Duplex Ultrasonography to Predict Internal Carotid by NASCET: The
10
Vascular Surgery VOLUME 33 SEPTEMBER/OCTOBER 1999 NUMBER 5 Duplex Ultrasonography to Predict Internal Carotid Artery Stenoses Exceeding 50% and 70% as Defined by NASCET: The Need for Multiple Criteria Edward D. Kreske, MD Seth W. Wolk, MD Charles J. Shanley, MD Richard M. Lampman, PhD James E. Knake, MD* Leslie A. Lange, MS" Errol E. Erlandson, MD and Walter M. Whitehouse, Jr, MD ANN ARBOR, MICHIGAN Carotid duplex scanning is being used more frequently as the sole preoperative diag- nostic imaging modality for patients considered candidates for carotid endarterectomy. The North American Symptomatic Carotid Endarterectomy Trial (NASCET) has demon- strated the benefit of surgical treatment in patients with carotid stenoses exceeding 70%. The purpose of this study was to determine duplex criteria that accurately predict carotid stenoses exceeding 50% and 70% as defined by NASCET arteriographic criteria. One hundred forty-one patients (264 carotid arteries) considered surgical candidates were prospectively studied over a 2-year period by use of both duplex scanning and digital subtraction cerebral arteriography. Carotid artery stenosis was determined by a single radiologist using NASCET arteriographic criteria. Peak systolic velocity (PSV) and end- diastolic velocity (EDV) were measured in the internal carotid (ICA) and common carotid (continued on next page) From the Departments of Surgery and *Radiology, St. Joseph Mercy Hospital, Ann Arbor; and School of Public Health, _tDepartment of Epidemiology, University of Michigan, Ann Arbor, Michigan. Supported by research funds, St. Joseph Mercy Hospital. Presented at the Ninth Annual Winter Meeting of the Peripheral Vascular Surgery Society, Snowbird, Utah, January 1999. t)1999 Westminster Publications, Inc., 708 Glen Cove Avenue, Glen Head, NY 11545, U.S.A. 497
Transcript of Duplex Ultrasonography to Predict Internal Carotid by NASCET: The

Vascular Surgery
VOLUME 33 SEPTEMBER/OCTOBER 1999 NUMBER 5
Duplex Ultrasonography to Predict Internal CarotidArtery Stenoses Exceeding 50% and 70% as Defined
by NASCET: The Need for Multiple Criteria
Edward D. Kreske, MDSeth W. Wolk, MD
Charles J. Shanley, MDRichard M. Lampman, PhD
James E. Knake, MD*Leslie A. Lange, MS"
Errol E. Erlandson, MDand Walter M. Whitehouse, Jr, MD
ANN ARBOR, MICHIGAN
Carotid duplex scanning is being used more frequently as the sole preoperative diag-nostic imaging modality for patients considered candidates for carotid endarterectomy.The North American Symptomatic Carotid Endarterectomy Trial (NASCET) has demon-strated the benefit of surgical treatment in patients with carotid stenoses exceeding 70%.The purpose of this study was to determine duplex criteria that accurately predict carotidstenoses exceeding 50% and 70% as defined by NASCET arteriographic criteria. Onehundred forty-one patients (264 carotid arteries) considered surgical candidates wereprospectively studied over a 2-year period by use of both duplex scanning and digitalsubtraction cerebral arteriography. Carotid artery stenosis was determined by a singleradiologist using NASCET arteriographic criteria. Peak systolic velocity (PSV) and end-diastolic velocity (EDV) were measured in the internal carotid (ICA) and common carotid
(continued on next page)
From the Departments of Surgery and *Radiology, St. Joseph Mercy Hospital, Ann Arbor; and Schoolof Public Health, _tDepartment of Epidemiology, University of Michigan, Ann Arbor, Michigan.Supported by research funds, St. Joseph Mercy Hospital.Presented at the Ninth Annual Winter Meeting of the Peripheral Vascular Surgery Society, Snowbird,Utah, January 1999.t)1999 Westminster Publications, Inc., 708 Glen Cove Avenue, Glen Head, NY 11545, U.S.A.
497

Vascular Surgery September/October 1999
(Abstract continued)(CCA) arteries by use of duplex scanning. ICA/CCA velocity ratios were calculated forPSV and EDV. Sensitivity, specificity, positive and negative predictive values, andaccuracy were calculated. PSVICA/CCA provided the highest sensitivity, and EDVICA thehighest specificity in this study. Arteriographic stenoses exceeding 50% and 70% werereliably predicted with use of these duplex criteria. It is concluded that duplex criteria canpredict carotid stenoses exceeding 50% and 70% as defined by NASCET arteriographiccriteria. These criteria should be independently validated by other vascular laboratories.
Introduction
The collaborators of the North American Symp-tomatic Carotid Endarterectomy Trial (NASCET)recently published results of a randomized multi-center clinical trial of carotid endarterectomy inpatients with symptomatic moderate carotidstenoses of 50-69%.1 A small, but statistically sig-nificant, benefit was found for endarterectomy inthis group when compared to medical therapy.Also, durable benefits were noted in surgicallytreated patients with stenoses exceeding 70% at 8years' follow-up.
Duplex scanning is the most commonly usednoninvasive diagnostic imaging modality for eval-uation of carotid artery stenosis. Additionally, du-plex scanning is being used more frequently asthe sole preoperative diagnostic imaging modali-ty before carotid endarterectomy. Commonlyused traditional duplex criteria, developed bycomparison studies with arteriography, report thecarotid bifurcation as normal, 1-15% stenosis,16-49% stenosis, 50-79% stenosis, 80-99%stenosis, and occluded.2 These categories are notappropriate for the evaluation of stenoses ex-ceeding 50% and 70%.
