DIVERTICULITIS Management Dilemmas. Diverticulitis Common in Western and industrialised societies ~...
59
DIVERTICULITIS DIVERTICULITIS Management Management Dilemmas Dilemmas
-
Upload
lee-crawford -
Category
Documents
-
view
224 -
download
0
Transcript of DIVERTICULITIS Management Dilemmas. Diverticulitis Common in Western and industrialised societies ~...

DIVERTICULITISDIVERTICULITIS
Management Management DilemmasDilemmas

DiverticulitisDiverticulitis Common in Western and industrialised societies
~ 300,000 hospitalisations yearly in the United States 1.5million days of inpatient care + 1.5million OPD visits
M≈F Increases with age,
~ 10% in adults < 40 years to 50 to 70% among those ≥80 years
80% of patients are ≥ 50 years Affects the sigmoid and descending colon in
>90% of patients ~20% of patients with diverticulosis will develop
diverticulitis over their lifetime

First to describe three stage proceduredefunction, resection, closure stoma
WJ Mayo & LB Wilson, SGO 1907
‘‘Appendicitis on the left side’Appendicitis on the left side’

AetiologyAetiology Exact cause is unknown Associations with diets low in
fibre and high in refined carbohydrates Low fibre – diminished stool
bulk – slower GI transit time and changes in colonic motility – elevated intraluminal pressures – herniations at areas of weakness
Other factors include physical inactivity, constipation, obesity, smoking, and treatment with NSAIDs

Hinchey ClassificationHinchey Classification Stage I: small, confined
pericolic or mesenteric abscesses
Stage II: pelvic/retroperitoneal abscess
Stage III: purulent peritonitis
Stage IV: faecal peritonitis
Mortality: <5% for Stage I+II, 13% for Stage III and 43% for Stage IV
with permission; Jacobs D. N Engl J Med 2007;357:2057-2066, Copyright© 2007 Massachusetts Medical Society, all rights preserved

Current GuidelinesCurrent Guidelines
ACPGBIACPGBI2011 - 2011 - ACPGBI Position Statement on
Elective Resection for DiverticulitisWGO
2007 – Diverticular Disease (used by NICE)ASCRS
2014 - Practice Parameters for Sigmoid Diverticulitis

InvestigationsInvestigations Diagnosis based solely on clinical findings will Diagnosis based solely on clinical findings will
be incorrect in 33% of casesbe incorrect in 33% of cases
CT abdomen with contrast is the investigation of CT abdomen with contrast is the investigation of choice (WGO,ASCRS,ACPGBI) (sensitivity 93-choice (WGO,ASCRS,ACPGBI) (sensitivity 93-97%; specificity 75-100%; level of evidence III; 97%; specificity 75-100%; level of evidence III; Grade A recommendation) Grade A recommendation)
Other modalities such as ultrasound scan, MRI Other modalities such as ultrasound scan, MRI or contrast enema can be performed if CT not or contrast enema can be performed if CT not availableavailable

Management of Acute Management of Acute DiverticulitisDiverticulitis
The debate continues........The debate continues........

““sigmoid colitis with an acute component in the presence of diverticulosis likely to represent sigmoid colitis with an acute component in the presence of diverticulosis likely to represent diverticulitis. No perforation or collection”diverticulitis. No perforation or collection”
Acute Uncomplicated DiverticulitisAcute Uncomplicated Diverticulitis
Admit or discharge home.....??Admit or discharge home.....??Recommendations:
OPD management of uncomplicated diverticulitis with 7-10 days PO antibiotics
Pt to be reviewed within 48-72 hoursResolution of acute diverticulitis in 85% ~1/3 will have a recurrent attack often
within one year

Antibiotic Therapy – Is IV Antibiotic Therapy – Is IV TherapyTherapy NeededNeeded??
RCT – 79 patients with acute, uncomplicated diverticulitis
41 patients received oral therapy, 38 received IV
Regimens included ciprofloxacin and metronidazole
Complete resolution of symptoms in both groups
No patient had to be converted to IV from the oral group

Antibiotic Therapy – Is IV Antibiotic Therapy – Is IV TherapyTherapy NeededNeeded??
RCT 132 pts – 66 pts received PO antibiotics, 66 pts received IV antibiotics (co-amoxiclav)
No statistical difference in treatment failure between the groups
*Biondo et al 2013 Ann Surg Outpatient Versus Hospitalization Management for Uncomplicated Diverticulitis

