Diagnosis and Repair 2 nd degree tears and episiotomy.
55
Diagnosis and Repair 2 nd degree tears and episiotomy
-
Upload
anissa-allen -
Category
Documents
-
view
222 -
download
0
Transcript of Diagnosis and Repair 2 nd degree tears and episiotomy.

Diagnosis and Repair2nd degree tears and episiotomy

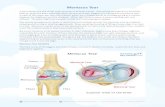
Perineal trauma
Episiotomy Spontaneous tears
Tears not involving anal sphincter
Tears involving anal sphincter
SecondFirst FourthThird

Classification of Trauma Classification of Trauma Classification of Trauma Classification of Trauma
First degree involving skin only
Second degree involving Second degree involving the perineal muscles – the perineal muscles – bulbocavernosusbulbocavernosus transverse perineal transverse perineal if very deep may involve if very deep may involve
pubococcygeus pubococcygeus but not the sphincter complexbut not the sphincter complex

EpisiotomyEpisiotomyEpisiotomyEpisiotomy
RML RML episiotomyepisiotomy Midline Midline
episiotomyepisiotomy
“A surgical incision made intentionally to increase the diameter of the vulval outlet to facilitate delivery”

Episiotomy
When routine -v- restrictiveHow midline -v- mediolateral

Routine versus restrictiveCarroli & Belizan. Cochrane library, Issue 3, 2004.
Routine versus Restrictive (6 studies)Routine versus Restrictive (6 studies)
After restrictive use:Less posterior perineal traumaLess suturingFewer healing complicationsMore anterior perineal trauma

Indications for episiotomy
Minimise multiple & extensive tearsThick & inelastic perineumForceps deliveryMalpresentation & malposition
Expedite deliverySuspected fetal distressShoulder dystocia

Why do we repair perineal trauma?
To control bleedingTo control bleedingTo prevent infectionTo prevent infection If the wound is left unsutured it will heal If the wound is left unsutured it will heal
by secondary intention & healing occurs by secondary intention & healing occurs by the formation of granulation tissue by the formation of granulation tissue which eventually contracts to form scar which eventually contracts to form scar tissuetissue

Perineal haematoma
Before After

Evidence based practice
Which suture material?

Vicryl Rapide Vicryl Rapide vsvs Vicryl Suture Material Vicryl Suture MaterialGemynthe Gemynthe et al et al 1996; McElhinney 1996; McElhinney et al et al 2000; Kettle2000; Kettle et al 2002 et al 2002
3 RCT (n = 2003 women) 3 RCT (n = 2003 women) A more rapidly absorbed synthetic suture A more rapidly absorbed synthetic suture material (Vicryl Rapide™) material (Vicryl Rapide™) versusversus absorbable absorbable synthetic material (Vicryl™) synthetic material (Vicryl™) Significant reduction in pain when ‘walking’ (2 trials)Significant reduction in pain when ‘walking’ (2 trials)Reduction in the need for pain relief (1 trial)Reduction in the need for pain relief (1 trial)Significant reduction in suture removal (3 trials)Significant reduction in suture removal (3 trials)Reduction in superficial dyspareunia (1 trial)Reduction in superficial dyspareunia (1 trial)

Evidence based practice
Which technique?

Repair Techniques Repair Techniques Kettle C, Ismail K 2007Kettle C, Ismail K 2007
Cochrane systematic review - 7 RCT’s (n = 3822) Cochrane systematic review - 7 RCT’s (n = 3822) found that found that continuous subcuticularcontinuous subcuticular stitches stitches compared to compared to interruptedinterrupted is associated with : - is associated with : -
Less short term pain at 10 days Less short term pain at 10 days
Reduction in analgesia use Reduction in analgesia use
No significant difference in dyspareuniaNo significant difference in dyspareunia

Recommended material and technique Recommended material and technique 22ndnd degree tears or episiotomy degree tears or episiotomy
Level 1a evidenceLevel 1a evidence
Vicryl Rapide suture material Vicryl Rapide suture material &&
The continuous non-locking technique The continuous non-locking technique for perineal repair - all layersfor perineal repair - all layers

Prior to commencing the repair
Check extent of perineal trauma – perform per Check extent of perineal trauma – perform per vaginal and per rectal examinationvaginal and per rectal examination
Check equipment - suture pack, materials Check equipment - suture pack, materials If needed ensure that appropriate If needed ensure that appropriate
supervision/support is available prior to supervision/support is available prior to commencing the repaircommencing the repair
Adequate lightingAdequate lighting Ensure that the wound is adequately Ensure that the wound is adequately
anaesthetised (10-20mls Lignocaine 1%) - don’t anaesthetised (10-20mls Lignocaine 1%) - don’t inject local through the skininject local through the skin

