
Dr. Ganasani
54
Sreeni Gangasani, M.D. • Cardiologist at Gwinnett Heart Specialists • American Board of Internal Medicine Cardiovascular Disease • American Board of Internal Medicine Internal Medicine • AOA Board of Internal Medicine Cardiology • Special interests include general Cardiology, Echocardiography, Nuclear, Preventive Cardiology Medical School: Kurnool Medical College Residency: William Beaumont Hospital Fellowship: William Beaumont Hospital
-
Upload
athens-heart-center-specialty-clinics -
Category
Health & Medicine
-
view
33 -
download
2
Transcript of Dr. Ganasani
Sreeni Gangasani, M.D.• Cardiologist at Gwinnett Heart
Specialists
• American Board of Internal Medicine Cardiovascular Disease
• American Board of Internal MedicineInternal Medicine
• AOA Board of Internal MedicineCardiology
• Special interests include general Cardiology, Echocardiography, Nuclear, Preventive Cardiology
Medical School:Kurnool Medical College
Residency:William Beaumont
Hospital
Fellowship:William Beaumont
Hospital
Tailoring NOAC’s for your individual patient
Sreeni Gangasani MD, FACC

04/18/2023 Gwinnett Heart Specialists
• 1. We hate sleeping.2. We have enjoyed our life in childhood.3. We can't live without tension.4. We want to have a disturbed life.5. We want to take revenge on ourselves.6. We love dreaming about diseases .7. We love to work on holidays.8. We can't live without mobile hooked on our ears even in the bathroom .9.When we make money its already too late
9 reasons why we chose Medicine as a profession:
04/18/2023 Gwinnett Heart Specialists
• Which one is the newest of direct Factor X inhibitors ?
• A) Darbigatran• B) Edoxaban• C) Rivaraxoban• D) Epixaban• E) Betrixaban
Question 1


Newer Anti-coagulants(NOAC)(Dabigatran/Rivaroxaban/Apix
aban/Edoxaban)
Practical Issues
04/18/2023 Gwinnett Heart Specialists
• Prevention and treatment of venous thromboembolism (VTE)
• Stroke prophylaxis in non-valvular atrial fibrillation (AF),
Newer Oral Anticoagulants

04/18/2023 Gwinnett Heart Specialists
• Low-molecular-weight heparin (LMWH) or unfractionated heparin (UFH) is used initially in the treatment of acute VTE or A fib, followed by long-term vitamin K antagonist (VKA) therapy.
• For stroke prophylaxis in AF, long-term anticoagulation with the VKA warfarin is the standard of care
Traditional care

04/18/2023 Gwinnett Heart Specialists
• Inter patient variability with regard to clinical response because of genetic polymorphisms, particularly upon initiating therapy.
• Drug-drug and drug-food interactions necessitate more frequent monitoring of international normalized ratio (INR) and may complicate management.
• Major and non–major bleeding events,• Supra and Sub therapeutic INRs management• In older patients, warfarin is the most common
cause of drug-related emergency hospitalization
Problems with Warfarin

