
Guided implant surgery and immediate implant placement in ...ijmdcr.com/eJournals/_eJournals/92_CASE...
5
1 International Journal of Medical and Dental Case Reports (2018), Article ID 180618, 5 Pages CASE REPORT Guided implant surgery and immediate implant placement in esthetic zone Afsheen Tabassum 1,2 1 Department of Preventive Dentistry, Princess Nourah Bint Abdulrahman University, College of Dentistry Riyadh, Kingdom of Saudi Arabia, 2 Department of Oral Implantology and Prosthetic Dentistry, Academic Centre for Dentistry Amsterdam (ACTA), University of Amsterdam and Vrije University Amsterdam, Gustav Mahlerlaan 3004, 1081 LA Amsterdam, the Netherlands Abstract With the introduction of digital imaging techniques such as computerized tomography (CT) and lately cone beam computed tomography (CBCT), anatomical structures of the oral and maxillofacial region can be appreciated in three dimensions. The aim of this article is to familiarize clinicians with a workflow for guided implant surgery based on the use of CBCT and intraoral scanner in case of immediate implant placement. A CBCT was recorded for the patient and a digital impression was registered using an intraoral scanner (Lava COS). Codiagnostix® software was used for the coupling of cone beam computed tomography (CBCT) and intraoral scan data and virtual treatment planning. Ideal implant position and suprastructure were planned by digitally integrating the anatomic situations and future prosthetic demands. In the present case, digital planning software and fabricated surgical guide were beneficial in accurate immediate implant placement in the esthetic zone. The positioning of implants is more precise with guided implant surgery which will help clinicians to achieve prosthetically driven implant placement as it offers many advantages in terms of favorable esthetic, desirable occlusion, phonetics, and long-term peri-implant hard and soft tissues stability. Keywords: Dental implants, guided surgery, oral implantology Correspondence: Afsheen Tabassum, Department of Preventive Dentistry, Princess Nourah Bint Abdulrahman University, College of Dentistry Riyadh, PO Box 84428, Kingdom of Saudi Arabia. Phone: 00966-536051182. E-mail: afshali114@gmail. com Received 1 May 2018; Accepted 20 June 2018 doi: 10.15713/ins.ijmdcr.92 How to cite this article: Tabassum A, Guided implant surgery and immediate implant placement in esthetic zone. Int J Med Dent Case Rep 2018;5:1-5. Introduction The field of implant dentistry has entered in a new era due to advances in computer-aided design/computer-assisted manufacture (CAD/CAM) technology. [1] With the introduction of CBCT, anatomical structures of the oral and maxillofacial region can be appreciated in three dimensions. CBCT scanners are smaller in size, employ low radiation dose, and cost-effective as compared to the computerized tomography (CT) scanning devices. [2] The images obtained from CBCT can be transformed to a simulated three-dimensional model of the jaws. [3] In addition, intraoral scanning machines have recently started to play a key role in modern dentistry with respect to digital treatment planning. [4] The digital planning involves the coupling of digital imaging and communications in medicine (DICOM) format data from CBCT and standard triangulation language (STL) file data from an intraoral scanner. [3,4] With the help of digital planning, software identifiable structures (e.g., teeth) obtained from CBCT images and intraoral scanning is superimposed on each other. A 3D view of the dental hard and soft tissues of a patient is created by the software which gives a realistic view of the anatomical structures of the patient. Subsequently, surgeons can virtually execute the implant surgery in an accurate manner. A digital tooth setup can also be added to this treatment planning to assist the dental technician in relation to the future prosthetic restoration. [5] Finally, this process results in the transfer of virtual implant treatment planning from the computer to the surgical site. This function is completed by the fabrication of surgical guides by rapid prototyping technique or stereolithographic technology. [5,6] With this case report, the author describes a workflow for guided implant surgery in case of immediate implant placement based on the use of CBCT and intraoral scanner. The 3D implant planning software (Codiagnostix®) assisted the author to digitally plan the treatment of a patient and to design and fabricate a surgical guide for immediate implant placement in the esthetic zone. Case Report A 62-year-old male patient presented to the Department of Oral Function and Restorative Dentistry/Section Oral
Transcript of Guided implant surgery and immediate implant placement in ...ijmdcr.com/eJournals/_eJournals/92_CASE...