Recent North American randomized multi-center trials evaluating carotid endarterectomyinclude, in addition to NASCET, the Asymptom-atic Carotid Atherosclerosis Study (ACAS) andthe Veterans Affairs (VA) Cooperative Trial.1'3'4These trials measured carotid stenosis by usingan arteriographic method comparing the point ofmaximal stenosis with the distal disease-free in-ternal carotid artery. This arteriographic methoddiffers from those used to establish traditionalduplex criteria. The arteriographic techniquesused to establish traditional duplex criteria donot provide results equivalent to the methods
used in the randomized trials.5 The purpose ofthis study was to prospectively develop duplexcriteria to reliably predict carotid stenoses ex-ceeding 50% and 70% as defined by the arterio-graphic method used in NASCET.
Methods
Between March 1996 and June 1998, 141 pa-tients (264 carotid arteries) were prospectivelystudied with both duplex scanning and carotid ar-teriography within 30 days of each other. Most ofthese patients were being evaluated for possiblesurgical treatment of carotid disease, and thisgroup represents all patients who had technicallyadequate examinations during the study interval.All duplex studies and carotid arteriographieswere performed at St. Joseph Mercy Hospital,Ann Arbor, Michigan.
Digital subtraction percutaneous catheter ar-teriograms with a 1,024 x 1,024 matrix were ob-tained in all patients. At least two views of eachcarotid bifurcation, as well as intracranial views,were obtained. The arteriographic stenosis wasdetermined by a single radiologist using NASCETcriteria.5'6 The radiologist was masked to the re-sults of corresponding duplex examinations.
Duplex scanning was performed with anAcuson 128XP10 Duplex Scanner (MountainView, CA) with a 5-MHz linear array transducer.Peak systolic velocity (PSV) and end-diastolic ve-locity (EDV) measurements were taken in the dis-tal common carotid artery (CCA) and the inter-nal carotid artery (ICA). All examinations wereperformed by one of four vascular laboratorytechnologists using an identical protocol in a lab-
498
Kreske Duplex Criteria to Predict Carotid Stenoses > 50%, 70%o
oratory accredited by the Intersocietal Commis-sion for the Accreditation of Vascular Laborato-ries. In some cases, duplex examination followedarteriography. No attempt was made to mask thetechnologists to the results of carotid arteriogra-phy when it preceded duplex examination.
Maximum PSV and EDV measurements at thecarotid bifurcation (PSVICA and EDVICA) werecompared with the maximum diameter reductionarteriographic stenosis. Additionally, ICA/CCAvelocity ratios were calculated for PSV and EDV,respectively (PSVICA/CCA and EDVICA/CCA). Theseratios were also compared with the maximum di-ameter reduction arteriographic stenosis. Sensi-tivity (SENS), specificity (SPEC), positive predic-tive value (PPV), negative predictive value(NPV) and accuracy (ACCUR) were calculatedfor each criterion (PSVICA, EDVICA, PSVICA/CCAand EDVICA/cCA) at two levels of arteriographicstenosis: 50% or greater and 70% or greater.
Results
Arteriographic occlusion was present in 15 (5%)of the 282 carotid arteries available for compar-ison. Occluded vessels were excluded from analy-sis while contralateral vessels were included.Also, three patients had only one artery studied
with duplex scanning, thus leaving 264 carotidarteries available for analysis. Stenosis greaterthan or equal to 50% was present in 134 (51%)arteries. Stenosis greater than or equal to 70%was present in 78 (30%) arteries. Sensitivity,specificity, positive predictive value, negativepredictive value and accuracy have been plottedfor the measured values of EDVICA and PSVICA,and also for the calculated ratios EDVICA/CCA andPSVICA/CCAA
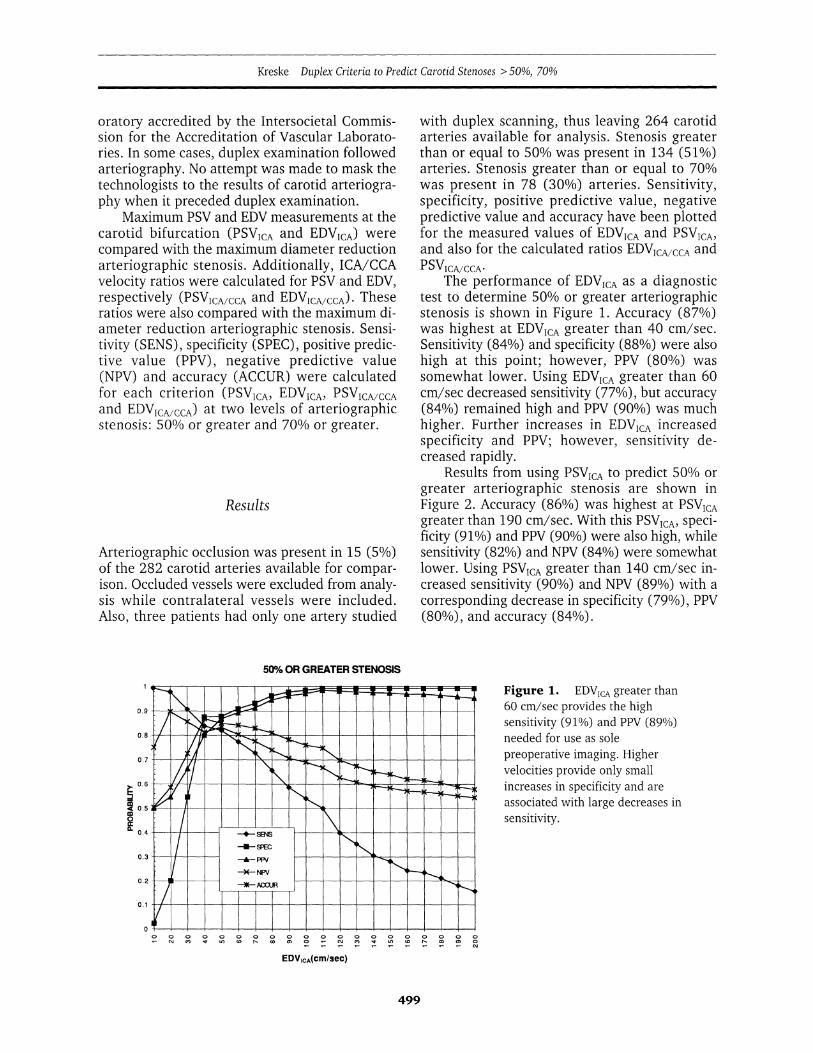
The performance of EDVICA as a diagnostictest to determine 50% or greater arteriographicstenosis is shown in Figure 1. Accuracy (87%)was highest at EDVICA greater than 40 cm/sec.Sensitivity (84%) and specificity (88%) were alsohigh at this point; however, PPV (80%) wassomewhat lower. Using EDVICA greater than 60cm/sec decreased sensitivity (77%), but accuracy(84%) remained high and PPV (90%) was muchhigher. Further increases in EDVICA increasedspecificity and PPV; however, sensitivity de-creased rapidly.