04/18/2023 Gwinnett Heart Specialists
04/18/2023 Gwinnett Heart Specialists
Edoxoban
04/18/2023 Gwinnett Heart Specialists
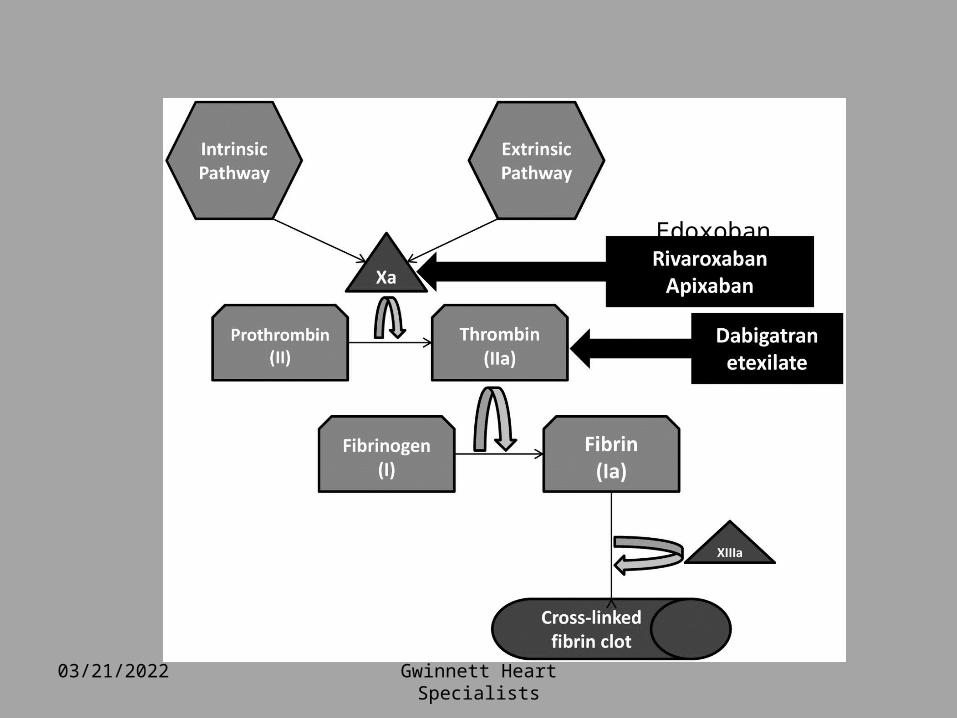
• Dabigatran and Rivaroxaban and Apixaban Edoxaban have successfully completed phase III trials for acute VTE treatment, Prophylaxis and are currently approved for the reduction of risk of stroke and systemic embolism in patients with non-valvular AF
Newer Anticoagulants

04/18/2023 Gwinnett Heart Specialists
• Direct thrombin inhibitors
- dabigatran( Pradaxa)
Factor IIa Inhibitors

04/18/2023 Gwinnett Heart Specialists
• The pro-drug dabigatran etexilate is converted
completely to active dabigatran
• Terminal elimination t½ of 14–17 hours
• Bioavailability of 3.5–6.5%
• No food interactions
• Eliminated mainly by renal excretion (80%)
Dabigatran (Pradaxa)
Stangier et al. J Clin Pharmacol 2005; Liesenfeld et al. Br J Clin Pharmacol 2006;
Stangier et al. Br J Clin Pharmacol 2007
04/18/2023 Gwinnett Heart Specialists
• Must be stored in the original blister pack with desiccant and not crushed.
Dabigatran
04/18/2023 Gwinnett Heart Specialists
VIIa
Xa
IXa
XIa
XIIa
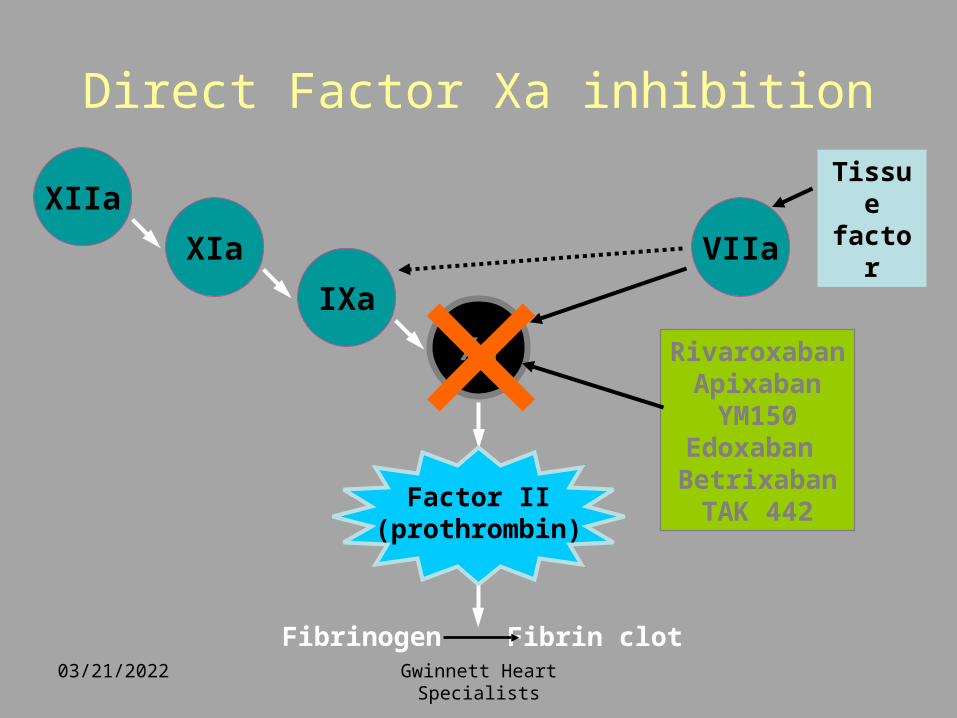
Direct Factor Xa inhibitionTissue factor
Fibrinogen Fibrin clot
Factor II(prothrombin)
RivaroxabanApixaban
YM150Edoxaban Betrixaban
TAK 442
×

