
Drainage Implant Surgery
25
Drainage Implant Surgery In an attempt to maintain patency of a drainage fistula in glaucoma filtering op erations , a wide va riety of forei gn ma te rials have be en impl anted in th e eye, exte ndin g from th e anteri or chamber to a subconjunctival space. These were once referred to as s e t o n s , because the implants consisted of solid structures, such as threads, wires, or hairs, that were placed in a wound to form a drainage, permitting aqueous to run alongside the surface of the inserted material. These p r oc e d u r es we r e u n i fo r m l y u n s u cc e ssf u l i n m ai n t a i n i n g a p a t e n t f is t u l a . Newe r de v i c es u se t u b es t h a t d r a i n a q u eo u s o u t of t h e e ye in t o p os t e r i o r l y p l a c e d ex t e r n a l r ese r v oi r s a n d h a ve b e e n s h ow n t o h a ve clinical benefit. This chapter reviews the more commonly used drainage impl ant devices, the surgica l techniques o f implantati on, the complications and their management, and the comparative merits and indications for this group of glaucoma surgical procedures. PATHOPHYSIOLOGY OF DRAINAGE IMPLANTS All modern drainage implant devices have the same basic design, which typically consists of a silicone tube that extends from the anterior chamber or, in some cases, the vitreous cavity! to a plate, disc, or encircling element beneath conjunctiva and Tenon"s capsule. The edge of the external plate has a ridge, through which the distal end of the tube inserts onto the upper surface of the plate. The ridge decreases the ris# of obst ru ct ion of the posterior opening of the tube with the surrounding tissue and fibrous capsule. The plates of the glaucoma drainage devices have large surface areas and promote the formation of the filtering bleb posteriorly, near the equator. The mechanism by which drai nage impl ant devi ces cont ro l the intraocular pressure I$%! relates to a fibrous capsule that forms a filtering bleb around the external portion of the draining device. The morphology of this filtering bleb appears to be different from that of the blebs seen after trabecule ctomy. After insertion of the drai nage device, a thin coll agenous capsule, surrounded by a granulomatous reaction, is present at & month. The granulomatous reaction resolves after ' months, capsule thic#ness re mains re lati ve ly stable, and the coll agen st ro ma becomes less compact. The fibrous capsule matures over time and becomes thinner after ( months in rabbit eyes &!. Although the bleb histology in the rabbit mo del is similar to that of hu mans and other pri mates, the eventual development of a fibroblastic inner lining in the rabbit model differs from that in humans, in whom the inner lining remains only as a meshwor# of collagen)li#e bundles at some areas of the inner bleb wall &,*!. +ven though the filtering bleb around the implant is l ined with a thic# layer of connective tissue, microcystic spaces within that layer, seen on light and electron microscopy, may serve as the channels for aqueous drai nage * !. tudies of mon#ey eyes wi th si ngle)p late -olteno implants indicat e th at th e caps ule functions by a passive mechanism, shunting the flow of aqueous humor to the surrounding
-
Upload
hendy-chrisandy -
Category
Documents
-
view
215 -
download
0
Transcript of Drainage Implant Surgery

7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 1/25
Drainage Implant Surgery
In an a t tempt to mainta in patency of a drainage f is tula in glaucomafi lter ing operat ions, a wide var iety of fore ign mater ials have beenimp lanted in the eye , extending f rom the anter io r chamber to a
subconjunctival space. These were once referred to as setons , becausethe implants consis ted of solid s tructures , such as threads , wires , or ha i rs , tha t were p laced in a wound to form a dra inage , pe rmit t ingaqueous to run a longside the surface of the inserted materia l . These
procedures were uniformly unsuccessful in maintaining a patent fistula. Newer devices use tubes that drain aqueous out of the eye into posteriorly placed external reservoirs and have been shown to haveclinical benefit. This chapter reviews the more commonly used drainagei mp la nt d ev ic es , t he s ur gi cal t ech ni que s of i mp la nt at io n, t hecomplications and their management, and the comparative merits andindications for this group of glaucoma surgical procedures.
PATHOPHYSIOLOGY OF DRAINAGE IMPLANTS
All modern drainage implant devices have the same basic design, whichtypica l ly cons is ts o f a s i l icone tube tha t ex tends f rom the an te r ior chamber or, in some cases , the vi treous cavity! to a pla te , d isc , or encircling element beneath conjunctiva and Tenon"s capsule. The edgeof the external pla te has a r idge, through which the dis ta l end of thetube inserts onto the upper surface of the plate. The ridge decreases ther is# o f obs truc tion o f the pos te rior opening o f the tube with thesurrounding t issue and fibrous capsule . The pla tes of the glaucomadrainage devices have large surface areas and promote the formation of the filtering bleb posteriorly, near the equator.The mechani sm by which d ra inage imp lant dev ices con trol theintraocular pressure I$%! re la tes to a f ibrous capsule that forms afiltering bleb around the external portion of the draining device. Themorphology of this filtering bleb appears to be different from that of the blebs seen after trabecule ctomy.
After insert ion of the drainage device, a thin collagenous capsule ,surrounded by a granulomatous reaction, is present a t & month. Thegranulomatous reaction resolves after ' months , capsule thic#ness
remains relat ively s table, and the col lagen s troma becomes l es scompact. The fibrous capsule matures over time and becomes thinner after ( months in rabbit eyes &!. Although the bleb his tology in therabbi t model i s s imi lar to that o f humans and o ther p r imates, theeventual development of a fibroblastic inner lining in the rabbit modeldiffers from that in humans, in whom the inner lining remains only as ameshwor# of collagen)li#e bundles at some areas of the inner bleb wall&,*!. +ven though the filtering bleb around the implant is l ined with athic# layer of connective tissue, microcystic spaces within that layer,seen on light and electron microscopy, may serve as the channels for aqueous d ra inage *! . tudies o f mon#ey eyes with s ingle)plate
-olteno implants ind ica te tha t the capsu le func t ions by a pass ivemechanism, shunting the f low of aqueous humor to the surrounding

7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 2/25
orbita l t issues !. All surfaces of the f ibrous capsule contribute tofiltration, which is consistent with echographic studies in human eyesthat reveal bleb formation on both sides of the plate in successful cases'!. /istopathologic studies of human eyes enucleated * to ( years after -olteno implant surgery revealed patent tubes with no appreciable
anterior chamber reaction and minimal inflammatory reaction in theouter layers of the bleb wall 0!.-easurement of the flow resistance using modified 1aerveldt plates inrabbits showed a direct re la t ionship between the surface area of theimplants and the filtering capacity of their surrounding capsule (!. Atthe same time, reduction of the bleb diameter decreases surface tensionon the b leb, capsu lar f ibros is, and th ic#ness, which increases theeffectiveness of the filtering surface 2,3!.4rainage devices with open tubes are li#ely to be complicated by early
postoperative hyp otony and therefore should be temporarily closed witha ligature or stent. 5p to 367 of eyes with temporary tube closure or a
valved device may exhibit a hypertensive phase 8! from & to * wee#sto ( months postoperatively &6!.The fa i lure of the f i l tering bleb after surgery may occur due to theincreased thic#ness of f ibrous capsule around the drainage implant .-ovement of the drainage plate against the scleral surface may be themechanism of glaucoma implant failure resulting from the stimulationof the low)level%.(&&
wound hea l ing response , increased col lagen scar format ion , andincreased fibrous capsule thic#ness &&!.
IMPLANT DESIGNS
%er fo rmance o f s imilar d ra inage dev ices can vary s igni fi cant ly,depending on the standards in manufacturing. This causes a wide rangeof clinical outcomes and indicates a strong need for enhanced qualitycontro l p rocedures in the device manufacturing process &*! . Theglaucoma drainage devices also differ according to the si9e, shape, andm at er ia ls f ro m w hi ch t he e xt er nal c omp on en t an d t he t ub e a reconstructed. +xternal portions of glaucoma drainage devices are madefrom materials that prevent fibroblast adherence. 4ifferent materialsmay influence the amount of in flammat ion in surrounding t i ssues.
%olypropylene, used in Ahmed and -olteno implants, appears to causemore inflammation than silicone that is used in 1aerveldt and :rupinimplan ts . ; lex ib le p lates appeared to cause less inf lammat ion insubconjunctival space of rabbit eyes than the rigid ones &,&'!.Al te rna tive mater ials , such as hydroxylapa ti te &0! and expanded
polytetrafluoroethyl ene e%T;+! &(,&2!, which increasevasculari9at ion of the f ibrous capsule around the pla te , may offer atheoretical advantage by enhancing the efficacy, decreasing the capsulesi9e, and increasing the functional lifetime of the implant &0!.$ne of the most fundamental design differences, however, is whether the device has an open, unobstructed drainage tube or one that contains
a pressure)regulating valve. 1aerveldt, -olteno, and choc#et implantsare the examples of open tube implants . Ahmed and :rupin implants

7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 3/25
are designed to have a flow)restricting valve mechanism.OPEN TUBE DRAINAGE DEVICES
Baervelt Implant
The unique fea tu re o f thi s s er ie s o f popular nonva lved d ra inageimplants is the large surface area of the plates, which are designed in
such a way that they can be easi ly implanted through a one)quadrantconjunctival incis ion. A s i l icone tube is a t tached to a soft barium)impregnated silicone plate ;ig. '&.&! with a surface area of *06 mm *
*6 <= & mm!, 06 mm * * <= &' mm!, or 066 mm * ( <= &2.0mm! &3!. The 06 mm * implant is currently a preferred si9e, in that itappears to be safer and s l ight ly more e ffec tive than the 066)mm *
implant.
Figure !"#"# 1aerveldt implant.
The plate is positioned under the rectus muscle insertions, typically inthe superotempora l quadrant ; ig . '&.*! . The 1aerveldt p late hasfenest rat ions tha t a l low growth of f ibrous t i ssue th rough the p la teserving to reduce the height of the bleb and secure the implant in place&8!. A fibrous capsule forms after the first to ( postoperative wee#sinto which fluid can drain and from which fluid can be absorbed by thesurrounding tissues.

