drogas, dependencia quimica, ibogaina,
16
——Chapter 4—— DRUG DISCRIMINATION STUDIES WITH IBOGAINE Scott Helsley 1 , Richard A. Rabin, 2 And J. C. Winter 2 1 Department of Anesthesiology Duke University Medical Center Durham, NC 27710 2 Department of Pharmacology and Toxicology SUNY Buffalo Buffalo, New York 14214 I. Introduction.................................................................................................................. II. Ibogaine in Drug Discrimination Studies .................................................................... A. Ibogaine as a Discriminative Stimulus .................................................................. B. Serotonergic Agents in Ibogaine-Trained Rats ...................................................... C. Beta-carboline Agents in Ibogaine-Trained Rats................................................... D. Tryptaminergic Hallucinogens in Ibogaine-Trained Rats ..................................... E. NMDA Antagonists in Ibogaine-Trained Rats ...................................................... F. Opioids in Ibogaine-Trained Subjects ................................................................... G. Sigma Ligands in Ibogaine-Trained Rats .............................................................. H. Noribogaine............................................................................................................ III. Summary ...................................................................................................................... References .................................................................................................................... I. Introduction Drug discrimination is a useful technique in the search for the mechanism of action of psychotropic drugs. Perhaps its utility has been best demonstrated in efforts to elucidate those neurotransmitter receptors involved in the mediation of the perceptual effects of phenethylamine (DOM) and indoleamine (LSD) hallucinogens (1). As far as biological assays of pharmacological activity are concerned, drug discrimination is relatively easy to understand. Specifically, the goal of such THE ALKALOIDS, Vol.56 Copyright © 2001 by Academic Press 0099-9598/01 $35.00 All rights of reproduction in any form reserved 63
-
Upload
dra-cleuza-canan -
Category
Health & Medicine
-
view
251 -
download
2
description
Dependencia química / Ibogaina Tratamento de drogas O atual momento da ibogaína merece uma tomada de consciência e um grande senso de responsabilidade das pessoas... Estão aparecendo a cada dia novas pseudo-clínicas, todas alardeando uma experiência e um conhecimento que não possuem, buscando atrair os incautos pacientes e familiares que, desesperados, tentam qualquer coisa sem pensar direito no que estão fazendo. Como sempre dizemos, o tratamento com ibogaína é um procedimento que não é isento de riscos, deve ser feito em ambiente médico-hospitalar, com o paciente internado, para ser protegido e monitorado. O paciente deve estar limpo de drogas e de remédios por um tempo variável, de acordo com cada situação individual, e deve ser submetido a uma bateria de exames antes do procedimento. E a medicação utilizada, deve ser GMP, ou seja, fabricada segundo as boas práticas farmacêuticas. Não confie em locais que usam, como diferencial para fazer propaganda, o argumento de que não é necessária internação, nem exames e nem abstinência prévia. Pelo menos 60 dias de internação são necessárias sim, para inclusive proteger o paciente de qualquer evento adverso . Não confie em locais e sites que dão a entender que a ibogaína é a "cura" da dependência química, isso é simplificar demais um problema sério. Desde que se descobriram os efeitos anti-dependência da ibogaína, em 1962, ocorreram cerca de 20.000 tratamentos em todo o mundo. Nestes 20.000 tratamentos, ocorreram 19 mortes, todas relacionadas a problemas de saúde prévios ( que teriam sido detectados se o paciente tivesse feito um check-up antes do procedimento) e também a uso de drogas muito perto do uso da ibogaína ( o que teria sido evitado se o paciente estivesse sob vigilância especializada). Então, não confie em pessoas que menosprezam o poder da substância, que não entendem do assunto e visam apenas lucro. Não confie tambem em locais que indicam a ibogaína como uma panacéia, que cura tudo, desde a dependência até queda de cabelo. Claramente, isso é uma tentativa de angariar mais pacientes e aumentar os lucros. Mesmo sendo derivada de uma planta, certos cuidados devem ser tomados. Não é toda medicação derivada de plantas que é "tranquila" ou "fraquinha", quem fala isso demonstra que não entende do assunto. A ibogaína é muito eficiente, principalmente se comparada aos outros tratamentos disponíveis, mas para atingir bons resultados, é necessária uma expertise que alguns locais que fazem propaganda disseminada não possuem. Apenas a título de informação, aqui está o link para um trabalho científico comentando essas mortes às quais me referi. Observe como no texto é dito que esses casos todos foram de pacientes com problemas de saúde prévios, usando medicação de origem desconhecida.
Transcript of drogas, dependencia quimica, ibogaina,

