Dr Bernadette Daelmans WHO Presentation
20
Implementing the Every Newborn Action Plan Towards ending preventable maternal and newborn mortality Bernadette Daelmans Department of Maternal, Newborn, Child and Adolescent Health
-
Upload
maternal-and-child-survival-program-mcsp -
Category
Documents
-
view
101 -
download
0
description
Implementing the Every Newborn Action Plan: Towards Ending Preventable Maternal and Newborn MortalityPresentation by Dr. Bernadette Daelmans
Transcript of Dr Bernadette Daelmans WHO Presentation

Implementing the Every Newborn Action Plan
Towards ending preventable maternal and newborn mortality
Bernadette Daelmans Department of Maternal, Newborn, Child and Adolescent Health

Building a movement
x World Health
Assembly
The end of MDGs brings new clarity about what is left behind on the agenda – newborns, stillbirths, adolescents
Presenter
Presentation Notes
We are climbing from success to success Lancet stillbirths, in April 2011 -- more than 2.6 m stillbirths per year, with barely more than 1% annual progress in reduction. Testimonials from parents. Multi city launch. 600 m reach global media. But no concrete advocacy plan, just noise. Born Too Soon learned lesson. This time broad-based report, 40+ partners working through PMNCH health professional constituency, 1.1m global media but linked to commitments, foreword from SG and linked to EWEC and CoIA/iERG reporting, Uganda champion country. Strategic advocacy post launch at WHA (minister's breakfast with MoH China) and follow up with partners to form basis for EN A Promise Renewed for Child Survival by India, Ethiopia, the US, and supported by UNICEF in June 2012. 175+ governments have signed a pledge to scale up progress, as well as 400 CSOs. About 10 countries have held national launches. The five strategic shifts of the Promise Renewed roadmap include focus on newborn and equity. Leadership of USAID and UNICEF key, and repeated with Every Newborn. * Save the Children with its annual State of the World's Mother's report and its in-country work through Saving Newborn Lives, supported by the Gates Foundation, have driven attention at national, regional and global levels together with other major NGO groups like World Vision through its work on the Child Health Now campaign platform. First ever global newborn conference in Johannesburg in April 2013, hosted by the Government of South Africa. 500 participants, including champions like Graca Machel. Launch pad for Every Newborn effort. * Every Newborn: consultation meetings in 17 countries and two regions, with bottleneck analyses in these countries to determine where gaps needs to be priortized and filled in support of sharpening costed national plans. Website and toolkit. World Prematurity Day, which led to events in more than 60 countries, many driven by parent groups, Empire State building in purple, FB, NY and GVA events, 24 hour Twitter relay, Celine Dion PSAs on CNN, new research, global media coverage, est reach of 1.4 b. 40+ partner agencies. Save the Children’s Ending Preventable Deaths report launched in February 2014 leveraged media attention and launch efforts were used to promote Every Newborn consultation process in countries. * Launch of The Lancet Every Newborn series - the clearest picture so far of the ongoing slow progress in newborn survival and stillbirths, providing new focus beyond survival, and combining research and reality in countries to set targts for post-2015 to ensure that every newborn has a healthy start in life. +90 individual media hits with articles across the world; +100 million twitter impressions in first week and 12 million people reached through social media Launch events in NYC and Geneva to coincide with WHA WHA endorsed the Every Newborn Action Plan with more than 50 countries took to the floor during the debate to express their support, including those who represented regional blocs. The resolution calls on all member-states to implement the plan and to report on progress to the World Health Assembly through 2030. The Saving Every Woman, Every Child Summit in Toronto from May 28 to 30, 2014 resulted in powerful high-level moment including Prime Minister Harper announcement of Canada's commitment of $3.5 billion to improve the health of mothers and children for the period of 2015–2020. The Partners Forum and the launch of the ENAP – high level participants make supporting statements, over 40 new commitments to EWEC, Blanket of Hope to mobilize civil society, +100 tweeter impressions

Every Newborn Series 5 papers
6 comments
55 authors from 18+ countries
60+ partner organisations
Every Newborn Action Plan Based on the evidence from the Series Co-led by WHO and UNICEF Consultation >60 country governments >80 organisations, >1000 individuals World Health Assembly 2014 resolution Launched June 2014
Now to action in many countries…
Main funders: Bill & Melinda Gates Foundation, USAID, Children’s Investment Fund Foundation
@joylawn
Presenter
Presentation Notes
Strong evidence base in Lancet Wide ownership and UN leadership in ENAP Now moving to country implementation and a key issue is to have the right metrics