7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 4/25
Figure !"#$# 1aerveldt implant is positioned under the superior and temporalrectus muscles.
In terms of I$% control, a 06)mm* 1aerveldt implant was found to becomparable with the double)plate -olteno implant discussed next! in
patients with uncontrolled, complicated glaucoma *6!. In an &3)months prospective s tudy, the 06 mm * implan t was shown to havesimilar rate of success but lower ris# of complication than the 066)mm *
m od el &8 !. I n o ne r et ro sp ec ti ve s tu dy, t he 06 )mm * implantmainta ined I$% below *& mm /g in 327 of the eyes , compared with267 with the 066)mm * implant after years *&!. The success ra tedeclined to 287 in the 06)mm * g roup and to ((7 in the 066)mm *
group after 0 years . >omplicat ions ra te was comparable between thetwo groups, but occurred s l ightly more often in the 066)mm * group*&!.M%lten% Implant
This is the prototype drainage implant device and has had the longestand mos t extensive c lin ical exper ience s ince i t was in troduced by-olteno in &8(8 **!. The original design consists of a single plate of th in ac ry l ic wi th a d iamete r o f & mm and an a rea of &0 mm * . Asil icone tube with an external diameter of 6 .(* mm and an internaldiameter of 6 .6 mm connects to the upper surface of the pla te . The
plate has a thic#ened rim, which is perforated to al low suturing to thesclera ;ig. '&.!.ubsequent modifications addressed various problems encountered witht he o ri gi nal d es ig n. uc ce ss r at es w it h s in gl e) pl at e - ol ten oi mplantation for glaucomas with poor surgical prognoses
apha#ic?pseudopha#ic eyes, prior failed filters, neovascular glaucoma,and patients younger than years of age! ranged from *07 to '(7 in

7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 5/25
one study, but rose to '67 to 2&7 with implantation of a second plate*! . A double)p la te -olteno implan t combines two p lates , one of which is attached to the silicone tube in the anterior chamber, while asecond tube connects the two plates, giving an increased surface areaof *26 mm * *'!. In a randomi9ed trial of single)plate versus double)
plate implants, the latter provided better I$% control but was associatedwith a greater ris# of complications, most of which were related to%.(&*
hypotony *0!. Another modification, which addresses the problem of hypotony, is the dual)chamber, s ingle)plate implant, in which a @)shaped BCpressure ridgeB on the upper surface of the plate encasesan area of &6.0 mm * a round the opening of the s i l icone tube *(!. Inconcept, the pressure ridge and overlying Tenon"s capsule regulate theflow of aqueous into the mai n bleb cavit y during the earl y
postoperative period, thereby minimi9ing excessive filtration and
hypotony. The validity of this concept was supported in one study of '6consecu tive pat ient s *2 !, but the r idge e ffec t was found to beunpredictable in a more recent study *3!.
Figure !"#&# -olteno implant.
S'(%')et Tu*e S(unt
choc#e t and associa tes *8,6! developed a technique in which as i l icone, or s i las t ic , tube is extended from the anterior chamber to a(6)degree encirc ling s i l icone band, as used in re t inal detachmentrepair ;ig '&.'!, which functioned in developing the reservoir for
aqueous drainage. -odificat ions have included insert ion of the tubeinto a band extending for only 86 degrees beneath two rectus muscles&! or into the preexisting encircling band in eyes with glaucoma after sc lera l buc#ling surgery *!. A long :rupin)4enver valve implantdiscussed later under BC:rupin ImplantsB! has a lso been used incombination with a &36)degree scleral band !.