The Debate – How Long Is The Debate – How Long Is Really Needed?Really Needed?
Uncomplicated sigmoid diverticulitis (Hinchey 1)
Used ertapenem
123 patients assigned to treatment arms
After 4 days, treatment successful on clinical grounds in 98% After 7 days, treatment deemed successful in 98.2% of cases

The Controversy – Are Antibiotics The Controversy – Are Antibiotics Really Needed At All?Really Needed At All?
All major guidelines recommend antibiotic treatment however......

Prospective, multicentre, randomised trial in Sweden and Iceland between 2003 and 2010
623 patients were enrolled 309 no antibiotics, 314 antibiotics
1 year follow-up No significant difference in complication rates, length
of hospital stay or readmission rates*Chabok et al 2012 BJS Randomized clinical trial of antibiotics in acute uncomplicated diverticulitis
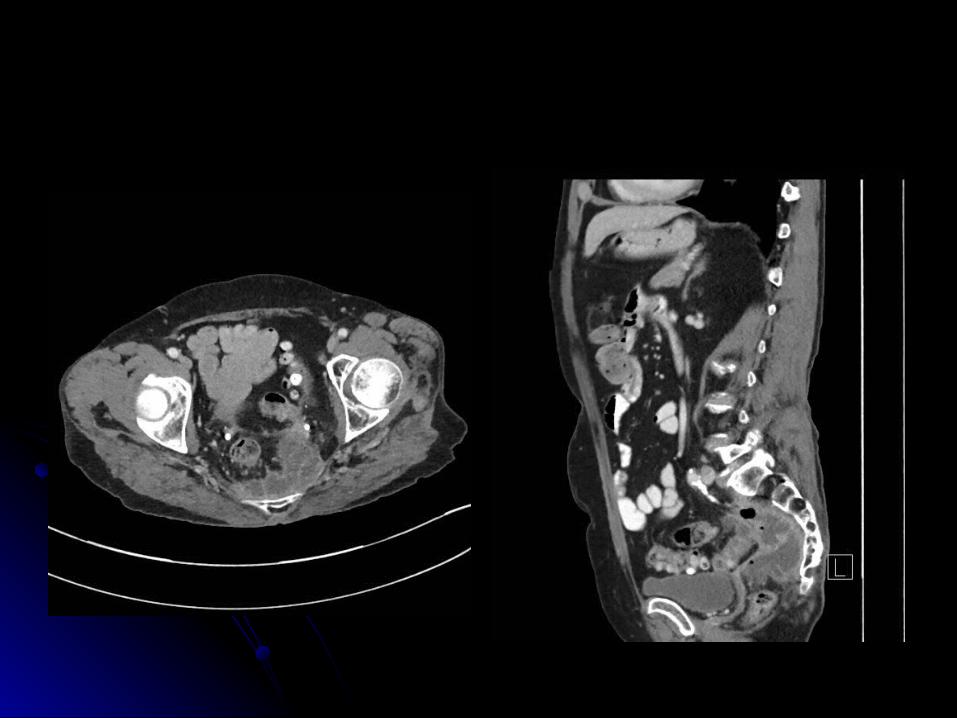
Diverticular AbscessDiverticular Abscess Radiologically guided percutaneous drainage is usually
the most appropriate treatment for patients with a large diverticular abscess (ASCRS, level of evidence: III; Grade B recommendation)
~15% of patients with acute diverticulitis will develop a pericolonic or intramesenteric abscess Hospitalisation and IV antibiotics are indicated
Abscesses <2 cm in diameter may resolve without further intervention (some say <4cm)
Larger abscesses are candidates for percutaneous catheter drainage; the majority of patients can avoid an emergency operation by using this intervention
136 pts 19: localised free air, 45: abscess <4 cm/distant free air <2 cm,
66 abscess >4 cm/distant free air >2 cm, 6: distant free air + free fluid
38 patients (28%) percutaneous abscess drains 5 patients (3.7%) urgent surgery on admission 7 (5%) urgent surgery for failed non-operative management Overall success rate of non-operative management: 91% 25/27 (92.5%) patients with free air remote from the perforation
site were successfully treated non-operatively
*Dharmarajan et al 2011 DCR The Efficacy of Nonoperative Management of Acute Complicated Diverticulitis

