Development of Novel Immune Interventions for Prostate Cancer
9
Development of Novel Immune Interventions for Prostate Cancer Neeraj Agarwal, 1 Sumanth Padmanabh, 1 Nicholas J. Vogelzang 2 Abstract Prostate cancer is the leading cause of cancer-related morbidity and mortality in men in the Western world. Use of traditional and newer therapeutic regimens is constrained in terms of tolerance, efficacy, and cross-resistance. There is a need for newer therapies without overlapping mechanisms of action and toxicities to improve the outcome. Advances in the field of immunology and cancer biology have led to an improved understanding of the interactions between the immune system and tumors, propelling the field of cancer vaccines to the forefront of clinical investi- gation. Recent US Food and Drug Administration approval of sipuleucel-T, an autologous dendritic cell– based vaccine for the treatment of castration refractory prostate cancer, represents a significant advancement in the field of cancer vaccines. However, the overall survival benefits with sipuleucel-T are modest at best, and the field of cancer vaccine therapy is in a continuous state of evolution and expansion. Further improvements are expected to result from the selection of more appropriate tumor antigens, which circumvent immune tolerance, and from the development of more effective immunization strategies aimed at inducing an effective cytotoxic T-cell response. This review sum- marizes recent developments in the field of immunotherapy in prostate cancer with a focus on dendritic cell vaccines, virus-based vaccines, DNA-based vaccines, cell-based vaccines, peptide-based vaccine and therapies blocking immune checkpoints to break peripheral immune tolerance. Clinical Genitourinary Cancer, Vol. 10, No. 2, 84–92 © 2012 Elsevier Inc. All rights reserved. Keywords: Immune checkpoints blockade, Immunotherapy, Prostate cancer, Vaccine therapy Immune System and Cancer In terms of immunotherapy, the adaptive immune response is of more interest, because it can be instructed and taught to act against foreign antigens vs. self-antigens. The adaptive immune system is composed of the antigen presenting cells (APC) that include den- dritic cells (DC), the most effective APCs, and CD4 and CD8 T cells. 1 CD4 T cells include both T helper cell and regulatory T cell (T REG ) populations. APCs, such as DCs and Langerhans cells, can activate T cells by efficiently processing exogenous as well as endog- enous antigens, and present them to T cells at the plasma membrane through the major histocompatibility complex (MHC) antigen pro- cessing machinery (Figure 1). Stimulation of T cells through T-cell receptors (TCR) alone often results in a nonresponsive state (anergy), which results in the failure of T cells to respond to antigens as well as becoming refractory to restimulation. 2 Costimulation of other cell surface receptors on T cells is required for the avoidance of anergy and optimal T-cell acti- vation. Conversely, the timely activation of negative regulatory sig- nals in T cells is required to prevent an inappropriate immune re- sponse. The inhibitors of TCR signaling include adapter proteins (such as Dok-1 and Dok-2), Cbl proteins (c-Cbl, Cbl-b), serine/threonine kinase, C-terminal src kinase, SH2 domain-containing protein-tyrosine- phosphatase, and feedback inhibitory receptors, such as cytotoxic T- lymphocyte antigen-4 (CTLA-4) and programmed death-1 (PD-1). As a negative feedback, peak expression of inhibitory receptors occurs ap- proximately 24 to 48 hours after stimulation of T cells and is essential for maintaining tolerance for self antigens. 