
Document of The World Bankdocuments.worldbank.org/curated/en/356301468267339490/pdf/ICR... ·...
57
Document of The World Bank Report No: ICR0000786 IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-33810) ON A CREDIT IN THE AMOUNT OF SDR 28.6 MILLION (US$ 38 MILLION EQUIVALENT) TO THE REPUBLIC OF INDONESIA FOR A PROVINCIAL HEALTH PROJECT June 26, 2008 Health, Nutrition and Population Human Development Sector Unit East Asia and Pacific Region Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized
Transcript of Document of The World Bankdocuments.worldbank.org/curated/en/356301468267339490/pdf/ICR... ·...

Document of The World Bank
Report No: ICR0000786
IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-33810)
ON A
CREDIT
IN THE AMOUNT OF SDR 28.6 MILLION (US$ 38 MILLION EQUIVALENT)
TO THE
REPUBLIC OF INDONESIA
FOR A
PROVINCIAL HEALTH PROJECT
June 26, 2008
Health, Nutrition and Population Human Development Sector Unit East Asia and Pacific Region
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized

CURRENCY EQUIVALENTS
(Exchange Rate Effective April 30, 2008)
Currency Unit = Indonesian Rupiah (IDR) IDR 1.00 = US$ 0.00011
US$ 1.00 = IDR 9,234
FISCAL YEAR Government of Indonesia January 1 – December 31
ABBREVIATIONS AND ACRONYMS
ADB Asian Development Bank JPS-BK Social Safety Net, Health Component
Askeskin Health Insurance for the Poor Kanwil Kesehatan
Ministry of Health Provincial Office
Bappeda Regional Development Planning Agency KPKN Treasure Office Bappenas National Development Planning Agency MD and
RM Grant Managing Decentralization and Resource Mobilization Grant
BLU General Service Unit MOF Ministry of Finance BPKP Central Audit Bureau MOH Ministry of Health BPS Central Bureau of Statistics MOHA Ministry of Home Affairs CAS Country Assistance Strategy NGO Non Government Organization CPCU Central Project Coordination Unit OECD Organization for Economic
Cooperation and Development Dinas Kesehatan
Local Government Health Department PCAR Procurement Capacity Assessment Report
DIPA Development Budgets Allocations PCIU Provincial Central Implementation Unit
DIU District Implementation Units PHP Provincial Health Project DPRD District Assembly PHPB Provincial Health Promotion Board GOI Government of Indonesia PMM Project Management Manual HIS Health Information System RU Research Unit IDA International Development Association SK Decree IG Inspectorate General TA Technical Assistance Jamkesos Health Insurance Scheme in Yogyakarta TF Task Force JHC Joint Health Council TRT Technical Review Team
Vice President: James W. Adams Country Director: Joachim von Amsberg
Sector Manager: Fadia M. Saadah Project Team Leader: Puti Marzoeki
ICR Team Leader: Puti Marzoeki

INDONESIA Provincial Health Project
CONTENTS
Data Sheet A. Basic Information B. Key Dates C. Ratings Summary D. Sector and Theme Codes E. Bank Staff F. Results Framework Analysis G. Ratings of Project Performance in ISRs H. Restructuring I. Disbursement Graph
1. Project Context, Development Objectives and Design............................................... 12. Key Factors Affecting Implementation and Outcomes .............................................. 53. Assessment of Outcomes .......................................................................................... 114. Assessment of Risk to Development Outcome......................................................... 205. Assessment of Bank and Borrower Performance ..................................................... 206. Lessons Learned ....................................................................................................... 227. Comments on Issues Raised by Borrower/Implementing Agencies/Partners .......... 24Annex 1. Project Costs and Financing.......................................................................... 26Annex 2. Outputs by Component ................................................................................. 27Annex 3. Economic and Financial Analysis................................................................. 30Annex 4. Bank Lending and Implementation Support/Supervision Processes ............ 31Annex 5. Beneficiary Survey Results ........................................................................... 33Annex 6. Stakeholder Workshop Report and Results................................................... 34Annex 7. Summary of Borrower's ICR and/or Comments on Draft ICR..................... 35Annex 8. Comments of Cofinanciers and Other Partners/Stakeholders....................... 43Annex 9. List of Supporting Documents ...................................................................... 44Map IBRD 36233.......................................................................................................... 45

i
A. Basic Information Country: Indonesia Project Name: Provincial Health I Project ID: P049545 L/C/TF Number(s): IDA-33810 ICR Date: 06/26/2008 ICR Type: Core ICR Lending Instrument: SIL Borrower: GOI Original Total Commitment:
XDR 28.6M Disbursed Amount: XDR 22.3M
Environmental Category: C Implementing Agencies: Ministry of Health Cofinanciers and Other External Partners: B. Key Dates
Process Date Process Original Date Revised / Actual Date(s)
Concept Review: 08/14/1998 Effectiveness: 08/21/2000 08/21/2000 Appraisal: 02/16/2000 Restructuring(s): Approval: 06/15/2000 Mid-term Review: 05/10/2004 Closing: 06/30/2006 12/31/2007 C. Ratings Summary C.1 Performance Rating by ICR Outcomes: Moderately Satisfactory Risk to Development Outcome: Substantial Bank Performance: Moderately Satisfactory Borrower Performance: Moderately Satisfactory
C.2 Detailed Ratings of Bank and Borrower Performance (by ICR) Bank Ratings Borrower Ratings
Quality at Entry: Moderately Satisfactory Government: Moderately Satisfactory
Quality of Supervision: Moderately Satisfactory Implementing Agency/Agencies: Moderately Satisfactory
Overall Bank Performance: Moderately Satisfactory Overall Borrower
Performance: Moderately Satisfactory
C.3 Quality at Entry and Implementation Performance Indicators
Implementation Performance Indicators QAG Assessments
(if any) Rating
Potential Problem Project at any time (Yes/No):
No Quality at Entry (QEA):
Satisfactory

ii
Problem Project at any time (Yes/No):
No Quality of Supervision (QSA):
None
DO rating before Closing/Inactive status:
Moderately Satisfactory
D. Sector and Theme Codes
Original Actual Sector Code (as % of total Bank financing) Central government administration 9 9 Compulsory health finance 5 5 Health 84 84 Sub-national government administration 2 2
Theme Code (Primary/Secondary) Decentralization Primary Primary Health system performance Primary Primary Injuries and non-communicable diseases Secondary Secondary Other communicable diseases Secondary Secondary Participation and civic engagement Secondary E. Bank Staff
Positions At ICR At Approval Vice President: James W. Adams Jemal-ud-din Kassum Country Director: Joachim von Amsberg Mark Baird Sector Manager: Fadia M. Saadah Alan Ruby Project Team Leader: Puti Marzoeki Samuel S. Lieberman ICR Team Leader: Puti Marzoeki ICR Primary Author: Adrian Hayes F. Results Framework Analysis Project Development Objectives (from Project Appraisal Document) 1. To bring about effective health sector decentralization in the provinces of Lampung and Yogyakarta. The challenge during this period of institutional change and limited economic recovery is to protect health services which are essential for the poor and public at large while implementing key sector reforms and putting health financing on a firm footing.
iii
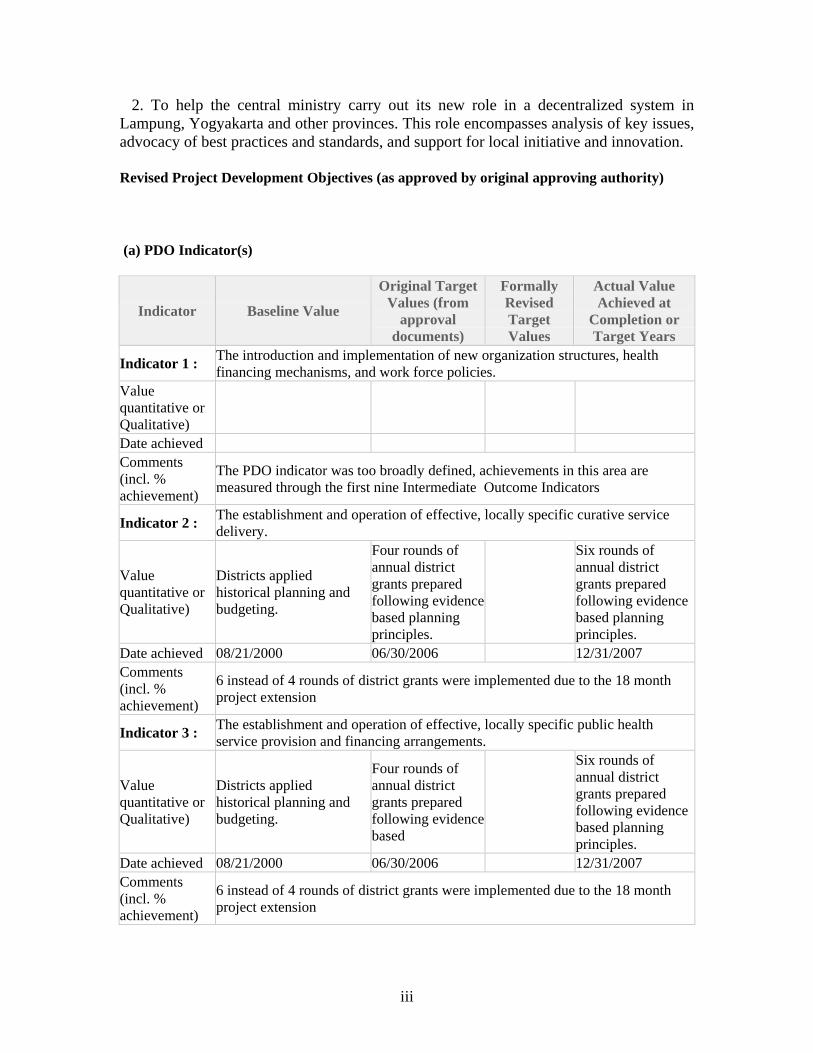
2. To help the central ministry carry out its new role in a decentralized system in Lampung, Yogyakarta and other provinces. This role encompasses analysis of key issues, advocacy of best practices and standards, and support for local initiative and innovation. Revised Project Development Objectives (as approved by original approving authority) (a) PDO Indicator(s)
Indicator Baseline Value
Original Target Values (from
approval documents)
Formally Revised Target Values
Actual Value Achieved at
Completion or Target Years
Indicator 1 : The introduction and implementation of new organization structures, health financing mechanisms, and work force policies.
Value quantitative or Qualitative)
Date achieved Comments (incl. % achievement)
The PDO indicator was too broadly defined, achievements in this area are measured through the first nine Intermediate Outcome Indicators
Indicator 2 : The establishment and operation of effective, locally specific curative service delivery.
Value quantitative or Qualitative)
Districts applied historical planning and budgeting.
Four rounds of annual district grants prepared following evidence based planning principles.
Six rounds of annual district grants prepared following evidence based planning principles.
Date achieved 08/21/2000 06/30/2006 12/31/2007 Comments (incl. % achievement)
6 instead of 4 rounds of district grants were implemented due to the 18 month project extension
Indicator 3 : The establishment and operation of effective, locally specific public health service provision and financing arrangements.
Value quantitative or Qualitative)
Districts applied historical planning and budgeting.
Four rounds of annual district grants prepared following evidence based
Six rounds of annual district grants prepared following evidence based planning principles.
Date achieved 08/21/2000 06/30/2006 12/31/2007 Comments (incl. % achievement)
6 instead of 4 rounds of district grants were implemented due to the 18 month project extension