——Chapter 4——
DRUG DISCRIMINATION STUDIESWITH IBOGAINE
Scott Helsley1, Richard A. Rabin,2
And J. C. Winter2
1Department of AnesthesiologyDuke University Medical Center
Durham, NC 27710
2Department of Pharmacology and ToxicologySUNY Buffalo
Buffalo, New York 14214
I. Introduction..................................................................................................................II. Ibogaine in Drug Discrimination Studies ....................................................................
A. Ibogaine as a Discriminative Stimulus ..................................................................B. Serotonergic Agents in Ibogaine-Trained Rats......................................................C. Beta-carboline Agents in Ibogaine-Trained Rats...................................................D. Tryptaminergic Hallucinogens in Ibogaine-Trained Rats .....................................E. NMDA Antagonists in Ibogaine-Trained Rats ......................................................F. Opioids in Ibogaine-Trained Subjects ...................................................................G. Sigma Ligands in Ibogaine-Trained Rats ..............................................................H. Noribogaine............................................................................................................
III. Summary ......................................................................................................................References....................................................................................................................
I. Introduction
Drug discrimination is a useful technique in the search for the mechanism ofaction of psychotropic drugs. Perhaps its utility has been best demonstrated inefforts to elucidate those neurotransmitter receptors involved in the mediation ofthe perceptual effects of phenethylamine (DOM) and indoleamine (LSD)hallucinogens (1).
As far as biological assays of pharmacological activity are concerned, drugdiscrimination is relatively easy to understand. Specifically, the goal of such
THE ALKALOIDS, Vol.56 Copyright © 2001 by Academic Press0099-9598/01 $35.00 All rights of reproduction in any form reserved63

studies is to produce drug-induced stimulus control. This condition is said to existwhen, in the presence of a stimulus, an animal subject emits a conditionedresponse (2). An example of a conditioned response might be pressing a specificlever when presented with a two-lever choice, or entering a specific arm of a two-arm maze (T-maze). The stimulus (or discriminative stimulus) is the interoceptivestate produced by the drug used to establish stimulus control. To illustrate this byway of example, assume that one wishes to establish stimulus control with drugX. The discriminative stimulus will be the interoceptive cue, which is simply theeffect experienced by the subject after receiving drug X. In this case the subjectis a rat. However, pigeons, other rodents, and primates can also be used. Thesubject, over several weeks, has been taught to press levers in a two-lever operantchamber for a food reward in a process known as shaping. During this process,the ratio of response to reward is gradually increased from 1 to 10 or more. Sincea certain fixed number of responses is required for a reward, this is known as afixed ratio schedule of reinforcement. If 10 responses are required for a reward,then a fixed ratio of 10 (FR 10) is the schedule. Once the rat has mastered this, itis time to establish stimulus control.
In order to accomplish this, the rat is trained with once daily sessions, whichalternate between drug and vehicle treatment. Thus, using a specific pretreatmenttime (e.g., 15 minutes prior to the session), the training drug (drug X) or itsvehicle are given on alternating days. On days when drug X is given, onlyresponses on one lever (left or right) are rewarded. On vehicle days, onlyresponses on the other lever are rewarded. After a number of sessions the subjectwill learn to press the drug appropriate lever only on those days when that drugis administered. On vehicle days, the subject should only respond on the vehicle-appropriate lever. Once the subject is responding reliably in a treatment-appropriate manner, stimulus control is said to be present. Having establishedstimulus control in a given subject investigations can begin regarding the receptorinteractions mediating the discriminative cue of drug X. Test drugs (drug Y) thatare known agonists or antagonists at certain receptors can be given during testsessions. If these produce responses on the drug X-appropriate lever, then the testdrug is said to substitute for the training drug, alternatively, by convention, thetraining drug stimulus is said to generalize to that of the test drug. Thisterminology is often reversed by some authors resulting in confusion on the partof the readers. If responding is on the vehicle-appropriate lever then nosubstitution or generalization is present. Often there is an intermediate degree ofsubstitution or generalization (partial generalization) suggesting that theinteroceptive cues are similar, but not identical. Another test is that ofantagonism. In these tests, a drug with known receptor binding properties is givenwith the training drug (e.g., drugs X and Y together). If responding is seen onlyon the vehicle appropriate-lever then drug Y has antagonized the interoceptivecue produced by drug X. Alternatively, responding on the drug X-appropriate
64 helsley et al.