2 Mechanisms of Immune Evasion by Cancer These mechanisms include defective antigen presentation by APCs, an immunosuppressive microenvironment and cytokines, T-cell coinhi- bition, TCR dysfunction, and upregulation of regulatory T cells. 3-5 Defect in Antigen Presentation. Presentation of tumor-associated antigens (TAA) with MHC class I antigen by APCs is a crucial step 1 Division of Medical Oncology, Department of Internal Medicine, Huntsman Cancer Institute, University of Utah, Salt Lake City, UT 2 Developmental Therapeutics, US Oncology Research, Comprehensive Cancer Centers, Las Vegas, NV Submitted: Nov 17, 2011; Revised: Jan 9, 2012; Accepted: Jan 19, 2012; Epub: Mar 10, 2012 Address for correspondence: Nicholas J. Vogelzang, MD, Developmental Therapeutics US Oncology Research, Comprehensive Cancer Centers, 3730 S. Eastern Ave, Las Vegas, NV 89169 Fax: 702-343-4397; e-mail contact: [email protected] Review 84 Clinical Genitourinary Cancer June 2012 1558-7673/$ - see frontmatter © 2012 Elsevier Inc. All rights reserved. doi: 10.1016/j.clgc.2012.01.012
-
Upload
neeraj-agarwal -
Category
Documents
-
view
212 -
download
0
Transcript of Development of Novel Immune Interventions for Prostate Cancer

c(aetc
I
C
Review
84 C
Development of Novel Immune Interventionsfor Prostate Cancer
Neeraj Agarwal,1 Sumanth Padmanabh,1 Nicholas J. Vogelzang2
AbstractProstate cancer is the leading cause of cancer-related morbidity and mortality in men in the Western world. Use oftraditional and newer therapeutic regimens is constrained in terms of tolerance, efficacy, and cross-resistance. Thereis a need for newer therapies without overlapping mechanisms of action and toxicities to improve the outcome.Advances in the field of immunology and cancer biology have led to an improved understanding of the interactionsbetween the immune system and tumors, propelling the field of cancer vaccines to the forefront of clinical investi-gation. Recent US Food and Drug Administration approval of sipuleucel-T, an autologous dendritic cell–basedvaccine for the treatment of castration refractory prostate cancer, represents a significant advancement in the fieldof cancer vaccines. However, the overall survival benefits with sipuleucel-T are modest at best, and the field of cancervaccine therapy is in a continuous state of evolution and expansion. Further improvements are expected to result fromthe selection of more appropriate tumor antigens, which circumvent immune tolerance, and from the development ofmore effective immunization strategies aimed at inducing an effective cytotoxic T-cell response. This review sum-marizes recent developments in the field of immunotherapy in prostate cancer with a focus on dendritic cell vaccines,virus-based vaccines, DNA-based vaccines, cell-based vaccines, peptide-based vaccine and therapies blockingimmune checkpoints to break peripheral immune tolerance.
Clinical Genitourinary Cancer, Vol. 10, No. 2, 84–92 © 2012 Elsevier Inc. All rights reserved.
Keywords: Immune checkpoints blockade, Immunotherapy, Prostate cancer, Vaccine therapyrorcvnsakplapm
Immune System and CancerIn terms of immunotherapy, the adaptive immune response is of
more interest, because it can be instructed and taught to act againstforeign antigens vs. self-antigens. The adaptive immune system iscomposed of the antigen presenting cells (APC) that include den-dritic cells (DC), the most effective APCs, and CD4� and CD8� Tells.1 CD4� T cells include both T helper cell and regulatory T cellTREG) populations. APCs, such as DCs and Langerhans cells, canctivate T cells by efficiently processing exogenous as well as endog-nous antigens, and present them to T cells at the plasma membranehrough the major histocompatibility complex (MHC) antigen pro-essing machinery (Figure 1).