iv
(b) Intermediate Outcome Indicator(s)
Indicator Baseline Value
Original Target Values (from
approval documents)
Formally Revised
Target Values
Actual Value Achieved at
Completion or Target Years
Indicator 1 : Merging of Kanwil Kesehatan and Dinas Kesehatan, and establishment of a new health organization structure by June 1, 2001.
Value (quantitative or Qualitative)
At the province level, Kanwil and Dinas Kesehatan are separate organizations.
Merging of Kanwil and Dinas Kesehatan by June 1, 2001.
Kanwil & Dinas Kesehatan were merged as one office Introduction of Joint Health Council (JHCs), Technical Review Team (TRTs) and Task Forces (TFs) at the province level.
Date achieved 01/01/2000 06/01/2001 01/01/2001 Comments (incl. % achievement)
Lampung province has actually achieved the status before project effectiveness
Indicator 2 : Implementation of new personnel policies related to recruitment, redeployment, retraining, early retirement and career development by January 1, 2002.
Value (quantitative or Qualitative)
Personnel policy was centralized and guided by the civil service law. Career development was not based on merit or performance but rather on seniority.
Implementation of new personnel policies related to recruitment, redeployment, retraining, early retirement and career development by January 1, 2002.
Personnel policy was centralized and guided by the civil service law. Career development was not based on merit or performance but rather on seniority.
Date achieved 08/21/2000 01/01/2002 12/31/2007 Comments (incl. % achievement)
Provinces could not implement new personnel policy because of the absence of civil service reform and personnel regulation remained centralized in general.
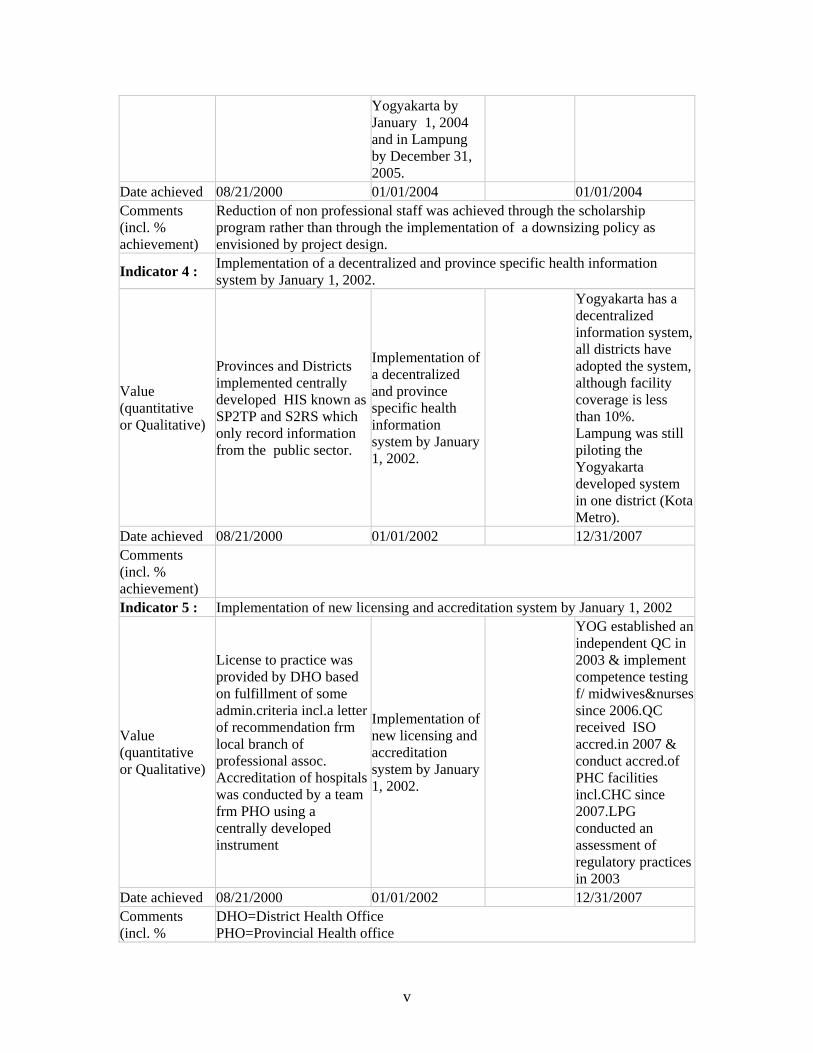
Indicator 3 : Reduction of number of non-professional staff at the provincial and district health offices by 20% in Yogyakarta by January 1, 2004 and in Lampung by December 31, 2005.
Value (quantitative or Qualitative)
The number of non professional staff in Yogyakarta was 889 in Lampung was 82 .
Reduction of number of non-professional staff at the provincial and district health offices by 20% in
The number of non-professional staff was 639 in Yogya and 126 in Lampung
v
Yogyakarta by January 1, 2004 and in Lampung by December 31, 2005.
Date achieved 08/21/2000 01/01/2004 01/01/2004 Comments (incl. % achievement)
Reduction of non professional staff was achieved through the scholarship program rather than through the implementation of a downsizing policy as envisioned by project design.
Indicator 4 : Implementation of a decentralized and province specific health information system by January 1, 2002.
Value (quantitative or Qualitative)
Provinces and Districts implemented centrally developed HIS known as SP2TP and S2RS which only record information from the public sector.
Implementation of a decentralized and province specific health information system by January 1, 2002.
Yogyakarta has a decentralized information system, all districts have adopted the system, although facility coverage is less than 10%. Lampung was still piloting the Yogyakarta developed system in one district (Kota Metro).
Date achieved 08/21/2000 01/01/2002 12/31/2007 Comments (incl. % achievement)
Indicator 5 : Implementation of new licensing and accreditation system by January 1, 2002
Value (quantitative or Qualitative)
License to practice was provided by DHO based on fulfillment of some admin.criteria incl.a letter of recommendation frm local branch of professional assoc. Accreditation of hospitals was conducted by a team frm PHO using a centrally developed instrument
Implementation of new licensing and accreditation system by January 1, 2002.
YOG established an independent QC in 2003 & implement competence testing f/ midwives&nurses since 2006.QC received ISO accred.in 2007 & conduct accred.of PHC facilities incl.CHC since 2007.LPG conducted an assessment of regulatory practices in 2003
Date achieved 08/21/2000 01/01/2002 12/31/2007 Comments (incl. %
DHO=District Health Office PHO=Provincial Health office
vi
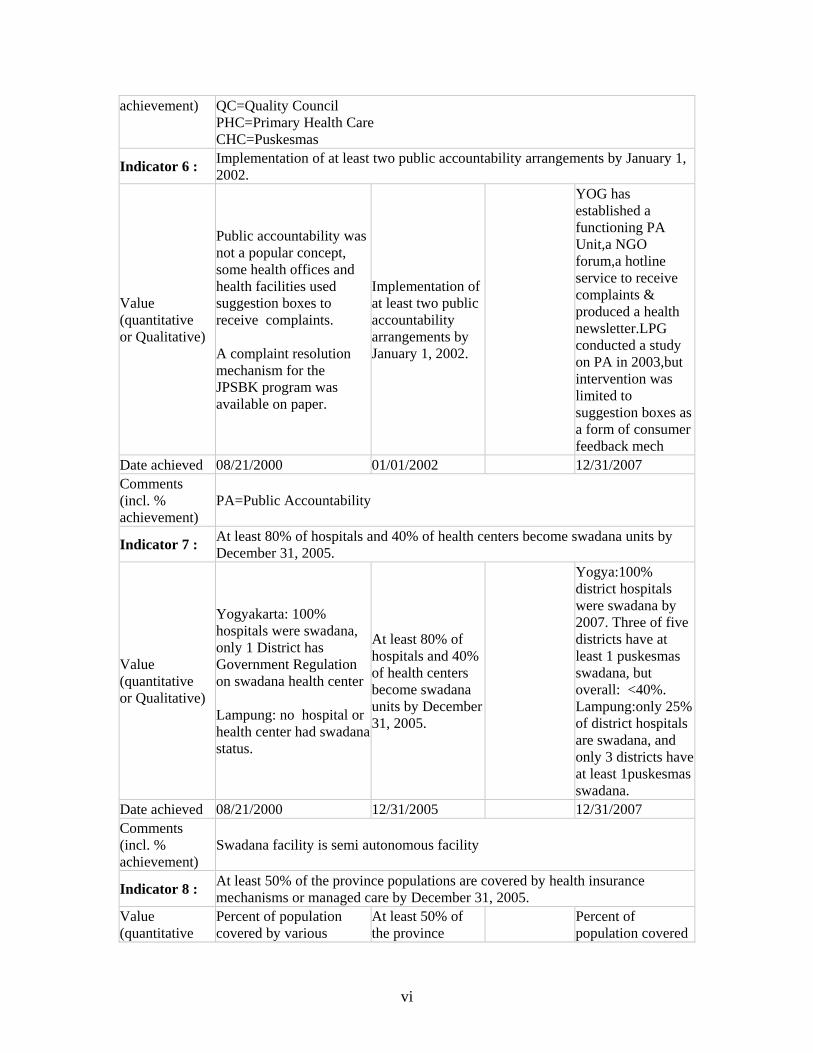
achievement) QC=Quality Council PHC=Primary Health Care CHC=Puskesmas
Indicator 6 : Implementation of at least two public accountability arrangements by January 1, 2002.
Value (quantitative or Qualitative)
Public accountability was not a popular concept, some health offices and health facilities used suggestion boxes to receive complaints. A complaint resolution mechanism for the JPSBK program was available on paper.
Implementation of at least two public accountability arrangements by January 1, 2002.
YOG has established a functioning PA Unit,a NGO forum,a hotline service to receive complaints & produced a health newsletter.LPG conducted a study on PA in 2003,but intervention was limited to suggestion boxes as a form of consumer feedback mech
Date achieved 08/21/2000 01/01/2002 12/31/2007 Comments (incl. % achievement)
PA=Public Accountability
Indicator 7 : At least 80% of hospitals and 40% of health centers become swadana units by December 31, 2005.
Value (quantitative or Qualitative)
Yogyakarta: 100% hospitals were swadana, only 1 District has Government Regulation on swadana health center Lampung: no hospital or health center had swadana status.
At least 80% of hospitals and 40% of health centers become swadana units by December 31, 2005.
Yogya:100% district hospitals were swadana by 2007. Three of five districts have at least 1 puskesmas swadana, but overall: <40%. Lampung:only 25% of district hospitals are swadana, and only 3 districts have at least 1puskesmas swadana.
Date achieved 08/21/2000 12/31/2005 12/31/2007 Comments (incl. % achievement)
Swadana facility is semi autonomous facility
Indicator 8 : At least 50% of the province populations are covered by health insurance mechanisms or managed care by December 31, 2005.
Value (quantitative
Percent of population covered by various
At least 50% of the province Percent of
population covered
vii
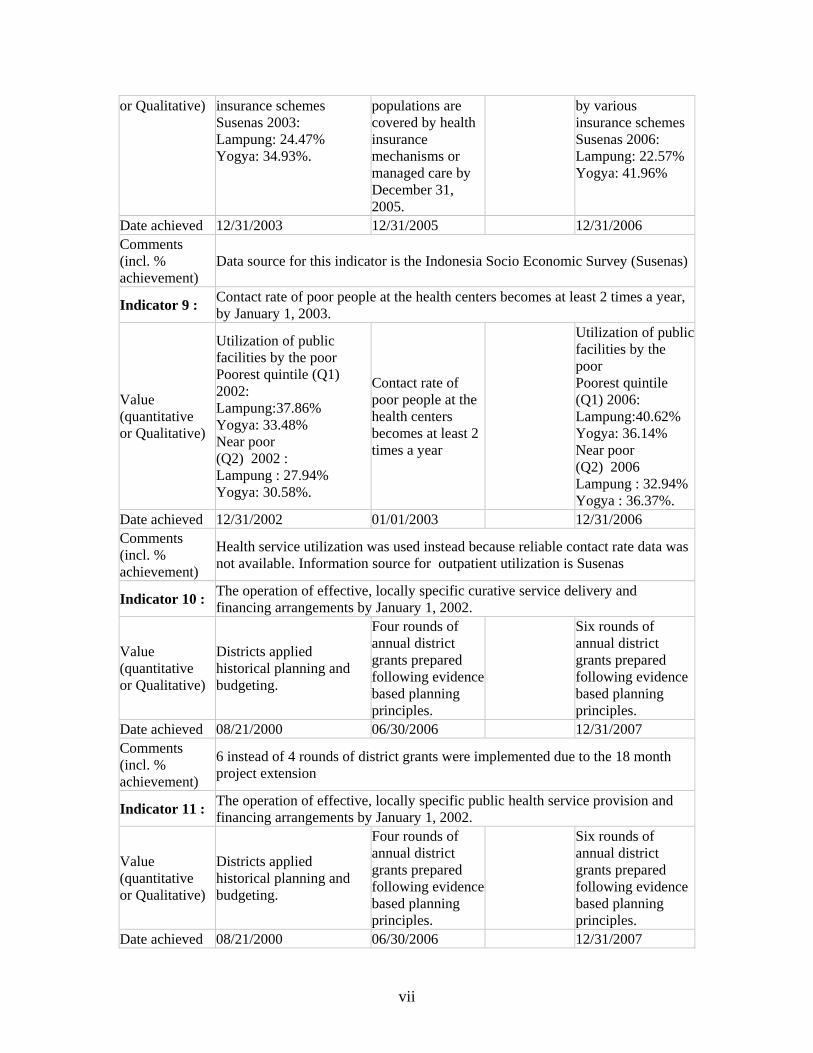
or Qualitative) insurance schemes Susenas 2003: Lampung: 24.47% Yogya: 34.93%.
populations are covered by health insurance mechanisms or managed care by December 31, 2005.
by various insurance schemes Susenas 2006: Lampung: 22.57% Yogya: 41.96%
Date achieved 12/31/2003 12/31/2005 12/31/2006 Comments (incl. % achievement)
Data source for this indicator is the Indonesia Socio Economic Survey (Susenas)
Indicator 9 : Contact rate of poor people at the health centers becomes at least 2 times a year, by January 1, 2003.
Value (quantitative or Qualitative)
Utilization of public facilities by the poor Poorest quintile (Q1) 2002: Lampung:37.86% Yogya: 33.48% Near poor (Q2) 2002 : Lampung : 27.94% Yogya: 30.58%.
Contact rate of poor people at the health centers becomes at least 2 times a year
Utilization of public facilities by the poor Poorest quintile (Q1) 2006: Lampung:40.62% Yogya: 36.14% Near poor (Q2) 2006 Lampung : 32.94%Yogya : 36.37%.
Date achieved 12/31/2002 01/01/2003 12/31/2006 Comments (incl. % achievement)
Health service utilization was used instead because reliable contact rate data was not available. Information source for outpatient utilization is Susenas
Indicator 10 : The operation of effective, locally specific curative service delivery and financing arrangements by January 1, 2002.
Value (quantitative or Qualitative)
Districts applied historical planning and budgeting.
Four rounds of annual district grants prepared following evidence based planning principles.
Six rounds of annual district grants prepared following evidence based planning principles.
Date achieved 08/21/2000 06/30/2006 12/31/2007 Comments (incl. % achievement)
6 instead of 4 rounds of district grants were implemented due to the 18 month project extension
Indicator 11 : The operation of effective, locally specific public health service provision and financing arrangements by January 1, 2002.
Value (quantitative or Qualitative)
Districts applied historical planning and budgeting.
Four rounds of annual district grants prepared following evidence based planning principles.
Six rounds of annual district grants prepared following evidence based planning principles.
Date achieved 08/21/2000 06/30/2006 12/31/2007

