Drug delivery across BBB
14
Aman Kumar Naik Integrated M.Sc. Drug Delivery across the Blood–Brain Barrier(BBB)
-
Upload
aman-kumar-naik -
Category
Science
-
view
299 -
download
0
Transcript of Drug delivery across BBB

9/11/2015 :: National Institute of Science Education and Research ::
http://biology.niser.ac.in/ 1/1
:: quick links ::
Webmail
Holiday list
Phone book
photo gallery
Home • School of Biological Sciences
Welcome to the Schoo l o f B io log i ca l Sc iences
Vision
The School of Biological Sciences aims to establish itself as a leading international centre for research andteaching with harmonious synthesis of classical and modern biology always promoting scholarship, originalthinking, innovative ideas and cutting edge research.
Mission
To strive to become a centre of excellence in education and research in biological sciences providing trainingat undergraduate, graduate, doctoral and postdoctoral level.To provide effective interdisciplinary learning ambience through extensive subject coverage in all fields ofmodern biology and interphasing with other scientific disciplines.To equip its students to keep pace with recent developments in the field of scientific research.To undertake high quality research activities in defined areas of biosciences so as to make an impact atnational and international level.To impart professional training for skilled human resource development across the state and country throughshort term training courses.To strive to develop state of the art infrastructure comparable to best anywhere in the world.
IOP DAE Indian Railways Indian Airlines
NISER Home
Home
Programmes
Courses
Research
Facilities
People
Aman Kumar Naik Integrated M.Sc.
Drug Delivery across the Blood–Brain Barrier(BBB)

(junctional adhesion molecule-1, occludin, and claudins) with cy-toplasmic accessory proteins (zonula occludens-1 and -2, cingulin,AF-6, and 7H6). They are linked to the actin cytoskeleton [9],thereby forming the most intimate cell to cell connection. The TJare further strengthened and maintained by the interaction orcommunication of astrocytes and pericytes with brain endotheliacells [10];
3) the expression of various transporters including GLUT1 glucosecarrier, amino acid carrier LAT1, transferring receptors, insulin re-ceptors, lipoprotein receptors and ATP family of efflux trans-porters such as p-glycoprotein (P-gp) and multidrug resistance-related proteins MRPs [3,11]. Some of these aid the transportinto the brain while others prevent the entry of many molecules;
4) the synergistic inductive functions and upregulating of BBB featuresby astrocytes, astrocytic perivascular endfeet, pericytes, perivascularmacrophages and neurons, as suggested by the strong evidencefrom cell culture studies [12–14];
5) the lack of lymphatic drainage, and absence of major histocompat-ibility complex (MHC) antigens in CNS with immune reactivity in-ducible on temporary demand in order to provide maximumprotection to neuronal function [15]. The BBB has a strict limitfor the passage of immune cells, especially lymphocytes [16] andits immune barrier is made by the association between BBB endo-thelia cells and perivascular macrophages and mast cells [17]. Ad-ditionally, this immune barrier is reinforced by local microglialcells [18].
All these characteristics lead to BBB to possess multiple functionsas a physical barrier (TJ), a transport barrier (P-gp), a metabolic or en-zymatic barrier (specialised enzyme systems [11,19] and an immuno-logical barrier.
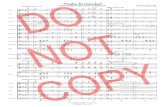
3. Transport routes across the blood–brain barrier
It has been well established that there are several transport routesby which solute molecules move across the BBB [11,20]. Diffusion ofsubstances into the brain can be divided into paracellular and trans-cellular. As illustrated in Fig. 2.a, small water-soluble molecules sim-ply diffuse through the TJ but not to any great extent. Small lipidsoluble substances like alcohol and steroid hormones penetrate trans-cellularly by dissolving in their lipid plasma membrane (Fig. 2.b).
However, for almost all other substances, including essential mate-rials such as glucose and amino acids, transport proteins (carriers),specific receptor-mediated or vesicular mechanisms (adsorptivetranscytosis) are required to pass the BBB.
In the case of transport proteins or known as carrier-mediatedtransport (Fig. 2.c), there is binding of a solute such as glucose oramino acids to a protein transporter on one side of the membranethat triggers a conformational change in the protein, resulting in thetransport of the substance to the other side of the membrane, fromhigh to low concentration. If compounds need to be moved againsta concentration gradient, ATP may provide the energy to facilitatethe process. Efflux pumps or transporters (Fig. 2.d) are responsiblefor extruding drugs from the brain and this mechanism is a major ob-stacle for the accumulation of a wide range of biologically active mol-ecules in the brain, with the ATP binding cassette (ABC) transporterP-gp and multidrug resistant protein (MRP) being the principle effluxmechanism of these agents [21]. Inhibition of P-gp in pre-clinicalstudies has enhanced the penetration of paclitaxel into the brain, in-dicating the feasibility of achieving improved drug delivery to thebrain by suppression of P-gp [22].
Receptor-mediated transcytosis (RMT) (Fig. 2.e) provides a meansfor selective uptake of macromolecules. Endothelial cells have recep-tors for the uptake of many different types of ligands, includinggrowth factors, enzymes and plasma proteins. For example, insulinmolecules first bind to receptors that collect in specialized areas ofthe plasma membrane known as coated pits. When bound to ligandthese pits invaginate into the cytoplasm and then pinch free of theplasma membrane to form coated vesicles. After acidification of theendosome, the ligand will dissociate from the receptor and cross theother side of membrane. RMT has been extensively studied for braintargeting [23]. Those well-characterised systems include transferringreceptor (TfR), insulin receptor, lipoprotein receptors, scavenger re-ceptors class B type I, diphtheria toxin receptor and glutathione trans-porter [3].
Adsorptive-mediated transcytosis (AMT), also known as the pino-cytosis route (Fig. 2.f), is triggered by an electrostatic interaction be-tween a positively charged substance, usually the charged moiety ofa peptide, and the negatively charged plasma membrane surface(i.e. heparin sulphate proteoglycans). Adsorptive-mediated transporthas a lower affinity but higher capacity than RMT. The developmentof many new drug delivery technologies focuses on AMT [24]. AMT-
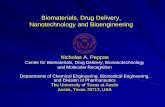
Fig. 1. Schematic representation of the blood–brain barrier (BBB) and other components of a neurovascular unit (NVU).Reproduced with permission from reference [11].
642 Y. Chen, L. Liu / Advanced Drug Delivery Reviews 64 (2012) 640–665
Schematic representation of the blood–brain barrier (BBB)
© 2006 Nature Publishing Group
*Wolfson Centre for Age-Related Diseases, King’s College London, UK. ‡Institute of Clinical Neuroscience, The Sahlgrenska Academy at Göteborg University, Göteborg, Sweden. Correspondence to N.J.A. e-mail: [email protected]:10.1038/nrn1824
Neurovascular unitA functional unit composed of groups of neurons and their associated astrocytes, interacting with smooth muscle cells and endothelial cells on the microvessels (arterioles) responsible for their blood supply, and capable of regulating the local blood flow.
Gliovascular unitA proposed functional unit composed of single astrocytic glial cells and the neurons they surround, interacting with local segments of blood vessels, and capable of regulating blood flow at the arteriolar level and BBB functions at the capillary level.
Astrocyte–endothelial interactionsat the blood–brain barrierN. Joan Abbott*, Lars Rönnbäck‡ and Elisabeth Hansson‡
Abstract | The blood–brain barrier, which is formed by the endothelial cells that line cerebral microvessels, has an important role in maintaining a precisely regulated microenvironment for reliable neuronal signalling. At present, there is great interest in the association of brain microvessels, astrocytes and neurons to form functional ‘neurovascular units’, and recent studies have highlighted the importance of brain endothelial cells in this modular organization. Here, we explore specific interactions between the brain endothelium, astrocytes and neurons that may regulate blood–brain barrier function. An understanding of how these interactions are disturbed in pathological conditions could lead to the development of new protective and restorative therapies.
Neuroscience has traditionally focused on the neurons of the central and peripheral nervous systems, and, increasingly, on their interactions with the glial cells that support their function. It is now becoming clear that neurons, glia and microvessels are organized into well-structured neurovascular units, which are involved in the regulation of cerebral blood flow1. Within this organization, further modular structure can be detected; in particular, the proposed gliovascular units, in which individual astrocytic glia support the function of particular neuronal populations and territories, and communicate with associated segments of the micro-vasculature2,3. Several recent studies have highlighted the importance of the brain endothelial cells that form the blood–brain barrier (BBB) in this modular organization, and the physiology and pharmacology of the signalling between glia and endothelium that is involved in regulating the BBB. Here, we describe the properties of the brain endothelium that contribute to its barrier function, and how cell–cell interactions lead to induction of the specialized features of the BBB and associated cell types. We review work showing that the BBB is a dynamic system, and discuss the ways in which BBB permeability and transport can be modulated. We then consider the important role of astrocytes and the BBB in brain ion and volume regulation. Finally, we discuss some of the pathologies that involve BBB dys-function, and the development of protective strategies for the brain endothelium that may reduce secondary neural damage in both acute and chronic neurological conditions.
Barriers of the CNSThe cerebral ventricles and subarachnoid space contain cerebrospinal fluid (CSF), which is secreted by choroid plexuses in the lateral, third and fourth ventricles4. Three barrier layers limit and regulate molecular exchange at the interfaces between the blood and the neural tissue or its fluid spaces (FIG. 1): the BBB formed by the cerebro vascular endothelial cells between blood and brain interstitial fluid (ISF), the choroid plexus epithelium between blood and ventricular CSF, and the arachnoid epithelium between blood and subarachnoid CSF5. Individual neu-rons are rarely more than 8–20 µm from a brain capillary6, although they may be millimetres or centimetres from a CSF compartment. Hence, of the various CNS barriers, the BBB exerts the greatest control over the immediate microenvironment of brain cells.
The blood–brain barrierThe BBB is a selective barrier formed by the endothelial cells that line cerebral microvessels7–10 (FIG. 2). It acts as a ‘physical barrier’ because complex tight junctions between adjacent endothelial cells force most molecular traffic to take a transcellular route across the BBB, rather than moving paracellularly through the junctions, as in most endothelia11,12 (FIG. 3). Small gaseous molecules such as O2 and CO2 can diffuse freely through the lipid membranes, and this is also a route of entry for small lipophilic agents, including drugs such as barbiturates and ethanol. The presence of specific transport systems on the luminal and abluminal membranes regulates the transcellular traffic of small hydrophilic molecules, which provides
R E V I E W S
NATURE REVIEWS | NEUROSCIENCE VOLUME 7 | JANUARY 2006 | 41
© 2006 Nature Publishing Group
*Wolfson Centre for Age-Related Diseases, King’s College London, UK. ‡Institute of Clinical Neuroscience, The Sahlgrenska Academy at Göteborg University, Göteborg, Sweden. Correspondence to N.J.A. e-mail: [email protected]:10.1038/nrn1824
Neurovascular unitA functional unit composed of groups of neurons and their associated astrocytes, interacting with smooth muscle cells and endothelial cells on the microvessels (arterioles) responsible for their blood supply, and capable of regulating the local blood flow.
Gliovascular unitA proposed functional unit composed of single astrocytic glial cells and the neurons they surround, interacting with local segments of blood vessels, and capable of regulating blood flow at the arteriolar level and BBB functions at the capillary level.
Astrocyte–endothelial interactionsat the blood–brain barrierN. Joan Abbott*, Lars Rönnbäck‡ and Elisabeth Hansson‡
Abstract | The blood–brain barrier, which is formed by the endothelial cells that line cerebral microvessels, has an important role in maintaining a precisely regulated microenvironment for reliable neuronal signalling. At present, there is great interest in the association of brain microvessels, astrocytes and neurons to form functional ‘neurovascular units’, and recent studies have highlighted the importance of brain endothelial cells in this modular organization. Here, we explore specific interactions between the brain endothelium, astrocytes and neurons that may regulate blood–brain barrier function. An understanding of how these interactions are disturbed in pathological conditions could lead to the development of new protective and restorative therapies.
Neuroscience has traditionally focused on the neurons of the central and peripheral nervous systems, and, increasingly, on their interactions with the glial cells that support their function. It is now becoming clear that neurons, glia and microvessels are organized into well-structured neurovascular units, which are involved in the regulation of cerebral blood flow1. Within this organization, further modular structure can be detected; in particular, the proposed gliovascular units, in which individual astrocytic glia support the function of particular neuronal populations and territories, and communicate with associated segments of the micro-vasculature2,3. Several recent studies have highlighted the importance of the brain endothelial cells that form the blood–brain barrier (BBB) in this modular organization, and the physiology and pharmacology of the signalling between glia and endothelium that is involved in regulating the BBB. Here, we describe the properties of the brain endothelium that contribute to its barrier function, and how cell–cell interactions lead to induction of the specialized features of the BBB and associated cell types. We review work showing that the BBB is a dynamic system, and discuss the ways in which BBB permeability and transport can be modulated. We then consider the important role of astrocytes and the BBB in brain ion and volume regulation. Finally, we discuss some of the pathologies that involve BBB dys-function, and the development of protective strategies for the brain endothelium that may reduce secondary neural damage in both acute and chronic neurological conditions.
Barriers of the CNSThe cerebral ventricles and subarachnoid space contain cerebrospinal fluid (CSF), which is secreted by choroid plexuses in the lateral, third and fourth ventricles4. Three barrier layers limit and regulate molecular exchange at the interfaces between the blood and the neural tissue or its fluid spaces (FIG. 1): the BBB formed by the cerebro vascular endothelial cells between blood and brain interstitial fluid (ISF), the choroid plexus epithelium between blood and ventricular CSF, and the arachnoid epithelium between blood and subarachnoid CSF5. Individual neu-rons are rarely more than 8–20 µm from a brain capillary6, although they may be millimetres or centimetres from a CSF compartment. Hence, of the various CNS barriers, the BBB exerts the greatest control over the immediate microenvironment of brain cells.
The blood–brain barrierThe BBB is a selective barrier formed by the endothelial cells that line cerebral microvessels7–10 (FIG. 2). It acts as a ‘physical barrier’ because complex tight junctions between adjacent endothelial cells force most molecular traffic to take a transcellular route across the BBB, rather than moving paracellularly through the junctions, as in most endothelia11,12 (FIG. 3). Small gaseous molecules such as O2 and CO2 can diffuse freely through the lipid membranes, and this is also a route of entry for small lipophilic agents, including drugs such as barbiturates and ethanol. The presence of specific transport systems on the luminal and abluminal membranes regulates the transcellular traffic of small hydrophilic molecules, which provides
R E V I E W S
NATURE REVIEWS | NEUROSCIENCE VOLUME 7 | JANUARY 2006 | 41
© 2006 Nature Publishing Group
*Wolfson Centre for Age-Related Diseases, King’s College London, UK. ‡Institute of Clinical Neuroscience, The Sahlgrenska Academy at Göteborg University, Göteborg, Sweden. Correspondence to N.J.A. e-mail: [email protected]:10.1038/nrn1824
Neurovascular unitA functional unit composed of groups of neurons and their associated astrocytes, interacting with smooth muscle cells and endothelial cells on the microvessels (arterioles) responsible for their blood supply, and capable of regulating the local blood flow.
Gliovascular unitA proposed functional unit composed of single astrocytic glial cells and the neurons they surround, interacting with local segments of blood vessels, and capable of regulating blood flow at the arteriolar level and BBB functions at the capillary level.
Astrocyte–endothelial interactionsat the blood–brain barrierN. Joan Abbott*, Lars Rönnbäck‡ and Elisabeth Hansson‡
Abstract | The blood–brain barrier, which is formed by the endothelial cells that line cerebral microvessels, has an important role in maintaining a precisely regulated microenvironment for reliable neuronal signalling. At present, there is great interest in the association of brain microvessels, astrocytes and neurons to form functional ‘neurovascular units’, and recent studies have highlighted the importance of brain endothelial cells in this modular organization. Here, we explore specific interactions between the brain endothelium, astrocytes and neurons that may regulate blood–brain barrier function. An understanding of how these interactions are disturbed in pathological conditions could lead to the development of new protective and restorative therapies.
