Disclosures and Acknowledgements Longevity, …...1 Longevity, health, and well-being in our...
14
1 Longevity, health, and well-being in our patients Prasanna Jagannathan, M.D. Assistant Professor Division of HIV, ID, and Global Medicine UCSF Disclosures and Acknowledgements No Disclosures Goals: Life expectancy and wellness in HIV Mind the (life expectancy) gap HIV in 2016 What makes up the gap? Some strategies to narrow the gap Mind the (quality of life) gap! What makes up the gap? Some strategies to narrow the gap Case 1: C.C. 55 yo man with HIV receiving primary care at Ward 86, ZSFG HIV: Diagnosed 1990, CD4 nadir 50, now in low 200s History of thrush, no other OIs ART: VL suppressed since 2003 2001-03: Trizivir + TFV 2003-08: EFZ + TFV + 3TC + DDI 2008-current: atripla
Transcript of Disclosures and Acknowledgements Longevity, …...1 Longevity, health, and well-being in our...

1
Longevity, health, and well-being in our patients
Prasanna Jagannathan, M.D.
Assistant Professor
Division of HIV, ID, and Global Medicine
UCSF
Disclosures and Acknowledgements
No Disclosures
Goals: Life expectancy and wellness in HIV
Mind the (life expectancy) gap HIV in 2016 What makes up the gap?
Some strategies to narrow the gap
Mind the (quality of life) gap! What makes up the gap?
Some strategies to narrow the gap
Case 1: C.C.
55 yo man with HIV receiving primary care at Ward 86, ZSFG
HIV: Diagnosed 1990, CD4 nadir 50, now in low 200s History of thrush, no other OIs
ART: VL suppressed since 2003 2001-03: Trizivir + TFV
2003-08: EFZ + TFV + 3TC + DDI
2008-current: atripla

2
Case 1: C.C.
PMH:
HCV Genotype 1a Portal HTN on imaging (esophageal varices)
h/o seizures (?ETOH-related)
h/o depression (not on treatment)
SH: Stays in his home most of the day caring for very ill partner
Substances:
ETOH: up to 6 pack of beer per night
Smokes ½ - 1 ppd
If you are this patient’s PCP in 2016: What are you most worried about?
0A B C D E
A) Curing his HCV
B) Poor immune recovery/Modernizing his ART
C) Alcohol use
D) Smoking cessation
E) Lack of physical activity
F) Something else
CC’s priorities
Resources to support care of his partner
Tobacco Has cut back and quit a few times, but always
resumes (partner also smokes)
HCV (once INF-sparing regimens became available)
Cutting back on his drinking (for his partner)
Life expectancy in HIV 2016: Closing the gap (Kaiser data)
*Marcus et al JAIDS 1 Sep 2016
N=24768HIV-infected
N=257600HIV-uninfected

3
What is the major driver of the persistent gap in life expectancy?
A) HBV/HCV co-infection
B) HIV-associated malignancies
C) Late ART initiation/immune activation
D) Drug/alcohol use
E) Smoking
F) Something else
0A B C D E F
Life expectancy in HIV 2016: Closing the gap
*Marcus et al JAIDS 1 Sep 2016
Smoking in HIV-infected individuals
Prevalence in HIV-infected: 40-70% General population prevalence 20% HIV-infected also significantly less likely to quit
Several studies link smoking in PLWHA to: Decreased virologic/immunologic response Worse adherence to ART Increased rates of non AIDS-defining malignancies (lung,
head/neck) Low BMD Significantly more CAD, myocardial infarctions
Mdodo et al Ann Intern Med. 2015Sigel et al AIDS 2012Stead et al Cochrane Reviews 2012Rasmussen CID 2015
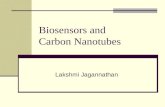
Smoking in HIV-infected individuals: 16 less years of life?
Helleberg CID 2013
A 35-year-old HIV patient had a median life expectancy of 62.6 years (95% CI, 59.9–64.6) for smokers and 78.4 years (95% CI, 70.8–84.0) for nonsmokers.