04/18/2023 Gwinnett Heart Specialists
Direct Factor Xa Inhibitors
Rivaroxaban (Xarelto)
Apixaban (Eliquis)
Edoxaban( Savaysa)
Rivaroxaban: oral direct Factor Xa inhibitor (Xarelto)
• Predictable pharmacology
• High bioavailability • Low risk of drug–
drug interactions• Fixed dose• No requirement for
monitoringPerzborn et al. 2005; Kubitza et al. 2005; 2006; 2007; Roehrig et al, 2005
Rivaroxaban® – rivaroxaban
N NO
NH
O
SCl
O
O
O
Gwinnett Heart Specialists 04/18/2023
Apixaban(Eliquis)• Oral, direct, selective factor Xa inhibitor• Produces concentration-dependent
anticoagulation• No formation of reactive intermediates• No organ toxicity or LFT abnormalities in
chronic toxicology studies • Low likelihood of drug interactions or QTc
prolongation• Good oral bioavailability • No food effect • Balanced elimination (~25% renal) • Half-life ~12 hrs
He et al., ASH, 2006, Lassen, et al ASH, 2006
N
N
NO
N O
NH2
O
O
Gwinnett Heart Specialists04/18/2023

Edoxaban( Savaysa)
• Half-life:6-11 hrs• Dosing 30 or 60 mg orally once daily• Absorption is unaffected by food• Renally excreted• Substrate for P glycoprotein• Reduced efficacy in nonvalvular atrial
fibrillation in patients with a high creatinine clearance
(CrCL >95 mL/minute)04/18/2023 Gwinnett Heart Specialists

04/18/2023 Gwinnett Heart Specialists
• Laboratory testing should include • Prothrombin time (PT) • Activated partial thromboplastin time
(aPTT),
• Serum creatinine, as a baseline and for potential dose adjustment in the event of renal insufficiency.
Testing before starting NOAC
04/18/2023 Gwinnett Heart Specialists
• NOAC are contraindicated in what valvular heart disease conditions ?
• A) Moderate mitral regurgitation• B) Mild Aortic stenosis• C) Moderate to severe tricuspid
regurgitation• D) Prosthetic mechanical aortic valve• E)Bicuspid aortic valve with minimal aortic
regurgitation
Question 2

04/18/2023 Gwinnett Heart Specialists
• Many of the major clinical trials subsequent meta-analyses have excluded patients with
• prosthetic heart valves, • with mitral stenosis, • with decompensated valvular heart
disease who were likely to require valve replacement in the near future.
• Based on these studies, the newer anticoagulants should not be prescribed for these patients
Valvular heart disease and NAC

04/18/2023 Gwinnett Heart Specialists
• Which of the NOAC is approved for use in ESRD?
• A) Epixaban• B) rivaroxoban• C) Edoxaban• D) None of the above
Question 3


04/18/2023 Gwinnett Heart Specialists
Renal Insufficiency

04/18/2023 Gwinnett Heart Specialists
Time to fully active: 5 days vs 2-3 hrs
Time to being out of system :5-7 days vs 24-48hrs
Cost : NOAC more expensive(About $200/month)
Safety:• Same risk of major bleeding, but lower risk of
bleeds into the head with NOAC
Differences between VKA vs NOAC

