
ECG Monitoring in the Elderly - UCSF Medical … · ECG Monitoring in the Elderly Preop ECG’s-...
8
1 Department of Anesthesia and Perioperative Care advancing health worldwide TM UC S F ECG Monitoring in the Elderly William A. Shapiro, M.D. http://anesthesia.ucsf.edu/shapiro Latest version of the slides http://www.anesthesia.ucsf.edu/shapiro This does NOT work Email: [email protected] Department of Anesthesia and Perioperative Care advancing health worldwide TM UC S F ECG Monitoring in the Elderly What is old? What is a ‘normal’ old heart? What ECG abnormalities increase with age? What ECG rhythms increase with age? What are current recommendations for preop ECG’s? What surgeries are common in the elderly population? Rhythm devices, anything new? Biomarkers, what are they, and how might they help? Department of Anesthesia and Perioperative Care advancing health worldwide TM UC S F World Health Organization: ECG Monitoring in the Elderly http://www.who.int/healthinfo/survey/ageingdefnolder/en/index.html The world's elderly population -people 60 years of age and older- is 650 million. By 2050, the ‘greying’ population is forecast to reach 2 billion. What is old? There is no United Nations standard numerical criterion, but the UN agreed cutoff is 60 years to refer to the older population United Nations: Department of Anesthesia and Perioperative Care advancing health worldwide TM UC S F ECG Monitoring in the Elderly The definition of retirement in the US is typically 65 years A society is considered relatively old when the fraction of the population aged 65 and over exceeds 8-10%. 1900- elderly fraction in the US was 4.1% 2000- elderly fraction in the US was 12.6% 2030- projected to increase to 20% Gavrilov L.A., Heuveline P. “Aging of Population.” 2007 http://longevity-science.org/Population_Aging.htm What is old in the US?
Transcript of ECG Monitoring in the Elderly - UCSF Medical … · ECG Monitoring in the Elderly Preop ECG’s-...

1
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the Elderly
William A. Shapiro, M.D.
http://anesthesia.ucsf.edu/shapiro
Latest version of the slides
http://www.anesthesia.ucsf.edu/shapiroThis does NOT work
Email: [email protected]
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the Elderly
� What is old?
� What is a ‘normal’ old heart?
� What ECG abnormalities increase with age?
� What ECG rhythms increase with age?
� What are current recommendations for preop ECG’s?
� What surgeries are common in the elderly population?
� Rhythm devices, anything new?
� Biomarkers, what are they, and how might they help?
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
World Health Organization:
ECG Monitoring in the Elderly
http://www.who.int/healthinfo/survey/ageingdefnolder/en/index.html
The world's elderly population -people 60 years of age and older- is 650 million. By 2050, the ‘greying’ population is forecast to reach 2 billion.
What is old?
There is no United Nations standard numerical criterion, but the UN agreed cutoff is 60 years to refer to the older population
United Nations:
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the Elderly
� The definition of retirement in the US is typically 65 years
� A society is considered relatively old when the fraction of the population aged 65 and over exceeds 8-10%.
� 1900- elderly fraction in the US was 4.1%
� 2000- elderly fraction in the US was 12.6%
� 2030- projected to increase to 20%
Gavrilov L.A., Heuveline P. “Aging of Population.” 2007 http://longevity-science.org/Population_Aging.htm
What is old in the US?

