The role of probiotics in helicobacter pylori infection - Helda
Upload
javed-yakoobCategory
view
212download
0
APMIS 108: 4 8 2 4 . 2000 Printed in Denmark . All rights reserved
Copyrigl i t 0 A P M I S 2000
lWKdU8 ISSN 0903-4641
Diversity of Helicobacter pylori among Chinese persons with H. pylori infection
JAVED YAKOOB,' GUO LING HU,' XUE GONG FAN,' HUI XIANG YANG,' SHUANG HU LIU,' DE MING TAN,' TIE GAN LI' and ZHENG ZHANG
'Department of Infectious Diseases and 2Gastroenterology, Xiangya Hospital, Hunan Medical University, Changsha, Hunan, F! R. China
Yakoob J, Hu GL, Fan XG, Yang HX, Liu SH, Tan DM, Li TG & Zhang Z. Diversity of Helicobacter pylori among Chinese persons with H. pylori infection. APMIS 2000; 108:482-6.
To determine whether there is diversity among clinical isolates of Helicobacter pylori in Chinese pa- tients with peptic ulcer disease, 40 strains of H. pylori were isolated from antral biopsy specimens obtained at the gastroenterology clinic of Xiangya Hospital from January 1996 to June 1998. Total protein profile by sodium dodecyl sulphate-polyacrylamide gel electrophoresis (SDS-PAGE) and DNA diversity by polymerase chain reaction-random amplified polymorphic DNA (PCR-RAPD) finger- printing were performed with these isolates. All the isolates from peptic ulcer disease were relatively homogeneous in protein profiles, but they showed a great DNA sequence diversity by PCR-RAPD fingerprinting. In Chinese patients H. pylori demonstrated an enormous diversity. The diversity among clinical isolates of H. pylori could be distinctly demonstrated and this observation will be helpful in the management of intrafamilial and recurrent H. pylori infection. PCR-RAPD finger- printing is an efficient method of distinguishing between clinical isolates of H. pylori.
Key words: H. pylori; Chinese persons; DNA diversity; PCR-RAPD fingerprinting.
J. Yakoob, Department of Infectious Diseases, Xiangya Hospital, Hunan Medical University, Chang- sha, Hunan, F! R. China. e-mail: [email protected]
Helicobacter pylori colonizes the human gastric mucosa and has been shown to be an etiological agent of gastritis and peptic ulcer disease (1-2). It is a major risk factor for the development of gastric cancer and primary B-cell gastric lymphoma ( 3 4 ) . The critical period for deter- mining the eventual overall prevalence of H. py l - ori infection is the early years of life (5 ) . A num- ber of virulence factors, including hemagglutin- ins, flagella, cytotoxins and urease, enable the survival of the organism in the gastric mucosa. H. py lor i produces a highly active urease that both catalyzes the hydrolysis of urea and elicits an immune response (6). The species is so di- verse that distinctly different genetic strains are
Received September 23, 1999. Accepted March 1, 2000.
generally recovered from each patient. This gen- etic diversity might explain the different mani- festations of H. pylori infection, varying from asymptomatic carrier to peptic ulcer disease and risk of gastric malignancies. For this reason it is essential to determine the factors which cause one strain to be an asymptomatic carrier and another the cause of clinical manifestations. There is still a greater diversity among H . py lor i strains with respect to many traits, including drug resistance, adherence specificity and cyto- toxin production. The diversity among H. pylor i strains has been well documented in Western countries by various typing methods, including restriction digests of genomic DNA (7-8), ri- botyping (9), protein profiling (lo), random amplified polymorphic DNA (RAPD) analysis (1 1 ) and polymerase chain reaction-restriction
482

DIVERSITY OF H. PYLORI AMONG CHINESE PERSONS
fragment length polymorphism analysis (PCR- RFLP)(12). Among these, we used SDS-PAGE for protein profiling and RAPD fingerprinting for differentiating clinical isolates of H. pylori. In clinical practice, bacterial typing systems are applied primarily to address one basic issue - whether two isolates are identical or not. This issue arises in patient management, epidemio- logical investigations and studies of the patho- genesis of bacterial infections. The present study was designed to show diversity among clinical isolates of H. pylori from a symptomatic Chinese population
