Disease Surveillance System in Malaysia
13
The increasing significance of communicable diseases, especially emerging and reemerging infections is attracting greater attention, not only from the public health and medical communities but also the lay public. About 65% of the world’s first news about infectious disease events now comes from informal sources, including press reports and the internet which are now easily accessed by everyone.There is a need to improve surveillance systems in order to recognize emerging threats, both in the community and in hospitals & health facilities, and to respond to them in a timely manner. Surveillance, namely the continuous monitoring of diseases and health determinants in populations, has gained much attention over the past fifteen years. Surveillance can be defined as the ongoing, systematic collection, verification, analysis, and interpretation of data, and the dissemination of information regarding diseases and health events to those who need to know, for use in public health action to reduce morbidity and mortality and to improve health. Surveillance data so analysed and interpreted can provide public health officials and policy-makers with evidence-based information for decision making. Such reports also enable public health professionals to detect early signals of outbreaks and to take quick remedial measures to control them. If the surveillance data are not analysed, it is often difficult to detect warning signals on communicable disease outbreaks from raw surveillance data alone. The analysed data/information generated should not be filed away but to be used for timely actions. The impact of communicable diseases has grave implications for the social and economic well being of the peoples in every nation. Therefore, the Disease Control Division has planned and implemented a wide range of programmes and activities, nation-wide, to reduce the incidences of communicable diseases. Strengthening the surveillance of communicable diseases is one of more important strategies to keep them at bay. New surveillance systems were introduced to detect early communicable disease outbreaks, especially newly emerging & reemerging ones, & to respond rapidly to them. This will also help in monitoring them. The establishment of Communicable Disease Surveillance Section under the Disease Control Division is another step to strengthen coordination of communicable disease surveillance in our country. I hope the publication of this monthly Bulletin of Infectious Diseases will further strengthen dissemination of information and also sharing of information for those in the health & health related agencies in the country. DR. HJ. RAMLEE BIN RAHMAT Director, Disease Control Division Ministry of Health Malaysia Message From The Director Disease Control Division, Ministry of Health Malaysia 1 2 3 8 Announcement 11 12 Contents Message from Director Disease Control Division Ministry of Health Malaysia From the Desk of Chief Editor Articles : Surveillance System in Malaysia Developing Critical Appraisal Skill Disease Reports : Towards Measles Elimination AGE Outbreak, Tapah, Perak Surveillance Reports: Notification of Infectious Disease, May 2005 Report of Weekly Infectious Disease Notifications 1990 - 2004 Photo Gallery : Food for Thought: i) Heart - Anywhere & Anytime ii) Do We Know Our Roles FAO/WHO Consultation on AI & Human Health ; Risk Reduction Measure in Producing, Marketing & Living with Animals in Asia 4-6 July 2005 Renainsance Hotel, Kuala Lumpur Fifth Inter - Regional Training Course on Public Health and Emergency Management in Asia and the Pacific 4-15 July 2005 Bangkok, Thailand
-
Upload
azmi-mohd-tamil -
Category
Health & Medicine
-
view
6.170 -
download
10
Transcript of Disease Surveillance System in Malaysia

The increasing significance of communicable diseases, especially emerging and reemerging infections is attracting greater attention, not only from the public health and medical communities but also the lay public. About 65% of the world’s first news about infectious disease events now comes from informal sources, including press reports and the internet which are now easily accessed by everyone. There is a need to improve surveillance systems in order to recognize emerging threats, both in the community and in hospitals & health facilities, and to respond to them in a timely manner.
Surveillance, namely the continuous monitoring of diseases and health determinants in populations, has gained much attention over the past fifteen years. Surveillance can be defined as the ongoing, systematic collection, verification, analysis, and interpretation of data, and the dissemination of information regarding diseases and health events to those who need to know, for use in public health action to reduce morbidity and mortality and to improve health.
Surveillance data so analysed and interpreted can provide public health officials and policy-makers with evidence-based information for decision making. Such reports also enable public health professionals to detect early signals of outbreaks and to take quick remedial measures to control them. If the surveillance data are not analysed, it is often difficult to detect warning signals on communicable disease outbreaks from raw surveillance data alone. The analysed data/information generated should not be filed away but to be used for timely actions.
The impact of communicable diseases has grave implications for the social and economic well being of the peoples in every nation. Therefore, the Disease Control Division has planned and implemented a wide range of programmes and activities, nation-wide, to reduce the incidences of communicable diseases. Strengthening the surveillance of communicable diseases is one of more important strategies to keep them at bay. New surveillance systems were introduced to detect early communicable disease outbreaks, especially newly emerging & reemerging ones, & to respond rapidly to them. This will also help in monitoring them. The establishment of Communicable Disease Surveillance Section under the Disease Control Division is another step to strengthen coordination of communicable disease surveillance in our country.
I hope the publication of this monthly Bulletin of Infectious Diseases will further strengthen dissemination of information and also sharing of information for those in the health & health related agencies in the country.
DR. HJ. RAMLEE BIN RAHMATDirector,Disease Control DivisionMinistry of Health Malaysia
Message From The Director Disease Control Division, Ministry of Health Malaysia1
2
3
8
Announcement
11
12
Contents
Message from DirectorDisease Control Division
Ministry of Health Malaysia
From the Desk of Chief Editor
Articles :
Surveillance System in Malaysia
Developing Critical Appraisal Skill
Disease Reports :
Towards Measles Elimination
AGE Outbreak, Tapah, Perak
Surveillance Reports:
Notification of Infectious Disease, May 2005
Report of Weekly Infectious DiseaseNotifications 1990 - 2004
Photo Gallery :
Food for Thought:
i) Heart - Anywhere & Anytimeii) Do We Know Our Roles
FAO/WHO Consultation on AI & Human Health ; Risk Reduction Measure in Producing, Marketing
& Living with Animals in Asia4-6 July 2005
Renainsance Hotel, Kuala Lumpur
Fifth Inter - Regional Training Course on Public Health and Emergency Management
in Asia and the Pacific 4-15 July 2005
Bangkok, Thailand

LATAR BELAKANG Notifikasi penyakit berjangkit
kemungkinan telah dilaksanakan pada zaman jajahan British
dan dikuatkuasakan melalui beberapa ‘enactment’ atau
‘ordinance’ seperti ‘Quarantine and Prevention of Disesase
Enactment’ untuk negeri-negeri bersekutu, ‘Quarantine and
Prevention of Disease Ordinance 1939 untuk negeri Sabah dan
Sarawak dan ‘Quarantine and Prevention of Disease Enactment,
untuk negeri Kelantan, Johor, Terengganu, Kedah dan Perlis.
Kementerian Kesihatan telah mengkaji semula semua senarai
penyakit-penyakit berjangkit yang telah
dinotifikasi dan menggazetkan senarai
baru pada tahun 1971 di mana terdapat
36 jenis penyakit berjangkit yang perlu
dinotifikasikan. Pada tahun 1988, Akta
Pencegahan dan Pengawalan Penyakit
Berjangkit 1988 telah dikuatkuasakan.
Bilangan penyakit berjangkit yang
Sistem Survelandi
MalaysiaOleh
Cawangan Survelan Penyakit Berjangkit
perlu dinotifikasikan telah dikurangkan kepada 26 di
mana penyakit seperti antrax, meningococcal meningitis,
chickenpox, filariasis, leptospiral infections, mumps, opthalmia
neonatorum, puerperal septic abortion, trachoma dan yaws
telah dikeluarkan dari notifikasi penyakit berjangkit.
