Introduction, kala azar situation and outline of kala-azar in bangladesh dr shahjada selim
Upload
shahjada-selimCategory
view
275download
3
Diabetic Neuropathy
Dr Shahjada SelimAssistant Professor
Department of Endocrinology
Bangabandhu Sheikh Mujib Medical University
Dhaka, Bangladesh
Global Situation Prevalence: 22.7% T1DM, 32.1% T2DM USA: 17% of costs of treating diabetic
complications (approx $300 per patient per year)
UK: £13 million p.a on diabetic foot complications
1. Young MJ, Boulton AJ, MacLeod AF, Williams DR, Sonksen PH. Diabetologia 1993;36(2):150-4.
2. Caro, J. J., A. J. Ward, et al. (2002). Diabetes Care 25(3): 476-81.
HISTORY• 1864-Marchal de calve -DM affects nervous sys
• 1890-Buzzard -motor weakness
• 1893-Leyden -classification
• 1936-Jordan -autonomic neuropathy
• 1947-1973 Pirart -25 yr prospective study
• Dyck & co -Rochester diabetic neuropathy study

Pathology
Axonal loss, focal demyelination & regeneration
↓ conduction velocity and ↑ sensory thresholds

www.plymouthdiabetes.org.uk/
Pathophysiology-biochemical and vascular factors
Risk Factors
Glycaemic control-DCCT ↑ with age: 5% 20-29 years, 44.2% 70-79
years > 50% T2DM >60 years of age ↑ with duration of diabetes: 20.8% < 5years,
36.8%>10 years ↑ Smoking ↑ Microalbuminuria ↑Height ? Nutritional factors

Presentations
3 types of neuropathy:
1. Progress steadily with increasing duration of diabetes and associated with other diabetic complications-common
2. Acute onset with resolution over period of months-rare
3. Pressure palsies

Presentations
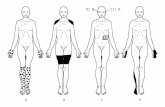
Diffuse symmetrical sensorimotor polyneuropathy
Predominantly sensory Predominantly feet ↓ pain and temperature sensation Parasthesiae and numbness Neurogenic pain/allodynia Neuropathic oedema Wasting occurs only if severe

Diffuse symmetrical sensorimotor polyneuropathy
Problems: Pain and oedema Diabetic foot ulceration
Present in 80% of foot ulcers Principle cause in 39% of ulcers Partly responsible in 36% of ulcers

www.plymouthdiabetes.org.uk/

www.plymouthdiabetes.org.uk/

Autonomic Neuropathy Closely associated with sensorimotor
neuropathy Signs are common if looked for (40%
subjects have abnormal CVS tests) but symptoms are rare (<1%)
Affects the response to hypos but not awareness
If symptoms: mortality=30-50% over 10 years

www.plymouthdiabetes.org.uk/

Diffuse Small Fibre Neuropathy
T1DM Young, ♀ > ♂ Selective damage to small nerve fibres Pain and temp lost but LT retained Symptomatic autonomic neuropathy,
Charcot arthropathy and foot ulcers ? autoimmune

www.plymouthdiabetes.org.uk/
Mononeuropathies
Acute ? Secondary to ischaemia Pain and weakness (severe) Resolve over months
Amyotrophy (Older > )♂ ♀ 3rd nerve 6th nerve Truncal radiculopathies

Diabetic Amyotrophy

www.plymouthdiabetes.org.uk/
Insulin Neuritis
Acute & diffuse May be painful Follows improvement of blood
glucose control ?steal phenomenon
Acute diffuse painful neuropathy Not related to duration of diabetes or
complications Association with marked weight loss severe burning/shooting pain, “electric
shocks”, allodynia Resolve spontaneously, usually with weight
gain, 6-8 months. Some 2 years. Does not relapse Signs may be lacking and dissociated from
symptoms

www.plymouthdiabetes.org.uk/

Pressure Palsies
↑ susceptibility to pressure damage
Limited joint mobility (soft tissue)
Carpal tunnel Ulnar nerve Lateral popliteal nerve
DiagnosisAnnual review Enquire annually for:· Painful neuropathy· Loss of sensation· Erectile impotence Note duration of DM, treatment,
complications & weight Ask about other manifestations of
autonomic neuropathy if:· Other complications are present· Anaesthesia is contemplated· Blood glucose control is erratic