Results from using PSVICA to predict 50% orgreater arteriographic stenosis are shown inFigure 2. Accuracy (86%) was highest at PSVICAgreater than 190 cm/sec. With this PSVICA, speci-ficity (91%) and PPV (90%) were also high, whilesensitivity (82%) and NPV (84%) were somewhatlower. Using PSVICA greater than 140 cm/sec in-creased sensitivity (90%) and NPV (89%) with acorresponding decrease in specificity (79%), PPV(80%), and accuracy (84%).
50% OR GREATER STENOSIS
0.9
0.8
0.7
Q 0.6
0.5
0.4
0.3
0.2
0.1
Figure 1. EDVICA greater than60 cm/sec provides the highsensitivity (91%) and PPV (89%)needed for use as solepreoperative imaging. Highervelocities provide only smallincreases in specificity and areassociated with large decreases insensitivity.
CM Xl) 1-t U)n CD r- co 0DICV COm/U )(
EDVICA(Cm/sec)
499
0 0 0 0- co 0) 0
cli
Vascular Surgery September/October 1999
50%h OR GREATER STENOSIS
0.9
0.8 I
0.6
0.5
0.4 SENS
0o o 0o 0 0 0 0 0 0 0 0 0 0 0 0o N t a) ax 0 Nq C CD O CQ CO C0 0
m CY N N 0) )co )co co
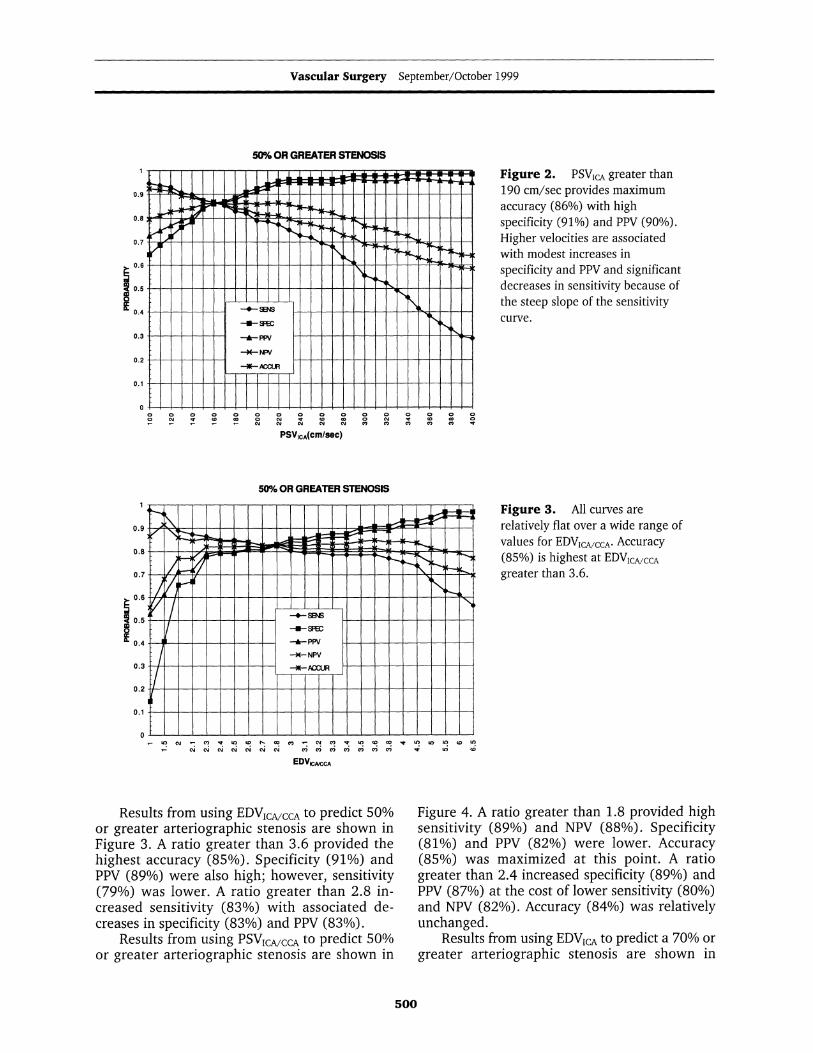
Figure 2. PSVICA greater than190 cm/sec provides maximumaccuracy (86%) with highspecificity (91%) and PPV (90%).Higher velocities are associatedwith modest increases inspecificity and PPV and significantdecreases in sensitivity because ofthe steep slope of the sensitivitycurve.
PSVICA(cm/sec)
50°h OR GREATER STENOSIS
Figure 3. All curves arerelatively flat over a wide range ofvalues for EDVICAMCCA. Accuracy(85%) is highest at EDVIcAcCAgreater than 3.6.