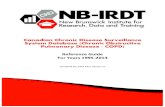
SISTEM SURVELAN PENYAKIT BERJANGKIT
Terdapat beberapa jenis sistem survelan untuk penyakit
berjangkit di Malaysia dan aliran data survelan dan maklumat
adalah seperti ditunjukkan pada rajah ‘1’ iaitu:-
• Sistem survelan mandatori notifikasi
• Sistem survelan berpandu makmal
• Sistem survelan berpandu klinikal
• Survelan penyakit berjangkit oleh lain-lain agensi
• Sistem survelan berpandu komuniti
Survelan BerpanduMakmal
Survelan MandatoriNotifikasi Penyakit
SurvelanBerpandu Klinikal(Sentinel/Sindromik Kebangsaan)
Survelan BerpanduKomuniti
Survelan Boleh lain-lainAgensi
Mikrobiologi Awam:Klinik Kesihatan
Hospital Swasta :
Klinik SwastaHospital
Sentinel Klinik PilihanSindromik Kebangsaan
(hospital) A&E/Wad/Klinik
Komuniti/ Media/Sumber
Antarabangsa
Jab. PerkhidmatanHaiwan (Penyakit
Zoonotik
FOMEMA Sdn. Bhd.
Pej. Kesihatan Daerah
IMR/KKM Kebangsaan : BahagianKawalan Penyakit, KKM
Pejabat KesihatanNegeri
Isolasi dan NotifikasiMikrooganisma
Keputusan
NotifikasiMikrooganisma
NotifikasiMikrooganisma
Sistem survelan mandatori notifikasi penyakit berjangkit
memerlukan notifikasi mandatori di bawah Akta Pencegahan
dan Pengawalan Penyakit Berjangkit 1988. Di jadual 1 dan 2
Akta tersebut, terdapat 26 penyakit berjangkit yang mesti
dinotifikasikan. Senarai penyakit yang perlu dinotifikasi
sentiasa disemak dari masa ke semasa. Di bawah sistem
sekarang, laporan penyakit berjangkit dibuat secara manual
dengan menggunakan borang notifikasi yang terdapat di
bawah Akta. Walaubagaimana, laporan secara elektronik yang
di panggil Sistem Maklumat Kawalan
Penyakit Berjangkit (CDCIS) telah pun
diimplmentasikan sejak tahun 2001.
Sistem survelan berpandu makmal
di mana pemantauan agen penyakit
berjangkit telah diperkenalkan
pada Ogos 2002. Sistem ini adalah
berkomplemen sistem survelan notifikasi mandatori penyakit
berjangkit. Di bawah sistem ini, ia melibatkan laporan
mikroorganisma yang diisolasi oleh semua makmal awam
atau swasta di Malaysia kepada pihak berkuasa kesihatan
yang relevan. Sekarang ini, terdapat 6 jenis bakteria iaitu V.
cholerae, H. influenzae B, Salmonella spp., S.typhi/paratyhpi, N.
meningitides dan Leptospira telah dipilih untuk dipantau oleh
makmal-makmal mikrobiologi yang telah ditentukan di bawah
Kementerian Kesihatan Malaysia.
Sistem survelan berpandu klinikal dihadkan untuk penyakit
berjangkit yang bukan spesifik samaada berasaskan
kebangsaan (lumpuh flaccid akut, konjuntivitis dan
gastroenteritis akut) atau sentinel (penyakit tangan, kaki dan
mulut). Survelan berpandukan makmal juga digunakan untuk
Artikel 1
32 Infectious Disease Bulletin Infectious Disease Bulletin
Rajah 1 : Mekanisma SistemSurvelan di Malaysia

PENCEGAHAN DAN PENGAWALAN PENYAKIT BERJANGKITJADUAL PERTAMA
(Seksyen 2)PENYAKIT-PENYAKIT BERJANGKIT
BAHAGIAN 11.2.3.4.5.6.7.7A8.9.10.11.12.12A13.14.15.16.17.18.19.20.21.22.23.24.
Batuk KokolCampakChancroidDemam Denggi dan Demam Denggi BerdarahDemam KuningDifteriaDisenteri (Semua jenis)EbolaJangkitan Gonococcal (Semua jenis)Keracunan MakananKoleraKustaMalariaMyocarditisPlaguePoliomielitis (Akut)RabiesRelapsing FeverSifilis (Semua jenis)Tetanus (Semua jenis)Tifoid dan Salmonoloses lain.Tifus dan Ricketsioses lain.Tuberkulosis (Semua jenis)Viral EnsefalitisViral HepatitisApa-apa jangkitan microbial lain yang mengancam nyawa
##
***#
#**##
***#########
BAHAGIAN II Human Immunodeficiency Virus Infection (Semua jenis) # Catitan: ( * ) - Notifikasi melalui talipon dan diikuti notifikasi bertulis (dalam masa 24 jam)
( # ) - Notifikasi bertulis dalam masa 1 minggu selepas diagnosa
notifikasi kes penyakit berjangkit secara ‘syndromes’ (sindrom
jaundice akut, sindrom neurologikal akut, sindrom pernafasan
akut, sindrom dermatological akut dan sindrom demam berdarah
akut) bukan secara penyakit spesifik dan mula diimplementasi di
seluruh negara pada tahun 2004.
Survelan penyakit berjangkit oleh agensi lain seperti Jabatan
Perkhidmatan Haiwan dan FOMEMA Sdn. Bhd. juga membuat
survelan untuk penyakit berjangkit tertentu. Survelan untuk
penyakit berjangkit di kalangan pekerja asing dibuat oleh
FOMEMA dan dilaporkan kepada Bahagian Kawalan Penyakit,
KKM. Jabatan Perkhidmatan Haiwan Malaysia pula membuat
survelan untuk penyakit zoonotik. Sekiranya berlaku kejadian
luar biasa penyakit zoonotik pada haiwan seperti rabies,
nipah, avian influenza, JE, vancomycin resistant enterococcus,
bovine tuberculosis, bovine spongiform encephalopathy,
brucellosis, anthrax, toxoplasmosis dan leptospirosos. Jabatan
Perkhidmatan Haiwan perlu melaporkan kepada Cawangan
Survelan Penyakit Berjangkit, KKM seperti dipersetujui oleh
Jawatankuasa Kawalan Penyakit Zoonotik antara Kementerian.
Survelan berpandu komuniti termasuklah pemantauan rumur
atau aduan penyakit berjangkit oleh masyarakat atau orang
awam dan yang disiarkan melalui media cetak dan elektronik.
NOTIFIKASI PENYAKIT BERJANGKIT
Berikut adalah penyakit-penyakit berjangkit yang terdapat di
Jadual 1, Seksyen 2 Akta Pencegahan dan Kawalan Penyakit
Berjangkit 1988 di mana pengamal perubatan perlu memberi
notis kepada Pegawai Kesihatan yang berhampiran seperti
yang ditetapkan di bawah Akta.
From Page 12Photo Gallery
OUTBREAK / CRISIS / DISASTER
Incident command center
HEART
National
State
District
Hospitals
Laboratories
Other Agencies
Disease Control Division proposed to established an
Emergency Preparedness and Response Center under the
CDC Malaysia plan for RM9.