viii
Comments (incl. % achievement)
6 instead of 4 rounds of district grants were implemented due to the 18 month project extension
G. Ratings of Project Performance in ISRs
No. Date ISR Archived DO IP
Actual Disbursements (USD millions)
1 06/30/2000 Satisfactory Satisfactory 0.00 2 12/12/2000 Satisfactory Satisfactory 1.00 3 03/01/2001 Satisfactory Satisfactory 1.00 4 08/24/2001 Satisfactory Satisfactory 1.00 5 12/18/2001 Satisfactory Satisfactory 1.27 6 06/02/2002 Satisfactory Satisfactory 3.30 7 11/26/2002 Satisfactory Satisfactory 9.15 8 06/12/2003 Satisfactory Satisfactory 11.92 9 12/23/2003 Satisfactory Satisfactory 15.38 10 06/25/2004 Satisfactory Satisfactory 16.74 11 12/08/2004 Satisfactory Satisfactory 21.76 12 05/13/2005 Satisfactory Satisfactory 21.76 13 12/19/2005 Satisfactory Satisfactory 21.76 14 01/12/2007 Moderately Satisfactory Moderately Satisfactory 28.47 15 07/05/2007 Moderately Satisfactory Moderately Satisfactory 30.72 16 12/27/2007 Moderately Satisfactory Moderately Satisfactory 31.26
H. Restructuring (if any) Not Applicable

ix
I. Disbursement Profile

1
1. Project Context, Development Objectives and Design
1.1 Context at Appraisal The First Provincial Health Project (PHP I) was launched in August 2000, during a turbulent period in Indonesia’s history. Indonesia was hit hard by the Asian economic crisis of the late 1990s. This introduced a period of rapid and major change in governance. Complex and unpredictable processes of democratic reform and decentralization provided the context for the design and final preparation phases of PHP I, especially new legislation on “regional autonomy” (decentralization) announced in 1999.1 The changes in governance and society provided both opportunities and risks for the health sector, which was itself still recovering from the economic crisis. The project’s primary aim was effective decentralization of the health sector, mainly in the provinces of Lampung and DI Yogyakarta.2 This aim entailed protecting health services essential for the poor and the public at large, initiating key sector reforms, improving health financing, and helping the Ministry of Health (MOH) assume new roles. These objectives could be expected to contribute to achieving the CAS post-economic crisis goal of reinforcing social safety nets and strengthening institutions to support sustainable growth. The Project provinces were selected to provide different lessons and experiences. Yogya presented a more developed province with capacity and ability to undertake reforms and provide key lessons for how other provinces can handle decentralization, while Lampung had more limited capacity and as such can provide important lessons on how capacity and reforms can be developed that are suited to the provincial and district needs.
1.2 Original Project Development Objectives (PDO) and Key Indicators The PDO as stated in the PAD were: a. Bring about effective health decentralization in the provinces of Lampung and
Yogyakarta. This involves protecting health services of the poor and the public at large, initiating key sector reforms, and putting health financing on a firm footing.
b. Help the central health ministry (MOH) carry out its new role to provide analysis of key issues, advocacy of best practices and standards, and support for local initiative and innovation.
1 Notably Law 22 of 1999 on Regional Autonomy (Pemerintahan Daerah) and Law 25 on Financial Balance between Central and Regional Government (Perimbangan Keuangan Antara Pemerintah Pusat dan Daerah).
2 For historical reasons the Province of Yogyakarta goes by the title Daerah Istimewa Yogyakarta (Special Region of Yogyakarta); this is often abbreviated to Yogyakarta, or simply Yogya.

2
The PAD listed three key performance indicators for the PDO to gauge project performance: a. The introduction and implementation of new organization structures, health financing
mechanisms, and work force policies.
b. The establishment and operation of effective, locally specific curative service delivery, and financing arrangements.
c. The establishment and operation of effective, locally specific public health service provisions, and financing arrangements.
The above three Key Performance Indicators for the PDO are too broad and an impediment for arriving at a meaningful assessment of the extent to which the two PDOs have been achieved. Because of the lack of specificity of the PDO Indicators the ICR team decided to assess the extent to which the two PDOs were achieved by examining (in Section 3.2, “Achievement of Project Development Objectives”) the extent to which the objectives specific to each of the eight components were achieved.
1.3 Revised PDO (as approved by original approving authority) and Key Indicators, and Reasons/Justification The PDO were not revised. The implementation period was extended for 18 months from June 30, 2006, to December 31, 2007, by amendment of the Credit Agreement; it was agreed that for this period activities in Lampung Province would concentrate on efforts to reduce infant and maternal mortality, but still within the existing framework of the project, while in Yogyakarta, activities would continue with health reform efforts, especially in health financing, workforce regulation, and health information systems.
1.4 Main Beneficiaries The main beneficiaries were identified as poor households living in Lampung and Yogyakarta, estimated to comprise approximately 570,000 individuals in Yogyakarta and 1.5 million in Lampung in 1999. According to the Central Bureau of Statistics, household expenditure data (cited in the PAD), the percentage of poor people in the two provinces combined was just under 11 percent in 1996, but had risen to 18 percent in early 1999 due to the economic crisis.

3
1.5 Original Components (as approved) As described in the PAD (pp. 8-9), the project had two main parts: a Provincial/district part that consists of 5 components (referred to as A1-A5 below) and a central part that consists of 3 components (referred to as B1 to B3). Most of the activities of the central component as well as key developmental aspects of the provincial ones were expected to be completed in the first phase of the project (expected to be about 18 months) Having established an appropriate institutional framework for implementation and having the Task Forces studied the relevant issues and made their recommendations in the first phase, the second phase would then focus mostly on awarding of block grants to districts and implement key recommendations. Table 1: Project Components Province and District Level
Component A1 Managing Decentralization Component A2 Mobilizing Resources Component A3 Improving Health Service Access and Quality Component A4 Grants Component A5 Project Management Central Level
Component B1 Managing Decentralization Component B2 Resource Mobilization Component B3 Project Management
Province and District Level: Component A1. Managing Decentralization (District and Provincial) – $3.81 million (a) restructuring health service organizations; (b) reorganizing the management structures of entities implementing health services; (c) developing and implementing new human resource management policies; (d) at the provincial level, developing and implementing new health information systems covering health indicators, and service delivery, facility and staffing information; (e) strengthening public accountability mechanisms; and (f) strengthening the policy regulatory framework for health services, including the establishment of a health council and a health care accreditation agency at the provincial level.
Component A2. Mobilizing Resources (District and Provincial) – $1.73 million (a) at the provincial level, developing and implementing decentralized health service planning, budgeting and financing systems designed to permit Districts to plan and develop efficient, effective and equitable programs according to community needs; (b) converting hospitals, health centers and other health service units into autonomous units (swadana) which will possess, inter alia, the authority to apply cost recovery measures; and (c) at the provincial and district/municipal levels, developing, piloting and, if appropriate, implementing a health insurance system and/or managed care.

4
Component A3. Improving Health Service Access and Quality (District and Provincial) – $4.17 million This component was only implemented during 2000 and 2001 (Phase 1) and aimed at: (a) implementing specific health service activities, including the refurbishing of health care facilities, upgrading medical equipment, increasing the number of mobile health service facilities and contracting private health service providers for the delivery of basic health services to designated areas; (b) implementing quality assurance programs and upgrading the quality of health sector personnel through the implementation of fellowship programs; (c) establishing a health promotion board in Yogyakarta to coordinate health with public and private sector promotion activities; and (d) providing specific drugs and supplies based on district/municipal proposals. Component A4. Grants (Districts) – $63.71 million Financing (a) Eligible Activities through the provision of MD and RM Grants and (b) Eligible Programs through the provision of District Grants. The distinction between the two grants disappeared during implementation as managing decentralization and resource mobilization efforts became an integral part of the District Grant proposals.
Component A5. Project Management (District and Provincial) – $0.78 million Establishing, at the provincial and district/municipal levels, a management and administrative structure appropriate for the coordination and carrying out of health service program and Project activities.
Central Level: Component B1. Managing Decentralization (Central) – $2.87 million Strengthening (a) the institutional capacity of MOH to provide support to provinces and districts in fulfilling their health sector responsibilities allocated to them under the Law on Regional Government, No. 22/1999 through conducting policy studies, sponsoring national seminars and workshops, and strengthening its policy and technical analytical capabilities and its health service advocacy and information dissemination services and (b) national capacity to evaluate health policy interventions through the establishment of an independent research unit. Component B2. Resource Mobilization (Central) – $0.56 million Strengthening the institutional capacity of MOH to develop and administer a program for the financing of specific health-related programs at the provincial and district/municipal levels by providing Matching Grants. Component B3. Project Management (Central) – $1.00 million Strengthening the institutional capacity of the MOH to carry out its management responsibilities for the Project through the provision of technical assistance, training, and office equipment and supplies, and the carrying out of workshops.
5
1.6 Revised Components No revised components.
1.7 Other Significant Changes No other significant changes, although it is worth noting that Ministry of Health (MOH) assigned the core management group at the Ministry with the Central Project Coordination Unit (CPCU) for PHP I similar responsibilities for PHP II during the last 14 months of its activities (closing June 302007), after the latter project’s own management group was implicated in documented corruption. On May 30, 2006, upon request from the Government, the World Bank cancelled a part of the loan amounting US$ 2.9 million.
2. Key Factors Affecting Implementation and Outcomes
2.1 Project Preparation, Design and Quality at Entry Background analysis was sound in the way it drew on experience with the Bank’s 16 previous health projects in Indonesia and identified “entrenched problems” in Indonesia’s health sector.3 Decentralization has a long and complex history in Indonesia going back to colonial times.4 The idea for a Bank project facilitating effective decentralization of the health sector dates from the early nineties, although what was proposed then was certainly a more limited transfer of authority to the regions than that envisioned in the late nineties. With the advantage of hindsight, further analysis would have been helpful looking at how decentralization could be expected to impact the underlying causes of the entrenched problems in the sector. The Bank identified many factors behind the “unsatisfactory health system performance in the 1990s” and the “disengaged worldview” within the health labor force.5 Few would argue with the Bank’s view that “decentralization and related steps can lead to conditions in which providers have the incentives, skills, supervision, material support, and discretionary authority needed to offer high quality services, and clients have the information, financial means, and bargaining power required to elicit appropriate responses.” The key phrase which did not receive sufficient analysis is “can lead to conditions.” There were many things wrong with the health
3 World Bank, 2000. Health Strategy in a Post-Crisis, Decentralizing Indonesia. (Report No. 21318-IND)
4 Wihana Kirana Jaya and Howard Dick, 2002. “The Latest Crisis of Regional Autonomy in Historical Perspective,” in Indonesia Today: Challenges of History, ed. Grayson Lloyd and Shannon Smith. Singapore: Institute of Southeast Asian Studies.
5 See Health Strategy, pp. iii-iv.
6
system before decentralization, but they were not all due to centralized governance. Decentralization per se could not be expected to sweep away all the underlying causes of the system’s poor performance. Further analysis of underlying causes was needed to distinguish those underlying causes of poor performance which could be transformed by decentralization and those which would likely be unaffected by decentralization. Final plans and the drafting of documents for PHP I were completed unusually quickly,6 as indeed was the case for the Government’s 1999 decentralization laws themselves. Bank officials knew that decentralization was going to happen whether the Bank had an approved project or not. The Bank can be commended that it was the only donor with a project already in place to assist decentralization of the health sector before the so-called “Big Bang” on January 1, 2001.7 No one could see clearly how the implementation of decentralization would evolve; the important thing was to put mechanisms in place which could respond well to opportunities and risks (both anticipated and unanticipated) which the sector would experience following implementation of the 1999 laws. One especially strong feature of project design was the way those of its components which focused on regional governance (i.e. components A1-A5) assigned explicit functions and roles to the province. Law 22/1999 transferred most authority for health (and other sectors) to the districts; it eliminated the province-district hierarchy and left few explicit functions for the province to perform. It was perceptive of the Bank team to recognize that there were nevertheless still crucial and indispensable functions and roles in the health system that had to be performed at an intermediate level between center and district (e.g. technical support and quality control for district programs, communicable disease surveillance and control, health promotion, medium to large volume procurement, regulatory tasks and personnel management). It was a bold move to propose specific and innovative mechanisms (JHC, TRT, Task Forces, and the Provincial Health Promotion Board) so that the provinces could perform these functions and roles even though the need for them was not clearly stated or recognized in the 1999 laws.8 A significant weakness in design, at least according to regional government officials interviewed by the ICR team, was that while the project proposed a lot of innovative changes it did not give much guidance about how to prioritize them or arrange them in some temporal sequence, or indeed give much guidance about how actually to set about designing and implementing them. “We were expected to implement too much all at once,” they said, and this at a time when they already had to adapt to far-reaching changes in the principles and structures of governance, (especially around the time of the
6 For example the Project Administration Manual was still only in rough draft when the credit was signed.
7 Many of the prescriptions of the 1999 laws were supposed to take effect on January 1, 2001, including the transfer of hundreds of thousands of civil servants to regional governments who had before been under the direct management of the central government. In Indonesia this event is often referred to as the “Big Bang.”
8 The need was however recognized later (in broad terms) in Law 32/2004, which superseded Law 25/1999.
7
“Big Bang” during the first year of the project) quite apart from those changes highlighted for special attention by the project. The project aimed to build capacity, but its design also implicitly presupposed the prior existence of significant capacity, sometimes more than was actually the case. Based on its findings, the ICR team rates Quality at Entry as Moderately Satisfactory although QAG rating for QEA was Satisfactory.
2.2 Implementation The ISRs consistently rated Implementation Progress (IP) as satisfactory or moderately satisfactory. In fact implementation of the project varied considerably by government level and by province. Implementation in Yogyakarta was generally satisfactory, in Lampung moderately satisfactory, and at the central level generally unsatisfactory. Different factors affected implementation at different levels and Yogyakarta was better able to counter negative factors than Lampung. On the positive side the innovative instruments introduced by the project at the provincial level (TRT, JHC, TFs, etc.) were, overall, successful and contributed to the success of the district grants component. Of these mechanisms the Technical Review Team (TRT) was the most successful, although it was difficult to find enough members with sufficient expertise in Lampung. Experience with the Joint Health Council (JHC) confirmed the need for a mechanism supporting cross-district discussion of health issues but it proved unrealistic to expect district heads to attend regular meetings on health, and the mechanism needed fine-tuning. Similarly, Task Force (TF)s proved essential to the reform process but once again Lampung was handicapped by the lack of local expertise. Short term technical assistance (TA) was used but it is less than ideal option for building capacity and providing continuous support. Yogyakarta enjoyed a tremendous advantage in this regard in that it had first-rate consultants close-at-hand at Gadjah Mada University, and the provincial government has a long tradition of working closely with them. According to those responsible for implementing the project, the factor that had the most serious negative impact on project implementation was the lateness in the disbursement of funds by the central government. This problem was outside the control of the implementing agency (MOH). It reached its lowest point when funds for FY 2005 were not released to the districts until October. This was at a time when the Ministry of Finance was introducing a new accounting system; but even in “normal” years funds would not arrive before June or July (May at the earliest). This not only affected the regions’ capacity for implementing activities and their absorption rates, it also undermined the very concept the project was trying to foster, namely, responsible integrated planning and budgeting at local level. Another factor which constrained reform and innovation in the health system at regional levels was that the policy environment produced by the central level was constantly shifting and changing; precise details regarding the distribution of authorities across government levels are still far from perfectly clear. Provinces and districts were reluctant

