month prevalence rates were 7.1% and 2.6% for MDD, 0.9% and 0.5% for manic episodes and 0.8%, and 0.5% for dysthymia. The highest risk for the development of MDD, dysthymia and BD was in 15-19 years, but in MDD and dysthymia another peak was found in the forties. MDD was associates with higher rates of dysthymia and all anxiety disorders, BD was associated with the occurrence of generalized anxiety disorder and panic disorder and dysthymia was associated with MDD and anxiety disorders. Zonda et al (2000) used the Diagnostic Interview Schedule and Beck’s Depression Inventory to interview a representative sample from a region (n=750) and found the point and lifetime prevalence of affective disorders to be: major depression 3.7% and 10.9%, dysthymia 2.9% and 5.3% and bipolar disorders zero and 1.07%. The risk of suicide was high in those with major depression and dysthymia. Kopp et al (2000) conducted a survey on depression in nationally representative samples of 21 000 adults in 1988 and 12 370 adults in 1995 using a modified version of Beck’s Depression Inventory. In surveys done in 1988 and 1995, 2.9% and 7.1% suffered from severe depression requiring treatment. Between 1988 and 1995 depression increased among the socially deprived, i.e. those with low education, unemployed and elderly. Rihmer et al (2001) assessed 2953 adults regarding comorbidity between anxiety and affective disorders using the Diagnostic Interview Schedule. The prevalence of generalized anxiety disorder, agoraphobia and simple phobia was highest among bipolar II patients (20.8%, 37.5% and 16.7%, respectively); social phobia was most prevalent in major depression (17.6%) and panic disorder was equally prevalent in the major depressive and bipolar II subgroups (12.4% and 12.5%, respectively). Women had a higher risk for comor-bidity between anxiety disorders and MDD. Szabo and Tury (1991) conducted a two-stage survey to determine the prevalence of bulimia in two non-clinical samples. In an adolescent sample no bulimic subjects were found. In the college sample 1.3% of females and 0.8% of males met DSM-III-R diagnostic criteria for bulimia nervosa. La Vecchia et al (1994) analysed suicide data from the World Health Organization mortality database. Hungary had the highest rate of suicide for men (52.1 per 100 000) and the second highest rate for women (17.6 per 100 000). The high rate of suicide in Hungary is probably related to similarly high rates in Eastern Europe (Sartorius, 1995). Toero et al (2001) reported that Hungary has the highest suicide rate among children and adolescents. Zonda (1999) found that suicide rate was associated with locality (rural), gender (male/female ratio was 4:1), age (elderly), marital status (divorced/widowed) and psychiatric (60.1%) and multiple somatic illnesses (8.8%). In a community sample, Szadoczky et al (2000) found that suicide attempts occurred more frequently among women and divorced/widowed persons. The presence of any lifetime anxiety and/or affective disorder, comorbidity, recurrence and chronicity were significant predictors of suicide attempts. Osvath et al (2001) reported that chronic physical and mental problems were frequent among suicide attempters and many of them were on medication. Czeizel et al (1990) assessed 1276 school age children with mental retardation and estimated that 3% of school age children had an IQ of less than 50 and that low IQ was associated with 58 years of life lost.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is absent.A mental health policy constitutes an important chapter of the National Public Health Strategy voted for by the government and to be submitted for the Parliament in 2001.
Substance Abuse Policy A substance abuse policy is present. The policy was initially formulated in 2000.
National Mental Health Programme A national mental health programme is present. The programme was formulated in 2001.Some national mental health programmes including one against drug misuse have been elaborated/reframed during the last five years. A new version of the national mental health programme is in preparation, taking into account the shift in the concept of health (e.g. the Ottawa and Jakarta Declarations) and the priorities of the World Health Organization. The National Mental Health

© 2005 World Health OrganizationMental Healthatlas
228
E –
I
Programme constitutes one of the 20 sub-programmes of the recently initiated National Public Health Programme which is to be implemented over the next 10 years.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. It was formulated in 2000.
Mental Health Legislation The Health Act (No CL IV) of 1997 relates to mental health. A new Health Act, voted by the Parliament in 1998, came into effect in 1999. There is no special law on mental health, but this Act contains a chapter on mental disorders and their treatment, including hospitalization and compulsory measures. The legislation on mental health issues, with the protection of human rights of mental patients, conforms to EU requirements. The legislation was modified with more precision on coercive measures in 2001 and in 2004.The latest legislation was enacted in 1997.
Mental Health Financing There are budget allocations for mental health.The country spends 8% of the total health budget on mental health.The primary sources of mental health financing in descending order are social insurance and tax based.The health service is based on insurance system. Due to this, emphasis is more on short term medical treatment and psychotherapy has lost out. As outpatient care is financed to a lesser degree than inpatient care, institutions have tended to develop their inpatient facilities to a greater extent. The American mechanism of ‘diagnostic related groups’ was adopted to finance hospital services. In outpatient care, the ‘German score system’ was introduced. Care of handicapped children is financed by the social welfare budget.The country has disability benefits for persons with mental disorders.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is not available at the primary level. There are mental health centres all over the country to cater to primary care.Regular training of primary care professionals is carried out in the field of mental health. In the last two years, about 500 personnel were provided training. Training facilities for primary care doctors are present. Family doctors treat a significant proportion of psy-chiatry patients.There are community care facilities for patients with mental disorders. Community care is mainly provided by some mental health centres and universities. The development of community care and primary care facilities is dependent on grants and is occurring at a gradual pace. A few halfway institutions are in operation.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 9.6Psychiatric beds in mental hospitals per 10 000 population 2.3Psychiatric beds in general hospitals per 10 000 population 7.2Psychiatric beds in other settings per 10 000 population 0.1Number of psychiatrists per 100 000 population 9Number of neurosurgeons per 100 000 population 1Number of psychiatric nurses per 100 000 population 19Number of neurologists per 100 000 population 7Number of psychologists per 100 000 population 2Number of social workers per 100 000 population 1
There are 3080 other kind of mental health professionals. Over the last decade, substantial reduction (one-third) in psychiatry hos-pital beds has occurred. A reform of psychiatric institutions offering care to chronic psychotic patients is also under way and many of them now offer rehabilitative services. The private sector is small and is limited to outpatient care. About 160 beds are available with child and adolescent psychiatry departments. There is a system of psychiatric outpatient services staffed by psychiatrists, clini-cal psychologists, social workers, psychiatric nurses, etc. Though the significance of multidisciplinary teamwork seems to be gener-ally acknowledged, the health system is medically dominated, and non-medical professionals play a secondary role. There are very few psychologists and almost no social workers or occupational therapists. Within psychiatry, however, specialized qualifications like addictology, forensic psychiatry, psychotherapy and child psychiatry are available. A full fledged child psychiatry training programme was started as a part of TEMPUS project funded by the European Union.
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in advocacy, promotion, prevention and rehabilitation. There are different self-help groups.
Information Gathering System There is mental health reporting system in the country. Mental health forms part of the statistical reports of the National Institute of Statistics.The country has data collection system or epidemiological study on mental health. Annual reports of services are collected at the state mental hospitals.
HUNGARY

© 2005 World Health OrganizationMental Healthatlas
229
E –
I
Programmes for Special Population The country has specific programmes for mental health for refugees, elderly and children. Child psychiatry is underdeveloped and dependent on outpatient facilities. There are some child and youth guidance centres, which are usually run by psychologists. Larger schools employ psychologists. A separate school network deals with developmental disorders and learning difficulties. Substance abuse, forensic psychiatry services are also developing. There are regional drug outpatient depart-ments all over the country and all psychiatry wards are obliged to admit patients in withdrawal. Churches also help in management of patients of drug dependence. A Government programme of mental hygiene was established to support and coordinate local ini-tiatives. The forensic psychiatric institution is under the charge of Ministry of Justice.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, ethosuximide, phenobarbital, phenytoin sodium, sodium valproate, amitriptyline, chlorpromazine, diazepam, fluphena-zine, haloperidol, lithium, biperiden, carbidopa, levodopa.The costs of most important drugs are reimbursed by the social insurance. All modern anti-psychotics and anti-depressants are avail-able and are covered by social insurance. The full cost of anti-psychotics and 90% of the cost of anti-depressants is covered.
Other Information Before the 19th century there were no psychiatric care facilities, and monasteries took care of mentally ill patients. The first psychiatric institution was founded in 1840. From the beginning of the 20th century mental departments were being established in general hospitals and some psychiatric hospitals were being transformed into general hospitals. Psychiatry and neurology remained united till 1960. Psychiatry begun in universities in the middle of the 19th century. Hungary has contributed a lot to the development of psychiatry through the works of many psychiatrists. It developed under the influence of the German school of psychopathology. Psychiatric research is funded by a National Research Fund (Tringer, 1999).
Additional Sources of InformationCzeizel, A., Sankaranarayanan, K., Szondy, M. (1990) The load of genetic and partially genetic diseases in man. III. Mental retardation. Mutation Research, 232, 291-303.
Kopp, M., Csoboth, C. (2001) Smoking and alcohol abuse in the Hungarian population. Fogorvosi Szemle, 94, 177-182.
Kopp, M. S., Skrabski, A., Szedmak, S. (2000) Psychosocial risk factors, inequality and self-rated morbidity in a changing society. Social Science & Medicine, 51, 1351-1361.
La Vecchia C., Lucchini, F., Levi, F. (1994) Worldwide trends in suicide mortality, 1955-1989. Acta Psychiatrica Scandinavica, 90, 53-64.
Maylath, E. (2000) Diagnosis-related group financing and its influence on hospital financing – a comparison with Hungary: Could this be a useful model for German conditions? Gesundheitswesen, 62, 633-645.
Osvath, P., Fekete, S., Abraham, I. (2001) Physical illness and suicidal behavior. Review of results at the Pecs Center of the WHO/EURO Multicenter Study of Parasuicide. Orvosi Hetilap, 142, 127-131.
Rihmer, Z., Szadoczky, E., Furedi, J., et al (2001) Anxiety disorders comorbidity in bipolar I, bipolar II and unipolar major depression: results from a popula-tion-based study in Hungary. Journal of Affective Disorders, 67, 175-179.
Sartorius, N. (1995) Recent changes in suicide rates in selected Eastern European and other European countries. International Psychogeriatrics, 7, 301-308.
Szabo, P., Tury, F. (1991) The prevalence of bulimia nervosa in a Hungarian college and secondary school population. Psychotherapy & Psychosomatics, 56, 43-47.
Szadoczky, E., Papp, Z., Vitrai, J., et al (1998) The prevalence of major depressive and bipolar disorders in Hungary. Results from a national epidemiologic survey. Journal of Affective Disorders, 50, 153-162.
Szadoczky, E., Rihmer, Z., Papp, Z., et al (2000) Epidemiology of dysthymic disorder. Psychiatria Hungarica, 15, 66-75.
Szadoczky, E., Vitrai, J., Rihmer, Z., et al (2000) Suicide attempts in the Hungarian adult population. Their relation with DIS/DSM-III-R affective and anxi-ety disorders. European Psychiatry: the Journal of the Association of European Psychiatrists, 15, 343-347.
Toero, K., Nagy, A., Sawaguchi, T., et al (2001) Characteristics of suicide among children and adolescents in Budapest. Pediatrics International, 43, 368-371.
Tringer, L. (1999) Focus on psychiatry in Hungary. British Journal of Psychiatry, 174, 81-85.
van Benium, M.E., McGuiness, D., Csik. V. et al (1998) Contrasting child and adolescent psychiatry services in Szeged, Hungary and Glasgow, Scotland.
Vetro, A. (1999) Child and adolescent psychiatry in hungary. In: H. Remschmidt, H. van Engeland (Eds). Child and Adolescent Psychiatry in Europe. Historical Development, Current Situation and Future Perspectives. Darmstadt, Steinkopff. pp151-164.
Zonda, T. (1999) Suicide in Nograd County, Hungary, 1970-1994. Crisis: Journal of Crisis Intervention & Suicide, 20, 64-70.
Zonda, T., Bartos, E., Nagy, G. (2000) Affective disorders in a district of Budapest. Hungarian. Orvosi Hetilap, 141, 1443-1447.
HUNGARY