2
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the Elderly
http://www.cdc.gov/nchs/fastats/lifexpec.htm
Life expectancy at Birth
US- by race, sex
1970-2006
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
http://www.livestrong.com/article/128972-normal-pulse-rate-elderly/
• Although normal pulse rate values change a bit with advancing age, those differences are insignificant
• A 21-year-old man in good physical condition, for example, typically has a pulse rate between 62 and 65 beats per minutes
• This norm fluctuates a little over the years, but at age 65, it is still between 62 and 65
• If not in good physical condition, the resting heart rate is determined by disease and medication effects
ECG Monitoring in the Elderly
What is the normal age-related heart rate
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the Elderly
What are the most common ECG Abnormalities� Abnormalities increase with age
� Approx 50% of 50 year olds have ECG abnormalities
� LVH
� Increases in PR, QRS, and QT intervals
� Decrease in QRS amplitude
� Left ward axis shift in the frontal plane
� Prior MI
� Bundle branch block and Atrial Fibrillation
� Non-specific ST-segment and T-wave changes
Summary of References: 7-10
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the Elderly
Preop ECG Abnormalities- age > 70 (n=513)
� 75% had at least one ECG abnormality� 76% in patients with a cardiac history
� 71% in patients without cardiac history� Q-waves- 34%
� Left axis deviation- 19%� LVH- 7%� ST-T wave abnormalities- frequent
� Atrial fibrillation- 3.5%� No ECG abnormality was predictive of a post op event
Liu, et al. J Am Geriatr Soc 50:1186-91, 2002
3
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the Elderly
� Age not considered a reason to obtain a preop ECG� Symptoms determine testing
- ASA Preop Practice Advisory: No added predictive risk value of the preop ECG over symptoms
- Centers for Medicare and Medicaide Services do not reimburse for preop ECG’s, or age-based ECG’s
� AHA/ACC Recommendations for a preop ECG- Determined by clinical risk factors AND
- Type of surgery
Preop ECG’s- When are they indicated?
Summary of References: 1-6
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the Elderly
AHA/ACC Clinical Risk Factors- coronary artery disease- heart failure- diabetes
- cerebrovascular disease- creatinine >2.0 mg/dL
ACC/AHA 2007 guidelines for noncardiac surgery. Anesth Analg. 2008 Mar;106(3):685-712
Preop ECG’s- When are they indicated?
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the Elderly
Preop ECG’s- When are they indicated?
AHA/ACC Recommendations for preop ECG- Class I: Recommended� At least 1 clinical risk factor for vascular surgery
- Class IIa: Reasonable� No clinical risk factors and vascular surgery