1Division of Medical Oncology, Department of Internal Medicine, Huntsman Cancernstitute, University of Utah, Salt Lake City, UT
2Developmental Therapeutics, US Oncology Research, Comprehensive Cancerenters, Las Vegas, NV
Submitted: Nov 17, 2011; Revised: Jan 9, 2012; Accepted: Jan 19, 2012; Epub: Mar10, 2012
Address for correspondence: Nicholas J. Vogelzang, MD, DevelopmentalTherapeutics US Oncology Research, Comprehensive Cancer Centers, 3730 S.Eastern Ave, Las Vegas, NV 89169
Fax: 702-343-4397; e-mail contact: [email protected]linical Genitourinary Cancer June 2012
Stimulation of T cells through T-cell receptors (TCR) alone oftenesults in a nonresponsive state (anergy), which results in the failuref T cells to respond to antigens as well as becoming refractory toestimulation.2 Costimulation of other cell surface receptors on Tells is required for the avoidance of anergy and optimal T-cell acti-ation. Conversely, the timely activation of negative regulatory sig-als in T cells is required to prevent an inappropriate immune re-ponse. The inhibitors of TCR signaling include adapter proteins (suchs Dok-1 and Dok-2), Cbl proteins (c-Cbl, Cbl-b), serine/threonineinase, C-terminal src kinase, SH2 domain-containing protein-tyrosine-hosphatase, and feedback inhibitory receptors, such as cytotoxic T-
ymphocyte antigen-4 (CTLA-4) and programmed death-1 (PD-1). Asnegative feedback, peak expression of inhibitory receptors occurs ap-roximately 24 to 48 hours after stimulation of T cells and is essential foraintaining tolerance for self antigens.2
Mechanisms of Immune Evasion by CancerThese mechanisms include defective antigen presentation by APCs,
an immunosuppressive microenvironment and cytokines, T-cell coinhi-bition, TCR dysfunction, and upregulation of regulatory T cells.3-5
Defect in Antigen Presentation. Presentation of tumor-associated
antigens (TAA) with MHC class I antigen by APCs is a crucial step1558-7673/$ - see frontmatter © 2012 Elsevier Inc. All rights reserved.doi: 10.1016/j.clgc.2012.01.012

sanM
caenr
n; IL �for pros
for the differentiation and expansion of cytotoxic T cells againstTAAs and the eventual destruction of tumor cells. However, tumorcells can downregulate the expression of MHC class I antigens thatallow them to escape presentation and subsequent recognition byCTLs. The diminished expression of HLA class I antigens have beenreported in several prostate cancer lines, as well as in primary andmetastatic prostate cancer.3,6,7 Other mechanisms that have been de-cribed in this context include loss of ability to express MHC class IIntigens, alterations in the expression profile of MHC antigens andatural killer cell activating and/or acquired expression of nonclassicalHC class I antigens by the cancer cells to escape immune surveillance.8
Immunosuppressive Tumor Microenvironment and Cytokines. Animbalance in the production of proinflammatory (Th1) cytokines withrespect to anti-inflammatory (Th2) cytokines may promote T-cell an-ergy and cancer cell proliferation. Resultant skewing toward the Th2
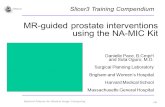
Figure 1 DC-Based Immunotherapeutic Strategies for ProstateT-cell Responses and Emerged as Promising CandidaDCs are Loaded With PCa Associated Antigen-Derivedof HLA-Peptide-Complexes and Costimulatory Molecucells. CD8� CTLs Possess a Profound Capability to RCapacity of DCs to Induce CTLs by the Interaction BeIn Addition, They Provide Help for the Maintenance aEradicate Tumor Cells Directly
tumor peptidetumor proteinRNA coding
for tumor protein
activation
activation
ap
HLA I
HLA II
TCR
B7
B7
CD28
CD28
CD4
CTL
TCR
DC
Abbreviations: CTLs � cytotoxic T cells; DCs � dendritic cells; HLA � human leukocyte antige(Reproduced from Jahnisch H, Fussel S, Kiessling A et al. Dendritic cell-based immunotherapy
response and upregulation of immunosuppressive cytokines, such as in-
terleukin (IL) 4, IL-6, and IL-10 may account for this. Higher levels ofTh2 cytokines have been reported in prostate cancer, when comparedwith normal controls.3,9,10 Furthermore, the tumor microenvironmentan promote upregulation of other immunosuppressive cytokines, suchs tumor necrosis factor, transforming growth factor-beta, and vascularndothelial growth factor. These promote the accumulation of immu-osuppressive, myelo-derived suppressive cells, tumor-associated mac-ophages, or tolerogenic DCs in the tumor microenvironment.4,11,12
Myelo-derived suppressive cells not only promote immunosuppressionbut also tumor growth by stimulating angiogenesis.13
Upregulation of T-Cell Coinhibitory Signals. Coinhibitory signal-ing pathway mediated by PD-1 ligand or B7 homolog 1 (PD-L1/B7-H1) and PD-1 is highly upregulated in prostate cancer tumor infil-trating immune cells.5 More than 90% of CD8� cytotoxic T cellshave been shown to express PD-1 in some patients.14 These CD8� T
er. DCs Display a Unique Capacity to Induce and Maintainor Vaccination Strategies in Prostate Cancer Therapy. Thus,tides, Protein, or RNA. Due to Their High Surface ExpressionCs Efficiently Activate and Expand CD8� CTLs and CD4� T
nize and Destroy Tumor Cells. CD4� T Cells Enhance then CD40 on DCs and CD40 Ligand on Activated CD4� T Cells.pansion of CTLs by Secreting Cytokines and are Able to
activation
DCantigen
presentation
sis
optosis
TU
IFN-γγCD40L-CD40
L-2 CTL
TU
interleukin; IFN � interferon; TCR � T Cell receptor; TU � tumor cells.tate cancer. Clin Dev Immunol 2010:8 [Article ID 517493, doi:10.1155/2010/517493]).