© 2005 World Health OrganizationMental Healthatlas
230
E –
I
IcelandGENERAL INFORMATIONIceland is a country with an approximate area of 103 thousand sq. km. (UNO, 2001). Its population is 0.291 million, and the sex ratio (men per hundred women) is 101 (UNO, 2004). The proportion of population under the age of 15 years is 22% (UNO, 2004), and the proportion of population above the age of 60 years is 15% (WHO, 2004). The literacy rate is 99% for men and 99% for women (UNESCO/MoH, 2004).The country is a high income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 9.2%. The per capita total expenditure on health is 2643 international $, and the per capita government expenditure on health is 2192 international $ (WHO, 2004).The main language(s) used in the country is (are) Icelandic. The largest ethnic group(s) is (are) Icelandic (Norwegian and Celtic descent). The largest religious group(s) is (are) Christian.The life expectancy at birth is 78.4 years for males and 81.8 years for females (WHO, 2004). The healthy life expectancy at birth is 72 years for males and 74 years for females (WHO, 2004).
EPIDEMIOLOGYThere is substantial epidemiological data on mental illnesses in Iceland in internationally accessible literature. No attempt was made to include this information here.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is absent.No specific mental health policy is being implemented but mental health is regarded as one of 7 identified key areas in long-term health planning in Iceland. Important developments in mental health care in the first years of the 21st century include stronger advocacy groups, mental health promotion schemes, more focus on prevention, evidence-based treatment and more active rehabili-tation.
Substance Abuse Policy A substance abuse policy is present. The policy was initially formulated in 1974. Amendments to the policy are due to be discussed in Parliament, partly reflecting EU-law and practices in other countries within the European Economic Area.
National Mental Health Programme A national mental health programme is present. The programme was formulated in 2001.The Icelandic Ministry of Health and the Health Committee of the Icelandic Parliament put forward a plan for national health tar-gets in 2001 extending to the year 2010. This plan emphasizes long-term objectives in health. Among the main objectives is a 25% reduction in suicide rates. However, no specific budget is set aside in order to try and implement this plan.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is absent.
Mental Health Legislation Iceland has mental health legislation. The law concerning care, treatment and rehabilitation of men-tal patients is mainly included in the legislation for health services; the legislation for social security and the legislation for national health insurance is included in the law no 97/1990 relating to health services; law no 59/1992 is related to the disabled; law no 117/1993 is related to social and health insurance; law no 39/1964 is related to treatment of alcoholics and people under the influ-ence of alcohol. There is no separate Mental Health Act in Iceland. The necessary legislation, e.g. for involuntary hospital admission, is included under the law on legal capacity. This ensures, among other things, the rights of patients to an appeal and an independ-ent medical review.The latest legislation was enacted in 1997.
Mental Health Financing There are no budget allocations for mental health.Details about expenditure on mental health are not available.The primary sources of mental health financing in descending order are tax based and out of pocket expenditure by the patient or family.There are no separate budget allocations for mental health, the costs being covered as part of overall expenditure on health services. Inpatient treatment is free, but patients pay a modest fee for outpatient treatment; psychiatrist consultations in outpatient settings are subsidized by the Ministry of Health.The country has disability benefits for persons with mental disorders. Iceland provides rehabilitation benefits for up to 18 months and disability benefits both short- and long-term for persons suffering from psychiatric disorders.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is available at the primary level. Mental health services work in close liaison with primary health care system. The primary health serv-ice is mainly run from health centres which have no beds and admissions are only made at specialist wards in the major hospitals.Regular training of primary care professionals is carried out in the field of mental health. Training opportunities for primary care pro-fessionals are on offer through the Departments of Psychiatry at the two hospitals in Iceland. The Ministry of Education is responsi-ble for the training of health care workers.

© 2005 World Health OrganizationMental Healthatlas
231
E –
I
There are community care facilities for patients with mental disorders. Non-governmental organizations and local authorities are gradually developing psychiatric care and other support services in the community, although this development has still not been fully achieved.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 5Psychiatric beds in mental hospitals per 10 000 population 0Psychiatric beds in general hospitals per 10 000 population 5Psychiatric beds in other settings per 10 000 population 0Number of psychiatrists per 100 000 population 25Number of neurosurgeons per 100 000 population 2Number of psychiatric nurses per 100 000 population 33Number of neurologists per 100 000 population 6Number of psychologists per 100 000 population 60Number of social workers per 100 000 population 110
The psychiatric services have been deinstitutionalized in recent decades and all psychiatric beds are now within general hospitals although in separate buildings on site or on special sites. The number of acute beds has decreased by about 25% since 1997 but day-patient and outpatient facilities have expanded at the same time. Psychiatric care is primarily provided by multidisciplinary teams. In recent years, the numbers of psychiatrists, psychologists and social workers have followed the growth of the population, but there continues to be a relative shortage of psychiatric nurses.
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in promotion, prevention and treatment. The role of NGOs is of growing importance, e.g. in terms of residential care, treatment facilities for sub-stance abusers and as promoters of patients’ rights. In addition to residential support, NGOs have important roles in non-hospital care.
Information Gathering System Details about mental health reporting systems are not available. Details about data collection system or epidemiological study on mental health are not available. There is no ongoing systemic mental health reporting taking place at present in the country. In recent years, requirement for col-lecting and storing personal data on subjects have become much tighter than they used to be, even to the degree where this may hamper epidemiological studies into sensitive subjects like mental health.
Programmes for Special Population The country has specific programmes for mental health for refugees, disaster affected popu-lation, elderly and children. Specialized psychiatric services for children and adolescents have improved over the last decade and are currently expanding further. This is regarded a priority to facilitate multidisciplinary early assessment, intervention and treatment.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, ethosuximide, phenobarbital, phenytoin sodium, sodium valproate, amitriptyline, chlorpromazine, diazepam, fluphena-zine, haloperidol, lithium, biperiden, levodopa.
Other Information There is considerable intersectoral cooperation at Government level, e.g. among the Ministries of Health, Social Affairs and Education as well as local authorities. NGOs, the Surgeon General of Health and others with the help of the media have promoted awareness in the public of mental health through publications and other activities.
Additional Sources of Information
ICELAND

© 2005 World Health OrganizationMental Healthatlas
232
E –
I
IndiaGENERAL INFORMATIONIndia is a country with an approximate area of 3287 thousand sq. km. (UNO, 2001). Its population is 1.081 billion, and the sex ratio (men per hundred women) is 106 (UNO, 2004). The proportion of population under the age of 15 years is 32% (UNO, 2004), and the proportion of population above the age of 60 years is 8% (WHO, 2004). The literacy rate is 68.4% for men and 45.4% for women (UNESCO/MoH, 2004).The country is a low income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 5.1%. The per capita total expenditure on health is 80 international $, and the per capita government expenditure on health is 14 interna-tional $ (WHO, 2004).The main language(s) used in the country is (are) Hindi, English and 14 other official languages. The largest ethnic group(s) is (are) Indo-Aryan, and the other ethnic group(s) are (is) Dravidian. The largest religious group(s) is (are) Hindu, and the other religious group(s) are (is) Muslim, Sikh and Christian.The life expectancy at birth is 60.1 years for males and 62 years for females (WHO, 2004). The healthy life expectancy at birth is 53 years for males and 54 years for females (WHO, 2004).
EPIDEMIOLOGYA meta-analysis of 13 psychiatric epidemiological studies (n=33 572) yielded an estimated prevalence rate of 5.8% (Reddy & Chandrashekar, 1998). Organic psychosis (0.04%), alcohol/drug dependence (0.69%), schizophrenia (0.27%), affective disorders (1.23%), neurotic disorders (2.07%), mental retardation (0.69%) and epilepsy (0.44%) were commonly diagnosed. Psychiatric morbidity was associated with residence (urban), gender (females), age group (35-44 years), marital status (married/widowed/divorced), socioeconomic status (lower) and family type (nuclear). Epilepsy and hysteria were significantly more common in rural communities. Nandi et al (2000) reported that psychiatric morbidity decreased from 11.7% to 10.5% over 20 years in a rural set-ting. Rao (1993) reported that mental morbidity was present in 8.9% of the elderly (above 60 years), with depression being the most common disorder (6%). Psychiatric morbidity was associated with physical diseases. Many studies (e.g. Vas et al, 2001) have evaluated large samples (n=2077 to 24 488) of subjects above the age of 55 years with standardized instruments (e.g. Mini Mental State Examination, Clinical Dementia Rating Scale) and diagnostic criteria (e.g. DSM-IV, NINCDS-ADRDA) using a two/three stage procedure. The rate of dementia was reported to be in the range of 0.8% to 3.4% and that of Alzheimer’s disease in the range of 0.6% to 1.5%. Gender (female) and age were associated with higher prevalence rates. The incidence rates per 1000 person-years for Alzheimer’s disease was 3.2 for those over 65 years and 1.7 for those over 55 years (Chandra et al, 2001). Mohan et al (2002) assessed 10 312 urban subjects with an instrument based on DSM-III-R criteria at two points of time one year apart. The prevalence of tobacco, alcohol, cannabis and opioids use among males was 27.6%, 12.6%, 0.3% and 0.4%, respectively. The annual incidence rates among males for any drug use and use of alcohol, tobacco, cannabis and opioids were 5.9%, 4.2%, 4.9%, 0.02% and 0.04%, respectively. Among females, incidence of any drug use was 1.2%. Gupta (1996) assessed 99 598 individuals above 35 years of age. Almost 69.3% of men and 57.5% of women reported current use of tobacco (23.6% of men smoked, most women consumed smokeless tobacco). Educational level was inversely associated with tobacco use of all kinds except cigarette smoking. Based on quantity/frequency index analysis, Mohan et al (1984) reported that almost 4.2% of their sample of rural subjects was depend-ent on alcohol. Kartikeyan et al (1992) assessed 9863 subjects from an urban slum. The prevalence of drug dependence was 1.1% (83.7% heroin, 10.7% cannabis and 5.8% opium). Chandran et al (2002) assessed 359 women in the last trimester of pregnancy and 6-12 weeks after delivery. The incidence of post-partum depression was 11%. Rate of post-partum depression was associ-ated with low income, birth of a daughter, relationship difficulties, adverse life events during pregnancy and lack of practical help. Lester et al (1999) reported that in 1991, the national suicide rate was 9.2 per 100 000 per year (males: 10.6 and females: 7.9). The most common methods for suicide were poisoning and hanging. The only predictor of the regional variation in suicide rates was population density, while the time-series suicide rate was predicted by female participation in labour force and fertility. Mayer and Ziaian (2002) reported that there was an increase in the rate of suicide over six years. The incidence of suicides was highest in the 30-44 year-old category. Suicide rates were nearly equal for young women and men. Vijayakumar and Rajkumar (1999) con-ducted psychological autopsies on 100 suicide victims and 100 controls and found that the presence of a personal or family history of mental disorder and recent life events were significant risk factors for suicide. Bhatia et al (2000) reviewed records of patients who had suicidal ideations (n=260), had made suicide attempts (n=58) or had completed suicide (n=55). Suicidal phenomena were associated with depression and adjustment disorder, previous suicide attempts (6.9%-18.2% in various subgroups) and a family history of depression. Organophosphorus poisoning and hanging were the commonest methods of attempting suicide. Siwach and Gupta (1995) reported that in a sample of 559 cases of acute poisoning, suicidal attempt was suspected to be the cause in 91.4% of cases. A number of studies (e.g. Shenoy et al, 1998) have evaluated large samples of children and adolescents (n=348 to 1535) with standardized instruments (e.g. Children’s Behaviour Questionnaire, Child Behaviour Checklist) using a two stage procedure. The prevalence of psychiatric morbidity was in the range of 14.4% to 31.7%. Higher rates were obtained on parent reports in com-parison to teacher reports. Boys manifested more externalizing problems and girls more internalizing problems. Hackett et al (1999) assessed 1403 children and found the prevalence of psychiatric disorders to be 9.4% as per ICD-10. Psychiatric morbidity was asso-ciated with gender (male), socioeconomic status (low), parental education (poor), attainment in school (impaired) and life events. Malhotra et al (2002) examined 933 urban school children using the Rutter-B Scale (teachers’ assessment) and the Childhood