7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 6/25
Figure !"#!# choc#et implant.
Two randomi9ed trials compared choc#et tube shunts to double)plate-olteno implants . 4espite the fact that the choc#et shunt typically
provides a larger surface area of the reservoir than the -oltenoimplants, the latter provided lower final I$% in both studies ',0!.FLOW-RESTRICTED DRAINAGE DEVICES
Dittle resistance is offered to aqueous outflow until the plate becomesencapsulated. The incorporation of a valve mechanism in implantsseems to decrease early postoperative hypotony by providing resistanceto the flow and therefore regulating the pressure within a desired range.A(me Glau'%ma +alve
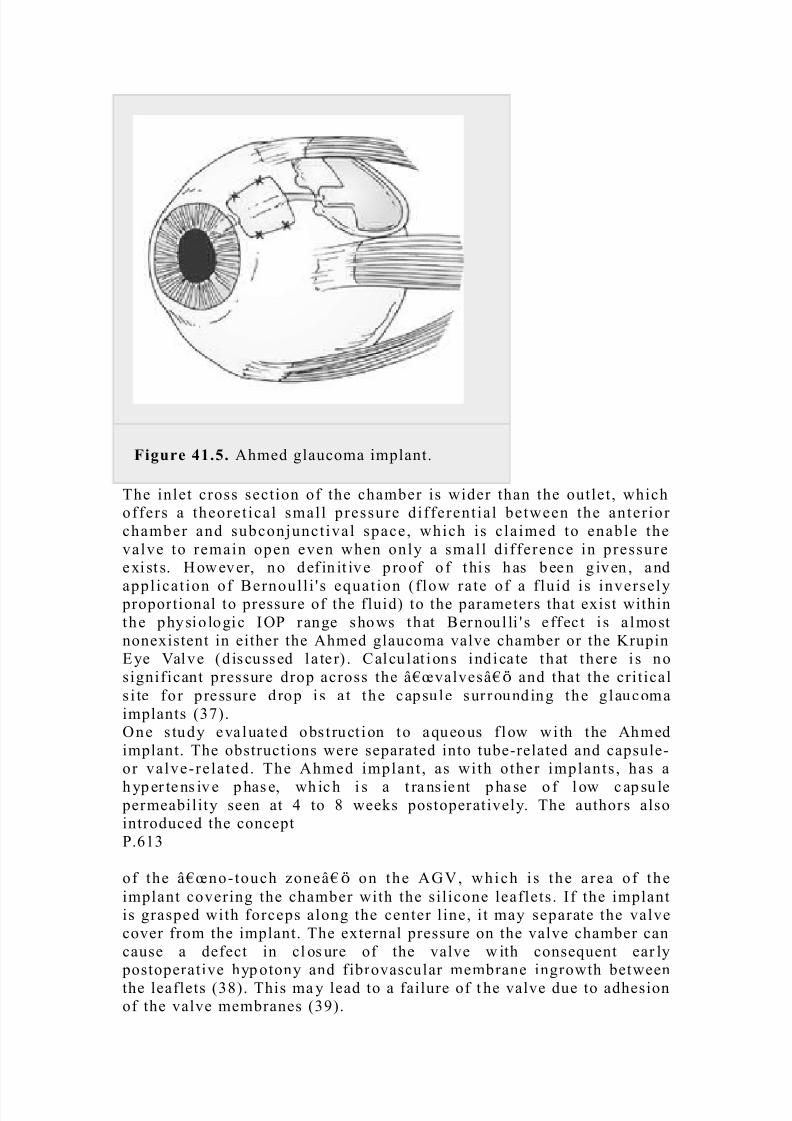
Ahmed g laucoma va lve implan t i s one of the more commonly usedflow)restricted implants in difficult glaucomas.In this valved drainage implant design, a silicone tube is connected to a
silicone sheet valve, which is held in a polypropylene body (! ;ig'&.0!. The body of a most commonly used * model has a surface areaof &3' mm * &( <= & mm! and is &.8 mm thic#. The valve mechanismconsis ts of two thin s i l icone e las tomer membranes , 3 mm long and 2mm wide, which allows one)way regulation of the flow with a goal of #eeping the I$% between 3 and &6 mm /g in the early postoperat ive
period.
7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 7/25
Figure !"#,# Ahmed glaucoma implant.
The inlet cross section of the chamber is wider than the outlet, whichoffers a theoret ical small pressure differentia l between the anterior chamber and subconjunctival space, which is c la imed to enable thevalve to remain open even when only a small difference in pressureexi st s. /owever, no def in it ive p roof o f thi s has been g iven , and
applicat ion of 1ernoull i " s equation f low rate of a f luid is inversely proportional to pressure of the fluid! to the parameters that exist withinthe physio logic I$% range shows that 1ernoul li " s e ffec t i s a lmostnonexistent in either the Ahmed glaucoma valve chamber or the :rupin+ye @alve d iscussed la te r! . >alcu lat ions ind ica te that there i s nosignificant pressure drop across the BCvalvesB and that the criticals i te for p ressure drop is a t the capsu le surrounding the g laucomaimplants 2!.$ne s tudy eva lua ted obs t ruct ion to aqueous f low wi th the Ahmedimplant. The obstructions were separated into tube)related and capsule)or valve)re la ted. The Ahmed implant , as with other implants , has a
h yp er te ns iv e p has e, wh ic h i s a t ra ns ie nt p ha se o f l ow c ap su le permeability seen at ' to 3 wee#s postoperatively. The authors alsointroduced the concept%.(&
of the BCno)touch 9oneB on the AE@, which is the a rea of theimplant covering the chamber with the silicone leaflets. If the implantis grasped with forceps along the center line, it may separate the valvecover from the implant. The external pressure on the valve chamber cancause a defect in cl os ure of the valve w ith consequent ear ly
postoperative hyp otony and fibrovascular membrane ingrowth betweenthe leaflets 3!. This ma y lead to a failure of t he valve due to adhesionof the valve membranes 8!.
7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 8/25
-rupin Implant.
The concept of a one)way valve that opens at a predetermined I$% levelto avoid the early postoperative complications of excessive drainageand hypotony was introduced by :rupin and associates in &82( '6!.The o rigina l :rupin)4enver valve was composed o f an interna l
upramid tube cemented to an external s i las t ic tube '6!. The valveeffect was created by ma#ing s l i ts in the c losed external end of thesilastic tube, designed to open at an I$% between 8 and && mm /g. Thetube was short, extending only a few millimeters subconjunctivally, andhad no ext er nal pl at e. Al though pr el imi nar y experi enc e wasencouraging '&,'*!, f ibrosis eventually c losed the subconjunctival
portion of the valved tube '!, which led to fai lure in most cases.In a subsequent technique, a long :rupin)4enver drainage tube, withthe same one)way valve design, was attached to a &36)degree choc#et)t yp e s cl er al ex pl an t, as p re vi ou sl y d es cr ib ed !. Th is l ed t odevelopment of the :rupin +ye @alve with 4isc, which is the design in
cur rent u se . A s il as ti c tube i s a tt ached to an ova l s il as ti c d is c,conformed to the curvature of the globe, & <= &3 mm, with &.20)mmhigh side walls ''!. The valve at the distal end of the tube is the samedes ign a s in the ear li er :rupin imp lant s and i s manomet ri ca llycalibrated to open at pressures between &6 and &* mm /g. In the newer design of the :rupin implant, the valve lies inside the rim of the plateat its insertion and as such is exposed directly to the subconjunctivaltissues '0!. A review of && patients with the :rupin eye valve withdisc implants identified eight patients with primary valve malfunctionrequiring surgical revision, which involved manipulation, replacementof the valve, and amputation of the valve. Transient postoperat ivehypotony was noted in three patients and chronic hypotony with loss of light perception in one patient. $ne explanted valve was examined andf ou nd t o h av e p ar ti al ly f us ed l eaf le ts , p os si bl y r el at ed t o t hesterili9ation process and prolonged storage before implantation '0!.Ot(er Drainage Devi'e.
$ther valved implants include the Foseph tube silicone tube with slitvalve in its side, calibrated to open between ' and *6 mm /g, attachedto a 8)mm)wide s i l icone rubber s trap! '(!, the $pti-ed Elaucoma%ressure Gegulator &36 to *66 microtubules in a <= * <= * mm
polymethylmethacryl ate box, which allows aqueous to escape into the
subconjunctival space when the I$% exceeds &6 mm /g! '2!, and theH hi te p ump s hu nt whi ch h as a s ur fac e ar ea o f 3 6 m m* and amechanism that may be activated by touching or by blin#ing to allow
pumping of the reservoir to maintain patency of the tube! '3,'8!. Anew miniature glaucoma implant without an external plate, +x)%G+,has become recently available. The study of this implant in rabbit eyeshas shown that the local t issue reaction consis ted of a thin , f ibroticcapsule without significant inflammation 06!.COMPARISON OF IMPLANT DEVICES
The :rupin, 1aerveldt, Ahmed, and $pti-ed implants were comparedat physiologic flow rates in vitro and in vivo in rabbits '2!. Hith all
devices, opening pressures were higher in v ivo t han in vi tro due totissue)induced resistance around the explant. %ressures with all devices

7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 9/25
dropped to 9ero after conjunctival wound disruption. In air, the :rupinand Ahmed implants had opening pressures of 2.* and 8.* mm /g andc los ing pressures of .8 and 0 .* mm, respec t ively. The $pt i-edimplant had the highest res is tance values , with I$%s of &8.( mm /gc omp ar ed w it h 2 .0 m m / g w it h t he Ah me d i mp la nt i n v ivo. T h e
resis tance was s imilar for the 1aerveldt , :rupin, and -olteno dual)chamber implants in vivo . 1oth Ahmed and :rupin valves functioned asf low) res t rict ing devices , rather than t rue valves a t the f low ra tesstudied, but did not close after initial perfusion with fluid. Neither theAhmed nor :rupin devices had demonstrab le opening or c los ing
pressures in balanced salt solution. In another comparative study, theFoseph implants provided s l ightly lower I$%s and had s ignificantlyfewer fai lu re s than the choc#e t dev ices , a lthough the -ol tenoimplants provided the lowest pressures at &* months among eyes withsuccessful I$% control 0&!.Gesistance and pressure responses of the $pti-ed, :rupin, and Ahmed
drainage devices were compared using a 6)gauge cannula as a simpleresis tor to determine whether the devices func tion as t rue valves .Gesistance remained relatively constant for the :rupin, and $pti-edimplants, whereas the Ahmed offered a variable resistance over a rangeof f low rates and pressures between &* and &0 mm /g. The Ahmeddevice functioned as a valve that closely regulated pressure within adesired range by decreasing or increasing resistance as a function of flow 0*!.In a re trospec tive rev iew, the double)p la te -olteno implant wi thmitomycin)> -->! was more li#ely to result in I$% below &0 mm /gthan the AE@ with --> 0!. uccess rates at & year were 367 for the-olteno implant, 87 for the :rupin +ye @alve with 4isc, and 07 for the AE@. /owever , AE@ was less l i#e ly to cause compl ica t ionsrequiring another surgery 0!.The success rate for the Hhite pump shunt was found to be far belowrates reported for other drainage implants, probably, because the distaltube often closes secondary to fibrosis resulting from the absence of areservoir '8,0'!.S/RGI0AL TE0HNI1/ES
BASIC PRINCIPLES
Although certa in varia t ions of surgical techniques are required for
implan tat ion of the d i fferent implan t des igns, the bas ic surgica l principles apply in general to all drainage implant devices.%.(&'
Adequate surgical exposure is dependent on proper placement of atraction suture. A (B6 polyglactin @icryl! or sil# traction suture on aspatulated needle is placed through superficial cornea near the superior limbus and attached to the dr ape beneath the eye.A fornix)based conjunctival)Tenon"s capsule flap is created, usually inthe superotemporal quadrant , to expose the sc lera l bed ;ig. '&.(A!.The f lap is s l igh t ly e leva ted to a l low for b lun t d issec t ion be tween
Tenon "s and episclera wi th b lun t Hes tco t t scissors . 1ecause i t i snecessary to have surgical exposure to or beyond the equator of the