Towards ending preventable maternal and
newborn mortality
By 2030 in EVERY COUNTRY: MMR reduction of at least 2/3 from 2010 and MMR less than 140 NMR of less than 12 per 1000 live births Still births less that 12 per 1000 total births
In 2013 : 289.000 maternal deaths 2.9 million newborn deaths 2.6 million stillbirths
More than 3.0 million babies and women could be saved each year

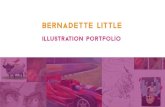
Addressing the main causes of mortality
Causes of maternal mortality Causes of newborn mortality

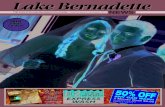
Care around the time of birth: a triple return on investment
Source: Special analysis detailed in The Lancet Every Newborn Series, launched 19 May 2014
Almost 3 million babies and women could be saved each year through investing in quality care around the time of birth.
Presenter
Presentation Notes
Over a third of all maternal and newborn deaths as well as stillbirths occur during labour and childbirth. Many of these deaths and complications can be prevented by ensuring provision of high-quality, essential care for every pregnant woman and every baby around the time of labour, childbirth and in the first 24 hours and week after birth. Based on a preliminary analysis conducted for The Lancet Every Newborn Series, care around the time of birth (labour, childbirth and the first day after birth) provides a unique period along the continuum of care to prevent maternal and newborn deaths as well as intrapartum stillbirths. By strengthening and investing in this critical window, it is a triple return on investment.

Strategic objectives
Address all major causes of maternal and newborn mortality, morbidity and related disabilities as well as stillbirths;
Invest in and improve quality care for women and newborns, especially around the time of childbirth;
Address inequities in access to and quality of reproductive, maternal, perinatal and newborn health care services;
Harness the power of parents, families and communities; empower women and girls
Ensure universal coverage of essential interventions for reproductive, maternal and newborn health care
Improve metrics globally and nationally and ensure accountability

5 things to do differently
Integrated Plans Integrated service
delivery, continuum of care, coordination
Implementation & Innovation
Address health system bottlenecks, Every Mother Every Newborn initiative
Indicators & metrics Targets in post 2015
Measurement of progress and impact
Intentional leadership
development Especially in countries with highest burden
Investment for impact
Governance, community participation, partner
alignment
Presenter
Presentation Notes
The action plan relies on five guiding principles: Country leadership: Countries have the primary ownership and responsibility for establishing good governance and providing effective and good-quality reproductive, maternal and newborn health services. Community participation is a key feature of such leadership as it is one of the most effective transformational mechanisms for action and accountability for newborn health. Development partners should align their contributions and harmonize action. Integration: Providing every woman and every newborn with good-quality care requires integrated service delivery with coordinated health system approaches between multiple programmes, stakeholders and initiatives across the continuum of reproductive, maternal, newborn and child health are essential, without losing visibility for newborn specific content. Equity: Equitable and universal coverage of high-impact interventions, and a focus on reaching the most vulnerable and poorest population groups are central to realizing the right of every woman and every newborn, girl and boy, to health. Accountability: Transparency, oversight and accountability are prerequisites for equitable coverage, quality of care and optimal use of resources. Innovation: Evidence has been accumulating over the past decade of strategies that broaden the coverage of interventions for newborns and reduce mortality. Nevertheless, innovative thinking is needed about ways to reach the poorest and most underserved populations. Optimizing the application of knowledge of which interventions and strategies are most effective still needs more research and development.

WHO recommendations for maternal, perinatal and newborn care
http://www.who.int/maternal_child_adolescent/documents/mnca-recommendations/en/

Resuscitation: what is new?
No routine suctioning even before ventilation, only for babies born through meconium-stained amniotic fluid who do not start breathing on their own
Preference of bulb syringe in the absence of mechanical equipment
Start Positive Pressure Ventilation within 1 minute
Preference of self-inflating bag
Measurement of heart rate after 60 seconds
Recommendation to stop resuscitation after 10 min, if no detectable heart rate

Cord care
Daily chlorhexidine (4%) application to the umbilical cord stump during the first week of life is recommended for newborns who are born at home in settings with high neonatal mortality (30 or more neonatal deaths per 1000 live births).
Clean, dry cord care is recommended for newborns born in health facilities and at home in low neonatal mortality settings.
Use of chlorhexidine in these situations may be considered only to replace application of a harmful traditional substance such as cow dung, to the cord stump.