© 2005 World Health OrganizationMental Healthatlas
233
E –
I
Psychopathology Measurement Schedule. Psychiatric disorders according to ICD-10 were diagnosed in 6.3% of subjects. Hackett et al (2001) reported that the 1-year prevalence of enuresis and encopresis was 18.6% and 4.3%, respectively. Chopra et al (1999) administered the Disability Screening Schedule (DSS) to 3560 children (0-6 years) from urban slums. Almost 6.9% of children were assessed as having disabilities. Mathur et al (1995) assessed 1545 children through a two stage procedure and found that the rate of mental disability was 2.7%.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is absent.The National Health Policy – 2002 incorporates most of the suggestions made in the draft of the National Mental Health Policy, hence the latter was not pursued as a separate document. The National Mental Health Programme (NMHP), launched in 1982, was restrategized during 2002 for implementation during the 10th Five Year Plan (2002-2007) with a quantum increase in fiscal alloca-tion (Rs 190 crore, up from Rs 28 crore during the 9th Plan). It forms the basis for public health initiatives in the field of mental health. The restrategized national mental health programme under implementation aims to provide a balanced mix of closely net-worked services, with dedicated budgetary support for modernization of the Government mental hospitals, strengthening of medical college departments of psychiatry, implementation of the district mental health programme in 100 districts across the country in the first phase, focussed information, education, communication (IEC) strategies, training and research.
Substance Abuse Policy A substance abuse policy is absent. A national master plan for substance abuse (1994) focused on the establishment of treatments and rehabilitation centres, human resource development, intersectoral collaboration and pub-lic education. These programmes are guided by the Ministry of Health and Family Welfare and the Ministry of Social Justice and Empowerment. Many Indian states have now banned smoking in public places and on public transport (e.g. Delhi Prohibition of Smoking and Non-Smokers Health Protection Act – 1996).
National Mental Health Programme A national mental health programme is present. The programme was formulated in 1982.Pilot projects have been undertaken to look at the feasibility of extending mental health services to the community and primary care levels. A review of the national mental health programme by the Central Council in 1995 led to the launch of the District Mental Health Programme (it covers 24 districts currently, with plans for expansion to 100 districts in the near future and to all districts by 2020).
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. Details about the year of formulation are not available.A large, mostly indigenous, pharmaceutical industry ensures that most psychotropic drugs are available in India, often at a fraction of their cost in high-income countries.
Mental Health Legislation The Mental Health Act of 1987 simplified admission and discharge procedures, provided for separate facilities for children and drug abusers and promoted human rights of the mentally ill. In 2002, it was implemented in 25 out of 30 states and Union Territories from which information was available. Other acts relevant to the mental health field are: the Juvenile Justice Act, the Persons with Disabilities Act and the Narcotic Drugs and Psychotropic Substances Act (amended in 2001).The latest legislation was enacted in 1987.
Mental Health Financing There are budget allocations for mental health.The country spends 2.05% of the total health budget on mental health.The primary sources of mental health financing in descending order are tax based, out of pocket expenditure by the patient or fam-ily, private insurances and social insurance.Government funding for health services are provided both by the states and the centre. Services provided at Government health centres are free. Certain industrial/governmental organizations provide health care schemes for their employees. In the 10th Five Year Plan estimates, mental health constitutes 2.05% of the total plan outlay for health.The country has disability benefits for persons with mental disorders. Disability benefits have become available recently and in a lim-ited way.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is available at the primary level. Mental health care in primary care is available in 22 districts out of about 600 districts. It will be extended to over 100 districts in the next few years.Regular training of primary care professionals is carried out in the field of mental health. In the last two years, about 600 personnel were provided training. Many workshops for the sensitization/training of programme officers, voluntary agencies, health directorate personnel and mental health professionals, have been undertaken. A range of training materials were developed and field tested. However, training facilities are available in some districts of the country only.
INDIA

© 2005 World Health OrganizationMental Healthatlas
234
E –
I
There are community care facilities for patients with mental disorders. Mental health facilities in community care is available in some designated districts. In addition, various non-governmental organizations provide different types of services ranging from telephone hotlines to residential rehabilitative services.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 0.25Psychiatric beds in mental hospitals per 10 000 population 0.2Psychiatric beds in general hospitals per 10 000 population 0.05Psychiatric beds in other settings per 10 000 population 0.01Number of psychiatrists per 100 000 population 0.2Number of neurosurgeons per 100 000 population 0.06Number of psychiatric nurses per 100 000 population 0.05Number of neurologists per 100 000 population 0.05Number of psychologists per 100 000 population 0.03Number of social workers per 100 000 population 0.03
There are 200 mental health workers of other types. One third of mental health beds are in one state (Maharashtra) and several states have no mental hospitals. Some mental hospitals have more than 1000 beds and several still have a large proportion of long-stay patients. During the past two decades, many mental hospitals have been reformed through the intervention of the voluntary organizations (e.g. Action Aid India), media, National Human Rights Commission and judiciary (courts), and yet a survey in 2002 showed that about a quarter had shortages in terms of drugs/treatment modalities and three quarters in terms of staff. The current emphasis is on general health psychiatry units that support voluntary admissions and encourage family members to stay with the patient. Some beds are allocated to treatment of drug abuse and for child psychiatry. Very few mental health professionals are based in rural areas. Most states allow public sector psychiatrists to have private clinics. Many mental health professionals have emigrated. In 2003 itself, more than 82 psychiatrists sought short-term and long-term employment in the United Kingdom in response to the latter’s international recruitment drive. Psychologists do not have prescription privileges, and there is no formal system of licensing clinical psychologists.
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in advocacy, promotion, prevention, treatment and rehabilitation. NGOs are involved in counselling, suicide prevention, training of lay counsellors and provision of rehabilitation programmes through day care, sheltered workshops, halfway homes, hostels for recovering patients and long-term care facilities. Parents and other family members of mentally ill persons have recently come together to form self-help groups.
Information Gathering System There is mental health reporting system in the country. Mental health is reported, but in a limited manner only by mental hospitals.The country has no data collection system or epidemiological study on mental health. A major multi-site study on the epidemiology of mental disorders, using WMH-2000 (Revised/updated), is nearing completion at 11 geographically widely distributed sites, and the data emerging from this project are likely to substantially augment the evidence-base in this regard.
Programmes for Special Population The country has specific programmes for mental health for disaster affected population and elderly. Services for special population are provided in few places.In the 1980s, the Government with the help of the UNDCP set up 68 drug dependence treatment centres and trained about one thousand psychiatrists and medical officers in the treatment of substance use disorders. Simultaneously, the Ministry of Welfare supported the establishment of 341 counselling and rehabilitation centres in the voluntary sector under its Community Drug Rehabilitation and Workplace Drug Prevention Programmes. No formal school mental health programme exists, but some academic centres and NGOs participate in school health initiatives. Residential facilities are available for mentally challenged and mentally ill children.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, phenobarbital, phenytoin sodium, sodium valproate, amitriptyline, chlorpromazine, diazepam, fluphenazine, haloperi-dol, lithium, carbidopa, levodopa.None of these drugs are routinely distributed by the Government at the primary health care level except for some designated dis-tricts where a special programme is operational.
Other Information The National Human Rights Commission has published its report on Quality Assurance in Mental Health relat-ing to mental hospitals in the country.
INDIA

© 2005 World Health OrganizationMental Healthatlas
235
E –
I
The traditional Indian medical systems of Ayurved and Unani recognized mental illness and provided necessary treatment. Recently, a document ‘Mental Health: An Indian Perspective (1946-2003)’ that summarizes mental health initiatives with relevance to public mental health in India was released by the Ministry for Health and Family Welfare.
Additional Sources of InformationAgarwal, S. P. (2004) Mental Health: An Indian Perspective (1946-2003). New Delhi: Directorate General of Health Services, Ministry of Health and Family Welfare.
Bhatia, M. S., Aggarwal, N. K., Aggarwal, B. B. (2000) Psychosocial profile of suicide ideators, attempters and completers in India. International Journal of Social Psychiatry, 46, 155-163.
Central Council of Health and Family Welfare (1999) Notes from Proceedings & Resolutions of the South Conference on Central Council of Health and Family Welfare.
Chandra, V., Pandav, R., Dodge, H. H., et al (2001) Incidence of Alzheimer’s disease in a rural community in India: the Indo-US study. Neurology, 57, 985-989.
Chandran, M., Tharyan, P., Muliyil, J., et al (2002) Post-partum depression in a cohort of women from a rural area of Tamil Nadu, India. Incidence and risk factors. British Journal of Psychiatry, 181, 499-504.
Chisholm, D., Sekar, K., Kumar, K., et al. (2000). Integration of mental health care into primary care: demonstration cost-outcome study in India and Pakistan. British Journal of Psychiatry, 176, 581-588.
Chopra, G., Verma, I. C., Seetharaman, P. (1999) Development and assessment of a screening test for detecting childhood disabilities. Indian Journal of Pediatrics, 66, 331-335.
Drug Dependence Treatment Centre and Ministry of Health and Family Welfare (1997) Summary and Recommendations of the National Workshop on Alcohol Policy.
Ganju, V. (2000) The mental health system in India: history, current system, and prospects. International Journal of Law & Psychiatry, 23, 393-402.
Gupta, P. C. (1996) Survey of sociodemographic characteristics of tobacco use among 99,598 individuals in Bombay, India using handheld computers. Tobacco Control, 5, 114-120.
Hackett, R., Hackett, L., Bhakta, P., et al (1999) The prevalence and associations of psychiatric disorder in children in Kerala, South India. Journal of Child Psychology & Psychiatry & Allied Disciplines, 40, 801-807.
Hackett, R., Hackett, L., Bhakta, P., et al (2001) Enuresis and encopresis in a south Indian population of children. Child: Care, Health & Development, 27, 35-46.
Isaac, M. (2000) Bridging the Gap. Health Action, 6-9.
Issac, M., Thara, R., Nagpal, J., et al. (2004) Mental health and substance abuse control programmes in India: Role of World Health Organization. New Delhi: WHO (SEARO).
Kartikeyan, S. K., Chaturvedi, R. M., Bhalerao, V. R. (1992) Role of the family in drug abuse. Journal of Postgraduate Medicine, 38, 5-7.
Khandelwal, S. K., Jhingan, H. P., Ramesh, S. (2004) India mental health country profile. International Review of Psychiatry, 16, 126-141.
Lester, D., Agarwal, K., Natarajan, M. (1999) Suicide in India. Archives of Suicide Research, 5, 91-96.
Malhotra, S., Kohli, A., Arun, P. (2002) Prevalence of psychiatric disorders in school children in Chandigarh, India. Indian Journal of Medical Research, 116, 21-28.
Mathur, G. P., Mathur, S., Singh, Y. D., et al (1995) Detection and prevention of childhood disability with the help of Anganwadi workers. Indian Pediatrics, 32, 773-777.
Mayer, P., Ziaian, T. (2002) Suicide, gender, and age variations in India. Are women in Indian society protected from suicide? Crisis: Journal of Crisis Intervention & Suicide, 23, 98-103.
Mellor D. (2003) Commentary: Recruitment is ethical. British Medical Journal, 327, 928.
Mohan, D., Chopra, A., Sethi, H. (2002) Incidence estimates of substance use disorders in a cohort from Delhi, India. Indian Journal of Medical Research, 115, 128-135.
Mohan, D., Sundaram, K. R., Advani, G. B., et al (1984) Alcohol abuse in a rural community in India. Part II: characteristics of alcohol users. Drug & Alcohol Dependence, 14, 121-128.
Nandi, D. N., Banerjee, G., Mukherjee, S. P., et al (2000) Psychiatric morbidity of a rural Indian community. Changes over a 20-year interval. British Journal of Psychiatry, 176, 351-356.
National Human Rights Commission (1999) Quality Assurance in Mental Health – Report of the National Human Rights Commission Project, New Dehli, NHRC.
Patel V, Saxena S. (2002) Psychiatry in India. International Psychiatry, 1, 16-18.
Prasadarao, P. S. D. V., Sudhir, P. M. (2001) Clinical psychology in India. Journal of Clinical Psychology in Medical Settings, 8, 31-38.
Ramana R., Saxena, S. (1991) India: quality and access are the priorities. In: L. Appleby, R. Araya (Eds). Mental Health Services in the Global Village, 3-13, London, Gaskell: The Royal College of Psychiatrists.
Rao, A. V. (1993) Psychiatry of old age in India. International Review of Psychiatry, 5, 165-170.
Reddy, M. V., Chandrashekar, C. R. (1998) Prevalence of mental and behavioral disorders in India: a meta-analysis. Indian Journal of Psychiatry, 40, 149-157.
Shenoy, J., Kapur, M., Kaliaperumal, V. G. (1998) Psychological disturbance among 5- to 8-year-old school children: a study from India. Social Psychiatry & Psychiatric Epidemiology, 33, 66-73.
Siwach, S. B., Gupta, A. (1995) The profile of acute poisonings in Harayana-Rohtak Study. Journal of the Association of Physicians of India, 43, 756-759.
The Narcotic Drugs and Psychotropic Substances Act (1985) Universal Law Publishing Co. Pvt. Ltd.
Vas, C. J., Pinto, C., Panikker, D., et al (2001) Prevalence of dementia in an urban Indian population. International Psychogeriatrics, 13, 439-450.
Vijayakumar, L., Rajkumar, S. (1999) Are risk factors for suicide universal? A case-control study in India. Acta Psychiatrica Scandinavica, 99, 407-411.
Weiss, M. G., Issac, M., Parkar, S. R., et al (2001) Global, national and local approaches to mental health: examples from India. Tropical Medicine & International Health, 6, 4-23.
INDIA

