Dr. Cindy PY Chiu Specialist-in-Psychiatrycme.hkdu.org/files/symposia/handouts/symposium768... ·...
48
Dr. Cindy PY Chiu Specialist-in-Psychiatry MBBS (HK) MRCPSYCH (UK) FHKCPSYCH FHKAM (PSYCHIATRY) DIP MED (CUHK) GRAD DIP CHILD P.S. (MONASH) 13 May 2016
Transcript of Dr. Cindy PY Chiu Specialist-in-Psychiatrycme.hkdu.org/files/symposia/handouts/symposium768... ·...
Dr. Cindy PY Chiu
Specialist-in-PsychiatryMBBS (HK)
MRCPSYCH (UK) FHKCPSYCH
FHKAM (PSYCHIATRY)DIP MED (CUHK)
GRAD DIP CHILD P.S. (MONASH)
13 May 2016

Psychological reaction in adaptation to new
circumstances
Life changes – life events
Reaction is understandably related to the
stressful experience, and in proportion
Individual characteristics taken into account
at least one stressor
Symptoms begin soon after the change
Starts within three months, usually within
one month (ICD-10 criteria)
Social and occupational decline
Symptoms resolution within 6 months upon
removal/ resolution of stressor

A quantified measure of life events
Higher score -> “higher” stress
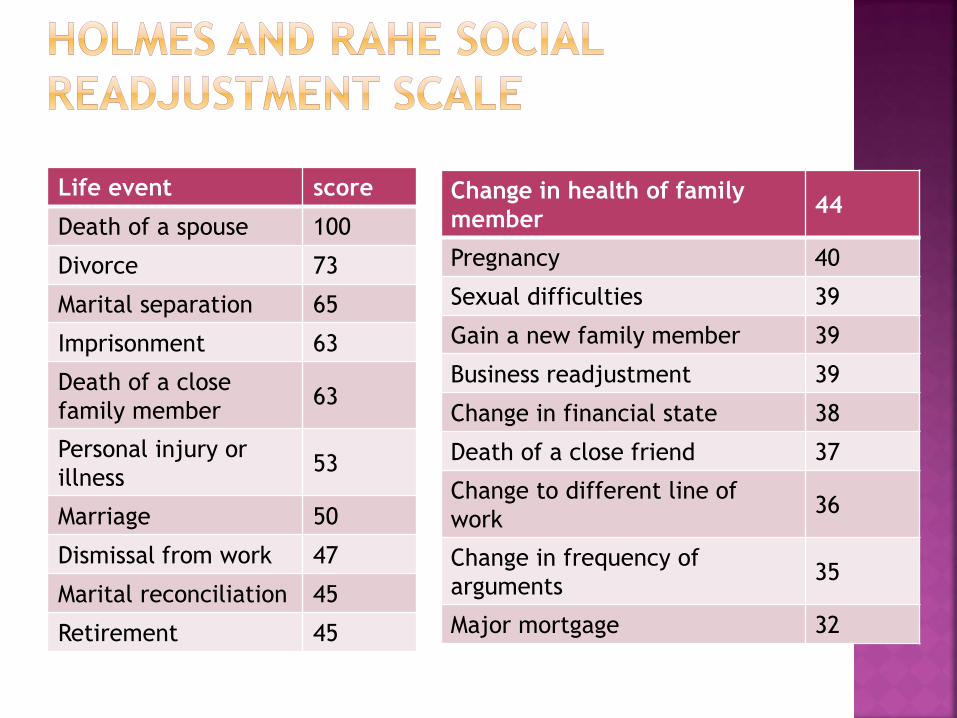
Life event score
Death of a spouse 100
Divorce 73
Marital separation 65
Imprisonment 63
Death of a close
family member63
Personal injury or
illness53
Marriage 50
Dismissal from work 47
Marital reconciliation 45
Retirement 45
Change in health of family
member44
Pregnancy 40
Sexual difficulties 39
Gain a new family member 39
Business readjustment 39
Change in financial state 38
Death of a close friend 37
Change to different line of
work36
Change in frequency of
arguments35
Major mortgage 32

Foreclosure of
mortgage or loan30
Change in
responsibilities at
work
29
Child leaving home 29
Trouble with in-laws 29
Outstanding personal
achievement28
Spouse starts or stops
work26
Begin or end school 26
Change in living
conditions25
Trouble with boss 23
Change in working
hours or conditions20
Change in residence 20
Change in schools 20
Change in recreation 19
Change in social
activities18
Minor mortgage or loan 17
Vacation 13
Christmas 12
Minor violation of law 11

Depressive reaction
Mixed anxiety and depressive reaction
Predominant disturbance of other emotions
Predominant disturbance of conduct
Mixed disturbance of emotions and conduct
Experienced or witnessed extreme stressors (life-threatening scenarios)
Response is intense, prolonged and sometimes delayed
Hyperarousal
Intrusions
Avoidance