- Class IIb: May be reasonable� At least 1 clinical risk factor and intermediate risk surgery
- Class III: Not indicated� Asymptomatic persons for low-risk (out-pt) surgeries
ACC/AHA 2007 guidelines for noncardiac surgery. Anesth Analg. 2008 Mar;106(3):685-712
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the Elderly
AHA/ACC: Arrhythmias to postpone elective surgery
�High grade block or Mobitz II AV block- High-Grade: ≥2 sinus P waves block consecutively in the
context of periodic AV conduction
�3rd degree AV block
�Symptomatic ventricular arrhythmias
�SVT with an uncontrolled ventricular rate
�Symptomatic bradycardia
�Newly recognized VT
ACC/AHA 2007 guidelines for noncardiac surgery. Anesth Analg. 2008 Mar;106(3):685-712
Preop ECG’s- Significant Arrhythmias
4
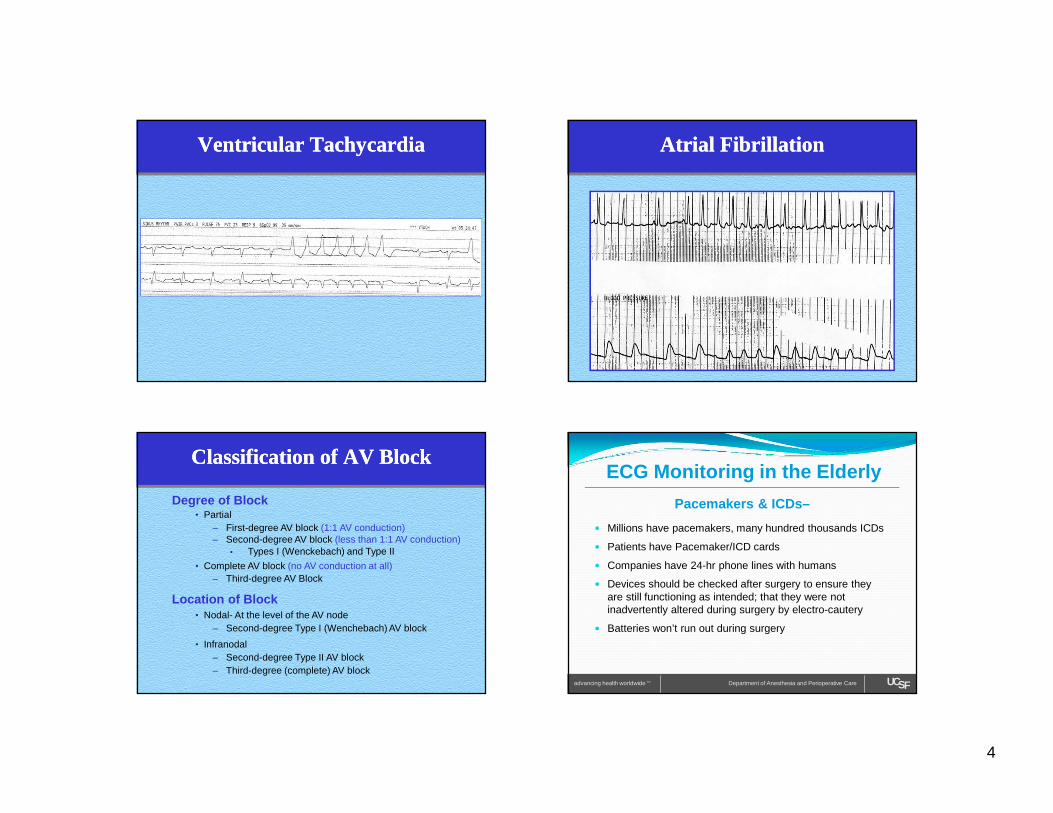
Ventricular TachycardiaVentricular Tachycardia
Classification of AV BlockClassification of AV Block
• Partial– First-degree AV block (1:1 AV conduction)– Second-degree AV block (less than 1:1 AV conduction)
• Types I (Wenckebach) and Type II
• Complete AV block (no AV conduction at all)– Third-degree AV Block
Degree of Block
Location of Block• Nodal- At the level of the AV node
– Second-degree Type I (Wenchebach) AV block
• Infranodal– Second-degree Type II AV block – Third-degree (complete) AV block
Atrial FibrillationAtrial Fibrillation
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the Elderly
� Millions have pacemakers, many hundred thousands ICDs
� Patients have Pacemaker/ICD cards
� Companies have 24-hr phone lines with humans
� Devices should be checked after surgery to ensure they are still functioning as intended; that they were not inadvertently altered during surgery by electro-cautery
� Batteries won’t run out during surgery
Pacemakers & ICDs–

5
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the Elderly
� ICD devices should be deactivated for surgery when the surgeon uses unipolar cautery
� When an ICD is deactivated, backup defibrillation must be immediately available
� Intermittent unipolar cautery does not guarantee the ICD will not discharge
� CVP placement is not contraindicated, but deserves special consideration in a patient with a pacemaker or an ICD, as there is potential for lead wire dislocation or infection
Pacemakers & ICDs–
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the Elderly
� Converts a “regular” pacemaker from the inhibited, or synchronous mode, to the asynchronous, or fixed-rate mode
� Deactivates the ICD sensing, and subsequent therapy,for atrial (SVT) or ventricular (VT, VF) tachycardias
� May do nothing at all
� Can active threshold testing mode
� Can ‘theoretically’ cause R-on-T induced arrhythmias
Pacemakers & ICDs– What will the magnet do?
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the Elderly
Paced rhythm with “R on T” Arrhythmia