lever would indicate absence of antagonism. During test sessions, rewards shouldnot be given and the session should be terminated after a fixed number ofresponses. This is to minimize learning during the test session, which mightconfuse the subjects. Furthermore, the subjects should only be tested every thirdor fourth day (after they have demonstrated reliable treatment appropriateresponding in the prior two or three training sessions). Training doses, test doses,and pretreatment times are usually based on reports of pharmacological effects ofthe drug in question found in the literature.
Drug discrimination is a remarkably simple, yet elegant, technique. Using thisparadigm, investigators can often gain insight into the mechanism of action of agiven agent. The results of these studies can then be correlated with other studies,such as receptor binding studies and second messenger assays.
Like other techniques, drug discrimination does have its shortcomings.Because the interoceptive cue is what is being evaluated, other drug effects andtheir specific mechanisms may not be accounted for. No technique is perfect.Nonetheless, for studying drugs with psychotropic effects, drug discriminationremains a powerful weapon in the arsenal of the behavioral pharmacologist.
II. Ibogaine in Drug Discrimination Studies
A. Ibogaine as a Discriminative Stimulus
Before there was any evidence supporting the antiaddictive effects of ibogaine,this agent was known first and foremost as a hallucinogen. Because of this, drugdiscrimination seems well suited to the study of ibogaine. Knowledge of thosereceptors involved in the ibogaine discriminative cue could contributesignificantly to our understanding of its mechanism of action, both as ahallucinogen and possibly as a therapy for substance abuse conditions.
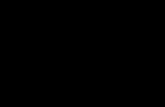
Figure 1a shows the dose-response effects ibogaine (�), harmaline (�), andnoribogaine (10-hydroxyibogamine) (�) in rats trained with 10.0 mg/kg ibogaineas a discriminative stimulus. All drugs were administered i.p. 60 minutes beforetesting. Each point represents one determination in each of 10 subjects unlessotherwise noted by the number of subjects completing the test over the numberof subjects tested. The ED50 for ibogaine was 4.6 mg/kg.
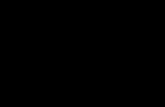
Figure 1b shows the time course for the ibogaine-trained stimulus. Maximalsubstitution was observed at a pretreatment time of 60 minutes (94%). Followingthis, a time-dependent decrease in ibogaine-appropriate responding wasobserved. (Modified from reference 3 with permission.)
654. drug discrimination studies with ibogaine

B. Serotonergic Agents in Ibogaine-Trained Rats
The structural similarity between ibogaine and serotonin taken together withthe fact that the 5-HT2A receptor is the primary mediator of the discriminativestimulus effects of the classical hallucinogens lysergic acid diethylamide (LSD)and (-)-2,5-dimethoxy-4-methyl-amphetamine (DOM) (4-6) makes serotonergicagents a natural starting point in the study of ibogaine.
Palumbo and Winter (7) were the first to look at ibogaine in drugdiscrimination studies. They found that ibogaine produced an intermediate levelof substitution in both LSD and DOM-trained subjects. This effect was blockedby the 5-HT2 antagonist pizotylene. The first report in which ibogaine was trainedas a discriminative stimulus was by Schecter and Gordon (8). These authorsobserved an intermediate level of substitution by the 5-HT releasing agentfenfluramine. This evidence suggested a possible role for serotonergic receptorsin the stimulus effects of ibogaine. Further investigations have revealed that the5-HT2A receptor plays a role, although this does not appear to be essential to theibogaine-induced discriminative stimulus. This is evidenced by the observation
66 helsley et al.
Figure 1a. Dose response for ibogaine �, harmaline �, and noribogaine (10-hydroxyibogamine) �.