Hyperarousal
Persistent anxiety
Insomnia
Irritability
Poor concnetration
hypervigilance
Intrusions
Flashbacks (intrusive imagery)
Recurrent Nightmares
Difficulty in recalling the stressful event at will
Depressive symptoms

Avoidance
Avoidance of the reminders of the event
Detachment
Emotional numbness
Social isolation, withdrawal
Diminished interest in activities
Other symptoms
Guilt (amongst survivors)
Maladaptive coping eg alcohol and substance
abuse
Increased suicide rate, divorce rate

Anyone but not everyone exposed to the
same extreme stressor develop PTSD
Proximity to the stressful situation, length of
exposure
Not limited to Victims, but also firefighters,
rescue workers, health professionals, army,
volunteers, reporters etc
Personality factors – non expressive
Maladaptive coping
History of previous trauma

Mania
Hypomania
Euthymia
Mild to moderate depression
Severe depression

Depressed mood – melancholic, miserable. note diurnal variation, usu. worse in mornings
Pessimistic thoughts
Depressive cognition : past (self reproach, guilt, focusing on unhappy past
events),
present (useless, worthless, hypochondriacal)
Future (hopelessness, pessimism, apprehension, nihilism, life not worth living beware of SUICIDAL IDEATION)
Beck’s cognitive triad (Beck et al 1976) Self (e.g. I am useless and undeserving)
World (e.g. Everyone thinks I am a failure, my children do not respect me, people laugh at me)
Future (e.g. I am doomed, I will lose everything)
Lack of enjoyment – no enjoyment in usual
pleasurable activities
Reduced energy – finds tasks effortful, easily
fatiguable, lethargy, anhedonia
Social withdrawal
Slowness – psychomotor retardation
Agitation and irritability
Cognitive symptoms – poor memory,
decreased concentration or perseverance

Sleep disturbance
Unrefreshed sleep
Early morning wakening – > 2 hours earlier than
usual, lying in bed with pessimistic thoughts,
does not want to get up to face the day
Diurnal variation
Waking in the night, difficulty falling asleep
Some patients may have excessive sleep

Decreased appetite
Not wanting to eat, not hungry
Finds food tasteless, picking at food
Some may have excessive eating and/or binging
Weight loss (>10%)
Loss of libido
Constipation
Amenorrhea (women)
Psychotic symptoms
Delusions – mood congruent (worthlessness,
guilt, persecutory) or mood incongruent
Cotard’s syndrome – nihilistic delusions
hallucinations

Elevated mood –excessive cheerfulness, euphoria, elation, infectious gaiety
Lability of mood
Increased activity –restlessness, physically exhausted
Expansive ideas –grandiosity (can be delusional), recklessness, overspending)
Disinhibition- social, sexual
Irritability and agitation –may be violent
Decreased need for sleep
Increased appetite
Overtalkativity – pressure of speech, flight of ideas, loud-spoken
Thought disorder – racing thoughts, punning, clang association
Delusions of persecution and reference, Hallucinations -congruency vs incongruency with mood
Poor insight (often)
Appearance – brightly-coloured clothing, excessively accessorized, inappropriate dress, overfriendly and verbose

Extreme form of psychomotor retardation
Characterized by muteness and motionless
Some may display catatonic motor
disturbances
Rare
Responds to ECT

Depressed mood most of the time for 2 years
at least (1 year for children, can be irritable
rather than depressed in mood)
Functional impairment
Lifetime prevalence 4.4%
F:M = 2:1
Double depression – depressive episode
superimposed on underlying dysthymia

Chronic fluctuating periods of hypomanic and
depressive symptoms for a 2 year period,
absence of symptoms < 2 months
Lifetime risk around: 0.4-1%
Equal amongst both gender
Onset adolescence or early adulthood
15-50% risk of developing into Bipolar
Disorder

