Ebola
55
EBOLA VIRAL DISEASE GUIDE AND MODERATOR --- Dr. P.S. SINGH HOD, DEPARTMENT OF INTERNAL MEDICINE PRESENTED BY --- HIMANSHU SHARMA PG - 1, DEPARTMENT OF INTERNAL MEDICINE
-
Upload
himanshu-sharma -
Category
Health & Medicine
-
view
194 -
download
4
description
COMPREHENSIVE REVIEW OF EBOLA VIRAL DISEASE
Transcript of Ebola
EBOLA VIRAL DISEASE
GUIDE AND MODERATOR --- Dr. P.S. SINGHHOD, DEPARTMENT OF INTERNAL MEDICINE
PRESENTED BY --- HIMANSHU SHARMAPG - 1, DEPARTMENT OF INTERNAL MEDICINE
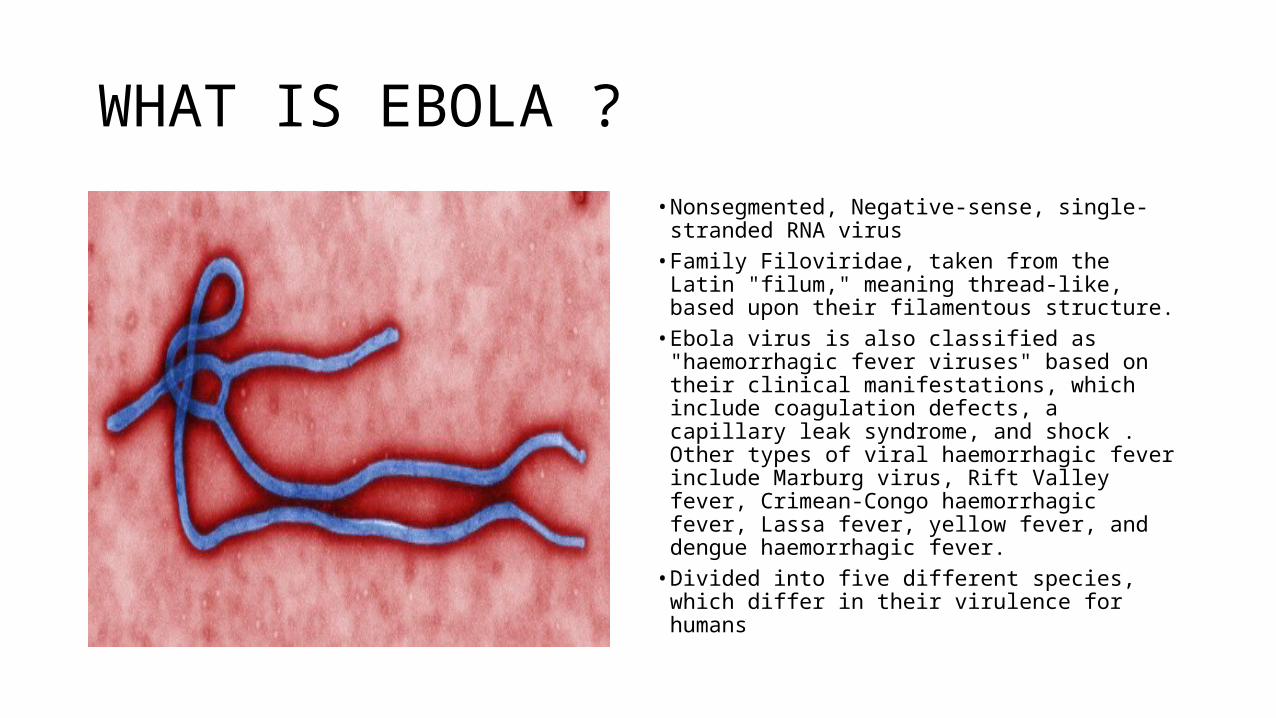
WHAT IS EBOLA ?
• Nonsegmented, Negative-sense, single-stranded RNA virus
• Family Filoviridae, taken from the Latin "filum," meaning thread-like, based upon their filamentous structure.
• Ebola virus is also classified as "haemorrhagic fever viruses" based on their clinical manifestations, which include coagulation defects, a capillary leak syndrome, and shock . Other types of viral haemorrhagic fever include Marburg virus, Rift Valley fever, Crimean-Congo haemorrhagic fever, Lassa fever, yellow fever, and dengue haemorrhagic fever.
• Divided into five different species, which differ in their virulence for humans
SPECIES
• First recognized in 1976, the Zaire species has caused multiple large outbreaks with mortality rates of 55 to 88 percent
• Sudan virus has been associated with an approximate 50 percent case-fatality rate in four known epidemics: two in Sudan in the 1970s, one in Uganda in 2000, and another in Sudan in 2004
• Ivory Coast virus has only been identified as the causative agent in one person, who survived. The exposure occurred when an ethologist performed a necropsy on a chimpanzee
• Bundibugyo virus emerged in Uganda in 2007, causing an outbreak of hemorrhagic fever with a lower case-fatality rate (approximately 30 percent)
• Reston virus, differs markedly from the others, because it is apparently maintained in an animal reservoir in the Philippines and has not been found in Africa NO HUMAN INFECTION TILL DATE
The name Ebola
• August 26, 1976 in Yambuku, a town in the north of Zaïre. A 44-year-old school teacher returned from a small hike. His went to the doctor and because of his high fever they gave him a quinine shot which is good against malaria.
• A week later, he had uncontrolled vomiting, bloody diarrhea, trouble breathing and then bleeding from his nose, mouth, and anus.
• He died 14 days after the onset of symptoms.
• He started an epidemic that killed 280 of the 313 infected persons (88%).