04/18/2023 Gwinnett Heart Specialists
Factor WarfarinEnoxaparin (LMWH)
Dabigatran etexilate
Rivaroxaban Apixaban
Routine laboratory monitoring required
X
Antidote available
X X
Dose adjustment for renal insufficiency
X X X X
Rapid onset and offset of action
X X X
Comparison of key considerations for new oral anticoagulants
FactorWarfarin
Enoxaparin (LMWH) Dabigatran Rivaroxaban Apixaban
Routine laboratory monitoring required
X
Antidote available X X
Dose adjustment for renal insufficiency
X X X X
Rapid onset and offset of action
X X X
04/18/2023 Gwinnett Heart Specialists
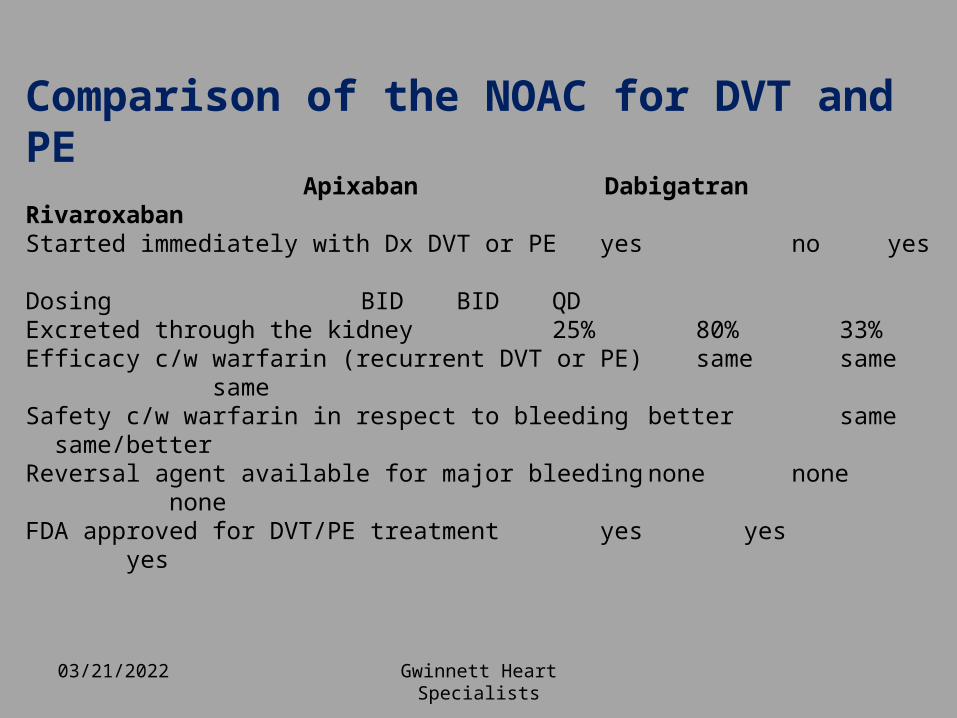
Comparison of the NOAC for DVT and PE Apixaban Dabigatran Rivaroxaban
Started immediately with Dx DVT or PE yes no yes Dosing BID BID QD
Excreted through the kidney 25% 80% 33%
Efficacy c/w warfarin (recurrent DVT or PE) same same same
Safety c/w warfarin in respect to bleeding better same same/better
Reversal agent available for major bleeding none none none
FDA approved for DVT/PE treatment yes yes yes
04/18/2023 Gwinnett Heart Specialists
• 68% relative risk (RR) reduction of ischemic stroke compared with placebo;
• Aspirin has a less-robust RR reduction of 21% compared with placebo
Warfarin

Gwinnett Heart Specialists
04/18/2023

04/18/2023 Gwinnett Heart Specialists

04/18/2023 Gwinnett Heart Specialists

04/18/2023 Gwinnett Heart Specialists
• Difficult achieving stable anti-coagulation
• Drugs proven to cause INR fluctuations
• Better compliance with once a day than bid (rivaroxiban vs dabigatran/apixaban)
Who should switch?

04/18/2023 Gwinnett Heart Specialists
• GI bleeds (increased risk with dabigatran and rivaroxiban) either stay on VKA or apixaban
• Previous acute coronary syndromes??? Conflicting data with dabigatran
• Populations excluded from trials: pediatric, pregnant patients, prosthetic valves (Re-ALIGN a negative trial)
Who should NOT switch?
04/18/2023 Gwinnett Heart Specialists
• When to stop NOACs?• Risk of stroke when off ACs• Duration off vs CHADS2 score
How to deal with Surgery?