Neuroscience has traditionally focused on the neurons of the central and peripheral nervous systems, and, increasingly, on their interactions with the glial cells that support their function. It is now becoming clear that neurons, glia and microvessels are organized into well-structured neurovascular units, which are involved in the regulation of cerebral blood flow1. Within this organization, further modular structure can be detected; in particular, the proposed gliovascular units, in which individual astrocytic glia support the function of particular neuronal populations and territories, and communicate with associated segments of the micro-vasculature2,3. Several recent studies have highlighted the importance of the brain endothelial cells that form the blood–brain barrier (BBB) in this modular organization, and the physiology and pharmacology of the signalling between glia and endothelium that is involved in regulating the BBB. Here, we describe the properties of the brain endothelium that contribute to its barrier function, and how cell–cell interactions lead to induction of the specialized features of the BBB and associated cell types. We review work showing that the BBB is a dynamic system, and discuss the ways in which BBB permeability and transport can be modulated. We then consider the important role of astrocytes and the BBB in brain ion and volume regulation. Finally, we discuss some of the pathologies that involve BBB dys-function, and the development of protective strategies for the brain endothelium that may reduce secondary neural damage in both acute and chronic neurological conditions.
Barriers of the CNSThe cerebral ventricles and subarachnoid space contain cerebrospinal fluid (CSF), which is secreted by choroid plexuses in the lateral, third and fourth ventricles4. Three barrier layers limit and regulate molecular exchange at the interfaces between the blood and the neural tissue or its fluid spaces (FIG. 1): the BBB formed by the cerebro vascular endothelial cells between blood and brain interstitial fluid (ISF), the choroid plexus epithelium between blood and ventricular CSF, and the arachnoid epithelium between blood and subarachnoid CSF5. Individual neu-rons are rarely more than 8–20 µm from a brain capillary6, although they may be millimetres or centimetres from a CSF compartment. Hence, of the various CNS barriers, the BBB exerts the greatest control over the immediate microenvironment of brain cells.
The blood–brain barrierThe BBB is a selective barrier formed by the endothelial cells that line cerebral microvessels7–10 (FIG. 2). It acts as a ‘physical barrier’ because complex tight junctions between adjacent endothelial cells force most molecular traffic to take a transcellular route across the BBB, rather than moving paracellularly through the junctions, as in most endothelia11,12 (FIG. 3). Small gaseous molecules such as O2 and CO2 can diffuse freely through the lipid membranes, and this is also a route of entry for small lipophilic agents, including drugs such as barbiturates and ethanol. The presence of specific transport systems on the luminal and abluminal membranes regulates the transcellular traffic of small hydrophilic molecules, which provides
R E V I E W S
NATURE REVIEWS | NEUROSCIENCE VOLUME 7 | JANUARY 2006 | 41
© 2006 Nature Publishing Group
*Wolfson Centre for Age-Related Diseases, King’s College London, UK. ‡Institute of Clinical Neuroscience, The Sahlgrenska Academy at Göteborg University, Göteborg, Sweden. Correspondence to N.J.A. e-mail: [email protected]:10.1038/nrn1824
Neurovascular unitA functional unit composed of groups of neurons and their associated astrocytes, interacting with smooth muscle cells and endothelial cells on the microvessels (arterioles) responsible for their blood supply, and capable of regulating the local blood flow.
Gliovascular unitA proposed functional unit composed of single astrocytic glial cells and the neurons they surround, interacting with local segments of blood vessels, and capable of regulating blood flow at the arteriolar level and BBB functions at the capillary level.
Astrocyte–endothelial interactionsat the blood–brain barrierN. Joan Abbott*, Lars Rönnbäck‡ and Elisabeth Hansson‡
Abstract | The blood–brain barrier, which is formed by the endothelial cells that line cerebral microvessels, has an important role in maintaining a precisely regulated microenvironment for reliable neuronal signalling. At present, there is great interest in the association of brain microvessels, astrocytes and neurons to form functional ‘neurovascular units’, and recent studies have highlighted the importance of brain endothelial cells in this modular organization. Here, we explore specific interactions between the brain endothelium, astrocytes and neurons that may regulate blood–brain barrier function. An understanding of how these interactions are disturbed in pathological conditions could lead to the development of new protective and restorative therapies.
Neuroscience has traditionally focused on the neurons of the central and peripheral nervous systems, and, increasingly, on their interactions with the glial cells that support their function. It is now becoming clear that neurons, glia and microvessels are organized into well-structured neurovascular units, which are involved in the regulation of cerebral blood flow1. Within this organization, further modular structure can be detected; in particular, the proposed gliovascular units, in which individual astrocytic glia support the function of particular neuronal populations and territories, and communicate with associated segments of the micro-vasculature2,3. Several recent studies have highlighted the importance of the brain endothelial cells that form the blood–brain barrier (BBB) in this modular organization, and the physiology and pharmacology of the signalling between glia and endothelium that is involved in regulating the BBB. Here, we describe the properties of the brain endothelium that contribute to its barrier function, and how cell–cell interactions lead to induction of the specialized features of the BBB and associated cell types. We review work showing that the BBB is a dynamic system, and discuss the ways in which BBB permeability and transport can be modulated. We then consider the important role of astrocytes and the BBB in brain ion and volume regulation. Finally, we discuss some of the pathologies that involve BBB dys-function, and the development of protective strategies for the brain endothelium that may reduce secondary neural damage in both acute and chronic neurological conditions.
Barriers of the CNSThe cerebral ventricles and subarachnoid space contain cerebrospinal fluid (CSF), which is secreted by choroid plexuses in the lateral, third and fourth ventricles4. Three barrier layers limit and regulate molecular exchange at the interfaces between the blood and the neural tissue or its fluid spaces (FIG. 1): the BBB formed by the cerebro vascular endothelial cells between blood and brain interstitial fluid (ISF), the choroid plexus epithelium between blood and ventricular CSF, and the arachnoid epithelium between blood and subarachnoid CSF5. Individual neu-rons are rarely more than 8–20 µm from a brain capillary6, although they may be millimetres or centimetres from a CSF compartment. Hence, of the various CNS barriers, the BBB exerts the greatest control over the immediate microenvironment of brain cells.
The blood–brain barrierThe BBB is a selective barrier formed by the endothelial cells that line cerebral microvessels7–10 (FIG. 2). It acts as a ‘physical barrier’ because complex tight junctions between adjacent endothelial cells force most molecular traffic to take a transcellular route across the BBB, rather than moving paracellularly through the junctions, as in most endothelia11,12 (FIG. 3). Small gaseous molecules such as O2 and CO2 can diffuse freely through the lipid membranes, and this is also a route of entry for small lipophilic agents, including drugs such as barbiturates and ethanol. The presence of specific transport systems on the luminal and abluminal membranes regulates the transcellular traffic of small hydrophilic molecules, which provides
R E V I E W S
NATURE REVIEWS | NEUROSCIENCE VOLUME 7 | JANUARY 2006 | 41
© 2006 Nature Publishing Group
*Wolfson Centre for Age-Related Diseases, King’s College London, UK. ‡Institute of Clinical Neuroscience, The Sahlgrenska Academy at Göteborg University, Göteborg, Sweden. Correspondence to N.J.A. e-mail: [email protected]:10.1038/nrn1824
Neurovascular unitA functional unit composed of groups of neurons and their associated astrocytes, interacting with smooth muscle cells and endothelial cells on the microvessels (arterioles) responsible for their blood supply, and capable of regulating the local blood flow.
Gliovascular unitA proposed functional unit composed of single astrocytic glial cells and the neurons they surround, interacting with local segments of blood vessels, and capable of regulating blood flow at the arteriolar level and BBB functions at the capillary level.
Astrocyte–endothelial interactionsat the blood–brain barrierN. Joan Abbott*, Lars Rönnbäck‡ and Elisabeth Hansson‡
Abstract | The blood–brain barrier, which is formed by the endothelial cells that line cerebral microvessels, has an important role in maintaining a precisely regulated microenvironment for reliable neuronal signalling. At present, there is great interest in the association of brain microvessels, astrocytes and neurons to form functional ‘neurovascular units’, and recent studies have highlighted the importance of brain endothelial cells in this modular organization. Here, we explore specific interactions between the brain endothelium, astrocytes and neurons that may regulate blood–brain barrier function. An understanding of how these interactions are disturbed in pathological conditions could lead to the development of new protective and restorative therapies.
Neuroscience has traditionally focused on the neurons of the central and peripheral nervous systems, and, increasingly, on their interactions with the glial cells that support their function. It is now becoming clear that neurons, glia and microvessels are organized into well-structured neurovascular units, which are involved in the regulation of cerebral blood flow1. Within this organization, further modular structure can be detected; in particular, the proposed gliovascular units, in which individual astrocytic glia support the function of particular neuronal populations and territories, and communicate with associated segments of the micro-vasculature2,3. Several recent studies have highlighted the importance of the brain endothelial cells that form the blood–brain barrier (BBB) in this modular organization, and the physiology and pharmacology of the signalling between glia and endothelium that is involved in regulating the BBB. Here, we describe the properties of the brain endothelium that contribute to its barrier function, and how cell–cell interactions lead to induction of the specialized features of the BBB and associated cell types. We review work showing that the BBB is a dynamic system, and discuss the ways in which BBB permeability and transport can be modulated. We then consider the important role of astrocytes and the BBB in brain ion and volume regulation. Finally, we discuss some of the pathologies that involve BBB dys-function, and the development of protective strategies for the brain endothelium that may reduce secondary neural damage in both acute and chronic neurological conditions.
Barriers of the CNSThe cerebral ventricles and subarachnoid space contain cerebrospinal fluid (CSF), which is secreted by choroid plexuses in the lateral, third and fourth ventricles4. Three barrier layers limit and regulate molecular exchange at the interfaces between the blood and the neural tissue or its fluid spaces (FIG. 1): the BBB formed by the cerebro vascular endothelial cells between blood and brain interstitial fluid (ISF), the choroid plexus epithelium between blood and ventricular CSF, and the arachnoid epithelium between blood and subarachnoid CSF5. Individual neu-rons are rarely more than 8–20 µm from a brain capillary6, although they may be millimetres or centimetres from a CSF compartment. Hence, of the various CNS barriers, the BBB exerts the greatest control over the immediate microenvironment of brain cells.
The blood–brain barrierThe BBB is a selective barrier formed by the endothelial cells that line cerebral microvessels7–10 (FIG. 2). It acts as a ‘physical barrier’ because complex tight junctions between adjacent endothelial cells force most molecular traffic to take a transcellular route across the BBB, rather than moving paracellularly through the junctions, as in most endothelia11,12 (FIG. 3). Small gaseous molecules such as O2 and CO2 can diffuse freely through the lipid membranes, and this is also a route of entry for small lipophilic agents, including drugs such as barbiturates and ethanol. The presence of specific transport systems on the luminal and abluminal membranes regulates the transcellular traffic of small hydrophilic molecules, which provides
R E V I E W S
NATURE REVIEWS | NEUROSCIENCE VOLUME 7 | JANUARY 2006 | 41

based drug delivery typically involves either cationic proteins or cell-penetrating peptide such as Tat-derived peptides and Syn-B vectors.
Last, but not least, cell-mediated transcytosis (Fig. 2.g) is a morerecently identified route of drug transport across the BBB [25], al-though it is a well established mechanism for some pathogens suchas Cryptococcus neoformans and HIV entry into the brain, known as “Trojan horse” model [26,27]. This transport route relies on immunecells such as monocytes or macrophages to cross the intact BBB. Un-like aforementioned transport pathways which normally permitonly solute molecules with specific properties, cell-mediated transcy-tosis is unique in that it can be used virtually for any type of mole-cules or materials as well as particulate carrier systems [28].
Due to the unique properties of the TJs, paracellular transport ofhydrophilic drugs is virtually absent and transcellular transport bypassive diffusion is only available to molecules which fulfil certain cri-teria [4,29,30] such as: 1) molecular weight is less than 500 Da;2) compounds are unionised; 3) log P value of the drug is close to2; 4) cumulative number of hydrogen bonds is not more than 10. Un-fortunately only a small percentage of drugs fit these criteria [2]. Forother therapeutic molecules, their transport across the BBB willthen have to rely on either the integrity of the BBB or the drug ordrug carrier properties and their interaction with or affinity for recep-tors expressed at the BBB, as well as other biological or immunologi-cal processes occurring at the BBB. In other words, the BBB propertiesand related biological processes, and their roles in trafficking varioustypes of molecules are fundamental to the success of drug transportacross the BBB. This is the reason for the need to gain a thorough un-derstanding of the biological and pathological properties and process-es of the BBB.
4. Biological and pathological properties of BBB for drug transport
Recent progress in the study of the molecular biology of the BBBhas led to a greater understanding of the barrier functions under nor-mal physiological and pathological conditions, as well as when theBBB is subjected to external stimuli. More importantly, this knowl-edge empowers researchers to develop new strategies for therapeuticmolecules to target and transport across the BBB for treatment of
various CNS associated diseases. This section is focused on the physi-cal barrier and properties of the BBB undergoing pathological changeswhich may present potential opportunities for drug transport.
4.1. Physical barrier
The physical barrier of the BBB is a result of the formation of anelaborated junctional complex by TJ and adherens junctions (AJ) be-tween adjacent endothelial cells [31].
4.1.1. Tight junctionsTJ are located on the apical region of endothelia cells and structur-
ally formed by an intricate complex network made of a series of par-allel, interconnected, transmembrane and cytoplasmatic strands ofproteins [32,31]. The high level of integrity of TJ is reflected by thehigh electrical resistance of the BBB (1500–2000 Ω cm2), which de-pends on a proper extracellular Ca2+ ion concentration. There are ex-tensive reviews on the TJ elsewhere [31–33]. Here the focus of thisreview is placed on some key molecules involved in the formationand maintenance of TJ and the regulation of the permeability of TJ.
Among the identified molecules associated with TJ, the transmem-brane proteins claudins and occludin are most well studied. Claudinsform dimmers and bind homotypically to other claudin molecules inan adjacent brain capillary endothelia cell [34,35] thus forming theprimary seal of the TJ [31]. On the other hand, occludin is not essentialfor the formation of TJ, as indicted in the knockout and knockdownexperiments [9] and its main function appears to be for TJ regulationand as an additional support structure [10,36]. Of claudins, Claudin-5has been shown to be involved in size-selective loosening the perme-ability of BBB in mice [37] with permeability of molecules of size lessthan 800 Da affected. However, similar effects were not observedwith barrier function of non-BBB endothelium, such as human umbil-ical vein endothelial cells (HUVEC) [38]. In another experiment, treat-ment of claudin-5 by cyclic AMP (cAMP) lead to enhancement ofclaudin-5 activity along cell borders, rapid reduction in transendothe-lial electrical resistance (TER), and loosening of the claudin-5-basedendothelial barrier against mannitol, but not inulin [39]. These sug-gest that manipulation of claudin-5, or potentially other TJ proteins
Fig. 2. Transport routes across the blood–brain barrier. Pathways “a” to “f” are commonly for solute molecules; and the route “g” involves monocytes, macrophages and other im-mune cells and can be used for any drugs or drugs incorporated liposomes or nanoparticles.Adapted from reference [11].