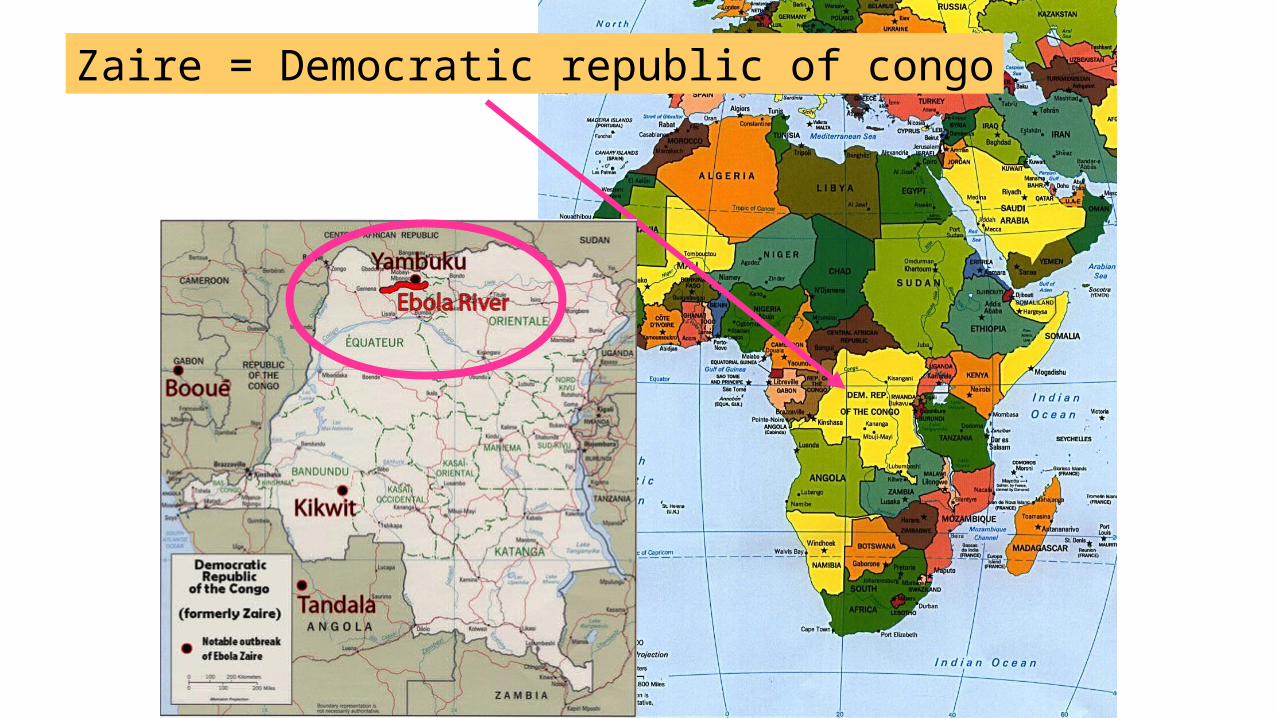
Zaire = Democratic republic of congo
EPIDEMIOLOGY
• Second major outbreak occurred in 1995 in the Democratic Republic of Congo, affecting 315 and killing 254
• Next major outbreak occurred in Uganda in 2000, affecting 425 and killing 224; in this case the Sudan virus was found to be the Ebola virus species responsible for the outbreak
• In 2003 there was an outbreak in the Republic of Congo that affected 143 and killed 128, a death rate of 90%, the highest to date
• In August 2007, 103 people were infected by a suspected hemorrhagic fever outbreak in the village of Kampungu, Democratic Republic of the Congo eventually affecting 264 individuals and resulted in the deaths of 187
• 30 November 2007, the Uganda Ministry of Health confirmed an outbreak of Ebola in the Bundibugyo District in Western Uganda WHO reported 149 cases of this new strain and 37 of those led to deaths
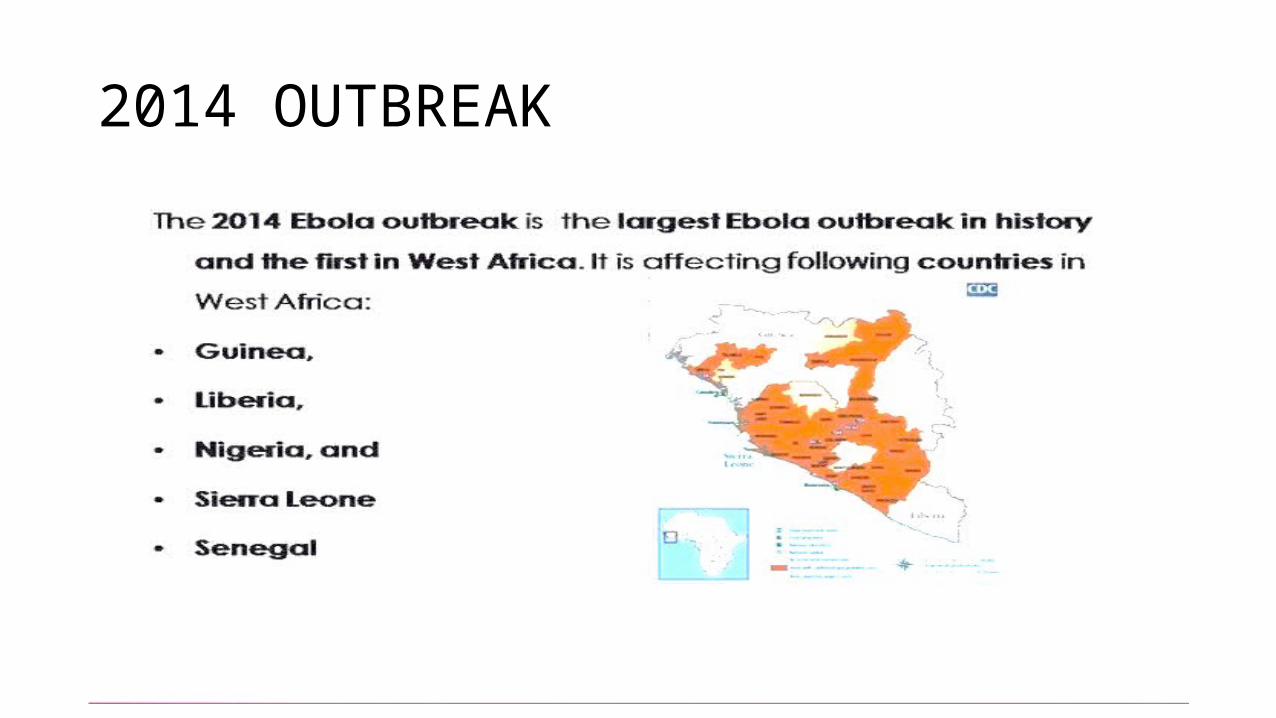
2014 OUTBREAK
Unrelated outbreak
• On august 26 democratic republic of congo confirmed an outbreak of ebola to WHO• Currently WHO update shows 66 cases and 37 deaths
TRANSMISSION
• Infection through direct contact of broken skin or mucous membranes with the blood or other bodily fluids or secretions (stool, urine, saliva, semen) of infected people• Infection can also occur if broken skin or mucous membrane comes in contact
with contaminated objects such as soiled clothing , linen or used needles• Contact with infected animals — Human infection with Ebola virus can occur
through contact with wild animals (e.g., hunting, butchering, and preparing meat from infected animals)• WHO does not advise families or communities to care for individuals who may
present with symptoms of Ebola in their homes • Patients are infectious as long as their blood and secretions contain the virus

• Nosocomial transmission — Medical procedures have played a major role in some of the largest Ebola and Marburg epidemics by amplifying the spread of infection. A tragic example of an iatrogenic point-source outbreak occurred in 1976, when an individual infected with Ebola virus was among the patients treated in a small missionary hospital in Yambuku, Zaire [65]. Because the medical staff routinely injected all febrile patients with antimalarial medications, employing syringes that were rinsed in the same pan of water, then reused, virus from the index case was transmitted simultaneously to nearly 100 people, all of whom developed fulminant Ebola virus disease and died [66]. Infection then spread to family caregivers, the hospital staff, and those who prepared bodies for burial. The Marburg epidemic in Angola in 2005 may have been initiated in similar fashion, through the reuse of contaminated blood bank equipment.