04/18/2023 Gwinnett Heart Specialists
How to deal with Surgery?
04/18/2023 Gwinnett Heart Specialists
• Depends on CHADS2
• For CHADS2 of ≥3 use bridge with lovenox or IV Heparin
Risk of stroke off Anticoagulants
04/18/2023 Gwinnett Heart Specialists
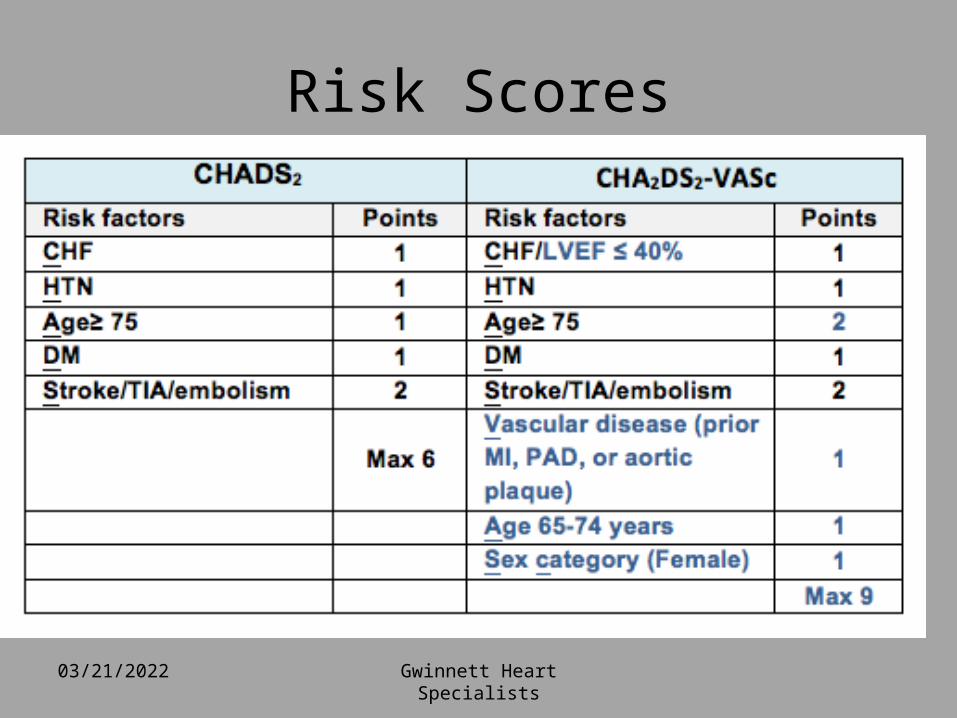
Risk Scores
04/18/2023 Gwinnett Heart Specialists
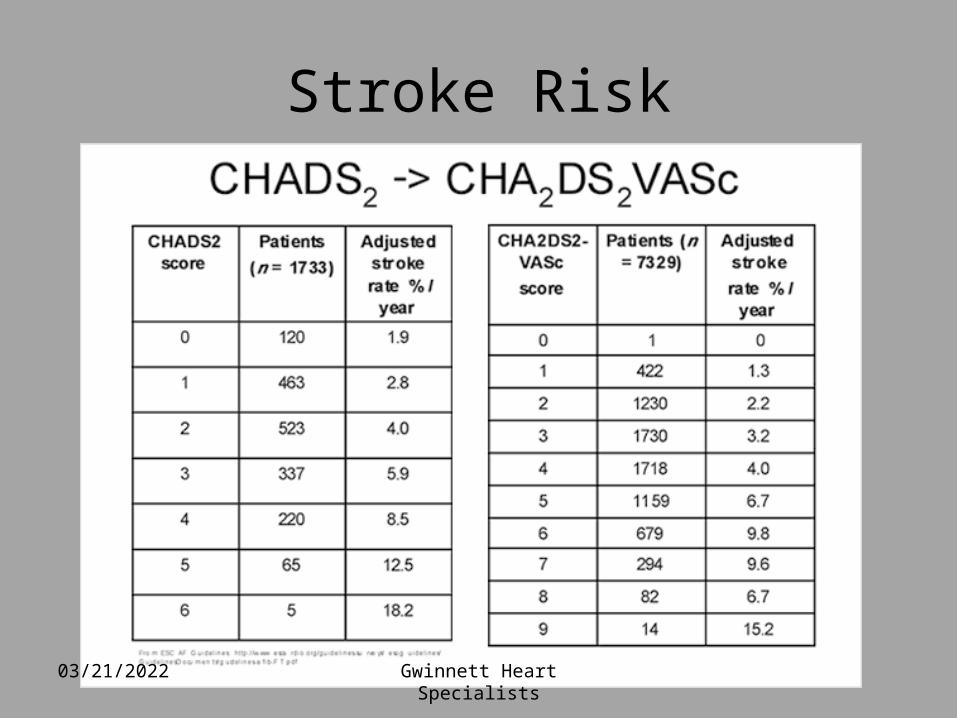
Stroke Risk
04/18/2023 Gwinnett Heart Specialists
• NOACs discontinued and procedure schedules 1-2 days later….if possible
• Risk of bleeding vs risk of delaying surgery
How to deal with Urgent Surgery?