Canctes f
Peples, Decogtweend Ex
opto
ap
I
cells also displayed restricted TCR or TCRV beta gene uses, which
Clinical Genitourinary Cancer June 2012 85

a
f
sb
ft(nc
wimtmsgwtarjfstctGp
8sp
Development of Novel Immune Interventions for Prostate Cancer
86 C
suggests limited tumor infiltration, or expansion of T-cell clones inprostate cancer, associated with upregulated PD-1 expression.5
Other coinhibitory molecules in the B7 family, such as B7x (B7-H4or B7S1) and B7-H3, have also been recognized in the downregula-tion of the immune response against prostate cancer. Upon bindingwith receptors on activated T cells, B7x downregulates T-cell prolif-eration and activation.5,15 Overexpression of B7x and related coin-hibitory ligand B7-H3 also is associated with a higher risk of invasivedisease, metastases, and recurrence in prostate cancer.16,17
Upregulation of Regulatory T Cells. Normally regulatory T cells(TREG) comprise 5% to 10% of the peripheral CD4� T-cell popu-lation.18 The key role of TREG is to inhibit cytotoxic T-cell responsegainst self antigens and maintain tolerance to self antigens.19 TREG
constitutively expresses CD25 (IL-2 receptor alfa chain) on their cellsurface and suppresses CD4� and CD8� effector T cells through therelease of immunosuppressive cytokines, consumption of IL-2, anddirect cell-to-cell contact. An increased number of TREG in periph-eral blood as well as in the tumor infiltrate has been reported inprostate cancer and is associated with reduced survival. Blockade ofTREG (CD4�, CD25� T cells) when using an anti-CD25 monoclo-nal antibody has shown to reduce prostate cancer growth both in aprostate tumor transplant model (TRAMP-C2) and in the sponta-neous prostate tumor model (12T-7s).20
Rationale for Immunotherapy inProstate Cancer
Prostate cancer provides an optimal setting for vaccine-based ther-apies for many reasons.21 First, prostate cancer is a relatively slow-growing cancer, which provides a period of opportunity for immu-notherapy to generate an optimal antitumor immune response.Second, it expresses many TAAs, which can be used for the develop-ment of vaccines. These include prostate-specific antigen (PSA),prostatic acid phosphatase (PAP), prostate-specific membrane anti-gen (PSMA), and prostate stem cell antigen, among others. Third,because of expendable nature of the prostate as an organ, a tissue-specific immune response is well tolerated. Finally, the prostate pro-vides a reliable tumor marker (PSA), which allows the use of immu-notherapy in the presence of minimal residual disease, when theimmunosuppressive effects of the tumor are relatively milder.
Immunotherapeutic Approaches in Prostate CancerTraditionally, cancer immunotherapy has been categorized into pas-
sive immunotherapy, where the immunotherapeutic agent has directantitumor effects, and active immunotherapy, where the immunother-apeutic agent induces a host antitumor immune response. Both activeand passive immunotherapy can further be classified into nonspecifictherapy, where the immunotherapeutic agent induces a generalized up-regulation of the host immune system or specific immunotherapy,where immune activation is targeted toward a specific TAA.22 Severalactive immunotherapy-based approaches (both specific and nonspecific)have been tested in prostate cancer, some of which have advanced tomature stages of clinical development and will be reviewed here.