643Y. Chen, L. Liu / Advanced Drug Delivery Reviews 64 (2012) 640–665Transport routes across the blood–brain barrier
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr

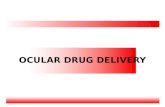
Tight junction opening
Biological stimuli
Zonula occludens toxin (Zot)
vasoactive compounds and inflammatory stimuli such as histamine, bradykinin and VEGF
H2 receptors NO and cyclic GMP production
Tight junction opening
Chemical stimuli
Arterial injection of hyperosmolar solution (e.g., mannitol, arabinose) Shrinkage of endothelial cells Opening gaps between cells
Sodium dodecyl sulphate (SDS)
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr

Physical stimuli
* FUS = Focused Ultrasound
Magnetic resonance monitoring of focusedultrasound/magnetic nanoparticle targeting deliveryof therapeutic agents to the brainHao-Li Liua,b,1, Mu-Yi Huac,1, Hung-Wei Yangc,1, Chiung-Yin Huangd, Po-Chun Chua, Jia-Shin Wua, I-Chou Tsengd,Jiun-Jie Wange, Tzu-Chen Yenb,f, Pin-Yuan Chend,g,2,3, and Kuo-Chen Weid,2,3
Departments of aElectrical Engineering, cChemical and Material Engineering, and eMedical Image and Radiological Sciences and gGraduate Institute of ClinicalMedical Sciences, Chang-Gung University, Taoyuan 333, Taiwan; bMolecular Imaging Center and fDepartment of Nuclear Medicine, Chang-Gung MemorialHospital, Taoyuan 333, Taiwan; and dDepartment of Neurosurgery, Chang-Gung University College of Medicine and Memorial Hospital, Taoyuan 333, Taiwan
Edited by Ralph Weissleider, Harvard Medical School, Boston, MA, and accepted by the Editorial Board July 13, 2010 (received for review March 16, 2010)
The superparamagnetic properties of magnetic nanoparticles(MNPs) allow them to be guided by an externally positionedmagnetand also provide contrast for MRI. However, their therapeutic use intreating CNS pathologies in vivo is limited by insufficient localaccumulation and retention resulting from their inability to traversebiological barriers. The combined use of focused ultrasound andmagnetic targeting synergistically delivers therapeutic MNPs acrossthe blood–brain barrier to enter the brain both passively and ac-tively. Therapeutic MNPs were characterized and evaluated bothin vitro and in vivo, andMRI was used tomonitor and quantify theirdistribution in vivo. The technique could be used in normal brains orin those with tumors, and significantly increased the deposition oftherapeutic MNPs in brains with intact or compromised blood–brainbarriers. Synergistic targeting and image monitoring are powerfultechniques for the delivery of macromolecular chemotherapeuticagents into the CNS under the guidance of MRI.
blood–brain barrier | brain drug delivery | focused ultrasound | magneticnanoparticles | magnetic targeting
Within the CNS, the blood–brain barrier (BBB) excludeslarger (>400 Da) molecules from entering the brain pa-
renchyma, protecting it from toxic foreign substances (1). How-ever, it also prohibits delivery of many potentially effectivediagnostic or therapeutic agents and restricts the enhanced per-meability and retention (EPR) of therapeutic nanoparticles.Many factors affect EPR, including the pH, polarity, and size ofthe delivered substance. Even when pathologic processes com-promise the integrity or function of the BBB, EPR can be limitedby microenvironmental characteristics such as hypovascularity,fibrosis, or necrosis (2–4).In the presence of microbubbles and with use of a low-energy
burst tone, focused ultrasound (FUS) can increase the perme-ability of the BBB (5). This noninvasive procedure disrupts theBBB locally rather than systemically, minimizing off-targeteffects. Furthermore, the disruption is reversible within severalhours, providing a window of opportunity to achieve local deliveryof chemotherapeutic agents in brains with intact or compromisedBBBs. However, drug delivery in such cases is passive, relying onthe free diffusion of the agents across the barrier.Advances innanotechnology andmolecular biologyhaveallowed
development of novel nanomedical platforms (6–8). Suchapproaches allow simultaneous diagnostic imaging and drug de-liverymonitoring in vivo in real time (9, 10).Magnetic nanoparticles(MNPs) have intrinsic magnetic properties that enable their use ascontrast agents in MRI (8, 11). Because MNPs are also sensitive toexternal magnetic forces, magnetic targeting (MT) actively enhan-ces their deposition at the target site, increasing the therapeuticdose delivered beyond that obtainable by passive diffusion (12).This study combines FUS and MT of nanoparticles as a syn-
ergistic delivery system for chemotherapeutic agents concurrentwith MRI monitoring for treating CNS diseases. FUS creates the
opportunity to deliver therapeutic MNPs by passive local EPR,and externally applied magnetic forces actively increase the localMNP concentration. When combined, these techniques permitthe delivery of large molecules into the brain (Fig. 1). Further-more, the deposition of the therapeutic MNPs can be monitoredand quantified in vivo by MRI.
ResultsCharacterization of Therapeutic MNPs. The saturated magnetiza-tion, mean hydrodynamic size, and particle size of the com-mercially available MNP Resovist and the newly synthesizedMNPs generated for this study are summarized in Table S1. Asmeasured by transmission EM (TEM), MNP-3 had a mean di-ameter of 12.3 nm (Fig. 2A). This was significantly smaller thanthe hydrodynamic sizes measured by dynamic light scattering (64nm for Resovist, 74–83 nm for MNPs-1–3; Fig. S1A and TableS1), although such differences could be attributable to solventeffects. The measured zeta potentials of all of the synthesizedMNPs were similar to that of Resovist (approximately 45 mV).Magnetization of MNPs is crucial for their utility in MT, and
crystallinity significantly affects this parameter. During synthesis,the crystallinity of the MNPs was manipulated by controlling thereaction conditions. MNP-3 exhibited the best crystallinity amongthe MNPs tested (Fig. S1C) and also displayed the highest degreeof magnetization (Fig. S1B).Administration of the MNPs into biological tissues profoundly
alters the spin–spin relaxation rate (R2), and thus can serve as anindicator of the MRI contrast agent. The R2, and hence the de-tection sensitivity, of MNP-3 was twice that of Resovist by MRI(Fig. 2 E and F and Table S1).The polymer poly[aniline-co-N-(1-one-butyric acid)] aniline
(SPAnH) was used to encapsulate iron oxide (Fe3O4). This pro-cess decreases the aggregation typical of MNPs and improvestheir stability in aqueous solutions. Fourier transform IR (FT-IR)spectroscopy indicated that the surface of the Fe3O4 particles wascovered with a layer of the SPAnH polymer, and that the out-
Author contributions: H.-L.L., M.-Y.H., H.-W.Y., P.-Y.C., and K.-C.W. designed research;H.-L.L., M.-Y.H., H.-W.Y., C.-Y.H., P.-C.C., J.-S.W., I.-C.T., J.-J.W., T.-C.Y., and P.-Y.C. per-formed research; H.-L.L., M.-Y.H., and H.-W.Y. contributed new reagents/analytic tools;H.-L.L., M.-Y.H., H.-W.Y., C.-Y.H., P.-C.C., J.-S.W., I.-C.T., J.-J.W., T.-C.Y., P.-Y.C., and K.-C.W.analyzed data; and H.-L.L., M.-Y.H., H.-W.Y., and K.-C.W. wrote the paper.
The authors declare no conflict of interest.
This article is a PNAS Direct Submission. R.W. is a guest editor invited by the EditorialBoard.
Freely available online through the PNAS open access option.1H.-L.L., M.-Y.H., and H.-W.Y. contributed equally to this work.2P.-Y.C. and K.-C.W. contributed equally to this work.3To whom correspondence may be addressed. E-mail: [email protected] [email protected].
This article contains supporting information online at www.pnas.org/lookup/suppl/doi:10.1073/pnas.1003388107/-/DCSupplemental.
www.pnas.org/cgi/doi/10.1073/pnas.1003388107 PNAS | August 24, 2010 | vol. 107 | no. 34 | 15205–15210
MED
ICALSC
IENCE
S
Magnetic resonance monitoring of focusedultrasound/magnetic nanoparticle targeting deliveryof therapeutic agents to the brainHao-Li Liua,b,1, Mu-Yi Huac,1, Hung-Wei Yangc,1, Chiung-Yin Huangd, Po-Chun Chua, Jia-Shin Wua, I-Chou Tsengd,Jiun-Jie Wange, Tzu-Chen Yenb,f, Pin-Yuan Chend,g,2,3, and Kuo-Chen Weid,2,3
Departments of aElectrical Engineering, cChemical and Material Engineering, and eMedical Image and Radiological Sciences and gGraduate Institute of ClinicalMedical Sciences, Chang-Gung University, Taoyuan 333, Taiwan; bMolecular Imaging Center and fDepartment of Nuclear Medicine, Chang-Gung MemorialHospital, Taoyuan 333, Taiwan; and dDepartment of Neurosurgery, Chang-Gung University College of Medicine and Memorial Hospital, Taoyuan 333, Taiwan
Edited by Ralph Weissleider, Harvard Medical School, Boston, MA, and accepted by the Editorial Board July 13, 2010 (received for review March 16, 2010)
The superparamagnetic properties of magnetic nanoparticles(MNPs) allow them to be guided by an externally positionedmagnetand also provide contrast for MRI. However, their therapeutic use intreating CNS pathologies in vivo is limited by insufficient localaccumulation and retention resulting from their inability to traversebiological barriers. The combined use of focused ultrasound andmagnetic targeting synergistically delivers therapeutic MNPs acrossthe blood–brain barrier to enter the brain both passively and ac-tively. Therapeutic MNPs were characterized and evaluated bothin vitro and in vivo, andMRI was used tomonitor and quantify theirdistribution in vivo. The technique could be used in normal brains orin those with tumors, and significantly increased the deposition oftherapeutic MNPs in brains with intact or compromised blood–brainbarriers. Synergistic targeting and image monitoring are powerfultechniques for the delivery of macromolecular chemotherapeuticagents into the CNS under the guidance of MRI.
blood–brain barrier | brain drug delivery | focused ultrasound | magneticnanoparticles | magnetic targeting
Within the CNS, the blood–brain barrier (BBB) excludeslarger (>400 Da) molecules from entering the brain pa-
renchyma, protecting it from toxic foreign substances (1). How-ever, it also prohibits delivery of many potentially effectivediagnostic or therapeutic agents and restricts the enhanced per-meability and retention (EPR) of therapeutic nanoparticles.Many factors affect EPR, including the pH, polarity, and size ofthe delivered substance. Even when pathologic processes com-promise the integrity or function of the BBB, EPR can be limitedby microenvironmental characteristics such as hypovascularity,fibrosis, or necrosis (2–4).In the presence of microbubbles and with use of a low-energy
burst tone, focused ultrasound (FUS) can increase the perme-ability of the BBB (5). This noninvasive procedure disrupts theBBB locally rather than systemically, minimizing off-targeteffects. Furthermore, the disruption is reversible within severalhours, providing a window of opportunity to achieve local deliveryof chemotherapeutic agents in brains with intact or compromisedBBBs. However, drug delivery in such cases is passive, relying onthe free diffusion of the agents across the barrier.Advances innanotechnology andmolecular biologyhaveallowed
development of novel nanomedical platforms (6–8). Suchapproaches allow simultaneous diagnostic imaging and drug de-liverymonitoring in vivo in real time (9, 10).Magnetic nanoparticles(MNPs) have intrinsic magnetic properties that enable their use ascontrast agents in MRI (8, 11). Because MNPs are also sensitive toexternal magnetic forces, magnetic targeting (MT) actively enhan-ces their deposition at the target site, increasing the therapeuticdose delivered beyond that obtainable by passive diffusion (12).This study combines FUS and MT of nanoparticles as a syn-
ergistic delivery system for chemotherapeutic agents concurrentwith MRI monitoring for treating CNS diseases. FUS creates the
opportunity to deliver therapeutic MNPs by passive local EPR,and externally applied magnetic forces actively increase the localMNP concentration. When combined, these techniques permitthe delivery of large molecules into the brain (Fig. 1). Further-more, the deposition of the therapeutic MNPs can be monitoredand quantified in vivo by MRI.
ResultsCharacterization of Therapeutic MNPs. The saturated magnetiza-tion, mean hydrodynamic size, and particle size of the com-mercially available MNP Resovist and the newly synthesizedMNPs generated for this study are summarized in Table S1. Asmeasured by transmission EM (TEM), MNP-3 had a mean di-ameter of 12.3 nm (Fig. 2A). This was significantly smaller thanthe hydrodynamic sizes measured by dynamic light scattering (64nm for Resovist, 74–83 nm for MNPs-1–3; Fig. S1A and TableS1), although such differences could be attributable to solventeffects. The measured zeta potentials of all of the synthesizedMNPs were similar to that of Resovist (approximately 45 mV).Magnetization of MNPs is crucial for their utility in MT, and
crystallinity significantly affects this parameter. During synthesis,the crystallinity of the MNPs was manipulated by controlling thereaction conditions. MNP-3 exhibited the best crystallinity amongthe MNPs tested (Fig. S1C) and also displayed the highest degreeof magnetization (Fig. S1B).Administration of the MNPs into biological tissues profoundly
alters the spin–spin relaxation rate (R2), and thus can serve as anindicator of the MRI contrast agent. The R2, and hence the de-tection sensitivity, of MNP-3 was twice that of Resovist by MRI(Fig. 2 E and F and Table S1).The polymer poly[aniline-co-N-(1-one-butyric acid)] aniline
(SPAnH) was used to encapsulate iron oxide (Fe3O4). This pro-cess decreases the aggregation typical of MNPs and improvestheir stability in aqueous solutions. Fourier transform IR (FT-IR)spectroscopy indicated that the surface of the Fe3O4 particles wascovered with a layer of the SPAnH polymer, and that the out-
Author contributions: H.-L.L., M.-Y.H., H.-W.Y., P.-Y.C., and K.-C.W. designed research;H.-L.L., M.-Y.H., H.-W.Y., C.-Y.H., P.-C.C., J.-S.W., I.-C.T., J.-J.W., T.-C.Y., and P.-Y.C. per-formed research; H.-L.L., M.-Y.H., and H.-W.Y. contributed new reagents/analytic tools;H.-L.L., M.-Y.H., H.-W.Y., C.-Y.H., P.-C.C., J.-S.W., I.-C.T., J.-J.W., T.-C.Y., P.-Y.C., and K.-C.W.analyzed data; and H.-L.L., M.-Y.H., H.-W.Y., and K.-C.W. wrote the paper.
The authors declare no conflict of interest.
This article is a PNAS Direct Submission. R.W. is a guest editor invited by the EditorialBoard.
Freely available online through the PNAS open access option.1H.-L.L., M.-Y.H., and H.-W.Y. contributed equally to this work.2P.-Y.C. and K.-C.W. contributed equally to this work.3To whom correspondence may be addressed. E-mail: [email protected] [email protected].