ICD-10 DSM-IV
Depressive episode
Mild, Moderate, Severe, Severe
with psychosis
Major depressive episode
Mild, Moderate, Severe, Severe
with psychosis
Other depressive episodes
Atypical depression
Recurrent depressive disorders
Currently mild
Currently moderate
Currently severe
Currently severe with psychosis
In remission
Major depressive disorder
recurrent
Persistent mood disorders
Cyclothymia
Dysthymia
Dysthymic disorder
Other mood disorders
Recurrent brief depression
Depressive disorder NOS
Recurrent brief depression
Role change
Physical change : illness, hormonal changes
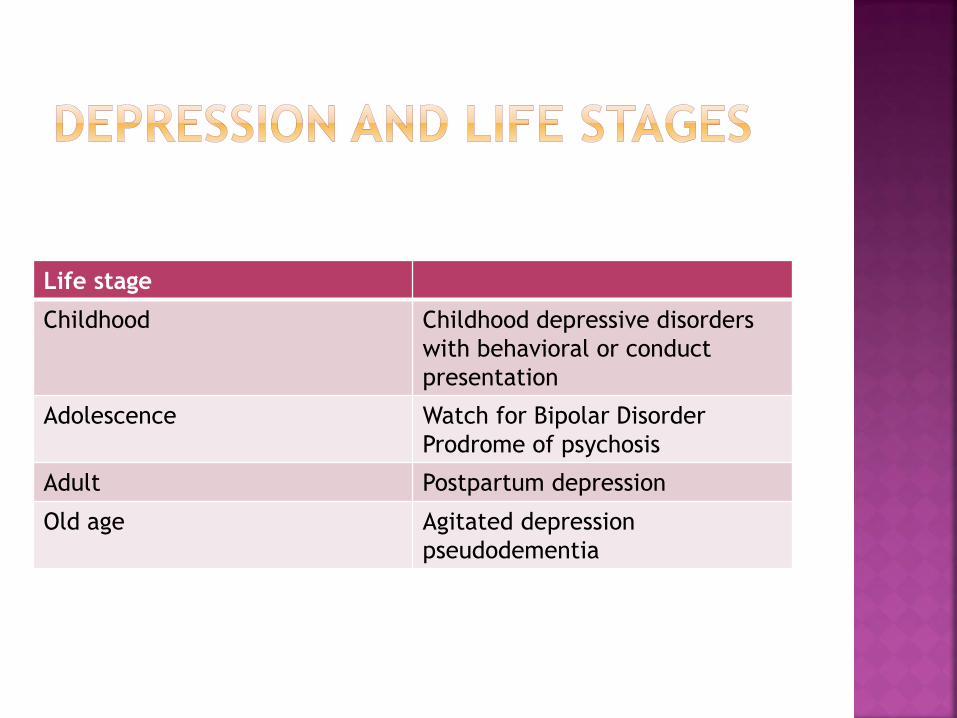
Life stage
Childhood Childhood depressive disorders
with behavioral or conduct
presentation
Adolescence Watch for Bipolar Disorder
Prodrome of psychosis
Adult Postpartum depression
Old age Agitated depression
pseudodementia
Symptoms may not be as typical as in adult
depressive picture
Child may have more somatic symptoms,
refuse school, become weepy and clingy
may become more moody, irritable, get into
trouble in school or become socially isolated
Care to avoid over-diagnosis
need to exclude other possibilities e.g. abuse

Depression in Children and
Adolescents
pre-school Typical depressive features (such as negative
thoughts) may not be evident. May present with
irritability, sadness, crying, agitation.
middle
childhood
Miserable, poor motivation, depressed mood may
be more evident in some children. May present
with headaches, abdominal pain, academic
deterioration, irritability, social withdrawal.
adolescence Clinical picture similar to adults, sleep and appetite
changes, negative outlook with feelings of
worthlessness, low self esteem, behavioural and/or
conduct problems, temper outbursts.
Watch out for drug and alcohol use .
27

Clinical picture similar to adult presentation
Presenting problems may include academic
deterioration, strained relationship with
parents, conduct problems, addiction
problems
may precede psychosis (prodromal phase)
initial episode of Bipolar Affective Disorder
often depressive
consistent with the high rate of switching
32% prepubertal depression prepubertal mania
20% depressed adolescents adolescent-onset
mania

2016/5/27Dr. LIU KWONG SUN 29
Post-partum blues Post-partum depression
Up to 50% 10-15%
Short term emotional
disturbances:
- nervousness, low mood
- irritation
- crying bouts
- poor concentration
- not feeling attached towards
baby
- insomnia
Usually occurs 3-5 days
postpartum and last for 1-2
days, then resolve
Symptoms emerge 3 – 14 days
post-partum:- faitgue, anxiety, tension,
miserable
- insomnia, guilty, loss of
confidence and self esteem
-Poor concentration
- feels ineffective as a mother
-Overworries about own and
baby’s health
-Worries about harming baby
-Suicidal tendency
More severe persistent c.f.
postpartum blues

‧role change to mother
‧lack of experience and perceived lack of ability
to care fo child, overwhelming feeling
‧fatigue and lack of sleep after delivery
‧ overly focused on baby, strain with spouse
‧ restricted social activities and feelings of
isolation
‧ loss of status and earnings, low self esteem
‧ anxiety and “failures” related to perfectionism
‧ previous history of depresion, or mood changes
during pregnancy predispose to postpartum
mood disorders

‧ lack of social support‧ conflicts with spouse, family members over baby care‧ stress from postnatal confinement (坐月) conventions ‧ difficulty dividing attention amongst baby and older children ‧ issues regarding helpers‧ change of residence or job after having new baby‧ financial pressure
+