U) N '- 0 7 U) to 1- cm - N 0)M U) CD CDW U7 U) I) CD 1)N N NI N N1CNCNC 0)0C6 ) 0 rCO U) CD
EDVCAtCCA
Results from using EDVICA/ccA to predict 50%or greater arteriographic stenosis are shown inFigure 3. A ratio greater than 3.6 provided thehighest accuracy (85%). Specificity (91%) andPPV (89%) were also high; however, sensitivity(79%) was lower. A ratio greater than 2.8 in-creased sensitivity (83%) with associated de-creases in specificity (83%) and PPV (83%).
Results from using PSVICA/CCA to predict 50%or greater arteriographic stenosis are shown in
Figure 4. A ratio greater than 1.8 provided highsensitivity (89%) and NPV (88%). Specificity(81%) and PPV (82%) were lower. Accuracy(85%) was maximized at this point. A ratiogreater than 2.4 increased specificity (89%) andPPV (87%) at the cost of lower sensitivity (80%)and NPV (82%). Accuracy (84%) was relativelyunchanged.
Results from using EDVICA to predict a 70% orgreater arteriographic stenosis are shown in
500
Kreske Duplex Criteria to Predict Carotid Stenoses > 50%, 70%
50% OR GREATER STENOSIS
- '" ~ C N ll U 1-: C~ N - N~ ll ~ C 1 C~ U
PSVKAMCCA
70% OR GREATER STENOSIS
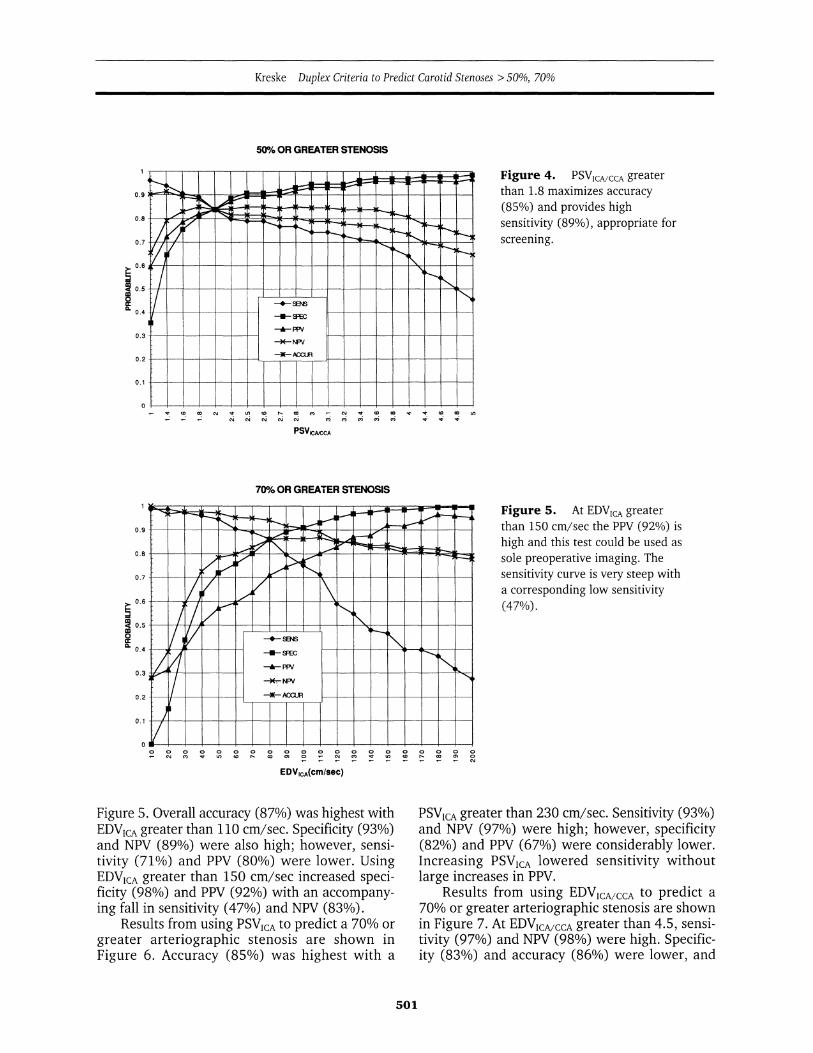
Figure 4. PSVICA/CCA greater
than 1.8 maximizes accuracy(85%) and provides highsensitivity (89%), appropriate forscreening.
Figure 5. At EDVICA greaterthan 150 cm/sec the PPV (92%) ishigh and this test could be used assole preoperative imaging. Thesensitivity curve is very steep witha corresponding low sensitivity(47%).
EDVICA(cm/sec)
Figure 5. Overall accuracy (87%) was highest withEDVICA greater than 110 cm/sec. Specificity (93%)and NPV (89%) were also high; however, sensi-tivity (71%) and PPV (80%) were lower. UsingEDVICA greater than 150 cm/sec increased speci-ficity (98%) and PPV (92%) with an accompany-ing fall in sensitivity (47%) and NPV (83%).