that both DOM and LSD produced intermediate levels of substitution foribogaine that was blocked by the 5-HT2A antagonist pirenpirone (9). Theconclusion that this component is nonessential stems from the fact that whilepirenpirone blocked the ibogaine-appropriate responding produced by LSD andDOM, it did not affect the ibogaine-appropriate responding produced by ibogaineitself (9) (Figure 3). For a detailed discussion of nonessential stimuluscomponents, see reference 10.
A possible explanation for the differences in ibogaine-appropriate respondingproduced by LSD illustrated above, compared to the work of Schecter andGordon (34.5% substitution) (8), could be accounted for by rat strain differencesand/or pretreatment time differences for ibogaine training (60 minutes vs. 30
674. drug discrimination studies with ibogaine
Figure 1b. Ibogaine time course.

minutes, respectively).In addition to 5-HT2A receptors, there is evidence for the involvement of the
5-HT2C receptor. In contrast, the 5-HT1A and 5-HT3 subtypes do not appear toplay a major role in the ibogaine-mediated discriminative stimulus (11).Interestingly, the phenomenon observed with the 5-HT2A component is also seenwith the 5-HT2C component of the ibogaine cue. That is, involvement of the5-HT2C receptor in the ibogaine-trained discriminative stimulus appears to benonessential. As illustrated in Table I, the 5-HT2C agonists MK 212 and mCPPboth produced intermediate levels of substitution, which were blocked bymetergoline, an agent that has antagonist properties at 5-HT2C receptors. Incontrast, the ibogaine-appropriate responding produced by ibogaine itself was notaffected by mesulergine (10) or metergoline (11).
These studies have demonstrated a role for 5-HT2A and 5-HT2C receptors in theibogaine discriminative cue. A role for the 5-HT2A receptor is further supportedby biochemical studies, which provided evidence for in vivo occupancy of these
68 helsley et al.
Figure 2. The dose response relationships for pirenpirone (75 minutes presession) in the presence ofLSD (�), DOM (�), and ibogaine (�) in rats trained to discriminate ibogaine (10.0 mg/kg, i.p., 60minutes presession) from vehicle. The ratio adjacent to each of the points represents the number ofsubjects completing the test session over the number of subjects participating in each test session.From reference 9 with permission.

receptors by ibogaine (10). Although these receptor interactions are not essentialto the ibogaine stimulus, they provide a link between ibogaine and classicalhallucinogens such as LSD and DOM. This is further supported by a recent studyinvestigating the effects of monoamine reuptake inhibitors on the stimulus effectsof hallucinogens. Specifically, the DOM, LSD, and ibogaine discriminative cueswere all potentiated by the monoamine reuptake inhibitors fluoxetine,venlafaxine, and fluvoxamine (12). The exact mechanism for this is unknown atpresent. Certainly, further insights into this area of study will enhance ourknowledge both of hallucinogens and of antidepressant medications, which arecommonplace in psychiatric practice.
C. Beta-Carboline Agents In Ibogaine-Trained Rats
694. drug discrimination studies with ibogaine
TABLE I.
% ibogaine-appropriate RateDrug treatment Responses (Responses/min) n/N
Ibogaine 94.0 14.3 10/10Ibogaine (10 mg/kg) + 100.0 36.4 4/4Metergoline (1.0 mg/kg)MK 212 (0.3 mg/kg) + 10.0 16.1 7/8Metergoline (1.0 mg/kg)** [79.6]*mCPP (0.8 mg/kg) 23.8 13.0 6/8Metergoline (1.0 mg/kg)** [76.4]*
The ratio n/N represents the number of animals responding (n) out of the number of animals tested (N). The %ibogaine-appropriate responding produced by both mCPP and MK-212 alone is enclosed in brackets. Treatmentsessions were compared to immediately preceding ibogaine training sessions using Wilcoxon’s signed ranks test.
*Reflects significant differences from the ibogaine-treatment condition (p<0.05).**Reflects significant differences between the drug alone and the drug + antagonist conditions as determined by
the Mann-Whitney Rank Sum test. Modified from reference 11 with permission.