4
Quitting smoking could result in an increase of 4-6 years of life expectancy
Reddy et al JID 1 Nov 2016
Relative gains in life expectancy for different interventions
Reddy et al JID 1 Nov 2016
The image part with relationship ID rId3 was not found in the file.
How would you advise him with smoking cessation?
Pick a quit date and:
A) Advise him to quit cold turkey
B) Advise him to cut back slowly
0A B
How would you help him with smoking cessation?
A) Counsel + Nicotine patch/lozenge
B) Counsel + E-cigarettes
C) Counsel + Bupropion SR (Wellbutrin)
D) Counsel + Varenicline
0A B C D

5
USPSTF Guidance: Updated 2015
http://www.uspreventiveservicestaskforce.org/
RCT of abrupt vs gradual smoking in 2 weeks before quitting Used NRT before and after quit date
Outcome: prolonged validated abstinence 4 wks after quit date
Abstinent, n (%)
Time after quitting
Gradual cessation (n=342)
Abrupt cessation (n=355)
RR (95% CI)
4 wks 134 (39.2) 174 (49) 0.80 (0.66-0.93)
6 wks 100 (29.2) 130 (36.6) 0.80 (0.62-0.95)
6 months 53 (15.5) 78 (22.0) 0.71 (0.46-0.91)
Lindson-Hawley et al Annals of Internal Med 2016
Cochrane meta-analysis of pharmacologic interventions for smoking cessation: 2013
Cahill et al Cochrane Library 2013
0.5 1.0 1.5 2.0 2.5
Posterior Median Odds
Better Efficacy
Bupropion vs NRT
Varenicline vs NRT
Varenicline vs Bupropion
Varenicline vs Combo NRT
Is varenicline safe?
Thomas et al BMJ 2015
Meta analysis of 39 RCTs (>10000 patients)
-- No increased risk of suicide or attempted suicide, suicidal ideation, depression, or death in varenicline users compared with placebo users -- Varenicline was associated with an increased risk of sleep disorders, insomnia, andabnormal dreams

6
What about in patients with psychiatric co-morbidities?
Anthenelli et al Lancet 2016
Large RCT of safety and efficacy of varenicline vs buproprion vs nicotine patch vs placebo
8144 patients 4116 to psychiatric cohort
4028 to non-psychiatric cohort
What about in patients with psychiatric co-morbidities?
Anthenelli et al Lancet 2016
-4 -2 0 2 4
Absolute Risk Difference in primary neuropsychiatric endpoint
Favors varenicline
Varenicline vs Placebo
Varenicline vs NRT
Varenicline vs Bupropion
Non-psychiatric cohortPsychiatric cohort
Favors comparator
No significant difference in primary composite neuropsychiatric endpoint No difference in secondary endpoints including
suicadality
What about in patients with psychiatric co-morbidities?
Anthenelli et al Lancet 2016
Varenicline more effective than bupropion and nicotine replacement in non-psychiatric and psychiatric populations
0.5 1.0 1.5 2.0 2.5
Odds Ratio
Better Efficacy
Bupropion vs NRT
Varenicline vs NRT
Varenicline vs Bupropion
Non-psychiatric cohortPsychiatric cohort
Can varenicline be used in patients not ready to quit?
Ebbert et al JAMA 2015
RCT of 1510 patients not ready to quit in next month -- Randomized to varenicline or
placebo for 24 weeks
-- Clinically significant reductions in abstinencerates at end of treatmentand at 1 year

7
Pharmacist-led interventions in HIV clinics
Cropsey et al JAIDS 2015: Randomized trial of algorithm-based pharmacotherapy of tobacco vsstandard of care in HIV clinics Research staff with no specific prior training in
tobacco cessation administered questionnaire and assessed patient’s readiness to quit
If patient ready, algorithmic approach of medications (varenicline if no kidney impairment or history of suicide; then wellbutrin; then NRT)
Results: more quit attempts, greater smoking reduction, more cessation readiness
What about E-cigarettes? Would you recommend vaping to patients to consider quitting smoking?
Yes
No
0A B
Vaping – what controversy?
USPSTF statement on E-cigarettes: September 2015
We conclude that available data on the use of ENDS (electronic nicotine delivery systems) for smoking cessation are quite limited and suggest no benefit among smokers intending to quit.”
“the evidence on the use of ENDS for tobacco smoking cessation … is insufficient, and the balance of benefits and harms cannot be determined.
“the lack of well-designed, randomized, controlled trials (RCTs) on ENDS that report smoking abstinence or adverse events as a critical gap in the evidence.”
Patnode et al Ann Int Med 2015