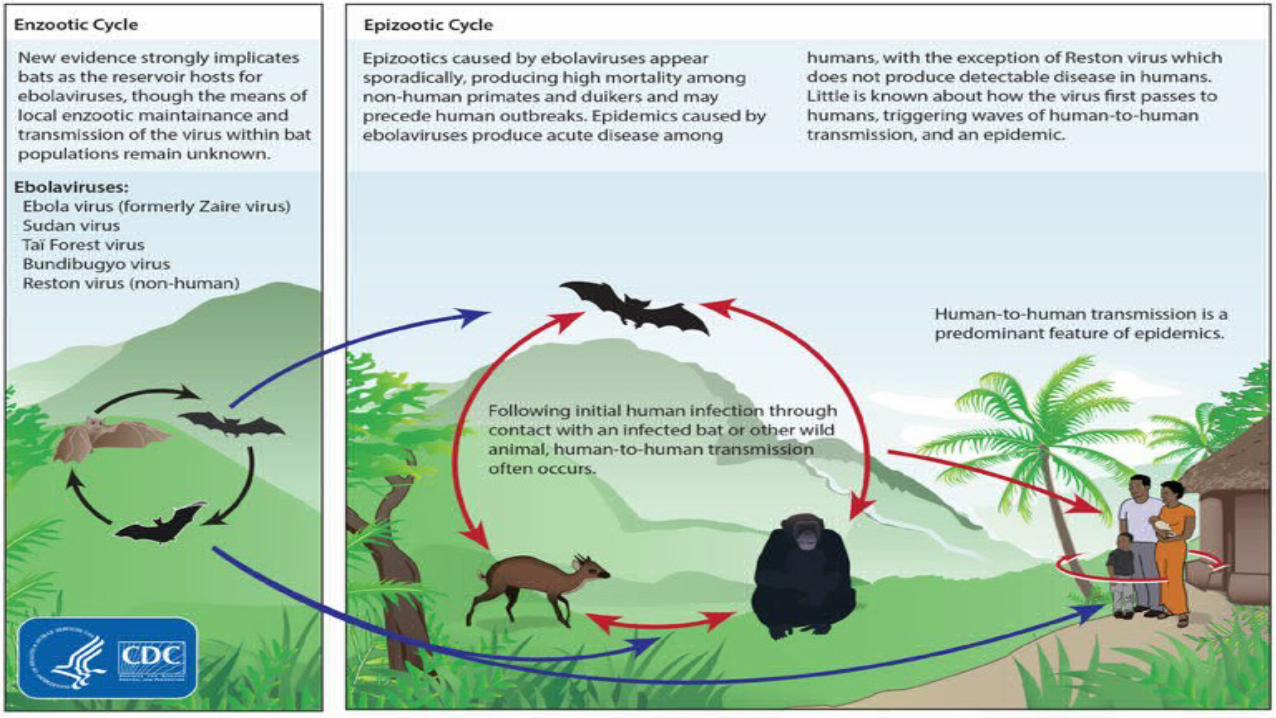
Reservoirs
• Nonhuman primates were initially suspected to be maintenance hosts for Ebola virus after infected monkeys introduced the agent into Europe. However, subsequent studies have shown that these animals are at least as susceptible as humans to rapidly lethal filoviral disease, precluding any role as a host for persistent viral infection• it appears likely that Ebola viruses are maintained in species of small
animals that serve as a source of infection for both humans and wild primates. Bats have long headed the list of suspects, because they have been present in large numbers at the sites of several filovirus outbreaks
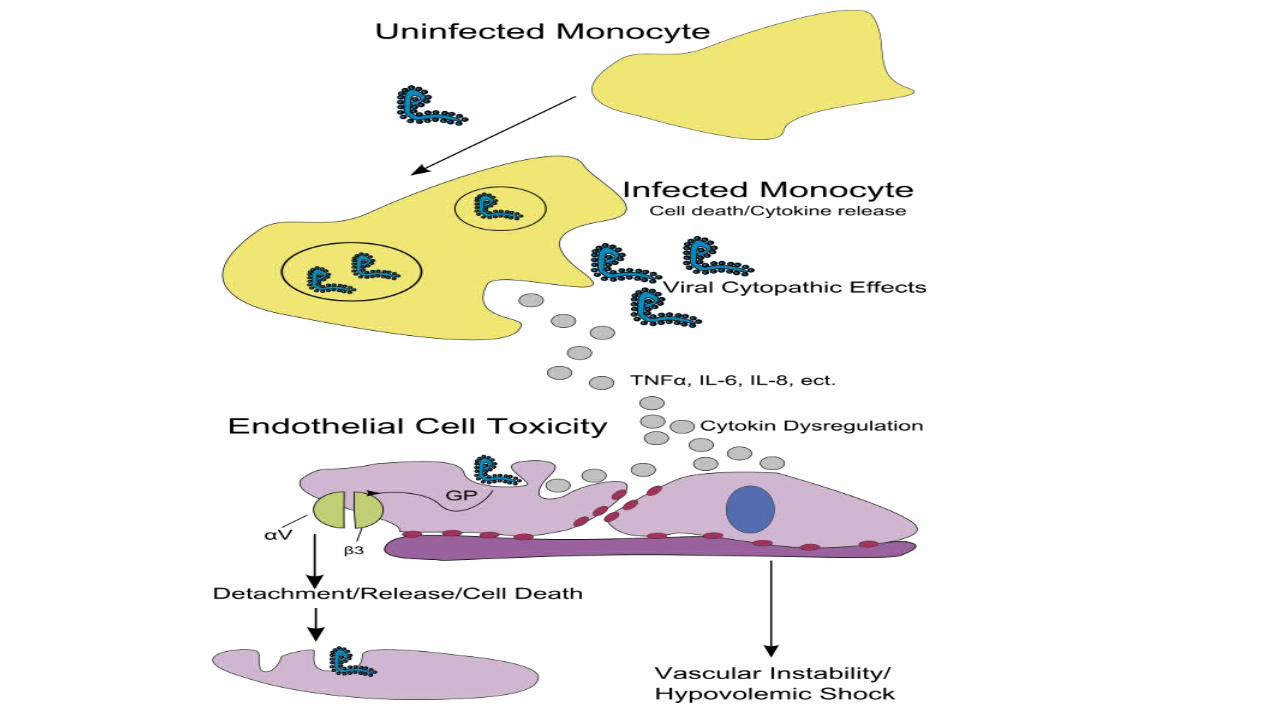
Pathogenesis
• Ebola virus enters the body through mucous membranes, breaks in the skin, or parenterally. The pathogen infects many cell types, including monocytes, macrophages, dendritic cells, endothelial cells, fibroblasts, hepatocytes, adrenal cortical cells, and epithelial cells• Macrophages and dendritic cells are probably the first cells to be infected. • Rapid systemic spread is aided by virus-induced suppression of type I
interferon responses• Systemic inflammatory response — In addition to causing extensive tissue
damage, filoviruses also induce a systemic inflammatory syndrome by inducing the release of cytokines, chemokines, and other proinflammatory mediators from infected macrophages and other cells
• Coagulation defects — The coagulation defects seen in Marburg and Ebola virus disease are also induced indirectly. Virus-infected macrophages synthesize cell-surface tissue factor (TF), triggering the extrinsic coagulation pathway. Proinflammatory cytokines also induce macrophages to produce TF• Impairment of adaptive immunity — Failure of adaptive immunity,
through impaired dendritic cell function and lymphocyte apoptosis, helps to explain how these viruses are able to cause severe, frequently fatal illness
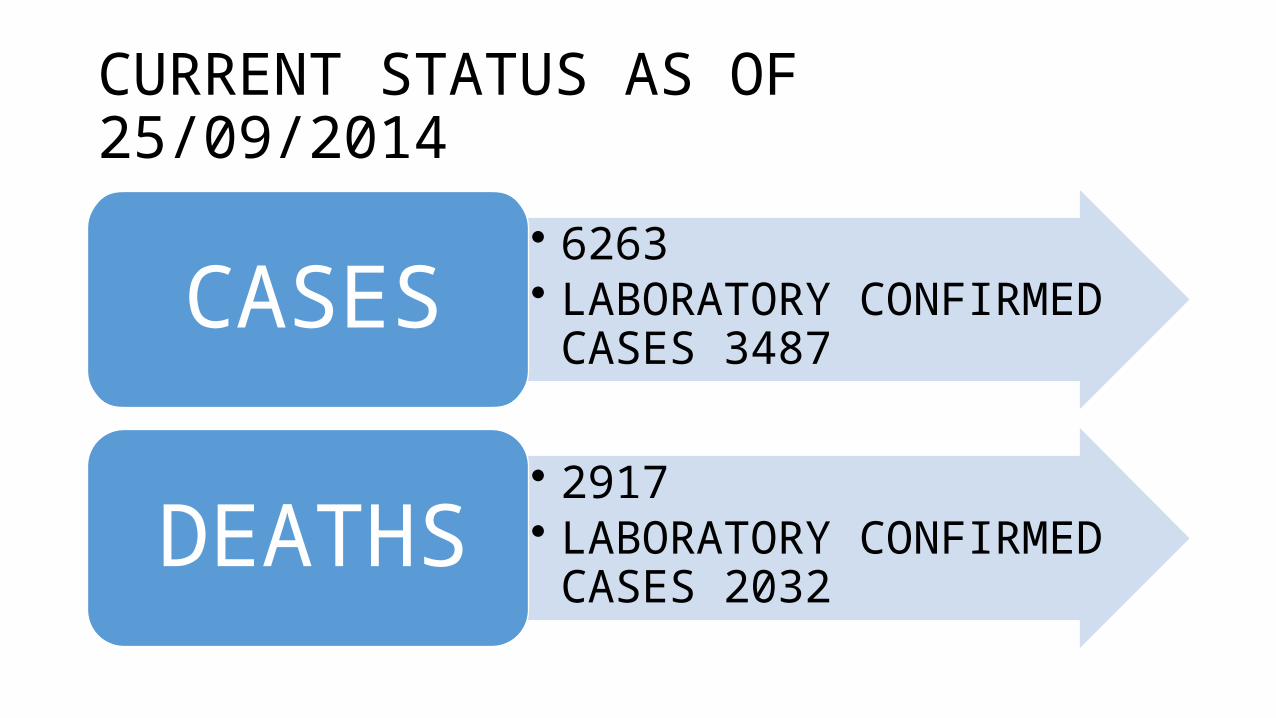
CURRENT STATUS AS OF 25/09/2014
• 6263• LABORATORY CONFIRMED
CASES 3487 CASES
• 2917• LABORATORY CONFIRMED
CASES 2032 DEATHS
CURRENT STATUS INDIA
• ON august 8 INDIA placed all of its airports on high alert and stepped surveillance of all travellers entering the country from Ebola affected regions• From AUGUST 9, passengers coming from Ebola affected countries