DC Vaccines. In vitro, mature DCs can be generated by exposingmultipotent CD34� hematopoietic progenitor cells, first to stem cell
actor and FLT3 ligand, and second to granulocyte-monocyte colony rlinical Genitourinary Cancer June 2012
timulating factor (GM-CSF), IL-4 and tumor necrosis factor � ory exposing myeloid progenitor CD14� cells to GM-CSF and IL-4,
which can then be pulsed with the TAA23 with the objective ofenabling them to present both MHC-I– and MHC-II–derived TAAon their cell surface. During this process, DCs can be pulsed withtumor antigens, which are then phagocytosed, processed, and pre-sented by the DCs to the CTLs in the context of MHC machinery.Although a successful and widely used strategy is to use peptides orfusion proteins to pulse DCs in vitro, clinical trials that use messen-ger RNA (mRNA) encoding TAAs to transfect DCs or use tumorlysates to pulse DCs have been reported in prostate cancer.24
Sipuleucel-T (Provenge, APC8015, Dendreon Corp, Seattle,WA) was approved by the US Food and Drug Administration fortreatment of castration-resistant prostate cancer (CRPC) in April,2010, and consists of autologous APCs enriched for a CD54� DCraction harvested by leukophoresis and cultured with a fusion pro-ein (PA2024) composed of PAP and GM-CSF.8,25 In a phase 3 trialthe IMPACT trial) of 512 men with asymptomatic chemotherapyaive metastatic CRPC were randomized in a 2:1 ratio to sipuleu-el-T or placebo.26 The primary and secondary endpoints of the
IMPACT trial were overall survival (OS) and progression-free sur-vival (PFS), respectively. The median OS was significantly improvedin the sipuleucel-T group when compared with the placebo group,with a relative reduction of 22% in the risk of death in the sipuleu-cel-T group (hazard ratio 0.78; P � .03). Notably, the response rate
as minimal, and the time to objective disease progression was sim-lar in the 2 study groups. Thus, OS was improved, without any
easurable antitumor effect, although this may be attributed to theime delay in the translation of immunologic effects to clinicallyeasurable antitumor effects seen with immunotherapy, which re-
ulted in initial progression followed by delayed reduction of tumorrowth. Antibody response against the immunizing antigen PA2024as observed in 66% of patients in the sipuleucel-T group and 3% in
he placebo group. It is interesting to note that, although both T cellnd antibody responses to sipuleucel-T were observed, only antibodyesponses were associated with an extension of survival.26 The ma-ority of adverse events were mild to moderate and included chills,ever, fatigue, nausea, and headache. Notably, the survival benefit ofipuleucel-T was observed consistently across the subgroup of pa-ients, including those with adverse prognostic factors, such as in-reased levels of PSA, lactate dehydrogenase, and alkaline phospha-ase as well as an increased number of bone metastases, increasedleason score, decreased performance status, and the presence ofain. Two smaller randomized trials reported similar results.27 Sev-
eral other trials of sipuleucel-T are underway or have been completedin various settings of prostate cancer. In a recently reported phase 2trial, 176 patients with nonmetastatic prostate cancer with biochem-ical recurrence after radical prostatectomy received 3 to 4 months ofandrogen deprivation therapy (ADT) and were then randomized(2:1) to receive sipuleucel-T (n � 117) or control (n � 59), in adouble-blind fashion.28 The control consisted of APCs held at 2°C-°C, without the addition of PA2024. In the 2 arms, there was noignificant difference in time to biochemical failure, the primary end-oint, defined as serum PSA � 3.0 ng/mL. However, patients who
eceived sipuleucel-T had a 48% increase in PSA doubling time after
s
Neeraj Agarwal et al
Table 1 Selected Trials of Sipuleucel-T and Prostvac-VF in Prostate Cancer
Study(No. Patients) Treatment Eligibility Design Endpoints Results
Small et al66 (127)Three infusions of
sipuleucel-T or placeboevery 2 wk
Asymptomatic metastaticCRPC
2:1 randomization; phase III;crossover to the vaccine was
allowed; for patients onplacebo upon disease
progression
Primary: TTP;secondary: OS
No significant difference inthe TTP; OS was
significantly improved in thesipuleucel-T arm (25.9 vs.