To Scope or Not To Scope?To Scope or Not To Scope?
After resolution of an initial episode of acute diverticulitis, the colon should be adequately evaluated to confirm the diagnosis (ASCRS level of evidence: 1C; grade of recommendation: strong)
Investigation of the colonic lumen by endoscopic means or barium enema after the acute attack is mandatory (ACPGBI, Grade C)

Recent papers and meta-analysis question the Recent papers and meta-analysis question the need for colonoscopy; especially after need for colonoscopy; especially after uncomplicated diverticulitisuncomplicated diverticulitis
To Scope or Not To Scope?To Scope or Not To Scope?

458 patients – 249 (54%) underwent colonosocpy 458 patients – 249 (54%) underwent colonosocpy within 1 yearwithin 1 year
77 (31%) polyps, 19 (7.6%) advanced adenomas, 4 (1.6%) 77 (31%) polyps, 19 (7.6%) advanced adenomas, 4 (1.6%) invasive malignancy = 23 (9.2%) had clinically significant invasive malignancy = 23 (9.2%) had clinically significant neoplasianeoplasia
Patients with complicated diverticulitis had higher incidence Patients with complicated diverticulitis had higher incidence of adenoma (p=0.001) and invasive malignancy (p=0.007) of adenoma (p=0.001) and invasive malignancy (p=0.007) than uncomplicated diverticulitisthan uncomplicated diverticulitis
Incidence of significant neoplasia in uncomplicated Incidence of significant neoplasia in uncomplicated diverticulitis was similar to average risk patientdiverticulitis was similar to average risk patient

292 patients – 205 had colonic evaluation292 patients – 205 had colonic evaluation50 (24.4%) polyps; 20 (9.8%) hyperplastic polyps; 50 (24.4%) polyps; 20 (9.8%) hyperplastic polyps;
19 (9.3%) adenomas; 11 (5.4%) colonic neoplasia 19 (9.3%) adenomas; 11 (5.4%) colonic neoplasia (10 advanced adenomas and 1 CRC); 1 pt had (10 advanced adenomas and 1 CRC); 1 pt had IBDIBD
The yield of advanced colonic neoplasia was The yield of advanced colonic neoplasia was equivalent to that detected in screening ptsequivalent to that detected in screening pts

11 studies from 7 countries included Risk of malignancy pooled proportional risk 1.6% (CI 0.9-
2.8%) (22/1970 pts) 1497 uncomplicated diverticulitis PPR 0.7% (CI 0.3-1.4%) 79 complicated diverticulitis PPR 10.8% (CI 5.2-21%)
Risk of malignancy low in uncomplicated diverticulitis but significant risk in those with complicated diverticulitis