have to complete a form before landing; the form contains a checklist of symptoms and asks travellers from west Africa for information about places visited ,length of stay and other relevant information• In NEW DELHI Ram Manohar Lohia Hospital has been designated as a
treatment centre for Ebola virus disease cases• Phone numbers are 011 – 23061469,3205 and 1302

Clinical features
•Incubation period is typically 8 to 10 days, but can range from 2 to 21 days.•Patient is not infective during incubation period•Qurantine period is for 30 days
CLINICAL FEATURES
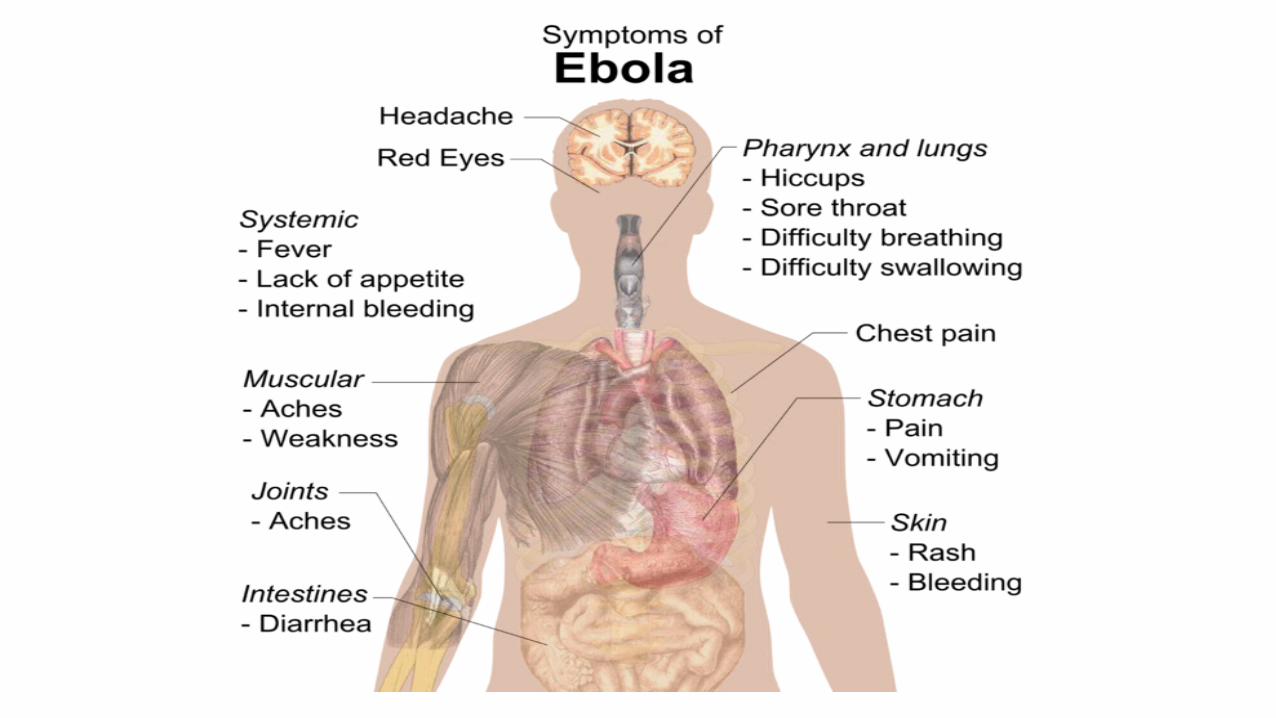
• Nonspecific flu-like symptoms — Ebola and Marburg haemorrhagic fever typically begin with the abrupt onset of fever, chills, and general malaise. Other signs and symptoms include weakness, anorexia, severe headache, and pain in the muscles of the trunk and lower back High fever may be accompanied by relative bradycardia, as seen in typhoid fever. A non-productive cough and pharyngitis, with the sensation of a lump or "ball" in the throat, are also frequently present.• Rash — Some patients develop a diffuse erythematous, nonpruritic
maculopapular rash by day five to seven of illness. The rash usually involves the face, neck, trunk, and arms, and can desquamate

• Gastrointestinal — Gastrointestinal signs and symptoms usually develop several days after the initial presentation. These include watery diarrhea, nausea, vomiting, and abdominal pain.• Hemorrhage — Bleeding is not universally present but can manifest later in
the course of disease as petechiae, ecchymosis/bruising, oozing from venipuncture sites, and/or mucosal hemorrhage. Frank hemorrhage is less common• Other findings — Patients with Ebola virus disease can present with
additional findings such as hiccups, chest pain, shortness of breath, headache, confusion, seizures, and/or cerebral edema. Conjunctival injection and dark red discoloration of the soft palate are common physical findings
Early clinical features of Ebola
• Intense tiredness, weakness, malaise • Conjunctivitis • Sudden onset of fever(define as
38.0˚C axillary)• Nausea and loss of appetite• Throat pain and difficulty
swallowing • Headache• Abdominal pain
• Myalgia(muscle pain)• Diarrhoea (can be bloody )• Arthralgia (joint pain)• Hiccups
• Note: There is often an overlap of early and late symptoms. Patients often do not develop all the signs and symptoms.