8
to introduce innovative changes (for example, concerning licensing arrangements, locally-specific HIS, or health insurance) if it was not perfectly clear that they had the legal authority to do so, or if they were concerned that their efforts would be thwarted or annulled later by new regulations issued by the central government. Perhaps more importantly was the shifting role of the province in various formulations of how decentralization will work from very limited role to one to provide capacity and support or to provide the linchpin between the center and the districts. The institutional uncertainty did not provide the supportive environment for more innovation to take place. Civil servants faced considerable uncertainty around the time of the Big Bang, and although the process as a whole went smoothly many individuals were worried by potential loss of status and security. Under these circumstances it was highly ambitious to expect all the activities listed for Phase 1 in the PAD to be completed in 18 months and many took longer.9 A longer period for the first phase may have helped provinces with less capacity like Lampung be more prepared for phase II. The provinces experienced difficulties in conducting reform on human resource management policies as foreseen by the project. The lack of major civil service reform at the national level remains an enormous obstacle to health sector reform.10 When the project was designed it was reasonable to assume that with decentralization regions would enjoy much more control over their personnel than has turned out to be the case; even as civil servants have been transferred to regional offices they still remain part of a national civil service system, and PP 25/2000 and subsequent policy instruments make it clear that the central government retains essential control over the entire service. There were significant changes in the national policy for regulatory framework during the course of the project. Law 29/2004 (on medical practice of doctors and dentists) provides a good model for establishing a legal framework for setting national standards for health professionals on the one hand, and for licensing health professionals at the regional levels in a way that incorporates competency tests based on national standards on the other. Draft legislation for the licensing of nurses is currently before the parliament. Meanwhile, the licensing of midwives is regulated by a 2002 MOH decree. In 2005 a new health financing scheme, Askeskin, was introduced to cover the poor using Government money saved by reducing the oil subsidy. Askeskin is built on the social safety net model (JPS-BK) developed at the time of the Asian financial crisis. In the PAD the Bank, while recognizing the merits of JPS-BK as an emergency measure cautioned against its adoption and extension over the long term because of issues of sustainability
9 Because of delays in starting the project Phase 1 was already truncated and totaled less than 18 months, adding to the difficulties of completing Phase 1 activities before the scheduled end of the phase.
10 See Staffan Synnerstrom, “The Civil Service: Towards Efficiency, Effectiveness and Honesty,” in Indonesia: Democracy and the Promise of Good Governance, ed. Ross H. McLeod and Andrew MacIntyre. Singapore: Institute of Southeast Asian Studies, 2007.

9
and other distortion effects. When Askeskin became a national policy, project provinces had little option but to adopt the scheme. Yogyakarta province combined Askeskin financing with their own insurance program developed under the project, Jamkesos, and increase coverage to include the non-poor population. Until February 2006, the Project Director position at MOH was assigned to the Secretary General because PHP I is a sector-wide project and involves all divisions, while the Deputy Director position was assigned to the Head of Bureau of Planning. However, these positions within MOH are not normally involved with project implementation. The unit was soon overwhelmed with the project management tasks and delegated most management responsibilities to the CPCU. This was even more pronounced when 4 other similar projects (two new projects each financed by the World Bank and the ADB) were also put under the Bureau of Planning. Because the CPCU was an ad hoc unit, it did not have the credibility to bring key central level units into project implementation and this, for the large part, explained the poor performance of the central level components. Implementation in Yogyakarta was seriously disrupted by the 2006 earthquake.
2.3 Monitoring and Evaluation (M&E) Design, Implementation and Utilization M&E was uneven and overall less than satisfactory. M&E Design M&E design was weak. As discussed in Section 1.2, the three key performance indicators for the PDO listed in the PAD were too broad. The PAD (Annex 1) also contained a large number of output indicators (with 9 of them in the Credit Agreement). The output indicators actually included both process and output variables and ranged across 3 components (A1, A2 and A4). There was no clear rationale given for some of the targets sets for some indicators. For example setting a target of reducing non-health staff by 20 percent across the board seems arbitrary. Other indicators were not easy to measure and with some effort could have been better aligned with existing surveys (e.g. the contact rate of poor people at health centers): More effort could have been made in terms of ensuring availability of reliable data for some of the indicators. M&E Implementation The weak M&E design and the week capacity of the unit put in charge of this activitiy - the independent Research Unit (RU) resulted in difficulty in getting a good idea about the performance of the operation. The consultancy company contracted by the MOH to run the RU seems to have lacked some of the necessary social research skills. The MOH gave the contract for the “second” Final Review, conducted at the end of 2007, to another company which did a better job. In addition, for some indicators related to financing or budgets, the fragmentation and changes in the system made it very hard to get data or trends as the system kept changing. Additional studies were commissioned for providing data needed for the mid term review and end of project implementation.

10
M&E Utilization M&E utilization by project management was slight. Those responsible for managing the project rarely had the data they needed for analyzing problems in depth and improving performance. The project was also subjected to a number of GOI and Bank audits, which did uncover some financial irregularities. This focused management attention much more on the fiduciary monitoring and less so on the outputs and outcomes of the operation.
2.4 Safeguard and Fiduciary Compliance Private auditors selected by the implementing agency for conducting interim audits in the early years of PHP I did not perform well. When corruption at the MOH was uncovered in 2005 involving the CPCU for PHP II, the MOH took action, while the Bank conducted a special mission and proposed an action plan to strengthen financial control of the whole series of provincial operations (3 in total) of which the current project is the first (referred to as PHP I, PHP II and PHP III) and send a clear message of deterrence to all PHP staff, as well as attempting to resolve the specific issues of PHP II. The action plan included (i) strengthening of controls by removing financial and procurement management control from the Bureau of Planning to relevant units within MOH, (ii) recruiting a firm to conduct internal audits of the projects while working with the IG’s office to strengthen internal control within MOH, (iii) expanding investigations to include more samples to determine the full extent of ineligible expenditures, (iv) appointing BPK to replace BPKP as external auditors, and (v) temporary withholding payment in PHP II until immediate actions were taken. All actions except for (iii) and (v) were also applied to PHP I and PHP III. Until the end of the project, recruitment of a firm to conduct internal audit has not been completed. Occasional financial irregularities occurred in PHP I, especially involving procurement at the district level. In general, findings involved small contracts and did not result in the Bank declaring misprocurement. District staff were not familiar with Bank rules and procedures and despite efforts to clarify project management manual and increase the frequency of procurement training and supervision, officials told the ICR team that it remains difficult to reconcile Bank auditing and procurement requirements with those of the GOI. This is obviously an area that needs closer attention in the design of future projects.
2.5 Post-Completion Operation/Next Phase Yogyakarta assured the ICR team they have mechanisms in place to sustain positive outcomes beyond the life of the project. The province released a Governor decree to legalize the existence of the provincial health insurance body (Jamkesos) and the quality council (Badan Mutu). It also continued to allocate funding for expanding the implementation of the integrated health information system in collaboration with the five districts in the province. Without block grants to support spending for health development, the district health offices have no option but to compete with other sectors for local government funding as happened prior to the project. Nevertheless, there was
11
consensus among those interviewed by the ICR team that the project has contributed to improving the capacity of the districts in developing a stronger plan, useful for advocating for more resources for health. The central government has cut funding for health in FY 2008 (although there were significant increases in earlier years so the net effect is not clear and a health financing study is currently underway).
3. Assessment of Outcomes
3.1 Relevance of Objectives, Design and Implementation The two PDO were both of high strategic relevance to the development of the health sector at the time of credit approval, and they remain of high strategic relevance today. Bringing about effective health decentralization in the provinces is still an important policy objective, and the MOH still needs help in carrying out its new roles and responsibilities under decentralization. The relevance of some of the more specific objectives and targets of specific project components, however, shifted during the history of the project as the central government progressively revised and redefined elements of the national policy environment within which the project was being implemented. Law 1/2004, for example, introduced the concept of Badan Layanan Umum (BLU, or General Service Unit), which introduced new principles regarding how government units might retain and utilize revenues obtained from providing services to the public: this meant the project’s focus on converting hospitals and health centers to “swadana” status as part of a more general resource mobilization strategy in the health sector needed to be reconsidered and aligned with the new policy. A series of decrees and regulations issued by the Ministry of Home Affairs (MOHA) defining and redefining the functions, responsibilities and organizing principles for provincial and district governments was especially important. While the flexibility in the project design was very helpful in light of all these changes, the government system and budget revisions to allow the project to use the flexibility delayed implementation and at times limited the flexibility offered by the design.
3.2 Achievement of Project Development Objectives The Project Development Objectives of PHP I were defined broadly, and so were the three PDO Indicators specified in the PAD. In view of this, the ICR uses the more specific objectives and outputs of the eight project components in order to arrive at an assessment of the extent to which the two PDOs were achieved. In the subsections below we first assess the extent to which the project achieved the first PDO by achieving the objectives of the first 5 components; we then assess the extent of achievement of the second PDO by reviewing the achievements of the last 3 components First PDO/Provincial Level: Bring about effective health decentralization in the provinces of Lampung and Yogyakarta. This involves protecting health services of the

12
poor and public at large, initiating key sector reforms, and putting health financing on a firm footing. Component A1. Managing Decentralization (District and Provincial) Performance on items (a) restructuring health service organizations and (b) reorganizing the management structures of entities implementing health services are rated by the ICR team satisfactory in both Yogyakarta and Lampung provinces.11 The transfer of scores of civil servants previously working for local offices of the central government (Kanwil and Kandep) in the 2 provinces to local government health offices (Dinas) under the provincial governor or the district head went smoothly, as indeed was the case throughout the country, and the governors and district heads involved promptly passed relevant decrees establishing appropriate organizational structures in accordance with prevailing laws. Project resources were used to fine-tune and augment the new organizational structures and socialize its principles and mechanisms. The introduction of Joint Health Councils (JHCs), Technical Review Teams (TRTs) and Task Forces (TFs) at the province level proved especially valuable. Yogyakarta went further than Lampung and established some additional innovative structures, for example, Provincial Health Promotion Board (HPB), Provincial Health Service Quality Board (BMPK), and Technical Assistance Teams (TATs) that are not to be found in Lampung. Performance on item (c) developing and implementing new human resource management policies, is rated moderately satisfactory in Yogyakarta and moderately unsatisfactory in Lampung. Achieving the objective of developing and implementing new human resource management policies was essentially beyond the control of those responsible for the project without further enabling regulations from the central government. Nonetheless regional governments do have significant control over the allocation of staff and various privileges, and Yogyakarta appears to have taken advantage of these opportunities more than Lampung for example by undertaking systematic study of their personnel needs and pushing against the limits of national policy as much as possible. Performance for item (d) at the provincial level, developing and implementing new health information systems covering health indicators, and service delivery, facility and staffing information, is rated satisfactory for Yogyakarta and unsatisfactory for Lampung. Yogyakarta is now well on the way to having a good HIS. Lampung’s plans to introduce a province-specific HIS have been less successful although they are working to adopt some of the work done by Yogyakarta. The major uncertainty relates to the center. Ideally the center should provide general guidance and the provinces tailor the model to their needs and conditions. However, the delays and lack of certainty from the center have hindered this. The hope is that the center will take into account and build on these positive developments if they move forward on a new HIS.
11 More data and analysis used by the ICR team to determine their ratings are given in Annex 2.

13
Performance on item (e) strengthening public accountability mechanisms, is rated satisfactory in Yogyakarta and unsatisfactory in Lampung. There are effective public accountability mechanisms throughout Yogyakarta province for example, the complaint hotline service, public accountability forum, health newsletter and so forth, but not yet in Lampung. Performance on item (f) strengthening the policy regulatory framework for health services, including the establishment of a health council and a health care accreditation agency at the provincial level, is rated satisfactory for Yogyakarta and unsatisfactory for Lampung. Yogyakarta has had new licensing systems for midwives and nurses which include competency tests since 2003, as well as having taken the lead on licensing for doctors and dentists since before the new 2004 national law. An important part of the system is a Quality Council (Badan Mutu) established by the province as a semi-independent body for conducting provider assessment against national standards and providing recommendation for licensing and accreditation. Lampung is behind on this path. Component A2. Mobilizing Resources (District and Provincial) Performance on item (a) at the provincial level, developing and implementing decentralized health service planning, budgeting and financing systems designed to permit districts to plan and develop efficient, effective and equitable programs according to community needs, is rated satisfactory in Yogyakarta and moderately satisfactory in Lampung. The capacity for planning and budgeting increased markedly in all districts and the districts gained considerable experience in this area through preparing annual grant proposals under the project. The province-level systems supporting these activities are more advanced and better organized in Yogyakarta than in Lampung. Performance on item (b) converting hospitals, health centers and other health service units into autonomous units (swadana)12 which will possess, inter alia, the authority to apply cost recovery measures, is rated moderately satisfactory in Yogyakarta and moderately unsatisfactory in Lampung, although this is one of those objectives which maybe should have been adjusted to bring it more into line with a changing national policy agenda. The 2007 Project Final Review shows that in Yogyakarta all 5 district hospitals are swadana, and 3 of the 5 districts have at least 1 puskesmas swadana (all are swadana in Slemen District), but overall the percentage is less than 40 percent. In Lampung only 2 of 10 district hospitals are swadana, and only 3 districts have at least 1 puskesmas swadana. Law 1/2004 supersedes the earlier MOHA decree and introduces the idea of Badan Layanan Umum (BLU). A BLU is given considerably more autonomy regarding the way
12 According to the original definition (MOHA decree 92/1993) “swadana” status means a unit has been granted authority to retain revenues from its provision of services and to use them for operational expenses. Following decentralization the term came to be used in a variety of ways expressing some idea of relative autonomy.