One group of hallucinogens that has received little attention is the beta-carboline (or Harmala) alkaloids group. Interestingly, these agents bear a strongstructural resemblance to ibogaine. Anecdotal reports suggest that thetremorigenic and subjective effects of agents, such as harmaline and harmine, arenot unlike those of ibogaine (13). Several of these alkaloids were tested inibogaine-trained rats (10). The results are shown in Figure 3. Full generalizationwas observed with 6-methoxyharmalan and harmaline, while partialgeneralization was seen with harmine, harmane, harmalol, and THBC(tetrahydro-beta-carboline). No generalization was seen to 6,7-dimethoxy-4-ethyl-β-carboline-3-carboxylate (DMCM) or norharmane.
Unfortunately, the mechanism of action of the harmala alkaloids remainsunknown. However, this is not the case for other beta-carbolines like DMCM.This agent has inverse agonist properties at benzodiazepine sites (14). We found
70 helsley et al.
Figure 3. Dose-response relationships for beta-carbolines in rats trained with 10.0 mg/kg ibogaineas a discriminative stimulus. All agents were administered i.p., 60 minutes presession. The ratioadjacent to each of the points is the number of subjects completing the test session over the numberof subjects participating in each test session. Where no ratio is shown, a ratio of 8/8 is implied.Modified from reference 19 with permission.

it interesting that the iboga alkaloid, tabernanthine, is reported to havebenzodiazepine inverse agonist effects in rats (15). Nonetheless, as shown above,ibogaine itself did not generalize to DMCM. Likewise, in vitro work by Deecherand colleagues (16) showed ibogaine, as well as harmaline, to be without effecton GABA-stimulated chloride uptake in the mouse brain.
The results of these studies with beta carbolines have implications regardingthe potential antiaddictive effects of ibogaine. In morphine self-administrationstudies, Glick et al. (17) showed that, unlike ibogaine, harmaline did not producea sustained decrease in morphine consumption by rats. If the self-administrationparadigm used by these researchers is an accurate model of substance abuse inhumans, then it appears that mimicry of the ibogaine discriminative stimulus isnot effective in predicting antiaddictive activity in light of the fact that harmalinefully mimics ibogaine (3). Furthermore, norharmane, an agent that did notsubstitute for ibogaine in the present study, attenuates naloxone-precipitatedwithdrawal from morphine, as does ibogaine (18). For further information on theeffects of beta carbolines in ibogaine-trained subjects, see reference 19.
Interestingly, recent work by Grella and colleagues (20) shows significantharmaline-appropriate responding by the hallucinogen DOM (76%). Theseobservations, taken together with our findings (10), support a role for the 5-HT2A
receptor subtype in the stimulus effects of ibogaine and harmaline.
714. drug discrimination studies with ibogaine
Figure 4. Dose response relationships for DMT and MDMT in rats trained with ibogaine. Note that* refers to statistically significant difference from vehicle condition (p<0.05) (Helsley, et al.,previously unpublished data).