Late clinical features of Ebola
• Confusion and irritability • Seizures • Chest pain • Diarrhoea(watery or bloody) • Vomiting (sometimes bloody) • Skin rash • Internal and/or external bleeding
including: • Shock • Respiratory distress• Fever may be absent in late stages
• oozing from puncture sites• epistaxis • rashes suggestive of easy bleeding• hematemesis• haemoptysis• dark blood in stool• bleeding from the gums • unexplained vaginal bleeding in women• conjunctival haemorrhage• haematuria
• Pregnant patients with VHF often miscarry. However, vaginal bleeding and miscarriage can occur in any pregnancy. During an Ebola/Marburg or CCHF outbreak, fever with miscarriage or abnormal vaginal bleeding (other than normal menstruation) should prompt a PCR test to rule out VHF• Patients with fatal disease usually develop more severe clinical signs
early during infection and die between days 6 and 16 of complications including MODS and septic shock• Non fatal cases improve typically around day 6-11 may have
prolonged convalescence

Convalescence
• Patients who survive infection with Ebola virus typically show signs of clinical improvement during the second week of illness. In these patients, viremia also resolves during the second week, in association with the appearance of virus-specific antibodies• The convalescent period of Ebola virus disease is prolonged, and
marked by weakness, fatigue, and failure to regain weight that was lost during illness. Extensive sloughing of skin and hair loss are commonly observed, possibly as a result of virus-induced necrosis of infected sweat glands and other dermal structures
LABORATORY FINDINGS
• Leukopenia- Leukopenia usually presents as lymphopenia and is then followed by an elevated neutrophil count, with an increased percentage of immature forms• Thrombocytopenia- Platelet counts are usually in the range of 50,000
to 100,000/microL Platelet counts typically reach a nadir around day six to eight of illness• Transaminase elevations- multifocal hepatic necrosis, blood chemistry
tests usually demonstrate elevated serum aspartate aminotransferase (AST) and alanine aminotransferase (ALT) levels, with the former typically increasing more than the latter.
• Renal abnormalities- Proteinuria is a common finding, and renal insufficiency occurs with progression of illness• Coagulation abnormalities- Prothrombin (PT) and partial
thromboplastin times (PTT) are prolonged and fibrin degradation products are elevated, consistent with disseminated intravascular coagulation (DIC). These changes are most prominent in severe and fatal cases.• Marked decrease in total plasma protein (reflective of a capillary leak
syndrome)• Elevated amylase levels
Prognostic factors
• Patients who have evidence of severe intravascular volume depletion, metabolic abnormalities, and impaired oxygen delivery are most likely to have a poor outcome.• Signs and symptoms that are manifestations of these abnormalities
include tachypnea, anuria, delirium, coma, and irreversible shock • In addition, patients with persistently high or increasing Ebola virus
RNA levels in the bloodstream are likely to die• Novel biomarkers- proinflammatory cytokines have been associated
with viremia, haemorrhage, and death while soluble CD40 ligands have been associated with non-fatal outcome no clinical utility at present

Person Under Investigation (PUI)
1. Clinical criteria, which includes fever of greater than 38.6 degrees Celsius or 101.5 degrees Fahrenheit, and additional symptoms such as severe headache, muscle pain, vomiting, diarrhea, abdominal pain, or unexplained hemorrhage; AND
2. epidemiologic risk factors within the past 21 days before the onset of symptoms, such as contact with blood or other body fluids or human remains of a patient known to have or suspected to have EVD; residence in—or travel to—an area where EVD transmission is active*; or direct handling of bats or non-human primates from disease-endemic areas.
Probable Case
A PUI whose epidemiologic risk factors include high or low risk exposure(s)
High risk exposures
• A high risk exposure includes any of the following:• Percutaneous (e.g., needle stick) or mucous membrane exposure to
blood or body fluids of EVD patient• Direct skin contact with, or exposure to blood or body fluids of, an
EVD patient without appropriate personal protective equipment (PPE)• Processing blood or body fluids of a confirmed EVD patient without
appropriate PPE or standard biosafety precautions• Direct contact with a dead body without appropriate PPE in a country
where an EVD outbreak is occurring
Low risk exposures
• A low risk exposure includes any of the following• Household contact with an EVD patient• Other close contact with EVD patients in health care facilities or community
settings. Close contact is defined as• being within approximately 3 feet (1 meter) of an EVD patient or within the patient’s