14
it can spend its revenues. The central government’s policy is that all public service units will eventually become BLU. Thus, while it may appear disappointing that more units did not become “autonomous” in the swadana sense during the course of PHP I, the fact is the 2004 law effectively meant it was often not worth districts investing in swadana when a new definition of “autonomy” was being promoted by the central government. The project component objective here needed to be adjusted to stay relevant, but the more important point is that the central government has introduced policies which move in the direction supported by the project, and in fact go further in this direction than the project envisioned. Performance on item (c) at the provincial and district/municipal levels, developing, piloting and, if appropriate, implementing a health insurance system and/or managed care, is rated satisfactory in Yogyakarta and moderately satisfactory in Lampung, although a large part of the increase in health insurance coverage in both provinces is due to the introduction of Askeskin, a new MOH health-scheme targeted at the poor. According to Susenas 2006, health insurance total coverage was 42% in Yogyakarta and 22.6% in Lampung. The percentage may have increased in 2007 with the expansion of the Askeskin program. This is almost certainly the case in Yogyakarta, which has successfully introduced its own province-wide health insurance scheme, Jamkesos. Yogyakarta believes they now have 60 percent total coverage. Jamkesos appears to be developing well; the Bank’s aide-memoires have suggested in fact that it may be developing too quickly. Kota Metro in Lampung has fragmentary plans to introduce its own health insurance system but has successively delayed implementation through lack of funds. Component A3. Improving Health Service Access and Quality (District and Provincial). This component was only implemented during 2000 and 2001. Performance on item (a) implementing specific health service activities, including the refurbishing of health care facilities, upgrading medical equipment, increasing the number of mobile health service facilities and contracting private health service providers for the delivery of basic health services to designated areas, is rated moderately unsatisfactory since relatively little was procured under this component during Phase 1 and no provider contracting took place. Performance on item (b) implementing quality assurance programs and upgrading the quality of health sector personnel through the implementation of fellowship programs, is rated moderately satisfactory since many fellowships were awarded.

15
Table 2. Fellowship Program 2000-2007
Location D3 S1 S2
Lampung Province 478 246 101 Yogyakarta Province 276 139 94 Central level 7 13 Total Fellowship 754 392 208
Note: D3: Academy level, S1: Bachelor level, S2: Masters level Performance on item (c) establishing a health promotion board in Yogyakarta to coordinate health public and private sector promotion activities, is moderately satisfactory. The health promotion board was established and despite some shortcomings performed well, but rather than continue to become an independent unit, the board became an integral part of the Provincial Health Office. Performance on item (d) providing specific drugs and supplies based on district/municipal proposals, is not rated since relatively little was procured under this component during Phase 1. Component A4. Grants (Districts). This component aimed at: “Financing (a) Eligible Activities through the provision of MD and RM Grants and (b) Eligible Programs through the provision of District Grants”. The distinction between the two grants disappeared during implementation as managing decentralization and resource mobilization efforts became an integral part of the District Grant proposals. Performance on the District Grants is rated satisfactory for Yogyakarta and moderately satisfactory for Lampung. Four rounds of annual district grants supporting effective decentralization of health at the district level were implemented. The process was extremely difficult for many districts in the first and second years, but officials have learned from experience and implementation was much smoother by the end of the project. The Final Review document showed this improvement, and district-level officials acknowledge how they have learned to plan and budget the district health system with the support of the project. Province-level teams supporting the proposal writing and proposal assessment process have also learned from working with project support. The main problem with using the financing mechanism in Lampung is that some district heads regard the mechanisms as a way to fund routine health services. Some districts have embraced the idea of innovation more enthusiastically than others. The main problem with implementation was the late disbursement of funds by the central government. Component A5. Project Management (District and Provincial). This component aimed at: “Establishing, at the provincial and district/municipal levels, a management and administrative structure appropriate for the coordination and carrying out of health service program and Project activities”. This component is rated satisfactory in Yogyakarta and moderately satisfactory in Lampung. The management structures comprising Provincial Central Implementation Units (PCIU) and District Implementation Units (DIU) were established and performed well, despite specific shortcomings in some units.

16
The Contribution of Component Outputs to the First PDO Table 3 summarizes the achievement of project component objectives for province and district levels in Yogyakarta and Lampung. Table 3. Achievement of Project Component Objectives for Components A1-A5
Component Objective Yogyakarta Lampung
Component A1: (a) and (b) Restructuring & reorganization
Satisfactory Satisfactory
(c) New HR policies Moderately satisfactory Moderately unsatisfactory (d) HIS Satisfactory Unsatisfactory (e) Public accountability Satisfactory Unsatisfactory (f) Regulatory framework Satisfactory Unsatisfactory
Component A2: (a) Decentralized planning & budgeting
Satisfactory Moderately satisfactory
(b) Swadana units Moderately satisfactory Moderately unsatisfactory (c) Health insurance Satisfactory Moderately satisfactory Component A3: (a) Health service activities Moderately unsatisfactory Moderately unsatisfactory (b) Quality assurance Moderately satisfactory Moderately satisfactory (c) Health promotion board Moderately Satisfactory Not applicable (d) Drugs & supplies Not rated Not rated
Component A4: District Grants Satisfactory Moderately satisfactory
Component A5: (a) Management structure Satisfactory Moderately satisfactory
Overall Assessment of First PDO Outcomes
Satisfactory Moderately satisfactory
Source: Data abstracted from aide-memoires, ISRs, mid-term and final reviews, Susenas, and ICR interviews. In the case of Yogyakarta it appears that all five project components reached a satisfactory level of performance in achieving their respective objectives. Health services in Yogyakarta have been strengthened; resource mobilization capacities have been enhanced; health service access and quality have been improved; successive rounds of annual grants to districts were successfully implemented; and a viable management and administrative structure at both province and district levels were established for the health service program and project activities. Instances where component outcomes were rated less than satisfactory do not appear to be so serious as to jeopardize effective health decentralization in the province as a whole. The ICR team rates overall assessment of the First PDO Outcomes in Yogyakarta as satisfactory.

17
Project components in Lampung were not so successful in achieving their respective objectives. The ICR team rates overall assessment of the First PDO Outcomes in Lampung as moderately satisfactory. However, one should note that it may have been too much to expect the two very different provinces to meet the same targets. In fact Lampung showed significant progress in terms of the quality of the district proposals and activities during the life of the operation. Second PDO/Central level: Help the central ministry (MOH) carry out its new role to provide analysis of key issues, advocacy of best practices and standards, and support for local initiatives and innovation. Component B1. Managing Decentralization (Central). This component aimed at: “Strengthening (a) the institutional capacity of MOH to provide support to provinces and districts in fulfilling their health sector responsibilities allocated to them under the Law on Regional Government, No. 22/1999 through conducting policy studies, sponsoring national seminars and workshops, and strengthening its policy and technical analytical capabilities and its health service advocacy and information dissemination services and (b) national capacity to evaluate health policy interventions through the establishment of an independent research unit”. Performance on item (a) is rated unsatisfactory. Seminars and workshops were conducted, but no significant policy-related studies were completed under the project and the project’s impact on strengthening MOH’s analytical and advocacy capabilities appears negligible. Some specific proposals regarding the restructuring of the organization of the central Ministry, intergovernmental fiscal transfers, decentralized workforce policies and decentralized information systems were agreed during project midterm review. MOH hardly used project resources to move those agenda forward and little was achieved at project closing. Performance on item (b) is similarly rated unsatisfactory. An independent research unit was established but it was under funded and contributed little to expanded MOH’s capacity for evaluating policy interventions. Component B2. Resource Mobilization (Central). This component aimed at: Strengthening the institutional capacity of MOH to develop and administer a program for the financing of specific health-related programs at the provincial and district/municipal levels by providing Matching Grants. This component is rated moderately unsatisfactory. There was good demand from districts for the matching grants as indicated by the number of proposals received by the CPCU after the availability of the grant was announced. Nevertheless, the idea to use the grant as a tool for MOH to influence district spending for health was not institutionalized. Although a MOH technical unit helped the CPCU in reviewing district proposal, day to day management of the Matching Grants program was the task of the CPCU, an ad hoc unit. Matching grants were no longer offered to the districts after the midterm review.
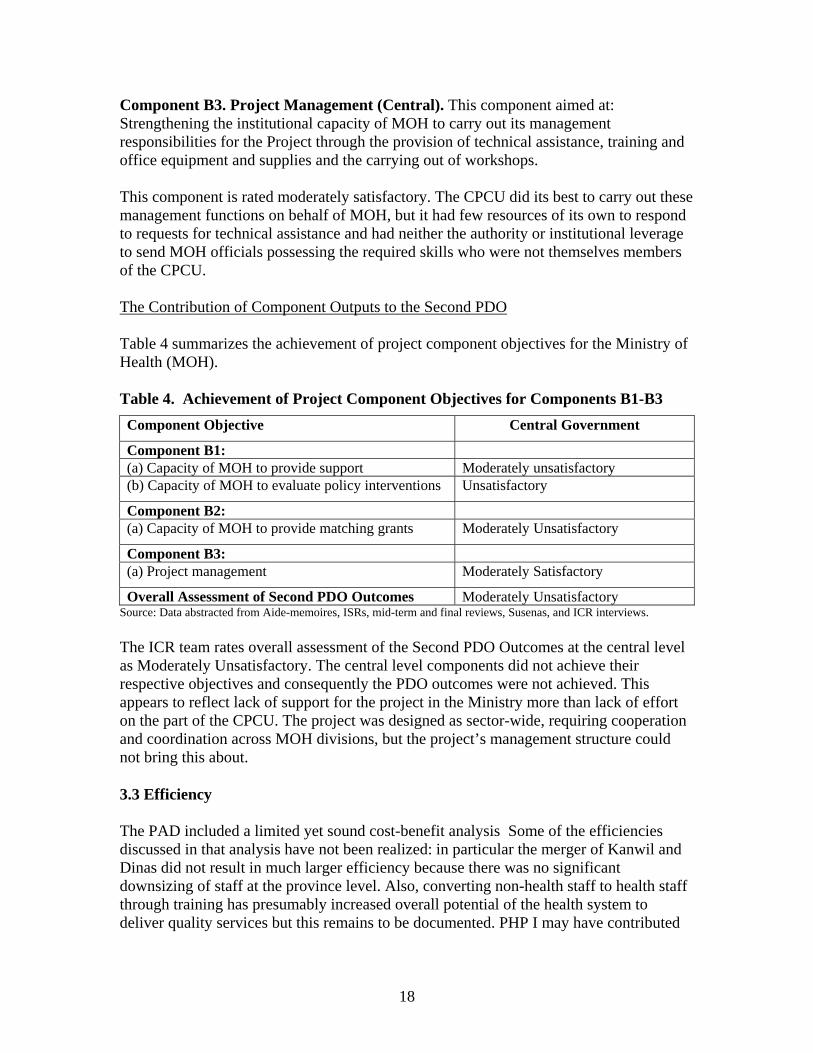
18
Component B3. Project Management (Central). This component aimed at: Strengthening the institutional capacity of MOH to carry out its management responsibilities for the Project through the provision of technical assistance, training and office equipment and supplies and the carrying out of workshops. This component is rated moderately satisfactory. The CPCU did its best to carry out these management functions on behalf of MOH, but it had few resources of its own to respond to requests for technical assistance and had neither the authority or institutional leverage to send MOH officials possessing the required skills who were not themselves members of the CPCU. The Contribution of Component Outputs to the Second PDO Table 4 summarizes the achievement of project component objectives for the Ministry of Health (MOH). Table 4. Achievement of Project Component Objectives for Components B1-B3 Component Objective Central Government
Component B1: (a) Capacity of MOH to provide support Moderately unsatisfactory (b) Capacity of MOH to evaluate policy interventions Unsatisfactory
Component B2: (a) Capacity of MOH to provide matching grants Moderately Unsatisfactory
Component B3: (a) Project management Moderately Satisfactory
Overall Assessment of Second PDO Outcomes Moderately Unsatisfactory Source: Data abstracted from Aide-memoires, ISRs, mid-term and final reviews, Susenas, and ICR interviews. The ICR team rates overall assessment of the Second PDO Outcomes at the central level as Moderately Unsatisfactory. The central level components did not achieve their respective objectives and consequently the PDO outcomes were not achieved. This appears to reflect lack of support for the project in the Ministry more than lack of effort on the part of the CPCU. The project was designed as sector-wide, requiring cooperation and coordination across MOH divisions, but the project’s management structure could not bring this about.
3.3 Efficiency The PAD included a limited yet sound cost-benefit analysis Some of the efficiencies discussed in that analysis have not been realized: in particular the merger of Kanwil and Dinas did not result in much larger efficiency because there was no significant downsizing of staff at the province level. Also, converting non-health staff to health staff through training has presumably increased overall potential of the health system to deliver quality services but this remains to be documented. PHP I may have contributed