1
International Journal of Medical and Dental Case Reports (2018), Article ID 180618, 5 Pages
C A S E R E P O R T
Guided implant surgery and immediate implant placement in esthetic zoneAfsheen Tabassum1,2
1Department of Preventive Dentistry, Princess Nourah Bint Abdulrahman University, College of Dentistry Riyadh, Kingdom of Saudi Arabia, 2Department of Oral Implantology and Prosthetic Dentistry, Academic Centre for Dentistry Amsterdam (ACTA), University of Amsterdam and Vrije University Amsterdam, Gustav Mahlerlaan 3004, 1081 LA Amsterdam, the Netherlands
AbstractWith the introduction of digital imaging techniques such as computerized tomography (CT) and lately cone beam computed tomography (CBCT), anatomical structures of the oral and maxillofacial region can be appreciated in three dimensions. The aim of this article is to familiarize clinicians with a workflow for guided implant surgery based on the use of CBCT and intraoral scanner in case of immediate implant placement. A CBCT was recorded for the patient and a digital impression was registered using an intraoral scanner (Lava COS). Codiagnostix® software was used for the coupling of cone beam computed tomography (CBCT) and intraoral scan data and virtual treatment planning. Ideal implant position and suprastructure were planned by digitally integrating the anatomic situations and future prosthetic demands. In the present case, digital planning software and fabricated surgical guide were beneficial in accurate immediate implant placement in the esthetic zone. The positioning of implants is more precise with guided implant surgery which will help clinicians to achieve prosthetically driven implant placement as it offers many advantages in terms of favorable esthetic, desirable occlusion, phonetics, and long-term peri-implant hard and soft tissues stability.
Keywords: Dental implants, guided surgery, oral implantology
Correspondence: Afsheen Tabassum, Department of Preventive Dentistry, Princess Nourah Bint Abdulrahman University, College of Dentistry Riyadh, PO Box 84428, Kingdom of Saudi Arabia. Phone: 00966-536051182. E-mail: [email protected]
Received 1 May 2018; Accepted 20 June 2018
doi: 10.15713/ins.ijmdcr.92
How to cite this article: Tabassum A, Guided implant surgery and immediate implant placement in esthetic zone. Int J Med Dent Case Rep 2018;5:1-5.
Introduction
The field of implant dentistry has entered in a new era due to advances in computer-aided design/computer-assisted manufacture (CAD/CAM) technology.[1] With the introduction of CBCT, anatomical structures of the oral and maxillofacial region can be appreciated in three dimensions. CBCT scanners are smaller in size, employ low radiation dose, and cost-effective as compared to the computerized tomography (CT) scanning devices.[2] The images obtained from CBCT can be transformed to a simulated three-dimensional model of the jaws.[3] In addition, intraoral scanning machines have recently started to play a key role in modern dentistry with respect to digital treatment planning.[4] The digital planning involves the coupling of digital imaging and communications in medicine (DICOM) format data from CBCT and standard triangulation language (STL) file data from an intraoral scanner.[3,4] With the help of digital planning, software identifiable structures (e.g., teeth) obtained from CBCT images and intraoral scanning is superimposed on each other. A 3D view of the dental hard and soft tissues of a patient is created by the software which gives a realistic view of
the anatomical structures of the patient. Subsequently, surgeons can virtually execute the implant surgery in an accurate manner. A digital tooth setup can also be added to this treatment planning to assist the dental technician in relation to the future prosthetic restoration.[5] Finally, this process results in the transfer of virtual implant treatment planning from the computer to the surgical site. This function is completed by the fabrication of surgical guides by rapid prototyping technique or stereolithographic technology.[5,6]
With this case report, the author describes a workflow for guided implant surgery in case of immediate implant placement based on the use of CBCT and intraoral scanner. The 3D implant planning software (Codiagnostix®) assisted the author to digitally plan the treatment of a patient and to design and fabricate a surgical guide for immediate implant placement in the esthetic zone.