7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 10/25
globe, radial relaxing incisions should be placed on one or both sidesof the conjunctival flap. A muscle hoo# is then used to isolate the tworectus muscles on either side of the surgical site.
Figure !"#2# A3 >reation of subconjunctival space in the superotemporal quadrant.of plate into subconjunctival space. 0 J >utting the tube to the appropriate length.
Hhenever possib le , the superonasa l quadran t should be avoided ,
especially with the larger plate designs, to reduce the ris# of inducingstrabismus, which is discussed later 00!. It has also been shown thatthe Ahmed implan t , when p laced in the superonasa l quadrant , maycome within & mm of the optic nerve 0(!.Hith valved implants, it is necessary to irrigate balanced salt solutionthrough the tube using *2)gauge cannula, before the insertion into theanterior chamber, to ensure that the valve opens proper ly.The external pla te is then tuc#ed posteriorly into sub)Tenon"s space;ig. '&.(1! and sutured to sclera with 8B6 %rolene sutures throughthe anterior positional holes of the plate, with the anterior border 3 to&6 mm posterior to the limbus. @ariations of this technique are required
for different plate designs. I mplants with plates of l arger c ircumferentia l dimensions , such as the 1aerveldt , must be tuc#edunder adjacent rectus muscles, whereas choc#et)type designs requiredissection of one or more additional quadrants, depending on the extentof the encirc l ing band. In the case of the Ahmed implant , which haslarger anteroposterior dimensions, it may be advisable not to extend theanterior border of the plate more than 3 mm behind the limbus.Hith nonvalved devices , res tr ic t ion of aqueous f low to avoid severeearly postoperat ive hypotony can be achieved by using a two)stageimplantat ion technique, in which the external pla te is placed in thesubconjunc tival space wi thout inse rt ing the tube in to the ante rior
chamber . The tube is inse r ted ( to 3 wee#s la te r , a f te r the f ib rouscapsu le has formed a round the external p la te 02,03 ,08! . A more
7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 11/25
popular technique is to occlude the tube by a ligature of (B6, 2B6,or 3B6 @icryl before inserting it into the anterior chamber. Injectionof 1 on *2)gauge cannula into the tube helps to ensure that the tubeis totally occluded. This procedure prevents any drainage of aqueousuntil ' to ( wee#s after the operation when the @icryl suture dissolves,
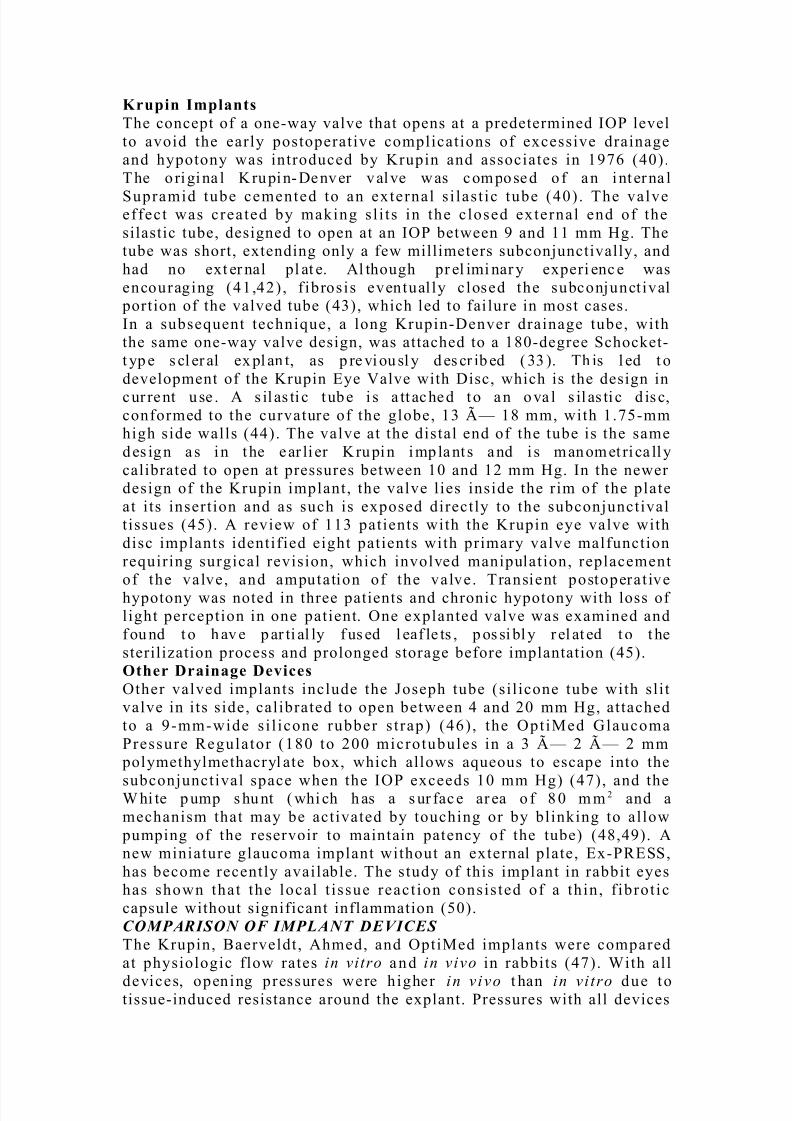
allowing aqueous to drain into the preformed capsule. This technique provides the advantage over the two)stage technique of avoiding asecond operation (6!. @arious tube ligatures and stents have been usedto min imi9e pos topera tive hypotony and a re d iscussed la te r under BC>omplicationsJ %revention and -anagement.BThe tube is then cut, bevel up, to permit its extension * to mm intothe anterior chamber ;ig. '&.(>!. 1efore insert ing the tube into theanterior chamber, a limbal area is cauteri9ed to prevent bleeding fromthe inse rt ion . A paracentes is i s nex t made in fe ro temporal ly a t thelimbus with a number 20 sharp, tapered blade, and a small amount of v is coelas ti c c an be injec ted into the anter io r chamber without
displacing iris posteriorly.
Figure !"#4# +ntering the anterior chamber through the limbal area with a *)gauge or a **)gauge needle parallel to t he iris plane.
The anterior chamber is then entered through the cauteri9ed limbal areawith a *)gauge, or a **)gauge needle, parallel to the iris plane ;ig.'&.2!. The needle creates a watertight seal, preventing lea#age aroundthe tube and thus%.(&0
reducing the ris# of postoperative hypotony (&!. The angle at whichthe needle enter s the anter io r chamber i s c ri ti ca l, because i t i simportant that the tube, which will pass through this needle trac#, is

7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 12/25
positioned between cornea and iris, without touching the cornea.The tube is then inserted into the anterior chamber via the needle trac# using nontoothed or specia l ly designed tube insert ion forceps ;ig.'&.3!, and is secured to the sclera with a loose 8B6 %rolene suture.>ontact of the tube with the iris does not seem to cause any clinically
noticeable problems, a l though tube occlusion by the ir is (*! and adistortion of the pupil (! have been reported. The anterior chamber may need to be deepened with balanced salt solution, or viscoelastic,via the paracentesis, and the tube is chec#ed for proper position in theanterior chamber.
Figure !"#5# Tube insert ion into the anterior chamber via the needle trac#,using nontoothed or specially designed tube insertion forceps.
The tube may occasionally erode through both sc lera and overlyingconjunctiva at the limbus. To avoid this potential complication, mostsurgeons suture a rectangle of preserved donor tissue of approximately0 <= 2 mm over the tube a t the l imbus ('! ;ig. '&.8!. %rocessed
pericardium Tut oplast!, donor sclera, dura, and fascia lata areavailable commercially for this purpose.

7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 13/25
Figure !"#6# uturing of Tutoplast over the tube area at the limbus.
The conjunc t iva i s then su tured bac# to i t s o r ig ina l pos i t ion us ing@icryl sutures. ubconjunctival steroids and antibiotics are injected atthe completion of the procedure in a quadrant away from the surgicalsite. The basic postoperative management is the same as described in
>hapter '6 for f i l tering surgery, us ing topical s teroid)antibiotic andmydriatic)cycloplegic preparations for the first several wee#s. MODIFICATIONS OF BASIC TECHNIQUE
omet imes t he conj uncti va i s scarr ed at the li mbus, ma#i ngconjunctival dissection impossible without destroying much of theconjunctival tissue. In this case, the initial conjunctival incision may
be made approximately 3 mm from the limbus to create a limbal basedconjunc t iva l f lap . Another op t ion is to use the in fe ro tempora l o r asuperonasal quadrant.@ar ious occ lus ion l iga tures inc lude a pos ter ior ly p laced suture , areleasable suture, and an anterior chamber tube ligature. A 0B6 nylon
suture can be threaded into the tube at the plate end and secured withone or two absorbable sutures around t he tube (0,((!. The exposed endof the nylon suture is positioned subconjunctivally near the limbus for subsequent removal. 1iodegradable stents, such as collagen lacrimal
plugs (2! or 'B6 chromic suture (3!, have also been evaluated, butthey have been less satisfactory because they do not always dissolve.The internal and external occlusion techniques may be combined. ;or example, a 0B6 nylon or B6 upramid internal occlusion suture is
placed, along with an external @icryl ligature around the tube. Theinternal stent is then pulled without difficulty in the office treatmentroom (0!.
5s ing a c lea r cornea l g ra f t , t ied wi th 3B6 nylon , ins tead of the pericardium or scleral graft to cover the outer portion of the tube