19
to improved services at health centers but average number of staff per center has not declined and the health centers are still overstaffed.
3.4 Justification of Overall Outcome Rating The ICR team rates overall outcome as moderately satisfactory (consistent with ISR ratings). More specifically, the overall outcome rating for Yogyakarta is satisfactory, for Lampung moderately satisfactory, and the overall outcome rating for the central level is unsatisfactory. The justification for these ratings is as follows: Project objectives and project design were largely appropriate to the challenges brought upon by decentralization in health, but during implementation it became clear that the design was too broad and ambitious, particularly for under resourced and low capacity provinces like Lampung province. Project performance is much driven by the performance of the provinces as project design and components gave more emphasis on reform at the sub-national level, and the District Grants were by far the largest component of PHP I. The achievement of the first PDO in Yogyakarta is satisfactory as the province has initiated key sector reforms and has made significant strides towards putting health financing on a firm footing. The performance of Lampung Province is moderately satisfactory. The province has discussed and planned a number of key sector reforms but so far has implemented few, and likewise is still far from putting health financing on a firm footing. However, the project does appear to have considerably enhanced overall capacity of the sector, even if that has not resulted yet in a lot of institutional changes or reform. Achievement of the second PDO is Moderately Unsatisfactory. The MOH has begun to perform new roles since decentralization but for the most part it has not chosen to do so in the ways envisioned by the project. The analysis of key issues it provides the sector is short on quantity and quality, its advocacy of best practices and standards is more rule-oriented than results-oriented, and it is not proactive in supporting local innovations.
3.5 Overarching Themes, Other Outcomes and Impacts (a) Poverty Impacts, Gender Aspects, and Social Development Many of the project activities in Yogyakarta and Lampung were seen by the project as pro-poor, but it is difficult to assess their impact. According to Susenas data, utilization of outpatient care in public facilities by the poor (the lowest income quintile) in Lampung has increased from 37.86% in 2002 to 40.62% in 2006 and from 33.48% to 36.14% in Yogyakarta for the same years. An increase for the same years was also observed for the second lowest quintile, from 27.94% to 32.94% in Lampung, and from 30.58% to 36.37 % in Yogyakarta. The percentage may have increased further in 2007 because of the expansion of the Askeskin program. The introduction of Askeskin in 2005 has undoubtedly improved access for many poor people. It seems reasonable to conclude that availability and accessibility of health services for the poor have to some extent been protected.

20
(b) Institutional Change/Strengthening No further institutional change in addition to that discussed elsewhere in the ICR. (c) Other Unintended Outcomes and Impacts (positive or negative) Based on what they have learned from and achieved with PHP I, both provinces have indicated a follow-up project would be welcome. Attitudes at the central level towards a follow-up project are currently colored somewhat by the experience of corruption being uncovered at the MOH in the case of PHP II and the Bank’s response to this.
3.6 Summary of Findings of Beneficiary Survey and/or Stakeholder Workshops No Beneficiary Survey conducted.
4. Assessment of Risk to Development Outcome ICR Rating: Substantial The ICR team rates the risk to development outcomes achieved in Yogyakarta as negligible to low. Yogyakarta’s health system is robust and the benefits gained from PHP I are well institutionalized. The system is forward-looking and well supported by the province. The ICR team rates the risk to development outcomes achieved in Lampung as substantial. Lampung’s health system is far less advanced than Yogyakarta’s and the benefits it has gained from PHP I are more in the nature of milestones reached towards attainment of the project’s objectives rather than achieving the objectives themselves (e.g. regarding health insurance or HIS). With reduced funds from the central government likely and the local budget very limited, there is significant risk these milestone benefits will fade. The risk to development outcomes at the central level is high since these outcomes were themselves rated unsatisfactory; whatever benefits the center gained from the project are diffuse.
5. Assessment of Bank and Borrower Performance
5.1 Bank Performance (a) Bank Performance in Ensuring Quality at Entry The ICR team rating for QEA is Moderately Satisfactory. Project objectives were very relevant and project design was an appropriate response to the challenges confronted at the time by a rapidly changing health sector. However, project scope was very ambitious and took on too broad a range of reform activities given the turmoil introduced by decentralization. Monitoring and evaluation was weak resulting in difficulties in conducting routine monitoring of project performance.

21
(b) Quality of Supervision The ICR team rates quality of supervision as Moderately Satisfactory. The archived ISR and aide-memoires show that the Bank monitored the project’s progress carefully, discussed problems with the implementing agency and other stakeholders, and made constructive suggestions when necessary.13 Bank staff assumed a heavy workload for the project (and other PHP projects) when they undertook to review all district grant proposals (at least for the early years of this granting process) and their supervision contributed to the success of this component. Government officials interviewed in the two provinces by the ICR team were appreciative of the expertise and support the Bank provided and welcome interactions with the Bank; in fact they made it clear the provinces would like more contact with the Bank in the future if possible. (c) Justification of Rating for Overall Bank Performance Overall Bank performance rating Moderately Satisfactory.
5.2 Borrower Performance (a) Government Performance Moderately Unsatisfactory. The enabling environment provided by the central government had significant shortcomings for project implementation from the point of view of lateness in disbursement of funds, confusion over precise allocation of authorities among government levels, and inadequate response to shortcomings at the MOH. (b) Implementing Agency or Agencies Performance Moderately Satisfactory. There were significant shortcomings at the MOH: (i) the Ministry has not reorganize or downsized in a way consistent with its new functions under decentralization; and (ii) despite the best efforts of those on the CPCU the MOH has not been able to provide much constructive support or technical guidance to the provinces and districts. Officials in the provinces expressed considerable frustration with the MOH to the ICR team. On the other hand, performance of the provinces and districts were Satisfactory for Yogyakarta and Moderately Satisfactory for Lampung. Yogyakarta particularly was not much influenced by the absence of the center, and many of its reform ideas were an inspiration to the other provinces, even those beyond Lampung. (c) Justification of Rating for Overall Borrower Performance The ICR rates Borrower Performance as Moderately Satisfactory. This rating reflects the Moderately Satisfactory rating of the two provinces combined, and the fact that the project put much larger weight on investment and interventions in the province and district components.
13 See also S. Lieberman and P. Marzoeki, 2004. “Decentralization in Indonesia’s Health Sector: The Central Government’s Role.”

22
6. Lessons Learned A number of lessons can be drawn from this assessment of PHP I experience. Positive institutional change is a valuable public good and needs to be promoted as such. The big success of PHP I is in Yogyakarta. Although the project’s first development objective (PDO) is vaguely worded there is broad consensus that the changes brought about in the health in Yogyakarta sector since 2001 do add up to an unambiguous case of “effective health decentralization.” Yogyakarta started off at the beginning of PHP I as a relatively well resourced province and it enjoys a unique status within Indonesia. Local officials at both the province and district level argue that support from the project did in fact make a big difference. The gains are not for the people of Yogyakarta alone. Officials from around the country come to Yogyakarta to study the Yogyakarta model and learn practical lessons from Yogyakarta’s experience. The success of Yogyakarta illustrates the indispensable role of sound technical advice. The city of Yogyakarta is home to one of the country’s preeminent universities. Experts from Gadjah Mada University have a long history of working closely with the provincial government. The PHP I design relied heavily on technical inputs and expert advice on the Technical Review Teams, Task Forces, and in some cases on Joint Health Councils; and consultants were needed to undertake special studies and operational research. Lampung lacks such expertise locally and had to import it from elsewhere, mostly from Yogyakarta, but in their experience this was often not fully effective. Special attention needs to be given to making technical inputs more effective for less-developed provinces like Lampung. There is a need over the longer term to develop the capabilities of local consultants. Projects dealing with decentralization should pay special attention to the quality and quantity of the TA available for the local governments. The same point can be made more generally, not just with regard to technical inputs. Projects designed to bring about more effective health decentralization in provinces need to include special interventions to make sure the inequalities across regions are addressed. The central government has limited capacity for decentralization and has not adequately adjusted its structure and functions to respond to the needs. In the early days of decentralization in Indonesia expert and policymakers focused on the limited capacity of districts and provinces to assume their new responsibilities. That the central government needed to scale back on its implementation activities and assume new leadership roles was assumed to be a relatively easy transition. But in time the inability of the MOH to restructure and change its mind-set have emerged as major obstacles to effective decentralization of the health system. Future projects need to address or adapt to the weak leadership from the central level. In turbulent times projects need a flexible decision-making and management structure. PHP I was designed to respond to the government’s decentralization laws of 1999 and to implement reforms within the framework of that legislation. While the project design was quite flexible and built in annual reviews of the district block grants and operational manual that could be changed as the project advanced, the flexibility was not always used. This is in part due to the momentum and time it takes to get some activities underway as
23
well as the rigid government system and budget. Moreover, the flexibility was great for the stronger province but provinces with weaker capacity can benefit from more focused approach. As stated in the Guidelines for the PAD, Project Development Objectives should focus on the outcome for which the project can be held accountable given the project’s duration, resources and approach. Performance indicators (PI) need to be selected more thoughtfully, defined more precisely, and measured much more carefully. If performance indicators with targets must be set, maybe such targets could be conditional given the uncertainty surrounding current changes in governance. Moreover, both GOI and Bank could have tried to formally revise the indicators during the life of the operation. While the Project gave excellent insights on institutional changes and why those should happen, in many areas it was less specific on the how. While that is part of the flexibility of the design, in many areas the provinces and districts needed some more guidance and lessons from other provinces and countries to learn how best to proceed. Projects aimed at reforming institutions need to be grounded in a realistic understanding of how, when and why institutions change, and how they can be expected to change in the specific political and cultural contexts in which the projects operate. The PHP I PAD was rich in insights about the kind of changes in institutional arrangements needed to bring about effective decentralization of the health sector, and about how to sustain reformed institutions with new financial arrangements. It was not so rich in insights regarding how one goes about designing the reformed institutions in any detail (what are the principles of institutional design which should be employed?), or about how one gets rid of the old ways of doing things and replaces them with the new (how do you overcome vested interests in the old order and align incentive structures with the new?). Simply proposing new and better ways of doing things is never enough; change invariably means some gain more than others. Governance in Indonesia is a hybrid of patrimonial and legal-rational structures and processes. The implications of this, needs to be thought through more carefully in future during project preparation. More lessons could undoubtedly be drawn by undertaking a comparative study of all decentralization experience including those supported by donors like the World Bank and ADB. Such a study could focus on the different ways provinces have established the province-district relationship, the relative costs and benefits of each, and the variety of ways districts and provinces have developed to exercise autonomy in the health sector despite continuing lack of clarity in the policy environment and their dependency on central government funding.

24
7. Comments on Issues Raised by Borrower/Implementing Agencies/Partners (a) Borrower/Implementing Agencies The following is the summary of comments received from MOH. Many of these comments are consistent with findings of the ICR team: - The start of project implementation coincided with the launch of decentralization
giving large autonomy to the district level. This made collaboration between the province and the districts difficult because the districts disregarded the role of the province although in reality many districts had weak capacity.
- PHP I proposed innovative ways to change the health system, but a five year project is too short for large system changes envisioned by the project.
- The timeline for achieving performance indicators was too short given the long time required to carry on systems reform. Some of the indicators, particularly those related with personnel policies, were contradictory to existing laws.
- The length of the preparation phase (Phase I) was too short to produce meaningful outputs for adoption by the districts, and therefore the work of the task forces had to continue to Phase II.
- Implementation of the District Grants is considered as an innovative way to build capacity of the districts in planning and budgeting.
- The role of the JHC was only limited to approval of district proposal rather than the expected larger role of developing province level health policies. Limited involvement of the Bupatis (Head of the District) in JHC assemblies was seen as the main reason for ineffectiveness of the JHC.
- The TRT is considered successful in improving the capacity of districts/cities in developing annual proposals.
- The weak capacity of Lampung compared to that of Yogyakarta was mainly because some districts in Lampung were new districts with less qualified human resources and the lack of technical assistance from a locally based University.
- The provinces and districts benefited from PHP I because the project gave the opportunity to conduct health reform trials, and pilots that usually could not be financed by government own budget.
- Contradiction between the Bank’s procurement guidelines and the Government’s Keppres 18 was the source of confusion to the implementing units, although the use of procurement plans was considered as a useful tool for monitoring procurement activities. Moreover, procurement activities were often delayed because of delays in developing procurement plans, changes among procurement committee members and

25
their insufficient knowledge of Bank procurement guidelines, weak capacity in TOR development, and lengthy process in obtaining Bank no objection letter.
- World Bank requirements sometimes caused delays in execution of procurement, for example the requirement to conduct a feasibility study prior to construction of a new facility, or requirement to reach consensus on performance indicators prior to buying computers for developing the health information system.
- Project Management Reports (PMR) is a useful tool for project monitoring. On the other hand, multiple audit activities were considered too many and time consuming. Moreover, the auditors do not always have the same perception when interpreting Bank regulations.
- Disbursement of project funds was very much influenced by procedures and regulations from MOF that often resulted in delays in budget release.
(b) Cofinanciers N/A (c) Other Partners and Stakeholders N/A

26
Annex 1. Project Costs and Financing
(a) Project Cost by Component (in USD Million equivalent)
Components Appraisal Estimate (USD millions)
Actual/Latest Estimate (USD
millions)
Percentage of Appraisal
A1 MANAGING DECENTRALIZATION (DISTRICT AND PROVINCIAL)
3.81 4.57 120
A2 MOBILIZING RESOURCES (DISTRICT AND PROVINCIAL)
1.73 1.42 82
A3 IMPROVING HEALTH SERVICE ACCESS & QUALITY (DISTRICT AND PROVINCIAL)
4.17 1.90 45.6
A4 GRANTS 63.71 99.27* 155.8 A5 PROJECT MANAGEMENT (DISTRICT AND PROVINCIAL)
0.78 2.00 256
B1 MANAGING DECENTRALIZATION (CENTRAL)
2.87 1.46 50.9
B2 RESOURCE MOBILIZATION (CENTRAL) 0.56 0.13 23.2
B3 PROJECT MANAGEMENT (CENTRAL) 1.00 2.29 229
Total Project Costs 78.63 113.04* 143.8
Total Financing Required 78.63 113.04* 143.8
* Including 2 year District Grant extension
(b) Financing
Source of Funds Type of Cofinancing
Appraisal Estimate
(USD millions)
Actual/Latest Estimate
(USD millions)
Percentage of Appraisal
International Development Association (IDA) 38.00 31.26 82.3