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
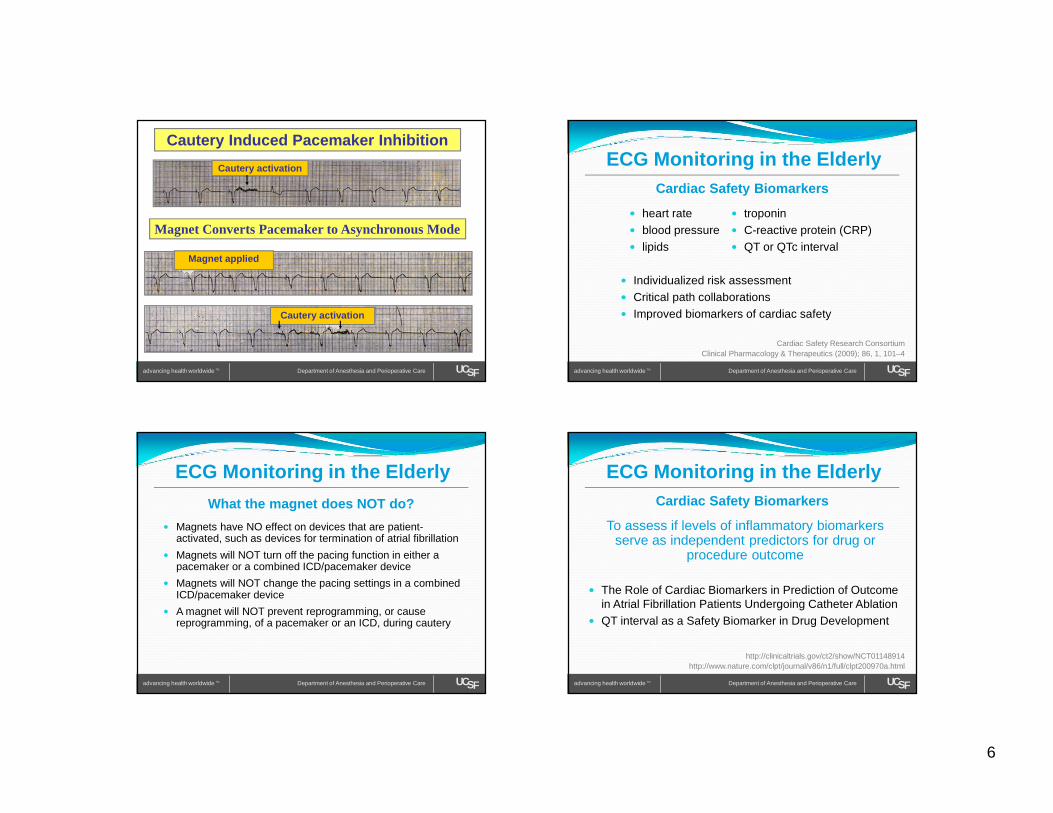
Cautery Pacemaker Inhibition
Magnet Converts Pacemaker to Asynchronous Mode
Cautery activation
Cautery activation
6
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
Magnet Converts Pacemaker to Asynchronous Mode
Cautery activation
Magnet applied
Cautery activation
Cautery Induced Pacemaker Inhibition
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the Elderly
What the magnet does NOT do?
� Magnets have NO effect on devices that are patient-activated, such as devices for termination of atrial fibrillation
� Magnets will NOT turn off the pacing function in either a pacemaker or a combined ICD/pacemaker device
� Magnets will NOT change the pacing settings in a combined ICD/pacemaker device
� A magnet will NOT prevent reprogramming, or cause reprogramming, of a pacemaker or an ICD, during cautery
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the Elderly
� heart rate� blood pressure� lipids
Cardiac Safety Biomarkers
� Individualized risk assessment� Critical path collaborations � Improved biomarkers of cardiac safety
Clinical Pharmacology & Therapeutics (2009); 86, 1, 101–4Cardiac Safety Research Consortium
� troponin� C-reactive protein (CRP)� QT or QTc interval
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the ElderlyCardiac Safety Biomarkers
� The Role of Cardiac Biomarkers in Prediction of Outcome in Atrial Fibrillation Patients Undergoing Catheter Ablation
� QT interval as a Safety Biomarker in Drug Development
http://clinicaltrials.gov/ct2/show/NCT01148914
To assess if levels of inflammatory biomarkers serve as independent predictors for drug or
procedure outcome
http://www.nature.com/clpt/journal/v86/n1/full/clpt200970a.html
7
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the ElderlySummary
� Elderly, in years, depends on your perspective� Resting heart rate is unchanged in healthy older adults� Static 12-lead ECG abnormalities increase with age� Preop ECG abnormalities not associated with
symptoms are not predictive of postop complications� No consensus exists for a preop ECG based on age� Future preop testing may measure biomarkers to
identify patients at risk for postop arrhythmias, or to better individualize postop cardiac risk assessment
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the Elderly
� Don’t obtain a preop ECG based solely on age� Obtain an ECG if the history, or symptoms, of cardiac
disease is present� Obtain a preoperative ECG for vascular surgery� Cataract surgery using topical anesthesia does not
require a preop ECG� A preop ECG can be useful for postop comparison � Use your judgment, document your reasons
Recommendations
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the Elderly
William A. Shapiro, M.D.