Step 1 - suturing the vagina
Identify the apex of the vaginal Identify the apex of the vaginal woundwound
Close the vaginal trauma with Close the vaginal trauma with a loose continuous stitcha loose continuous stitch
Continue to suture the vagina Continue to suture the vagina until the hymenal remnants are until the hymenal remnants are reached and re-approximatedreached and re-approximated
At the fourchette insert the At the fourchette insert the needle through the skin to needle through the skin to emerge in the centre of the emerge in the centre of the perineal traumaperineal trauma

Step 2 - suturing the muscle layer
Check the depth of the Check the depth of the trauma - it may be trauma - it may be necessary to insert two necessary to insert two layers of sutureslayers of sutures
Continue to close the Continue to close the perineal muscle with a perineal muscle with a continuous non-locking continuous non-locking stitch - taking care not stitch - taking care not to leave any dead spaceto leave any dead space

Step 3 - suturing the perineal skin At the inferior end of the wound At the inferior end of the wound
bring the needle out under the bring the needle out under the skin surfaceskin surface
The stitches are placed below The stitches are placed below the skin surface in the the skin surface in the subcutaneous layer - thus subcutaneous layer - thus avoiding the profusion of nerve avoiding the profusion of nerve endingsendings
Continue taking bites of tissue Continue taking bites of tissue from each side of the wound from each side of the wound until the hymenal remnants are until the hymenal remnants are reachedreached
Secure the finished repair with Secure the finished repair with a loop knot tied in the vaginaa loop knot tied in the vagina

Finally
Check the finished repair is anatomically correctCheck the finished repair is anatomically correct No bleedingNo bleeding PV - insert two fingersPV - insert two fingers PRPR Check swabs & instrumentsCheck swabs & instruments Complete documentationComplete documentation

Rationale – continuous techniqueRationale – continuous technique
No knots – sutures accommodate themselves to No knots – sutures accommodate themselves to swelling as it occursswelling as it occurs
Tight sutures cause pain especially if the wound Tight sutures cause pain especially if the wound becomes oedematous - may cause tissue hypoxia becomes oedematous - may cause tissue hypoxia and delay healingand delay healing
Deep & superficial muscles closed in one layerDeep & superficial muscles closed in one layer Skin sutures inserted into subcutaneous layer thus Skin sutures inserted into subcutaneous layer thus
avoiding nerve endings in skin surface – less painavoiding nerve endings in skin surface – less pain Economical – single suture usedEconomical – single suture used

Risk factors for anal sphincter injuries
birth weight over 4 kg (up to 2%) ● persistent occipitoposterior position (up to 3%) ● nulliparity (up to 4%) ● induction of labour (up to 2%) ● epidural analgesia (up to 2%) ● second stage longer than 1 hour (up to 4%) ● shoulder dystocia (up to 4%) ● midline episiotomy (up to 3%) ● forceps delivery (up to 7%)

Guidelines
Clinicians need to be aware of the risk factors for obstetric anal sphincter injury but also recognise that known risk factors do not readily allow its prediction or prevention.
Where episiotomy is indicated, the mediolateral technique is recommended, with careful attention to the angle -60 degree- cut away from the midline.

Anal Sphincter Rupture - ClassificationSultan AH, Clinical Risk 1999;5:193-6
RCOG GreenTop Guidelines 2001; ICI 2002
1st degree = vaginal epithelium
2nd degree = perineal muscles
3rd degree = anal sphincter
3a = <50% external sphincter thickness
3b = > 50% external sphincter thickness
3c = internal sphincter torn
4th degree = anal epithelium torn
+
+
+

Anal Sphincter Rupture - ClassificationSultan AH, Clinical Risk 1999;5:193-6
RCOG GreenTop Guidelines 2001; ICI 2002

If there is any doubt about the grade of third-degree tear, it is advisable to classify it to the higherdegree rather than lower degree.

When repair of the EAS muscle is being performed, either monofilament sutures such as polydiaxanone (PDS) or modern braided sutures such as polyglactin (Vicryl®) can be used with equivalent outcome.
When repair of the IAS muscle is being performed, fine suture size such as 3-0 PDS and 2-0 Vicryl may cause less irritation and discomfort.