D. Tryptamine Hallucinogens in Ibogaine-Trained Rats
The tryptamines form another subgroup of indoleamine hallucinogens. Asshown in Figure 4, these agents appear to be less like ibogaine in terms of thestimulus cues compared to the beta-carboline, indoleamine, and phenethylaminehallucinogens, although weak partial generalization is seen with MDMT. Apossible explanation for this finding lies in the observation that the stimuluseffects of the tryptaminergic hallucinogen MDMT are mediated chiefly throughinteractions with 5-HT1A receptors (21, 22). These receptors do not appear to beinvolved in the ibogaine stimulus (11).
Figure 4 also shows dose response relationships for DMT and MDMT in ratstrained with ibogaine (10 mg/kg) as a discriminative stimulus. All agents wereadministered i.p., 15 minutes presession. The ratio adjacent to each of the pointsis the number of subjects completing the test session over the number of subjectsparticipating in each test session. Also next to each point is the response rate inresponses per minute.
E. NMDA Antagonists in Ibogaine-Trained Subjects
NMDA antagonists are often classified as hallucinogens because of theirpsychotomimetic effects. These agents occupy a binding site within a calciumchannel; in so doing they occlude the channel. This calcium channel is normallygated by the excitatory neurotransmitter glutamate (for review of NMDAantagonists, see reference 23). The best known of these agents is phencyclidine(angel dust, PCP). This agent was originally marketed as an anesthetic agent, butit was quickly removed from the market because of extreme psychotic reactions.Interestingly, ketamine, another NMDA antagonist, is still used today as ananesthetic. Emergence reactions are significantly milder than those seen withphencyclidine and are usually easily controlled with benzodiazepines.
A possible role for ibogaine acting at NMDA receptors is supported by theobservation that ibogaine has appreciable affinity for this binding site (24,25).Popik and associates investigated the effects of ibogaine on MK 801(dizocilpine)-trained mice in a T-maze. These authors observed approximately70% dizocilpine-appropriate responding at an ibogaine dose of 100 mg/kg (26).Subsequent studies suggest that this interaction does not play a major role in thestimulus effects of ibogaine at lower doses, as neither phencyclidine nor MK 801produced significant substitution in ibogaine-trained subjects (27).Correspondingly, ibogaine failed to substitute for phencyclidine in phencylidine-trained rats and monkeys (28) and MK 801-trained rats (29). The most plausibleexplanation for the contrast between these results and those of Popik, et al. wouldbe dose and species differences.
72 helsley et al.

F. Opioids in Ibogaine-Trained Subjects
Ibogaine’s effects on addiction and withdrawal phenomena naturally lead toquestions regarding its effects on opiate systems. The results of drugdiscrimination studies with opioids in ibogaine-trained subjects are quiteinteresting. Specifically neither mu- nor kappa-agonists substituted for ibogaine.No substitution, but weak partial antagonism, was seen with the pure antagonistnaloxone. An intermediate level of substitution, but no significant antagonism,was observed with naltrexone (55.6%) (27). Also, in rats trained with the kappa-agonist U50,488, no substitution was seen with ibogaine (29). However,significant generalization (60-70%) was observed with the mixedagonist/antagonist compounds pentazocine, diprenorphine, and nalorphine (27).
Interestingly, the intermediate substitution produced by diprenorphine andnalorphine was antagonized by naloxone (27). Although the implications of these
734. drug discrimination studies with ibogaine
Figure 5. The dose response relationships for s ligands in rats trained to discriminate ibogaine (10.0mg/kg, i.p., 60 minutes presession) from water. All agents were administered i.p., 30 minutespresession. The ratio adjacent to each of the points represents the number of subjects completing thetest session over the number of subjects participating in each test session. Taken from reference 27with permission.

results are not clear, they do suggest a role for opiate receptors in the mechanismof action of ibogaine. Further studies will be necessary to clarify this.
G. Sigma Ligands in Ibogaine-Trained Rats
In keeping with its unusual pharmacological profile, ibogaine has appreciableaffinity for sigma (σ) receptors of the σ2 subtype (30,31). Sigma receptors are arelatively new discovery, and hence, compared to other receptors, little is knownabout them. Thus, we are only beginning to characterize pharmacological agentsas agonists or antagonists at these receptors. Nonetheless, ibogaine appearsrelatively selective for the σ2 subtype. Several sigma ligands were tested inibogaine-trained rats, and it was observed that nonselective sigma ligands (DTG,(+)-3-PPP) produced intermediate levels of substitution (Figure 5), while the σ1
selective agents (+)-SKF 10,047 and (+)-pentazocine failed to substitute (27).Unfortunately no σ2-selective agents were available at the time of these
studies. Because we are still in the early stages in the study of the pharmacologyof these receptors, all that can be concluded from these studies is that sigmareceptors of the σ2 subtype play a role in the ibogaine discriminative stimulus. Asmore selective sigma ligands are discovered, the exact role of these receptors inibogaine’s mechanism of action will hopefully become more clear.
H. Noribogaine
In radioligand binding assays, ibogaine shows remarkably low affinity for mostknown receptors (micromolar vs. nanomolar) (32). This, taken together with theobservation that ibogaine’s pharmacological activity is relatively long lived,suggests the possibility that a long-acting metabolite may mediate many ofibogaine’s pharmacological effects; noribogaine (10-hydroxyibogamine) isthought to be such an agent (33).
10-Hydroxyibogamine appears to be similar to ibogaine in its stimulusproperties, but it does not substitute completely for the parent compound, asillustrated in Figure 1 (3). Zubaran and colleagues (29) observed similar results.These authors also looked at brain levels of ibogaine and its metabolite.Interestingly, they found the metabolite to be more potent than the parentcompound in eliciting ibogaine-appropriate responding with ED50 values of 1.98and 4.51 mg/kg, respectively. Brain levels of noribogaine were similar atbehaviorally equi-effective doses of both agents (1.11 µg/g after administration ofthe ED50 of 10-hydroxyibogamine and 1.23 µg/g after the ED50 of ibogaine).These results suggest that the stimulus effects of ibogaine are mediated mainly by10-hydroxyibogamine (29). Further studies will be necessary to confirm this.
74 helsley et al.