04/18/2023 Gwinnett Heart Specialists
• Which of the NOAC is class B in Pregnancy?
• A) Endoxaban• B) Epixaban• C) Darbigatran• D)Rivaraxoban
Question 4

04/18/2023 Gwinnett Heart Specialists
• Eliquis: Class B ( No adverse effects demonstrated but not enough data)
• Xarelto: Class C ( Use with caution)• Pradaxa : Class C
• Lactation: Not indicated(safety unknown)
Pregnancy and Lactation
04/18/2023 Gwinnett Heart Specialists
• Ecarin clotting time has shown to be a reliable assay to assess coagulation in patients taking dabigatran etexilate
• Availability of this assay is limited . • Prothrombin time assays may be useful for
assessing coagulation in patients receiving rivaroxaban or apixaban (dilute prothrombin time), but because of a lack of standardization, as is the case with INR, results may be difficult to interpret.
• Anti–factor Xa assays used for nonroutine monitoring of LMWHs may prove to be the best method to monitor rivaroxaban or apixaban
Laboratory monitoring

04/18/2023 Gwinnett Heart Specialists
• The new oral anticoagulants do not have specific antidotes
• For non–major bleeding events, temporary cessation
• Activated prothrombin complex concentrates (PCCs) and recombinant factor VII have been explored in early studies as reversal agents for the new anticoagulants, but data are limited
Management of bleeding events

04/18/2023 Gwinnett Heart Specialists
• A study in healthy human subjects demonstrated that 4-factor PCCs that are available in Europe immediately and completely reverse the effect of rivaroxaban, but they did not have any influence on dabigatran at the dose studied.
• Recombinant factor Xa is currently being explored as a reversal agent for factor Xa inhibitors
Management of bleeding events
04/18/2023 Gwinnett Heart Specialists
• Emergency dialysis may be considered
• Partially dialyzable,
• Maintain renal perfusion with intravenous fluids.
• Need to develop protocols for institution for major bleeds
Darbitrigan

04/18/2023 Gwinnett Heart Specialists

04/18/2023 Gwinnett Heart Specialists
• Name: Husband Symbol: Hb
• Atomic Weight:-Light when first found...-tends to get heavier over the years with time.
•Physical Properties :- Boils at any time with inlaws- Melts if sees other women- Very Bitter if questioned
• Chemical Properties :- Very Reactive- Highly Unstable- Possess Strong resistance to Gold, Silver,Diamond, Platinum, Credit cards&Cheque books
• Occurrence :- Mostly found in front of the TV
A new metal is added to chemistry:
04/18/2023 Gwinnett Heart Specialists
• Which NOAC should not be used when Cr Cl is over 95?
• A) Endoxoban• B) Epixaban• C) rivaraxoban• D) Darbigatran
Question 5:

04/18/2023 Gwinnett Heart Specialists
• No data head to head between agents
• Insurance
• Familiarity with agent
• Availability of samples
• Side effect profile
• Compliance issues: Qd vs BID
NOAC Agent of choice
04/18/2023 Gwinnett Heart Specialists
04/18/2023 Gwinnett Heart Specialists
Thank You for your attention


