Incidence Command Center
HEART
In House Training
Office of Emergency Preparedness & Response
Communications
Intelligence & Documentation
Stockpiling & Logistic
EIP Malaysia, an in-house training program provides an experiential training environment
which incorporate epidemiological knowledge, laboratory & clinical component and
emergency response, aims to produce competent and skilled epidemiologist to strengthen
our public health workforce.
Dr Fadzilah Kamaludin (Director EIP Malaysia)
54 Infectious Disease Bulletin Infectious Disease Bulletin

MO
NTH
LY I
NFE
CTI
OU
S D
ISEA
SE R
EPO
RT
FOR
MA
LAY
SIA
Nu
mb
er o
f cas
es a
nd
dea
th n
oti
fied
(man
dat
ory
by
Act
34
2) t
o M
inis
try
of H
ealt
h, M
alay
sia
WEE
KST
ATE
S
DIS
EASE
S
Ch
ole
ra
Dys
entr
y
Foo
d P
ois
on
ing
Hep
atit
is A
Typ
ho
id &
Par
atyp
ho
id
Den
gu
e Fe
ver
Den
gu
e H
aem
orr
hag
ic F
ever
Mal
aria
Rel
apsi
ng
Fev
erV
iral
En
cep
hal
itis
Yello
w F
ever
Dip
ther
iaM
easl
esPo
liom
yelit
is, A
cute
Teta
nu
s (O
ther
s)Te
tan
us
Neo
nat
oru
mW
ho
op
ing
Co
ug
hC
han
cro
idG
on
oco
ccal
Infe
ctio
nH
IV In
fect
ion
A
IDS
Syp
hili
s (A
ll Fo
rms)
Vir
al H
epat
itis
(All
Form
s)
Hep
atit
is B
H
epat
itis
C
Hep
atit
is O
ther
(Un
clas
sifie
d)
Lep
rosy
Tub
ercu
losi
s( A
ll Fo
rms)
Ebo
laPl
agu
eR
abie
sTy
ph
us
& O
ther
Ric
kett
sio
ses
HFM
D/M
yoca
rdit
is
Tota
l No
tific
atio
n
0 1 0 0 0 16 2 0 0 0 0 0 0 0 0 0 0 0 0 3 1 0 0 0 0 0 0 11 0 0 0 0 5 39
Perlis
No
te: C
ase
(dea
th)
Dat
a so
urc
es: C
DC
IS 2
01N
o d
ata
avai
lab
le fo
r W
P La
bu
anC
ase
no
tific
atio
n fo
r WP
Kual
a Lu
mp
ur s
tart
ing
fro
m w
eek
25
Kedah
P.Pinang
Perak
Selangor
Negeri Sembilan
Melaka
Johor
Pahang
Terengganu
Kelantan
Sabah
WP KL
WP Labuan
Cu
mm
ula
tive
cas
es(d
eath
)
MA
Y 2
00
5 (1
- 2
8 .5
.20
05
)
un
til
May
TOTAL
Same Period2004
Median00-04
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Case
Death
0 8 43 0 3 81 2 6 0 2 0 0 16 0 0 0 0 0 5 13 5 2 4 2 2 0 0 81 0 0 0 0 149
420
0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 4 0 0 0 0 0 0 3 0 0 0 0 0 9
Case
Death
Case
Death
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 2 0 0 0 0 0 0 0 0 0 0 0 0 3
Case
Death
Case
Death
Case
Death
Case
Death
Case
Death
Case
Death
Case
Death
Case
Death
Case
Death
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Case
Death
Case
Death
Case
Death
Case
Death
Case
Death
Case
Death
20
05
20
04
Sarawak
Surv
eila
nce
Re
po
rts
10 Infectious Disease Bulletin
0 1 7 0 1 127 8 0 0 3 0 0 0 0 0 0 0 0 0 6 3 5 2 1 1 0 1 59 0 0 0 0 95 318
0 0 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 0 0 0 0 0 2
0 3 1 0 0 125 3 3 0 0 0 0 5 0 0 0 0 0 0 7 2 1 6 2 4 0 0 55 0 0 0 0 61 272
0 0 4 0 0 80 5 0 0 0 0 0 8 0 0 0 0 0 1 0 1 3 5 4 1 0 0 42 0 0 0 0 51 200
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 1 0 0 0 0 0 0 0 0 0 1
0 0 56 0 1 71 4 0 0 0 0 0 2 0 0 0 0 0 0 4 4 0 0 0 0 0 0 39 0 0 0 0 36 217
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 2 0 0 0 0 0 0 1 0 0 0 0 0 4
0 0 0 0 0 77 7 0 0 0 0 0 3 0 0 0 0 0 2 18 0 0 1 1 0 0 0 26 0 0 0 0 51 185
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
0 0 55 0 0 36 2 0 0 0 0 0 4 0 0 0 0 0 5 23 1 5 32 10 22 0 3 99 0 0 0 0 105
370
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 1 0 0 0 0 0 0 1 0 0 0 0 0 3
0 2 96 1 3 56 1 15 0 1 0 0 38 0 0 0 0 0 3 82 7 4 45 16 28 0 1 45 0 0 0 0 114
513
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 6 3 0 2 0 2 0 0 0 0 0 0 0 0 11
0 4 2 0 7 22 0 0 0 0 0 0 1 0 0 0 0 0 0 3 0 0 4 2 2 0 0 19 0 0 0 0 5 67
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 0 0 1 0 1 0 0 1 0 0 0 0 0 3
0 9 20 2 772
64 8 1 0 0 0 1 36 0 0 0 0 0 1 83 1 0 20 3 11 4 0 66 0 0 0 0 12 1094
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 1
12 2 13 0 3 56 4 21 0 0 0 0 3 0 0 0 0 0 16 10 1 3 34 27 7 0 1 79 0 0 0 0 12 270
0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 2 0 0 0 0 0 0 0 1 0 0 0 0 0 4
0 6 10 0 0 36 1 92 0 1 0 0 8 0 0 1 0 0 30 1 0 16 8 7 0 1 0 54 0 0 0 0 175
439
12 36 307 3 790
847
47 138 0 7 0 1 124 0 0 1 0 0 63 253
26 39 161
75 78 5 6 675 0 0 0 0 871
4404
0 0 1 0 1 0 0 0 0 1 0 0 0 0 0 0 0 0 0 14 12 0 4 1 3 0 0 8 0 0 0 0 0 41
1 17 622 1 28 16
52 65 396 0 9 0 0 991 0 2 1 3 0 58 283 0 63 143
92 47 3 12 1003 0 0 0 3 23 5375
77 133
2838
102
416
5801
407
2140 0 30 0 1 952 0 10 5 9 0 408
1294 0 476
1479
1137
243
49 56 5077 0 0 0 13 2094
39 174
1717 20 1796
6281
497
699 0 41 0 2 699 0 4 2 19 0 214
1106
125
272
897
538
312
27 40 3492 0 0 0 7
3054
0 0 2 0 2 1 7 2 0 2 0 0 0 0 0 0 1 0 0 58 43 1 11 4 7 0 0 50 0 0 0 0 1
77 133
2838 44 160
7800
410
2181 0 48 0 1
3545 0 8 4 9 0 334
1294 0 341
1143
783
271
45 69 5592 0 0 0 12 109
0 0 1 0 0 3 6 9 0 0 0 1 0 0 0 0 4 0 0 325 0 0 0 0 0 0 0 148 0 0 0 0 0

WEE
KST
ATE
S
DIS
EASE
S
Ch
ole
ra
Dys
entr
y
Foo
d P
ois
on
ing
Hep
atit
is A
Typ
ho
id &
Par
atyp
ho
id
Den
gu
e Fe
ver
Den
gu
e H
aem
orr
hag
ic F
ever
Mal
aria
Rel
apsi
ng
Fev
erV
iral
En
cep
hal
itis
Yello
w F
ever
Dip
ther
iaM
easl
esPo
liom
yelit
is, A
cute
Teta
nu
s (O
ther
s)Te
tan
us
Neo
nat
oru
mW
ho
op
ing
Co
ug
hC
han
cro
idG
on
oco
ccal
Infe
ctio
nH
IV In
fect
ion
A
IDS
Syp
hili
s (A
ll Fo
rms)
Vir
al H
epat
itis
(All
Form
s)
Hep
atit
is B
H
epat
itis
C
Hep
atit
is O
ther
(Un
clas
sifie
d)
Lep
rosy
Tub
ercu
losi
s( A
ll Fo
rms)
Ebo
laPl
agu
eR
abie
sTy
ph
us
& O
ther
Ric
kett
sio
ses
HFM
D/M
yoca
rdit
is
Tota
l No
tific
atio
n
0 1 0 0 0 16 2 0 0 0 0 0 0 0 0 0 0 0 0 3 1 0 0 0 0 0 0 11 0 0 0 0 5 39
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
0 8 43 0 3 81 2 6 0 2 0 0 16 0 0 0 0 0 5 13 5 2 4 2 2 0 0 81 0 0 0 0 149
420
0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 4 0 0 0 0 0 0 3 0 0 0 0 0 9
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 2 0 0 0 0 0 0 0 0 0 0 0 0 3
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Introduction
Under the schedule 1 and 2 of the Prevention and Control
of Infectious Disease Act 1988 (PCID), there are 26 infectious
diseases which every medical practitioner who treats or
become aware of these infectious diseases occurring in
any premises shall, with the least practicable delay, gives
notice of the existence of the said infectious diseases to
the nearest Medical Officer of Health using form 1 of the
Act.