Internal sphincter defectsMahony R et al 2007
500 consecutive OASIS Persistent internal sphincter defects
independently associated with an severe anal incontinence
OR 5.1 (95% CI = 1.5 – 22.9)

Diagnosis
History Examination Special Investigation

Obstetric Anal Sphincter InjurieSOASIS
History
Vaginal delivery
- undiagnosed
- suboptimal repair

Identification of EAS



End-to-end primary anal sphincter repair

Primary end-to-end sphincter repair

I



Faecal incontinence
0
20
40
60
80
100
6 weeks 3 months 6 months 12 months
Overlap
End to endp=0.01p=0.01
% Patients
Overlap vs end-to-end n = 64Overlap vs end-to-end n = 64
Fernando R et al 2006

Suture materials Sultan AH, Thakar R 2002
Anal Mucosa - interrupted 3-0 Vicryl with knot in anal canal
Internal Anal Sphincter - Mattress end-to-end 3-0 PDS/ Vicryl 2-0
External Anal Sphincter- Mattress/Overlap 3-0 PDS/ Vicryl 2-0

Principles of the overlap repair Sultan AH et al 1999
Operating theatre Lighting and equipment Regional or general anaesthesia Antibiotics Augmentin or ceph & met. Monofilament sutures PDS but can use Vicryl Foleys catheter Laxatives Lactulose

Recommended Practice Thakar R, Sultan AH 2003
Rectal examination after every delivery Adopt the new classification OASIS repair by experienced doctor in theatre Regional or GA External sphincter - end-to-end or overlap repair Repair torn internal sphincter - 3-0 PDS or Vicryl 2-0 Lactulose 15mls bd for 2 week Antibiotics Ensure bowels opened Follow-up @ hospital by a senior obstetrician

Post natal review
All women should be offered physiotherapy and pelvic-floor exercises for 6–12 weeks after obstetric anal sphincter repair.
All women who have had obstetric anal sphincter repair should be reviewed 6–12 weeks postpartum by a consultant obstetrician and gynaecologist.

When to refer?
If a woman is experiencing incontinence or pain at follow-up, referral to a specialist gynaecologist or colorectal surgeon for endoanal ultrasonography and anorectal manometry should be considered.
A small number of women may require referral to a colorectal surgeon for consideration of secondary sphincter repair.

Post delivery counseling
Women should be advised that the prognosis following EAS repair is good, with 60–80% asymptomatic at 12 months.
Most women who remain symptomatic describe incontinence of flatus or faecal urgency

Counseling Post delivery
All women who sustained an obstetric anal sphincter injury in a previous pregnancy should be counselled about the risk of developing anal incontinence or worsening symptoms with subsequent vaginal delivery.
All women who sustained an obstetric anal sphincter injury in a previous pregnancy should be advised that there is no evidence to support the role of prophylactic episiotomy in subsequent pregnancies.
All women who have sustained an obstetric anal sphincter injury in a previous pregnancy and who are symptomatic or have abnormal endoanal ultrasonography and/or manometry
should have the option of elective caesarean birth.

Documentation and Information
When third- and fourth-degree repairs are performed, it is essential to ensure that the anatomical structures involved, method of repair and suture materials used are clearly documented and that instruments, sharps and swabs are accounted for.
The woman should be fully informed about the nature of her injury and the benefits to her of follow-up. This should include written information where possible.

Thank You


Episiotomy: midline -v- mediolateralCoats et al 1980
Randomised 407 primiparae
Incidence of OASIS
• midline = 12%
• mediolateral = 2%

Benefits of midline episiotomy blood loss Easier to recognise 3o tear Easier to repair Better anatomical result pain risk of infection dyspareunia
Disadvantage of midline episiotomy 30 and 40 tears

Vagina
Anal canal
Episiotomya
c
αb
Angle of episiotomyAndrews et al 2005

EpisiotomyAndrews et al BJOG 2004 Andrews et al Birth 2006
254 primipsNo midwife and only 13 (22%) doctors
performed a truly mediolateral episiotomy (between 40 to 60 degrees from the midline)
Episiotomies angled closer to the midline significantly associated with OASIS (26 vs 37 degrees)

EpisiotomyEogan et al BJOG 2006
Case-control study (54 versus 46 controls)Mean angle of episiotomy smaller (30%
versus 38% p<0.001)50% risk reduction for every 6°from
midlineThe relationship of episiotomy angle with
risk of OASIS was sig (p<0.001)

Training Sultan et al J Obstet Gynaecol 1995
Interviewed 75 doctors and 75 midwives
Less than 20% of doctors and 50% of midwives were satisfied that they had a good level of training at the time of repairing their first episiotomy unsupervised

ConclusionConclusion
It is imperative that women receive high quality It is imperative that women receive high quality evidenced based care wherever childbirth takes evidenced based care wherever childbirth takes placeplace
Practices that reduce the adverse effects of Practices that reduce the adverse effects of perineal trauma and make vaginal birth more perineal trauma and make vaginal birth more desirable are to be encourageddesirable are to be encouraged
Improved perineal care may decrease the Improved perineal care may decrease the escalating interest in caesarean section as an escalating interest in caesarean section as an alternative mode of deliveryalternative mode of delivery