Case Report
A 62-year-old male patient presented to the Department of Oral Function and Restorative Dentistry/Section Oral
Tabassum Guided implant surgery
2
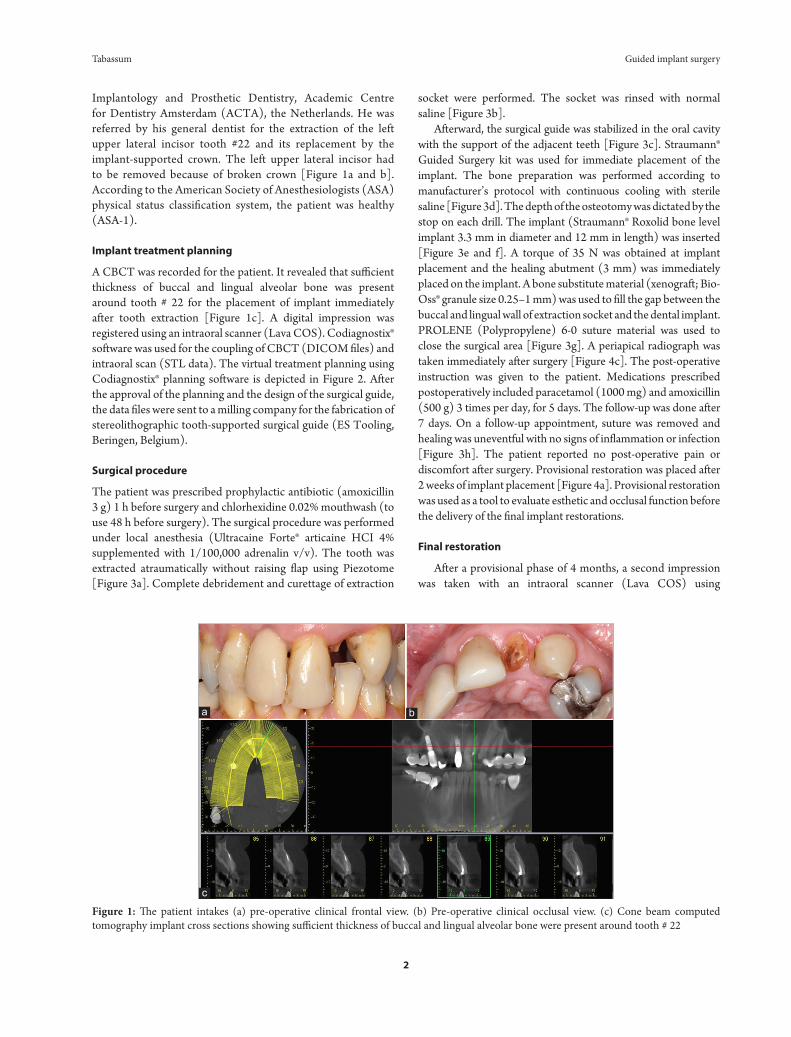
Implantology and Prosthetic Dentistry, Academic Centre for Dentistry Amsterdam (ACTA), the Netherlands. He was referred by his general dentist for the extraction of the left upper lateral incisor tooth #22 and its replacement by the implant-supported crown. The left upper lateral incisor had to be removed because of broken crown [Figure 1a and b]. According to the American Society of Anesthesiologists (ASA) physical status classification system, the patient was healthy (ASA-1).