© 2005 World Health OrganizationMental Healthatlas
236
E –
I
IndonesiaGENERAL INFORMATIONIndonesia is a country with an approximate area of 1905 thousand sq. km. (UNO, 2001). Indonesia is an archipelago with five big islands and 13 669 small islands. Its population is 222.611 million, and the sex ratio (men per hundred women) is 100 (UNO, 2004). The proportion of population under the age of 15 years is 29% (UNO, 2004), and the proportion of population above the age of 60 years is 8% (WHO, 2004). The literacy rate is 92.5% for men and 83.4% for women (UNESCO/MoH, 2004).The country is a lower middle income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 2.4%. The per capita total expenditure on health is 77 international $, and the per capita government expenditure on health is 19 international $ (WHO, 2004).The main language(s) used in the country is (are) Bahasa Indonesia. The largest ethnic group(s) is (are) Javanese, and the other eth-nic group(s) are (is) Sundanese, Batak, Minang, Maduranese and coastal Malays. The largest religious group(s) is (are) Muslim (nine-tenths), and the other religious group(s) are (is) Christian, Hindu and Buddhist.The life expectancy at birth is 64.9 years for males and 67.9 years for females (WHO, 2004). The healthy life expectancy at birth is 57 years for males and 59 years for females (WHO, 2004).
EPIDEMIOLOGYBahar et al (1992) administered the Bahasa version of the 30-item General Health Questionnaire to a probability sample of 1670 adults. The Present State Examination was conducted on a weighted sub-sample of 100. Overall morbidity rates were similar to those in industrialized countries. A strong association was found between psychological symptoms and poverty. A mental health household survey conducted in 11cities by the Indonesian Psychiatric Epidemiologic Network suggested that the prevalence of mental disorders in adults was 18.5% (Personal Communication, 2004). Another study conducted in 16 cities (n=1600) using pro-portional sampling and CIDI (Composite International Diagnostic Interview) found that among those with mental disorders, the following diagnoses were common: drug abuse (44.0%), mental retardation (34.9%), mental dysfunction (16.2%) and mental dis-integration (5.8%) (Personal Communication, 2004). Suryani et al (1990) noted a relatively high prevalence (about 40%) of exces-sive alcohol consumption in a less developed village compared to a more developed one. Narendra et al (1990) noted an increase in risk taking behaviours like drug use among adolescents in Indonesia. Smet et al (1999) conducted a study on a random sample of schools (n=149) in Semarang (population 1.5 million) using a stratified sampling procedure (strata based on type of school and district). Within the schools, 186 classes were selected, targeting the 11, 13, 15 and 17 year olds. An anonymous, self-administered questionnaire was filled in by all students present at the day of the survey (n=6276). Among male students, smoking increased dramatically between the ages of 11 and 17, from 8.2% to 38.7%. Best friends’ smoking behaviour and attitudes towards smoking and older brothers’ smoking behaviour were important determinants of smoking. The variance explained by the regression model increased from 19.8% for 11 year olds to 53% for 17 year olds. Kurihara et al (2000) compared patients with schizophrenia in Bali and Tokyo during a 5-year follow-up study using standardized tools. They found that the clinical outcome was similar in the two sites. Waluyo et al (1996) found a high prevalence of musculoskeletal symptoms in assembly workers from Sweden and Indonesia. Greater stress and psychosomatic symptoms were reported by the Swedish group. Tanner and Chamberland (2001) found that the symptoms of Latah, a syndrome manifesting increased startle response, echolalia and echopraxia were similar to those described 100 years ago. Wignyosumarto et al (1992) examined 5120 children for non-verbal intelligence, social maturity behaviour or adap-tive skills and autistic features (with the Bryson’s screening scale). Sixty-six children who scored above 16 were assessed with CARS. The prevalence rate of autism within the birth cohort was 0.12%. Bleichrodt et al (1980) administered an extensive test battery to all children and adolescents in two village populations: one village in an area with severe iodine deficiency and a control village in a non-iodine-deficient area. No evidence of significant mental retardation was detected in the non-cretin group in the severely iodine-deficient area.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is present. The policy was initially formulated in 1999.The components of the policy are advocacy, promotion, prevention, treatment and rehabilitation. Mental health policy forms a part of the general health policy. A national training workshop focusing on planning and budgeting for service delivery and organization of services (Mental Health Policy Project) was held in 2003. Twelve trainers (senior mental health personnel) and 24 planners were trained.
Substance Abuse Policy A substance abuse policy is present. The policy was initially formulated in 1997. Two laws form the core of the substance abuse policy: Narcotic Law and Psychotropic Law (both were enacted in 1997). The National Narcotic Board that answers to the President coordinates the functioning of governmental and non-governmental activities in this area.
National Mental Health Programme A national mental health programme is present. The programme was formulated in 1995.The new national mental health programme has been developed in the year 2001.

© 2005 World Health OrganizationMental Healthatlas
237
E –
I
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. It was formulated in 1998.Shortages in the supply of the psychotropic drugs to some primary health centres and general hospitals have been noted and are probably due to underreporting of need by district /municipal health officials.
Mental Health Legislation The current mental health legislation is integrated into General Health Law. A specific mental health legislation has now been developed and awaits the approval of the Government.The latest legislation was enacted in 1992.
Mental Health Financing There are budget allocations for mental health.The country spends 1% of the total health budget on mental health.The primary sources of mental health financing in descending order are out of pocket expenditure by the patient or family, tax based, social insurance, private insurances and grants.The country has disability benefits for persons with mental disorders. Destitute psychotics and mentally retarded are considered as socially disabled, and the Government provides social institutional care in a limited way.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is available at the primary level. Training programmes for primary care physicians in treating mental disorders are present, and anti-psychotics (chlorpromazine and haloperidol) are available. Severe and disturbed psychotics are referred to mental hospitals, and families tend to bring the patients to traditional healers.Regular training of primary care professionals is carried out in the field of mental health. In the last two years, about 300 personnel were provided training. There are no community care facilities for patients with mental disorders. No systematic approach is present as limited facilities are available. However, traditional healers and nurses from Government mental hospitals make occasional visits.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 0.4Psychiatric beds in mental hospitals per 10 000 population 0.38Psychiatric beds in general hospitals per 10 000 population 0.02Psychiatric beds in other settings per 10 000 population 0.02Number of psychiatrists per 100 000 population 0.21Number of neurosurgeons per 100 000 population 0.01Number of psychiatric nurses per 100 000 population 0.9Number of neurologists per 100 000 population 0.06Number of psychologists per 100 000 population 0.3Number of social workers per 100 000 population 1.5
State mental hospitals are available in 24 out of 32 provinces. Private mental hospitals account for about 8% of all beds. Fifty beds are allocated for a drug abuse treatment centre.
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in advocacy, promotion, prevention, treatment and rehabilitation.
Information Gathering System There is mental health reporting system in the country. Mental health reporting is a part of hospi-tal reporting system and primary health centre reporting system.The country has no data collection system or epidemiological study on mental health. In the past epidemiological data had been col-lected with the support of the USA, but since 1996 it has not been done due to budget constraints.The data for mental health planning comes from the National Health Household Survey – Section on Mental Health, which is done every five years. The last survey was in 1995.
Programmes for Special Population The country has specific programmes for mental health for refugees, disaster affected popu-lation, elderly and children. Specific services are also available for drug abusers, HIV/AIDS patients, prisoners and workers.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, phenobarbital, phenytoin sodium, amitriptyline, chlorpromazine, diazepam, haloperidol.The most common anti-parkinsonian drug is trihexiphenidyl. The essential drug list is updated every year.
Other Information
INDONESIA

© 2005 World Health OrganizationMental Healthatlas
238
E –
I
Additional Sources of InformationBahar, E., Henderson, A. S., Mackinnon, A. J. (1992) An epidemiological study of mental health and socioeconomic conditions in Sumatera, Indonesia. Acta Psychiatrica Scandinavica, 85, 257-263.
Bleichrodt, N., Drenth, P. J., Querido, A. (1980) Effects of iodine deficiency on mental and psychomotor abilities. American Journal of Physical Anthropology, 53, 55-67.
Kurihara, T., Kato, M., Reverger, R., et al (2000) Outcome of schizophrenia in a non-industrialized society: comparative study between Bali and Tokyo. Acta Psychiatrica Scandinavica, 101, 148-152.
Narendra, M., Basuki, P. S., Soeharjono, L. B., et al (1990) Risk taking behavior of adolescents in Indonesia (country report). Paediatrica Indonesiana, 30, 319-324.
Smet, B., Maes, L., De Clercq, L., et al (1999) Determinants of smoking behaviour among adolescents in Semarang, Indonesia. Tobacco Control, 8, 186-191.
Suryani, L. K., Adnyana, T. A., Jensen, G. D. (1990) Palm wine drinking in a Balinese village: environmental influences. International Journal of the Addictions, 25, 911-920.
Tanner, C. M., Chamberland, J. (2001) Latah in Jakarta, Indonesia. Movement Disorders, 16, 526-529.
Waluyo, L., Ekberg, K., Eklund, J. (1996) Assembly work in Indonesia and in Sweden--ergonomics, health and satisfaction. Ergonomics, 39, 199-212.
Wignyosumarto, S., Mukhlas, M., Shirataki, S. (1992) Epidemiological and clinical study of autistic children in Yogyakarta, Indonesia. Kobe Journal of Medical Sciences, 38, 1-19.
INDONESIA

© 2005 World Health OrganizationMental Healthatlas
239
E –
I
Iran, Islamic Republic ofGENERAL INFORMATIONIran, Islamic Republic of is a country with an approximate area of 1648 thousand sq. km. (UNO, 2001). Its population is 69.789 mil-lion, and the sex ratio (men per hundred women) is 103 (UNO, 2004). The proportion of population under the age of 15 years is 31% (UNO, 2004), and the proportion of population above the age of 60 years is 6% (WHO, 2004). The literacy rate is 83.5% for men and 70.4% for women (UNESCO/MoH, 2004).The country is a lower middle income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 6.3%. The per capita total expenditure on health is 422 international $, and the per capita government expenditure on health is 183 international $ (WHO, 2004).The main language(s) used in the country is (are) Persian, Azari, Gilaki, Kurdish, Mazandarani, Baluchi, Arabic, Turkmani, Armenian and Ashuri. The largest ethnic group(s) is (are) Persian (half), and the other ethnic group(s) are (is) Azerbaijani, Gilaki, Kurd and Mazandarani. The largest religious group(s) is (are) Muslim (Shia), and the other religious group(s) are (is) Muslim (Sunni).The life expectancy at birth is 66.5 years for males and 71.7 years for females (WHO, 2004). The healthy life expectancy at birth is 56 years for males and 59 years for females (WHO, 2004).
EPIDEMIOLOGYAccording to the most recent epidemiologic survey (Noorbala et al, 2004) that used the General Health Questionnaire (GHQ-28) (n=35 014), 21% of the population (25.9% of the women and 14.9% of the men) were detected as likely to be suffering from mental illness. Interview of families by general practitioners revealed that the rates of mental retardation, epilepsy and psychosis were 1.4%, 1.2% and 0.6%respectively. Bash and colleagues (Bash & Bash-Liecht, 1978; Bash 1984) reported on psychiatric-epidemiological surveys (based partly on census studies, partly on random samples) that sampled rural, urban, tribal subjects above 6 years. The surveys employed questionnaires and tests in the screening phase and individual psychiatric examinations of all possible cases in the confirmation phase. Prevalence in various settings for any psychiatric disorder was: rural (14.9%), urban (16.6%), tribal (2.1%); for all psychoreactive cases (included in the foregoing): rural (8.7%), urban (9.8%), tribal (1.2%); for all psychosomatic cases (included in the psychoreactive): rural (1.7%), urban (2.3%), tribal (0.9%). Significant sex differences were found only in the poor strata. Alemi (1978) found the prevalence of opium use disorders in a survey of randomly chosen households from a rural community to be 6.9% in comparison to the rate of 1.1% estimated for the population based on registry of patients. Merchant et al (1976) found that 24% of the university students (n=607) reported life time use of drugs with 11% reporting use more than three times in their lives. The majority of drug users had used marijuana (54%). Use of drugs was significantly associated with sex, age, number of years of university attended, and father’s education. In another study on university students (n=501), Ahmadi and Yazdanfur (2002) reported that the prevalence of regular current use of various substances was: cigarettes (36.1%), alcohol (21.4%), opium (7.6%) and cannabis (3.0%). Substance use was significantly higher among males. Ahmadi and Javadpour (2001) found that among randomly selected health care students (n=346), 34.7% used sub-stances at some point in time. Almost 6.9% of the students were current regular users of substances (cigarettes: 5.5%, alcohol: 1.7%, opium: 1.4%, cannabis: 1.2%, heroin: 0.3% and LSD: 0.3%). Use of substances was significantly related to gender (11.3% of males and 1.4% of females were current regular users). Agahi and Spencer (1982) found that among 712 students aged 14-18 years, 11% had used some drugs of which opium was the commonest, followed by marijuana and heroin. Thornicroft and Sartorius (1993) reported the ten-year follow-up data of the WHO Collaborative Study on Depression (n=439). Almost 18% had very poor clinical outcome, 24% had severe social impairment for more than half of the follow-up period and 21% had no full remissions. The best clinical course (one or two reasonably short episodes of depression with complete remission between episodes) was more common in endogenous depres-sion (65%) in comparison to psychogenic depression (29%). A fifth (22%) had at least one episode lasting for more than 1 year, and 10% had an episode lasting over 2 years during follow-up. Death by suicide occurred in 11% of patients, with a further 14% making unsuccessful suicide attempts. Shokrollahi et al (1999) administered a sexual function questionnaire to 300 healthy married women (16-53 years old) attending a family planning centre. Approximately 38% of the women had at least one sexual dysfunction; the common ones were inhibited desire (15%), inhibited orgasm (26%), lack of lubrication (15%), vaginismus (8%) and dyspareunia (10%). There were significant correlations between sexual dysfunction in women and their knowledge (low) and attitude (conservative) towards sexu-ality and their husbands’ sexual dysfunction. Nobakht and Dezhkam (2000) conducted a two-stage study to assess eating disorders in 3100 schoolgirls in the age group of 15-18 years using the Persian translation of the Eating Attitudes Test (EAT-26), the Eating Disorder Diagnostic Inventory and a supplementary clinical interview. The lifetime prevalence of anorexia nervosa, bulimia nervosa and partial syndrome was 0.9%, 3.2% and 6.6%, respectively. Zarghami and Khalilian (2002) conducted interviews and/or psychological autopsies on 318 cases of self-burning. Self-immolation was associated with young age (average: 27 years), female gender (83%), housewife sta-tus, high school education, psychiatric (95%, mostly adjustment disorder) and chronic physical illnesses (30%) and high mortality (79%).
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is present. The policy was initially formulated in 1986.The components of the policy are advocacy, promotion, prevention, treatment and rehabilitation. Community education is a compo-nent of the policy.
Substance Abuse Policy A substance abuse policy is present. The policy was initially formulated in 1987. Alcohol is prohibited by both religion and legislation.