27
Annex 2. Outputs by Component
Province and District Component Component Yogyakarta Province Lampung Province
A.1: Managing Decentralization
Restructuring Health organization in the Provinces and Districts
2001, two health offices (Dinas and Kanwil) and two social welfare offices were merged into one office (Dinkesos) 2004, health and social welfare were split into two separate offices (Dinkes and Dinsos)
2000, merging of the two health offices
Human resource management and development
2002, staffing for the new organization structure including development of functional positions A study on incentive system was completed 2003, a study on career development and a fellowship plan was completed 2007, fellowship completed: D3: 276, S1:139, S2: 94
2002, a human resources master plan and a fellowship plan were developed 2003, a study on the use of credit points for assessing the performance of functional staff 2007, a survey of characteristics of public and private doctors, nurses, and midwives was completed. Data was used among others for selection of training participants. 2007, fellowship completed: D3: 478, S1: 246, S2: 101
Developing health information system
2001, a study on existing health information system was completed 2004, a prototype for an integrated health information system (IHIS) was completed 2006, IHIS manual was completed 2005-2007, piloting and expansion of IHIS implementation 2007, procurement of hardware for health centers
2002, an HIS master plan was developed 2003, software development and partial hardware procurement

28
Upgrading the regulatory framework
2001, a study on existing licensing and accreditation system was completed 2002, a model of a new licensing and accreditation system was developed, competence standards for midwives, nurses and doctors were developed 2003, concept for an independent Quality Council (BMPK) was developed 2004, Governor decree for the establishment of the BMPK 2006, procedures for competence testing, standards for accreditation of primary health care facilities, competence standards for dentists, pharmacists and sanitarians were completed 2006, BMPK website, badanmutu.or.id 2006-2007, BMPK conducted competence testing for licensing, and facility survey for accreditation 2007, ISO 9001:2000 certification for BMPK
2003, a study on existing licensing and accreditation system was completed 2004, comparative study to Yogyakarta
Strengthening public accountability
2001, a public accountability model was developed 2002, a health policy accountability unit (UPKK), a civil society communication forum, a health newsletter, and a community hotline service were established
2003, a study for developing a public accountability model for transparency in financing was completed 2004-2007, use of suggestion box in health centers
A.2: Mobilizing Resources
Developing new funding mechanism
2001, a study for a health insurance model (Jamkesos) was completed 2003-2004, implementation trial of Jamkesos only for the poor 2004, establishment of Bapel Jamkesos (Managed Care organization) and Board of Trustees 2005-2007, integration of the Askeskin program with Jamkesos 2006-2007, piloting the family doctor scheme under the Jamkesos program 2006, insurance coverage was 42% (SUSENAS) 2007, draft Governor regulation to legalize the status of Jamkesos as a prerequisite for premium collection from non-poor population
2002, a feasibility study on JPKM (health insurance model) was completed 2004, sporadic implementation of “managed care” type approach in some districts 2006, insurance coverage was 22.6% (SUSENAS)

29
Central Components B.1: Managing Decentralization
2002, Pilot implementation of the Family Doctor concept in Jakarta, adopted later by Yogyakarta, West Sumatera and East Kalimantan Provinces 2002, 2004, 2005, Journalist writing competition to increase awareness on health issues 2003, Formulation of Minimum Service Standards for services at the District level
B.2: Resource Mobilization
2002-2003, 11 from 60 district proposals were financed through the Matching Grants program 2004-2006, all project districts were trained in developing District Health Accounts
Converting to self sufficiency
2007, all 5 district hospitals are swadana, and 3 of the 5 districts have at least 1 puskesmas swadana (all are swadana in Slemen District), but overall the percentage is less than 40 percent.
2001, a feasibility study for swadana facilities and a training needs assessment for swadana were conducted 2002-2003, a pilot study for swadana health center in North Lampung, Tanggamus, and Bandar Lampung was conducted 2002, Metro hospital became a swadana hospital 2003, Lampung Selatan hospital became a swadana hospital 2007, 2 of 10 district hospitals are swadana, and only 3 districts have at least 1 puskesmas swadana
A.3: Improving Health Service Access and Quality
Intensifying health promotion
2002, Yogyakarta Health Promotion Board was established (BKPK) through a Governor Decree 2003, 47 health promotion from NGOs were received and 5 were financed 2004, the functions of BKPK was transferred to the health promotion division of the provincial health office
N/A
A.4: Grants 2002-2007: 6 rounds of district
grants were implemented 2002-2007: 6 rounds of district grants were implemented

30
Annex 3. Economic and Financial Analysis Not Applicable

31
Annex 4. Bank Lending and Implementation Support/Supervision Processes
(a) Task Team Members
Names Title Unit Responsibility/ Specialty
Lending Samuel S. Liberman Lead Economist EASHD Anthony Toft Chief Counsel LEGES Puti Marzoeki Senior Health Specialist EASHD William Hardi Consultant EAPCO Yogana Prasta Operation Adviser EACIF Naseer Ahmad Rana Adviser SARSQ Novira Kusdarti Asra Financial Management Specialist EAPCO Benedicta R. Sembodo Program Assistant EACIF
Supervision/ICR Puti Marzoeki Senior Health Specialist EASHD Novira Kusdarti Asra Financial Management Specialist EAPCO Jed Friedman Economist DECRG William Hardi Consultant EAPCO Pandu Harimurti Health Specialist EASHD Adrian Hayes Consultant EASHD Peter F. Heywood Consultant EASHD Edhie Santosa Rahmat Consultant EASHD Claudia Rokx Lead Health Specialist EASHD Imad Saleh Lead Procurement Specialist EAPCO Agus Sasmito Consultant EASHD Anita Kentjanawati Tuwo Procurement Specialist EAPCO Benedicta R. Sembodo Program Assistant EACIF Ryma F.J. Aguw Team Assistant EACIF
(b) Staff Time and Cost Staff Time and Cost (Bank Budget Only)
Stage of Project Cycle No. of staff weeks USD Thousands (including
travel and consultant costs)Lending
FY97 7.80 FY98 33.64 FY99 93.58 FY00 57 102.48 FY01 0.00 FY02 0.09 FY03 0.00
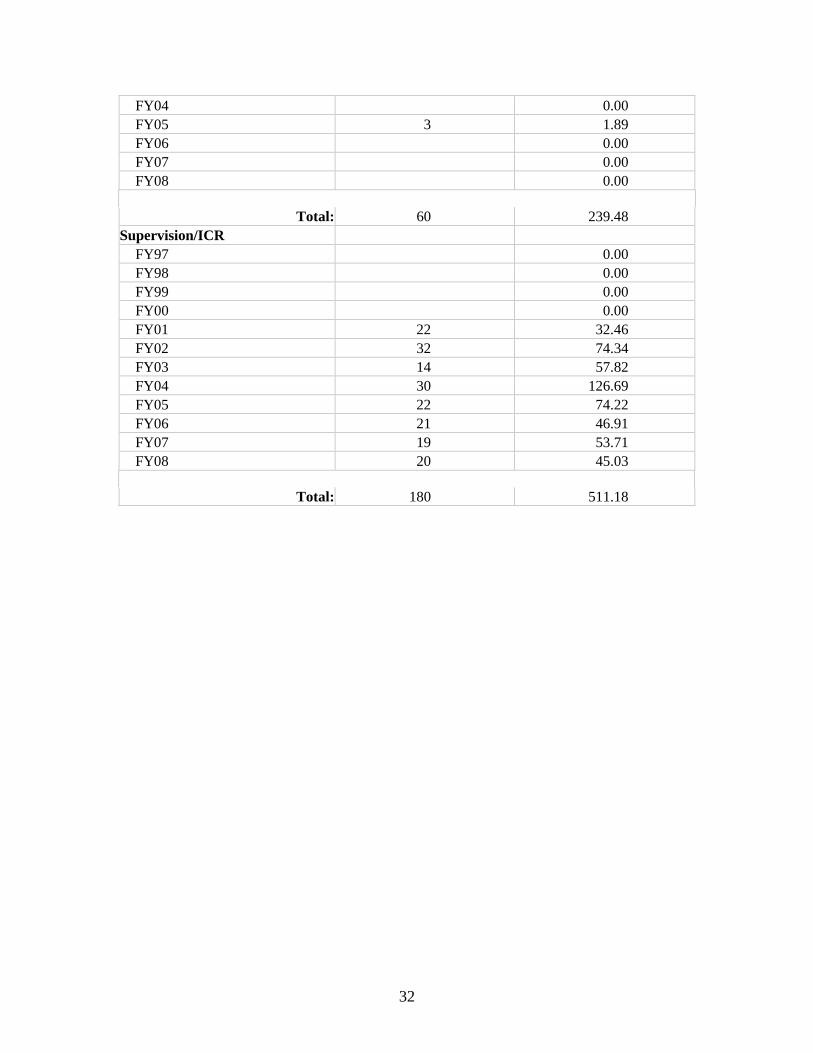
32
FY04 0.00 FY05 3 1.89 FY06 0.00 FY07 0.00 FY08 0.00
Total: 60 239.48
Supervision/ICR FY97 0.00 FY98 0.00 FY99 0.00 FY00 0.00 FY01 22 32.46 FY02 32 74.34 FY03 14 57.82 FY04 30 126.69 FY05 22 74.22 FY06 21 46.91 FY07 19 53.71 FY08 20 45.03
Total: 180 511.18

33
Annex 5. Beneficiary Survey Results Not conducted

34
Annex 6. Stakeholder Workshop Report and Results Not Conducted

35
Annex 7. Summary of Borrower's ICR and/or Comments on Draft ICR A. Comments on Draft ICR Despite unsatisfactory rating for the central level, there was positive performance/outcome of the central level as follows: 1. Well perfoming PDK (Pendamping Desentralisasi Kesehatan) from the
Decentralization Unit in assisting the regions in collaboration with the TRT so that districts were able to develop better/logical district proposals
2. MOH and University of Indonesia has conducted training on Integrated Health Planning and Budgeting and therefore districts were able to develop better health proposal compared to proposals from the first and second years of the project
3. MOH and University of Indonesia has conducted training on District Health Account so that districts were able to develop accurate DHA and health expenditures. This was used by the regions as an advocacy tool to negotiate budget allocation with district executive and legislative
4. Center of Health Data, MOH (Pusdatin) has conducted training of geographical Information System (GIS) to develop skills in preparing graphs and charts to make reports more communicative to the readers
B. Summary of Borrower’s ICR
I. General 1. Provincial Health Project I (PHP I) is a project that has a strong relationship with
decentralization. PHP I was launched at the same time with the enactment of Law 22/1999 regarding “local government”. PHP I started at August 2000 and finished at 30 June 2006. However PHP I was extended until 31 December 2007. PHP I is implemented at: Provinces Lampung and Yogyakarta, and Central. Generally activities implemented in PHP I are “Health Sector Reform” activities in all aspects. In following up changes due to the emerging of the new laws, a lot of preparations should be done, among others: institutions, human resource and other resources, and supporting regulations. Usually the above changes are beyond the capacity of the Ministry of Health. This means that we should prepare to overcome potential problems that may appear.
2. At the beginning of the implementation of decentralization, districts and cities felt free from the province, however the are not ready to receive the responsibilities, so that the provinces are difficult to coordinate, and even difficult to conduct supervision for providing guidance. In reality human resource in the districts/ cities were still weak and require “capacity building” by the province and central.

36
3. Data and information were extremely required by the districts/cities for developing health planning and proposals, however reporting system does not work as the expectations of the Ministry of Health. Ministry of Health and the World Bank overcome this problem by developing District/City Health Indicators based on the “Healthy Indonesia 2010” indicators, which was further used to develop proposals and monitor Districts/Cities.
II. Project Design 1. PHP I is a project developed to change a health system, from a centralistic character
to a decentralistic one. For this change, innovative activities were required in relation with capacity building, planning and health expenditure, improving accessibility and quality of health service delivery, etc. This change needs to be supported by a consistent central policy, which do not often change, including the human resources (tour of duty, tour of area, etc.).
2. A five-year period is too short to realize this relatively big system change. We consider the Performance Indicators as too ambitious and difficult to be achieved. Proxy-indicators would be better. Besides that, several indicators related to human resource were impossible to be achieved by the region because it was related to “human resource law” as an umbrella law for civil servants.
3. PHP I consists of two phases, Preparation phase and Operational phase. Preparation phase is considered necessary. The 17 months period (August 2000 – December 2001) of preparation phase was considered not enough to yield outputs as planned. In the PAD, at the Preparation phase, Task Forces should come up with outputs as planned. However the outputs are developed at the Operational phase, simultaneously with the implementation.
4. PHP I started at 1 August 2000 and closing date at 30 June 2006. The extension
request from the Ministry of Health was approved by Bappenas and the Ministry of Finance, the World Bank agree to extend PHP I for 1½ year (1 July 2006 – 31 December 2007). It means closing date of PHP I was 31 December 2007. The extension of PHP I is very useful for Lampung Province, because within the extension period, many nurses and midwives have been trained for topics such as: APN (Normal Delivery Care), PONED (Basic Emergency Obstetric and Neonatology Care), PONEK (Comprehensive Emergency Obstetric and Neonatology Care), Management of Asphyxia, etc. We are sure that these trainings are very useful for improving quality of health service and later, will be followed by the reduction of IMR/MMR. The same goes for Yogyakarta Province, it has successfully implementing Social and Health Security (Jamkessos), Regulation, Integrated Health Information System Development, all of these are very useful.
5. Implementation of District Grant (DG) is an innovative capacity building in the “comprehensive health planning and budgeting”. Districts and cities develop Plans of Action tailored to their needs in the form of proposals, complete with budget and its
37
source. Districts and cities develop a Master Plan (a five-year period plan) and a one-year plan based on their Master Plan. This proves to enhance personnel’s ability to develop a comprehensive health plan for their districts / cities.
6. The objective of establishing Joint Health Council (JHC) at the province is for dealing with health issues and development of health policies in the region. We assume that JHC’s members who are consisted of Bupati/Major, Professional organization, NGOs, cannot function well as it is hoped. JHC only provides proposal approval submitted by the District/Cities.
7. The objective of establishing Technical Review Team (TRT) at the province level is for assisting District/Cities in proposal development and reviewing it. TRT is considered successful in conducting its role, even though at the beginning there are rejections from the Districts/Cities with various reasons such as: inability to keep company, guidance for proposal development was not clear. However as time goes on, the role of TRT was well-accepted by the Districts/Cities. There was a significant capacity improvement of district’s planners.
III. Project Components. There are five components at provincial and three at central level. Those components are important to support health sector reform which was really required in the decentralization era (Organization, planning, health information, health financing, regulation, public accountability reforms, etc.). One among the components at central level is Matching Grant (MG), which many districts interested. However since the procedure and mechanism are complicated and lengthy, MG activity was discontinued. MG was only implemented for a period of two years. As an example the timing of proposal approval and implementation was not synchron due to delay of budget, delay of contract with the regions receiving MG.
IV. Output of Project Component a. Output at Province / District / City
Decentralization is executed based on Law 22 / 1999, which was then revised to Law 32 / 2004. For the implementer, Decentralization is a new issue. This is even more if it is linked to Health Sector Reform.
- Yogyakarta province has better quality of human resources as compared to
Lampung. Yogyakarta has the Gajahmada University with its professionals qualified in the aspect of decentralization. They assist Provincial/district/city health offices in the development of decentralization concepts. Yogyakarta has, therefore, outstanding Task Force performance/outputs.