This article contains supporting information online at www.pnas.org/lookup/suppl/doi:10.1073/pnas.1003388107/-/DCSupplemental.
www.pnas.org/cgi/doi/10.1073/pnas.1003388107 PNAS | August 24, 2010 | vol. 107 | no. 34 | 15205–15210
MED
ICALSC
IENCE
S
Magnetic resonance monitoring of focusedultrasound/magnetic nanoparticle targeting deliveryof therapeutic agents to the brainHao-Li Liua,b,1, Mu-Yi Huac,1, Hung-Wei Yangc,1, Chiung-Yin Huangd, Po-Chun Chua, Jia-Shin Wua, I-Chou Tsengd,Jiun-Jie Wange, Tzu-Chen Yenb,f, Pin-Yuan Chend,g,2,3, and Kuo-Chen Weid,2,3
Departments of aElectrical Engineering, cChemical and Material Engineering, and eMedical Image and Radiological Sciences and gGraduate Institute of ClinicalMedical Sciences, Chang-Gung University, Taoyuan 333, Taiwan; bMolecular Imaging Center and fDepartment of Nuclear Medicine, Chang-Gung MemorialHospital, Taoyuan 333, Taiwan; and dDepartment of Neurosurgery, Chang-Gung University College of Medicine and Memorial Hospital, Taoyuan 333, Taiwan
Edited by Ralph Weissleider, Harvard Medical School, Boston, MA, and accepted by the Editorial Board July 13, 2010 (received for review March 16, 2010)
The superparamagnetic properties of magnetic nanoparticles(MNPs) allow them to be guided by an externally positionedmagnetand also provide contrast for MRI. However, their therapeutic use intreating CNS pathologies in vivo is limited by insufficient localaccumulation and retention resulting from their inability to traversebiological barriers. The combined use of focused ultrasound andmagnetic targeting synergistically delivers therapeutic MNPs acrossthe blood–brain barrier to enter the brain both passively and ac-tively. Therapeutic MNPs were characterized and evaluated bothin vitro and in vivo, andMRI was used tomonitor and quantify theirdistribution in vivo. The technique could be used in normal brains orin those with tumors, and significantly increased the deposition oftherapeutic MNPs in brains with intact or compromised blood–brainbarriers. Synergistic targeting and image monitoring are powerfultechniques for the delivery of macromolecular chemotherapeuticagents into the CNS under the guidance of MRI.
blood–brain barrier | brain drug delivery | focused ultrasound | magneticnanoparticles | magnetic targeting
Within the CNS, the blood–brain barrier (BBB) excludeslarger (>400 Da) molecules from entering the brain pa-
renchyma, protecting it from toxic foreign substances (1). How-ever, it also prohibits delivery of many potentially effectivediagnostic or therapeutic agents and restricts the enhanced per-meability and retention (EPR) of therapeutic nanoparticles.Many factors affect EPR, including the pH, polarity, and size ofthe delivered substance. Even when pathologic processes com-promise the integrity or function of the BBB, EPR can be limitedby microenvironmental characteristics such as hypovascularity,fibrosis, or necrosis (2–4).In the presence of microbubbles and with use of a low-energy
burst tone, focused ultrasound (FUS) can increase the perme-ability of the BBB (5). This noninvasive procedure disrupts theBBB locally rather than systemically, minimizing off-targeteffects. Furthermore, the disruption is reversible within severalhours, providing a window of opportunity to achieve local deliveryof chemotherapeutic agents in brains with intact or compromisedBBBs. However, drug delivery in such cases is passive, relying onthe free diffusion of the agents across the barrier.Advances innanotechnology andmolecular biologyhaveallowed
development of novel nanomedical platforms (6–8). Suchapproaches allow simultaneous diagnostic imaging and drug de-liverymonitoring in vivo in real time (9, 10).Magnetic nanoparticles(MNPs) have intrinsic magnetic properties that enable their use ascontrast agents in MRI (8, 11). Because MNPs are also sensitive toexternal magnetic forces, magnetic targeting (MT) actively enhan-ces their deposition at the target site, increasing the therapeuticdose delivered beyond that obtainable by passive diffusion (12).This study combines FUS and MT of nanoparticles as a syn-
ergistic delivery system for chemotherapeutic agents concurrentwith MRI monitoring for treating CNS diseases. FUS creates the
opportunity to deliver therapeutic MNPs by passive local EPR,and externally applied magnetic forces actively increase the localMNP concentration. When combined, these techniques permitthe delivery of large molecules into the brain (Fig. 1). Further-more, the deposition of the therapeutic MNPs can be monitoredand quantified in vivo by MRI.
ResultsCharacterization of Therapeutic MNPs. The saturated magnetiza-tion, mean hydrodynamic size, and particle size of the com-mercially available MNP Resovist and the newly synthesizedMNPs generated for this study are summarized in Table S1. Asmeasured by transmission EM (TEM), MNP-3 had a mean di-ameter of 12.3 nm (Fig. 2A). This was significantly smaller thanthe hydrodynamic sizes measured by dynamic light scattering (64nm for Resovist, 74–83 nm for MNPs-1–3; Fig. S1A and TableS1), although such differences could be attributable to solventeffects. The measured zeta potentials of all of the synthesizedMNPs were similar to that of Resovist (approximately 45 mV).Magnetization of MNPs is crucial for their utility in MT, and
crystallinity significantly affects this parameter. During synthesis,the crystallinity of the MNPs was manipulated by controlling thereaction conditions. MNP-3 exhibited the best crystallinity amongthe MNPs tested (Fig. S1C) and also displayed the highest degreeof magnetization (Fig. S1B).Administration of the MNPs into biological tissues profoundly
alters the spin–spin relaxation rate (R2), and thus can serve as anindicator of the MRI contrast agent. The R2, and hence the de-tection sensitivity, of MNP-3 was twice that of Resovist by MRI(Fig. 2 E and F and Table S1).The polymer poly[aniline-co-N-(1-one-butyric acid)] aniline
(SPAnH) was used to encapsulate iron oxide (Fe3O4). This pro-cess decreases the aggregation typical of MNPs and improvestheir stability in aqueous solutions. Fourier transform IR (FT-IR)spectroscopy indicated that the surface of the Fe3O4 particles wascovered with a layer of the SPAnH polymer, and that the out-
Author contributions: H.-L.L., M.-Y.H., H.-W.Y., P.-Y.C., and K.-C.W. designed research;H.-L.L., M.-Y.H., H.-W.Y., C.-Y.H., P.-C.C., J.-S.W., I.-C.T., J.-J.W., T.-C.Y., and P.-Y.C. per-formed research; H.-L.L., M.-Y.H., and H.-W.Y. contributed new reagents/analytic tools;H.-L.L., M.-Y.H., H.-W.Y., C.-Y.H., P.-C.C., J.-S.W., I.-C.T., J.-J.W., T.-C.Y., P.-Y.C., and K.-C.W.analyzed data; and H.-L.L., M.-Y.H., H.-W.Y., and K.-C.W. wrote the paper.
The authors declare no conflict of interest.
This article is a PNAS Direct Submission. R.W. is a guest editor invited by the EditorialBoard.
Freely available online through the PNAS open access option.1H.-L.L., M.-Y.H., and H.-W.Y. contributed equally to this work.2P.-Y.C. and K.-C.W. contributed equally to this work.3To whom correspondence may be addressed. E-mail: [email protected] [email protected].
This article contains supporting information online at www.pnas.org/lookup/suppl/doi:10.1073/pnas.1003388107/-/DCSupplemental.
www.pnas.org/cgi/doi/10.1073/pnas.1003388107 PNAS | August 24, 2010 | vol. 107 | no. 34 | 15205–15210
MED
ICALSC
IENCE
S
Magnetic
resonancemonitoring
offocused
ultrasound/magnetic
nanoparticletargeting
deliveryof
therapeuticagents
tothe
brainHao-LiLiu
a,b,1,M
u-YiH
uac,1,H
ung-WeiY
angc,1,Chiung-Y
inHuang
d,Po-ChunChu
a,Jia-ShinW
ua,
I-ChouTseng
d,Jiun-Jie
Wang
e,Tzu-ChenYen
b,f,Pin-Y
uanChen
d,g,2,3,and
Kuo-Chen
Wei d
,2,3
Departm
entsof
aElectricalEngineering,cChem
icalandMaterialEngineering,and
eMedicalIm
ageand
RadiologicalSciencesand
gGraduate
Instituteof
ClinicalMedical
Sciences,Chang-G
ungUniversity,Taoyuan
333,Taiwan
;bM
olecularIm
agingCenter
andfD
epartment
ofNuclear
Medicine,
Chang-Gun
gMem
orialHospital,Taoyu
an333,Taiw
an;anddD
epartment
ofNeurosurg
ery,Chang-Gung
University
Collegeof
Medicine
andMem
orialHospital,Taoyu
an333,Taiw
an
Editedby
RalphW
eissleider,H
arvardMedicalScho
ol,Boston,M
A,and
acceptedby
theEditorialBoard
July13,2010
(receivedfor
reviewMarch
16,2010)
Thesuperparam
agneticproperties
ofmagnetic
nanoparticles(M
NPs)allow
themto
beguided
byan
externallypositioned
magnet
andalso
providecontrastforM
RI.How
ever,theirtherapeuticuse
intreating
CNS
pathologiesin
vivois
limited
byinsuffi
cientlocal
accumulation
andretention
resultingfrom
theirinabilityto
traversebiological
barriers.The
combined
useof
focusedultrasound
andmagnetic
targetingsynergistically
deliverstherapeutic
MNPs
acrossthe
blood–brain
barrierto
enterthe
brainboth
passivelyand
ac-tively.
TherapeuticMNPs
were
characterizedand
evaluatedboth
invitro
andin
vivo,andMRIw
asused
tomonitorand
quantifytheir
distributionin
vivo.Thetechnique
couldbe
usedin
normalbrains
orin
thosewith
tumors,and
significantly
increasedthe
depositionof
therapeuticMNPs
inbrains
with
intactorcomprom
isedblood
–brainbarriers.Synergistic
targetingand
image
monitoring
arepow
erfultechniques
forthe
deliveryof
macrom
olecularchem
otherapeuticagents
intothe
CNSunder
theguidance
ofMRI.
blood–brain
barrier|brain
drugdelivery|
focusedultrasound|
magnetic
nanoparticles|magnetic
targeting
Within
theCNS,
theblood
–brainbarrier
(BBB)excludes
larger(>
400Da)
molecules
fromentering
thebrain
pa-renchym
a,protectingitfrom
toxicforeign
substances(1).H
ow-
ever,it
alsoprohibits
deliveryof
many
potentiallyeffective
diagnosticor
therapeuticagents
andrestricts
theenhanced
per-meability
andretention
(EPR
)of
therapeuticnanoparticles.
Many
factorsaffectE
PR,including
thepH
,polarity,andsize
ofthe
deliveredsubstance.
Even
when
pathologicprocesses
com-
promise
theintegrity
orfunctionofthe
BBB,E
PRcan
belim
itedby
microenvironm
entalcharacteristics
suchas
hypovascularity,fibrosis,or
necrosis(2–4).
Inthe
presenceofm
icrobubblesand
with
useofa
low-energy
bursttone,
focusedultrasound
(FUS)
canincrease
theperm
e-ability
ofthe
BBB
(5).This
noninvasiveprocedure
disruptsthe
BBB
locallyrather
thansystem
ically,minim
izingoff-target
effects.Furthermore,the
disruptionis
reversiblewithin
severalhours,providing
awindow
ofopportunitytoachieve
localdeliveryofchem
otherapeuticagentsin
brainswith
intactorcomprom
isedBBBs.H
owever,drug
deliveryin
suchcases
ispassive,relyingon
thefree
diffusionofthe
agentsacross
thebarrier.
Advancesin
nanotechnologyandmolecularbiologyhaveallow
eddevelopm
entof
novelnanom
edicalplatform
s(6–8).
Suchapproaches
allowsim
ultaneousdiagnostic
imaging
anddrug
de-liverym
onitoringinvivo
inrealtim
e(9,10).M
agneticnanoparticles(M
NPs)have
intrinsicmagnetic
propertiesthatenabletheiruse
ascontrastagentsin
MRI(8,11).B
ecauseMNPsare
alsosensitive
toexternalm
agneticforces,m
agnetictargeting
(MT)actively
enhan-ces
theirdeposition
atthe
targetsite,increasing
thetherapeutic
dosedelivered
beyondthatobtainable
bypassive
diffusion(12).
This
studycom
binesFU
Sand
MT
ofnanoparticles
asasyn-
ergisticdelivery
systemfor
chemotherapeutic
agentsconcurrent
with
MRIm
onitoringfortreating
CNSdiseases.FU
Screatesthe
opportunityto
delivertherapeutic
MNPs
bypassive
localEPR
,and
externallyapplied
magnetic
forcesactivelyincrease
thelocal
MNPconcentration.
When
combined,
thesetechniques
permit
thedelivery
oflarge
molecules
intothe
brain(Fig.1).Further-
more,the
depositionofthe
therapeuticMNPs
canbe
monitored
andquantified
invivo
byMRI.
ResultsCharacterization
ofTherapeutic
MNPs.
The
saturatedmagnetiza-
tion,mean
hydrodynamic
size,and
particlesize
ofthe
com-
mercially
availableMNP
Resovist
andthe
newly
synthesizedMNPs
generatedfor
thisstudy
aresum
marized
inTable
S1.As
measured
bytransm
issionEM
(TEM),M
NP-3
hadamean
di-am
eterof
12.3nm
(Fig.2A).T
hiswas
significantlysm
allerthan
thehydrodynam
icsizes
measured
bydynam
iclightscattering
(64nm
forResovist,74
–83nm
forMNPs-1
–3;Fig.S1Aand
Table
S1),although
suchdifferences
couldbe
attributableto
solventeffects.
The
measured
zetapotentials
ofall
ofthe
synthesizedMNPs
were
similar
tothat
ofResovist
(approximately
45mV).
Magnetization
ofMNPs
iscrucialfor
theirutility
inMT,and
crystallinitysignificantly
affectsthis
parameter.D
uringsynthesis,
thecrystallinity
oftheMNPs
was
manipulated
bycontrolling
thereaction
conditions.MNP-3
exhibitedthe
bestcrystallinityam
ongthe
MNPstested
(Fig.S1C)and
alsodisplayed
thehighestdegree
ofmagnetization
(Fig.S1B).
Adm
inistrationofthe
MNPsinto
biologicaltissuesprofoundlyaltersthe
spin–spin
relaxationrate
(R2),and
thuscanserve
asanindicator
oftheMRIcontrastagent.T
heR2,and
hencethe
de-tection
sensitivity,ofMNP-3
was
twice
thatof
Resovist
byMRI
(Fig.2Eand
Fand
Table
S1).The
polymer
poly[aniline-co-N-(1-one-butyric
acid)]aniline
(SPAnH
)was
usedto
encapsulateiron
oxide(Fe
3 O4 ).T
hispro-
cessdecreases
theaggregation
typicalof
MNPs
andim
provestheirstability
inaqueoussolutions.Fouriertransform
IR(FT
-IR)
spectroscopyindicated
thatthesurface
oftheFe
3 O4 particlesw
ascovered
with
alayer
ofthe
SPAnH
polymer,and
thatthe
out-
Auth
orco
ntribu
tions:
H.-L.L.,
M.-Y
.H.,H.-W
.Y.,P.-Y
.C.,an
dK.-C
.W.design
edresearch
;H.-L.L.,
M.-Y
.H.,H.-W
.Y.,C.-Y
.H.,P.-C.C.,
J.-S.W.,I.-C.T.,
J.-J.W.,T.-C.Y
.,and
P.-Y.C.
per-form
edresearch;
H.-L.L.,
M.-Y
.H.,and
H.-W
.Y.contributed
newreagents/analytic
tools;H.-L.L.,M
.-Y.H.,H
.-W.Y.,C.-Y
.H.,P.-C.C.,J.-S.W
.,I.-C.T.,J.-J.W.,T.-C.Y
.,P.-Y.C.,and
K.-C.W
.analyzed
data;andH.-L.L.,M
.-Y.H.,H
.-W.Y.,and
K.-C.W
.wrote
thepaper.
Theauthors
declareno
conflict
ofinterest.
Thisarticle
isaPN
ASDirect
Submission.
R.W.is
aguest
editorinvited
bythe
EditorialBoard.
Freelyavailable
onlinethrough
thePN
ASopen
accessoption.
1H.-L.L.,M
.-Y.H.,and
H.-W
.Y.contributed
equallyto
thiswork.
2P.-Y.C.and
K.-C.W
.contributedequally
tothis
work.
3Towhom
correspondencemay
beaddressed.E-m
ail:kuochenwei@
adm.cgm
h.org.twor
pinyuanc@adm
.cgmh.org.tw
.
Thisarticle
containssupporting
information
onlineat
www.pnas.org/lookup/suppl/doi:10.