Facility stay after childbirth
After an uncomplicated vaginal birth in a health facility, healthy mothers and newborns should receive care in the facility for at least 24 hours after birth.
J. Lawn et al. Lancet 2014; 384: 189–205

Timing and number of postnatal contacts
Healthy mothers and newborns should receive care in the facility for at least 24 hours after birth.
If birth is at home, the first postnatal contact should be as early as possible within 24 hours of birth.
At least three additional postnatal contacts are recommended for all mothers and newborns: on day 3 (48–72 hours), between days 7–14, and 6 weeks after birth.
Home visits in the first week after birth are recommended for care of the mother and newborn.

Assessment of the newborn
The newborn should be referred for further evaluation if any of the signs is present:
1. stopped feeding well, 2. history of convulsions, 3. fast breathing (breathing rate ≥60 per minute), 4. severe chest in-drawing, 5. no spontaneous movement, 6. fever (temperature >37.5 °C), 7. low body temperature (temperature <35.5 °C), 8. any jaundice in first 24 hours of life, or yellow palms and
soles at any age.

Care for low birth weight babies

Feeding of low birth weight infants
LBW and VLBW infants should be fed mother's own breast milk. If the mother is not able to breastfeed, donor milk should be given
LBW should be put to the breast as soon as clinically stable after birth
LBW should be exclusively breastfed on demand for 6 months
LBW infants who can not be breastfed, but can swallow should be fed by cup and spoon (or cup with beak), based on hunger cues, but at least every 3 hours
http://www.who.int/maternal_child_adolescent/documents/infant_feeding_low_bw/en/

Forthcoming WHO recommendations
Antenatal corticosteroids for management of preterm labour and birth for women at risk of preterm birth from 24 weeks to 34 weeks of gestation
when the following conditions are met: gestational age assessment can be accurately undertaken preterm birth is considered imminent there is no clinical evidence of maternal infection adequate childbirth care is available (including the core functions of emergency
obstetric care) the preterm newborn can receive adequate care if needed (including resuscitation,
thermal care, feeding support, infection treatment and safe oxygen use).
Kangaroo mother care for neonates weighing ≤2000g at birth as soon as they are clinically stable;
care should be provided as continuously as possible

New evidence towards updated guidelines
Young infants 7 – 59 days old with fast breathing as a single sign, who are identified through home visits or spontaneously brought for care at outpatient clinics can be safely and effectively treated with oral amoxicillin for 7 days by appropriately trained health care provider.
Young infants 0 – 59 days old with any sign of clinical severe infection who are not critically ill, who are identified through home visits or spontaneously brought for care at outpatient clinics and whose caregivers cannot or do not accept hospitalization
Option 1: IM gentamicin 5-7.5 mg/kg once daily for 7 days and twice daily oral amoxicillin, 50 mg/kg per dose for 7 days. Close follow up is essential
Option 2: IM gentamicin 5-7.5 mg/kg once daily for 2 days and twice daily oral amoxicillin, 50 mg/kg per dose for 7 days. Close follow up is essential. A careful assessment on day 4 is mandatory.
Also see: AFRINEST and SATT studies, Lancet Global Health, published online April 2, 2015

Three main streams of activities are ensuring the action plan leads to real change in countries:
1. Country implementation: identifying and responding to technical support needs, supporting translation of evidence into action, including Every Mother Every Newborn quality improvement initiative.
2. Data and metrics: improving and institutionalizing metrics to track coverage and impact based on the goals and targets of the ENAP and five strategic objectives.
3. Advocacy: strengthening maternal and newborn health advocacy efforts globally and in countries, building a movement for change.
Every Newborn action now:
Research as cross cutting

www.lancet.com/series/everynewborn #EveryNewborn
An Action Plan To End Preventable Deaths
EVERY NEWBORN We are still building a
movement…
BE PART OF THE ACTION
For more information
visit www.everynewborn.org