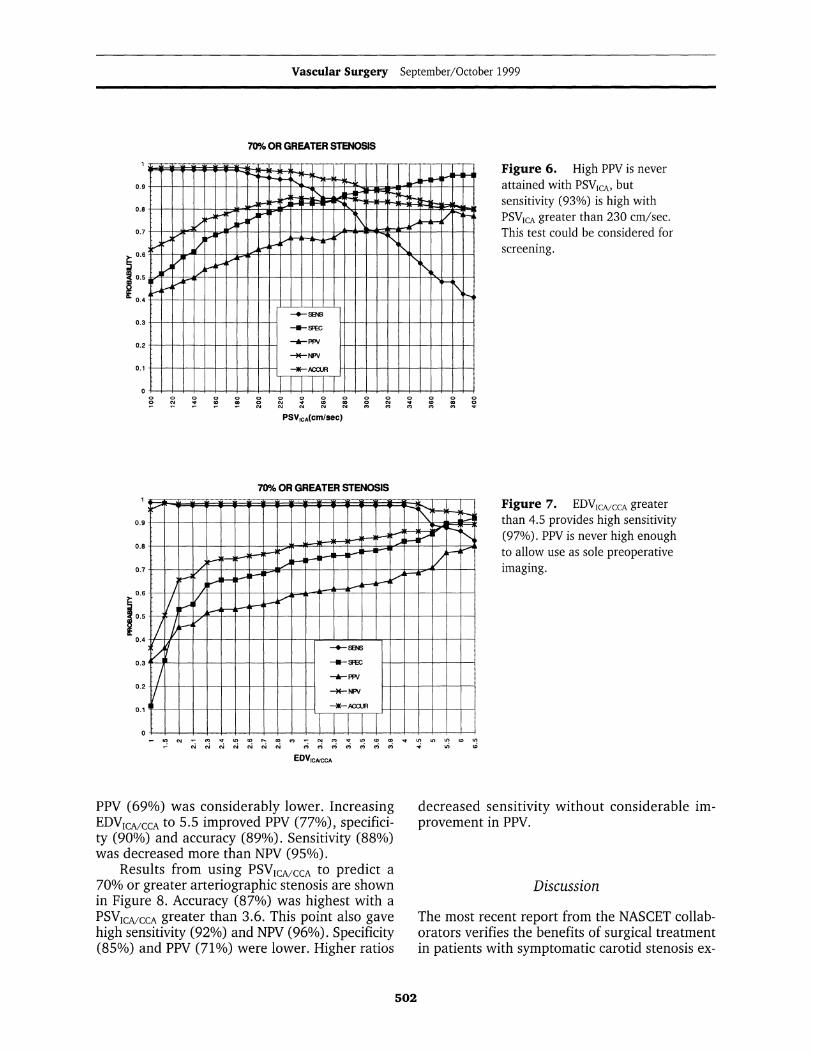
Results from using PSVICA to predict a 70% orgreater arteriographic stenosis are shown inFigure 6. Accuracy (85%) was highest with a
PSVICA greater than 230 cm/sec. Sensitivity (93%)and NPV (97%) were high; however, specificity(82%) and PPV (67%) were considerably lower.Increasing PSVICA lowered sensitivity withoutlarge increases in PPV.
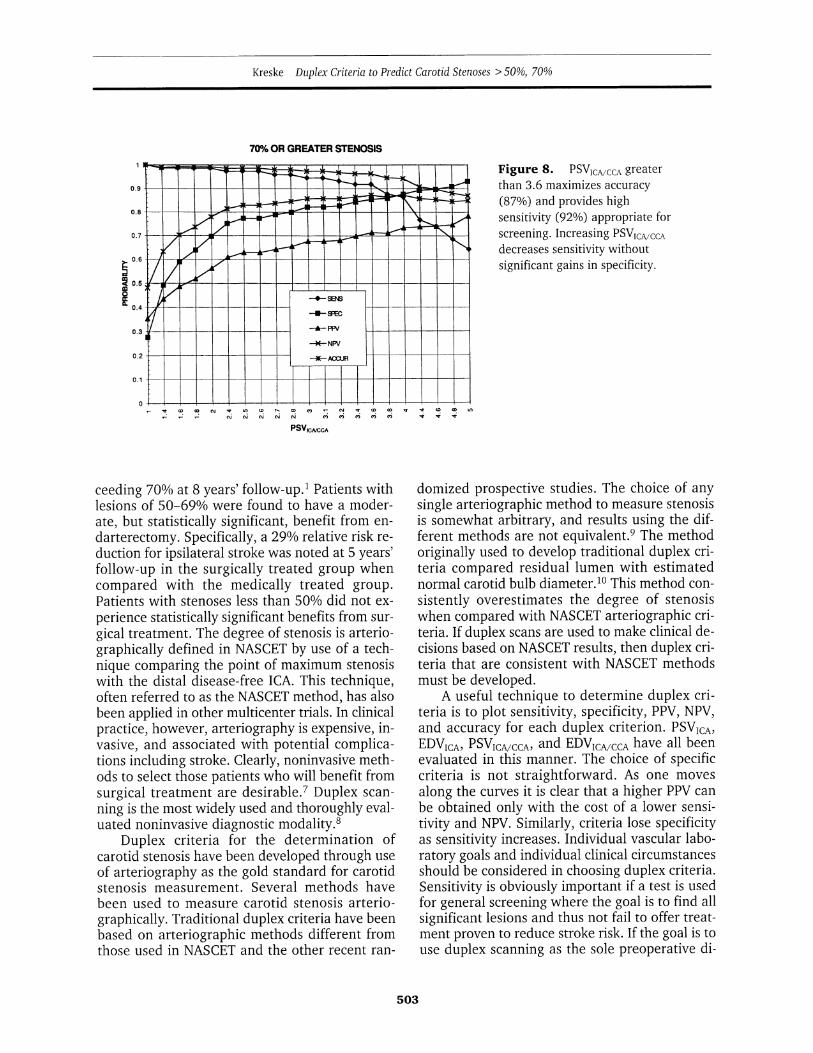
Results from using EDVICA/cCA to predict a
70% or greater arteriographic stenosis are shownin Figure 7. At EDVIcA/cCA greater than 4.5, sensi-tivity (97%) and NPV (98%) were high. Specific-ity (83%) and accuracy (86%) were lower, and
501
0.9
0.8
0.7
0.6
0.50
U.04
0.3
0.2
0.1
Vascular Surgery September/October 1999
Figure 6. High PPV is never-* attained with PSVICA, but
sensitivity (93%) is high withI PSVICA greater than 230 cm/sec.A1 This test could be considered for
screening.
_-_
0 o o cCY 1- co ccCli cl CM o\
PSVICA(Cm/sec)
70% OR GREATER STENOSIS
_ N e 0 t0- CM N U E 0
- C CN N NsN<C\ ( X X
EDVICA/CCA
PPV (69%) was considerably lower. IncreasingEDVICA/CCA to 5.5 improved PPV (77%), specifici-ty (90%) and accuracy (89%). Sensitivity (88%)was decreased more than NPV (95%).