http://anesthesia.ucsf.edu/shapiro
Latest version of the slides
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the Elderly
1. Preoperative Electrocardiogram Abnormalities Do Not Predict Postoperative Cardiac Complications in Geriatric Surgical Patients. Liu, et al. J Am Geriatr Soc 50:1186–91, 2002
2. Preoperative Electrocardiograms- Patient Factors Predictive of Abnormalities. Correll, et al. Anesthesiology 2009; 110:1217–22
3. The role of testing in the preoperative evaluation. Hepner DL. Cleveland Clinic Journal of Medicine volume 76 • supplement 4 November 2009
4. Preoperative Electrocardiograms- Obsolete or Still Useful? De Hert SG. Anesthesiology 2009; 110:1205–6. (Editorial)
5. The Preoperative Electrocardiogram- What Is the Role in 2007? Annals of Surgery. Fleisher, LA. Volume 246, Number 2, August 2007 (Editorial)
6. The additional value of routine electrocardiograms in cardiovascular risk management of older people- The Leiden 85-plus study. De Ruijter, et al. Scand J Prim Health Care. 2008;26(3):147-53
References- preop ECGs

8
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the Elderly
7. Prevalence, prognosis, and implications of isolated minor nonspecific ST-segment and T-wave abnormalities in older adults: Cardiovascular Health Study. Kumar, et al. Circulation, 2008 Dec 16;118(25):2790-6
8. Preoperative electrocardiogram abnormalities do not predict postoperatvie cardiac complications in geriatric surgical patients. Liu, et al. J Am Geriatr Soc 50:1186-91, 2002
9. Prevalences of ECG findings in large population based samples of men and women. Bacquer, et al. Heart 2000;84:625–633
10. Major electrocardiographic abnormalities in persons aged 65 years and older (the Cardiovascular Health Study). Cardiovascular Health Study Collaborative Research Group. Furberg, et al. Am J Cardiol. 1992 May 15;69(16):1329-35.
References- ECG findings in the elderly
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the Elderly
11. The value of routine preoperative medical testing before cataract surgery. Schein, et al. N Engl J Med 2000;342:168-75
12. Routine preoperative medical testing for cataract surgery (Review). Keay, et al. Cochrane Database Syst Rev. 2009 Apr 15;(2) [http://www.thecochranelibrary.com]
13. 24-hour ambulatory electrocardiographic monitoring is unhelpful in the investigation of older persons with recurrent falls. Davison, et al. Age Ageing. 2005 Jul;34(4):382-6
14. Trends in Hospital Volume and Operative Mortality for High-Risk Surgery. Finks, et al. N Engl J Med 2011;364:2128-37.
15. Inpatient hospital admission and death after outpatient surgery in elderly patients: importance of patient and system characteristics and location of care. Fleisher, et al. Arch Surg 2004; 139:67–72.
References- specific surgery
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the ElderlyReferences- guidelines & advisories
16. Guidelines for pre-operative cardiac risk assessment and perioperative cardiac management in non-cardiac surgery. The Task Force for Preoperative Cardiac Risk Assessment and Perioperative Cardiac Management in Non-cardiac Surgery of the European Society of Cardiology (ESC) and endorsed by the European Society of Anaesthesiology (ESA). European Heart Journal (2009) 30, 2769–2812
17. Practice Advisory for the Perioperative Management of Patients with Cardiac Implantable Electronic Devices: Pacemakers and Implantable Cardioverter-Defibrillators An Updated Report by the American Society of Anesthesiologists Task Force on Perioperative Management of Patients with Cardiac Implantable Electronic Devices. Anesthesiology, V 114 • No 2, 247 February 2011
18. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery). Anesth Analg. 2008 Mar;106(3):685-712
Department of Anesthesia and Perioperative Care advancing health worldwide TM UCSF
ECG Monitoring in the Elderly
19. STATEMENT ON ROUTINE PREOPERATIVE LABORATORY AND DIAGNOSTIC SCREENING. Standards and Practice Parameters (Approved by the ASA House of Delegates on October 15, 2003, and last amended on October 22, 2008) [http://asahq.org/For-Healthcare-Professionals/Standards-Guidelines-and-Statements.aspx]
20. Biomarkers in Atrial Fibrillation, Ventricular Arrhythmias, and Sudden Cardiac Death. Mountantonakis et al. Cardiovasc Ther 2010 Nov 11
21. QT as a Safety Biomarker in Drug Development. Whellan et al. Clinical Pharmacology & Therapeutics (2009); 86, 1, 101–4
References- biomarkers
References- guidelines & advisories


