© 2005 World Health OrganizationMental Healthatlas
240
E –
I
National Mental Health Programme A national mental health programme is present. The programme was formulated in 1986.The national mental health programme was evaluated in 1995 and 1997 and changes were made based on suggestions. In 1995, it was evaluated jointly by the WHO and the Teheran Psychiatric Institute. Recently, different sub-programmes on service delivery in urban areas, prevention and promotion have been added to the main body in accordance with the population shift and change of priorities. Other related programmes are Integration of Substance Abuse Prevention within the Primary Health Care and a Harm Reduction Programme.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. It was formulated in 1988.The essential drugs list was last updated in 2001.
Mental Health Legislation Though there are different laws regarding the mentally ill, there is no modern mental health legislation. Since last year, a team has been working on a draft for a new legislation. A mandate by the Minister of Health has been issued in 1997 to allocate 10% of all general hospitals to psychiatry beds. The Mental Health Department has recently started a nation-wide advocacy campaign to implement this mandate.Details about the year of enactment of the mental health legislation are not available.
Mental Health Financing There are budget allocations for mental health.The country spends 3% of the total health budget on mental health.The primary sources of mental health financing in descending order are tax based, out of pocket expenditure by the patient or fam-ily, social insurance and private insurances.The national health service in Iran is funded by the Government and health insurance. If covered by health insurance, patients pay 25% of the fee for outpatient and 10% of the fee for inpatient treatment (consultation, laboratory investigations or medicines). Fees do not vary across age ranges. All emergencies are treated immediately without prior payment. The private sector can accept patients without insurance but it provides a limited range of services and the fees are high. Psychologists cannot send bills to insur-ance companies directly.The country has disability benefits for persons with mental disorders. Since 2001, the disabled mentally ill patients are entitled to a stipend of about $30 per month if they do not receive other free services. Already, about 10 000 disabled patients are receiving dis-ability benefits and the number is increasing. Institutional care is free of charge for the disabled mentally ill.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is avail-able at the primary level. Mental health delivery for severe illnesses is one of the objectives in rural and deprived areas.Regular training of primary care professionals is carried out in the field of mental health. In the last two years, about 20185 person-nel were provided training. Mental health services at the primary care level are available to more than one-fifth of urban and more than four-fifths of the rural population. Behvarz (multipurpose health workers), who are selected from the target community have a pivotal role in the country’s primary health care network. Their training lasts two years and equips them for active case finding, appro-priate referral to the GP and active follow-up of the patients. Psychologists are playing a vital role at the level of primary health care and supervision of health houses. Postgraduate training facilities for medical and nursing graduates are available. Training facilities for general physicians and mental health workers (or Behvarz) is also present. Manuals for the training of medical doctors and Behvarz are available. A difficulty noted in the provision of primary mental health care was the rapid turnover of doctors at this level (average stay of 3-6 months), which often led to many of the posted doctors not having specific mental health training. To keep up with the urban shift in population, neighbourhood health volunteers are being trained for preventive and promotive activities and appropriate referral.There are community care facilities for patients with mental disorders. Mental health is integrated into the primary care system whose basis is community care. Community participation is sought through involvement of NGOs and religious establishments in mental health care and public education (e.g. during mental health week).
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 1.6Psychiatric beds in mental hospitals per 10 000 population 1.4Psychiatric beds in general hospitals per 10 000 population 0.2Psychiatric beds in other settings per 10 000 population 0.04Number of psychiatrists per 100 000 population 1.9Number of neurosurgeons per 100 000 population 0.4Number of psychiatric nurses per 100 000 population 0.5Number of neurologists per 100 000 population 0.6Number of psychologists per 100 000 population 2Number of social workers per 100 000 population 0.6
Among the other 325 professionals are occupational therapists and medical assistants. Facilities for treatment of drug abusers (300 beds) and re-orientation centres for drug abusers with criminal and social problems are available. At least 100 beds are available
IRAN, ISLAMIC REPUBLIC OF

© 2005 World Health OrganizationMental Healthatlas
241
E –
I
for children with behavioural disorders. Board certification in child psychiatry with a two-year additional training period is available. There is no requirement for licensure or certification of clinical psychologists and they do not have prescription privileges. There are numerous psychologists working outside the mental health sector. Guidelines have been developed and refresher/training workshops have been held for physicians, nurses and social workers on demand-reduction issues.
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in advocacy and promotion. In 2004, many joint activities between the Department of Mental Health and NGOs were started on prevention, promotion and homecare for mentally ill patients.
Information Gathering System There is mental health reporting system in the country. There is a simple information system for mental disorders like psychosis, depression, epilepsy, mental retardation, etc.The country has no data collection system or epidemiological study on mental health. The Department of Mental Health in the MOH has recently started collecting national data on mental health with collaboration of the National Health Research Center. A national epidemiological study on mental health was done in 1999 (Noorbala, 2004) as an adjunct to the periodic National Health Survey.
Programmes for Special Population The country has specific programmes for mental health for disaster affected population and children. Though the mental health programme caters to all populations, since 2003, children and adolescents have been receiving more attention.There are special facilities for child and adolescent psychiatry in the form of special departments, training facilities, school mental health programmes. Special projects on school mental health and on prevention of child abuse and violence against women (in col-laboration with UNICEF and WHO) are under way. Life skills training has gained impetus and cascade training of main focal points in all provinces was accomplished in 2003. Four foundations provide special services ranging from consultation to rehabilitation to populations affected by war. Under the national programme on mental health interventions in natural disasters, more than 70 000 survivors received planned interventions during the 8 months after Bam earthquake and over 400 psychiatrists/psychologists and 1500 teachers were trained. Pilot projects on suicide prevention, under way in 4 cities have shown promising results. Integration of substance abuse prevention within primary health care and harm reduction activities including methadone maintenance and out-reach activities for street drug users has been launched with collaboration of MOH and NGOs.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, phenobarbital, phenytoin sodium, sodium valproate, chlorpromazine, diazepam, fluphenazine, haloperidol, lithium, biperiden.In 2003, the list was amended to include 32 medications, e.g. nortryptiline, fluoxetine, trihexiphenedyl, risperidone, etc.
Other Information
Additional Sources of InformationAgahi, C., Spencer, C. (1982) Patterns of drug use among secondary school children in post-revolutionary Iran. Drug & Alcohol Dependence, 9, 235-242.
Ahmadi, J., Benrazavi, L. (2002) Substance use among Iranian nephrologic patients. American Journal of Nephrology, 22, 11-13.
Ahmadi, J., Javadpour, A. (2001) Assessing substance use among Iranian healthcare students. Journal of Substance Use, 6, 196-198.
Ahmadi, J., Yazdanfar, F. (2002) Current substance abuse among Iranian university students. Addictive Disorders & Their Treatment, 1, 61-64.
Alemi, A. A. (1978) The iceberg of opium addiction. An epidemiological survey of opium addiction in a rural community. Drug & Alcohol Dependence, 3, 107-112.
Bash, K. W. (1984) Epidemiology of psychosomatic disorders in Iran. Psychotherapy & Psychosomatics, 42, 182-186.
Bash, K. W., Bash-Liechti, J. (1978) Psychiatric resurvey of a central Iranian village thirteen years later. Nervenarzt, 49, 713-719.
Ghobari, B., Bolhari, J. (2001) The current state of medical psychology in Iran. Journal of Clinical Psychology in Medical Settings, 8, 39-43.
Hashemi, N., London, M. (2003) Psyciatric practice in Iran and the UK. Psychiatric Bulletin, 27, 190-191.
Merchant, N. M., Pournadeali, E., Zimmer, S. P., et al (1976) Factors related to drug abuse among Iranian university students. Pahlavi Medical Journal, 7, 516-528.
Nobakht, M., Dezhkam, M. (2000) An epidemiological study of eating disorders in Iran. International Journal of Eating Disorders, 28, 265-271.
Noorbala, A. A., Bagheri Yazdi, S. A., Yasamy, M. T.,et al (2004) Mental health survey of the adult population in Iran. British Journal of Psychiatry, 184, 70-73.
Shadpour K. (2000) Primary health care networks in the Islamic Republic of Iran. Eastern Mediterranean Health Journal, 6, 822-825.
Shokrollahi, P., Mirmohamadi, M., Mehrabi, F., et al (1999) Prevalence of sexual dysfunction in women seeking services at family planning centers in Tehran. Journal of Sex & Marital Therapy, 25, 211-215.
Thornicroft, G., Sartorius, N. (1993) The course and outcome of depression in different cultures: 10-year follow-up of the WHO Collaborative Study on the Assessment of Depressive Disorders. Psychological Medicine, 23, 1023-1032.
Yasamy, M. T., Shahmohammadi, D., Bagheri Yazdi, S. A., et al. (2001). Mental health in the Islamic Republic of Iran: achievements and the areas of need. Eastern Mediterranian Health Journal, 7, 381-391.
Zarghami, M., Khalilian, A. (2002) Deliberate self-burning in Mazandaran, Iran. Burns, 28, 115-119.
IRAN, ISLAMIC REPUBLIC OF

© 2005 World Health OrganizationMental Healthatlas
242
E –
I
IraqGENERAL INFORMATIONIraq is a country with an approximate area of 438 thousand sq. km. (UNO, 2001). Its population is 25.856 million, and the sex ratio (men per hundred women) is 103 (UNO, 2004). The proportion of population under the age of 15 years is 41% (UNO, 2004), and the proportion of population above the age of 60 years is 5% (WHO, 2004). The literacy rate is 54.9% for men and 23.3% for women (UNESCO/MoH, 2004).The country is a lower middle income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 3.2%. The per capita total expenditure on health is 97 international $, and the per capita government expenditure on health is 31 international $ (WHO, 2004).The main language(s) used in the country is (are) Arabic and Kurdish. The largest ethnic group(s) is (are) Arab (four-fifths), and the other ethnic group(s) are (is) Kurdish. The largest religious group(s) is (are) Muslim.The life expectancy at birth is 59.1 years for males and 63.1 years for females (WHO, 2004). The healthy life expectancy at birth is 49 years for males and 52 years for females (WHO, 2004).
EPIDEMIOLOGYAhmad et al (1998, 2000a) developed the Posttraumatic Stress Symptoms in Children (PTSS-C) and applied it to a group of chil-dren affected by a mass-escape tragedy in Kurdistan; they found the prevalence rate of PTSD to be 20% according to DSM-III-R criteria. PTSD symptoms reduced at 4 month follow-up but were again high at 14 and 26 month follow-up. Dyregrov et al (2002) interviewed a group of 94 children, who had been exposed to a bombing that killed more than 750 people, at 6 months, 1 year and 2 years intervals with the help of selected items from different inventories, including the Impact of Event Scale (IES). The children continued to experience sadness and remained afraid of losing their family. Although there was no significant decline in intrusive and avoidance reactions as measured by the IES from 6 months to 1 year following the war, reactions were reduced 2 years after the war. However, the scores were still high, indicating that symptoms persist, with somewhat diminished intensity over time. Ahmed et al (2000b) interviewed randomly selected 45 pairs of children and their caregivers (mostly mothers) in two displacement camps in Kurdistan with the help of PTSS-C and the Harvard Trauma Questionnaire (HTQ). PTSD was reported in 87% of children and 60% of their caregivers. Childhood PTSD was significantly predicted by child trauma score and the duration of captivity, but was unaf-fected by maternal PTSD. It did not disappear after the reunion with the PTSD-free father. In a 1-year follow up study, Ahmad and Mohamad (1996) found that children in orphanages showed greater behavioural symptoms and PTSD compared to children in fos-ter care. Yasseen and Al-Musawi (2001) and Hamamy et al (1990) performed karyotypic analyses on children suffering from severe mental retardation and Down’s syndrome. The former study showed that while two-thirds of patients had chromosomal abnormali-ties, only 10% had recognizable syndromes. In the latter study, 81.9% of children with Down’s syndrome were shown to have trisomy 21 and 18.1% to have 46/47 + G type of mosaic. Examination for parental consanguinity revealed that 77.9%, 16.2% and 5.9% of the trisomy 21 cases and 53.3%, 26.7% and 20.0% of the mosaic cases were from non-consanguineous, first-cousin and second-cousin marriages, respectively. Amin-Zaki et al (1978, 1979) studied 32 infants exposed to methylmercury exposure over a 5 year period. In nine cases of cerebral palsy, methylmercury exposure occurred only during the last trimester or post-natally via suck-ling. Whereas the mother’s symptoms usually improved, the damage to the fetal nervous system appears to be permanent. Milder cases (minimal brain damage syndrome) previously not identified in other studies were also reported. The syndrome consists of vary-ing degrees of developmental retardation in addition to exaggerated tendon reflexes and the pathologic extensor plantar reflex.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is present. The policy was initially formulated in 1981.The components of the policy are advocacy, promotion, prevention, treatment and rehabilitation.
Substance Abuse Policy A substance abuse policy is present. The policy was initially formulated in 1965.
National Mental Health Programme A national mental health programme is present. The programme was formulated in 1987.The national mental health programme was started in 1989 and is concerned primarily with the integration of mental health with primary care leading to improvement of the mental health status of the country. Promotion of proper research facilities and informa-tion gathering systems are also a part of the programme. Coordination of mental health is done by the Iraqi Committee for Mental Health Promotion, an advisory body to the Minister of Health. In 2004, an advisory body called the National Council for Mental Health has been established in the MOH, which is working to formulate/implement a mental health policy, a mental health legisla-tion, a substance abuse policy and a national mental health programme.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. It was formulated in 1986.
Mental Health Legislation There is a Public Health Act ( No. 89/1981). This includes mental health issues. A draft of the mental health legislation has recently been submitted to the Government for approval.The latest legislation was enacted in 1981.