8
UCSF Metaanalysis: E-cigarettes associated with less quit attempts
Kalkhoran et al Lancet Resp Med 2016
Key Recommendations• Smoking if the biggest avoidable
cause of death in the UK• Provision of nicotine without harmful
components of tobacco smoke can prevent most of the harm from smoking
• Hazard to health arising from long-term vapor inhalation from e-cigarettes is unlikely to exceed 5% harm from smoking tobacco
• In the interests of public health it is important to promote the use of e-cigarettes, NRT, and other nicotine products as a substitute for smoking
British Royal College of Physicians: Vaping as harm reduction: April 2016
C.C.
Cured his HCV with ledipasvir/sofosbuvir
Declined bupropion and varenicline due to black box warnings
Decided to use e-cigarettes – Quit regular cigarettes, but continues to vape
Case 2: S.B.
48 y.o man from Fiji Diagnosed with pulmonary TB at diagnosis in 2009
GFR of 45 at dx
Started on RIPE + EFZ + ABC/3TC

9
Case 2: S.B.
PMH No prior medical
problems
Social history: Undocumented
From Fiji
Gets $177/month GA
Family history Father with heart attack in
60s
Vitals: Height 5’8”, Weight: 172
lbs
BP 132/68
Labs CD4 50, VL 65000
HbA1C: 5.6
Case 2: S.B.
Excellent response to DOT RIPE + ART CD4 rise to >200, VL quickly suppressed
Housed through TB clinic
But… after DOT ended
23
no
v20
09
08
de
c20
09
05
ap
r20
10
22
jul2
01
02
1o
ct2
01
01
4ja
n2
01
11
4a
pr2
01
10
8se
p2
01
13
0n
ov2
01
10
1m
ar2
01
2
10
100
1000
10000
100000
0
100
200
300
400
500
600
Vira
l Loa
d
CD
4+ T
cells/uL
vl
cd4
EFZ +ABC/3TC
K103NM184V
GFR 45
What ART would you switch to now? (K103N, M184V, GFR 45)
A) DRV/r + TAF/FTC
B) DRV/r + ETR + 3TC
C) DRV/r + RAL + 3TC
D) DRV/r + DTG + 3TC
E) DTG/3TC
F) Something else
0A B C D E F

10
23
no
v20
09
08
de
c20
09
05
ap
r20
10
22
jul2
01
02
1o
ct2
01
01
4ja
n2
01
11
4a
pr2
01
10
8se
p2
01
13
0n
ov2
01
10
1m
ar2
01
21
4a
pr2
01
22
0ju
l20
12
06
de
c20
12
04
ap
r20
13
26
jul2
01
30
8n
ov2
01
30
3m
ar2
01
42
3m
ay2
01
42
0ju
n2
01
42
3fe
b2
01
52
4a
pr2
01
51
8d
ec2
01
50
8a
pr2
01
6
10
100
1000
10000
100000
0
100
200
300
400
500
600
Vira
l Loa
d
CD
4+ T
cells/uL
vl
cd4
EFZ +ABC/3TC
DRV/r BID+RAL BID+ 3TC
K103NM184V
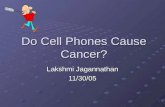
Sometimes getting ‘healthy’ has its consequences
23
no
v20
09
08
de
c20
09
05
ap
r20
10
22
jul2
01
02
1o
ct2
01
01
4ja
n2
01
11
4a
pr2
01
10
8se
p2
01
13
0n
ov2
01
10
1m
ar2
01
21
4a
pr2
01
22
0ju
l20
12
06
de
c20
12
04
ap
r20
13
26
jul2
01
30
8n
ov2
01
30
3m
ar2
01
42
3m
ay2
01
42
0ju
n2
01
42
3fe
b2
01
52
4a
pr2
01
51
8d
ec2
01
50
8a
pr2
01
61
5ju
l20
16
160
180
200
220
240
260
280
Wei
ght (
lbs)
80 lb weight gain over4 years
Sometimes getting ‘healthy’ has its consequences
23
no
v20
09
08
de
c20
09
05
ap
r20
10
22
jul2
01
02
1o
ct2
01
01
4ja
n2
01
11
4a
pr2
01
10
8se
p2
01
13
0n
ov2
01
10
1m
ar2
01
21
4a
pr2
01
22
0ju
l20
12
06
de
c20
12
04
ap
r20
13
26
jul2
01
30
8n
ov2
01
30
3m
ar2
01
42
3m
ay2
01
42
0ju
n2
01
42
3fe
b2
01
52
4a
pr2
01
51
8d
ec2
01
50
8a
pr2
01
61
5ju
l20
16
160
180
200
220
240
260
280
6
8
10
12
14
16
18
We
ight
(lb
s) HbA
1c
Metformin
Lantus+Metformin
Lantus+Aspart
Lost insurance
Case 2: S.B.
Activity
Walks daily
Uses gym (YMCA) a few times per week