Surgical InterventionSurgical Intervention
<10% of patients admitted with acute diverticulitis require <10% of patients admitted with acute diverticulitis require surgical treatment during the same admissionsurgical treatment during the same admission
Indications include:Indications include: generalised peritonitis, uncontrolled sepsis, uncontained visceral generalised peritonitis, uncontrolled sepsis, uncontained visceral
perforation, the presence of a large, undrainable abscess and perforation, the presence of a large, undrainable abscess and lack of improvement or deterioration within 3 days of medical lack of improvement or deterioration within 3 days of medical managementmanagement
characteristic of Hinchey stage III or IV disease.characteristic of Hinchey stage III or IV disease.
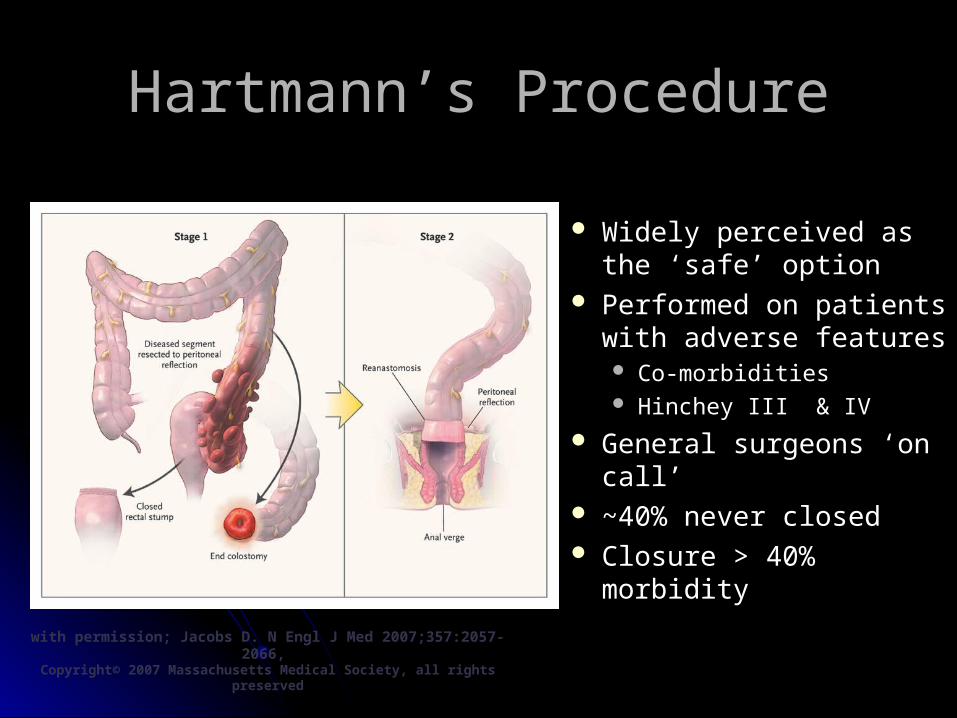
Widely perceived as the ‘safe’ option
Performed on patients with adverse features Co-morbidities Hinchey III & IV
General surgeons ‘on call’
~40% never closed Closure > 40% morbidity
with permission; Jacobs D. N Engl J Med 2007;357:2057-2066, Copyright© 2007 Massachusetts Medical Society, all rights preserved
Aydin et al, Dis Colon Rectum, 2005
Hartmann’s ProcedureHartmann’s Procedure

Experienced surgeon Stable patient, less
contamination + defunctioning stoma + intra-operative bowel
lavage
with permission; Jacobs D. N Engl J Med 2007;357:2057-2066, Copyright© 2007 Massachusetts Medical Society, all rights preserved
Primary Resection and Primary Resection and AnastomosisAnastomosis
62 pts (Hinchey III + IV) – 30 Hartmanns (HP), 32 Primary anastomosis + ileostomy (PA)
Overall complication rates comparable (80% vs 84%) Similar morbidity and mortality rates Secondary endpoints significantly different:
Stoma reversal rate 90% vs 57%, Grade IIIb-IV complications 0% vs 20%, operating time 73mins vs 183 mins, LOS 6 days vs 9 days and lower in hospital costs all favoured PA group
Hinchey IIIHinchey III
The Debate Continues.....

Am J Surg 1996, 171 432-434
8 patients over 37 months (1991-4) Mean age 57 (30-67) Generalised peritonitis – 1 had free air on
CXR (CT abdomen not readily available)
Laparoscopy Purulent peritonitis (Hinchey 3) Lavage & drainage
Outcome Mortality =0; Morbidity =2/8 Hospital stay = 10 days

Morbidity = 4%Mortality = 4%
Hospital stay = 8 days (7 -19)
8% conversion2% re-operation

DCR December 2014


The Final IssueThe Final Issue
Elective Resection
Indicated or Not?

Elective Resection - Elective Resection - 2006 ASCRS Guidelines2006 ASCRS Guidelines
Recommend elective resection after one episode of complicated diverticulitis treated non-operatively

Elective Resection - Elective Resection - 2014 ASCRS Guidelines2014 ASCRS Guidelines
‘The decision to recommend elective sigmoid colectomy after recovery from uncomplicated acute diverticultits should be indivualized. Grade of recommendation: Strong based on moderate-quality evidence, 1B’

Elective Resection - Elective Resection - 2011 ACPGBI Guidelines2011 ACPGBI Guidelines
“Majority of evidence for elective resection is... of poor quality”
“Decision on whether to resect should be made in conjunction with the radiologist, pathologist... and patient
themselves”