21.4 mo; P �.01)
Kantoff et al26 (512) Sipuleucel-T or placebo Asymptomatic chemo-naive; metastatic CRPC 2:1 randomized; phase III
Primary: OS;secondary, the time to
objective diseaseprogression
OS was significantimproved in the sipuleucel-T arm (unadjusted hazard
ratio for death in thesipuleucel-T group, 0.77;P � .02); no difference in
the time to objectivedisease progression
Beer et al28 (176) Sipuleucel-T or placeboNonmetastatic prostatecancer with biochemical
recurrence2:1 randomized phase II
Primary: time tobiochemical failure, ie,
PSA � 3 ng/mL;secondary: distantfailure, and survival
No difference in primaryendpoint; patients being
followed-up for secondaryendpoints
Clinical Trial Identifier:NCT0071510429 (40) Sipuleucel-T
Localized prostate cancerbefore surgery
(neoadjuvant setting)Open label, phase II
Primary: to assess theimmune response
within prostate tissueafter neoadjuvant
treatment withsipuleucel-T
Ongoing
Clinical Trial Identifier:NCT0143139131 (60) Sipuleucel-T
Nonmetastatic prostatecancer with biochemical
recurrenceOpen label, phase II
Primary: change inimmune response toPA2024; secondary:
safety, change inimmune response,
PSA response
Ongoing
Kaufman et al67 (64)
1 of 3 treatment arms: 4rF-PSA vaccines (arm A),
3 rF-PSA vaccinesfollowed by a single rV-PSA vaccine (arm B), ora single rV-PSA vaccine
followed by 3 rF-PSAvaccinations (arm C).
Biochemical recurrenceafter local therapy for
prostate cancer
Randomized to one of the 3arms, phase II
PSA response at 6 moand immunemonitoring
(measurements ofanti-PSA and anti-
vaccinia antibody titersand PSA-specific T-cell
responses)
Well tolerated; no objectivePSA responses (45.3% of
men had stable PSA at19.1 mo and 78.1%
demonstrated clinical PFS);no anti-PSA antibody
response, but 46% had anincrease in PSA-specific
T-cell response (byELISPOT assay)
Madan et al68 (42)
Primary vaccination with2 admixed recombinantvaccinia-based vaccines
(1 that contains thetransgenes for PSA and
the other for B7-1)followed by a monthlyboost of a recombinant
fowlpox-based PSAvaccine or nilutamide
Nonmetastatic castrationrefractory prostate cancer
1:1 randomized phase II;crossover allowed to receiveboth treatment at the time of
PSA progression
OS
No difference; however,there was a trend towardincreased OS in patientswho were randomized to
initially receive vaccine vs.nilutamide (P � .13)
Kantoff et al41 (125)
Prostvac-VF plus GM-CSF or to control empty
vectors plus salinesolution injections
Chemo-naive, minimallysymptomatic metastatic
CRPC2:1 randomized phase II PFS and OS
No difference in PFS;improved OS with Prostvac-
VF (25.1 vs. 16.6 mo;P � .0061)
Clinical Trial Identifier:NCT0132249042 (1200)
Prostvac-VF plus GM-CSF vs. Prostvac-VF plusplacebo vs. placebo plus
placebo
Chemo-naive, minimallysymptomatic metastatic
CRPC
Randomized (to 1 of the 3arms) phase III OS, PFS Ongoing
Abbreviations: chemo-naive � chemotherapy naive; CRPC � castration-resistant prostate cancer; ELISPOT � enzyme-linked immunosorbent spot; GM-CSF � granulocyte-monocyte colonytimulating factor; OS � overall survival; PFS � progression-free survival; PSA � prostate-specific antigen; rF-PSA � fowlpox-PSA; rV-PSA � single vaccinia-PSA; TTP � time to progression.
Clinical Genitourinary Cancer June 2012 87

amlc
pBcporPscabcu
RachnT
tmsi
evavvs
vepcvmcwsb(asnnM(aiadc
w0Hvm4m
Development of Novel Immune Interventions for Prostate Cancer
88 C
testosterone recovery (155 vs. 105 days; P � .038). The patients con-tinue to be followed up for safety and the secondary endpoints of distantfailure and survival.