7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 14/25
provides the view of the tube with the suture for postoperative laser suture lysis (8!.As an a l te rna t ive to the use of a p rese rved t i s sue , an au to logous ,
partial)thic#ness scleral patch graft crafted from the sclera adjacent tothe tube has been described. No complicat ions were reported in the
s tudy, but the r is# for per fo ra tion o f the g lobe exi st s dur ing thedissection of the f lap, and this may not be a good choice in the eyeswith high myopia or with scleritis 26!.ome surgeons combine stent occlusion with longitudinal slits in thetube to provide early I$% control 2&!, and a laboratory study indicatedthat a slit)valve of *.6 mm appears to provide an opening pressure of around &6 mm /g 2*!. 5sing the 06)mm * 1aerveldt implant, the roleo f fenes trat ions in the tube and ant imetabol it es was s tudied incontrolling I$% in the early postoperative period. An occlusive 2B6@icryl suture was p laced just anter ior to the p late, fo llowed by athrough)and)through penetration of the tube with a standard &0)degree
blade in longitudinal orientation just anterior to the ligature. The I$%was e levated a t day *& due to f ibrotic bloc#age of the fenestra t ions
before the ligature dissolved, but the pressure was well controlled byantiglaucoma medications or laser suture lysis of the 2B6 @icrylocc lus ion suture . The use of ant imetaboli tes d id not improve theoutcome 2!.Another potentia l complicat ion, as with a l l f i l t ra t ion procedures , isfailure due to excessive fi brosis. A rabbit study%.(&(
was per fo rmed with b il at eral imp lantat ion o f *66 mm * 1aerveldtimplants, in which one eye was exposed intraoperatively to --> 6.0mg?ml for 0 minutes 2'!. The -->)treated eyes had lower I$%s andhigher perfusion rates at *, ', and ( wee#s, and histologic examinationrevealed thinner f ibrous capsules with delayed maturat ion and lessinflammatory infi lt ra te . In one re trospective s tudy, implantat ion of AE@s combined with the use of --> achieved lower postoperat iveI$%, with fewer glaucoma medications and similar complication ratesthan the Ahmed valves implanted without antimetabolites 20!./owever, results in clinical trials have been conflicting with regard toreducing the complicat ion of excess ive f ibrosis with antimetaboli tes
2(,22!. At the present t ime there does not appear to be s ignificantc l inical benefi ts from applicat ion of antimetaboli tes in conjunctionwith drainage implants, and it is not recommended for most cases.
SPECIAL SITUATIONS
Par. Plana In.erti%n
In apha#ic or possibly pseudopha#ic! eyes, in which a vitrectomy has been performed, it is also possible to insert the tube through a pars plana incision into the vitreous cavity. The pars plana tube shunts areusually used when it is impossible or undesirable to place the tube intoanterior chamber, or when a need for pars plana vitrectomy coexists. A/offman e lbow has been des igned for pars p lana inser tion , and
excel lent r esul ts were demonst ra ted with the 1ae rveldt imp lantfo llowing pars p lana v i trectomy and f luid)gas exchange. A mean

7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 15/25
postoperative I$% of &' mm /g with an average of 6.( glaucomamedications was reported in one study 23!. The pars plana insertionhas the advantage of #eeping the tube away from the cornea especiallyafter penetra t ing #eratoplas ty! and ir is , and of reducing the r is# of epithelial downgrowth. It is especially important in eyes with corneal
grafts . Gepositioning of glaucoma implant tubes from anterior chamber into vi treous cavity after pars plana vitrectomy for anterior segmentcompl icat ions, such as cornea l decompensat ion , o r recurren t tubeerosion, is another option 28!.Pree7i.ting S'leral Bu')le
T he t rea tm en t o f a r et in al d et ach me nt ma y b e a ss oc ia te d w it h postoperative glaucoma. The presence of the scleral buc#le presents aspecial challenge in cases in which I$% cannot be controlled medically.>onjunc tiva l sca rring caused by ret ina l surgery can s ign if icant lydecrease success of trabeculectomy, even with the use of antimetabolites. >yclodestructive procedures can be used, but they are
quite unpredictable and may cause significant complications. Elaucomadra inage implan ts a re a use fu l op t ion to contro l I$% in such eyes ,although the presence of scleral buc#le ma#es placement of the platequite challenging.Hhen a sc le ra l buc#le has been p laced in the eye for more than months, a silicone tube can be inserted into the anterior chamber, withthe dis ta l end introduced into the f ibrous capsule of the preexis t ingsclera l buc#le, which serves as an exte rnal rese rvoir fo r aqueousdrainage. 1ecause the buc#le is already encapsulated, no ligation of thetube to res tr ic t the f low i s neces sa ry. In one s tudy, the I$% wassuccessfully controlled in 307 of patients *!.Dong :rupin)4enver valved implants with a flow restrictor at the distalend of the tube can further decrease chances of postoperative hypotonyin eyes wi th sc le ra l buc#le . I f the sc le ra l buc#le was p laced morerecently than months and the fibrous capsule has not formed yet, it is
possible to use a smaller 1aerveldt implant, and it is sometimesnecessary to trim the BCwingsB of the implant to position the plateundernea th the exist ing sclera l band. The f ibrous capsu le then isexpected to grow around the buc#le and the 1aerveldt implant 36!.uccessful insertion of a 1aerveldt drainage implant behind or over a
preexisting scleral buc#le, or in the segment without retinal hardware
has been described. +xcis ing the capsule overlying the band a l lowscontinuous encapsulat ion of the band and 1aerveldt pla te to achievegreater I$% reduction. After & year, I$% control was achieved withoutmedications in 237 of patients with 06)mm * plates, but in only *87of patients with *06)mm * plates 3&!.Pree7i.ting 0%rneal Gra8t
Elaucoma after penetrat ing #eratoplasty %:%! remains a difficultmanagement problem. %:% often causes additional damage to the angle,induc ing per iphe ra l anter io r synechiae forma tion , w ith fur ther impediment to aqueous outf low. >ontro l o f pos t )%:% g laucoma iscomplicated by the need to preserve graft clarity for visual function.
Hhen medica l management fai l s, i f the angle i s open and grosslynormal , a rgon laser t rabeculoplas ty may be an opt ion . I f fu rther

7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 16/25
in tervention is indicated, a glaucoma drainage implant , in eyes withgood visual potential, is recommended. ;or those eyes with poor visual
potential or for those patients who cannot undergo surgery!transscleral cyclophotocoagulation may be a better option 3*!./owever, placement of glaucoma drainage implants in the anterior
chamber may be complicated by tube)cornea touch and endothelialdecompensation, particularly after corneal transplantation. $nly 267and 007 of the corneal grafts survived at * and years, respectively,after inserting a glaucoma drainage implant into the anterior chamber 3!. A retrospective review of simultaneous %:% and the AE@ implantshowed 8*7 and 067 graft success and 8*7 and 3(7 I$% control at &and years, respectively 3'!.%ars p lana inser t ion is a reasonable opt ion for pat ien ts who haveundergone %:% or in whom %:% is anticipated, despite the need for acomplete pars p lana v it rec tomy. The pars p lana approach avoidscompl icat ions rela ted to l imbal tube p lacement and offers bet ter
c or ne al g ra ft s ur vi va l, b ut t he i nc id en ce o f p os te ri or s eg men tcomplications may be higher for pars plana insertion 30!.I mp la nt at io n o f t he t ub e t hr oug h t he c il ia ry s ul cu s i s an ot he r a l ternative to anterior chamber angle placement in pseudopha#ic or apha#ic eyes wi th re frac tory g laucoma and a h igh r is# for cornea ldecompensation, or eyes with shallow anterior chamber, or extensivesynechial angle closure. %ositioning of the tube under the iris may be
particularly advantageous in the presence of an anterior chamber I$D, because the tube would not disturb the lens. This procedure iscontra indicated in pha#ic eyes because of a possib le injury to thecrystalline lens 3(!.%.(&2
0OMPLI0ATIONS3 PRE+ENTION AND MANAGEMENT
HYPOTONY
5ntil the f ibrous capsule has developed around the external pla te toregulate aqueous f low, the open, nonvalved tube implants , as notedearlier, provide very low resistance to flow, and hypotony in the early
postoperative course with nonvalved implants is a seriouscomplication. 1y far the best way to prevent this potential complicationi s by t empora ri ly obs truc ting the tube lumen . A wide var ie ty o f
techniques have been described to achieve this goal. 1asic techniquesinclude suture ligation of the tube, as previously described, temporaryocclusion of the tube lumen with a stent, two)stage implantation, or useof a valved implant . +arly postoperat ive hypotony was found in lessthan &67 of patients after AE@ insertion &6,32!. If early postoperativehypotony happens in combinat ion with f lat ante rior chamber , theninject ion of dense viscoelas t ic into the anterior chamber and c loseobserva tion within the f ir st *' hou rs may be helpful . I f the f la tchamber and hypotony reoccurs , then removal of the tube from theanterior chamber is recommended to prevent corneal decompensationwith planning to reposition the tube into the anterior chamber within
the next few days.D at e h yp ot on y f ro m d ra in ag e i mp la nt s i s u su al ly t re at ed w it h