The notification data were collected and compiled on a
weekly basis by the District Health Office. A summary report
was sent to the State Health Department and Statistic Unit,
Disease Control Division, Ministry of Health Malaysia using
EPI-203 form.
The data contained in this report were based on information recorded on EPI-203 form as at 30 May 2005. Any changes
made to EPI-203 data after this date will not be reflected in this report. This report summarizes the data of weekly mandatory
infectious disease notifications collected & which were analysed over the period 1990 to 2004.
0
30000
60000
90000
1E+05
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004
Year
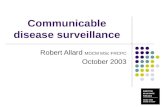
Graf 1: The number of infectious disease notified annually in Malaysia, 1990-2004
Tota
l No
tifi
cati
on
Results
The figure 1, below illustrates the total number of infectious diseases notified annually in Malaysia over the period of 1990
to 2004. The total number of notifications appeared to be decreasing from 1990 until 1992 and started to increase until
1996. From then on, 1997 to 2004, the total number of notifications of infectious diseases appeared to be fluctuating. The
factors which may contribute to the pattern seen may be more likely due to level of compliance in reporting and outbreak
occurrences in some years. Cholera outbreaks which occurred in 1995 and 1996 may have contributed to the increase in
the total number of notifications and in 1996 there was the added increase in dengue fever notifications when compared
the preceding years.
Infectious diseases for which there were no reports (zero notifications) 1990 to 2004 are as follow: yellow fever, plague and
ebola (Ebola made notifiable under the law in 1995). There was a single report of relapsing fever (1999) and three cases of
acute poliomyelitis in 1992. There were zero notifications for rabies cases except in years 1990 (1 case), 1992 (1 case), 1996
(5 cases), 1997 (7 cases), 1998 (1 cases) and 2001 (2 cases).
Malaria, tuberculosis, dengue fever, food poisoning and viral hepatitis were the top 5 infectious diseases being reported.
Tuberculosis, dengue fever and food poisoning were infectious diseases with increasing number of notifications whilst
malaria notifications have been declining.
Surveillance Report
11Infectious Disease Bulletin
In Malaysia - 1990-2004
0 1 7 0 1 127 8 0 0 3 0 0 0 0 0 0 0 0 0 6 3 5 2 1 1 0 1 59 0 0 0 0 95 318
0 0 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 0 0 0 0 0 2
0 3 1 0 0 125 3 3 0 0 0 0 5 0 0 0 0 0 0 7 2 1 6 2 4 0 0 55 0 0 0 0 61 272
0 0 4 0 0 80 5 0 0 0 0 0 8 0 0 0 0 0 1 0 1 3 5 4 1 0 0 42 0 0 0 0 51 200
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 1 0 0 0 0 0 0 0 0 0 1
0 0 56 0 1 71 4 0 0 0 0 0 2 0 0 0 0 0 0 4 4 0 0 0 0 0 0 39 0 0 0 0 36 217
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 2 0 0 0 0 0 0 1 0 0 0 0 0 4
0 0 0 0 0 77 7 0 0 0 0 0 3 0 0 0 0 0 2 18 0 0 1 1 0 0 0 26 0 0 0 0 51 185
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
0 0 55 0 0 36 2 0 0 0 0 0 4 0 0 0 0 0 5 23 1 5 32 10 22 0 3 99 0 0 0 0 105
370
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 1 0 0 0 0 0 0 1 0 0 0 0 0 3
0 2 96 1 3 56 1 15 0 1 0 0 38 0 0 0 0 0 3 82 7 4 45 16 28 0 1 45 0 0 0 0 114
513
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 6 3 0 2 0 2 0 0 0 0 0 0 0 0 11
0 4 2 0 7 22 0 0 0 0 0 0 1 0 0 0 0 0 0 3 0 0 4 2 2 0 0 19 0 0 0 0 5 67
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 0 0 1 0 1 0 0 1 0 0 0 0 0 3
0 9 20 2 772
64 8 1 0 0 0 1 36 0 0 0 0 0 1 83 1 0 20 3 11 4 0 66 0 0 0 0 12 1094
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 1
12 2 13 0 3 56 4 21 0 0 0 0 3 0 0 0 0 0 16 10 1 3 34 27 7 0 1 79 0 0 0 0 12 270
0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 2 0 0 0 0 0 0 0 1 0 0 0 0 0 4
0 6 10 0 0 36 1 92 0 1 0 0 8 0 0 1 0 0 30 1 0 16 8 7 0 1 0 54 0 0 0 0 175
439
12 36 307 3 790
847
47 138 0 7 0 1 124 0 0 1 0 0 63 253
26 39 161
75 78 5 6 675 0 0 0 0 871
4404
0 0 1 0 1 0 0 0 0 1 0 0 0 0 0 0 0 0 0 14 12 0 4 1 3 0 0 8 0 0 0 0 0 41
1 17 622 1 28 16
52 65 396 0 9 0 0 991 0 2 1 3 0 58 283 0 63 143
92 47 3 12 1003 0 0 0 3 23 5375
77 133
2838
102
416
5801
407
2140 0 30 0 1 952 0 10 5 9 0 408
1294 0 476
1479
1137
243
49 56 5077 0 0 0 13 2094
39 174
1717 20 1796
6281
497
699 0 41 0 2 699 0 4 2 19 0 214
1106
125
272
897
538
312
27 40 3492 0 0 0 7
3054
0 0 2 0 2 1 7 2 0 2 0 0 0 0 0 0 1 0 0 58 43 1 11 4 7 0 0 50 0 0 0 0 1
77 133
2838 44 160
7800
410
2181 0 48 0 1
3545 0 8 4 9 0 334
1294 0 341
1143
783
271
45 69 5592 0 0 0 12 109
0 0 1 0 0 3 6 9 0 0 0 1 0 0 0 0 4 0 0 325 0 0 0 0 0 0 0 148 0 0 0 0 0

The new International Health Regulations adopted bythe World Health Assembly in May 2005 (IHR 2005) repre-sents a major development in the use of international lawfor public health purposes. One of the most importantaspects of IHR 2005 is the establishment of a global sur-veillance system for public health emergencies of interna-tional concern. This article assesses the surveillancesystem in IHR 2005 by applying well-established frame-works for evaluating public health surveillance. Theassessment shows that IHR 2005 constitutes a majoradvance in global surveillance from what has prevailed inthe past. Effectively implementing the IHR 2005 surveil-lance objectives requires surmounting technical, resource,governance, legal, and political obstacles. Although IHR2005 contains some provisions that directly address theseobstacles, active support by the World Health Organizationand its member states is required to strengthen nationaland global surveillance capabilities.