MATERIALS AND METHODS
H. pylori strains Standard strain ATCC 49503 and 40 strains of H.
pylori, all clinical isolates from patients attending the gastroenterology department of Xiangya Hospital, Hunan Medical University, Changsha, Hunan, China, were used. The patients had undergone endo- scopy for symptoms in the upper gastrointestinal tract from January 1996 to June 1998 (mean age was 26.4 years; ma1e:female ratio 7:3; Table 1). All were diagnosed as having peptic ulcer disease, with super- ficial gastritis (SG) in 22 cases, duodenal ulcer (DU) in 10 cases, and gastric ulcer (GU) in 8 cases. Clinical isolates of H. pylori were obtained by biopsy from patients at the time of endoscopy. Biopsy tissue was suspended in phosphate-buffered saline (PBS, pH 7.4) and immediately cultured on chocolate agar plates (Columbia agar base, Lab M, Oxoid Ltd., Bury, England) containing 7% sheep blood, ampho- tericin B 2 mg/ml, vancomycin 10 mg/ml and poly- myxin B sulphate 2.5 mg/ml for 3-5 days. Using the commercial gas-generator system (Yiwu company, Zhejiang, China) the plates were incubated at 37 "C under microaerobic conditions in oxygen (0,) 5%, carbon dioxide (CO,) lo%, nitrogen (N2) 85% with high humidity. After incubation for 3 days the plates were examined daily for growth (13). If no growth of
TABLE 1. Clinical details of the mtients studied 1. Total no. 2. Sex (M/F) 3. Age (years)
mean range
4. Endoscopic diagnosis: Superficial gastritis (SG) Gastric ulcer (GU) Duodenal ulcer (DU) CLO test positive (rapid urease test)
40 28/12 26.4
21-64
22 8
10
H. pylori was observed after incubation for 7 days, the plates were discarded. Small rounded colonies were picked and subcultured twice to obtain a pure culture. Gram's stain, urease and catalase tests were used to confirm the identification of H. pylori isolates and to exclude the possibility of contamination. H. pylori was stored at -80°C in brain-heart infusion broth (Oxoid Ltd., Bury, England) with sheep blood 7%.
SDS-PAGE for protein profile Bacterial cells were collected from culture plates
and washed with PBS. The pellet was resuspended in 5 pl of SDS-PAGE sample buffer containing 250 mM trichloroacetic-hydrochloric acid (Tris-C1, pH 6 4 , 500 mM dithiothreitol, 10% SDS (electrophoresis grade), 0.5% bromophenol blue, 50% glycerol, and the mixture was boiled for 3 min prior to electro- phoresis. Extracted proteins were electrophoresed in a 12.5% acrylamide resolving gel (14) with a 4% stacking gel and visualized with 0.1% Coomasie bril- liant blue R250. SDS-PAGE was performed at room temperature for 8 h at 50 v.
Extraction of genomic D N A The bacterial cells on chocolate agar plates were
washed twice with PBS then centrifuged at 3000Xg for 20 min. H. pylori DNA was extracted using a phe- nol/chloroform method similar to that previously de- scribed by Majewski & Goodwin (8). Briefly, the bac- terial pellet was resuspended in Tris-C1 buffer con- taining ethylenediaminetetraacetate (T.E pH 8.0) and lysozyme (30 mg/ml) and then incubated at 37°C for 30 min. The suspension was treated with SDS (lo%), proteinase K (2.5 mg/ml) and RNase A (40 mg/ml). DNA was extracted with phenol/chloroform/isoamyl alcohol, precipitated using sodium acetate and ice- cold absolute alcohol, and washed with ice-cold alco- hol (70%). The pellet of DNA was finally resus- pended in TE buffer. DNA content and purity was determined by measuring the absorbance at 260 nm and 280 nm using a spectrophotometer (Beckman DU-600, USA).
PCR-RAPD fingerprinting PCR was carried out in a final volume of 50 pl
containing 5-100 ng of H. pylori genomic DNA, 3 mM magnesium chloride, 100 pmol of each primer, 2.0 units of Taq DNA polymerase, 4 mM each of dCTP, dGTP, dTTP and dATP in double distilled water. The mixture was overlaid with mineral oil. All the reagents were bought from the Sino-American Biotechnology Company (SABC), Shanghai, China. The primers used were a combination of two 10-nu- cleotide primers, obtained from the Genosys Europe, Cambridge, England. These are random primers which are not taken from any part of the H. pylori genome. For our study we used primer 128l(AAC GCG CAA C) and primer 1254 (CCG CAG CCA
483

YAKOOB et al.