Implant treatment planning
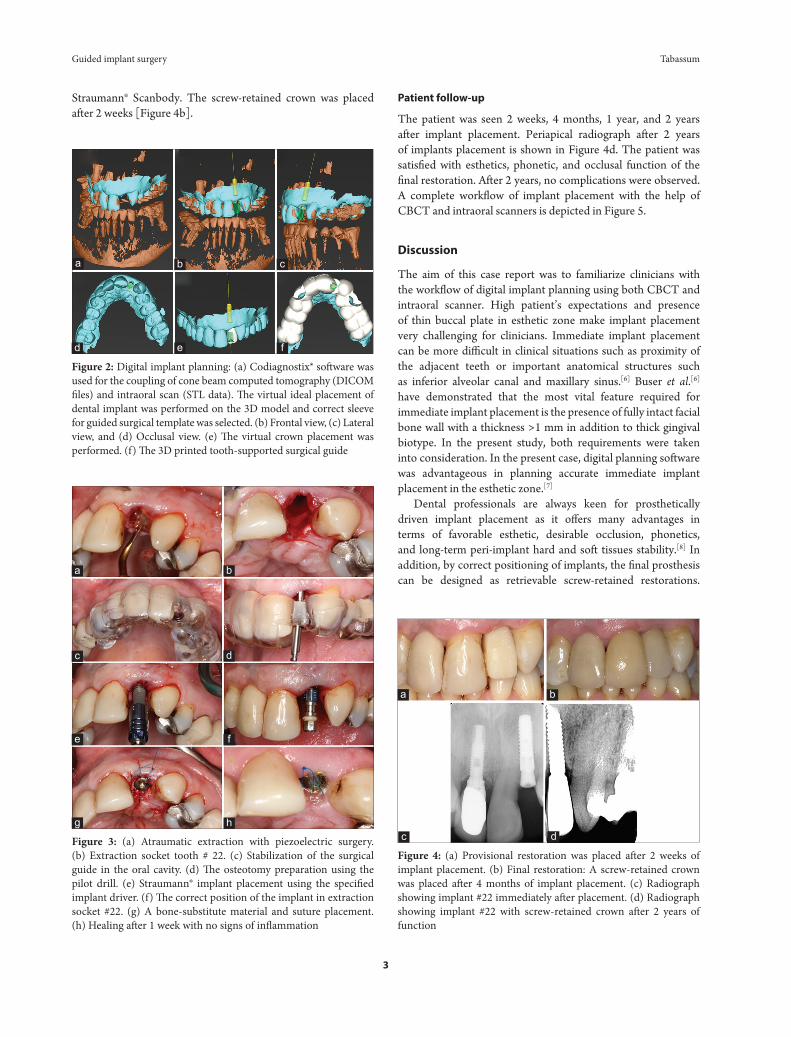
A CBCT was recorded for the patient. It revealed that sufficient thickness of buccal and lingual alveolar bone was present around tooth # 22 for the placement of implant immediately after tooth extraction [Figure 1c]. A digital impression was registered using an intraoral scanner (Lava COS). Codiagnostix® software was used for the coupling of CBCT (DICOM files) and intraoral scan (STL data). The virtual treatment planning using Codiagnostix® planning software is depicted in Figure 2. After the approval of the planning and the design of the surgical guide, the data files were sent to a milling company for the fabrication of stereolithographic tooth-supported surgical guide (ES Tooling, Beringen, Belgium).
Surgical procedure
The patient was prescribed prophylactic antibiotic (amoxicillin 3 g) 1 h before surgery and chlorhexidine 0.02% mouthwash (to use 48 h before surgery). The surgical procedure was performed under local anesthesia (Ultracaine Forte® articaine HCI 4% supplemented with 1/100,000 adrenalin v/v). The tooth was extracted atraumatically without raising flap using Piezotome [Figure 3a]. Complete debridement and curettage of extraction
socket were performed. The socket was rinsed with normal saline [Figure 3b].
