Diabetes Mellitus Zhao XiaoJuan Department of Endocrinology The First Hospital of China Medical...
68
Diabetes Diabetes Mellitus Mellitus Zhao XiaoJuan Zhao XiaoJuan Department of Endocrinology Department of Endocrinology The First Hospital of China Medical The First Hospital of China Medical University University 2007.10.23 2007.10.23
-
Upload
imogen-page -
Category
Documents
-
view
214 -
download
0
Transcript of Diabetes Mellitus Zhao XiaoJuan Department of Endocrinology The First Hospital of China Medical...

Diabetes MellitusDiabetes Mellitus
Zhao XiaoJuanZhao XiaoJuan
Department of EndocrinologyDepartment of Endocrinology
The First Hospital of China Medical UniversityThe First Hospital of China Medical University
2007.10.232007.10.23

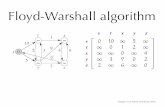
Adapted from Zimmet P et al. Diabet Med. 2003;20:693-702.
25.039.759%
25.039.759%
10.419.788%
10.419.788%
38.244.216%
38.244.216%
1.11.7
59%
1.11.7
59%
13.626.998%
13.626.998%
81.8 156.191%
81.8 156.191%
18.2 35.997%
18.2 35.997%
Prevalence of Diabetes MellitusPrevalence of Diabetes Mellitus
million
2007 : 246 000 000 2025 : 380 000 000
2003 : 189 000 000 2025 : 324 000 000 72%

OutlineOutline
1. Definition
2. Diagnosis
3. Classification
4. Complications
5. Management

1.Definition1.Definition
Diabetes mellitus is characterized by chronic hyperglycemia with disturbances of carbohydrate, fat, and protein metabolism resulting from defects in insulin secretion, insulin action, or both.

1.Definition1.Definition
The chronic hyperglycemia of
diabetes is associated with long-
term damage, dysfunction, and
failure of various organs, especially
the eyes, kidneys, nerves, heart, and
blood vessels.
American Diabetes Association, 2003

OutlineOutline
1. Definition
2. Diagnosis
3. Classification
4. Complications
5. Management

2. Diagnosis2. Diagnosis
Diagnostic Criteria (WHO 1999)
Symptoms of diabetes + Casual plasma glucose
11.1mmol/L ( 200mg/dl) or
Fasting plasma glucose ( FPG ) 7.0mmol/L ( 126mg/dl ) or
2h-Post load plasma glucose(2h-PG)
11.1mmol/L ( 200mg/dl ) If positive, confirm diagnosis with 7days

SymptomsSymptoms
thirst
polyuria
polyphagia
unexplained weight loss
weakness (fatigue)

Criteria for the diagnosis of DMCriteria for the diagnosis of DM
mmol/L (mg/dl)mmol/L (mg/dl) NormalNormal
Impaired Impaired
Fasting Fasting
Glucose (IFG)Glucose (IFG)
Impaired Impaired
Glucose Glucose
Tolerance Tolerance
(IGT)(IGT)
Diabetes Diabetes
MellitusMellitus
(DM)(DM)
Fasting plasma Fasting plasma
glucose (glucose (FPG)FPG) 6.1 6.1 and
7.0
--
7.0
2-Hour postload 2-Hour postload
glucose (glucose (2-hPG)2-hPG) 7.8 -- 7.8 and
11.1
11.1
Random Random plasma plasma
glucoseglucose-- -- 11.1 with
symptoms

Laboratory FindingsLaboratory Findings
1. Blood glucose (FPG and 2-hPG)
2. Urinary glucose
3. Urinary ketone
4. HbA1c and FA (fructosamine)
5. OGTT
6. Insulin / CP releasing test
7. Others (Blood lipid/ UAER/ Immune markers (anti-GAD,ICA,IAA)

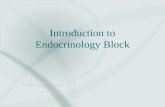
FPG 8-12 mmol/LFPG 12–15 mmol/L
FPG < 8 mmol/L
FPG > 18 mmol/L
normal
T2DM
0.40
1.00
0.80
0.60
insulin
0.20
0
–30 0 30 60 90 120 150 180 210 240
time (min)
nmol/L
Insulin releasing testInsulin releasing test

OutlineOutline
1. Definition
2. Diagnosis
3. Classification
4. Complications
5. Management

3. Classification 3. Classification (1999WHO)(1999WHO)
Type1 diabetes (T1DM)Type1 diabetes (T1DM) Immune mediated
Idiopathic
Type 2 diabetes (T2DM)Type 2 diabetes (T2DM) Other specific typesOther specific types Genetic defects of -cell function
Genetic defects of insulin action Disease of the exocrine pancreas Endocrinopathies Drug - or chemical-induced Infections Anti-insulin receptor antibodies Other genetic syndromes sometimes associated with diabetes
Gestational diabetes mellitus (GDM)Gestational diabetes mellitus (GDM)