A), which have been successfully used before (1 1, 15). A thermal cycler (Perkin-Elmer 480, Cetus, USA) was used for amplification. The cycling programme was as follows: four cycles of (94"C, 5 min; 36"C, 5 min; 72"C, 5 min), 30 cycles of (94"C, 1 min; 36"C, 1 min; 72"C, 2 min) and then 72°C for 10 min. After PCR, 15 pl aliquots of product, were electrophoresed in 2% agarose gels containing 0.5 pg/ml ethidium bromide in the gel and 1 x Tris-acetate running buf- fer. PCR product of standard strain ATCC 49503 was used as a positive control and double distilled water as a negative control for electrophoresis. The PCR marker (SABC) was used as a size marker (M) in all gels.
RESULTS
S D S - P A G E f o r protein projile SDS-PAGE of bacterial cells did not show
any notable differences among isolates (Fig. 1, lanes 2-9). There were 20-25 bands for each iso- late with molecular weights between 14 kDa-120 kDa, as described before (15). There were six major characteristic bands of 14 kDa, 32 kDa, 36 kDa, 38 kDa, 40 kDa and 97 kDa present in the protein profiles of all the isolates (Fig. 1, lanes 2-9). There were minor changes among isolates in the expression of some protein con- stituents mainly above 97 kDa (Fig. 1, lanes 6- 9). In one isolate (Fig. 1, lane 2) the protein profile showed a minor variation in the smaller protein component molecular weight between 20 kDa-3 1 kDa. The protein patterns of isolates
1 2 3 4 5 MNcPcBB AB BB A.E
I
Fig. 2. Reproducibility of PCR-RAPD fingerprinting of clinical isolates of H. pylori. Identical strain-speci- fic unique band patterns were obtained in five strains with profiles A and B. (M) PCR marker, (Nc) nega- tive control, (Pc) positive control with PCR product of standard strain ATCC 49503. Lanes 1 A-B, 2 A- B, 3 A-B, 4 A-B, 5 A-B show five different clinical isolates RAPD fingerprinted one month apart.
MNcPcl 2 3 4 5 6 7 8 910
M I 2 3 4 5 6 7 8 9
97.4 kDa 66.2 kDa
43 kDa 31 kDa
20.1 kDa
14.4 kDa
Fig. 1. SDS-PAGE for protein profiles of H. pylori isolates from eight different patients, showing simi- larity in terms of number of major bands, but minor changes among isolates in the expression of some protein constituents mainly above 97.4 kDa. Lanes: Marker (M), Lane 1: standard strain ATCC 49503, Lanes 2-9: clinical isolates of H. pylori.
484
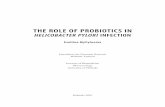
Fig. 3. PCR-RAPD fingerprinting of clinical isolates of H. pylori. The differences in profiles of strains show that a different strain was recovered from each biopsy specimen. (M) PCR marker, (Nc) negative control, (Pc) positive control with PCR product of standard strain ATCC 49503. Lanes 1-10: 10 clinical isolates of H. pylori.
were similar, but it was still possible to distin- guish between the profiles of the standard strain and each of the isolates. In our study, protein profiles differed in terms of total number of bands compared to in other studies (1 5-16), but gave similar results in terms of major bands and a similar profile from one strain to another.
Reproducibility of R A P D band patterns The reproducibility of RAPD fingerprint pat-
terns was tested using five different isolates. The

DIVERSITY OF H. PYLORI AMONG CHINESE PERSONS
isolates used were stored at -8OC for one month after primary examination. DNA prep- aration was made from separate cultures of each strain on separate days. Identical strain- specific unique band patterns were obtained (Fig. 2).
PCR-RAPD fingerprinting RAPD fingerprinting with a combination of
two 10- nucleotide primers yielded 4-8 bands on the agarose gels (Fig. 3 ) . The diversity of H. pyluri strains was exhibited by a unique band pattern in each of the clinical isolates.