1073/pnas.1003388107/-/DCSupplem
ental.
www.pnas.org/cgi/doi/10.1073/pnas.1003388107
PNAS
|August
24,2010|
vol.107|
no.34|
15205–15210
MEDICAL SCIENCES
Electromagnetic field (EMF) Pulse Protein kinase C signalling Translocation of tight junction's Protein ZO-1 Tight Junction Opening
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr

Transport system-mediated drug delivery
Nanocarriers for brain drug delivery
mdpi.com
• Nontoxic, biodegradable and biocompatible • Particle size less than 100 nm • Stable in blood (no aggregation and dissociation) • Non-immunogenic • BBB-targeted moiety• Applicable to carry small molecules, proteins, peptides or nucleic acids
Nano carriers May be Liposomes, Micelles, Polymeric Gels, Amphiphilic Gels
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr

Transport vectors Drugs
Molecular structure mimicking the endogenous nutrients Prodrugs
BBB
Drugs
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Dopamine
LevodopaDopaminelevodopa
Decarboxylase
CNSType 1 l-type
Amino-acid transporter
Levodopa contains the carboxyl and α-amino groups

Adsorptive-mediated transcytosis
journals.cambridge.org/
Cell-penetrating peptides (CPPs)
The application of CPPs is based on the premises that biologicallyactive cargo can be attached to CPPs and translocated into cells. Thelink between the CPPs and cargo is most commonly a covalent bondand seldom in non-covalent bond. A large variety of cargo mole-cules/materials have been effectively delivered into cells via CPPs, in-cluding small molecules, proteins, peptides, fragments of DNA,liposomes and nanoparticles [204]. Some can enter brain capillary en-dothelia cells or are even translocated into the brain tissues. Some ex-amples are highlighted here.
Adenot and colleagues studied brain uptake of a number of freeand SynB3 vectorized chemotherapeutic agents using both in situbrain perfusion and in vitro BBB/cell model [203]. They reportedthat SynB3's conjugation with various poorly brain-penetratingdrugs enhanced their brain penetration by a factor of 30 for doxorubi-cin, 7 for benzylpenicillin, 22 for paclitaxel, 18 for dalargin and 50 formorphine-6-glucuronide with no effect on tight junction integrity.Brain uptake of the enkaphalin analogue, dalargin, a hexapeptide,was enhanced significantly when conjugated to SynB and injected in-travenously in mice [208]. This study signalled the potential for deliv-ery of peptides or drugs for treatment of brain cancer, through thetargeting of brain tissue after systemic delivery.
TAT is a HIV-1 trans-activating transcriptor with 101 amino acids.The protein consists of five domains; probably the best-studied regionof TAT is located in domain 4, which contains a highly basic region(with two lysines and six arginines in nine residues) involved in nuclearand nucleolar localization [209]. While all CPPs listed in Table 3 abovehave been used mainly for small cargoes such as peptides and oligonu-cleotides, Schwarze et al. [210] synthesized full-length fusion proteinsthat contained a NH2-terminal 11-amino acid protein transduction do-main (PTD) from the HIV TAT protein. Transduction of the proteinsevaluated was non-cell-specific, and was seen to occur even acrossthe BBB. Further proof of this mode of peptide delivery was attainedby Cao et al. [211] who fused the antiapoptotic protein Bcl-xL to TATand injected the construct intraperitoneally into mice that were affect-ed by stroke. The Bcl-xL protein is expressed in adult neurons of the CNSand is believed to have an important role in the prevention of neuronalapoptosis that would normally occur during brain development, or re-sults from varying stimuli leading to pathology, including cerebralischemia. Protein transduction with this entity occurred in a rapid,concentration-dependent fashion, with entry into cells thought tooccur via the lipid bilayer component of the cellular membrane. Astudy byKilic et al. [212] using the samemodel showed that brain tissuewas progressively transduced with TAT proteins within 3–4 h after in-travenous delivery. TAT-Bcl-xL treatment reduced infarct volume andneurological deficits after long ischemic insults lasting 90 min, whenapplied both before and after ischemia.
Studies have also shown that even relatively large particles could bedelivered into various cells by TAT vector. A biocompatible 45 nm
nanoparticle with an iron core, a dextran coating, and covalently linkedTAT peptides was efficiently taken up by human hematopoietic CD34+
cells [213]. Even cytoplasmatic uptake of liposomes with a diameter of200 nm has been documented [214].
Taking the TAT-mediated nanoparticles delivery approach a stepfurther, one of the most exciting demonstrations of the effectivenessof TAT-shuttled nanocarriers across the BBB was accomplished byTAT-conjugated CdS:Mn/ZnS quantum dots (Qdots) [215]. Histologi-cal data clearly showed that TAT-Qdots migrated beyond endothelialcells and reached the brain parenchyma. TAT-mediated intracellulardelivery of large molecules and nanoparticles was proved to proceedvia the energy-dependent macropinocytosis with subsequent en-hanced escape from endosome into the cell cytoplasm [207]. Recent-ly, Liu et al. produced compelling evidence that TAT facilitates humanbrain endothelia cell uptake of nanoparticles self-assembled fromTAT-PEG-b-cholesterol in vitro and more importantly, the nanoparti-cles with TAT were able to cross the BBB and translocate around thecell nucleus of neurons [216]. This study demonstrates the effective-ness of TAT in promoting the transport of nanoparticles across theBBB. It confirms that nanocarriers conjugated with TAT could be apromising carrier system for transporting drug across the BBB forthe treatment of brain disorders.
In a more recent study by Wang et al., cationic nanoparticles fabri-cated from cholesterol-CG3R6TAT via self-assembly showed strong anti-microbial activity [217]. Biodistribution studies of FITC-loadednanoparticles in rabbits and efficacy studies in a C. neoformansmeningi-tis rabbit model revealed that these nanoparticles crossed the BBB andproduced antimicrobial activity against the pathological strains in thebrain tissue with a similar efficacy as amphotericin B, suggesting a ther-apeutic dose was delivered by TAT containing nanoparticles. Further-more, these nanoparticles avoided causing the side-effects associatedwith amphotericin. This study holds importance for TAT-containingnanoparticles as it has proven that it is possible to deliver a therapeuticdose, together with functional agents, via TAT-nanoparticles into thebrain for treatment of brain infections and tracking of nanoparticles invivo, a step closer to the development of a clinically applicable nanocar-riers for treatment as well as monitoring meningitis and other brain-related disorders.
Recent evidence showed that TAT can also enhance the delivery ofliposomes into the brain. Qin et al. prepared liposomes usingcholesterol-PEG2000-TAT (TAT-LIP) and compared them to liposomesfabricated from cholesterol-PEG2000 polymer (LLIP) and conventionalcholesterol formulation (LIP) in vitro and in vivo [218]. TAT-LIP accu-mulated most in the brain (including various regions of the brain)within 24 hr after administration via tail vein, although all were notselectively targeted to the brain. All liposomes showed a uniform dis-tribution across the brain. The study also suggested adsorptive trans-cytosis could be one of the mechanisms for TAT-LIP transport acrossthe BBB and the positive charge of the TAT-LIP played an importantrole in enhancing this transport [218].
In addition to CPPs, cationic protein can also enter the brain via anadsorptive-mediated mechanism and Poduslo and Curran demon-strated that polyamine modification of proteins (insulin, albuminand IgG) can dramatically increase the permeability of proteins atthe BBB with 1.7–2.0 fold increase for insulin, 54–165 folds for albu-min and 111–349 fold for IgG in normal adult rats [219]. It is, howev-er, unknown, if this chemical modification may lead to toxicity orimmunogenicity problems. In a study reported by Lu et al., cationicbovine serum albumin (CBSA) conjugated PEG-PLA nanoparticles(CBSA-NP) was compared to native PLA bovine serum albumin conju-gated nanoparticles (BSA-NP) and CBSA unconjugated PEGylatednanoparticles (NP) in brain transcytosis across the BBB cocultureand brain delivery in mice using a fluorescent probe [220]. Thisstudy confirmed that AMT is the mechanism of brain delivery ofCBSA-NP. Increasing the surface density of CBSA conjugated pernanoparticle promoted the transcytosis ability of nanoparticles
Table 3Principle features of the selected cell penetrating peptides (CPPs).
Peptide name Sequence Netcharge
Cell lyticactivity
MAP KLALKLALKALKAALKLA +5 YespAntp43–68 RQIKIWFQNRRMKWKK +8 NoTransportan GWTLNSAGYLLGKINLKALAALAKKIL +4 YesSBP MGLGLHLLVLAAALQGAWSQPKKKRKV +6 –
FBP GALFLGWLGAAGSTMGAWSQPKKKRKV +6 –
TAT48–60 GRKKRRQRRRPPQ +8 NoSynB1 RGGRLSYSRRRFSTSTGR +6 NoSynB3 RRLSYSRRRF +6 No
MAP: model amphipathic peptide; Antp: Antennapedia; SBP: sequence signal-basedpeptide; FBP, fusion sequence-based peptide; TAT, HIV-1 trans-activating transcriptor.The peptide residues in this table are expressed with one-letter-code: K—lysine; L—leucine; A—alanine; R—arginines; Q—glutamine; I—isoleucine; W—tryptophan; F—phenylalanine; N—asparagine;M—methionine; G—glycines; S—serine; T—threonine. Datawas collected from references [204,206,221,222,312–314].
654 Y. Chen, L. Liu / Advanced Drug Delivery Reviews 64 (2012) 640–665
The major dogma has been that CPPs enter cells by a receptor and energy-independent process but the exact mechanisms are not yet fully understood
SynB1, SynB1
TAT derived CPPs Lipid raft-mediated macropinocytosis
Endosomal transport
All are having Net Positive Charge but Internalization differed in each case.

Endogenous receptor-mediated transcytosis Receptor-ligand binding
Endocytosis at the luminal (blood) side
Movement through the endothelia cytoplasm
Exocytosis of the drug or ligand-attached drug or cargo at the abluminal (brain) side
mdpi.com
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr

1810 Wu et al.
(21). Therefore, the presence of any unconjugated 83-14 mAbin the formulation comprised of the 8314-SA complex wouldcompete with binding of 8314-SA conjugate to BBB insulin re-ceptor, and this would inhibit brain uptake of the conjugatedpeptide radiopharmaceutical. In parallel to the production of8314-SA conjugate, bio-Ab1–40 must be iodinated and purified.Ab1–40 is a relatively hydrophobic peptide, and subsequentbiotinylation and iodination further increases the hydropho-bicity of this molecule, which makes it difficult to release 125I-bio-Ab1–40 from reverse phase surfaces (our unpublished ob-servations). However, this problem is obviated and the percentrecovery of 125I-bio-Ab1–40 after iodination is high using HILC(Fig. 2). Similar results were demonstrated previously aftermonobiotinylation and iodination of a vasoactive intestinalpeptide analog (30).
The multifunctionality of the amyloid imaging agent is re-tained after attachment of 125I-bio-Ab1–40 to the 8314-SA con-jugate. The three domains are depicted in Fig. 11, and includethe amyloid-binding domain, a linker domain, and a BBBtransport domain. The mAb and avidin domains are joined bya thiol-ether linkage (-S- in Fig. 11), a much more stable bondthan the disulfide (-S-S-) linkage used in previous formulations(30). In this case (Fig. 11), the peptide is attached to the target-ing vector by a noncleavable bond that confers metabolic sta-bility and is used because Ab1–40 still binds to the target amy-loid despite attachment to the delivery system (Fig. 6). Highaffinity binding of 125I-bio-Ab1–40/8314-SA to the BBB insulinreceptor is demonstrated both in vitro with isolated brain cap-illaries (Figs. 4 and 5) and in vivo in rhesus monkeys (Fig. 8).The avid binding in vivo is consistent with previous studiesshowing that endogenous insulin exerts minimal inhibition of83-14 mAb binding to the BBB insulin receptor (21). The bi-otin-binding property of the 8314-SA conjugate is containedwithin the linker domain (Fig. 11), and is demonstrated withHPLC experiments in Fig. 3 and radioreceptor assays in Figs. 4and 5. The amyloid-binding domain is comprised of radiola-beled Ab1–40, and the retention of the amyloid-binding proper-ties of the peptide pharmaceutical after conjugation to theBBB delivery system is demonstrated with the emulsion auto-radiography experiments using Alzheimer’s disease tissue sec-tions (Fig. 6). These results are similar to previously reportedemulsion and film autoradiography experiments demonstrat-ing binding of 125I-bio-Ab1–40 to amyloid plaques of sections ofAlzheimer’s disease brain after conjugation of the peptide phar-maceutical to a conjugate of SA and the OX26 mAb (16),which is a murine mAb to the rat transferrin receptor (31). Inthese previous experiments, the biotin linkage was attached tothe e-amino group of an internal lysine residue (16). In con-trast, these experiments use an Ab1–40 analog in which the bi-otin moiety is attached to the amino terminus. Previous inves-tigations have demonstrated that attachment of biotin to theamino terminus of Ab1–40 does not impair deposition of thispeptide onto preexisting Ab amyloid plaques (32).
Pharmacokinetic studies demonstrate that 125I-bio-Ab1–40 isremoved rapidly from the bloodstream and is subjected torapid metabolic degradation, as indicated by the decrease inplasma TCA precipitability (Fig. 6). Although 125I-Ab1–40 is. 90% bound by human albumin (33), this binding is rela-tively weak in vivo and does not inhibit the rapid clearanceof 125I-bio-Ab1–40 in vivo (Fig. 7). The TCA-soluble Iodine-125radioactivity in plasma at 1–3 h after i.v. injection of the peptidemay arise from proteolysis of the peptide with release of iodo-
tyrosine. An alternative pathway is surface deiodination of theintact peptide, possibly by ectoenzymes on the endothelial sur-face of organ capillary beds. Evidence for this pathway is theobservation that the systemic clearance (C1, Table I) for the125I-bio-Ab1–40/OX26-SA conjugate, 2.6 ml/min/kg, is approxi-mately fourfold greater than the systemic clearance of the un-conjugated 125I-83-14 mAb in rhesus monkeys, 0.39–1.00 ml/min/kg (21). The rapid conversion of plasma radioactivity intoTCA-soluble metabolites shown in Fig. 7 indicates that radio-iodination may not be the optimal formulation for peptide ra-diopharmaceuticals used in the future, and that alternative ra-diolabeling procedures might be considered. For example,chelating agents may be attached to e-amino groups of internallysines of the Ab1–40 peptide, which would allow for radiolabel-ing with Indium-111 or Technetium-99m (34).
Despite the relatively rapid rate of plasma clearance ofconjugated bio-Ab1–40 from plasma (Fig. 7) and the relative re-duction in plasma AUC (Table I), there is still robust brain up-take of peptide radiopharmaceutical after attachment to 8314-SAconjugate (Figs. 8 and 9). There is a twofold greater enrich-ment in brain uptake of bio-Ab1–40 conjugated to 8314-SA vec-tor in gray matter versus white matter (Figs. 8 and 9), consis-tent with previous observations showing a greater abundanceof insulin receptor in gray matter versus white matter (21).This greater abundance of receptor is due to the approxi-mately three- to fourfold greater vascular density in gray mat-ter versus white matter, as demonstrated in previous morpho-metric studies in rhesus monkey brain (21).
There is no measurable brain uptake of unconjugated bio-Ab1–40 by the brain (Figs. 8 and 9), consistent with previousstudies in rats indicating lack of significant transport of Ab1–40
through the BBB in vivo (16). Earlier experiments reported abrain VD of unconjugated Ab1–40 after internal carotid arteryperfusion that exceeded the brain plasma volume measuredwith labeled sucrose (16, 35). However, these results are con-sistent with nonspecific absorption of Ab1–40 to the brain vas-culature (16). The nonspecific absorption of 125I-bio-Ab1–40 isfurther demonstrated with isolated brain capillaries in vitro, asshown by the experiments in Fig. 5, where the brain capillary
Figure 11. Scheme depicting the multifunctionality and three do-mains of the peptide radiopharmaceutical conjugated to the BBB de-livery system. The imaging agent is comprised of amyloid-binding do-main, a linker domain, and a BBB transport domain, the last constituted by the mAb to the HIR. The HIR is localized in human brain capillary endothelium (reference 21), which forms the BBB in vivo.