3.1 Type 1 diabetes3.1 Type 1 diabetes
β-cell destruction, usually leading to
absolute deficiency
1. Immune-mediated diabetes (Type1A)
Latent autoimmune diabetes in adults, LADA
2. Idiopathic diabetes (Type1B)

AutoantibodiesAutoantibodiesislet cell autoantibody (ICA)
autoantibody to insulin (IAA)
autoantibody to glutamic acid decarboxylase (GADA)
autoantibody to tyrosine phosphatases(IA-2 / IA-2)
Which reflects the autoimmune processes that
have led to -cell destruction

Type 1 DMType 1 DM
Generally <25 years
Rapid onset
Moderate to severe symptoms
Significant weight loss or lean
Ketonuria or keto-acidosis
Low fasting or post-prandial C-peptide
Immune markers (ICA,GADA, IA-2)

3.2 Type 2 diabetes3.2 Type 2 diabetes
Heterogeneous diseases
The most common form of diabetes
Disorders of insulin action and
insulin secretion
Specific etiology is not known

IR – a reduced response of target IR – a reduced response of target tissues to circulating insulintissues to circulating insulin
Glucose
Defective insulin secretion
Excessive fatty acid release
Reduced glucoseuptake
Excessive glucose
production
Carbohydrate
Resistance to the action of insulin
Insulin

3.2.2 3.2.2 -cell dysfunction-cell dysfunction
Reduced ability of -cells to secrete
insulin
Impaired ability of -cells to
compensate for IR
Genetic and environmental
pathophysiology

Features of Type 2 DMFeatures of Type 2 DM
Generally > 40 years
Slowly onset
Not severe symptoms
Obese
Ketoacidosis seldom occur
Nonketotic hyperosmolar syndrome
Normal or elevated C-peptide levels
Genetic predisposition

3.3 3.3 Other specific types of diabetesOther specific types of diabetes
Due to other causes, e.g: Due to other causes, e.g:
genetic defects of -cell function (MODY)
genetic defects of insulin action
disease of the exocrine pancreas
endocrinopathies
drug or chemical induced
others

3.4 3.4 Gestational diabetes mellitus (GDM)Gestational diabetes mellitus (GDM)
GDM is defined as any degree of glucose intolerance with onset or first recognition during pregnancy
6 weeks or more after delivery the woman should be reclassified

Course of diseaseCourse of disease
1. Normal glucose tolerance (NGT)
2. Impaired glucose homeostasis (IGH)
3. Diabetes mellitus (DM)
Impaired fasting glucose (IFG)
Impaired glucose tolerance (IGT)

Clinical stages Clinical stages
NormoglycemiaNormoglycemia
Normal glucose
tolerance
HyperglycemiaHyperglycemia
Impaired Impaired glucose glucose
regulationregulation
IGT / IFGIGT / IFG
Diabetes mellitusDiabetes mellitus
Not insulin Not insulin requiringrequiring
Insulin requiring Insulin requiring for controlfor control
Insulin requiring Insulin requiring for survivalfor survival
StagesStages
TypesTypes
Type 1Type 1
Type 2Type 2
Other Other Specific Specific TypesTypes
GDMGDM

Diabetes MellitusDiabetes Mellitus
Zhao XiaoJuanZhao XiaoJuan
Department of EndocrinologyDepartment of Endocrinology
The First Hospital of China Medical UniversityThe First Hospital of China Medical University
2007.11.12007.11.1

OutlineOutline
1. Definition
2. Diagnosis
3. Classification
4. Complications
5. Management

4. Chronic Complications4. Chronic Complications
Diabeticretinopathy
Diabeticnephropathy
Cardiovasculardisease
Stroke
Diabeticneuropathy
Peripheral vascular disease
Diabetic foot
macrovascularmacrovascularmicrovascularmicrovascular

DM: Impact on patientDM: Impact on patient
Blindness 10%
Loss of reading vision 15%
Amputation 12%
End stage kidney failure 30%
Myocardial infarction 2-4
Excess mortality 2-8

OthersOthers
Hypertension
Abnormalities of lipoprotein metabolism
Periodontal disease

Metabolic syndromeMetabolic syndrome
Abdominal obesity
IGR or DM
Hypertension
Increased triglycerides
Decreased HDL cholesterol
Microalbuminuria

Acute Acute ComplicationsComplications
Acute, life-threatening consequences:
Hyperglycemia with ketoacidosis
Nonketotic hyperosmolar syndrome

ComplicationsComplications
complications
MacrovasculaMacrovascularr
MicrovasculaMicrovascularr
acute chronic Infection
DKA
NHDC CerebrovascularCerebrovascular
CardiovascularCardiovascular
Peripheral VascularPeripheral Vascular
NephropathyNephropathy
RetinopathyRetinopathy
NeuropathyNeuropathy