DiagnosisExamine: For evidence of peripheral neuropathy
annually LT
OR if new symptoms Vibration LT ?Thermal thresholds ?Pain For postural hypotension if symptoms
of autonomic neuropathy

Examination-ANS
Ewing’s batteryAbnormal results common Valsalva-expiration for 15 secs against 40
mmHg. Rest 1 min then repeatx2. Avoid in proliferative retinopathy. RR max : RR min>1.21 =Normal, <1.20 = abnormal.
HR increase on standing RR 30:15 ratio > 1.04 HR↑ at max overshoot or 15 seconds ≥ 15bpm
(abnormal if<12)

Ewing’s battery
HR variation during deep breathing (6 breaths per minute) Max-min > 15bpm (<10 is abnormal)
Postural BP-2 mins after standing Fall< 10mmHg normal >30 mmHg abnormal

Diagnosis
Consider differential diagnoses HSMN Ethanol B12/folate Malignancy Renal failure Drugs AI disease Cord problems Leprosy

Prevention
Control DCCT (1995)
Tight control-3% neuropathy at 5 years Conventional-10%
UKPDS (1998) Tight control (HbA1c 7%)-31.2% neuropathy
at 15 years Conventional (HbA1c 7.9%)-51.7% P=0.005 No protective effect seen for BP control