7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 17/25
permanent occlusion of the proximal tube or removal of the tube fromthe anterior chamber, which permanently removes the effect of theentire implant . %ermanent l igat ion of the tube to the dis ta l pla te of double)plate -olteno implant, has the advantage of reducing, but notcompletely eliminating the effect of the implant 33!.
ELEVATED INTRAOCULAR PRESSURE 4rainage implant procedures can also be complicated by elevated I$%in e i ther the early or la te postoperat ive period. 1efore the l igaturearound the tube dissolves , there may be a transient e levation of theI$%. It can be prevented by combining a trabeculectomy without -->with the drainage implant, or it can be managed medically. Hithin thefirst 2 to &6 days after surgery a hypotensive phase may present withlow I$%, con junc tiva l and corneal edema , and a congest ion o f conjunctival blood vessels in tissues covering the plate of the implant.This may be fo llowed by a second, hyper tensive phase , which ischaracteri9ed by I$% elevation associa ted with the formation of the
capsule . 4uring this phase , the edema disappears and fibrous t issuedevelops in the deepest layers of the bleb. 4uring the first & to ' wee#sof th is phase , the b leb wal l becomes congested, causing the I$%elevation. >ongestion and inflammation subsequently subside, with I$%r educt ion and st abi li 9at ion over t he next to ( mo nths. Thehypertensive phase is common following implantat ion of the Ahmedvalve, occurring in 3*7 of patients &6!.+ lev at ed I $% i n t he e ar ly p os to per at iv e p er io d ma y b e d ue t oobstruction of the tube by fibrin, blood, iris , vitreous membranes, or silicone oil. This was observed in &&7 of eyes after AE@ implant 32!,wi th i r is and f ibr inous membranes being the mos t common t i ssuesresponsible for b loc#age 6.37 each! , fo llowed by a neovascula r membrane, a f ib rinous s trand, and an i ridoco rnea l endothe li alm emb ran e. I ri de ct om y a t t he s it e o f t he t ub e o st iu m h as b eenrecommended to p revent i ri s p lugg ing the tube o st ium 38 !, butrequires a larger inc ision . NeodymiumJytt r ium a luminum garnetNdJKAE! laser membranectomy was effective for reopening bloc#edglaucoma tube shunts and maintaining the patency over time in 3'.(7of the eyes in one retrospective study, but recurrence of the bloc#ageoccur red in 0.37 o f eyes within the f ir st && wee#s . %os tl aser complications included moderate anterior chamber reaction, hyphema,
corneal edema, pressure spi#e, and shallow anterior chamber 86!.4istal tube occlusion by fibrous tissue has been reported after placingtube shunts into the fibrous capsule around a preexisting scleral buc#le*,0&,8&!.Geported techniques to open the occluded tube have included irrigationof the tube wi th balanced sal t solu tion using a 6)gauge cannulathrough a paracentes is inc is ion 8*! , the use of NdJKAE 8! , o r
NdJyttr ium li thium fluoride 8'! to open occluded tubes, and theintracameral inject ion of tissue plasminogen activator 6.& cc of 0 to &LMg! to dissolve a fibrin clot 80,8(!.Date I$% elevation, especially when the intraocular portion of the tube
appears to be patent , is usually due to an excess ively thic# f ibrouscapsule. Needling revision can improve function of the encapsulated

7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 18/25
drainage implant. It is more successful when the implant has a larger surface area , a l though the r is# for severe complicat ions , includingendophthalmitis, exists 82!.H hen n eed li ng i s u ns ucc es sf ul a ft er a f ew a tt emp ts , i t ma y b e
beneficial to remove a portion of the encapsulated bleb beneath the
conjunctiva . In a re trospective s tudy on 80 eyes of 28 consecutive patients who underwent a single)stage -olteno implantat ion, &' eye s of &* patients developed recurrence of the encapsulated bleb. Hith a meanfo llow)up of 6 months, the mean I$% a f ter capsu le exc ision wassignificantly lower than the preoperative I$%, achieving 207 successrate 83!.It has also been reported that topical corticosteroids therapy can causeI$% elevation despite the presence of a functioning drainage implant88!.
MIGRATION, EXTRUSION, AND EROSION
Tube migrat ion may occur after glaucoma shunt procedures &66!. If
the tube i s not adequately s ecured to the s clera i t may mig ra te posteriorly out of the anterior chamber, which may requirerepositioning of the tube and securing it to the sclera with additional8B6 %rolene sutures. Anterior migration of the tube can occur due tothe dislocation of the external plate.In pediatric patients, the tube may retract out of the anterior chamber &6&,&6*! or even erode through the cornea &6!. +xtrusion of theimplant was the most common reason for repeat surgery in childrenwho received the AE@ &6'! . Thi s may occur a s the eye g rows ,requiring reposit ioning of the tube from the original s i te &60!. Thetube may also need to be reposit ioned when i t is bloc#ed by cornea,iris, or vitreous (&!. If the tube end is too short to allow repositioning,a s i las t ic s leeve or s i las t ic extension tube &6(! may be used. A **)gauge angiocatheter and a p iece of ped ia tr ic lac r imal tub ing , wi thinternal diameter 6 . mm and external diameter of 6 .(' mm, may beused for this purpose &62!.%.(&3
Avulsion of an implant after blunt trauma may force the tube againstthe cornea, causing corneal melting and requiring explantation of theimplant and possibly corneal grafting. %lacing a double)plate -olteno
implan t" s connect ing tube under the super ior rectus muscle mightdecrease the ris# of shunt avulsion after trauma &63!.+rosion of the s i l icone tube through the overlying conjunctiva is arecogni9ed complicat ion of the aqueous shunts. A part ia l) thic#nesssclera l f lap does not prevent erosion of the tube and, as previouslydescribed, the tube and fistula site should be covered with preservedsclera , dura , fascia la ta , or pericardium. /owever, pericardia l graftthinning &68!, melting &&6!, and conjunctival erosion despite the
patch graft &&&! have been reported.If a sc lera l graft is too thic#, i t may elevate the l imbal conjunctivaenough to produce dellen formation. >onversely, a thin scleral patch
g ra ft may p redi spose the tube to e rosion . Addi tional ly, immunereactions resulting in scleral melting have been reported &&*!. The use

7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 19/25
of preserved sclera a lso has the disadvantages of dependence on eye ban# supplies, precluding its use in emergency cases, possibly greater cost &&!, and concerns about infectious disease transmission, despitedonor screening &&'!. tudies utili9ing polymerase chain reaction haveshown the evidence of the human immunodef iciency v irus /I@!
genome in sc lera obtained from /I@)& seroposit ive donors , despitet rea tment wi th hea t, a lcohol, o r fo rmal in, but not a fter i r radia tion&&'!.olvent)prese rved cadaver per ica rd ium Tutoplas t ! o ffers severa ladvantages, including availability, lower cost, uniformity in si9e andtissue quality, and enhanced sterility. A dehydration process leaves thegraft devoid of antigenic s t imuli , yet preserves the t issue "s inherentstrength and flexibility &&0!. Tissue sterili9ation is achieved throughthe treatment with organic solvents fol lowed by low)dose radia t ion,which inactivates bacteria, fungi, and viruses, including /I@ &&',&&(!and >reut9feldt)Fa#ob disease virus &&2!.
Thin 6.*0 mm! e%T;+ patches were well tolerated in rabbit eyes andmay be an a l ternative to donor sc lera for re inforcement in glaucomadrain surgery &&3!.If the pla te of an implant migrates toward the medial rectus muscleinsert ion, myosit is may develop. This was reported to resolve after removal of the implant &&8!.
ENDOPHTHALMITIS
As mentioned previously, endophthalmitis may develop after needlingof the implant 82!.Gecurrent Propionibacterium acnes endophthalmitis has been reportedafter -olteno tube revis ion, based on a posit ive culture of anterior chamber needle aspira te. The patient responded poorly to repeatedintraocular vancomycin injections and required explantation of the tubeto achieve complete resolution of the infection. Tube reinsertion intothe anterior chamber resulted in recurrence of the infection &*6!.Gemoval of the glaucoma drainage implant in cases of endophthalmitismay be necessary to remove the contamina ted fore ign body. +ar ly
postoperative endophthalmitis, following placement of an implant, may be successfully treated by immediate removal of the implant andsurgical management of the infection, with subsequent placement of anew implant &*&!.
+ndophthalmit is may a lso occur in the la te pos topera tive course .+ xp os ur e o f t he t ub e s eem s t o be a ma jo r r is # f ac to r f or t he seinfections . urgical revis ion with a patch graft in a l l cases in whichthe re i s an exposed tube i s ind icated to p revent thi s poten ti al lydevastating complication &**!.terile endophthalmitis was also described approximately & month after discontinuation of postoperative corticosteroid therapy &*!.VISUAL LOSS
In one s er ie s o f '& pat ient s a ft er -ol teno imp lant surge ry, theincidence of reduced visual acuit y was **7, with hypotony and shallowanterior chambers being the most commonly associated events &*'!.
$ther reported mechanisms of visual loss include re t inal detachment&*',&*0,&*(,&*2!, vi treous hemorrhage &*',&*0!, cystoid macular