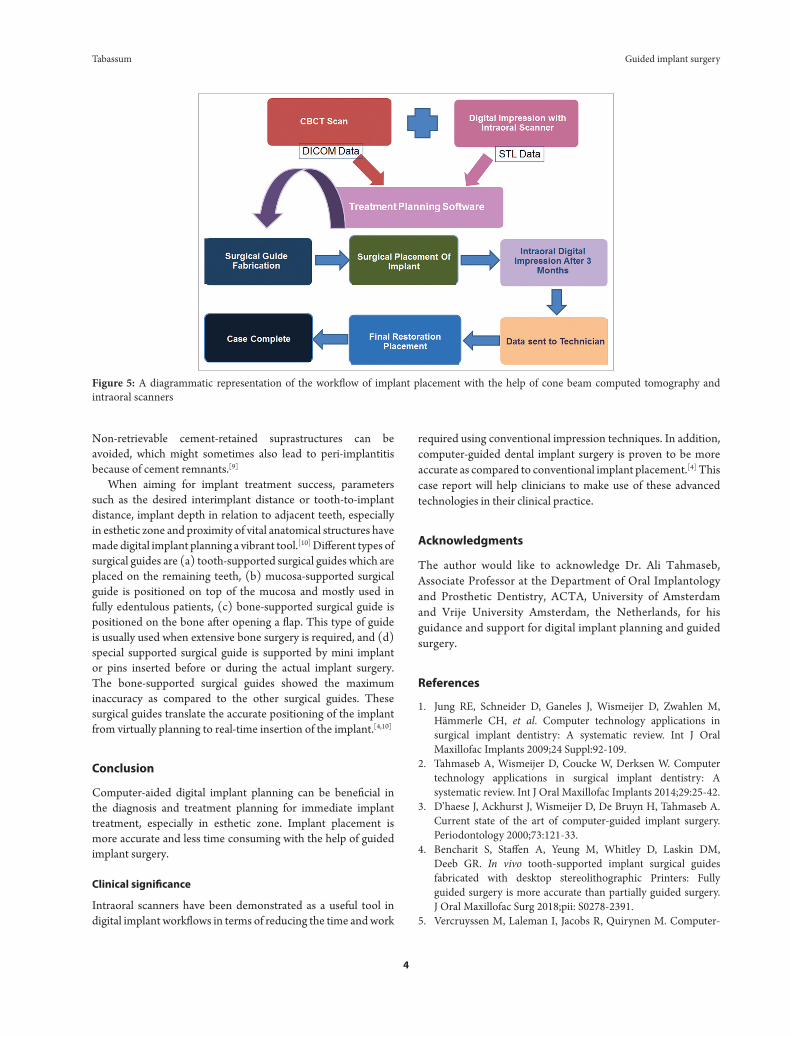
Afterward, the surgical guide was stabilized in the oral cavity with the support of the adjacent teeth [Figure 3c]. Straumann® Guided Surgery kit was used for immediate placement of the implant. The bone preparation was performed according to manufacturer’s protocol with continuous cooling with sterile saline [Figure 3d]. The depth of the osteotomy was dictated by the stop on each drill. The implant (Straumann® Roxolid bone level implant 3.3 mm in diameter and 12 mm in length) was inserted [Figure 3e and f]. A torque of 35 N was obtained at implant placement and the healing abutment (3 mm) was immediately placed on the implant. A bone substitute material (xenograft; Bio-Oss® granule size 0.25–1 mm) was used to fill the gap between the buccal and lingual wall of extraction socket and the dental implant. PROLENE (Polypropylene) 6-0 suture material was used to close the surgical area [Figure 3g]. A periapical radiograph was taken immediately after surgery [Figure 4c]. The post-operative instruction was given to the patient. Medications prescribed postoperatively included paracetamol (1000 mg) and amoxicillin (500 g) 3 times per day, for 5 days. The follow-up was done after 7 days. On a follow-up appointment, suture was removed and healing was uneventful with no signs of inflammation or infection [Figure 3h]. The patient reported no post-operative pain or discomfort after surgery. Provisional restoration was placed after 2 weeks of implant placement [Figure 4a]. Provisional restoration was used as a tool to evaluate esthetic and occlusal function before the delivery of the final implant restorations.