Identijicatiun of specijic patterns fu r endoscopic diagnosis subgroups
We tried to identify specific RAPD finger- print patterns in three endoscopic diagnosis subgroups, i.e. gastritis, gastric ulcer and duo- denal ulcer. We were unable to attribute single or multiple patterns to a particular endoscopic diagnosis. The patterns were not affected by changes in template DNA levels between 5 ng- 100 ng per 50 pl reaction.
.
DISCUSSION
H. pylori is believed to be transmitted orally and the risk of infection increases with age and crowding (1 7-1 9). In developed countries, the presence of antibodies against H. pylori antigen increases from <20% in people aged 30 years to >50% in those aged 60 years (20), while in developing countries > 80% of the population are infected by the age of 20 (19). The preva- lence of H. pyluri in southern China was found to be 44% (9, higher than in developed coun- tries but lower than in some developing coun- tries (21-22). The People’s Republic of China which is inhabited by more than one-fifth of the world’s population, shows large regional vari- ations in the prevalence of gastric cancer, rang- ing from 6 to >40 cases/105 person (23).
Similar data exist from different parts of the world, but knowledge of such data originating in China is inadequate. Our study furthermore agrees with that of van der Ende et al. (24). It is important that symptomatic H. pylori infec- tion be completely eradicated because of the long-term risk of gastric malignancies. Com-
plete eradication of H. pyluri infection requires identification of patients colonized by one or more strains of H. pyluri, and in cases of recur- rent infection establishing whether recrud- escence or re-infection is the cause. Members of a family may harbor the same or different strains. The possibility of cross-infection within a family will be shown by isolating similar strains of H. pyluri in different members of the family. In our study we distinguished each of 40 independent isolates by protein profile and DNA-based PCR-RAPD fingerprinting. SDS- PAGE protein patterns have less discriminatory power compared with PCR-RAPD. The protein profiles were similar from one strain to another (Fig. 1, lanes: 1-9). This technique appears to be useful for defining the similarities between isolates. The diversity of H. pyluri isolate fingerprints by the RAPD method reflects its greater sensitivity. This method, which uses an oligonucleotide of an arbitrarily chosen se- quence to prime DNA synthesis from sites to which it is matched or partially matched, results in a strain-specific DNA band pattern (Fig. 3 , lanes: 1-10). This sensitivity is attributable to the sampling of the entire genome essentially at random. Each of the H. pyluri isolates with two primers exhibited 4-8 bands on agarose gel. The DNA bands in our results were fewer compared to Akopyanz et al. (1 1) and Xia et al. (1 5). This divergence could be explained by isolates coming from different geographical locations and experiments carried out with thermostable Taq DNA polymerase from a different supplier (SABC). The DNA band patterns from H. pyl- ori isolates obtained at initial and follow-up bi- opsy can be used to distinguish between recrud- escence and re-infection. They will distinguish between person-to-person spread and infection from a common environmental source. At fol- low-up endoscopy it would be appropriate to try to isolate H. pyluri from various sites in the stomach and duodenum to determine whether the relapses that frequently occur after appar- ently successful antibacterial treatment are due to recrudescence of the infection with the same strain or to re-infection with a new strain. We believe that the pre- and posttreatment isolates will demonstrate identical patterns, indicating recrudescence of surviving bacteria rather than re-infection with a new strain.
In conclusion, this study has demonstrated
485

YAKOOB et al.
that there is a marked diversity among clinical isolates of H. pylori in the Chinese population. The protein profiles of SDS-PAGE are similar, but PCR-RAPD fingerprinting has a discrimi- natory capacity.
REFERENCES
1. Fan XG, Kelleher D, Fan XJ, Xia HX, Keeling PWN. Helicobacter pylori increases proliferation of gastroepithelial cells. Gut 1996;38: 19-22.
2. Fan XG, Fan XJ, Xia HX, Keeling PWN, Kel- leher D. Up-regulation of CD44 and ICAM -1 expression on gastric epithelial cells by H. pylori. APMIS 1995; 103:7448.
3. Sipponen I? Gastric cancer: a long term conse- quence of H. pylori infection? Scand J Gastro- enterol 1994;29:2&7.
4. Genta RM, Hammer HW, Graham DY. Gastric lymphoid follicles in H. pylori infection: fre- quency, distribution and response to triple ther- apy. Hum Pathol 1993;24:577-83.