On May 23, 2005, the World Health Assembly adoptedthe new International Health Regulations (IHR 2005)
(1) as an international treaty. This step concluded thedecade-long effort led by the World Health Organization(WHO) to revise the old regulations (IHR 1969) to makethem more effective against global disease threats.Originally adopted in 1951 (2) and last substantiallychanged in 1969 (3), IHR 1969 had lost its effectivenessand relevance by the mid-1990s, if not earlier (4).
The resurgence of infectious diseases noted in the firsthalf of the 1990s showed IHR 1969’s limitations. Forexample, after smallpox was eradicated in the late 1970s,IHR 1969 only applied to the traditionally “quarantinable”diseases of cholera, plague, and yellow fever. In addition,
IHR 1969 restricted surveillance to information providedonly by governments, lacked mechanisms for swiftlyassessing and investigating public health risks, containedno strategies for developing surveillance capacities andinfrastructure, and failed to generate compliance by WHOmember states. WHO began revising IHR 1969 in 1995(5), and IHR 2005’s adoption completed the modernizationof this important body of international law on publichealth.
IHR 2005 departs radically from IHR 1969 and repre-sents a historic development in international law on publichealth (6). IHR 2005 expands the scope of the regulations’application, strengthens WHO’s authority in surveillanceand response, contains more demanding surveillance andresponse obligations, and applies human rights principlesto public health interventions. The most dramatic of thesechanges involves a new surveillance system that far sur-passes what the IHR 1969 contained. After reviewing keysurveillance concepts and frameworks, this articledescribes IHR 2005’s surveillance regime and assesses itslikely performance. It concludes by discussing obstaclesthat could prevent IHR 2005 from becoming an effectiveglobal public health surveillance system and addressinghow these obstacles might be overcome.
Key Surveillance Concepts and Evaluation Framework
Public health surveillance has been defined as “theongoing systematic collection, analysis, and interpretationof outcome-specific data for use in the planning, imple-mentation, and evaluation of public health practice” (7). Asurveillance system requires structures and processes tosupport these ongoing functions (7).
The Centers for Disease Control and Prevention (CDC)developed guidelines that identify the essential elementsand attributes for an effective public health surveillance
Global Public Health Surveillanceunder New International Health
RegulationsMichael G. Baker* and David P. Fidler†
PERSPECTIVE
1058 Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 12, No. 7, July 2006
*Wellington School of Medicine and Health Sciences, Wellington,New Zealand; and †Indiana University School of Law,Bloomington, Indiana, USA

system (8). According to these guidelines, evaluating sur-veillance systems involves 2 main steps: 1) describing thepurpose, operation, and elements of the system and 2)assessing its performance according to key attributes. Thisarticle uses this 2-step approach to evaluate the global pub-lic health surveillance system prescribed by IHR 2005.
Surveillance System Specified in IHR 2005In the CDC framework, describing a surveillance sys-
tem includes 4 main elements: 1) health-related eventsunder surveillance and their public health importance, 2)purpose and objectives of the system, 3) components andprocesses of the system, and 4) resources needed to oper-ate it (8).
Health-related Events under SurveillanceIHR 2005 identifies health-related events that each
country that agrees to be bound by the regulations (a “stateparty”) must report to WHO. In terms of health-relatedevents that occur in its territory, a state party must notifyWHO of “all events which may constitute a public healthemergency of international concern” (article 6.1). Theseevents include any unexpected or unusual public healthevent regardless of its origin or source (article 7). IHR2005 also requires state parties, as far as is practicable, toinform WHO of public health risks identified outside theirterritories that may cause international disease spread, asmanifested by exported or imported human cases, vectorsthat may carry infection or contamination, or contaminat-ed goods (article 9.2).
IHR 2005 provides guidance to assist state parties’compliance with these obligations in 4 ways. First, IHR2005 defines a “public health emergency of internationalconcern” (PHEIC) as “an extraordinary event which isdetermined [by the WHO Director-General]… (i) to con-stitute a public health risk to other States through the inter-national spread of disease and (ii) to potentially require acoordinated international response” (article 1.1). UnlikeIHR 1969’s limited scope of application to just 3 commu-nicable diseases (3), IHR 2005 defines disease as an illnessor medical condition that does or could threaten humanhealth regardless of its source or origin (article 1.1). Thisscope therefore encompasses communicable and noncom-municable disease events, whether naturally occurring,accidentally caused, or intentionally created.
Second, IHR 2005 contains a “decision instrument”(annex 2) that helps state parties identify whether a health-related event may constitute a PHEIC and thereforerequires formal notification to WHO (Figure 1). The deci-sion instrument focuses on risk assessment criteria of pub-lic health importance, including the seriousness of thepublic health impact and the likelihood of internationalspread.
Third, IHR 2005 includes a list of diseases for which asingle case may constitute a PHEIC and must be reportedto WHO immediately. This list consists of smallpox,poliomyelitis, human influenza caused by new subtypes,and severe acute respiratory syndrome (SARS). A secondlist of diseases exists (Figure 1) for which a single caserequires the decision instrument to be used to assess theevent, but notification is determined by the assessment andis not automatic. Finally, IHR 2005 also encourages stateparties to consult with WHO over events that do not meetthe criteria for formal notification but may still be of pub-lic health relevance (article 8).
IHR 2005’s expansion of the range of public healthevents under surveillance and the use of risk assessmentcriteria in deciding what is reportable is possibly the singlemost important surveillance advance in IHR 2005. Thischange greatly enhances effective surveillance of emerg-ing infectious diseases, which are “infections that havenewly appeared in a population or have existed but are rap-idly increasing in incidence or geographic range” (9). IHR2005’s surveillance strategy, especially the decision instru-ment, has been specifically designed to make IHR 2005directly applicable to emerging infectious disease events,
Surveillance under International Health Regulations
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 12, No. 7, July 2006 1059
Figure 1. International Health Regulations (IHR) 2005 decisioninstrument (simplified from annex 2 of IHR).

which are usually unexpected and often threaten to spreadinternationally.
In addition to events that may constitute a PHEIC, IHR2005 also requires state parties to report the health meas-ures (e.g., border screening, quarantine) that they imple-ment in response to such events (article 6). State partiesare also specifically required to inform WHO within 48hours of implementing additional health measures thatinterfere with international trade and travel, unless theWHO Director-General has recommended such measures(article 43).