Final restoration
After a provisional phase of 4 months, a second impression was taken with an intraoral scanner (Lava COS) using
Figure 1: The patient intakes (a) pre-operative clinical frontal view. (b) Pre-operative clinical occlusal view. (c) Cone beam computed tomography implant cross sections showing sufficient thickness of buccal and lingual alveolar bone were present around tooth # 22
ba
c
Guided implant surgery Tabassum
3
Straumann® Scanbody. The screw-retained crown was placed after 2 weeks [Figure 4b].
Patient follow-up
The patient was seen 2 weeks, 4 months, 1 year, and 2 years after implant placement. Periapical radiograph after 2 years of implants placement is shown in Figure 4d. The patient was satisfied with esthetics, phonetic, and occlusal function of the final restoration. After 2 years, no complications were observed. A complete workflow of implant placement with the help of CBCT and intraoral scanners is depicted in Figure 5.
Discussion
The aim of this case report was to familiarize clinicians with the workflow of digital implant planning using both CBCT and intraoral scanner. High patient’s expectations and presence of thin buccal plate in esthetic zone make implant placement very challenging for clinicians. Immediate implant placement can be more difficult in clinical situations such as proximity of the adjacent teeth or important anatomical structures such as inferior alveolar canal and maxillary sinus.[6] Buser et al.[6] have demonstrated that the most vital feature required for immediate implant placement is the presence of fully intact facial bone wall with a thickness >1 mm in addition to thick gingival biotype. In the present study, both requirements were taken into consideration. In the present case, digital planning software was advantageous in planning accurate immediate implant placement in the esthetic zone.[7]
Dental professionals are always keen for prosthetically driven implant placement as it offers many advantages in terms of favorable esthetic, desirable occlusion, phonetics, and long-term peri-implant hard and soft tissues stability.[8] In addition, by correct positioning of implants, the final prosthesis can be designed as retrievable screw-retained restorations.
Figure 2: Digital implant planning: (a) Codiagnostix® software was used for the coupling of cone beam computed tomography (DICOM files) and intraoral scan (STL data). The virtual ideal placement of dental implant was performed on the 3D model and correct sleeve for guided surgical template was selected. (b) Frontal view, (c) Lateral view, and (d) Occlusal view. (e) The virtual crown placement was performed. (f) The 3D printed tooth-supported surgical guide
Figure 3: (a) Atraumatic extraction with piezoelectric surgery. (b) Extraction socket tooth # 22. (c) Stabilization of the surgical guide in the oral cavity. (d) The osteotomy preparation using the pilot drill. (e) Straumann® implant placement using the specified implant driver. (f) The correct position of the implant in extraction socket #22. (g) A bone-substitute material and suture placement. (h) Healing after 1 week with no signs of inflammation
Figure 4: (a) Provisional restoration was placed after 2 weeks of implant placement. (b) Final restoration: A screw-retained crown was placed after 4 months of implant placement. (c) Radiograph showing implant #22 immediately after placement. (d) Radiograph showing implant #22 with screw-retained crown after 2 years of function
a b c
d e f
b
d
f
h
a
c
e
g
a b
c d
Tabassum Guided implant surgery
4
Non-retrievable cement-retained suprastructures can be avoided, which might sometimes also lead to peri-implantitis because of cement remnants.[9]
When aiming for implant treatment success, parameters such as the desired interimplant distance or tooth-to-implant distance, implant depth in relation to adjacent teeth, especially in esthetic zone and proximity of vital anatomical structures have made digital implant planning a vibrant tool.[10] Different types of surgical guides are (a) tooth-supported surgical guides which are placed on the remaining teeth, (b) mucosa-supported surgical guide is positioned on top of the mucosa and mostly used in fully edentulous patients, (c) bone-supported surgical guide is positioned on the bone after opening a flap. This type of guide is usually used when extensive bone surgery is required, and (d) special supported surgical guide is supported by mini implant or pins inserted before or during the actual implant surgery. The bone-supported surgical guides showed the maximum inaccuracy as compared to the other surgical guides. These surgical guides translate the accurate positioning of the implant from virtually planning to real-time insertion of the implant.[4,10]
Conclusion
Computer-aided digital implant planning can be beneficial in the diagnosis and treatment planning for immediate implant treatment, especially in esthetic zone. Implant placement is more accurate and less time consuming with the help of guided implant surgery.