Prevention
Aldose reductase inhibitors Gamma Linoleic Acid Vasodilators-ACE? AGE inhibitors Antioxidants NGFs ? Smoking cessation, ? BP reduction
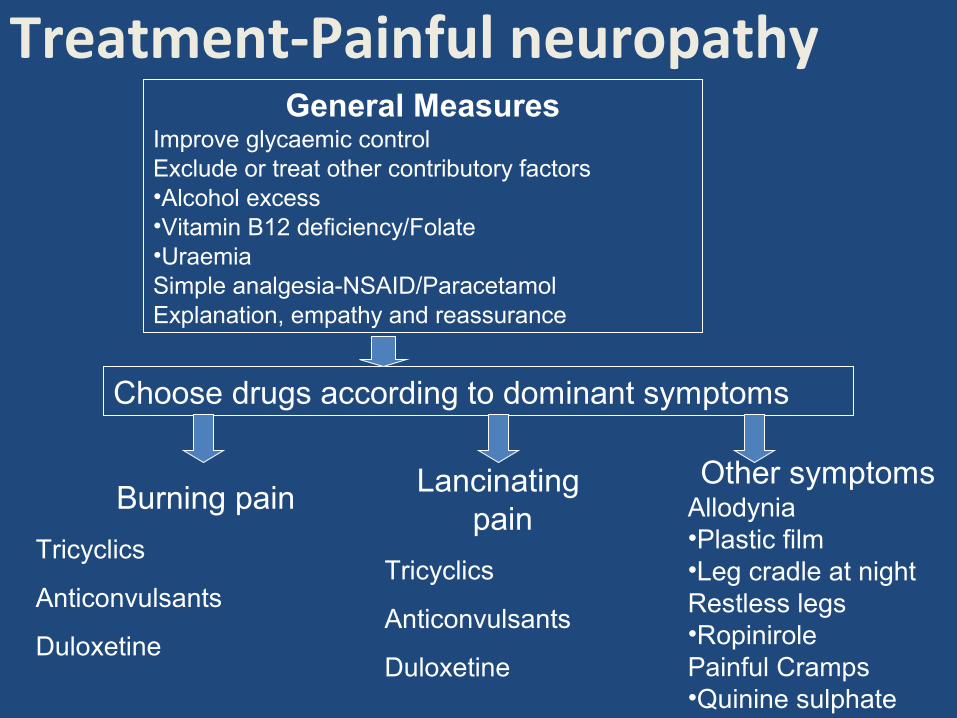
Treatment-Painful neuropathyGeneral Measures
Improve glycaemic controlExclude or treat other contributory factors•Alcohol excess•Vitamin B12 deficiency/Folate•UraemiaSimple analgesia-NSAID/ParacetamolExplanation, empathy and reassurance
Choose drugs according to dominant symptoms
Burning pain
Tricyclics
Anticonvulsants
Duloxetine
Lancinating pain
Tricyclics
Anticonvulsants
Duloxetine
Other symptomsAllodynia•Plastic film•Leg cradle at nightRestless legs•RopinirolePainful Cramps•Quinine sulphate
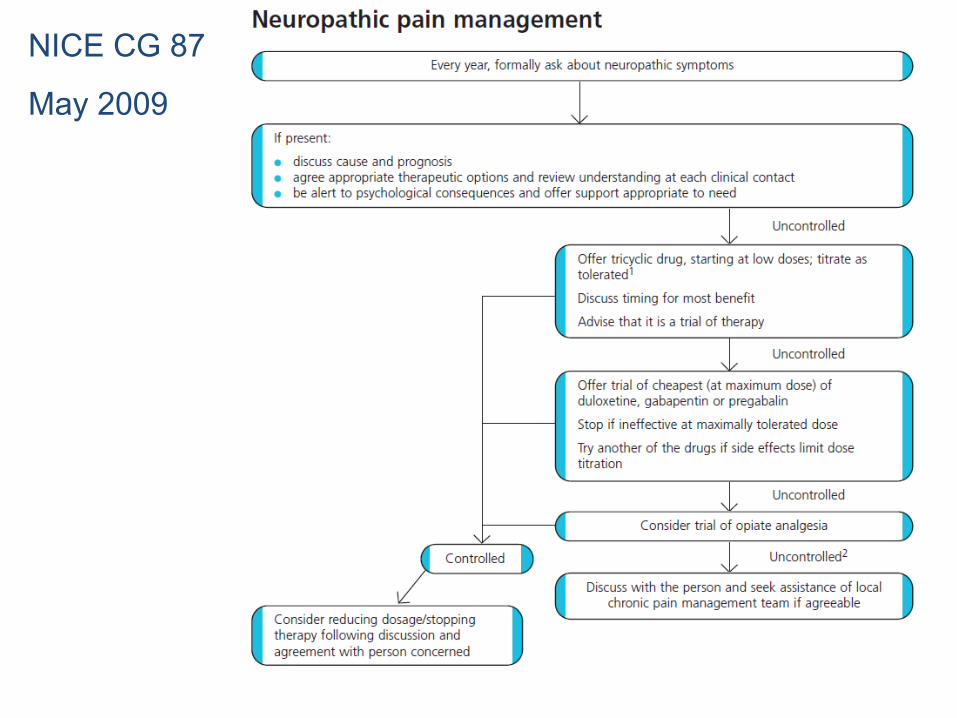
NICE CG 87
May 2009

Treatment -ANS
Postural hypotension Fludrocortisone NSAIDs Compression stockings Elevate the head of the bed
Treatment -ANS
Bladder Manual SP pressure ISC ? Anticholinesterase Cyclical antibiotics if recurrent infections
Sweating ?clonidine
Erectile dysfunction

Treatment -ANS
Gastroparesis Improve glycaemic control Prokinetic drugs
Metoclopramide, domperidone, cisapride, erythromycin (250 mg tds) Octreotide? If severe→admit for IV fluids, IV drugs ± NG tube ± IV/jejunal
feedingDiarrhoea Codeine/loperamide/diphenoxylate Clonidine or octreotide Treat bacterial overgrowth (oxytet/erythromycin) if
suspected/present