room or care area for a prolonged period of time (e.g., health care personnel, household members) while not wearing recommended personal protective equipment (i.e., standard, droplet, and contact precautions)
• having direct brief contact (e.g., shaking hands) with an EVD patient while not wearing recommended personal protective equipment.
• Brief interactions, such as walking by a person or moving through a hospital, do not constitute close contact
Confirmed case
• A patient with above features and laboratory confirmed diagnostic evidence of ebola virus infection by anyone of the following• Ig M ELISA
• Antigen detection
• RT-PCR
From outbreak area, no direct exposure• The approach to evaluating symptomatic individuals from an outbreak
area who have no high- or low-risk exposures is less clear. According to the CDC, individuals who have fever with other signs or symptoms of Ebola virus disease within 21 days of visiting an Ebola virus disease-affected country should have medical evaluation and optional consultation with public health authorities to determine if movement restrictions and infection control precautions are indicated
Asymptomatic or symptoms not meeting clinical criteria• Monitoring for symptoms and signs of Ebola virus disease should be
performed for certain asymptomatic persons, as well as for those who do not meet the clinical criteria described above. This includes individuals who have:
●A high- or low-risk exposure●Spent time in a country in which an Ebola virus disease outbreak has occurred within the past 21 days• Such individuals should be monitored for 21 days after the last known
exposure (or after leaving the country if no known exposure) and should immediately report the development of fever or other symptoms suggestive of Ebola virus disease
INVESTIGATIONS
• It is recommended that the following specimens be collected for the diagnosis of EVD:
1. Whole blood in EDTA (a minimum volume of 4mL), collected in plastic tubes from live patients;2.Oral swabs stored in a universal transport medium, collected from deceased patients or in situations where blood collection is not possible e.g. children.Swab collection from live patients is not recommended due to lower sensitivity for reverse transcription polymerase chain reaction (RT PCR) and antigen detection
• If specimens are collected less than 3 days after onset of symptoms, additional specimens will be needed if the test result on the first specimen is negative.• The second specimen should be collected at least 48 hours after the
first specimen.• Whole blood for serological testing can be collected after 8 days of
onset of symptoms• Biosafety recommendations for laboratories conducting diagnostic
testing for EVD with appropriate biosafety level 4 (BSL4)/BSL3 facilities
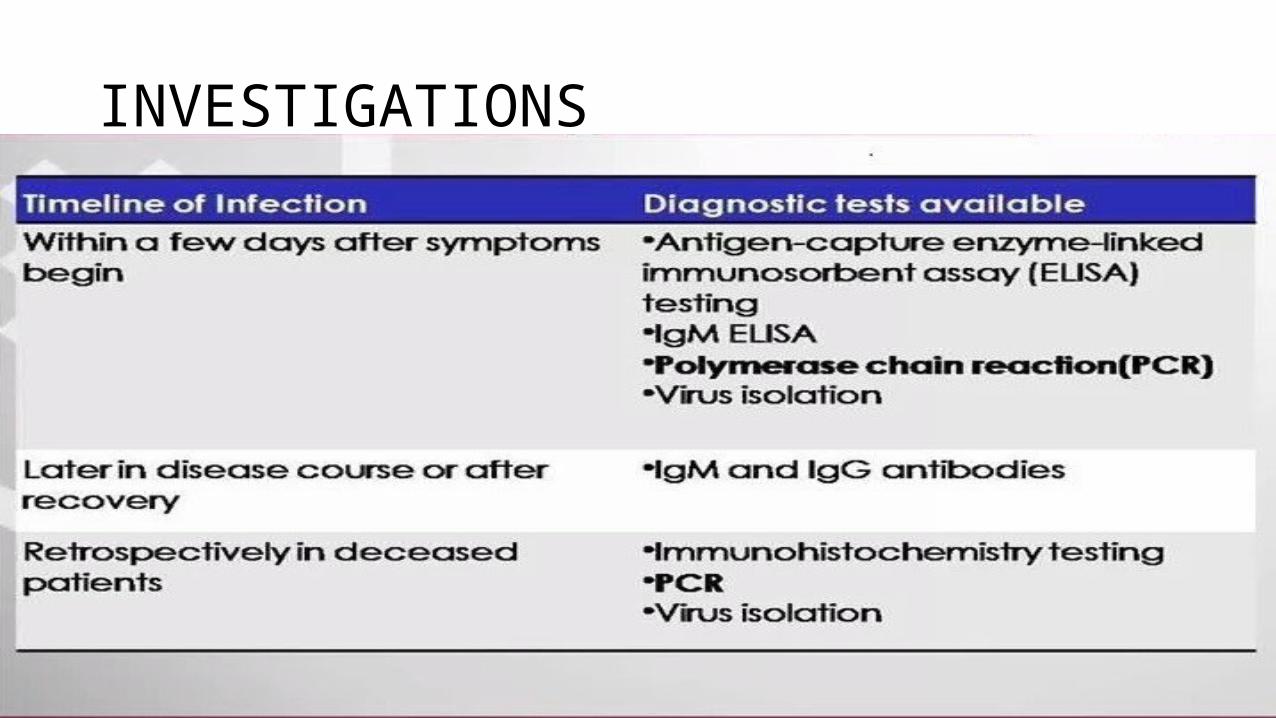
INVESTIGATIONS

• Virus is generally detectable by RT-PCR between 3 and 10 days after the onset of symptoms• Antigen detection may be used as a confirmatory test for immediate
diagnosis• Testing for IgM or IgG antibodies to Ebola virus may also be useful to
monitor the immune response over time and/or evaluate for past infection
TREATMENT
• Supportive care is the mainstay of treatment for patients with symptomatic Ebola viral disease• The manifestations of filoviral disease are caused principally by host
responses to infection, supportive care should focus on maintaining circulatory function and blood pressure, correction of severe coagulopathy, and other measures to keep the patient alive while the immune system mobilizes the antigen-specific immune responses needed to eliminate the pathogen
Experimental treatment
• Zmapp is an experimental treatment which combines three different monoclonal antibodies (c13C6 from MB-003 and two humanised mAbs from Zmab c2G4 and c4G7) that bind to protein of ebola virus• The WHO expert panel that convened in September 2014 has
identified the ChAd3(chimpanzee-adenovirus vaccine encoding the Ebola virus GP protected macaques) and VSV(recombinant vesicular stomatitis virus vector encoding Ebola surface GP), vaccines as the most advanced candidates for use in the West African outbreak• None of these has yet been tested in humans for safety or
effectiveness
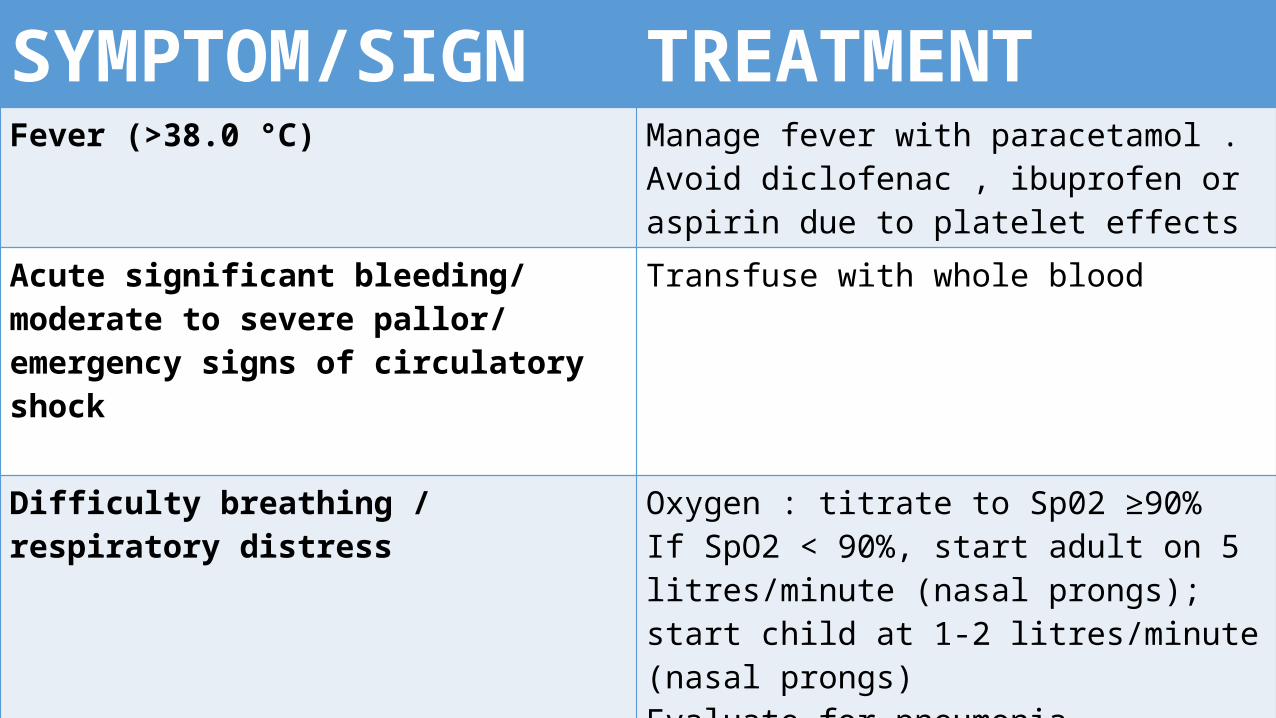
SYMPTOM/SIGN TREATMENTFever (>38.0 °C) Manage fever with paracetamol . Avoid
diclofenac , ibuprofen or aspirin due to platelet effects
Acute significant bleeding/ moderate to severe pallor/ emergency signs of circulatory shock
Transfuse with whole blood
Difficulty breathing / respiratory distress Oxygen : titrate to Sp02 ≥90% If SpO2 < 90%, start adult on 5 litres/minute (nasal prongs); start child at 1-2 litres/minute (nasal prongs) Evaluate for pneumonia, wheezing, fluid overload , congestive heart failure and manage accordingly. (Do not share nasal prongs –once used by a patient , dispose.)