© 2005 World Health OrganizationMental Healthatlas
243
E –
I
Mental Health Financing There are budget allocations for mental health.Details about expenditure on mental health are not available.The primary sources of mental health financing in descending order are tax based and out of pocket expenditure by the patient or family.The country has disability benefits for persons with mental disorders. The services provided by the Government are free, though payment has to be made for private services.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is available at the primary level. Drugs are supplied to needy patients at the primary care level after confirmation of the diagnosis by specialists.Regular training of primary care professionals is carried out in the field of mental health. Postgraduation in psychology and training for paramedical staff is also present. Training is also provided to teachers, social workers employed in special schools, primary care physicians and nurses. General practitioners in the primary health centres are being trained in psychiatry in order to deliver better psychiatric services at the primary level. Short training courses for orientation are provided.There are community care facilities for patients with mental disorders. Care is provided through the facilities of the Ministry of Social Welfare.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 0.63Psychiatric beds in mental hospitals per 10 000 population 0.55Psychiatric beds in general hospitals per 10 000 population 0.06Psychiatric beds in other settings per 10 000 population 0.02Number of psychiatrists per 100 000 population 0.7Number of neurosurgeons per 100 000 population 0.09Number of psychiatric nurses per 100 000 population 0.1Number of neurologists per 100 000 population 0.04Number of psychologists per 100 000 population 0.05Number of social workers per 100 000 population 0.2
There are approximately 300 beds for forensic psychiatry and 15 beds for treatment of drug dependence. Approximately half of mental health professionals are based in Baghdad. Most psychiatrists have private clinics.
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in advocacy, prevention, treatment and rehabilitation. Training facilities are also provided by NGOs. The Iraqi Society of Psychiatrists, which is an NGO, is actively involved in the promotion of mental health. The Iraqi Mental Health foundation UK focuses on training and aca-demic liaison in the post-war situation. The Red Cross helped in the rehabilitation of Al-Rashad Mental Hospital in Baghdad, which had been seriously damaged by mobs during the War.
Information Gathering System There is mental health reporting system in the country. The country has data collection system or epidemiological study on mental health. There is a lack of proper information gathering system and monitoring of existing mental health services is not possible due to lack of operational data and other information.
Programmes for Special Population The country has specific programmes for mental health for refugees, disaster affected popu-lation, elderly and children. Special services are limited in scope.There are 12 schools for the mentally challenged. In addition, some homes for the elderly and institutes for homeless children and orphans are available.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, phenobarbital, phenytoin sodium, sodium valproate, amitriptyline, chlorpromazine, diazepam, fluphenazine, haloperi-dol, levodopa.The drug supply is erratic and new generation drugs are lacking.
Other Information One of the earliest psychiatric centres was set up in Baghdad, but since 1990, mental health facilities have suf-fered due to the war and embargo.
IRAQ

© 2005 World Health OrganizationMental Healthatlas
244
E –
I
Additional Sources of InformationAhmad, A., Mohamad, K. (1996) The socioemotional development of orphans in orphanages and traditional foster care in Iraqi Kurdistan. Child Abuse & Neglect, 20, 1161-1173.
Ahmad, A., Mohamed, H. T., Ameen, N. M. (1998) A 26-month follow-up of posttraumatic stress symptoms in children after the mass-escape tragedy in Iraqi Kurdistan. Nordic Journal of Psychiatry, 52, 357-366.
Ahmad, A., Sundelin-Wahlsten, V., Sofi, M. A., et al (2000a) Reliability and validity of a child-specific cross-cultural instrument for assessing posttraumatic stress disorder. European Child & Adolescent Psychiatry, 9, 285-294.
Ahmad, A., Sofi, M. A., Sundelin-Wahlsten, V., et al (2000b) Posttraumatic stress disorder in children after the military operation ‘Anfal’ in Iraqi Kurdistan. European Child & Adolescent Psychiatry, 9, 235-243.
Amin-Zaki, L., Majeed, M. A., Clarkson, T. W., et al (1978) Methylmercury poisoning in Iraqi children: clinical observations over two years. British Medical Journal, 1, 613-616.
Amin-Zaki, L., Majeed, M. A., Elhassani, S. B., et al (1979) Prenatal methylmercury poisoning. Clinical observations over five years. American Journal of Diseases of Children, 133, 172-177.
Dyer, O. (2003) British Iraqi doctors set up charity to support Iraq’s mental health services. British Medical Journal, 327, 832-833.
Dyregrov, A., Gjestad, R., Raundalen, M. (2002) Children exposed to warfare: a longitudinal study. Journal of Traumatic Stress, 15, 59-68.
Hamamy, H. A., al Hakkak, Z. S., al Taha, S. (1990) Consanguinity and the genetic control of Down syndrome. Clinical Genetics, 37, 24-29.
Yasseen, A. A., Al-Musawi, T. A. (2001) Cytogenetics study in severely mentally retarded patients. Saudi Medical Journal, 22, 444-449.
IRAQ

© 2005 World Health OrganizationMental Healthatlas
245
E –
I
IrelandGENERAL INFORMATIONIreland is a country with an approximate area of 70 thousand sq. km. (UNO, 2001). Its population is 3.999 million, and the sex ratio (men per hundred women) is 99 (UNO, 2004). The proportion of population under the age of 15 years is 21% (UNO, 2004), and the proportion of population above the age of 60 years is 15% (WHO, 2004). The literacy rate is 99% for men and 99% for women (UNESCO/MoH, 2004).The country is a high income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 6.5%. The per capita total expenditure on health is 1935 international $, and the per capita government expenditure on health is 1470 international $ (WHO, 2004).The main language(s) used in the country is (are) English and Irish. The largest religious group(s) is (are) Roman Catholic.The life expectancy at birth is 74.4 years for males and 79.8 years for females (WHO, 2004). The healthy life expectancy at birth is 68 years for males and 72 years for females (WHO, 2004).
EPIDEMIOLOGYThere is substantial epidemiological data on mental illnesses in Ireland in internationally accessible literature. No attempt was made to include this information here.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is present. The policy was initially formulated in 1984.The components of the policy are advocacy, promotion, prevention, treatment and rehabilitation. An Expert Group on Mental Health Policy to prepare a national policy framework for the further modernization of the mental health services, updating the 1984 policy document, Planning for the Future, was established on 4th August 2003. The Group has completed an extensive consultation process which included consultation initiatives with various stakeholders, including users of the mental health services. The Group is expected to complete its work in 2005.
Substance Abuse Policy A substance abuse policy is present. The policy was initially formulated in 1983. A National Drugs Strategy was published in 2001 and runs to 2008. This Strategy covers the four pillars of prevention and education, supply reduc-tion, treatment and rehabilitation and research.
National Mental Health Programme A national mental health programme is absent.Further to the publication of the Report of the National Task Force on Suicide in 1998, work has commenced on a new Strategic Action Plan for Suicide Reduction which is expected to be completed by June 2005. All measures aimed at reducing the number of deaths by suicide will be considered in the context of the preparation of this action plan.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. Details about the year of formulation are not available.
Mental Health Legislation The Mental Health Act, which was enacted in July 2001, will significantly improve safeguards for men-tally disordered persons who are involuntarily admitted for psychiatric care and treatment. The Act will bring Irish law in this area into conformity with the European Convention for the Protection of Human Rights and Fundamental Freedoms. The Act provided for the establishment of an independent agency known as the Mental Health Commission whose primary function is to promote and foster high standards and good practices in the delivery of mental health services and to ensure that the interests of detained persons are protected.The latest legislation was enacted in 2001.
Mental Health Financing There are budget allocations for mental health.The country spends 6.8% of the total health budget on mental health.The primary sources of mental health financing in descending order are tax based, private insurances, social insurance and out of pocket expenditure by the patient or family.About one-third of the population invests in voluntary health insurance, although all are entitled to public services.The country has disability benefits for persons with mental disorders.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is available at the primary level. Primary care is provided by general physicians, community care and primary care nurses and family doctors.Regular training of primary care professionals is carried out in the field of mental health. There are community care facilities for patients with mental disorders. There are community care facilities for the patients with men-tal disorders. There are community psychiatry nursing services, community residences, day hospitals and day care centres, voluntary associations and other rehabilitation facilities.
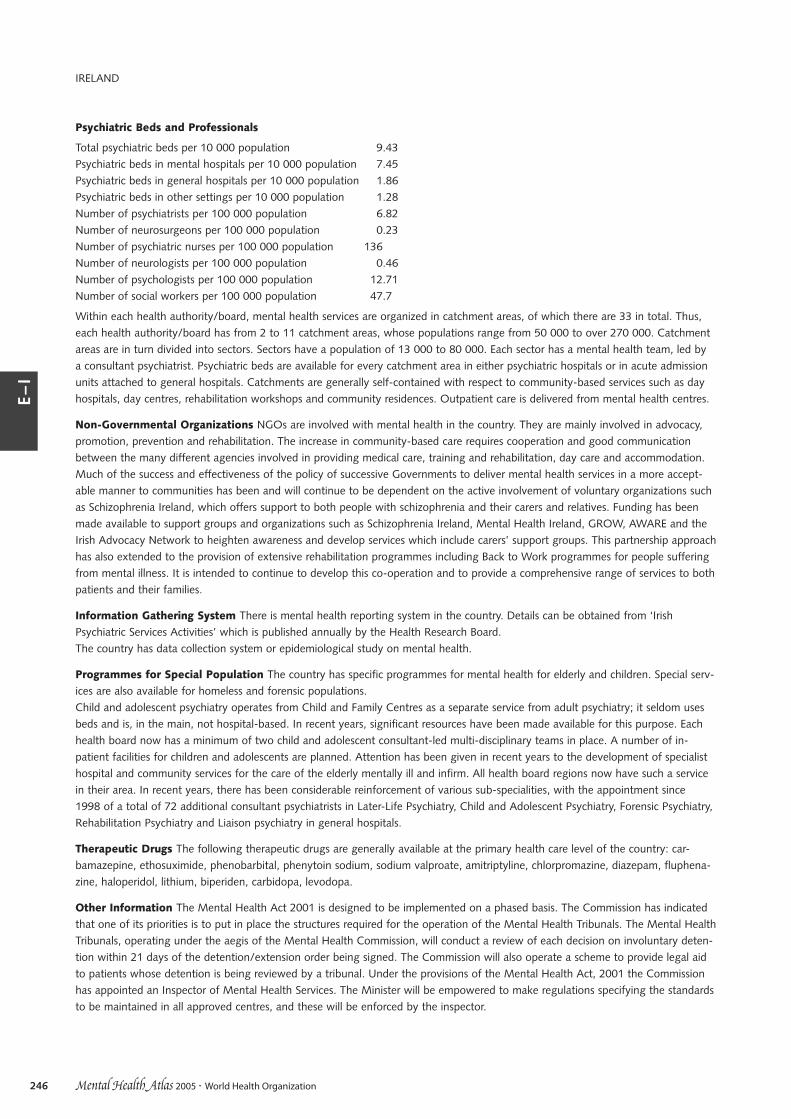
© 2005 World Health OrganizationMental Healthatlas
246
E –
I
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 9.43Psychiatric beds in mental hospitals per 10 000 population 7.45Psychiatric beds in general hospitals per 10 000 population 1.86Psychiatric beds in other settings per 10 000 population 1.28Number of psychiatrists per 100 000 population 6.82Number of neurosurgeons per 100 000 population 0.23Number of psychiatric nurses per 100 000 population 136Number of neurologists per 100 000 population 0.46Number of psychologists per 100 000 population 12.71Number of social workers per 100 000 population 47.7
Within each health authority/board, mental health services are organized in catchment areas, of which there are 33 in total. Thus, each health authority/board has from 2 to 11 catchment areas, whose populations range from 50 000 to over 270 000. Catchment areas are in turn divided into sectors. Sectors have a population of 13 000 to 80 000. Each sector has a mental health team, led by a consultant psychiatrist. Psychiatric beds are available for every catchment area in either psychiatric hospitals or in acute admission units attached to general hospitals. Catchments are generally self-contained with respect to community-based services such as day hospitals, day centres, rehabilitation workshops and community residences. Outpatient care is delivered from mental health centres.
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in advocacy, promotion, prevention and rehabilitation. The increase in community-based care requires cooperation and good communication between the many different agencies involved in providing medical care, training and rehabilitation, day care and accommodation. Much of the success and effectiveness of the policy of successive Governments to deliver mental health services in a more accept-able manner to communities has been and will continue to be dependent on the active involvement of voluntary organizations such as Schizophrenia Ireland, which offers support to both people with schizophrenia and their carers and relatives. Funding has been made available to support groups and organizations such as Schizophrenia Ireland, Mental Health Ireland, GROW, AWARE and the Irish Advocacy Network to heighten awareness and develop services which include carers’ support groups. This partnership approach has also extended to the provision of extensive rehabilitation programmes including Back to Work programmes for people suffering from mental illness. It is intended to continue to develop this co-operation and to provide a comprehensive range of services to both patients and their families.
Information Gathering System There is mental health reporting system in the country. Details can be obtained from ‘Irish Psychiatric Services Activities’ which is published annually by the Health Research Board.The country has data collection system or epidemiological study on mental health.
Programmes for Special Population The country has specific programmes for mental health for elderly and children. Special serv-ices are also available for homeless and forensic populations.Child and adolescent psychiatry operates from Child and Family Centres as a separate service from adult psychiatry; it seldom uses beds and is, in the main, not hospital-based. In recent years, significant resources have been made available for this purpose. Each health board now has a minimum of two child and adolescent consultant-led multi-disciplinary teams in place. A number of in-patient facilities for children and adolescents are planned. Attention has been given in recent years to the development of specialist hospital and community services for the care of the elderly mentally ill and infirm. All health board regions now have such a service in their area. In recent years, there has been considerable reinforcement of various sub-specialities, with the appointment since 1998 of a total of 72 additional consultant psychiatrists in Later-Life Psychiatry, Child and Adolescent Psychiatry, Forensic Psychiatry, Rehabilitation Psychiatry and Liaison psychiatry in general hospitals.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, ethosuximide, phenobarbital, phenytoin sodium, sodium valproate, amitriptyline, chlorpromazine, diazepam, fluphena-zine, haloperidol, lithium, biperiden, carbidopa, levodopa.
Other Information The Mental Health Act 2001 is designed to be implemented on a phased basis. The Commission has indicated that one of its priorities is to put in place the structures required for the operation of the Mental Health Tribunals. The Mental Health Tribunals, operating under the aegis of the Mental Health Commission, will conduct a review of each decision on involuntary deten-tion within 21 days of the detention/extension order being signed. The Commission will also operate a scheme to provide legal aid to patients whose detention is being reviewed by a tribunal. Under the provisions of the Mental Health Act, 2001 the Commission has appointed an Inspector of Mental Health Services. The Minister will be empowered to make regulations specifying the standards to be maintained in all approved centres, and these will be enforced by the inspector.
IRELAND