Purpose and Objectives of Surveillance under IHR 2005
IHR 2005’s purpose is to prevent, protect against, con-trol, and facilitate public health responses to the interna-tional spread of disease (article 2), and IHR 2005 makessurveillance central to guiding effective public healthaction against cross-border disease threats. The regulationsdefine surveillance as “the systematic ongoing collection,collation and analysis of data for public health purposesand the timely dissemination of public health informationfor assessment and public health response as necessary”(article 1.1). Surveillance is central to IHR 2005’s publichealth objectives, which explains why IHR 2005 requiresall state parties to develop, strengthen, and maintain coresurveillance capacities (article 5.1). This obligation goesbeyond anything concerning surveillance in IHR 1969,which did not address surveillance infrastructure and capa-bilities beyond a general requirement for a state party tonotify WHO of any outbreak of a disease subject to theregulations.
Components and Processes of IHR 2005 SurveillanceIHR 2005 describes key aspects of the surveillance
process from the local to the global level. As part of IHR2005’s core surveillance and response capacity require-ments, each state party has to develop and maintain capa-bilities to detect, assess, and report disease events at thelocal, intermediate, and national levels (article 5.1, annex1). Officials at the national level must be able to reportthrough the national IHR focal point to WHO whenrequired under IHR 2005 (articles 4.2 and 6). The regula-tions also mandate that WHO establish IHR contact pointsthat are always accessible to state parties (article 4.3).Connecting these levels produces the surveillance archi-tecture illustrated in Figure 2.
Requiring that a national IHR focal point be establishedis another surveillance initiative in IHR 2005. The focalpoint is designed to facilitate rapid sharing of surveillanceinformation because it is responsible for communicatingwith the WHO IHR contact points and disseminating infor-mation within the state party (article 4.2). By linking
national IHR focal points through WHO, IHR 2005 estab-lishes a global network that improves the real-time flow ofsurveillance information from the local to the global leveland also between state parties (article 4.4).
Resources Needed to Operate IHR 2005’s Surveillance System
Building and maintaining the surveillance system envi-sioned in IHR 2005 will require substantial financial andtechnical resources. State parties will be primarily respon-sible for providing resources needed to develop their coresurveillance capacities. Each state party has to assess itsability to meet the core surveillance requirements by June2009. In addition, each state party has to develop andimplement a plan for ensuring compliance with core sur-veillance obligations (articles 5.1 and 5.2, annex 1).
WHO is obliged to assist state parties in meeting theirsurveillance system obligations (article 5.3), but this provi-sion does not allocate any WHO funds for this purpose.State parties are required to collaborate with each other inproviding technical cooperation and logistical support forsurveillance capabilities and in mobilizing financialresources to facilitate implementation of IHR 2005 (article44.1).
Evaluating the IHR 2005 Surveillance System’sAttributes and Potential Performance
Key attributes of effective surveillance systems identi-fied by CDC are usefulness, sensitivity, timeliness, stabil-ity, simplicity, flexibility, acceptability, data quality,positive predictive value, and representativeness. Of these
PERSPECTIVE
1060 Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 12, No. 7, July 2006
Figure 2. Public health surveillance structures and processesspecified in International Health Regulations (IHR) 2005.

attributes, usefulness, sensitivity, timeliness, and stabilitywill be most critical to the success of the IHR 2005 sur-veillance system. Simplicity, acceptability, and flexibilitywill affect the establishment and sustainability of the sur-veillance system. Data quality, positive predictive value,and representativeness are central to accurately character-izing health-related events under surveillance. Table 1summarizes these attributes, provides commentary ontheir relevance to effective surveillance under IHR 2005,and assesses the likely performance of the IHR 2005 sur-veillance system for each attribute. The following para-graphs concentrate on assessing IHR 2005 with respect tothe key attributes of usefulness, sensitivity, timeliness,and stability.
Usefulness of the Surveillance SystemThe central premise of IHR 2005 is that rapidly detect-
ing PHEIC will support improved disease prevention andcontrol both within and between state parties. Ample evi-dence shows that delayed recognition and response toemerging diseases may result in adverse consequences interms of illness and death, spread to other countries, anddisruption of trade and travel (10). The usefulness of sur-veillance under IHR 2005 represents the sum of all the crit-ical system attributes and can only be assessed after thesystem is in operation, so this attribute is not discussedhere. However, for the future sustainability and develop-ment of IHR 2005, we must evaluate its overall usefulness
and document its contribution to prevention and control ofadverse health events. IHR includes mechanisms to reviewand, if necessary, amend its provisions and in particularrequires periodic evaluation of the functioning of the deci-sion instrument (article 54).
Sensitivity of the Surveillance SystemThe IHR 2005 surveillance provisions imply 100% sen-
sitivity as a standard, namely the reporting of all eventsthat meet notification requirements. The use of risk assess-ment criteria (Figure 1) also allows for higher sensitivityfor PHEIC than would be possible with a list of predeter-mined disease threats (as in IHR 1969). To test the poten-tial sensitivity of the decision instrument proposed indrafts of the revised IHR in 2004, investigators in theUnited Kingdom applied the then-proposed decisioninstrument to all events (N = 30) that were importantenough to have been published in the national surveillancebulletin for England and Wales during 2003 (11).According to this method, 12 of the 30 events would havebeen reportable under the decision instrument. Theseevents included all those that were considered potentialPHEIC. Investigators concluded that the decision instru-ment was highly sensitive for selecting outbreaks and inci-dents that require reporting under the proposed IHRrevision.
The sensitivity of the IHR 2005 surveillance systemwill probably be affected by 2 factors. First, in all likeli-
Surveillance under International Health Regulations
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 12, No. 7, July 2006 1061

hood, inadequate capacities at the local and intermediatelevels within state parties will limit the system’s sensitivi-ty more than capacities at the national level. Second, stateparties may not always be willing to comply with theirreporting obligations in the face of possible adverse polit-ical and economic consequences that may result fromalerting the world to a disease event in their territories.Fear of such adverse consequences undermined reportingobligations in IHR 1969.
IHR 2005 incorporates strategies to address thesepotential limitations. First, as noted above, IHR 2005requires state parties to build and maintain core local,intermediate, and national surveillance capabilities (article5.1, annex 1). Fulfillment of this obligation will improvesurveillance capacity vertically, from local to national lev-els, which should support higher sensitivity.
Second, IHR 2005 permits WHO to improve sensitivi-ty by collecting and using information from multiplesources. IHR 1969 only allowed WHO to use informationprovided by state parties (3), and failure of state parties toabide by their reporting obligations adversely affectedWHO surveillance activities (5). Under IHR 2005, WHOcan collect, analyze, and use information gathered fromgovernments, other intergovernmental organizations, andnongovernmental organizations and actors (article 9.1). Bypermitting WHO to cast its surveillance network beyondinformation it receives from governments, IHR 2005 cre-ates opportunities for WHO to improve the sensitivity ofthe surveillance system and avoid being blocked by gov-ernmental failure to comply with reporting requirements.
Timeliness of the Surveillance SystemPublic health practitioners understand how timely noti-
fication of public health risks is necessary for effectiveintervention strategies (12,13), lessons reiterated in theSARS pandemic (14). Timely surveillance is also stressedin connection with strategies to deal with pandemic influen-za (15,16). Timeliness may be the most important attributethat IHR 2005 will have to demonstrate to be effective.