7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 20/25
edema &*0!, and operating microscope)induced retinal phototoxicity&*3!. These complications often occurred despite successful control of I$%.
CORNEAL DECOMPENSATION AND GRAFT FAILURE
The causes of corneal decompensation and graft fa i lure in eyes withdrainage implant are not complete ly c lear, but may be re la ted to theret rograde f low f rom the encapsu la ted reservo ir to the anter io r chamber. eria l corneal endothelia l ce l l counts in &8 patients after uneventful -olteno implants revealed s l ight , c l inical ly insignificant
progressive cell loss &*8!. Tube)cornea touch is another cause of corneal decompensation. In one study of AE@ implantation in pediatric
patients, corneal)tube contact occurred in &3.07 &6!. Hhen the tube)corneal contact is seen, removal of the tube from the anterior chamber,shortening of the tube, and subsequent reinsertion may be necessary.1ecause this technique may require extensive revis ion with possible
complicat ions , a s impler technique was described for tr imming thesilicone tube in situ &&!.In one retrospective review, corneal edema developed on average after *& months in 067 of patients fol lowing -olteno shunt implantat ion,and in (.27 after multiple eye surgeries, including a trabeculectomy,
but not after the trabeculectomy alone &*!. In another study, whencornea l compl ica t ions thought to be unre la ted to the implan t wereexcluded from the defini t ion of fa i lure in a cohort of patients withAhmed implants with a mean follow)up for 6.0 months, only *&.07 of the eyes were considered fai lures, and cumulat ive probabi li t ie s o f s uc ces s a t & , * , , a nd ' ye ar s w er e 3 27 , 3 *7 , 2 (7 , a nd 2 (7 ,respectively. /owever, when corneal decompensation and corneal graftfailure were included in the definition of failure, '7 of the eyes wereconsidered failures, decreasing cumulative probabilities of success at &,* , , and ' years to 2(7, (37, 0'7, and '07, respectively. Thesecorneal problems may be secondary to the underlying ocular conditionor to the drainage device i tself &!. %hosphorylcholine polymer)coating of the glaucoma drainage devices was suggested to reduce therate of corneal endothelial failure &'!.A co mp ar at iv e s tu dy s ho wed t hat al th ou gh a n ad di ti on al t ub eimplantation provided better I$% control than with tube repositioning,
the most common complication with this approach%.(&8
was corneal edema &0!. Another study showed that tube replacementafter initial shunt failure has high corneal morbidity, reaching a cornealdecompensation rate of (7 &(!. /owever, an I$% below *& mm /gor *67 reduction in I$% after the second tube procedure was achievedin 3(.'7 with a )year follow)up.
DIPLOPIA AN D OCULAR MOTILITY DISTURBANCE
As prev iously noted , implan ts wi th larger p lates, e spec ial ly when
implanted in the superonasal quadrant, can interrupt extraocular 00!muscle function and cause s trabismus and diplopia. >haracterist ic

7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 21/25
patterns are exotropia, hyp ertropia, or limitation of ocular rotations&2,&3,&8,&'6,&'&!, although a 1rown"s superior oblique tendon)l i#e syndrome has a lso been descr ibed 00 ,&'* ,&'!. Hhi le thecomplication is usually associated with the larger plates, such as the06)mm * 1aerveldt implant &2,&3,&'*! and the :rupin valve with
d isc &8 ,&'6! , i t may a lso occur wi th smal le r p la tes , such as thesingle)plate or double)plate -olteno implants, especially in children&'&! . >or rect ive measu re s may requi re removal o f the imp lant ,r epl ace ment w ith a smal ler pla te design, or tr ansf er t o thesuperotemporal quadrant, which usually &8! relieves the diplopia.In one s tudy, postoperat ive moti l i ty dis turbance, including acquired1rown syndrome, superior oblique and lateral rectus palsy developed in&& *'7! of *' e yes af ter ( mont hs of double) pla te - olt enoimplantation, although this may resolve spontaneously with time &'!.
OTHER COMPLICATIONS
+pithelial downgrowth is uncommon, but is a potential ris#, especiallywith tubes inserted a t the l imbus. I t can cause fa i lure of the implantfunc t ion, cornea l decompensa t ion and , when assoc iated wi th theformation of a true Tenon"s cyst , s ignificant cosmetic deformity andmotility disturbance &''!.+pithelia l invasion into the f ibrous capsule with pers is tent aqueouslea# was descr ibed in four pat ien ts dur ing the ear ly pos topera tivecourse following 1aerveldt implant surgery &'0!. All reported cases of epithelial ingrowth occurred in previously operated eyes. To maintainuseful vis ion in advanced cases of epithelia l downgrowth associa tedwith secondary glaucoma, the combination of a tube shunt and %:%may be indicated &'(!.teri le hypopyon has been reported after removal of 'B6 chromicsuture stents &'2!.il icone oil dra inage from the vi treous cavity to the subconjunctivalspace through a -ol teno imp lant was repor ted in an eye with anante rior chamber -ol teno implan t , lensectomy, v it rec tomy, andintravitreal silicone oil injection. A drainage implant may thus not beappropriate in eyes with intravitreal silicone oil &'3!.ome patients may develop an irregular pupil years after implantationof a s i l icone tube because of adherence of ir is root to the tube (!.
/owever, i t is more important to place the intraocular port ion of thesi l icone tube away from the cornea to minimi9e corneal endothelia lloss, because contact with the iris stromal root does not typically causesignificant problems (!.Elobe perforat ion can occur while suturing the pla te to the sc lera ,causing retinal detachment or vitreous hemorrhage. The ris# is greater in buphthalmic or highly myopic eyes with thin sc lera . Implantat ionunder the scleral buc#le may be complicated by scleral perforation atthe site of severe ectasia underlying the previous buc#le &'0!.G et in al c omp li ca ti on s w it h d rai nag e i mp la nt s i nc lu de r et in aldetachment , suprachoroidal hemorrhage , choroidal e ffus ions , and
vitr eous hemorrhages. The most common ris# factors for suprachoro ida l hemorrhage a re o lder age , pos topera tive choroida l

7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 22/25
effusions, low I$% immediately after the tube opened, hypertension, or a therosclerosis . >omplete l igat ion of the proximal part of open tubedesign with a 2B6 @icryl suture , tes t ing for watert ightness before
placing the tube in the anterior chamber, may decrease the rate of retinal complications (&!. In one study with 1aerveldt implants, the
median onset of a postoperat ive re t inal complicat ion was &*.0 days ,with &6 patients 37! experiencing complicat ions within 0 days .erous choroidal effusions usually resolve spontaneously. eriousre tinal compl ica t ions were d is t ributed evenly among pat ien ts wi th:rupin valves with discs and -olteno and 1aerveldt devices &'8!.O/T0OME AND INDI0ATIONS
LONG-TERM OUTCOMES
$utcome s tud ies have been repor ted for the more commonly useddrainage implan t dev ices. The fo llowing data were der ived f romBClong)termB follow)ups usually a mean of &* months or more! of overal l s tudy popula tions in which BCsuccessB was typically
defined as a low)end cutoff of 0 to ( mm /g and a high end of *& to **mm /g with or without medication. In trials with -olteno implants, thesuccess ra tes were 27 to 2'7 with a mean &06! or minimum &0&!follow)up of &3 months and 027 with a mean follow)up of ' to ''months &0*,&0!. A success ra te of 2(7 &0'! was reported in eyeswith uveitic glaucoma and a follow)up period of 0 to &6 years. A studyof 3* blac# patients treated with -olteno implants and followed up for a mean of 6 months gave a similar success rate of 2*7 &00!. urvivalanalysis in a retrospective study showed that failure was most commonin the f irs t postoperat ive year, and s ignificant r is#s for fa i lure were
pseudopha#ia and neovascular glaucoma. %ostoperative I$% tended to be lower after double)plate than after single)plate implantation. Therewas no significant difference in outcome with -olteno implants basedon age, sex, race, previous %:%, or previous conjunctival surgery &0! .Hith choc#et)type implants, reported success rates were 8&7 with amean follow)up of &6 months &! and 3&7 with a &2.0)month meanfollow)up &0(!, but fell to 67 at ( months in one study using life)tables &02!.Geported success with 1aerveldt implants was 87 and 337 for 06)mm* and 066)mm* implan ts , respec t ively, a fte r &3 months &8! ,although other studies reported 2&7 to 2*7 success with a minimum of
( months &03!, a mean of &.( months &08!, and * years &(6! of follow)up.tudies wi th the :rupin valve and d isc revea led () and &*)monthsuccess rates of 3'7 and ((7, respectively%.(*6
&(&!, while another group found an 367 success ra te with a meanfollow)up of *0 months ''!. tudies with the Ahmed valve revealedsuccess rates of 227 to 327 at &)year of follow)up &6,(,32! and 207success rate at * years of follow)up 32!. The visual acuity improved or remained within one nellen line of the preoperative value in (*7 to
237 of the various s tudies , which is undoubtedly influenced by therelative proporti on of glaucoma types in each study.