When To Operate?When To Operate? 210 patients underwent
laparoscopic resections for acute sigmoid diverticulitis
Group 1 were operated on early (5-8 days after admission)
Group 2 were operated on late (4-6 weeks or later)
10 conversions (9 in Group 1) 8 anastomotic leaks (all in
Group 1)
Concluded that delaying surgery significantly decreased post-operative morbidity
Many papers, both in support of Many papers, both in support of elective resection...elective resection...
BJS, 2005 – MEDLINE Literature review After one episode, one-third recur Of those, a further third have another episode

...and favouring more cautious ...and favouring more cautious elective resection elective resection
BJS, 2010 - Retrospective chart review of all (502) patients admitted with
diverticulitis between 1997 – 2002 18.8% will recur, 4.7% will have two or more episodes Recurrence usually occurred within 12 months of the initial
presentation, a pattern more consistent with failure of the index episode to settle
Subsequent elective surgery to prevent recurrence and the development of symptoms should be used judiciously

In summary, there are no guidelines that cover the treatment of every patient with diverticulitis –
treatment must be tailored to the individual patient

Case DiscussionsCase Discussions


Case 2Case 2
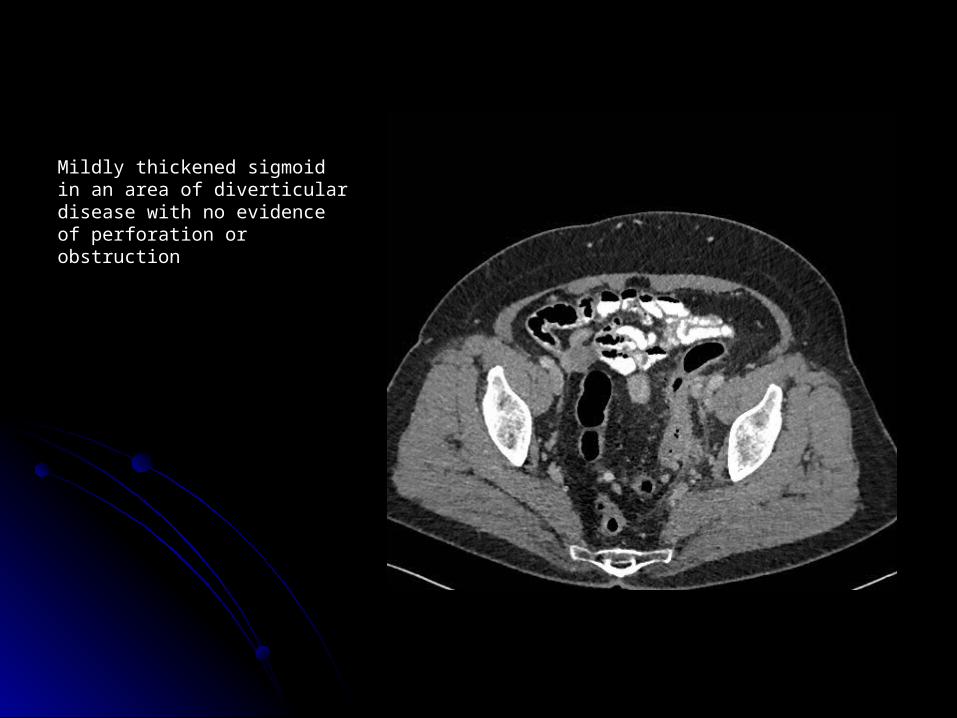
Mildly thickened sigmoid in an area Mildly thickened sigmoid in an area of diverticular disease with no of diverticular disease with no evidence of perforation or evidence of perforation or obstructionobstruction

What now?What now?
Diverticulitis with pericolic free gasDiverticulitis with pericolic free gas Small blebs free gas over liverSmall blebs free gas over liver

What next?What next?
SurgerySurgery
Laparoscopy and Lavage ?Laparoscopy and Lavage ?Resection? Resection?
Hartmanns?Hartmanns? Primary anastomosis?Primary anastomosis?
Defunction?Defunction?