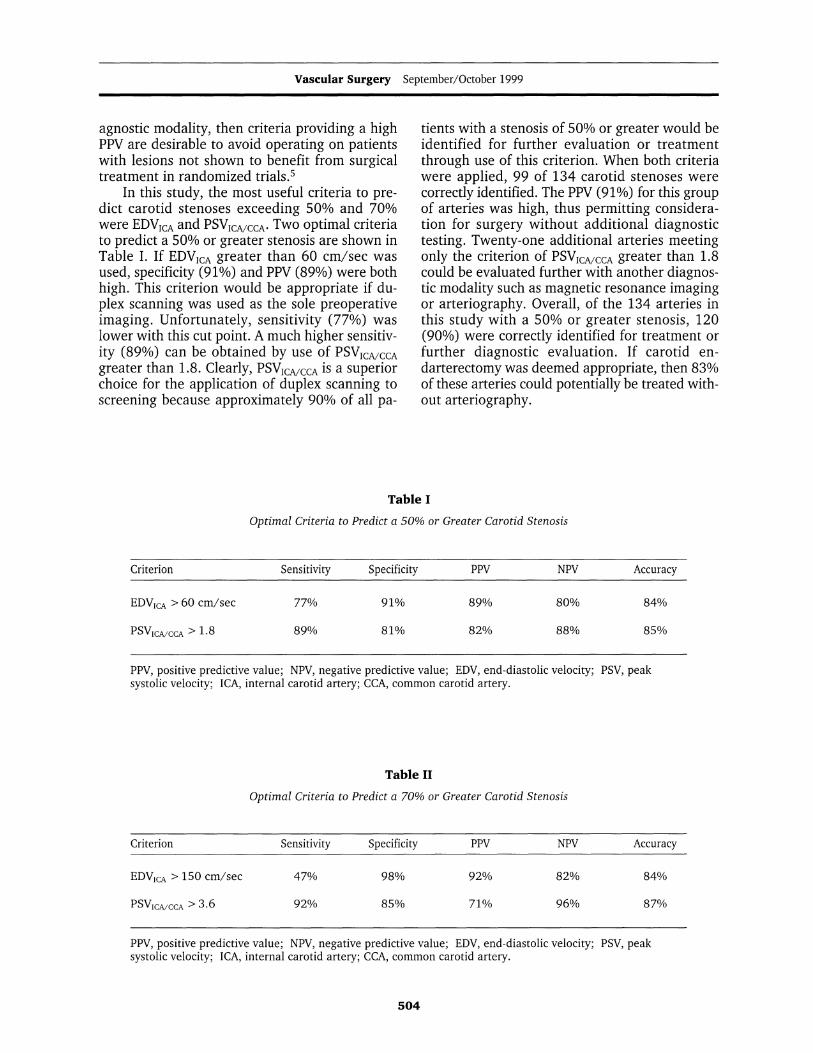
Results from using PSVICA/CCA to predict a
70% or greater arteriographic stenosis are shownin Figure 8. Accuracy (87%) was highest with a
PSVICA/CCA greater than 3.6. This point also gavehigh sensitivity (92%) and NPV (96%). Specificity(85%) and PPV (71%) were lower. Higher ratios
........Figure 7. EDVICVCCA greater
54e < than 4.5 provides high sensitivity(97%). PPV is never high enoughto allow use as sole preoperative
e -i imaging.
decreased sensitivity without considerable im-provement in PPV.
Discussion
The most recent report from the NASCET collab-orators verifies the benefits of surgical treatmentin patients with symptomatic carotid stenosis ex-
502
70% OR GREATER STENOSIS
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0
0.5
IL
-,
D 0 0 0 0
r
0 0 0 0 0 00 cli v co co 0
V CO el) CO CO CO
Kreske Duplex Criteria to Predict Carotid Stenoses > 50%, 70%
70% OR GREATER STENOSIS
Figure 8. PSVICA/CCA greaterthan 3.6 maximizes accuracy(87%) and provides highsensitivity (92%) appropriate forscreening. Increasing PSVICA/CCAdecreases sensitivity withoutsignificant gains in specificity.
3V cACAPSVr-AICCA
ceeding 70% at 8 years' follow-up.' Patients withlesions of 50-69% were found to have a moder-ate, but statistically significant, benefit from en-darterectomy. Specifically, a 29% relative risk re-duction for ipsilateral stroke was noted at 5 years'follow-up in the surgically treated group whencompared with the medically treated group.Patients with stenoses less than 50% did not ex-perience statistically significant benefits from sur-gical treatment. The degree of stenosis is arterio-graphically defined in NASCET by use of a tech-nique comparing the point of maximum stenosiswith the distal disease-free ICA. This technique,often referred to as the NASCET method, has alsobeen applied in other multicenter trials. In clinicalpractice, however, arteriography is expensive, in-vasive, and associated with potential complica-tions including stroke. Clearly, noninvasive meth-ods to select those patients who will benefit fromsurgical treatment are desirable.7 Duplex scan-ning is the most widely used and thoroughly eval-uated noninvasive diagnostic modality.8
Duplex criteria for the determination ofcarotid stenosis have been developed through useof arteriography as the gold standard for carotidstenosis measurement. Several methods havebeen used to measure carotid stenosis arterio-graphically. Traditional duplex criteria have beenbased on arteriographic methods different fromthose used in NASCET and the other recent ran-
domized prospective studies. The choice of anysingle arteriographic method to measure stenosisis somewhat arbitrary, and results using the dif-ferent methods are not equivalent.9 The methodoriginally used to develop traditional duplex cri-teria compared residual lumen with estimatednormal carotid bulb diameter.10 This method con-sistently overestimates the degree of stenosiswhen compared with NASCET arteriographic cri-teria. If duplex scans are used to make clinical de-cisions based on NASCET results, then duplex cri-teria that are consistent with NASCET methodsmust be developed.