Clinical significance
Intraoral scanners have been demonstrated as a useful tool in digital implant workflows in terms of reducing the time and work
required using conventional impression techniques. In addition, computer-guided dental implant surgery is proven to be more accurate as compared to conventional implant placement.[4] This case report will help clinicians to make use of these advanced technologies in their clinical practice.
Acknowledgments
The author would like to acknowledge Dr. Ali Tahmaseb, Associate Professor at the Department of Oral Implantology and Prosthetic Dentistry, ACTA, University of Amsterdam and Vrije University Amsterdam, the Netherlands, for his guidance and support for digital implant planning and guided surgery.
References
1. Jung RE, Schneider D, Ganeles J, Wismeijer D, Zwahlen M, Hämmerle CH, et al. Computer technology applications in surgical implant dentistry: A systematic review. Int J Oral Maxillofac Implants 2009;24 Suppl:92-109.
2. Tahmaseb A, Wismeijer D, Coucke W, Derksen W. Computer technology applications in surgical implant dentistry: A systematic review. Int J Oral Maxillofac Implants 2014;29:25-42.
3. D’haese J, Ackhurst J, Wismeijer D, De Bruyn H, Tahmaseb A. Current state of the art of computer-guided implant surgery. Periodontology 2000;73:121-33.
4. Bencharit S, Staffen A, Yeung M, Whitley D, Laskin DM, Deeb GR. In vivo tooth-supported implant surgical guides fabricated with desktop stereolithographic Printers: Fully guided surgery is more accurate than partially guided surgery. J Oral Maxillofac Surg 2018;pii: S0278-2391.
5. Vercruyssen M, Laleman I, Jacobs R, Quirynen M. Computer-
Figure 5: A diagrammatic representation of the workflow of implant placement with the help of cone beam computed tomography and intraoral scanners

Guided implant surgery Tabassum
5
supported implant planning and guided surgery: A narrative review. Clin Oral Implants Res 2015;26:69-76.
6. Buser D, Chappuis V, Belser SC, Chen S. Implant placement post extraction in esthetic single tooth sites: When immediate, when early, when late? Periodontology 2000;73:84-102.
7. Rungcharassaeng K, Caruso JM, Kan JY, Schutyser F, Boumans T. Accuracy of computer-guided surgery: A comparison of operator experience. J Prosthet Dent 2015;114:407-13.
8. Gunkel AR, Freysinger W, Thumfart WF. Experience with
various 3-dimensional navigation systems in head and neck surgery. Arch Otolaryngol Head Neck Surg 2000;126:390-5.
9. van der Meer WJ, Andriessen FS, Wismeijer D, Ren Y. Application of intra-oral dental scanners in the digital workflow of implantology. PLoS One 2012;7:e43312.
10. Ozan O, Turkyilmaz I, Ersoy AE, McGlumphy EA, Rosenstiel SF. Clinical accuracy of 3 different types of computed tomography-derived stereolithographic surgical guides in implant placement. J Oral Maxillofac Surg 2009;67:394-401.
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/ © Tabassum A. 2018


