5. Mitchell HM, Li YY, Hu PJ et al. Epidemiology of H. pylori in southern China: identification of early childhood as the critical period for acqui- sition. J Infect Dis 1992; 166: 149-53.
6. Mobley HLT, Cortesia MJ, Rosenthal LE, Jones BD. Characterization of urease from Campylo- bacter pylori. J Clin Microbiol 1988;26:831-6.
7. Simor AE, Shames B, Drumm B, Sherman P, Low DE, Penner JL. Typing of Campylobacter pylori by bacterial DNA restriction endonuclease analysis and determination of plasmid profile. J Clin Microbiol 1990;28:83-6.
8. Majewski SIH, Goodwin CS. Restriction endo- nuclease analysis of the genome of Campylo- bacter pylori with a rapid extraction method: evi- dence for considerable genomic variation. J In- fect Dis 1988;157:465-71.
9. Tee W, Lambert J, Small R, Schembri M, Ross BC, Dwyer B. Ribotyping of H. pylori from clin- ical specimens. J Clin Microbiol 1992;20:5137- 42.
10. Covacci A, Censini S, Bugnoli M, et al. Molecu- lar characterization of the 128-kDa immunodo- minant antigen of Helicobacter pylori associated with cytotoxicity and duodenal ulcer. Proc Natl Acad Sci USA 1990;90:5791-5.
11. Akopyanz N, Bukanov NO, Westblom TU, Kre- sovich S, Berg DE. DNA diversity among clinical
isolates of H. pylori detected by PCR-based RAPD fingerprinting. Nucleic Acids Res 1992; 20513742.
12. Akopyanz N, Bukanov NO, Westblom TU, Berg DE. PCR-based RFLP analysis of DNA se- quence diversity in the gastric pathogen H. pyl- ori. Nucleic Acids Res 1992;20:6221-5.
13. Fan XG, Li TG. Growth of Helicobacter pylori in candle jar. J Med Microbiol 1997;46:3545.
14. Sambrook J, Fritisch EF, Maniatis T. Molecular cloning: A Laboratory Manual. 2nd ed. Cold Spring Harbor Laboratory Press, Cold Spring Harbor. 1989:1847-55.
15. Xia HX, Windle HJ, Marshall DG, Smyth CJ, Keane CT, O’Morain CA. Recrudescence of H. pylori after apparently successful eradication: novel application of randomly amplified poly- morphic DNA fingerprinting. Gut 1995;37:304.
16. Megraud F, Bonnet F, Garnier M, Lamouliatte H. Characterization of Campylobacter pyloridis by culture, enzymatic profile and protein content. J Clin Microbiol 1985;22: 1007-10.
17. Mendall MA, Northfield TC. Transmission of Helicobacter pylori infection. Gut 1995;37: 1-3.
18. Xia HX, Talley NJ. Natural acquisition and spontaneous elimination of Helicobacter pylori infection: clinical implications. Am J Gastro- enterol 1997;92:1780-7.
19. Graham DY, Adam E, Reddy GT, et al. Seroepi- demiology of H. pylori infection in India. Com- parison of developing and developed countries. Dig Dis Sci 1991;36:10848.
20. Jones DM, Eldridge J, Fox AJ, Sethi P, Whorwell PJ. Antibodies to the gastric Campylobacter-like organism (“Campylobacter pyloridis”) - clinical correlations and distribution in the normal population. J Med Microbiol 1986;22:57-62.
21. Perez-Perez GI, Taylor DN, Bodhidatta L, Wongsrichanalai J, Baze WB, Dunn BE, et al. Seroprevalence of H. pylori infections in Thai- land. J Infect Dis 1990;161:123741.
22. Megraud E Brassens-Rabbe MA, Denis F, Belbouri A, Hoa DQ. Seroepidemiology of Campylobacter pylori infection in various popu- lations. J Clin Microbiol 1989;27: 1870-3.
23. Armstrong B. The epidemiology of cancer in the People’s Republic of China. Int J Epidemiol
24. van der Ende A, Pan ZJ, Bart A, van der Hulst RW, Feller M, Xiao SD, et al. CagA-positive Hel- icobacter populations in China and the Nether- lands are distinct. Infect Immun 1998;
1980;9:305-15.
66: 1822-6.
486