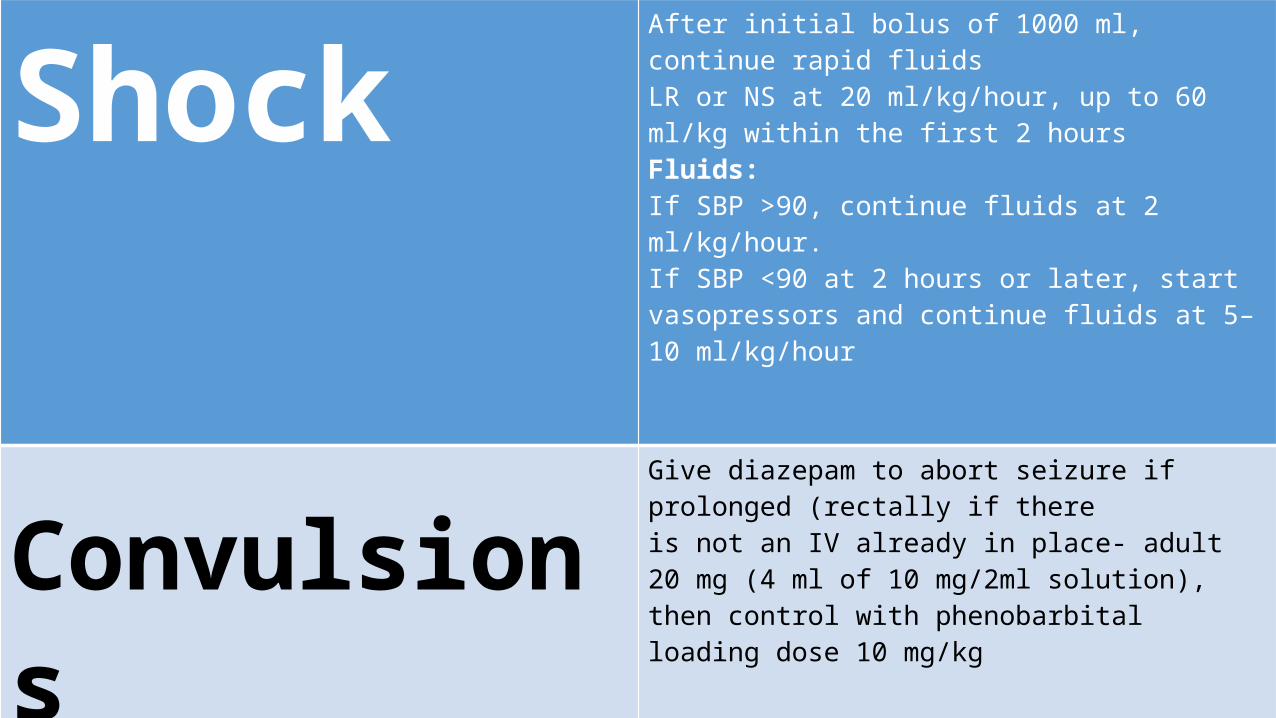
Shock After initial bolus of 1000 ml, continue rapid fluids LR or NS at 20 ml/kg/hour, up to 60 ml/kg within the first 2 hours Fluids: If SBP >90, continue fluids at 2 ml/kg/hour. If SBP <90 at 2 hours or later, start vasopressors and continue fluids at 5–10 ml/kg/hour
Convulsions Give diazepam to abort seizure if prolonged (rectally if there is not an IV already in place- adult 20 mg (4 ml of 10 mg/2ml solution), then control with phenobarbital loading dose 10 mg/kg
Diarrhoea, vomiting, signs of dehydration
Provide ORS even if no signs of dehydrationNausea and vomiting are common- anti-emetic medications may provide some relief and facilitate oral rehydration
Discharge of the patient
• Three or more days without fever or any significant symptom1. Symptoms that suggest ongoing shedding of virus (e.g. diarrhoea, coughing,
bleeding) should have completely disappeared. Viral shedding known to occur in the semen of male patients, and probably in the breast milk of lactating females, need not preclude discharge AND • Significant improvement in clinical condition AND • In a relatively good general condition: independently feeding and to carry out
other activities of daily life, like washing and walking, without assistance, taking into account any previous disabilities.
If laboratory testing is available
• A negative blood PCR for Ebola (regardless of any other serologic tests) on day 3 or later following onset of symptoms. • For patients with previous positive blood PCR tests, this
means a subsequent negative test 48 hours from the initial test (regardless of serology). • For previously blood PCR positive mothers, that are breast
feeding, it may be safer to delay discharge until PCR on breast milk turns negative as well

Protective measures for general public• To protect yourself, your family, and your community from EVD
transmission, immediately report to the nearest health facility if you develop symptoms indicative of EVD, including high fever, body aches, joint pain, vomiting, diarrhoea, or haemorrhaging. Isolation and professional clinical treatment increase a person’s chance of survival.• The risk of Ebola transmission is low. Becoming infected requires
direct, physical contact with the bodily fluids (vomit, faeces, urine, blood, semen, etc.) of people who have been infected with or died from Ebola virus disease