A useful technique to determine duplex cri-teria is to plot sensitivity, specificity, PPV, NPV,and accuracy for each duplex criterion. PSVICA,EDVICA, PSVICA/CCA, and EDVcAcCCA have all beenevaluated in this manner. The choice of specificcriteria is not straightforward. As one movesalong the curves it is clear that a higher PPV canbe obtained only with the cost of a lower sensi-tivity and NPV. Similarly, criteria lose specificityas sensitivity increases. Individual vascular labo-ratory goals and individual clinical circumstancesshould be considered in choosing duplex criteria.Sensitivity is obviously important if a test is usedfor general screening where the goal is to find allsignificant lesions and thus not fail to offer treat-ment proven to reduce stroke risk. If the goal is touse duplex scanning as the sole preoperative di-
503
Vascular Surgery September/October 1999
agnostic modality, then criteria providing a highPPV are desirable to avoid operating on patientswith lesions not shown to benefit from surgicaltreatment in randomized trials.5
In this study, the most useful criteria to pre-dict carotid stenoses exceeding 50% and 70%were EDVICA and PSVICA/CCA. Two optimal criteriato predict a 50% or greater stenosis are shown inTable I. If EDVICA greater than 60 cm/sec wasused, specificity (91%) and PPV (89%) were bothhigh. This criterion would be appropriate if du-plex scanning was used as the sole preoperativeimaging. Unfortunately, sensitivity (77%) waslower with this cut point. A much higher sensitiv-ity (89%) can be obtained by use of PSVICA/CCAgreater than 1.8. Clearly, PSVICA/CCA is a superiorchoice for the application of duplex scanning toscreening because approximately 90% of all pa-
tients with a stenosis of 50% or greater would beidentified for further evaluation or treatmentthrough use of this criterion. When both criteriawere applied, 99 of 134 carotid stenoses werecorrectly identified. The PPV (91%) for this groupof arteries was high, thus permitting considera-tion for surgery without additional diagnostictesting. Twenty-one additional arteries meetingonly the criterion of PSVICA/CCA greater than 1.8could be evaluated further with another diagnos-tic modality such as magnetic resonance imagingor arteriography. Overall, of the 134 arteries inthis study with a 50% or greater stenosis, 120(90%) were correctly identified for treatment orfurther diagnostic evaluation. If carotid en-darterectomy was deemed appropriate, then 83%of these arteries could potentially be treated with-out arteriography.
Table I
Optimal Criteria to Predict a 50% or Greater Carotid Stenosis
Criterion Sensitivity Specificity PPV NPV Accuracy
EDVICA > 60 cm/sec 77% 91% 89% 80% 84%
PSVICA/CCA > 1.8 89% 81% 82% 88% 85%
PPV, positive predictive value; NPV, negative predictive value; EDV, end-diastolic velocity; PSV, peaksystolic velocity; ICA, internal carotid artery; CCA, common carotid artery.
Table II
Optimal Criteria to Predict a 70% or Greater Carotid Stenosis
Criterion Sensitivity Specificity PPV NPV Accuracy
EDVICA > 150 cm/sec 47% 98% 92% 82% 84%
PSVICA/CCA > 3.6 92% 85% 71% 96% 87%
PPV, positive predictive value; NPV, negative predictive value; EDV, end-diastolic velocity; PSV, peaksystolic velocity; ICA, internal carotid artery; CCA, common carotid artery.
504

Kreske Duplex Criteria to Predict Carotid Stenoses > 50%, 70%
Similarly, Table II shows two optimal crite-ria to predict a 70% or greater stenosis. Again,EDVICA proved to be most useful as a potentialsole preoperative imaging criterion. When EDVICAwas greater than 150 cm/sec, the PPV (92%) washigh, resulting in a low false-positive rate. Spec-ificity (98%) and accuracy (84%) were also highat this cut point; however, sensitivity (47%) wasmuch lower. Unfortunately, the slope of the sen-sitivity curve is steep (Figure 5), resulting in theexclusion of about half of the diseased arteries ifa cut point is chosen to provide a PPV exceeding90%. Exactly what constitutes an appropriatePPV for sole preoperative imaging is not entirelyclear. Investigators in the Asymptomatic CarotidAtherosclerosis Study used a PPV of 95% forentry into the trial with a duplex scan.3 This PPVcorresponds to a false-positive rate of 5%. Theimportance of a high PPV as an entry criterionfor a clinical trial is clear; however, the choice ofan appropriate PPV for clinical application tosymptomatic and asymptomatic patients with dif-ferent levels of disease severity is not as straight-forward. Individual surgeons will likely have todecide what false-positive rate is acceptable forduplex scanning in the context of sole preopera-tive imaging and then choose cut points with anappropriate PPV. This type of clinical decisionmaking requires prior validation of vascular lab-oratory criteria.
Screening for high-grade lesions was moresuccessful in using PSVICA/CCA* Using PSVICA/CCAgreater than 3.6 provided high sensitivity (92%),although the PPV (71%) was considerably lower.Seventy-one of 77 stenoses greater than or equalto 70% were detected by use of this cut point.This performance is clearly more appropriate fora screening criterion. Note that the accuracy(877%) of this test was fairly high, with the broadapplication of this criterion primarily limited byits low PPV. In this study both carotid arteries ina single patient were considered as independentevents, although the influence of a contralateralocclusion on duplex measurements is well docu-mented.11,12 At the completion of patient enroll-ment the number of arteries with stenoses ex-ceeding 70% was lower than originally estimat-ed. This circumstance impacted PPV results sig-nificantly because false-positive results, mostlydue to contralateral occlusions, were more influ-ential in the reduced sample size. The original in-tent of the study was to develop and validate cri-teria encompassing the situation of an occluded
contralateral artery, occasionally encountered inall busy vascular laboratories. To accomplish thisobjective, arteries contralateral to occlusions withfalsely elevated duplex measurements were keptin the study.