III. Summary
The results of the studies described here support the hypothesis that ibogaineproduces its effects via selective interactions with multiple receptors. It appearsthat 5-HT2A, 5-HT2C, and σ2 receptors are involved in mediating the stimuluseffects of ibogaine. In addition, opiate receptors may also be involved. Incontrast, σ1, PCP/MK-801, 5-HT3, and 5-HT1A receptors do not appear to play amajor role.
Ibogaine’s hallucinogenic effects may be explained by its interactions with5-HT2A and 5-HT2C receptors, while its putative antiaddictive properties mayresult from its interactions with σ2 and opiate receptors. Alternatively, thepossibility that ibogaine’s hallucinogenic properties underlie its antiaddictiveeffects, as previously suggested (34), would support a role for 5-HT2 receptors inmediating the reported therapeutic effects of ibogaine.
Certainly many questions remain regarding ibogaine’s mechanism of action.Although drug discrimination will be useful for answering some of thosequestions, the true potential of this technique is realized when it is combined withother techniques. The next few years promise to be fruitful with respect to ourunderstanding of this agent. Reasons supporting this belief include advances inthe study of sigma receptors, interest in ibogaine’s effects on second messengersystems, and the development of ibogaine congeners such as 18-methoxycoro-naridine (35).
In conclusion, the aforementioned studies should serve to guide furtherendeavors. Pertinent questions have been generated: What is the role of sigmareceptors in the effects of ibogaine, especially with regard to addiction? Howdoes ibogaine affect opiate neurotransmission? What effects, if any, do theHarmala alkaloids have on addiction phenomena? What is the mechanism ofaction of harmaline? Can 10-hydroxyibogamine serve as a discriminativestimulus and, if so, what receptor interactions mediate its stimulus effects? Doesthe ibogaine-trained stimulus generalize to novel agents, including 18-methoxy-coronaridine?
Acknowledgments
These studies were supported, in part, by U.S. Public Health service grant DA 03385 [JCW, RAR],by National Research Service Award DA 05735 [SH], and by a grant from Schering-Plough ResearchInstitute [SH]. We thank Ms. Deborah Timineri for her technical assistance.
754. drug discrimination studies with ibogaine

