Venous thromboembolism (VTE) in obstetrics Dr. Yasir Katib MBBS, FRCSC, Perinatologist.
Upload
polly-petersCategory
view
226download
0
Dr. Yasir KatibMBBS, FRCSC, Perinatologest

Objectives Basic principlesIndications and contraindications of induction
of labourMethods of inductionPrediction of successInduction after cesarean

Histology The fundus is composed of myometrium,
predominantly smooth muscle cells and the endometrium
The normal pregnant cervix is 3.5 cm or longer and is composed predominantly of connective tissue, mainly collagen. In contrast to the fundus, it has only 10-15% smooth muscle

Introduction Definition It is an iatrogenic stimulation of uterine contractions to
accomplish delivery prior to the onset of spontaneous labor
Induction of labour is done when the benefits of expeditious delivery outweigh the potential maternal or fetal risks of the procedure
Rate 15-25%
Indications Either maternal or fetal indications with the
following criteria :1.Continuing the pregnancy is believed to be
associated with greater maternal or fetal risk than intervention to deliver the pregnancy
2.There is no contraindication to vaginal birth

IndicationsExamples of common and Obstetrical conditions postterm pregnancyprelabor (premature) rupture of membranesintrauterine fetal growth restriction fetal demise Medical conditionspreeclampsia/eclampsiaGDM on insulin

Gestational Age at Induction
11%24%
65%
34-37 wks 37-41wks > 41 wks
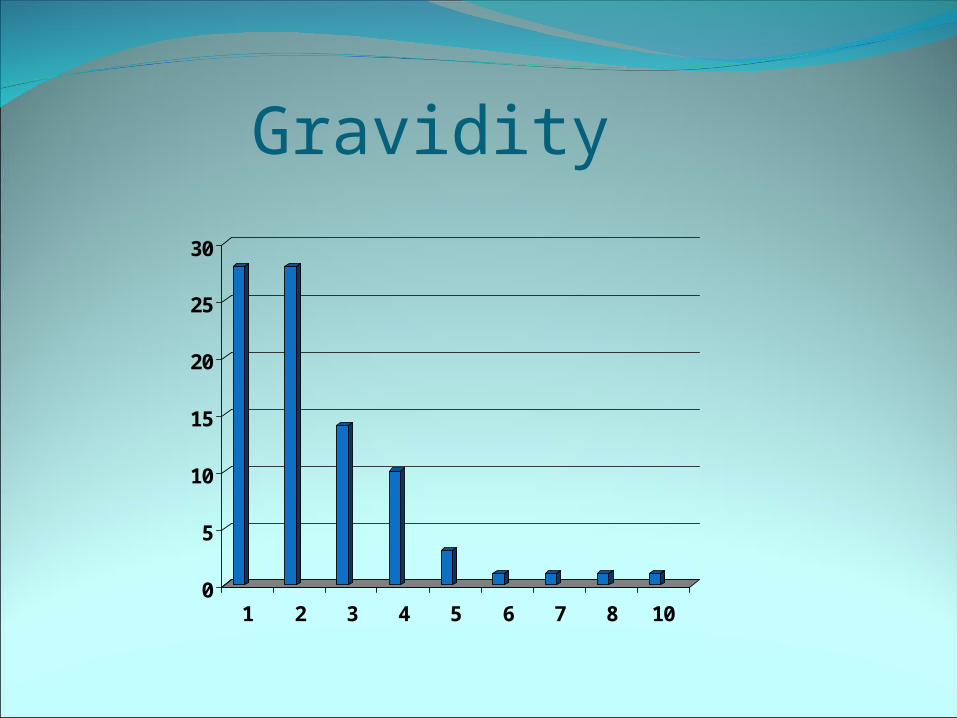
Gravidity
0
5
10
15
20
25
30
1 2 3 4 5 6 7 8 10

Parity
0
5
10
15
20
25
30
35
40
Fre
qu
ency
0 1 2 3 4 5 6 7 8
Parity
Concerns Major concerns Increase rates of cesarean deliveryIatrogenic prematurityCostNeonatal safetyMaternal safetyInfection

Contra-indications Absolute Prior classical uterine incision Prior transmural uterine incision entering the uterine cavity Active genital herpes infection Placenta or vasa previa Umbilical cord prolapse Transverse fetal lie
Relative (with caution)previous low transverse cesarean deliverymultifetal pregnancy
Methods of induction Mechanical 1.Membrane sweep2.Artificial rupture of membrane3.Balloon catheter 4.Laminaria Hormonal1.Prostaglandin 2.Oxytocin Natural methods1.Caster oil


Methods of Induction
05
10
15202530
354045
Oxy Oxy +ARM
PG + Oxy
PG + Oxy+ ARM
ARM
Cervical ripening Associated with cervical ripening is an increase in
the enzyme cyclooxygenase-2, which leads to a local increase of prostaglandin E2 (PGE2) in the cervix that led to:
1.Dilatation of small vessels in the cervix2.Increase in collagen degradation3.Increase in hyaluronic acid4.Increase in chemotaxis for leukocytes, which
causes increased collagen degradation5.Increase in stimulation of interleukin (IL)–8
release


PREDICTING A SUCCESSFUL INDUCTIONUsing Bishop scoreScore < 5 suggests further ripening is
neededScore 5-7 is equivocal score >7 suggests that ripening is completed

Type of Delivery
SVD79%
Forceps0%
C/S14%
Vac7%

Induction after cesareanInduced labor after cesarean delivery have a
2- to 3-fold increased risk of cesarean delivery compared with those who present with spontaneous labor
Associated risks:1.Rupture of uterus2.Emergency cesarean