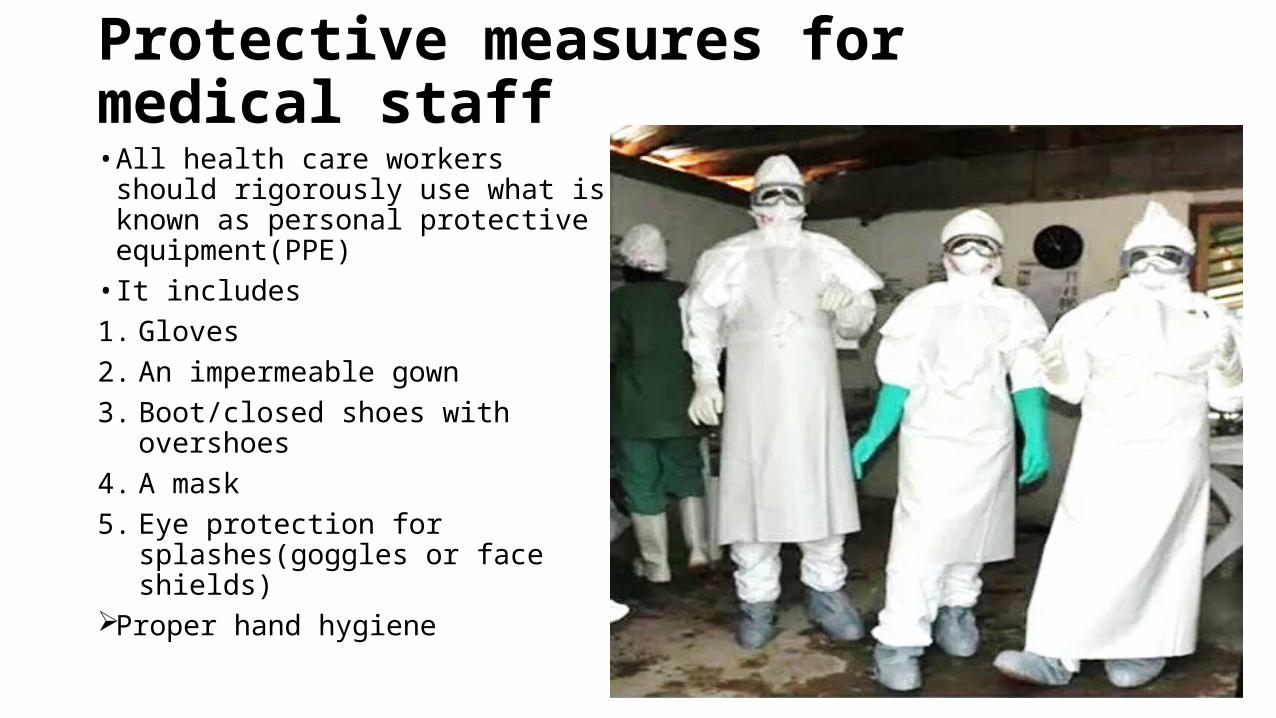
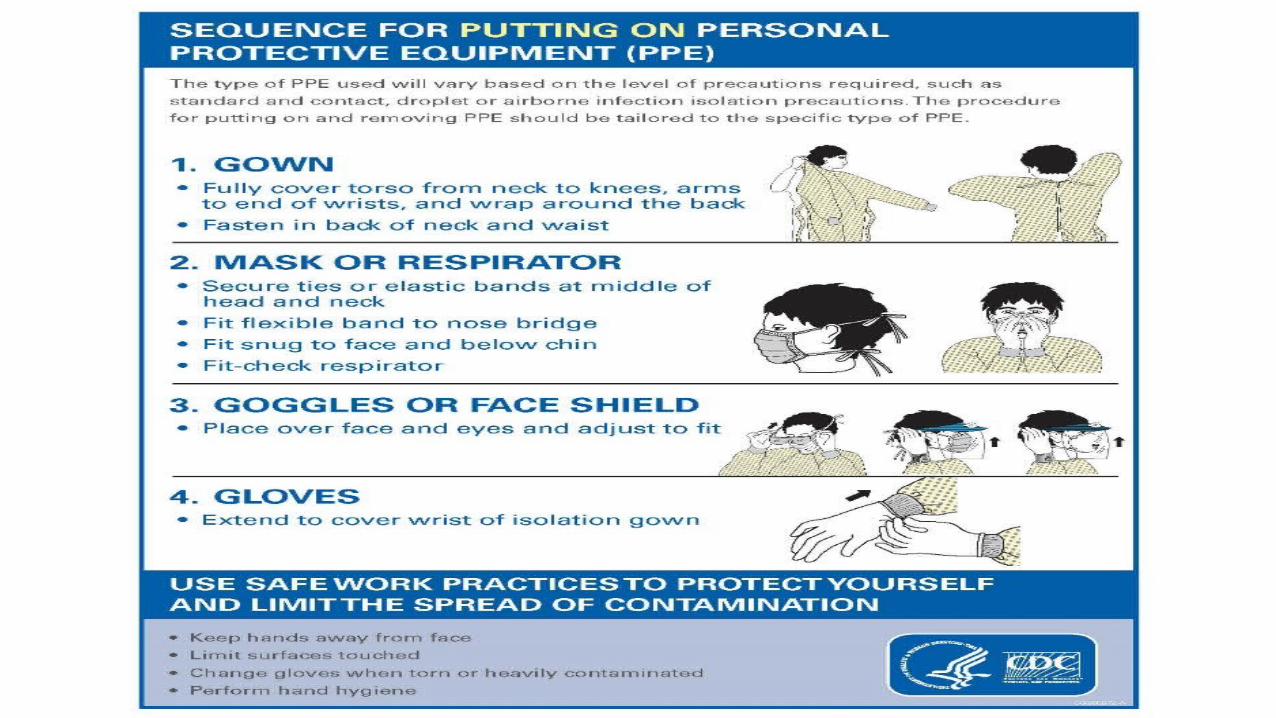
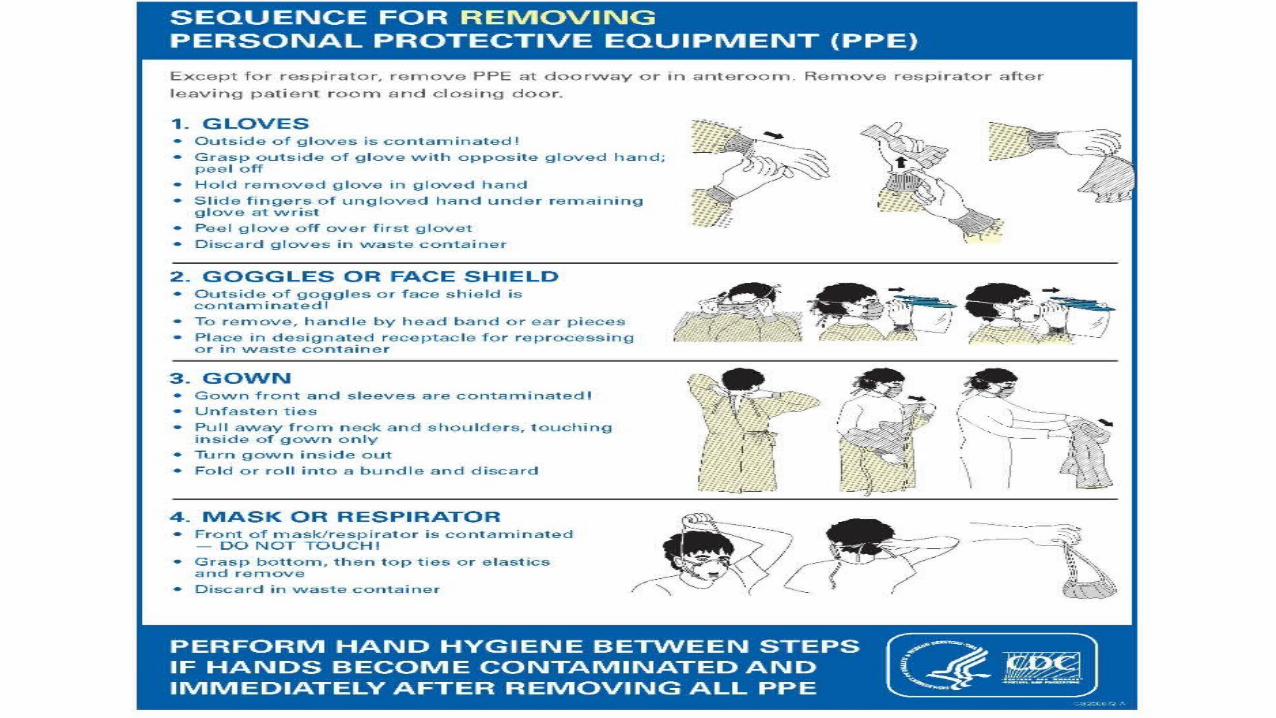
Protective measures for medical staff• All health care workers should
rigorously use what is known as personal protective equipment(PPE)• It includes1. Gloves2. An impermeable gown3. Boot/closed shoes with overshoes4. A mask5. Eye protection for
splashes(goggles or face shields)Proper hand hygiene

For laboratory medical staff• Suits known as
positive pressure biosafety suits are to be used at BSL 3 or BSL 4 labs• Proper waste
disposal is required
Conclusion
• Ebola virus is classified as "haemorrhagic fever virus" based on its clinical manifestations, which include coagulation defects, a capillary leak syndrome, and shock. Only 47% survival rate• Incubation period is typically 8 to 10 days, but can range from 2 to 21
day• An abrupt onset of non-specific symptoms, such as fever, malaise, and
myalgias. As the illness progresses, patients develop worsening prostration, stupor, and hypotension. Signs of impaired coagulation generally remain limited to conjunctival hemorrhages, easy bruising, and failure of venipuncture sites to clot
• Early symptoms are non specific, history of travel to affected area is important• Only supportive care can be given no specific treatment available• The most effective way to stop the current Ebola outbreak in west
Africa is meticulous case finding, isolating and caring for these patients and contact tracing for stopping the chain of transmission
BIBLIOGRAPHY
1. World Health Organization. Global Alert and Response. Ebola virus disease, West Africa
2. Centers for Disease Control and Prevention. Health advisory network 367: CDC Ebola Response Update
3. Uptodate Epidemiology, pathogenesis, and clinical manifestations of Ebola and Marburg virus disease
4. Uptodate Diagnosis and treatment of Ebola and Marburg virus disease
5. World Health Organization :Clinical Management of Patients with Viral Haemorrhagic Fever: A Pocket Guide
THANK YOU

![OCB Ebola Review Summary Report Finalcdn.evaluation.msf.org/.../ocb_ebola_review_summary_report_final_3… · OCB EBOLA REVIEWOCB EBOLA REVIEW SUMMARY REPORT [[[[AprilAprilApril 2012200112016666]]]]](https://static.fdocuments.in/doc/165x107/5b05e1847f8b9ad1768c04f0/ocb-ebola-review-summary-report-ebola-reviewocb-ebola-review-summary-report-aprilaprilapril.jpg)