1804
Wu et al.
J. Clin. Invest.© The American Society for Clinical Investigation, Inc.0021-9738/97/10/1804/09 $2.00Volume 100, Number 7, October 1997, 1804–1812http://www.jci.org
Drug Targeting of a Peptide Radiopharmaceutical through the Primate Blood–Brain Barrier In Vivo with a Monoclonal Antibody to the Human Insulin Receptor
Dafang Wu, Jing Yang, and William M. Pardridge
Department of Medicine, UCLA School of Medicine, Los Angeles, California 90095-1682
Abstract
Peptide radiopharmaceuticals are potential imaging agentsfor brain disorders, should these agents be enabled to un-dergo transport through the blood–brain barrier (BBB) in
vivo. Radiolabeled A
b
1–40
images brain amyloid in tissuesections of Alzheimer’s disease autopsy brain, but this pep-tide radiopharmaceutical cannot be used to image brainamyloid in vivo owing to negligible transport through theBBB. In these studies,
125
I-A
b
1–40
was monobiotinylated(bio) and conjugated to a BBB drug delivery and brain tar-geting system comprised of a complex of the 83-14 mono-clonal antibody (mAb) to the human insulin receptor, whichis tagged with streptavidin (SA). A marked increase inrhesus monkey brain uptake of the
125
I-bio-A
b
1–40
was ob-served after conjugation to the 8314-SA delivery system at3 h after intravenous injection. In contrast, no measurablebrain uptake of
125
I-bio-A
b
1–40
was observed in the absenceof a BBB drug delivery system. The peptide radiopharma-ceutical was degraded in brain with export of the iodide ra-dioactivity, and by 48 h after intravenous injection, 90% ofthe radioactivity was cleared from the brain. In conclusion,these studies describe a methodology for BBB drug deliveryand brain targeting of peptide radiopharmaceuticals thatcould be used for imaging amyloid or other brain disorders.
(
J. Clin. Invest.
1997. 100:1804–1812.) Key words: Alzhei-
mer’s disease
•
amyloid
•
monoclonal antibody
•
insulin re-ceptor
•
avidin
Introduction
Peptide radiopharmaceuticals have potential for diagnostic im-aging (1). The somatostatin receptor is overexpressed in cer-tain neuroendocrine tumors, as well as brain tumors such as
meningiomas or gliomas, and
125
I- or
111
In-labeled octreotide, asomatostatin peptide analog, has been used to image these tu-mors (2, 3). Owing to the small size of the peptide radiophar-maceutical, octreotide readily crosses the porous capillariesperfusing tumors in the periphery, or certain brain tumors such
as meningiomas, which lack a blood–brain barrier (BBB).
1
However, well-differentiated gliomas, which also overexpresssomatostatin receptors, have an intact BBB; it is not possibleto image these tumors with octreotide (3, 4), since this peptidedoes not cross the BBB in vivo (5).
In addition to tumors, it should also be possible to imageother medical disorders with peptide radiopharmaceuticals,such as amyloid. The deposition of amyloid in brain of Alz-heimer’s disease correlates with the degree of dementia in thisdisorder (6, 7). Extracellular amyloid in Alzheimer’s disease iscomprised of two types: senile (neuritic) plaque and vascularamyloid (8–12). Both types of amyloid in Alzheimer’s diseaseare comprised of a 43–amino acid amyloidotic peptide, desig-
nated A
b
1–43
. There are as well A
b
1–42
forms, produced fromthe abnormal proteolysis of a normal cellular protein, the amy-loid peptide precursor (13).
The A
b
amyloid of tissue sections of Alzheimer’s diseaseautopsy brain can be identified with dyes such as Congo Red,or with antibodies directed against certain epitopes of theA
b
1–42/43
peptide (14). However, the A
b
amyloid of brain sec-tions may also be identified in vitro by autoradiography with
125
I-A
b
1–40
, a peptide containing the first 40 amino acids of theA
b
1–42/43
peptide that deposits with high affinity onto preexist-ing A
b
amyloid (15). Therefore, radiolabeled A
b
1–40
is a po-tential peptide radiopharmaceutical that could be used forneurodiagnostic quantitation of the A
b
amyloid burden inAlzheimer’s disease brain of living subjects using standard ex-ternal detection methodologies, such as single photon emissioncomputed tomography or positron emission tomography.However,
125
I-A
b
1–40
does not cross the BBB in rats unless avector-mediated BBB drug delivery system is used (16). A
b
amyloid does not deposit in the brain of aged rats, but doesform in the brain of New World primates, such as the aged(15–20 yr) squirrel monkey, as vascular amyloid, and is pro-duced in the brain of Old World primates, such as the aged(27–30 yr) rhesus monkey, in neuritic plaque form (17–20).
These studies use
125
I-A
b
1–40
adapted to a BBB drug deliv-ery system that enables the peptide to enter the brain fromblood to a high degree, allowing for imaging of the distributionof the peptide radiopharmaceutical in the brain after systemic(intravenous, i.v.) injection. The goal of these studies is four-fold: first, to prepare radiolabeled peptide pharmaceutical con-jugated to the BBB delivery system; second, to demonstratethat the deposition of
125
I-A
b
1–40
on amyloid plaques in sec-
Address correspondence to William M. Pardridge, M.D., Departmentof Medicine, UCLA School of Medicine, Los Angeles, CA 90095-1682. Phone: 310-825-8858; FAX: 310-206-5163; E-mail: [email protected]
Received for publication 30 April 1997 and accepted in revisedform 7 August 1997.
1.
Abbreviations used in this paper:
A
b
1–40
, first 40 amino acids of
b
-peptide of Alzheimer’s disease; AUC, area under the plasma con-centration curve; BBB, blood–brain barrier; bio, biotinylated; HILC,hydrophilic interaction liquid chromatography; HIR, human insulinreceptor; OX26, murine mAb to rat transferrin receptor; PS, perme-ability–surface area product; RHB, Ringer-Hepes buffer; SA, strept-avidin; TEAP, triethylamine phosphate; V
D
, volume of distribution.
11/17/2015 Drug targeting of a peptide radiopharmaceutical through the primate blood-brain barrier in vivo with a monoclonal antibody to the human insulin receptor.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC508366/ 1/4
J Clin Invest. 1997 Oct 1; 100(7): 1804–1812.
doi: 10.1172/JCI119708
PMCID: PMC508366
Drug targeting of a peptide radiopharmaceutical through the primate bloodbrainbarrier in vivo with a monoclonal antibody to the human insulin receptor.D Wu, J Yang, and W M Pardridge
Department of Medicine, UCLA School of Medicine, Los Angeles, California 900951682, USA.
Copyright notice
This article has been cited by other articles in PMC.
Abstract
Peptide radiopharmaceuticals are potential imaging agents for brain disorders, should these agents be enabled toundergo transport through the bloodbrain barrier (BBB) in vivo. Radiolabeled Abeta140 images brain amyloidin tissue sections of Alzheimer's disease autopsy brain, but this peptide radiopharmaceutical cannot be used toimage brain amyloid in vivo owing to negligible transport through the BBB. In these studies, 125IAbeta140was monobiotinylated (bio) and conjugated to a BBB drug delivery and brain targeting system comprised of acomplex of the 8314 monoclonal antibody (mAb) to the human insulin receptor, which is tagged withstreptavidin (SA). A marked increase in rhesus monkey brain uptake of the 125IbioAbeta140 was observedafter conjugation to the 8314SA delivery system at 3 h after intravenous injection. In contrast, no measurablebrain uptake of 125IbioAbeta140 was observed in the absence of a BBB drug delivery system. The peptideradiopharmaceutical was degraded in brain with export of the iodide radioactivity, and by 48 h after intravenousinjection, 90% of the radioactivity was cleared from the brain. In conclusion, these studies describe amethodology for BBB drug delivery and brain targeting of peptide radiopharmaceuticals that could be used forimaging amyloid or other brain disorders.
Full TextThe Full Text of this article is available as a PDF (354K).
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
Fischman AJ, Babich JW, Strauss HW. A ticket to ride: peptide radiopharmaceuticals. J Nucl Med. 1993Dec;34(12):2253–2263. [PubMed]Krenning EP, Kwekkeboom DJ, Reubi JC, Van Hagen PM, van Eijck CH, Oei HY, Lamberts SW. 111Inoctreotide scintigraphy in oncology. Metabolism. 1992 Sep;41(9 Suppl 2):83–86. [PubMed]Reubi JC, Kvols L, Krenning E, Lamberts SW. Distribution of somatostatin receptors in normal and tumortissue. Metabolism. 1990 Sep;39(9 Suppl 2):78–81. [PubMed]Haldemann AR, Rösler H, Barth A, Waser B, Geiger L, Godoy N, Markwalder RV, Seiler RW, Sulzer M,Reubi JC. Somatostatin receptor scintigraphy in central nervous system tumors: role of bloodbrain barrierpermeability. J Nucl Med. 1995 Mar;36(3):403–410. [PubMed]Pardridge WM, Triguero D, Yang J, Cancilla PA. Comparison of in vitro and in vivo models of drugtranscytosis through the bloodbrain barrier. J Pharmacol Exp Ther. 1990 May;253(2):884–891. [PubMed]Tomlinson BE, Blessed G, Roth M. Observations on the brains of demented old people. J Neurol Sci. 1970Sep;11(3):205–242. [PubMed]Cummings BJ, Cotman CW. Image analysis of betaamyloid load in Alzheimer's disease and relation todementia severity. Lancet. 1995 Dec 9;346(8989):1524–1528. [PubMed]
Insulin receptor
Amyloid-β- peptide 125I-Abeta1–40 conjugated to 83–14 monoclonal antibody (mAb)
Insulin receptor Diagnostic probe for AD Receptor mediated Endocytosis
11/17/2015 Drug targeting of a peptide radiopharmaceutical through the primate blood-brain barrier in vivo with a monoclonal antibody to the human insulin receptor.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC508366/ 1/4
J Clin Invest. 1997 Oct 1; 100(7): 1804–1812.
doi: 10.1172/JCI119708
PMCID: PMC508366
Drug targeting of a peptide radiopharmaceutical through the primate bloodbrainbarrier in vivo with a monoclonal antibody to the human insulin receptor.D Wu, J Yang, and W M Pardridge
Department of Medicine, UCLA School of Medicine, Los Angeles, California 900951682, USA.
Copyright notice
This article has been cited by other articles in PMC.
Abstract
Peptide radiopharmaceuticals are potential imaging agents for brain disorders, should these agents be enabled toundergo transport through the bloodbrain barrier (BBB) in vivo. Radiolabeled Abeta140 images brain amyloidin tissue sections of Alzheimer's disease autopsy brain, but this peptide radiopharmaceutical cannot be used toimage brain amyloid in vivo owing to negligible transport through the BBB. In these studies, 125IAbeta140was monobiotinylated (bio) and conjugated to a BBB drug delivery and brain targeting system comprised of acomplex of the 8314 monoclonal antibody (mAb) to the human insulin receptor, which is tagged withstreptavidin (SA). A marked increase in rhesus monkey brain uptake of the 125IbioAbeta140 was observedafter conjugation to the 8314SA delivery system at 3 h after intravenous injection. In contrast, no measurablebrain uptake of 125IbioAbeta140 was observed in the absence of a BBB drug delivery system. The peptideradiopharmaceutical was degraded in brain with export of the iodide radioactivity, and by 48 h after intravenousinjection, 90% of the radioactivity was cleared from the brain. In conclusion, these studies describe amethodology for BBB drug delivery and brain targeting of peptide radiopharmaceuticals that could be used forimaging amyloid or other brain disorders.
Full TextThe Full Text of this article is available as a PDF (354K).
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
Fischman AJ, Babich JW, Strauss HW. A ticket to ride: peptide radiopharmaceuticals. J Nucl Med. 1993Dec;34(12):2253–2263. [PubMed]Krenning EP, Kwekkeboom DJ, Reubi JC, Van Hagen PM, van Eijck CH, Oei HY, Lamberts SW. 111Inoctreotide scintigraphy in oncology. Metabolism. 1992 Sep;41(9 Suppl 2):83–86. [PubMed]Reubi JC, Kvols L, Krenning E, Lamberts SW. Distribution of somatostatin receptors in normal and tumortissue. Metabolism. 1990 Sep;39(9 Suppl 2):78–81. [PubMed]Haldemann AR, Rösler H, Barth A, Waser B, Geiger L, Godoy N, Markwalder RV, Seiler RW, Sulzer M,Reubi JC. Somatostatin receptor scintigraphy in central nervous system tumors: role of bloodbrain barrierpermeability. J Nucl Med. 1995 Mar;36(3):403–410. [PubMed]Pardridge WM, Triguero D, Yang J, Cancilla PA. Comparison of in vitro and in vivo models of drugtranscytosis through the bloodbrain barrier. J Pharmacol Exp Ther. 1990 May;253(2):884–891. [PubMed]Tomlinson BE, Blessed G, Roth M. Observations on the brains of demented old people. J Neurol Sci. 1970Sep;11(3):205–242. [PubMed]Cummings BJ, Cotman CW. Image analysis of betaamyloid load in Alzheimer's disease and relation todementia severity. Lancet. 1995 Dec 9;346(8989):1524–1528. [PubMed]
Low-density lipoprotein receptor related proteins 1 and 2 (LRP1 and LRP2 receptors)
ApoE (Apolipoprotein E)Tissue plasminogen activator (tPA)Plasminogen activator inhibitor 1(PAI-1)Amyloid precursor protein (APP)LactoferrinMelanotransferrinα2 macroglobulin (α2 M)Receptor associated protein (RAP)HIV-1 TAT proteinHeparin cofactor IIHeat shock protein 96 (HSP-96)Engineered angiopeps
Binds to Specific LRP1 and LRP2 receptors in BBB Receptor-mediated transcytosis

Diphtheria toxin receptor (DTR)
Transferrin receptor
Expert Review
Blood–Brain Barrier Transport of Therapeutics via Receptor-Mediation
Angela R. Jones1 and Eric V. Shusta1,2
Received March 29, 2007; accepted May 3, 2007; published online July 10, 2007
Abstract. Drug delivery to the brain is hindered by the presence of the blood–brain barrier (BBB).Although the BBB restricts the passage of many substances, it is actually selectively permeable tonutrients necessary for healthy brain function. To accomplish the task of nutrient transport, the brainendothelium is endowed with a diverse collection of molecular transport systems. One such class oftransport system, known as a receptor-mediated transcytosis (RMT), employs the vesicular traffickingmachinery of the endothelium to transport substrates between blood and brain. If appropriatelytargeted, RMT systems can also be used to shuttle a wide range of therapeutics into the brain in anoninvasive manner. Over the last decade, there have been significant developments in the arena ofRMT-based brain drug transport, and this review will focus on those approaches that have beenvalidated in an in vivo setting.
KEY WORDS: antibody; blood–brain barrier; brain drug delivery; transcytosis.
INTRODUCTION
The blood–brain barrier (BBB) provides the brain withnutrients, prevents the introduction of harmful blood-bornesubstances, and restricts the movement of ions and fluid toensure an optimal environment for brain function. As a
consequence of its barrier properties, the BBB also preventsthe movement of drugs from the blood into the brain, andtherefore acts as an obstacle for the systemic delivery ofneurotherapeutics. Unless a therapeutic molecule is lipid-soluble with a molecular weight of 400–600 Da or less, brainpenetration is limited (1). Furthermore, efflux transportsystems may target the drugs that meet these criteria andexport them from the brain. As a result, the BBB excludesmany small-molecule pharmaceuticals, and nearly all bio-pharmaceuticals such as gene and protein medicines fail topenetrate into the brain tissue to an appreciable extent (1).Thus, although the surface area of the human brainmicrovasculature available for drug transport (õ20 m2) ismore than adequate for treating the entire brain volume, thebarrier properties of the BBB continue to restrict brain drugdelivery via the bloodstream (2).