Comparing this study with those of other au-thors demonstrates similar results. Moneta et al10proposed the use of PSVICA/CCA greater than 4.0 topredict stenoses exceeding 70%. A sensitivity of91%, specificity of 87%, and accuracy of 88%were reported.10 Neale et al1' reported the com-bination of PSV greater than 270 cm/sec and EDVgreater than 110 cm/sec to be 96% sensitive and91% specific, with an accuracy of 93%. Resultsfrom both prior studies are similar to those vali-dated in our study (Figures 5, 6, 8). We are notaware of any comparable studies that evaluatethe prediction of stenoses exceeding 50% in asimilar prospective manner.
The attractiveness of a single criterion, suchas EDVICA or PSVICA/CCA, to be used for both solepreoperative imaging and screening is obvious.However, an understanding of biologic dataanalysis, specifically the often inverse relationshipbetween sensitivity and positive predictive value,can spare vascular laboratories from the fre-quently futile task of forcing a single criterion tofunction effectively for all clinical purposes. Thisstudy supports the use of separate criteria forcarotid duplex imaging, depending on the in-tended use of the study. The use of multiple cri-teria is both desirable and necessary if individualvascular laboratories seek to maximize the valid-ity of carotid duplex imaging for the dual appli-cations presently utilized.
Duplex scanning can reliably predict carotidstenoses exceeding 50% and 70% as defined byNASCET arteriographic methods. In this studythe potential use of duplex scanning for sole pre-operative imaging was best accomplished withuse of EDVICA. Alternatively, PSVICA/CCA was thebetter criterion for application as a broad screen-ing test. Results from this study are similar tothose reported by other authors; however, thesesimilarities do not obviate the process of indi-vidual vascular laboratory validation.10"13,14 Sub-stantial variation between individual vascularlaboratories and equipment has been reportedin the literature.15'16 Although the use of regis-tered vascular technologists and accreditation oflaboratories by the Intersocietal Commission forthe Accreditation of Vascular Laboratories islikely to be helpful in managing the problems of
505

Vascular Surgery September/October 1999
variation, these measures are not substitutes forthe process of validation. The importance of thisprocess is emphasized by the NASCET collabo-rators, who recommend validation of noninva-sive studies at individual centers before arteri-ography is discarded.1
Seth W. Wolk, MDMichigan Heart and Vascular InstituteSuite #104P.O. Box 974Ann Arbor, MI 48106
References
1. Barnett HJM, Taylor DW, Eliasziw M, et al: Benefit ofcarotid endarterectomy in patients with symptomaticmoderate or severe stenosis. N Engl J Med 339:1415-1425, 1998.
2. Roederer GO, Langlois YE, Chan ATW, et al: Ultra-sonic duplex scanning of the extracranial carotid ar-teries: Improved accuracy using new features fromthe common carotid artery. J Cardiovasc Ultrasonog-raphy 1:373-380, 1982.
3. Executive Committee for the Asymptomatic CarotidAtherosclerosis study. Endarterectomy for asympto-matic carotid artery stenosis. JAMA 273:1421-1428,1995.
4. Veterans Administrative Cooperative Trialists. Roleof carotid endarterectomy in asymptomatic carotidstenosis. A Veterans Administration CooperativeStudy. Stroke 17:534-539, 1986.
5. Carpenter JP, Lexa FJ, Davis JT: Determination ofsixty percent or greater carotid artery stenosis by du-plex Doppler ultrasonography. J Vasc Surg 22:697-705, 1995.
6. Gagne PJ, Matchett J, MacFarland D, et al: Can theNASCET technique for measuring carotid stenosis bereliably applied outside the trial? J Vasc Surg 24:449-456, 1996.
7. Hankey GJ, Warlow CP, Sellar RJ: Cerebral angio-graphic risk in mild cerebrovascular disease. Stroke21:209-222, 1990.
8. Elmore JR, Franklin DP, Thomas DD, et al: Carotidendarterectomy: The mandate for high-quality du-plex. Ann Vasc Surg 12:156- 162, 1998.
9. Fox AJ: How to measure carotid stenosis. Radiology186:316-318, 1993.
10. Moneta GL, Edwards JM, Chitwood RW, et al:Correlation of North American Symptomatic CarotidEndarterectomy Trial (NASCET) angiographic defin-ition of 70-99% internal carotid artery stenosis withduplex scanning. J Vasc Surg 17:152-159, 1993.
11. van Everdingen KJ, van der Grond J, Kappelle LJ:Overestimation of a stenosis in the internal carotidartery by duplex sonography caused by an increase involume flow. J Vasc Surg 27:479-485, 1998.
12. Busuttil SJ, Franklin DP, Youkey JR, et al: Carotidduplex overestimation of stenosis due to severe con-tralateral disease. Am J Surg 172:144-148, 1996.
13. Neale ML, Chambers JL, Kelly AT, et al: Reappraisalof duplex criteria to assess significant carotid steno-sis with special reference to reports from the NorthAmerican Symptomatic Carotid Endarterectomy Trialand the European Carotid Surgery Trial. J Vasc Surg20:642-649, 1994.
14. Chen JC, Salvian AJ, Taylor DC, et al: Predictive abil-ity of duplex ultrasonography for internal carotidartery stenosis of 70%-99%: A comparative study.Ann Vasc Surg 12:244-247, 1998.
15. Fillinger MF, Baker RJ Jr, Zwolak RM, et al: Carotidduplex criteria for a 60% or greater angiographicstenosis: Variation according to equipment. J VascSurg 24:856-864, 1996.
16. Kuntz KM, Polak JF, Whittenmore AD, et al: Duplexultrasound criteria for the identification of carotidstenosis should be laboratory specific. Stroke 28:597-602, 1997.
506