IHR 2005 contains several provisions that relate to time-liness. National-level assessments with the decision instru-ment must be completed within 48 hours (annex 1, part A,6[a]). State parties must then notify WHO within 24 hoursof assessing any event that may constitute a PHEIC or thatis unexpected or unusual (articles 6.1 and 7). The same 24-hour requirement applies to reporting public health risk out-side a state party’s territory that may constitute a PHEIC(article 9). State parties must also respond within 24 hoursto all requests that WHO makes for verification of health-related events in their territories (article 10.2).
Timeliness of reporting is likely to be affected more byactions taken at local and intermediate levels than national-level provision of information to WHO. In this regard,
IHR 2005 includes the core surveillance capacity thatlocal and intermediate public health entities must be ableto carry out their reporting responsibilities immediately(annex 1).
WHO’s ability to draw on a wide array of sources ofinformation, including the Internet and nongovernmentalorganizations and actors, may enhance the timeliness ofthe IHR 2005 surveillance system (13,17). In countries thathave less well-developed local, intermediate, and nationalsurveillance systems, nongovernmental sources of infor-mation can often provide information faster than govern-ments. Accessing this type of information early and oftenhelps WHO contact countries sooner, which increases thechances of more effective interventions.
Stability of the Surveillance SystemThe obligations each state party has to build and main-
tain core capacities in surveillance at the local, intermedi-ary, and national levels, combined with the responsibilitiesfor surveillance WHO has globally, should construct aglobal surveillance system that will be stable and reliableover time. Recognizing that core capacities at the nationallevel and below will not develop overnight, IHR 2005gives state parties until June 2012 to develop these capac-ities (article 5.1). State parties can obtain a 2-year exten-sion on this deadline by submitting a justified need and animplementation plan and can request an additional 2-yearextension, which the WHO Director-General has the dis-cretion to approve or deny (article 5.2).
The 5-year grace period, and the possibility of 2-yearextensions, was a necessary compromise and reflects thedifficulties many developing states will have in improvingtheir surveillance systems. The stability and reliability ofthe IHR 2005 surveillance system are designed to increasesteadily as the grace period and any extensions come to anend.
Potential Obstacles to Achieving IHR 2005Surveillance System Objectives
Continued lamentations about the weaknesses of publichealth surveillance nationally and globally (18) illustratethat achieving useful, sensitive, timely, and stable surveil-lance through IHR 2005 will be a challenge for states andthe international community. Several potential obstacles,including technical, resource, governance, legal, and polit-ical concerns, will complicate and frustrate efforts toimprove national and global surveillance capabilities.Table 2 summarizes these potential barriers and possibleresponses.
Technical IssuesEmerging infectious diseases often create technical
challenges for surveillance, even for the most technologi-
PERSPECTIVE
1062 Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 12, No. 7, July 2006

cally advanced and well-resourced countries. The sensitiv-ity of surveillance systems for new pathogens has histori-cally been limited, particularly if such pathogens presentedthemselves in unusual or unexpected ways. Recent model-ing has shown that the ability to control the spread of anew pathogen is influenced by the proportion of transmis-sion that occurs before the onset of overt symptoms orthrough asymptomatic infection (19). This propertyexplains why diseases such as influenza and HIV may bemore difficult to control than smallpox or SARS.
Consequently, surveillance needs to be sufficiently sen-sitive to detect infectious agents that have not yet resultedin large numbers of diagnosed cases. One approach to thischallenge is syndromic surveillance (20), but such surveil-lance has not been effective in detecting emerging infec-tious diseases early (21). In fact, WHO abandonedsyndromic surveillance as a strategy for the revised IHRafter pilot studies demonstrated that it was not effective(22). Improved diagnostic technologies may also help pub-lic health authorities identify new pathogenic threats (23).Strategies for enhancing reporting processes have beenwell described (24).
Resource IssuesThe demands of IHR 2005 surveillance obligations will
confront many countries, particularly developing coun-tries, with resource challenges. IHR 2005 does not includefinancing mechanisms, which leaves each state party tobear the financial costs of improving its own local, inter-mediate, and national level surveillance capabilities. Theobligation on state parties and WHO to collaborate inmobilizing financial resources (article 44) is a weak obli-gation at best. The lack of economic resources will, if notmore vigorously addressed as recommended by the UNSecretary-General (25), retard progress on all aspects ofthe upgraded surveillance system. WHO, in conjunction
with the United Nations and the World Bank, could consid-er developing a global strategy to support the developmentand maintenance of core surveillance capacities.
Governance IssuesGovernance obstacles include managerial and adminis-
trative weaknesses in countries from the local to thenational level. Few countries have conducted a systematicreview of their surveillance systems, and thus most lackdetailed knowledge of gaps and limitations in their surveil-lance infrastructures and how to address these problems(26). Only a few states have assessed their ability to detectand respond to emerging disease threats, such as thoseposed by bioterrorism agents (27). The IHR 2005 require-ment that each state party assess the condition of its publichealth surveillance within 2 years of the regulations’ entryinto force should help countries improve their nationalgovernance for surveillance purposes. Again, many stateswill need external assistance with such work.
Legal IssuesState parties may face legal complications in imple-
menting IHR 2005 within their national legal and constitu-tional systems. For example, the United States hasindicated that requirements of US federalism may affect itscompliance with IHR 2005 (28). The US position suggeststhat other countries may also wish to formulate reserva-tions to IHR 2005 to account for the demands of theirnational constitutional structures and systems of law (29).Whether such reservations will undermine the IHR 2005surveillance system cannot be assessed, but this concernhas to be monitored closely as countries determine whetherreservations are required under their national constitution-al systems. IHR 2005 also specifies that domestic legisla-tion and administrative arrangements be adjusted fullywith IHR 2005 by June 2007, or by June 2008 after a
Surveillance under International Health Regulations
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 12, No. 7, July 2006 1063

suitable declaration to the WHO Director-General (article59.3). Helping state parties update their public health lawmay be technical assistance that industrialized countriescan provide.
Political IssuesQuestions remain about the level of political commit-
ment countries will demonstrate in implementing IHR2005. IHR 1969 suffered because state parties frequentlyfailed to report notifiable diseases and routinely appliedexcessive trade and travel restrictions (4). The relevance ofsuch trade and travel concerns was most recently illustrat-ed during the SARS pandemic through China’s initial fearsthat disclosing the pandemic would harm its economy andforeign trade (30,31). WHO’s access to nongovernmentalsources of surveillance information reduces the incentivesthat state parties once had to hide disease events, as wasdemonstrated during the SARS pandemic (32). In addition,IHR 2005 includes provisions that require WHO to recom-mend, and state parties to use, control measures that are nomore restrictive than necessary to achieve the desired levelof health protection (articles 17, 43). Uncertainty lingers,however, as to whether these obligations will fare better interms of state party compliance than similar ones in IHR1969.
ConclusionEstablishing effective global public health surveillance
is at the heart of IHR 2005. Evaluating the surveillancesystem specified by IHR 2005 is necessary to understandthe potential for this new set of international legal rules tocontribute to global health governance. IHR 2005 pre-scribes essential elements of a surveillance system andseeks to achieve the critical attributes of usefulness, sensi-tivity, timeliness, and stability. These features resonatewith other aspects of IHR 2005 that make it a seminaldevelopment for global health governance. In May 2006,the World Health Assembly adopted a resolution urgingWHO member states to comply immediately, on a volun-tary basis, with IHR 2005 in light of the threat posed byavian influenza (33).