Diagnosis procedureDiagnosis proceduresymptoms clues &risk factors
FPG / 2h-PG
equivocal raised valuesunder criteria
except DMOGTT NGTNGT
IFG/IGTIFG/IGT
DMDM
classifications
complicationcomplicationss

OutlineOutline
1. Definition
2. Diagnosis
3. Classification
4. Complications
5. Management

5. Management5. Management
1. Education
2. Food planning
3. Physical activity
4. Pharmacological treatment
5. Monitoring

5. 1Education of DM5. 1Education of DM
It is important that all diabetics are educated in self regulation:
The nature of the disorder
Risk of complications.
Individual targets of treatment
food intake, physical activity and drugs
Self-monitoring of blood or urine glucose
How to cope with emergencies such as
hypoglycemia

5.2 5.2 MonitoringMonitoring
Blood glucose levels
- before each meal
- at bedtime
Urine glucose testing
Urine ketone tests (should be performed during illness or when
blood glucose is 11.1mmol/L )

5.3 Food Planning5.3 Food Planning
Weight control
50-60%of the total dietary energy should
come from complex carbohydrates
20-25% from fats and oils
15-20% from protein
Restrict alcohol intake
Restrict salt intake to below 7g/d

5.45.4 Physical ActivityPhysical Activity
Physical activity play an important role
Help weight reductionHelp weight reduction
Improving insulin sensitivityImproving insulin sensitivity
Improving glyceamic controlImproving glyceamic control

5.45.4 Physical ActivityPhysical Activity
Do sparingly: avoid sedentary activities
Do regularly: participate in leisure activities and recreational sports
Do every day: adopt healthy lifestyle habits

5.5 pharmacological therapy 5.5 pharmacological therapy

5.5.1 Insulin5.5.1 Insulin
Indication
Preparation
Therapy
Adverse reaction

5.5.1.1 Indications of insulin5.5.1.1 Indications of insulin
T1DM&GDM
T2DM
Acute metabolic disturbance :NHDC /DKA
Pregnancy and lactation
surgery
Severe diabetics

5.5.1.2 Insulin Preparations5.5.1.2 Insulin PreparationsPreparationsPreparations
HumanHuman AnaloguesAnalogues AnimalAnimal
Ultra-shortUltra-short Lispro Lispro
aspartaspart
ShortShort Novolin RNovolin R
Humulin RHumulin R
R IR I
semilentesemilente
IntermediateIntermediate Novolin NNovolin N
Humulin NHumulin N
NPHNPH
LenteLente
LongLong Novolin ULNovolin UL
Humulin ULHumulin UL
PZIPZI
UltralenteUltralente
Ultra-longUltra-long GlargineGlargine
DetemirDetemir
MixtureMixture Novolin 30RNovolin 30R
Novolin 50RNovolin 50R
Humulin 70/30Humulin 70/30

Time actions of various types of insulinTime actions of various types of insulin
Type Onset of action
Peak effect
Duration of action
Ultra short-acting 1
Short-acting 0.5 2-4 6-8
Intermediate-acting 2-4 8-12 18-24
Long-acting 5-7 16-18 30-36
Ultra long-acting 1-2 - 24
Insulin mixtures Variable actions
page 981 table 7-24-9

Rapid Acting Insulin AnaloguesRapid Acting Insulin Analogues
Insulin Aspart
-Asp(B28)-Insulin
Insulin Lispro
-Lys(B28),Pro(B29)-Insulin

Long Acting Insulin AnaloguesLong Acting Insulin Analogues
Insulin Glargine
-Glycine(A21)+2 arginine(B30)
Insulin Detemir

5.5.1.3 Insulin Therapy5.5.1.3 Insulin Therapy
Breakfas Lunch Dinner Sleep
1 RI RI RI
2 RI+/-NPH +/- RI RI+/- NPH
3 RI RI RI NPH
4 RI+UL RI RI
5 RI+UL RI RI+UL
6 RI RI RI UL

4:004:00 16:0016:00 20:00 20:00 24:0024:00 4:004:00
BreakfastBreakfast LunchLunch DinnerDinner
Ideal Basal/Bolus Insulin Absorption PatternIdeal Basal/Bolus Insulin Absorption Pattern
8:008:0012:0012:008:008:00
TimeTime
Pla
sma
Insu
lin
Pla
sma
Insu
lin

Aspart Aspart – adding an additional injection– adding an additional injection

Continuous Subcutaneous Insulin Infusion Continuous Subcutaneous Insulin Infusion ( CSII)( CSII)