© 2005 World Health OrganizationMental Healthatlas
247
E –
I
Additional Sources of InformationDaly A., Walsh D. (2001) Irish Psychiatric Hospitals and Units Census. The Health Research Board.
Daly A., Walsh, D. (2002) Activities of Irish Psychiatric Services. The Health Research Board.
Ministry of Health. (2001) Mental Health Act.
Department of Health and Children (1998) Report of the National Task Force on Suicide
Department of Health and Children (2001) A National Drugs Strategy.
Department of Health and Children (2001) First Report of the Working Group on Child and Adolescent Psychiatric Services; Second Report (2003).
Department of Health and Children (2001) Health Strategy Quality and Fairness – A Health System for You.
Department of Health and Children (2004). Report of the Inspector of Mental Hospitals for the year ending 31st December, 2003.
McClelland, R., Webb, M., Mock, G. (2000) Mental health services in Ireland. International Journal of Law and Psychiatry, 23, 309-328.
Mental Health Commission, Annual Report (2003).
National Suicide Review Group, Annual Report (2003).
The Psychiatric Services – Planning for the Future: Report of a Study Group on the Development of Psychiatric Services. The Stationery Office (1984).
IRELAND

© 2005 World Health OrganizationMental Healthatlas
248
E –
I
IsraelGENERAL INFORMATIONIsrael is a country with an approximate area of 21 thousand sq. km. (UNO, 2001). Its population is 6.56 million, and the sex ratio (men per hundred women) is 98 (UNO, 2004). The proportion of population under the age of 15 years is 28% (UNO, 2004), and the proportion of population above the age of 60 years is 13% (WHO, 2004). The literacy rate is 97.3% for men and 93.4% for women (UNESCO/MoH, 2004).The country is a high income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 8.7%. The per capita total expenditure on health is 1839 international $, and the per capita government expenditure on health is 1272 international $ (WHO, 2004).The main language(s) used in the country is (are) Hebrew and Arabic. The largest ethnic group(s) is (are) Jew, and the other ethnic group(s) are (is) Arab. The largest religious group(s) is (are) Jew (four-fifths), and the other religious group(s) are (is) Muslim.The life expectancy at birth is 77.3 years for males and 81.4 years for females (WHO, 2004). The healthy life expectancy at birth is 70 years for males and 72 years for females (WHO, 2004).
EPIDEMIOLOGYThere is substantial epidemiological data on mental illnesses in Israel in internationally accessible literature. No attempt was made to include this information here.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is present. The policy was initially formulated in 1991.The components of the policy are advocacy, promotion, prevention, treatment and rehabilitation. The national mental health policy is not found in a single document. Besides the features mentioned above, the policy focuses on human resource training and safe-guarding patients’ rights. It is guided by community principles and great efforts are made to expand the network of community-based clinics and rehabilitation facilities. Integration of general health and mental health and constant pursuit of high quality and effective care provision are also a part of the basic principles of the policy.
Substance Abuse Policy A substance abuse policy is present. The policy was initially formulated in 1999.
National Mental Health Programme A national mental health programme is absent.Guidelines on a national mental health programme are present. A draft programme was formulated in 1995. Once adopted, the plan will be based on the following policy objectives, which are endorsed by almost all stakeholders: to promote the mental health of the population, to integrate mental health care within the general health system, to ensure equity of access to services in all parts of the country, to provide high-quality evidence-based and cost-effective care to persons with mental disorders, to promote the psy-chosocial rehabilitation of persons with mental disability, to strengthen and expand community-based care and reduce both hospital admission rates and length of stay, and to ensure the availability of emergency and crisis services, specially in security-related situa-tions.
National Therapeutic Drug Policy/Essential List of Drugs A national therapeutic drug policy/essential list of drugs is present. It was formulated in 1994.
Mental Health Legislation Mental health legislation has been advanced in recent years, e.g. The Community-Based Rehabilitation of the Mentally Disabled Act (2000); Patients’ Rights Act (1996); The Treatment of the Mentally Ill Act (1991); The Forensic Unit of the Mental Health Services Department of the Ministry of Health examines all subjects regarding compulsory admission, and along with the Ministry of Justice supervises some aspects of the work of the district psychiatric committees. The concept of diminished responsibility is reflected in the legislation – Law of Punishment (1977) and its amendment in 1995. There is also a provision for compulsory outpatient care. The 1996 Israel Law for Patients’ Rights introduces to the field of health legislation two new entities: internal examination committees and quality-control committees. The former investigates unusual, irregular or exceptional events related to diagnosis and/or treatment and shares its findings to the patient (or representatives). The Community-Based Rehabilitation of the Mentally Disabled Act (2000) grants all consumers whose degree of mental disability reaches 40%, as established by the National Insurance Institute, full entitlement to receive a set of rehabilitation services in the community.The latest legislation was enacted in 2000.

© 2005 World Health OrganizationMental Healthatlas
249
E –
I
Mental Health Financing There are budget allocations for mental health.The country spends 6.2% of the total health budget on mental health.The primary sources of mental health financing in descending order are tax based, social insurance, out of pocket expenditure by the patient or family and private insurances.By law, all residents are insured for health care and contribute to a national fund according to income. Most of the population is served by one of the four health maintenance organizations, the largest of which was established in the pre-State years (before 1948) by the labour unions. Importantly, the law that established this health system did not include either psychiatric care or geri-atric and nursing services. In 2002, the Government decided to transfer all responsibility for mental health care to the health main-tenance organizations; implementation of this decision is expected in 2005. Care provided by a general practitioner is free while a visit to a specialist (other than a psychiatrist) carries a nominal fee (less than US$5). Visits to a psychiatric clinic, care in a psychiatric hospital or hostel and drugs in the ‘basket of drugs’ are free of charge. The insurance schemes cover for a limited number of hours of psychotherapy, thus most patients needing psychotherapy pay for it privately. Preventive maternal and child health services are provided free by the municipalities and by the Ministry of Health. The budget for psychiatric community services is 29.4% of the budget allocated to mental health. The responsibility for psychosocial rehabilitation services is shared with the welfare services and, especially, with the National Insurance Institute. Disabled and dependent people are entitled to up to 95% of their rent (up to a cer-tain level). Rental payments are provided to eligible individuals by the Ministry of Housing.The country has disability benefits for persons with mental disorders.
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is available at the primary level. Regular training of primary care professionals is carried out in the field of mental health. There are community care facilities for patients with mental disorders. The rehabilitation facilities (about 224 in number) include sheltered housing, hostels, vocational rehabilitation units, employment services, social clubs and home care. The hostels are intended for those patients requiring intensive 24 hour care and assistance. Comprehensive hostels are for those with low level of functioning, but not requiring inpatient care. Sheltered housing are for those individuals who can live in the community, but still require some support in specific areas of their life. Other areas of community psychiatry (e.g. the rehabilitation of deviant youth, care for rape vic-tims) are covered by ministries other than health or by NGOs, which may or may not have governmental financial support.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 8.1Psychiatric beds in mental hospitals per 10 000 population 7.6Psychiatric beds in general hospitals per 10 000 population 0.4Psychiatric beds in other settings per 10 000 population 0.1Number of psychiatrists per 100 000 population 13.7Number of neurosurgeons per 100 000 population 0.8Number of psychiatric nurses per 100 000 population 10.7Number of neurologists per 100 000 population 3.6Number of psychologists per 100 000 population 35.6Number of social workers per 100 000 population 5.18
There are 2476 occupational therapists and 1742 creativity and self-expression therapists. About 6.6%, 16.3% and 2.6% of beds are for child and adolescents, geriatric and forensic services, respectively. Geographical inequality exists, thus central regions have many more beds than do northern and southern regions. A decline in the number of beds has occurred over the last two decades, but this has been more pronounced in the private sector. Private psychiatric hospitals mainly provide long-term care and are often similar to nursing homes. Their fee structure and management is regulated by the Government. In addition to psychiatric clinics in different settings, there are other clinics that provide outpatient care and rehabilitation facilities. Presently, most of the psychiatric care in the public sector is gratis and patients’ rights are embodied in special legislation. The six district offices are responsible for service planning, development, coordination and supervision of standards of work including those at general hospitals. About 156 psychiatrists specialize in child and adolescent practice. A postgraduate training programme for forensic psychiatry was initiated in 1997. About 67 psychiatrists have completed their diploma and 23 will complete it this year. A cadre of clinical criminologists, with training in academic criminology and sociology, psychology and health sciences also exists. Most psychologists working in the public sector supplement their income through private practice. Psychologists are not allowed to prescribe medication.
ISRAEL