38
- Lampung province: The addition of new districts during the decentralization period has a great impact on the overall quality of human resources. At Lampung, there are no Universities, with qualified experts in health decentralization which could assist, insufficient coordination within the Dinkes, the merger of Kanwil and Dinkes, followed with the addition of new districts and less-qualified human resources, all influenced the process of project implementation. As a consequence health sector reforms in Lampung are less, as compared to Yogyakarta Province.
- The benefit of regions implementing PHP I among others: Province and Districts
could develop innovative activities such as: trials/piloting/model until implementation which could not be financed from APBD or APBN. Innovative activities are very important in supporting motivation and capacity of human resource at the regions.
- Besides developing comprehensive district planning, the regional personnel can also develop reports and monitoring of District indicators, including data analysis, various data presentation from the simple one to GIS (Geographic Information System). The important thing is: region understand the benefit of data and information as a tool for advocating the local government and the legislative body.
b. Output at Central level
Organization change from “Ministry of Health and Social Welfare” to “Ministry of Health” brought forth mutation of personnel several times, interfering Task Force’s performance. Central’s prominent output is the development of the “Minimal Services Standard” which during the project has been revised twice. The conduction of the Family Doctor trial was used by Yogyakarta as reference, for the development of Jamkessos (Social and Health Security)
. c. Project Sustainability and Key Lessons Learned
- To increase involvement and sense of belonging of the local government (To gain
budget allocation) as well as the central MOH, PHP I collaborating with “Center for Management of Health Service” (PMPK), Gajahmada University, organized a seminar, two months prior the finish of PHP I, discussing activities considered as “Best Practices”.
- There should be a continuous advocative approach toward the local government including the local parliament in order to assure political commitment, so that implementation budget will be there.
- After the project ends, to maintain technical competence of the districts and
provinces, Ministry of Health must continue to provide technical assistance.
39
V. Project Management The establishment of Project Secretariat at the Central level, Province and all Districts/Cities was very helpful in the smoothness of project implementation: 1. In facilitating all project activities conducted by Technical Unit / Task Force at the
Ministry of Health, Provincial/District/City Health Offices.
2. In conducting project administration according to “loan agreement” such as: planning, procurement of goods/consultant, finance and monitoring project. Good coordination and cooperation in the project secretariat is very helpful in the smoothness of the project.
3. In managing inter-sectoral financing administration such as with the Ministry of Finance for replenishment and reimbursement of the budget.
VI. Comments on the World Bank a. Procurement 1. Several rules in the “Procurement Guideline” are contradictory with the Presidential
Decree (Keppres) causing confusement during the implementation, to the implementers as well as the auditor themselves.
2. The project is obliged to develop a “Procurement Plan” yearly, which must be
approved by the Bank. The plan contains district’s need. The Procurement Plan is very useful as assessment tool for yearly needs and for the monitoring the procurement activities.
3. Yearly procurement activities are always late/out of schedule, due to:
- Procurement plan developments are behind schedule. - Procurement Committee members change every year. - Insufficient knowledge of the Committee regarding the Bank’s rules. - Development of TOR by the Technical Unit is also behind schedule. - The time needed by the Bank to issue the NOL.
4. Procurement of Computers to support the Health Information System is far too late in
procurement. Procurement was just implemented in 2007. This is because procurement may be done only after the performance indicators are approved by central.
5. Civil Works. Construction for the expansion of Public Hospital at Central Lampung
district, which was planned in 2002, was only conducted in 2006. This was because the Bank demanded a feasibility study to be done first, and approval from Directorate General of Medical Care and Directorate General of Community Health.

40
b. Project Management Report (PMR)
This is a comprehensive report, accommodating all project activities, including procurement, plan of the budget needed, current and cumulative financial status since the start of the project. It is a useful report. Information/ data are correct and accurate. However districts and provinces must continuously be guided and supported in this report making.
c. Audit
1. In line with the Loan Agreement, the project audit consists of:
- General Audit by BPKP, conducted each year: March – June, - Ex Post Review, each year conducted by different auditors, appointed by the
Bank: April – June, - Interim Audit, for district / cities twice yearly March and October. - Technical Audit, the Loan Agreement mention as twice yearly. The project
considers once a year to be sufficient: September – November. 2. The different audits, going through the same documents, executed at nearly the
same time / period, make it difficult for the implementers. 3. Very often they have different perception regarding the Bank’s regulation. The
guideline, a reference for the implementation of the project needs to be clear, free from possible mis/multiple perceptions by every component, especially the auditors.
d. Performance Indicator
1. Time target set in the Performance Indicator is too short, since changing the system (which is the goal of the project) cannot be achieved in such a short time. There should have been a preparation time for the regions, especially the manpower. Implementation time needs to be longer.
2. Other indicators not able to be fulfilled by the regions are those contradictory with the existing Law. For example: reducing number of personnel, early retirement, recruitment, etc.
e. Closing date
We suggest that the closing date of the next projects will not be at 31 December, but 30 June. The reason of this suggestion is because of: the project faces difficulties in conducting activities between closing date and closing account. The activities are among others: to finish up the administration: replenishment, reimbursement, writing final project report, follow up of audit/investigation report. These activities require certain budget. The budget is liquefied after DIPA issuance, and very often DIPA issuance is late.

41
VII. Comments on the Ministry of Finance Loan disbursement is very much depended upon budget withdrawal. In reality implementation is very often behind the schedule. This is due to:
1. Project implementation was behind schedule, due to error of DIPA software (mistake
was at the budget proportion of GOI). Software revision is required and this takes time.
2. The different perception with the KPKN / KPPN managers in Lampung and Yogyakarta in translating the Circular Letter from Directorate General of Budget regarding the implementation of District Grant, caused a delay in money withdrawal for Districts / Cities.
3. Transition of the new rule of “Unified Budget” system needs time.
4. The establishment of “travel efficiency budget” policy in the amount of 70 % on August 2007. At the beginning it also applied for “Foreign Loan and Grant” (PHLN). The budget efficiency policy was repealed at the early November 2007, and the dispensation to use the money was approved at the late November 2007.
VIII. Comments on the Ministry of Health. 1. There was no matching budget available at the beginning of the project.
2. The changes of project management line (which in the beginning under Secretariat
General) were moved to “main unit” (Directorate General of Community Health). This influenced budgeting mechanism (Changes of Working Unit/SATKER), and required a long time to settle.
3. Revision process must wait the Regional and Central DIPA compilation. It could not be processed separately.
4. Difficulties in recruiting “Working Unit Staff” and members for the Procurement Committee.
5. Project results, especially best practices, need to be well documented and disseminated so that other provinces can learn.
6. For the 7 years (84 months) working plan, in reality only implemented 54 months (64 %).

42
IX. Conclusion. 1. Decentralization in the autonomy era is not only delegation of authority or financial
distribution between central and region. Further more, how decentralization could improve services to the community. As a consequence many things should be anticipated, especially technical provider in the field.
2. In reality, the human resource in the provinces and districts are not yet prepared to implement the programs decentralized by the MOH, so that capacity building is required to achieve the development objectives of PHP I.
3. Managerial skill and good communication are very important to manage a project.
4. Project Extension (1 July 2006 – 31 December 2007), is very beneficial for the PHP I to achieve the objectives of activities, in Lampung Province and Yogyakarta
5. To obtain local government support after the project closing, political commitment is required through continuous policy dialogue.
6. After the project closes, the local governments are still required to further expand the technical support from MOH.

43
Annex 8. Comments of Cofinanciers and Other Partners/Stakeholders Not Available

44
Annex 9. List of Supporting Documents Project Appraisal Document Credit Agreement Implementation Supervision Reports (ISRs) Aide Memoires Project baseline, midterm, and final evaluation reports Tracking study reports
Puncak Jaya(5030 m)
Obi
Ceram
Buru
SULAWESISUMATERA
Bali
KALIMANTAN
Raba
Pematangsiantar
Sorong
Timika
FakfakAmahai
PaluJambi
Mataram
BandungSurabaya
Semarang
Palembang
Pekanbaru
Palangkaraya
Bandar Lampung
Serang
IRIAN JAYA(PAPUA)
19
21
22
26
29
20
23
25
24
2827
30
32
31
33
12
11
13
1415
8
67
3
54
2
1
16
17 18
10
9
PAPU
AN
EW G
UIN
EA
A U S T R A L I A
THAILAND
MYANMAR
19
21
22
26
29
20
23
25
24
2827
30
32
31
33
12
11
13
1415
8
67
3
54
2
1
16
17 18
10
9
Balikpapan
Parepare
Baubau
Tarakan
Raba
Ende
Waingapu
Pematangsiantar
Sorong
Merauke
Timika
FakfakAmahai
Palu
Ambon
Gorontalo
Jambi
Medan
Kupang
Padang
Manado
Mataram
Bandung
Kendari
Denpasar
Surabaya
Semarang
Bengkulu
Jayapura
Palembang
SamarindaPontianak
Pekanbaru
Yogyakarta
Banda Aceh
Bandjarmasin
PalangkarayaPangkalpinang
Makassar
Ternate
Bandar Lampung
Serang
Manokwari
Mamuju
Tanjungpinang
JAKARTA
PAPU
AN
EW G
UIN
EA
A U S T R A L I A
SINGAPORE
VIETNAM
THAILAND
MYANMAR
TIMOR-LESTE
BRUNEI
PHILIPPINES
MA L A Y
SI
A
CelebesSea
Java Sea BandaSea
Arafura Sea
SuluSea
PACIFIC OCEAN
I N D I A N O C E A N
IRIAN JAYA(PAPUA)
AruIs.
KaiIs.
TanimbarIs.
Halmahera
Biak
Yapen
Morotai
Misool
Waigeo
Peleng Obi
Muna
Ceram
Buru
SULAWESI Sula Is.
Timor
FloresAlor
WetarMoa
Babar
Sumba
SumbawaLombokJAWA
NatunaBesar
Belitung
Madura
SUMATERABangka
Lingga
Nias
Siberut
Enggano
Simeulue
TalaudIs.
Bali
KALIMANTAN
Men t a w
a i I s .
Puncak Jaya(5030 m)
0°
5°
5°
10°
10°
15°
0°
5°
10°
15°
15°
10°
95° 100° 105°
115° 120° 125°
95° 100° 105° 110° 115° 120° 125°
130° 135° 140°
135° 140°
INDONESIA
NANGGROE ACEH DARUSSALAMSUMATERA UTARARIAUSUMATERA BARATJAMBIBENGKULUSUMATERA SELATANLAMPUNGBANGKA-BELITUNGBANTEND.K.I. JAKARTA
123456789
1011
PROVINCES:
1213141516171819202122
JAWA BARATJAWA TENGAHD.I. YOGYAKARTAJAWA TIMURBALINUSA TENGGARA BARATNUSA TENGGARA TIMURRIAU KEPULAUANKALIMANTAN BARATKALIMANTAN TENGAHKALIMANTAN SELATAN
KALIMANTAN TIMURSULAWESI UTARAGORONTALOSULAWESI TENGAHSULAWESI BARATSULAWESI SELATANSULAWESI TENGGARAMALUKU UTARAMALUKUIRIAN JAYA BARATPAPUA (IRIAN JAYA)
2324252627282930313233
IBRD 36233
JUN
E 2008
INDONESIAFIRST PROVINCIALHEALTH PROJECT
PROJECT PROVINCES
SELECTED CITIES AND TOWNS
PROVINCE CAPITALS
NATIONAL CAPITAL
MAIN ROADS
RAILROADS
PROVINCE BOUNDARIES
INTERNATIONAL BOUNDARIES
This map was produced by the Map Design Unit of The World Bank. The boundaries, colors, denominations and any other information shown on this map do not imply, on the part of The World Bank Group, any judgment on the legal status of any territory, or any endorsement or acceptance of such boundaries.
0 200
0 100 200 300 400 Miles
400 Kilometers


