5.5.1.4 5.5.1.4 Problems associated with insulinProblems associated with insulin
Hypoglycemia reaction
Insulin resistance
Somogyi phenomenon
Osmotic lens change (visual
blurring)
Insulin edema

5.5.2 5.5.2 Oral anti-diabetic (OAD) agentsOral anti-diabetic (OAD) agents
1. Sulphonylureas
2. Biguanides
3. -Glucosidase inhibitors
4. Thiazolidinediones
5. Glinides
6. Other

5.5.2.1 SU5.5.2.1 SU
insulin secretagogueinsulin secretagogue
Main action is the stimulation of insulin
secretion from the pancreatic -cells
The first-line drug in type 2 diabetes
patients who are not very obese
Main adverse reaction is hypoglycemia

5.5.2.2Biguanides5.5.2.2Biguanides
insulin sensitizerinsulin sensitizer
Increases insulin sensitivity
Reduced hepatic glucose production
First-line therapy in the obese
Without weight gain and hypoglycemia.
Adverse reactions are gastrointestinal intolerance and lactic acidosis

5.5.2.3 5.5.2.3 -Glucosidase inhibitors-Glucosidase inhibitors
Decrease post-prandial hyperglycemia
Have weight-reducing effect.
First-line therapy with diet, or in
combination with SU, biguanides and
insulin.
Do not cause hypoglycemia

5.5.2.4 5.5.2.4 Thiazolidinediones (TZD)Thiazolidinediones (TZD)
Reduce insulin resistance
Do not enhance insulin production.
Do not cause hypoglycemia.
Conjunction with other antiglycemic agents

5.5.2.5 Glinides5.5.2.5 Glinides
A new generation of SU-like agents
Stimulate first-phase insulin
secretion
May be used as monotherapy
Combination with biguanides or
thiazolidinediones

5.5.2.6 Others5.5.2.6 Others
Lipaglutide (GLP-1 Analogues)

Drug Treatment inDrug Treatment in Type 2 Diabetes Type 2 DiabetesPancreas
LiverMuscle
Impaired insulin secretion
Reduced muscleglucose uptake
TZDMetformin
TZDMetformin
SulphonylureaGlinidesGlinides
Increased hepaticglucose production
Glucosidase inhibitors Metformin
Hyperglycemia
_
stomach intestin
e

Combination therapyCombination therapy
small doses of each drug
avoid the individual side-effects of
each agent

Combination therapy in T2DMCombination therapy in T2DM
SulphonylureasSulphonylureasGlinidesGlinides
-Glucosidase Glucosidase inhibitorsinhibitors
BiguanidesBiguanidesThiazolidinedionesThiazolidinediones
insulin

OAD + basal insulin OAD + multiple daily
insulin injections
OAD monotherapy
OAD combinations OADs
uptitration
7
6
9
8
10
Duration of diabetes
A1C = 7%
OAD = oral anti-diabetic
A1C = 6.5%
Adapted from Del Prato S, et al. Int J Clin Pract 2005; 59:1345-55.
A1C
(%
)Treatment to Target: Aggressive Management of Glycemic Control

ADA 2007
intensive insuln
+ SU
+TZD
+ basal insuln
intensive insuln or basal insuln metformin
TZD*
healthy lifestyle + metformin
+ basalinsuln
+ SU
+ TZD
HbA1C > 7%
HbA1C > 7%
HbA1C > 7%
lifesty
le +
metfo
rmin
+ basal insuln
Diabetes Care 2007 ; 30 ( SUPPLEMENT 1)

The Aims of TreatmentThe Aims of Treatment
Relief of hyperglycemic symptoms
Avoidance of acute metabolic disturbance
Prevent or delay the onset of the long-term complications
In children normal growth and development

Optimal
Fair Poor
Plasma glucose
(mmol/L)
FPG
2-hPG
4.4-6.1
4.4-8.0
7.0
10.0
>7.0
>10.0
HbA1c(%) < 6.5 <6. 5-7.5 >7.5
Blood pressure (mmHg) <130/80 >130/80-
<140/90
>140/90
BMI (kg/m2) Male
female
<25
<24
<27
<26
27
26
Total cholesterol(mmol/L) <4.5 4.5 6.0
HDL- cholesterol(mmol/L) >1.1 1.1-0.9 <0.9
Triglycerides(mmol/L) <1.5 <2.2 2.2
LDL- cholesterol(mmol/L) <3.0 2.5-4.0 >4.0
Targets for control

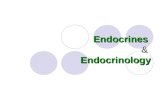
Number of persons
< 50005000–74,00075,000–349,000350,000–1,499,0001,500,000–4,999,000> 5,000,000No data available
Total cases > 370 million adults
WHO. Available at: www.who.int/diabetes/facts/world_figures/en/. Last accessed: January 2005.
Worldwide prevalence of diabetes in 2030 (projected)

Thank youThank you