More commonly seen in middle-aged or
elderly persons
Irritation
Motor agitation
Anger
Hypochondrical symptoms

Reversible condition
Decline of cognitive abilities at least partially
accountable by depressive mood
Objective performance on
neuropsychological tests may be better than
the patient’s subjective perception
During testing – may refuse to perform a task
rather than being unable to perform

Depressed mood Anxiety (psychic)
Feelings of guilt Anxiety (somatic)
Suicide Somatic symptoms (GI)
Insomnia: early in the night General somatic symptoms
Insomnia: middle of the night General symptoms (eg loss of
libido, menstrual disturbance)
Insomnia: early hours of the
morning
Hypochondriasis
Work and activities Weight loss (pt report or weekly
measurements
Retardation insight
agitation

Items are rated from 0-6 with regard to the state over the past
week:
Apparent sadness Concentration difficulties
Reported sadness Lassitude
Inner tension Inability to feel
Reduced sleep Pessimistic thoughts
Reduced appetite Suicidal thoughts
Psychotherapy (especially indicated for mild,
recent-onset depression)
Monitoring
guided self help
cognitive behavioural therapy
Antidepressants (recommended for moderate
to severe depression, dysthymia)
Special consideration for children and elderly
patients

Selective serotonin reuptake inhibitors (SSRI)
Serotonin–norepinephrine reuptake inhibitor (SNRI)
Noradrenergic and specific serotonergic antidepressant (NaSSA) (e.g. mirtazapine)
Tricyclic antidepressants (TCAs)
Monoamine oxidase inhibitors (MAOIs)
Melatonergic agonist (agomelatine)
Benzodiazepines
Hypnotics
Bupropion
Act on serotonin reuptake
Citalopram
Fluoxetine
Escitalopram
Paroxetine
Sertraline
Fluvoxamine
Generally well tolerated
Clinical response 2-4 weeks (may be less in some pts)
Beware of drug interaction – some SSRIs are potent inhibitors of cytochrome P450◦ Eg. Fluoxetine (CYP 2D6, CYP 3A4) – increases
levels of antipsychotics, carbamazepine, ciclosporin etc
SE of agitation especially upon initial administration – poorly tolerated in pts with insomnia, significant anxiety, agitation, suicidal ideation

Act on both serotonin and nonepinephrine, though more selective for serotonin reuptake inhibition
Venlafaxine – first SNRI
Desvenlafaxine – active metabolite of venlafaxine
Duloxetine – neuropathic pain
Efficacious in non-responders to SSRI (STAR*D)

Bupropion
Originally developed as an antidepressant for
smoking cessation therapy
NE and dopamine reuptake inhibition
Can be used as monotherapy
Or adjunct in major depression disorder
Less sexual dysfucntion, wt gain
May have agitation, insomnia, seizure

For severe depression: combination of CBT
and antidepressants recommended
For treatment resistant depression:
augmentation with Lithium, antipsychotic,
add second antidepressant
ECT (for severe and treatment resistant
depression)

Open label, pragmatic randomized trial (c.f. RCTs)
N=2876 (attendees of psychiatric/ family practices)
Inclusion criteria: 18-75 yo
Unipolar MDD
HAM –D 14 or above . This includes mildly depressive patients (45-70% of all clinic depressive patients), c.f. the usual RCT entry requirement of 18-22)
Equipoise-stratified randomization strategy : Patient choice taken into account under a 4-level algorithm Sinyor et al .Can J Psychiatry. 2010 Mar;55(3):126-35.

Primary outcome Secondary outcomes
Remission (HAM-D score of 7) Response (50%reduction of
symptoms, clinician and
patient self-report)
Functioning
QoL

Level 1 Flexible doses of Citalopram for
up to 14 weeks
• 12-month naturalistic follow-
up for remitters/responders
• Level 2 for non-reponders/
those who could not tolerate
citalopram
Level 2 •3 augmentation strategies
(Citalopram + bupropion SR,
Citalopram + buspirone,
Citalopram + CBT)
and
•4 switch strategies (bupropion
SR, sertraline, venlafaxine XR,
CBT)
Level 3 •an augmentation strategy
(lithium or T3), or
•a switch strategy (mirtazapine
or nortriptyline)
Level 4 randomized to
• tranylcypromine or
• combination of venlafaxine XR
and mirtazapine

Treatment Remission rate Dicontinuation
rate
Level 1 • Citalopram 28% 26.6%
Level 2 • Bupropion 21.3%
• Venlafaxine XR 24.8%
• Sertraline 17.6%
• + bupropion 29.7%
• + buspirone 30.1%
30.1%
Level 3 • Mirtazapine 12.3%
• Nortriptyline 19.8%
• + Lithium 15.9%
• + T3 24.7%
44.8%
Level 4 • Tranylcypromine 6.9%
• Mirtazapine + venlafaxine
XR 13.7%
60.1%