To date, strategies for the delivery of drugs that do nothave an appreciable BBB permeability have included bothinvasive and noninvasive approaches. Direct intracranialinjection, intraventricular administration and BBB disruptionare examples of invasive delivery techniques that have beenreviewed elsewhere (3). Instead, this review will focus on arapidly developing class of novel delivery reagents thatfunction in mediating noninvasive blood-to-brain transportby taking advantage of endogenous nutrient transportsystems present at the BBB. Nutrients and water-solublecompounds such as ions, amino acids, vitamins, and proteinsthat are necessary for brain function possess specific trans-port systems embedded in the plasma membranes of theBBB to allow brain entry. Three main classes of transportsystems function at the BBB. The first, carrier-mediatedtransport, relies on molecular carriers present at both theapical (blood) and basolateral (brain) membranes of theBBB (Fig. 1c). These carriers tend to be highly stereospecificand function in the selective transport of small molecules
1759 0724-8741/07/0900-1759/0 # 2007 Springer Science + Business Media, LLC
Pharmaceutical Research, Vol. 24, No. 9, September 2007 (# 2007)DOI: 10.1007/s11095-007-9379-0
1 Department of Chemical and Biological Engineering, University ofWisconsin-Madison, 1415 Engineering Drive, Madison, Wisconsin53706, USA.
2To whom correspondence should be addressed.(e-mail:[email protected])
ABBREVIATIONS: ADR, adriamycin; AEM, analytical electronmicroscopy; AUC, area under the curve; Av, avidin; AZT,azidothymidine; BBB, blood–brain barrier; BDNF, brain-derivedneurotrophic factor; bFGF, basic fibroblast growth factor; DSPE,distearoylphosphatidylethanolamine; EGFR, human epidermalgrowth factor receptor; FGF-2, fibroblast growth factor-2; GFAP,glial fibrillary acidic protein; GUS, b-glucuronidase; HB-EGF,heparin binding epidermal growth factor-like growth factor; HCEC,human cerebromicrovascular endothelial cells; HD, Huntington_sdisease; HIR, human insulin receptor; HRP, horseradish peroxidase;IGF-II, insulin-like growth factor II; LDL, low density lipoprotein;LRP1/2, low density lipoprotein receptor-related protein 1/2; M6P,mannose 6-phosphate; MAb, monoclonal antibody; MCAO, middlecerebral artery occlusion; NGF, nerve growth factor; NHS,N-hydroxysuccinimide; ODN, oligonucleotides; PBCA, poly(butylcyanoacrylate); PEG, poly(ethylene glycol); P-GUS, phosphorylatedb-glucuronidase; PNA, peptide nucleic acid; RAP, receptor-associated protein; RES, reticuloendothelial system; RMT, receptor-mediated transcytosis; rsCD4, recombinant human soluble CD4; SA/B,streptavidin/ biotin; SATA, N-succinimidyl S-acetylthioacetate; scFv,single-chain variable fragment; sdAb, single-domain antibodies;SMCC, Succinimidyl 4-[N-maleimidomethyl]-cyclohexane-1-carboxylate; SV40, simian virus 40; Tf, transferrin; TfR, transferrinreceptor; TH, tyrosine hydroxylase; tPA, tissue-type plasminogenactivator; VIP, vasoactive intestinal peptide.
Expert Review
Blood–Brain Barrier Transport of Therapeutics via Receptor-Mediation
Angela R. Jones1 and Eric V. Shusta1,2
Received March 29, 2007; accepted May 3, 2007; published online July 10, 2007
Abstract. Drug delivery to the brain is hindered by the presence of the blood–brain barrier (BBB).Although the BBB restricts the passage of many substances, it is actually selectively permeable tonutrients necessary for healthy brain function. To accomplish the task of nutrient transport, the brainendothelium is endowed with a diverse collection of molecular transport systems. One such class oftransport system, known as a receptor-mediated transcytosis (RMT), employs the vesicular traffickingmachinery of the endothelium to transport substrates between blood and brain. If appropriatelytargeted, RMT systems can also be used to shuttle a wide range of therapeutics into the brain in anoninvasive manner. Over the last decade, there have been significant developments in the arena ofRMT-based brain drug transport, and this review will focus on those approaches that have beenvalidated in an in vivo setting.
KEY WORDS: antibody; blood–brain barrier; brain drug delivery; transcytosis.
INTRODUCTION
The blood–brain barrier (BBB) provides the brain withnutrients, prevents the introduction of harmful blood-bornesubstances, and restricts the movement of ions and fluid toensure an optimal environment for brain function. As a
consequence of its barrier properties, the BBB also preventsthe movement of drugs from the blood into the brain, andtherefore acts as an obstacle for the systemic delivery ofneurotherapeutics. Unless a therapeutic molecule is lipid-soluble with a molecular weight of 400–600 Da or less, brainpenetration is limited (1). Furthermore, efflux transportsystems may target the drugs that meet these criteria andexport them from the brain. As a result, the BBB excludesmany small-molecule pharmaceuticals, and nearly all bio-pharmaceuticals such as gene and protein medicines fail topenetrate into the brain tissue to an appreciable extent (1).Thus, although the surface area of the human brainmicrovasculature available for drug transport (õ20 m2) ismore than adequate for treating the entire brain volume, thebarrier properties of the BBB continue to restrict brain drugdelivery via the bloodstream (2).
To date, strategies for the delivery of drugs that do nothave an appreciable BBB permeability have included bothinvasive and noninvasive approaches. Direct intracranialinjection, intraventricular administration and BBB disruptionare examples of invasive delivery techniques that have beenreviewed elsewhere (3). Instead, this review will focus on arapidly developing class of novel delivery reagents thatfunction in mediating noninvasive blood-to-brain transportby taking advantage of endogenous nutrient transportsystems present at the BBB. Nutrients and water-solublecompounds such as ions, amino acids, vitamins, and proteinsthat are necessary for brain function possess specific trans-port systems embedded in the plasma membranes of theBBB to allow brain entry. Three main classes of transportsystems function at the BBB. The first, carrier-mediatedtransport, relies on molecular carriers present at both theapical (blood) and basolateral (brain) membranes of theBBB (Fig. 1c). These carriers tend to be highly stereospecificand function in the selective transport of small molecules
1759 0724-8741/07/0900-1759/0 # 2007 Springer Science + Business Media, LLC
Pharmaceutical Research, Vol. 24, No. 9, September 2007 (# 2007)DOI: 10.1007/s11095-007-9379-0
1 Department of Chemical and Biological Engineering, University ofWisconsin-Madison, 1415 Engineering Drive, Madison, Wisconsin53706, USA.
2To whom correspondence should be addressed.(e-mail:[email protected])
ABBREVIATIONS: ADR, adriamycin; AEM, analytical electronmicroscopy; AUC, area under the curve; Av, avidin; AZT,azidothymidine; BBB, blood–brain barrier; BDNF, brain-derivedneurotrophic factor; bFGF, basic fibroblast growth factor; DSPE,distearoylphosphatidylethanolamine; EGFR, human epidermalgrowth factor receptor; FGF-2, fibroblast growth factor-2; GFAP,glial fibrillary acidic protein; GUS, b-glucuronidase; HB-EGF,heparin binding epidermal growth factor-like growth factor; HCEC,human cerebromicrovascular endothelial cells; HD, Huntington_sdisease; HIR, human insulin receptor; HRP, horseradish peroxidase;IGF-II, insulin-like growth factor II; LDL, low density lipoprotein;LRP1/2, low density lipoprotein receptor-related protein 1/2; M6P,mannose 6-phosphate; MAb, monoclonal antibody; MCAO, middlecerebral artery occlusion; NGF, nerve growth factor; NHS,N-hydroxysuccinimide; ODN, oligonucleotides; PBCA, poly(butylcyanoacrylate); PEG, poly(ethylene glycol); P-GUS, phosphorylatedb-glucuronidase; PNA, peptide nucleic acid; RAP, receptor-associated protein; RES, reticuloendothelial system; RMT, receptor-mediated transcytosis; rsCD4, recombinant human soluble CD4; SA/B,streptavidin/ biotin; SATA, N-succinimidyl S-acetylthioacetate; scFv,single-chain variable fragment; sdAb, single-domain antibodies;SMCC, Succinimidyl 4-[N-maleimidomethyl]-cyclohexane-1-carboxylate; SV40, simian virus 40; Tf, transferrin; TfR, transferrinreceptor; TH, tyrosine hydroxylase; tPA, tissue-type plasminogenactivator; VIP, vasoactive intestinal peptide.
* Here TfR is BBB specific
CNS diseases such as AD, Parkinson's disease, multiple sclerosis(MS), ischemia, encephalitis, epilepsy, tumour and lysosomal storage disease
Inflammation In BBB Upregulation of DTR
Diphtheria toxinMutated
Cross reacting material (CRM 197)
Target
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr
Modern methods for delivery of drugs across the blood–brain barrier
Yan Chen a,⁎, Lihong Liu b,1
a School of Pharmacy, CHIRI, WABRI, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australiab Institute of Bioengineering and Nanotechnology, 31 Biopolis Way, Singapore 138669, Singapore
a b s t r a c ta r t i c l e i n f o
Article history:Received 6 August 2011Accepted 21 November 2011Available online 28 November 2011
Keywords:Blood–brain barrierDrug deliveryReceptor-mediated transportCell-mediated transportNanoparticlesLiposomesPathological conditions
The blood–brain barrier (BBB) is a highly regulated and efficient barrier that provides a sanctuary to thebrain. It is designed to regulate brain homeostasis and to permit selective transport of molecules that are es-sential for brain function. Unfortunately, drug transport to the brain is hampered by this almost impermeable,highly selective and well coordinated barrier. With progress in molecular biology, the BBB is better under-stood, particularly under different pathological conditions. This review will discuss the barrier issue from abiological and pathological perspective to provide a better insight to the challenges and opportunities asso-ciated with the BBB. Modern methods which can take advantage of these opportunities will be reviewed.Applications of nanotechnology in drug transport, receptor-mediated targeting and transport, and finallycell-mediated drug transport will also be covered in the review. The challenge of delivering an effective ther-apy to the brain is formidable; solutions will likely involve concerted multidisciplinary approaches that takeinto account BBB biology as well as the unique features associated with the pathological condition to betreated.
Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6412. Physiology and biology of the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6413. Transport routes across the blood–brain barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6424. Biological and pathological properties of BBB for drug transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
4.1. Physical barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 643
Advanced Drug Delivery Reviews 64 (2012) 640–665
Abbreviations: a2M, alpha-2 macroglobulin; Aβ, amyloid β; ABC, ATP binding cassette; AD, Alzheimer's disease; AIDS, autoimmunodeficiency syndrome; AJ, adherens junction;AMT, adsorptive-mediated transport; AMP, adenosine monophosphate; ANG1005, angiopep 2 conjugated with 3 molecules of paclitaxel; Antp, Antennapedia; APP, amyloid betaprecursor protein; ApoE, Apolipoprotein E; ATP, adenosine triphosphate; AUC, area under curve; BBB, blood–brain barrier; BCSFB, blood–cerebrospinal fluid barrier; BSA-NP, bovineserum albumin conjugated nanoparticles; cAMP, cyclic AMP; CBSA, cationic bovine serum albumin; CBSA-NP, CBSA conjugated PEG-PLA nanoparticles; CED, convection enhanceddiffusion; CHP, hydrophobic cholesterol groups; CMC, critical micelle concentration; CMT, carrier-mediated transport; CNS, central nervous system; CPP, cell penetrating peptide;CRM, cross reacting material; CSF, cerebrospinal fluid; DT, diphtheria toxin; DTR, diphtheria toxin receptor; EAE, experimental autoimmune encephalomyelitis; EO, ethylene oxide;EC, endothelial cell; EMF, electromagnetic fields; FBP, fusion sequence-based peptide; g7, similopioid peptide; GMP, guanosine monophosphate; HB-EGF, heparin binding epider-mal growth factor; HIRMAb, human insulin receptor monoclonal antibody; HIV, human immunodeficiency virus; HLB, hydrophobic–hydrophilic balance; HSA, human serum albu-min; HSP-96, heat shock protein 96; HUVEC, human umbilical vein endothelial cells; ICH, intercerebral haemorrhage; ICV, intracerebroventricular; IgG, immunoglobulin G; IL,interleukin; INF, interferon; JAM, junction adhesion molecules; LDL, low density lipoprotein; LDLR, low density lipoprotein receptor; Lf, lactoferrin; LMV, large multilamellarvesicles; LPA, lysophosphatidic acid; LRP, lipoprotein receptor protein; LUV, large unilamellar vesicles; MAP, model amphipathic peptide; MAPK, mitogen activated protein kinase;MCP, monocyte chemotactic protein; MHC, major histocompatibility complex; MLCK, myosin light chain kinase; MP, mononuclear phagocytes; MRP, multidrug resistant pro-tein; MS, multiple sclerosis; NOS, nitric oxide syntheses; NP, nanoparticles; NVU, neurovascular unit; P97, melanotransferrin; PAI-1, plasminogen activator inhibitor 1;PHDCA, poly(hexadecylcyanoacrylate); PBCA, poly(butylcyanoacrylate); PEG, polyethylene glycol; PEG-PCL, PEG-polycaprolactone; PEG-G-CSF, PEGylated-recombinantmethionyl human granulocyted colony stimulating factor; PEG-PLA, polyethylene glycol-polylactic acid; P-gp, P-glycoprotein; PKA, protein kinase A; PKC, protein kinase C;PKG, protein kinase G; PLGA, poly(D,L-lactide-co-glycolide); PO, propylene oxide; PTD, protein transduction domain; PTK, protein tyrosine kinase; Qdots, quantum dots; RAP,receptor associated protein; RES, reticuloendothelial system; REV, reverse phase evaporation vesicles; RMT, receptor-mediated transport; R123, rhodamine 123; SA, sialicacid residue; SBP, sequence signal-based peptide; SUV, small unilamellar vesicles; TAT, HIV-1 trans-activating transcriptor; TEM, transmission electronmicroscopy; TER, transendothelialelectrical resistance; TfR, transferrin receptor; TJ, tight junction; TNF, tumour necrosis factors; tPA, tissue plasminogen activator; VE, vascular endothelial; VEGF, vascular endothelialgrowth factor; ZO, zonula occludens. This review is part of the Advanced Drug Delivery Reviews theme issue on “Delivery of Therapeutics to the Central Nervous System”.⁎ Corresponding author at: School of Pharmacy, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia. Tel.: +61 8 9266 2738; fax. +61 89266 2769.
E-mail address: [email protected] (Y. Chen).1 L Liu is currently funded as an Australian Postdoctoral Fellow by ARC Discovery Project DP110104599 at Chemical Engineering, Curtin University.
0169-409X/$ – see front matter. Crown Copyright © 2011 Published by Elsevier B.V. All rights reserved.doi:10.1016/j.addr.2011.11.010
Contents lists available at SciVerse ScienceDirect
Advanced Drug Delivery Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /addr

Inhibition of efflux Pumps
11/17/2015 PubMed Central, FIG. 1.: NeuroRx. 2005 Jan; 2(1): 86–98. doi: 10.1602/neurorx.2.1.86
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC539326/figure/f1/ 1/1
<< Prev FIG. 1. Next >>PMC full text: NeuroRx. 2005 Jan; 2(1): 86–98.doi: 10.1602/neurorx.2.1.86Copyright/License Request permission to reuse
FIG. 1.
Localization of selected drug efflux proteins on brain capillary endothelial cells that form the bloodbrain
barrier. Only transporters that are localized on the apical (luminal) side of the brain capillary endothelium
would be in a position to restrict brain uptake of xenobiotics. Note that the exact localization in endothelial
cells has not been demonstrated as yet for all transporters shown in the figure, but for some of the
transporters the localization (apical vs basolateral) was derived from studies on polarized epithelial celllines.