11
What about activity? DHHS guidelines for activity (2008)
For “substantial” health benefits: 150 minutes (2 hours and 30 minutes) per week
of moderate intensity aerobic exercise (i.e. brisk walking, general gardening, “doubles” tennis) OR
75 minutes (1 hour and 15 minutes) per week of vigorous-intensity aerobic exercise (jogging/running, swimming laps, hiking uphill, aerobic dancing) , or equivalent combination of moderate and vigorous activity
All adults should moderate or high intensity muscle training 2 or more times per week
How many of you in this room exercise this much?
“Substantial health benefits:” 2 hours 30 minutes of moderate-intensity, or 1 hour 15 minutes of vigorous intensity exercise + strength training at least 2 times per week
A) Yes
B) No
0A B
What about shorter periods of exercise?
25 sedentary men randomized to 12 weeks of exercise 3 times per week:- Current activity- 50 minute bicycle
(moderate intensity, MICT)- Sprint interval training (SIT)
(2 minute bike warm-up then 20 sec “sprint”, repeated 3 total times (10 minutes total))
Gillen et al PLoS One 2016
Peak oxygen intake
Insulin sensitivity
Would you recommend a Fitbit™ or other activity tracker?
A) YesB) No
0A B

12
Randomized trial of 471 participants, 77% women aged 18-35, 30% non-white Standard intervention: Self monitoring of diet/exercise
Enhanced: Wearable device to monitor diet/exercise
Results: Standard intervention had Greater weight loss (2.4 kg) over 24 months
Conclusion: Devices that monitor/provide feedback on physical activity may not offer an advantage over standard behavioral weight loss approaches.
Jakicic et al JAMA 2016
Back to case 1: C.C.
Early this year – partner of 30 years passed away from pancreatic CA Significant grief, anxiety from this loss Began drinking heavily
Feels like his quality of life was poor to begin with but has only gotten worse since the death of his partner
Van der Kolk et al. Clin Infect Dis. 2010;50:255-263
Poor health-related quality of life associated with reduced survival in HIV patients
Smoking cessation and HRQoL
Taylor et al BMJ 2014: Smoking cessation associated with reduced depression, anxiety, stress, and QOL.

13
Case 1: C.C.
Began walking daily for up to 3-4 hours (from Tenderloin to ocean and back)
Started talking to me about meditation and asking me if I have suggestions on “decalcifying his pineal gland”.
Evidence for meditation?
JAMA Intern Med. 2014;174(3):357-368.
Meditation: Positive impact on anxiety, depression, pain, and mental health-related quality of life.
What about meditation?
Mindfullness on 60 minutes
UCSF offers Mindfulness-based stress reduction program

14
Summary: Life expectancy and wellness in HIV
Mind the (life expectancy) gap! HIV in 2016 Gap narrowing but persists Smoking, Late ART initiation, ETOH/drugs, other co-
morbid conditions (hepatitis, obesity)
For smoking cessation Abrupt quitting may be more successful than gradual
quitting
Varenicline is safe and effective in patients with psychiatric conditions
Evidence gap remains on e-cigarettes
Summary: Life expectancy and wellness in HIV
Exercise May not need so much activity: Consider short interval training
Exercise trackers not quite ready for primetime
Mind the (quality of life) gap! Anxiety, depression, social isolation drive this gap
Consider mindfulness/meditation as an approach to improve this
Thanks! Extra Slides