The task of turning the IHR 2005 vision of an effectiveglobal public health surveillance system into reality isdaunting. Of the obstacles complicating this challenge,lack of financial resources to upgrade surveillance sys-tems, especially in developing countries, will be the mostdifficult to overcome. In IHR 2005, public health has beengiven a governance regime unlike anything in the historyof international law on public health. Turning the blueprintdetailed in IHR 2005 into functional architecture that ben-efits all is one of the great public health challenges of thefirst decades of the 21st century.
Dr Baker is a public health physician and senior lecturer atthe Wellington School of Medicine and Health Sciences. He hasworked as a short-term consultant to WHO during developmentand implementation of IHR 2005. His research interests includeemerging infectious diseases, surveillance and outbreak investi-gation, and the role of housing conditions as health determinants.
Mr Fidler is an international lawyer and professor of law atthe Indiana University School of Law, Bloomington, Indiana. Inconjunction with the Center for Law and the Public’s Health ofGeorgetown and Johns Hopkins Universities, he provided analy-sis to WHO of potential conflicts between IHR 2005 and otherinternational legal regimes. His research interests include globalhealth governance, biosecurity, and the role of international lawin global public health.
References
1. World Health Assembly. Revision of the International HealthRegulations, WHA58.3. 2005 [cited 2006 May 2]. Available fromht tp : / /www.who. in t /gb/ebwha/pdf_f i les /WHA58-REC1/english/Resolutions.pdf
2. United Nations. International Sanitary Regulations, 175 UN TreatySeries 214. 1951.
3. World Health Organization. International Health Regulations (1969).3rd ed. Geneva: The Organization; 1983.
4. Fidler D. International law and infectious diseases. Oxford:Clarendon Press; 1999.
5. World Health Organization. Global crises—global solutions: manag-ing public health emergencies through the revised InternationalHealth Regulations. Geneva: The Organization; 2002.
6. Fidler D. From international sanitary conventions to global healthsecurity: the new International Health Regulations. Chinese JInternational Law. 2005;4:325–92.
7. Thacker SB. Historical development. In: Teutsch ST, Churchill RE,editors. Principles and practice of public health surveillance. NewYork: Oxford University Press; 2000. p. 1–16.
8. Centers for Disease Control and Prevention. Updated guidelines forevaluating public health surveillance systems: recommendationsfrom the guidelines working group. MMWR Morb Mortal Wkly Rep.2001;50:1–36. Available from http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5030a5.htm
9. Morse SS. Factors in the emergence of infectious diseases. EmergInfect Dis. 1995;1:7–15.
10. Heymann DL, Rodier G. Global surveillance, national surveillance,and SARS. Emerg Infect Dis. 2004;10:173–5.
11. Morris J, Ward JD, Nicoll A. Proposed new International HealthRegulations 2005—validation of a decision instrument (algorithm).Euro Surveill. 2004;9:66–7. Available from http://www.eurosurveil-lance.org/eq/2004/04-04/pdf/eq_12_2004_66-67.pdf
12. Jajosky RA, Groseclose SL. Evaluation of reporting timeliness ofpublic health surveillance systems for infectious diseases. BMCPublic Health. 2004;4:29.
13. Grein TW, Kamara KB, Rodier G, Plant AJ, Bovier P, Ryan MJ, et al.Rumors of disease in the global village: outbreak verification. EmergInfect Dis. 2000;6:97–102.
14. Reflections on SARS. Lancet Infect Dis. 2004;4:651.15. Ferguson NM, Cummings DA, Cauchemez S, Fraser C, Riley S,
Meeyai A, et al. Strategies for containing an emerging influenza pan-demic in Southeast Asia. Nature. 2005;437:209–14.
16. Longini IM Jr, Nizam A, Xu S, Ungchusak K, Hanshaoworakul W,Cummings DA, et al. Containing pandemic influenza at the source.Science. 2005;309:1083–7.
PERSPECTIVE
1064 Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 12, No. 7, July 2006

17. Samaan G, Patel M, Olowokure B, Roces MC, Oshitani H; WorldHealth Organization Outbreak Response Team. Rumor surveillanceand avian influenza H5N1. Emerg Infect Dis. 2005;11:463–6.
18. Butler D. Disease surveillance needs a revolution. Nature.2006;440:6–7.
19. Fraser C, Riley S, Anderson RM, Ferguson NM. Factors that make aninfectious disease outbreak controllable. Proc Natl Acad Sci U S A.2004;101:6146–51.
20. Mandl KD, Overhage JM, Wagner MM, Lober WB, Sebastiani P,Mostashari F. Implementing syndromic surveillance: a practicalguide informed by the early experience. J Am Med Inform Assoc.2004;11:141–50.
21. Weber SG, Pitrak D. Accuracy of a local surveillance system for earlydetection of emerging infectious disease. JAMA. 2003;290:596–8.
22. Revision of the International Health Regulations. Progress report.Wkly Epidemiol Rec. 2001;76:61–3.
23. Cockerill FR, Smith T. Response of the clinical microbiology labora-tory to emerging (new) and reemerging infectious diseases. J ClinMicrobiol. 2004;42:2359–65.
24. Silk BJ, Berkelman R. A review of strategies for enhancing the com-pleteness of notifiable disease reporting. J Public Health ManagPract. 2005;11:191–200.
25. Secretary-General of the United Nations. In larger freedom: towardsdevelopment, security and human rights for all: report of the secre-tary-general, A/59/2005. New York: United Nations; 2005.
26. McNabb SJ, Chungong S, Ryan M, Wuhib T, Nsubuga P, Alemu W,et al. Conceptual framework of public health surveillance and actionand its application in health sector reform. BMC Public Health.2002;2:2.
27. Bravata DM, McDonald KM, Smith WM, Rydzak C, Szeto H,Buckeridge DL, et al. Systematic review: surveillance systems forearly detection of bioterrorism-related diseases. Ann Intern Med.2004;140:910–22.
28. Statement for the record by the Government of the United States ofAmerica concerning the World Health Organization’s revisedInternational Health Regulations. 2005 May 23 [cited 2006 May 2].Available from http://usinfo.state.gov/usinfo/Archive/2005/May/23-321998.html
29. Wilson K, McDougall C, Upshur R. The new International HealthRegulations and the federalism dilemma. PLoS Med. 2006;3:e1.
30. Hesketh T. China in the grip of SARS. BMJ. 2003;326:1095.31. Liu Y. China’s public health-care system: facing the challenges. Bull
World Health Organ. 2004;82:532–8.32. Fidler D. SARS, governance, and the globalization of disease.
Basingstoke (UK): Palgrave Macmillan; 2004.33. World Health Assembly. Application of the International Health
Regulations (2005). WHA59.3. 26 May 2006 [cited 2006 June 1].Available from http://www.who.int/gb/ebwha/pdf_files/WHA59/WHA59_2-en.pdf
Address for correspondence: Michael G. Baker, Department of PublicHealth, Wellington School of Medicine and Health Sciences, Box 7343,Wellington South, New Zealand; email: [email protected]
Surveillance under International Health Regulations
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 12, No. 7, July 2006 1065
Use of trade names is for identification only and does not implyendorsement by the Public Health Service or by the U.S.Department of Health and Human Services.
Searchpast issues