7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 23/25
uccess tends to be somewhat lower in pediatr ic populat ions . AE@&(*! imp lantat ion in chi ld ren was repor ted to have cumulat ive
probabilities of success of 22.87 at &* and (6.(7 at *' months, whichi s s im il ar t o t ho se o f o th er i mp lan ts w he n u sed i n a p ed ia tr ic
population &6'!. An other study showed that ( months after tube)shunt
surge ry in the managemen t o f chi ldhood g laucoma, the I$% wascontrolled in 2*.*7 with or without glaucoma medication, decreasingto ''.'7 after * or more years. Although 3.87 remained within oneline of preoperative vision or improved, *2.37 lost light perception.-ost children required additional surgical procedures to control I$% or manage tube)re la ted complicat ions . The l imited success ra te in thisstudy, the relatively high complication rate, and the need for frequentsurgical intervention suggest caution regarding the prognosis of tube)shunt surgery in children with glaucoma &(!.
INDICATIONS
4rainage implant surgery is typically reserved for patients in whom
trabeculectomy with adjunctive antimetabolite therapy has either failedor is thought to have a very low chance of success, and in whom thereis s t i l l a reasonable potentia l for vis ion. Indications include young
patients individuals with neovascular glaucoma, glaucoma associatedwith uve it is , s evere con junc tiva l s ca rr ing, r ef ractory ped ia tr icglaucoma, or glaucoma in apha#ia or pseudopha#ia and patients withother prior surgery, such as vi treoret inal surgery and %:%. uccessrates vary with the different patient characteris tics and underlyingdisorders.Y%ung Patient.
As p reviously noted , d ra inage imp lant surge ry in the ped ia tr ic population & month to & years!, as with any surgery for childhoodglaucoma, is more problematic than in adults . Nevertheless , successrates of 007 to 807 have been reported, with no defini te advantage
between -olteno, 1aerveldt, or Ahmed implants&6&,&(',&(0,&((,&(2!.4rainage implant surgery may be especia l ly useful in children with
juvenile rheumatoid arthritis and uveitic glaucoma (*!, and withglaucoma associated with turge)Heber syndrome 08,&(3,&(8!. In thelatter situation, an advantage of drainage implants over trabeculectomywith ant imetaboli tes i s the reduced r is# of expuls ive hemorrhage
associa ted with mar#ed I$% reduction. 4rainage implants have a lso been shown to succeed in children after cycloablation &6!.>omplicat ions of d rainage implan tat ion in chi ldren inc lude tubemalposit ion &(2!, f la t anterior chamber, tube obstruction by ir is or vi treous, cataract , cornea)tube touch, choroidal detachment, cornealedema and corneal abrasion (*!.Ne%va.'ular Glau'%ma
4rainage implants have been successful in some eyes with neovascular glaucoma &26!, although the success declines with time. In one study,the success rate with -olteno implants was (*.&7 at & year, decliningto &6.7 at 0 years &2&!. Geported success with the 1aerveldt &2*!
and Ahmed 32! implants has been (67 to 367 with declining successover time and a generally lower success rate than with other forms of

7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 24/25
glaucoma. Elaucoma drainage implants have been reported to have better outcome in the eye s with neovascular glaucoma thancyclophotocoagulation &2,&2'!./veiti' Glau'%ma
Ahmed valve implants have been shown to be a safe alt ernative in high)
ris# patients with uncontrolled uveitic glaucoma who have had multiple previous ocular surgeries &20,&2(!. uccess may be enhanced by preoperative and long)term postoperative immunotherapy. The mostcommon complications are encapsulated bleb, transient hypotony, andhyphema.Severe 0%n9un'tival S'arring an Previ%u. O'ula r Surgery
A failed trabeculectomy, especia l ly when the conjunctiva is scarreddown in both superior quadrants, could be an indication for a drainageimplant procedure. In addition, other types of ocular surgery may causesuch conjunctival scarring that an implant wil l have a better chancethan a t rabecu lectomy. 1oth -ol teno &22! and 1ae rveldt &23!
implants have been effective for glaucomas associated with apha#ia or pseudopha#ia. The -olteno implant has also been used with somesuccess in eyes with epi thel ia l downgrowth &28! . -ol teno andchoc#e t implan ts have been used in assoc iat ion wi th pars p lanavi trectomy in eyes wi th v it reoret ina l d isorders &36! , and in eyesfollowing %:% &3&,&3*!. The -olteno implant and the Ahmed valvehave also been used with success in eyes with prior cyclodestructivetherapy &6,&3!.Aniriia
-edical and surgical therapy may not always be efficient in controllingI$% in aniridia . -olteno implants &3'! and the Ahmed valve &30!have been used in these pat ients. I n a r etr ospect iv e review,implantat ion of a glaucoma drainage device in patients with aniridiahad a success rate of 337 after & year &3(!, reducing the I$% from 0mm /g to &0 mm /g , wi th mos t o f the eyes hav ing improved o r unchanged visual acuity.0OMPARISON :ITH ALTERNATI+E PRO0ED/RES
In patients with glaucomas that are at high ris# of surgical failure, asdescribed earlier, the surgeon usually must choose between a filteringope ra tion with adjunct ive ant imetabol it es , a d ra inage imp lant
procedure, or a cyclodestructive operation.
%.(*&
>omparable resu lts have been reported wi th s ing le )pla te -oltenoimplan ts and t rabeculectomy wi thout an adjunc t ive ant imetabol i te&32!, or trabeculectomy with postoperative 0)fluorouracil &33!, whiletrabeculectomy with intraoperative --> provided significantly greater I$% reduction &38!. In each of these studies, the t ypes of compl icat ions d i ffered between the two procedures, as p rev ious lyd iscussed, but they tended to be more f requent wi th the drainageimplant operations. /owever, a prospective randomi9ed comparison of Ahmed drainage implan t and t rabeculectomy wi th --> found no
difference in the ra te of complicat ions , a l though the I$% was better controlled in the trabeculectomy group during the f irs t year &86!.

7/25/2019 Drainage Implant Surgery
http://slidepdf.com/reader/full/drainage-implant-surgery 25/25
After years, the results were similar in both groups &8&!.4rainage implants have been shown to provide better I$% control ineyes with advanced uncontrolled glaucoma than cyclophotocoagulation,
but more often require repeat surgery and have a higher complicationrate, including vision loss &8*!. The two procedures were comparable
in one series of eyes with %:%, although there was a trend toward moregraft failure, hypotony, and visual loss with the laser surgery &8!. Asmentioned previously, in eyes with neovascular glaucoma, drainagei mp lants pr ovided bet ter I$% cont rol and visual acui ty t hancyclophotocoagulation &2,&2'!.S/MMARY
4rainage implant devices have been successful in controlling I$% sincethe development of tubes that dra in into subconjunctival reservoirscreated by external plates. Implant designs differ according to the si9eand shape of the external plate and whether the tube is open -olteno,choc#et, and 1aerveldt! or valved :rupin, Ahmed, Foseph, $pti-ed,
Hhite!. The basic surgical technique involves implantation of one endof the tube in the anterior chamber, with the other attached to the platenear the equator. A fibrous capsule develops around the plate, whichregulates the aqueous flow. >omplications include hypotony, elevatedI$%, ocular motility disturbance, and loss of visual acuity. Indicationsfor drainage implant surgery include previous fa i led f i l ters , young
patients, neovascular glaucoma, glaucoma associated with uveitis, andglaucomas following cataract and other ocular surgery. Hithin thishigh)ris# group, implant surgery was not as effective in controlling I$%as trabeculectomy with -->, but was somewhat more effective thancyclophotocoagulation


