References
1. J.C. Winter, NIDA Res. Monograph 146, 157 (1994).2. R.T. Kelleher and L.H. Morse, in "Reviews of Physiology, Biochemistry, and Behavior,"
Volume 60, pp. 2-56. Springer-Verlag, New York, 1968.3. S. Helsley, R.A.Rabin, and J.C. Winter, Life Sci. 60, PL147 (1997).4. D. Fiorella, R.A. Rabin, and J.C. Winter, Psychopharmacology 121, 347 (1995).5. D. Fiorella, R.A. Rabin, and J.C. Winter, Psychopharmacology 121, 357 (1995).6. D. Fiorella, S. Helsley, D.S. Lorrain, R.A. Rabin, and J.C. Winter, Psychopharmacology 121,
364 (1995).7. P.A. Palumbo and J.C. Winter, Pharmacol. Biochem. Behav. 43, 1221 (1992).8. M.D. Schechter and T.L. Gordon, Eur. J. Pharmacol. 249, 79 (1993).9. S. Helsley, D. Fiorella, R.A. Rabin, and J.C. Winter, Pharmacol. Biochem. Behav. 59, 419
(1998).10. J.C. Winter, Pharmacol. Biochem. Behav. 20, 201 (1984).11. S. Helsley, R.A. Rabin, and J.C. Winter, Prog. Neuro-Psychopharmacol. Biol. Psych. 23, 317
(1999).12. J.C. Winter, S. Helsley, D. Fiorella, and R.A. Rabin, Pharmacol. Biochem. Behav. 63, 507
(1999).13. C. Naranjo, Clin. Toxicol. 2, 209 (1969).14. E.N. Petersen, Eur. J. Pharmacol. 94, 117 (1983).15. J.-H. Trouvin, P. Jacqmin, C. Rouch, M. Lesne, and C. Jacquot, Eur. J. Pharmacol. 140, 303
(1987).16. D.C. Deecher, M. Teitler, D.M. Soderlund, W.G. Bornmann, M.E. Kuehne, and S.D. Glick,
Brain Res. 571, 242 (1992).17. S.D. Glick, M.E. Kuehne, J. Raucci, T.E. Wilson, D. Larson, R.W. Keller, Jr., and J.N. Carlson,
Brain Res. 657, 14 (1994).18. S.L.T. Cappendijk, D. Fekkes, and M.R. Dzoljic, Behav. Brain Res. 65, 117 (1994).19. S. Helsley, R.A. Rabin, and J.C. Winter, Eur. J. Pharmacol. 345,139 (1998).20. B. Grella, M. Dukat, R. Young, M. Teitler, K. Herrick-Davis, C.B. Gauthier, and R.A.
Glennon, Drug Alc. Dep. 50, 99 (1998).21. D.G. Spencer, T. Glaser, and J. Traber, Psychopharmacology 93, 158 (1987).22. J.C. Winter, R.A. Fillipink, D.M. Timineri, S. Helsley, and R.A. Rabin, Pharmacol. Biochem.
Behav. 65, 75 (2000).23. J. Willetts, R.L. Balster, and J.D. Leander, Trends Pharmacol. Sci. 11, 423 (1990).24. P. Popik, R.T. Layer, and P. Skolnick, Psychopharmacology 114, 672 (1994).25. R.T. Layer, P. Skolnick, C.M. Bertha, U.K. Bandarage, M.E. Kuehne, and P. Popik, Eur. J.
Pharmacol. 309, 159 (1996).26. P. Popik, R.T. Layer, L.H. Fossom, M. Benveniste, B. Geter-Douglass, J.M. Witkin, and P.
Skolnick, J. Pharmacol. Exp. Ther. 275, 753 (1995).27. S. Helsley, R. Filipink, W.D. Bowen, R.A. Rabin, and J.C. Winter, Pharmacol. Biochem.
Behav. 59, 495 (1998).28. H.E. Jones, H. Li, and R. Balster, Pharmacol. Biochem. Behav. 59, 413 (1998).29. Zubaran, M. Shoaib, I.P. Stolerman, J. Pablo, and D.C. Mash, Neuropsychopharmacol. 21, 119
(1999).30. R.H. Mach, C.R. Smith, and S.R. Childers, Life Sci. 57, PL 57 (1995).31. W.D. Bowen, B.J. Vilner, W. Williams, C.M. Bertha, M.E. Kuehne, and A.E. Jacobson, Eur. J.
Pharmacol. 279, R1 (1995).32. P.M. Sweetnam, J. Lancaster, A. Snowman, J.L. Collins, S. Perschke, C. Bauer, and J. Ferkany,
Psychopharmacology 118, 369 (1995).33. D.C. Mash, J.K. Staley, M.H. Baumann, R.B. Rothman, and W.L. Hearn, Life Sci. 57, PL 45
76 helsley et al.

(1995).34. J.H. Halpern, Addiction Res. 4,177 (1996).35. S.D. Glick, M.E. Kuehne, I.M. Maisonneuve, U.K. Bandarage, and H.H. Molinari, Brain Res.
719, 29 (1996).
774. drug discrimination studies with ibogaine