© 2005 World Health OrganizationMental Healthatlas
250
E –
I
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in advocacy, promotion, prevention, treatment and rehabilitation. There are a number of self-help groups which are involved in activities related to mental health promotion and prevention of mental disorders. They also lobby with the Government on policy and service issues and provide support for families. In addition, several non-government organizations are active in mental health care, such as ERAN, which offers telephone first-aid assistance nationally, and another one that provides initial guidance to foreign workers. Eshet col-laborates with the Ministry of Health for occupational rehabilitation of mentally ill people. Volunteers’ activities in psychiatric institu-tions is expanding.
Information Gathering System There is mental health reporting system in the country. The country has data collection system or epidemiological study on mental health. A psychiatric case register that has been in operational since 1950. It records data related to psychiatric inpatient and day care facili-ties. More recently, the database has included information from most outpatient services. The confidentiality of the database is spe-cifically protected by law.
Programmes for Special Population The country has specific programmes for mental health for minorities, disaster affected pop-ulation, elderly and children. Services that cater to the needs of new immigrants are available.There are community centres and day-care centres for the treatment of autistic children and children with selected developmental disorders. There are psychological services in the school system as well. The Ministry of Education has a programme for promoting healthy life skills. The national strategies on drug abuse, including health promotion and prevention activities, is coordinated by an autonomous council. The services, such as methadone supply, however, are the responsibility of the Ministry ofHealth, in association with the welfare system. Special inpatient facilities are available for the treatment of adolescents with drug abuse and for patients with dual diagnosis. The Ministry of Social Affairs’ Division for Mental Retardation is in contact with approxi-mately 23 000 persons of all ages. Residential care is provided to about 6000 persons in 54 institutions countrywide. In addition, 2000 persons receive residential care in hostels or protected apartments within the community. More than 50 other settings provide vocational and educational services to 15 000 persons (day-care kindergartens, day-treatment centres, sheltered workshops or inte-grated care within the community). Secure facilities for treatment of mentally ill offenders are available. During the current wave of terrorist attacks, the Ministry of Health and several NGOs have established mental health activities that are provided as early as pos-sible in the emergency rooms and wards of general hospitals that treat casualties. The Ministry has trained several teams of mental health specialists that are attached to general hospitals. Half of them are trained to care for children and adolescents. Trained per-sonnel in outpatient clinics are entrusted with the care of persons affected by acute stress disorders or post-traumatic stress disorder. At the time of a national emergency, these outpatient clinics are open 24 hours a day.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, ethosuximide, phenobarbital, phenytoin sodium, sodium valproate, amitriptyline, chlorpromazine, diazepam, fluphena-zine, haloperidol, lithium, biperiden, carbidopa, levodopa.
Other Information The Division of Mental Health Services of the Ministry of Health is advised by two intersectoral advisory boards – one on mental health care and one responsible for psychosocial rehabilitation. Both boards include representatives from users of services and their families. The Division includes a special unit responsible for substance abuse that coordinates activities with the National Council against Drug Use. Since 1950, the Division cumulatively records all psychiatric admissions to inpatient facilities. Intersectoral cooperation has been facilitated by the social welfare orientation of the country. Primarily, the Ministry of Health coor-dinates with the Ministry of Labour and Welfare, the National Insurance Institute, the Judicial system and others. This cooperation operates at both the central and peripheral level. There has been a revamping of mental health services in Israel since the report by the Netanyahu Commission (1990) and the report of the State Comptroller’s office (1991). Details can be obtained from the docu-ment Mental Health in Israel (2000).
Additional Sources of InformationBarak, P., Gordon, H. (2002) Forensic psychiatry in Israel. Psychiatric Bulletin, 26, 143-145.
Laufer, N., Jecsmien, P., Hermesh, H., et al (1998) Application of models of working at the interface between primary care and mental health services in Israel. Israel Journal of Psychiatry & Related Sciences, 35, 120-127.
Mark, M., Rabinowitz, J., Feldman, D. (1997) Revampign mental health care in Israel: from the Netanyahu Commission to National Health Insurance Law. Social Work in Health Care, 25, 119-129.
Ministry of Health (2000) Mental Health in Israel. Annual Statistics 2000. Ministry of Health, Mental Health Services, Department of Information and Evaluation, Jerusalem.
Ministry of Health (1990) Report of the State Commission of Inquiry into the Operation and Efficiency of the Health Care System in Israel, Jerusalem.
Levav, I., Grinshpoon, A. (2004) Mental health services in Israel. International Psychiatry, 4, 10-14.
Merrick, J., Kandel, I. (2003) Medical services for persons with intellectual disability in Israel. Public Health Reviews, 31, 45-68.
Mester, R., Mozes, T., Spivak, B., et al (2000) The patient’s right to know, in the 1996 Israel law for the rights of the patient: the pains of progress. Israel Journal of Psychiatry & Related Sciences, 37, 95-102.
ISRAEL

© 2005 World Health OrganizationMental Healthatlas
251
E –
I
ItalyGENERAL INFORMATIONItaly is a country with an approximate area of 301 thousand sq. km. (UNO, 2001). Its population is 57.346 million, and the sex ratio (men per hundred women) is 94 (UNO, 2004). The proportion of population under the age of 15 years is 14% (UNO, 2004), and the proportion of population above the age of 60 years is 24% (WHO, 2004). The literacy rate is 98.9% for men and 98% for women (UNESCO/MoH, 2004).The country is a high income group country (based on World Bank 2004 criteria). The proportion of health budget to GDP is 8.4%. The per capita total expenditure on health is 2204 international $, and the per capita government expenditure on health is 1660 international $ (WHO, 2004).The main language(s) used in the country is (are) Italian. The largest ethnic group(s) is (are) Italian. The largest religious group(s) is (are) Roman Catholic.The life expectancy at birth is 76.8 years for males and 82.5 years for females (WHO, 2004). The healthy life expectancy at birth is 71 years for males and 75 years for females (WHO, 2004).
EPIDEMIOLOGYThere is substantial epidemiological data on mental illnesses in Italy in internationally accessible literature. No attempt was made to include this information here.
MENTAL HEALTH RESOURCESMental Health Policy A mental health policy is present. The policy was initially formulated in 1994.The components of the policy are advocacy, promotion, prevention, treatment and rehabilitation. The mental health policy is broadly defined in the National Plan for Mental Health. The first such plan was launched in 1994-96 and was essentially directed at the process of deinstitutionalization and the creation of community care facilities. The plan of 1998-2000, provided objectives and intervention strategies in order to monitor the progress and maintain uniform levels of care. The latest official policy is a part of the National Plan for Health (2003-2005) that includes a specific section about mental health.
Substance Abuse Policy A substance abuse policy is present. The policy was initially formulated in 1990.
National Mental Health Programme A national mental health programme is present. The programme was formulated in 1999.
National Therapeutic Drug Policy/Essential List of Drugs Details about the national therapeutic drug policy/essential list of drugs are not available.
Mental Health Legislation In Italy, the national laws are generally a wide framework of norms, the application of which is defined at local level by regional laws. Each region has a certain degree of autonomy. The most recent law is the ‘Target Project 1998-2000’; the first important approach was included in the Laws No. 180/1978 and No. 833/1978 (articles 33, 34, 35 and 64), the latter included the former. The reform law was then incorporated into a more comprehensive legislation setting up the National Health Service, which aimed to provide sectorized community based integrated services. Other than these, there are a number of articles under the Penal Code that guide forensic psychiatrists in criminal cases. Offenders suffering from mental disorders that make them liable to dangerous offenses are required to undergo treatment at a forensic psychiatry hospital and the others are treated in the community set-ups or general hospitals.The latest legislation was enacted in 1998.
Mental Health Financing There are budget allocations for mental health.Details about expenditure on mental health are not available.The primary sources of mental health financing in descending order are tax based, out of pocket expenditure by the patient or fam-ily and private insurances.The amount for mental health budget is defined by each regional programme and then more precisely at the level of local health units. Taxes are the primary source of financing for public services and out of pocket payments and private insurances for private services. Each citizen is registered with a primary care doctor under the National Health Service. Citizens have unlimited coverage, but need to contribute some proportions of the drug prescriptions, laboratory charges and diagnostic tests. There are local health districts catering to the needs of the catchment population, but it is not compulsory for residents to go to their local doctors only. Each local district has its own budget and is free to access services provided by non-governmental centres on payment of predeter-mined cost.The country has disability benefits for persons with mental disorders.

© 2005 World Health OrganizationMental Healthatlas
252
E –
I
Mental Health Facilities Mental health is a part of primary health care system. Actual treatment of severe mental disorders is available at the primary level. Mental health services are considered to be primary care services. Referral from primary care doctors is not required.Details about training facilities are not available. Training of medical doctors provide special emphasis on community care and they are trained to work in close contact with primary care doctors.There are community care facilities for patients with mental disorders. Mental Health Departments provide actual treatment for persons with mental disorders. These departments include and coordinate four different services: community facilities, day care facili-ties, residential facilities, and general hospital psychiatry wards. Though the implementation of community care in mental health has made mental health accessible to all, the quality of care is not uniform across the country. At present, there were 707 CMHC oper-ating in the country. There are more than more than 1552 residential facilities (17 101 beds) and 612 day care facilities. There are also more than 13 000 vocational organizations operating in the social sector that involve over 260 000 participants. Regional distri-bution of these facilities, however, is uneven, with only 20% located in the south. Territorial Pacts for Mental health is a new strat-egy promoting the functional integration of health, social, economic and vocational resources (both public and private) available in a given catchment area. The community itself is also expected to play a crucial role through vocational and self-help organizations.
Psychiatric Beds and Professionals
Total psychiatric beds per 10 000 population 4.63Psychiatric beds in mental hospitals per 10 000 population 0Psychiatric beds in general hospitals per 10 000 population 0.92Psychiatric beds in other settings per 10 000 population 3.7Number of psychiatrists per 100 000 population 9.8Number of neurosurgeons per 100 000 population Number of psychiatric nurses per 100 000 population 32.9Number of neurologists per 100 000 population Number of psychologists per 100 000 population 3.2Number of social workers per 100 000 population 6.4
There are 120 sociologists and 171 psychiatric rehabilitation therapists associated directly with mental health facilities. Also, there are more than 3700 workers (non mental health professionals) working in the social sector and the field of rehabilitation. All mental hospitals were gradually phased out with the last one being closed in 1999. General hospital psychiatry wards have a maximum of 15 beds. Non-residential medium and long-term facilities now account for more beds than the hospital sector. The service providing units are the mental health centre, psychiatric services for diagnosis and care, day hospital, day centre, residential facilities. The dis-trict services vary from region to region and also from centre to centre. Private care facilities have more than 50% of the acute short term beds in the country. Patients requiring long-term residential care are catered by non-hospital residential facilities (NHRFs).
Non-Governmental Organizations NGOs are involved with mental health in the country. They are mainly involved in advocacy, promotion, prevention, treatment and rehabilitation. Families are fundamental stakeholders in health administration and their asso-ciations have become very influential on national and regional mental health policies. They are involved in 60% of the organizations working in the mental health sector. There are twice as many voluntary organizations in the north as in the south.
Information Gathering System There is no mental health reporting system in the country. A national mental health reporting sys-tem is being developed. This system will become operational in 2006. However, six regional reporting systems that record data on mental health departments already exist.The country has data collection system or epidemiological study on mental health. These operate at regional level.
Programmes for Special Population The country has specific programmes for mental health for minorities, elderly and children. Substance misuse disorders, mental disorders in children and adolescents and forensic psychiatric sector are managed by specialist services which are not under the department of mental health. In the past, these facilities rarely contacted mental health, but now there is better integration of services.
Therapeutic Drugs The following therapeutic drugs are generally available at the primary health care level of the country: car-bamazepine, ethosuximide, phenobarbital, phenytoin sodium, sodium valproate, amitriptyline, chlorpromazine, diazepam, fluphena-zine, haloperidol, lithium, biperiden, carbidopa, levodopa.Atypical anti-psychotics like risperidone, clozapine, olanzapine and quetiapine are also available.
Other Information The deinstitutionalization movement was started by the psychiatrist Franco Basaglia in the state hospital of Gorizia and later this was modelled upon to formulate Law 180 in 1978. The 1990s witnessed the development of a comprehensive community care network. A recent study by the EPSILON Group showed that in Verona there were limited provisions for long stay residential services for patients suffering from schizophrenia and community care was the mainstay.
ITALY

© 2005 World Health OrganizationMental Healthatlas
253
E –
I
Additional Sources of InformationBarbato, A. (1998) Psychiatry in Transition: Outcomes of Mental Health Policy Shift in Italy. Australian and New Zealand Journal of Psychiatry, 32, 673-679.
Becker T., Hullsmann, S., Knudsen, H. C. et al & the EPSILON Group (2002) Provision of services for people with schizophrenia in five European regions. Journal of Social Psychiatry and Psychiatric Epidemiology, 37, 465-474.
Burti, L. (2001) Italian psychiatric reform 20 years plus years after. Acta Psychiatrica Scandinavica, 104 (suppl. 410), 41-46.
Crepet, P. (1990) A transition period in psychiatric care in Italy ten years after the reform. British Journal of Psychiatry, 156, 27-36.
De Salvia, D., Barbato, A. (1993) Recent trends in mental health services in Italy. Canadian Journal of Psychiatry, 38, 185-186.
de Girolamo, G., Cozza, M. (2000) The Italian psychiatric reform. International Journal of Law and Psychiatry, 23, 197-214.
de Girolamo, G., Picardi, A., Micciolo, R., et al for the PROGRES Group (2002) Residential care in Italy. British Journal of Psychiatry, 181, 220-225.
Fioritti, A., Bassi, M., de Girolamo, G. (2003) Italian psychiatry – 25 years of change. International Psychiatry, 2, 14-17.
Gazzetta Ufficiale Della Republica Italiana (1998) Approvazione del Piano Sanitario Nazionale per il Triennio 1998 – 2000.
Government document (1999) Mental Health Act Review – Mental Health Care in Italy.
Liffredo, C., Callegaro, D., Gallino, G. et al (1993) The role of the professional nurse in mental health service. Minerva Psichiatrica, 34, 117-120.
Piccinelli, M., Politi, P., Barale, F. (2002) Focus on psychiatry in Italy. British Journal of Psychiatry, 181, 538-544.
Traverso, G. B., Ciappi, S., Ferracuti, S. (2000) The treatment of the criminally insane in Italy. International Journal of Law and Psychiatry, 23, 493-508.
ITALY