6
Blood-Brain Barrier Active Efflux Transporters: ATP-BindingCassette Gene Family
Wolfgang Loscher and Heidrun Potschka
Department of Pharmacology, Toxicology, and Pharmacy, University of Veterinary Medicine Hannover,Hannover D-30559, Germany
Summary: The blood-brain barrier (BBB) contributes to brainhomeostasis by protecting the brain from potentially harmfulendogenous and exogenous substances. BBB active drug effluxtransporters of the ATP-binding cassette (ABC) gene familyare increasingly recognized as important determinants of drugdistribution to, and elimination from, the CNS. The ABC effluxtransporter P-glycoprotein (Pgp) has been demonstrated as akey element of the BBB that can actively transport a hugevariety of lipophilic drugs out of the brain capillary endothelialcells that form the BBB. In addition to Pgp, other ABC effluxtransporters such as members of the multidrug resistance pro-tein (MRP) family and breast cancer resistance protein (BCRP)seem to contribute to BBB function. Consequences of ABC
efflux transporters in the BBB include minimizing or avoidingneurotoxic adverse effects of drugs that otherwise would pen-etrate into the brain. However, ABC efflux transporters mayalso limit the central distribution of drugs that are beneficial totreat CNS diseases. Furthermore, neurological disorders suchas epilepsy may be associated with overexpression of ABCefflux transporters at the BBB, resulting in pharmacoresistanceto therapeutic medication. Therefore, modulation of ABC ef-flux transporters at the BBB forms a novel strategy to enhancethe penetration of drugs into the brain and may yield newtherapeutic options for drug-resistant CNS diseases. KeyWords: P-glycoprotein, multidrug resistance proteins, epi-lepsy, antiepileptic drugs, depression, AIDS.
INTRODUCTION
ATP-binding cassette (ABC) transporters are multido-main integral membrane proteins that use the energy ofATP hydrolysis to translocate solutes across cellularmembranes in all mammalian species.1 ABC transportersform one of the largest of all protein families and arecentral to many important biomedical phenomena, in-cluding resistance of cancers and pathogenic microbes todrugs.2 Elucidation of the structure and function of ABCtransporters is essential to the rational design of agents tocontrol their function.
ABC transporters are increasingly recognized to beimportant for drug disposition and response.3–7 P-glyco-protein (Pgp), the encoded product of the human multi-drug resistance (MDR1) (ABCB1) gene, is of particularclinical relevance in that this transporter has a broadsubstrate specificity, including a variety of structurallydivergent drugs in clinical use today.7–9 Moreover, ex-
pression of this efflux transporter in certain tissue com-partments such as the gastrointestinal tract and braincapillary endothelial cells limits oral absorption and CNSentry of many drugs.7 The use of Pgp-expressing celllines, the generation of Pgp knockout mice as well asstudies using Pgp inhibitors in animals, contributed to abetter understanding on the role of active transport pro-cesses for drug disposition.8 In addition to Pgp, the ABCtransporters of the multidrug resistance protein (MRP;ABCC) family and the breast cancer resistance protein(BCRP; ABCG2) have a role in drug disposition.6,9 Thefamily of mammalian ABC transporters, however, is farmore extensive, and functionally highly diverse.1 In thisreview, we limit ourselves to the following ABC trans-porters: Pgp, MRPs 1-6, and BCRP, i.e., ABC transport-ers that are expressed at the blood-brain barrier (BBB)and, particularly Pgp, are involved in the regulation ofbrain uptake and extrusion of drugs.6,7,9,10
WHICH ABC TRANSPORTERS AREEXPRESSED AT THE BBB?
Drug uptake into the brain is dependent on a variety offactors, including the physical barrier presented by the
Address correspondence and reprint requests to Dr. W. Loscher,Department of Pharmacology, Toxicology and Pharmacy, University ofVeterinary Medicine Hannover, Foundation, Bunteweg 17, D-30559Hannover, Germany. E-mail: [email protected].
NeuroRx!: The Journal of the American Society for Experimental NeuroTherapeutics
Vol. 2, 86–98, January 2005 © The American Society for Experimental NeuroTherapeutics, Inc.86
Advanced Drug Delivery Reviews 55 (2003) 151–164www.elsevier.com/ locate /drugdeliv
P luronic block copolymers as modulators of drug effluxtransporter activity in the blood–brain barrier
*Alexander V. Kabanov , Elena V. Batrakova, Donald W. MillerDepartment of Pharmaceutical Sciences, University of Nebraska Medical Center, 986025 Nebraska Medical Center, Omaha, NE 68198,
USA
Received 6 July 2002; accepted 11 August 2002
Abstract
Drug efflux transporters can influence the absorption, tissue distribution and elimination of many therapeutic agents.Modulation of drug efflux transporter activity is being explored as a means for improving the pharmacokinetic andpharmacodynamic properties of various drugs. In this regard, several polymer formulations have been shown to inhibit drug
efflux transporters such as P-glycoprotein (P-gp). The current review will focus on Pluronic block copolymers in particular,the mechanisms involved in the effects of Pluronic on drug efflux transporters, and the optimal polymer compositions
required for inhibition of drug efflux transporters. Special emphasis will be placed on the potential applications of Pluronicin enhancing the blood–brain barrier (BBB) penetration of drugs. 2002 Elsevier Science B.V. All rights reserved.
Keywords: Blood–brain barrier; Multidrug resistance (MDR); P-glycoprotein; Multidrug resistant protein (MRP); Block copolymer
Contents
1 . Introduction ............................................................................................................................................................................ 1512 . Overview of Pluronic block copolymers in pharmaceutics ........................................................................................................ 152
3 . Pluronic block copolymers in drug resistant cancer .................................................................................................................. 1524 . Effects of Pluronic on P-gp activity in the blood–brain barrier.................................................................................................. 154
5 . Mechanism of Pluronic -induced inhibition of P-gp in brain endothelial cells ............................................................................. 1555 .1. ATP depletion in the presence of Pluronic block copolymers ............................................................................................ 155
5 .2. Membrane interactions of Pluronic and inhibition of P-gp ATPase activity......................................................................... 1566 . Optimization of Pluronic compositions for P-gp inhibition in brain endothelial cells .................................................................. 157
7 . Effects of Pluronic on drug transport across BBB: in vitro and in vivo evaluation ...................................................................... 1588 . Toxicological considerations of Pluronic block copolymers ...................................................................................................... 160
9 . Conclusion.............................................................................................................................................................................. 161Acknowledgements ...................................................................................................................................................................... 161References .................................................................................................................................................................................. 161
*Corresponding author. Tel.: 11-402-559-9364; fax: 11-402-559-9543.E-mail address: [email protected] (A.V. Kabanov).
0169-409X/02/$ – see front matter 2002 Elsevier Science B.V. All rights reserved.PI I : S0169-409X( 02 )00176-X
Advanced Drug Delivery Reviews 55 (2003) 151–164www.elsevier.com/ locate /drugdeliv
P luronic block copolymers as modulators of drug effluxtransporter activity in the blood–brain barrier
*Alexander V. Kabanov , Elena V. Batrakova, Donald W. MillerDepartment of Pharmaceutical Sciences, University of Nebraska Medical Center, 986025 Nebraska Medical Center, Omaha, NE 68198,
USA
Received 6 July 2002; accepted 11 August 2002
Abstract
Drug efflux transporters can influence the absorption, tissue distribution and elimination of many therapeutic agents.Modulation of drug efflux transporter activity is being explored as a means for improving the pharmacokinetic andpharmacodynamic properties of various drugs. In this regard, several polymer formulations have been shown to inhibit drug
efflux transporters such as P-glycoprotein (P-gp). The current review will focus on Pluronic block copolymers in particular,the mechanisms involved in the effects of Pluronic on drug efflux transporters, and the optimal polymer compositions
required for inhibition of drug efflux transporters. Special emphasis will be placed on the potential applications of Pluronicin enhancing the blood–brain barrier (BBB) penetration of drugs. 2002 Elsevier Science B.V. All rights reserved.
Keywords: Blood–brain barrier; Multidrug resistance (MDR); P-glycoprotein; Multidrug resistant protein (MRP); Block copolymer
Contents
1 . Introduction ............................................................................................................................................................................ 1512 . Overview of Pluronic block copolymers in pharmaceutics ........................................................................................................ 152
3 . Pluronic block copolymers in drug resistant cancer .................................................................................................................. 1524 . Effects of Pluronic on P-gp activity in the blood–brain barrier.................................................................................................. 154
5 . Mechanism of Pluronic -induced inhibition of P-gp in brain endothelial cells ............................................................................. 1555 .1. ATP depletion in the presence of Pluronic block copolymers ............................................................................................ 155
5 .2. Membrane interactions of Pluronic and inhibition of P-gp ATPase activity......................................................................... 1566 . Optimization of Pluronic compositions for P-gp inhibition in brain endothelial cells .................................................................. 157
7 . Effects of Pluronic on drug transport across BBB: in vitro and in vivo evaluation ...................................................................... 1588 . Toxicological considerations of Pluronic block copolymers ...................................................................................................... 160
9 . Conclusion.............................................................................................................................................................................. 161Acknowledgements ...................................................................................................................................................................... 161References .................................................................................................................................................................................. 161
*Corresponding author. Tel.: 11-402-559-9364; fax: 11-402-559-9543.E-mail address: [email protected] (A.V. Kabanov).
0169-409X/02/$ – see front matter 2002 Elsevier Science B.V. All rights reserved.PI I : S0169-409X( 02 )00176-X
Advanced Drug Delivery Reviews 55 (2003) 151–164www.elsevier.com/ locate /drugdeliv
P luronic block copolymers as modulators of drug effluxtransporter activity in the blood–brain barrier
*Alexander V. Kabanov , Elena V. Batrakova, Donald W. MillerDepartment of Pharmaceutical Sciences, University of Nebraska Medical Center, 986025 Nebraska Medical Center, Omaha, NE 68198,
USA
Received 6 July 2002; accepted 11 August 2002
Abstract
Drug efflux transporters can influence the absorption, tissue distribution and elimination of many therapeutic agents.Modulation of drug efflux transporter activity is being explored as a means for improving the pharmacokinetic andpharmacodynamic properties of various drugs. In this regard, several polymer formulations have been shown to inhibit drug
efflux transporters such as P-glycoprotein (P-gp). The current review will focus on Pluronic block copolymers in particular,the mechanisms involved in the effects of Pluronic on drug efflux transporters, and the optimal polymer compositions
required for inhibition of drug efflux transporters. Special emphasis will be placed on the potential applications of Pluronicin enhancing the blood–brain barrier (BBB) penetration of drugs. 2002 Elsevier Science B.V. All rights reserved.
Keywords: Blood–brain barrier; Multidrug resistance (MDR); P-glycoprotein; Multidrug resistant protein (MRP); Block copolymer
Contents
1 . Introduction ............................................................................................................................................................................ 1512 . Overview of Pluronic block copolymers in pharmaceutics ........................................................................................................ 152
3 . Pluronic block copolymers in drug resistant cancer .................................................................................................................. 1524 . Effects of Pluronic on P-gp activity in the blood–brain barrier.................................................................................................. 154
5 . Mechanism of Pluronic -induced inhibition of P-gp in brain endothelial cells ............................................................................. 1555 .1. ATP depletion in the presence of Pluronic block copolymers ............................................................................................ 155
5 .2. Membrane interactions of Pluronic and inhibition of P-gp ATPase activity......................................................................... 1566 . Optimization of Pluronic compositions for P-gp inhibition in brain endothelial cells .................................................................. 157
7 . Effects of Pluronic on drug transport across BBB: in vitro and in vivo evaluation ...................................................................... 1588 . Toxicological considerations of Pluronic block copolymers ...................................................................................................... 160
9 . Conclusion.............................................................................................................................................................................. 161Acknowledgements ...................................................................................................................................................................... 161References .................................................................................................................................................................................. 161
*Corresponding author. Tel.: 11-402-559-9364; fax: 11-402-559-9543.E-mail address: [email protected] (A.V. Kabanov).
0169-409X/02/$ – see front matter 2002 Elsevier Science B.V. All rights reserved.PI I : S0169-409X( 02 )00176-X
Advanced Drug Delivery Reviews 55 (2003) 151–164www.elsevier.com/ locate /drugdeliv
P luronic block copolymers as modulators of drug effluxtransporter activity in the blood–brain barrier
*Alexander V. Kabanov , Elena V. Batrakova, Donald W. MillerDepartment of Pharmaceutical Sciences, University of Nebraska Medical Center, 986025 Nebraska Medical Center, Omaha, NE 68198,
USA
Received 6 July 2002; accepted 11 August 2002
Abstract
Drug efflux transporters can influence the absorption, tissue distribution and elimination of many therapeutic agents.Modulation of drug efflux transporter activity is being explored as a means for improving the pharmacokinetic andpharmacodynamic properties of various drugs. In this regard, several polymer formulations have been shown to inhibit drug
efflux transporters such as P-glycoprotein (P-gp). The current review will focus on Pluronic block copolymers in particular,the mechanisms involved in the effects of Pluronic on drug efflux transporters, and the optimal polymer compositions
required for inhibition of drug efflux transporters. Special emphasis will be placed on the potential applications of Pluronicin enhancing the blood–brain barrier (BBB) penetration of drugs. 2002 Elsevier Science B.V. All rights reserved.
Keywords: Blood–brain barrier; Multidrug resistance (MDR); P-glycoprotein; Multidrug resistant protein (MRP); Block copolymer
Contents
1 . Introduction ............................................................................................................................................................................ 1512 . Overview of Pluronic block copolymers in pharmaceutics ........................................................................................................ 152
3 . Pluronic block copolymers in drug resistant cancer .................................................................................................................. 1524 . Effects of Pluronic on P-gp activity in the blood–brain barrier.................................................................................................. 154
5 . Mechanism of Pluronic -induced inhibition of P-gp in brain endothelial cells ............................................................................. 1555 .1. ATP depletion in the presence of Pluronic block copolymers ............................................................................................ 155
5 .2. Membrane interactions of Pluronic and inhibition of P-gp ATPase activity......................................................................... 1566 . Optimization of Pluronic compositions for P-gp inhibition in brain endothelial cells .................................................................. 157
7 . Effects of Pluronic on drug transport across BBB: in vitro and in vivo evaluation ...................................................................... 1588 . Toxicological considerations of Pluronic block copolymers ...................................................................................................... 160
9 . Conclusion.............................................................................................................................................................................. 161Acknowledgements ...................................................................................................................................................................... 161References .................................................................................................................................................................................. 161
*Corresponding author. Tel.: 11-402-559-9364; fax: 11-402-559-9543.E-mail address: [email protected] (A.V. Kabanov).
0169-409X/02/$ – see front matter 2002 Elsevier Science B.V. All rights reserved.PI I : S0169-409X( 02 )00176-X

Cell-mediated drug transport across the blood–brain barrier
pharmacy.sites.unc.edu/
troy-movie.stasi.co.uk
Macrophages and monocytes/neutrophils are phagocytic and have a tendency to endocytose colloidal materials, for example, nano or microparticles, liposomes and subsequent exo- cytosis to release drug and/or colloidal materials to external media. A high payload of drug can be incorporated/loaded into nanocar- riers or microcarriers, then taken up by Trojan horse cells .

Thanks All for a Patient Ear
kinetophil.tripod.com/ moraxella.deviantart.com/
![Bimodal Gastroretentive Drug Delivery Systems of ......a gastroretentive floating drug delivery system[12]. The drug concentrations can be controlled by formulating bimodal drug delivery](https://static.fdocuments.in/doc/165x107/5e6f0293269d113bd9170da6/bimodal-gastroretentive-drug-delivery-systems-of-a-gastroretentive-floating.jpg)