2 months post Hartmann2 months post Hartmann
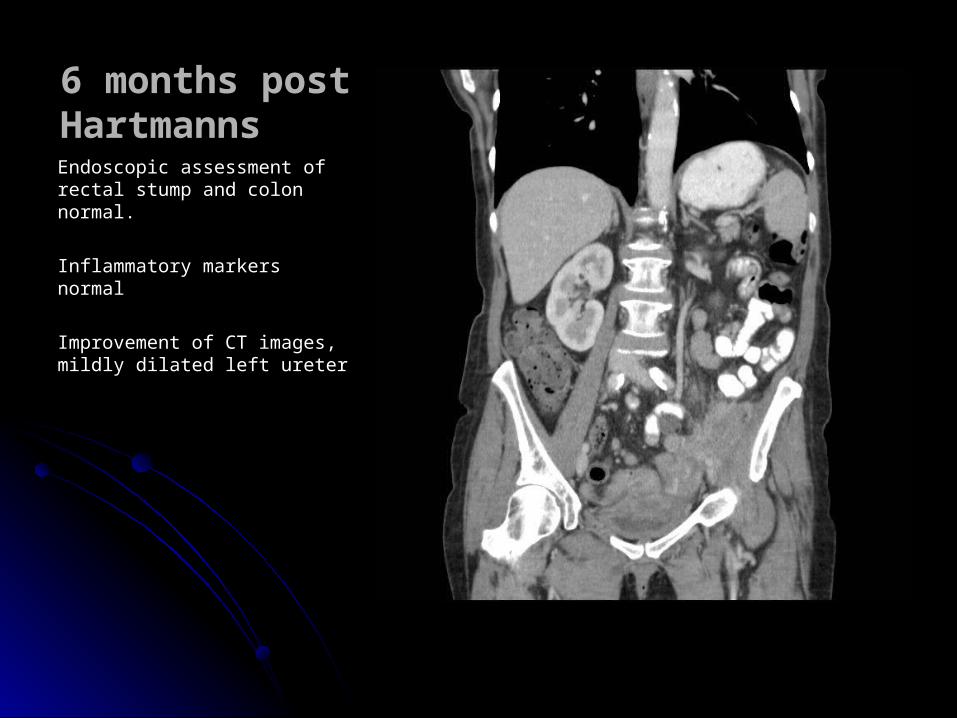
6 months post 6 months post HartmannsHartmanns
Endoscopic assessment of rectal Endoscopic assessment of rectal stump and colon normal.stump and colon normal.
Inflammatory markers normalInflammatory markers normal
Improvement of CT images, mildly Improvement of CT images, mildly dilated left ureterdilated left ureter

Case 3Case 3

66yo female, crampy abdominal pain, loose stool, Flexi sig to distal desc colon normal66yo female, crampy abdominal pain, loose stool, Flexi sig to distal desc colon normal
SurgerySurgery
Mass palpable in LIFMass palpable in LIF Midline laparotomyMidline laparotomy Multiple odematous loops sm. bowel adherent to Multiple odematous loops sm. bowel adherent to
sigmoid and dome of bladdersigmoid and dome of bladder Sharp dissection of sm. bowel loops to identify Sharp dissection of sm. bowel loops to identify
abscess cavity at dome of bladder with sigmoid abscess cavity at dome of bladder with sigmoid perforation which fed into itperforation which fed into it
““raggedy” sm. bowel, 2 serosal tears, 1 raggedy” sm. bowel, 2 serosal tears, 1 enterotomy proximal jejeunumenterotomy proximal jejeunum
Hartmanns procedureHartmanns procedure Oversew serosal tearsOversew serosal tears Repair enterotomyRepair enterotomy Robinson drain x 2 to pelvisRobinson drain x 2 to pelvis High jejeunostomyHigh jejeunostomy

Prolonged hospital stayProlonged hospital stayHickmann line, TPNHickmann line, TPNRestricted oral intakeRestricted oral intakeCystogram Cystogram
When to reverse jejeunostomy?When to reverse jejeunostomy?

Water soluble contrast examWater soluble contrast exam

• Started feed down distal limb of Started feed down distal limb of jejeunostomyjejeunostomy
• Continued TPNContinued TPN• No abdominal pain, no rise in inflammatory No abdominal pain, no rise in inflammatory
markersmarkers• Effluent came out end colostomyEffluent came out end colostomy
• What now?What now?

Case 4Case 4