A neoadjuvant phase 2 study of sipuleucel-T, administered beforeradical prostatectomy in localized prostate cancer, that assessed im-mune response within prostate tissue has completed accrual.29 Aninnovative pilot study is testing the feasibility and immunologic im-pact of sipuleucel-T and low-dose cyclophosphamide with or with-out anti-PD-1 monoclonal Ab (CT-011) in men with CRPC.30 In arandomized phase 2 study, patients with nonmetastatic prostate can-cer with biochemical recurrence will be randomized to ADT beforeor after sipuleucel-T, with a primary objective of assessment of im-mune response in these 2 arms.31 In addition, in a phase 3 trial with
primary endpoint of OS, patients with new androgen-dependentetastatic prostate cancer will receive ADT to achieve castration-
evel testosterone and then will be randomized 1:1 to receive sipuleu-el-T or continue on ADT alone (Table 1).32
Stimulation of CD40 receptors enables DCs to cross-present an-tigen and overcome peripheral T-cell tolerance.33 Drug-inducibleCD40 is a ligand-independent approach to enhance CD40 signalingin DCs. In drug-inducible CD40, CD40 is re-engineered by fusingthe cytoplasmic domain of CD40 to drug-binding domains, whichallows it to respond to the lipid-permeable, high-affinity dimerizerdrug (AP1903) while circumventing ectodomain-dependent nega-tive-feedback mechanisms. An open phase I/II trial for men with upto 1 prior systemic regimen for metastatic CRPC is evaluating theintradermal administration of an autologous DC vaccine (BPX-101)pulsed with PSMA and transduced with inducible human CD40,followed 24 hours later (when DCs are likely to have migrated toregional lymph nodes) by intravenous infusion of AP1903.33 In a
reliminary report on the phase I portion of this trial, treatment withPX-101-was safe, and associated with PSA, and objective responses,ontrary to the growing consensus that cancer vaccine therapy im-roves survival without short-term response.34 Of 12 patients, 2 wentff protocol due to progression, and the remaining 10 achieved a bestesponse of stable disease or better. Notably, 2 patients had significantSA responses (46% and 85%, respectively). Among measurable re-ponses by RECIST (Response Evaluation Criteria In Solid Tumors)riteria, 1 patient after receiving docetaxel experienced partial response,nd 1 patient who was chemotherapy naive with extensive visceral andone metastases experienced a complete response with docetaxel-basedhemotherapy after induction with BPX-101 and AP1903, and had anndetectable PSA at 14 months after enrollment.
Strategies that use treatment with DCs transfected with tumorNA have also been shown to be safe and feasible in prostate cancernd are capable of stimulating the expansion of tumor-specific poly-lonal T cells in immunized patients. Multiple early-phase studiesave shown that vaccines, by using RNA from autologous or alloge-eic tumor cells, to transfect autologous DCs, induced a cytotoxic-cell response, and, in many instances, a PSA response.24,35,36
Vaccines With Viral Vectors. The use of viruses as vehicles to deliverumor antigens into the APCs in vivo is a very promising strategy forany reasons. The inherent immunogenicity of the virus leads to a
trong inflammatory response, directed against the viral protein. This
nflammatory response in turn may lead to an improved immune clinical Genitourinary Cancer June 2012
response against the tumor antigens being expressed by the virusitself.37 Further enhancement is achieved by the high level of genexpression seen with viral vectors. Additional factors in favor of airal-based vaccine include the relative ease to engineer viral vectorsnd their ability to carry a large amount of genetic material. Poxviralectors are used the most in these vaccines. The prototype is theaccinia virus, which has been used worldwide in the eradication ofmallpox.38,39 The poxvirus family is composed of double-stranded
DNA viruses that do not integrate with the host cell genome andinstead replicate within the cytoplasm of infected cells. The hostimmune response to the vaccinia virus leads to strong neutralizingantibody titers, after which a proportion of these undergo cell death.Cellular debris, including the encoded antigen (such as PSA) is thentaken up by infiltrating APCs, which in turn present the antigens tohelper and cytotoxic T cells in a proinflammatory atmosphere. Pox-virus vectors can also induce an immune response by direct infectionof APCs, such as Langerhans cells present in the skin. A major limi-tation of poxvirus-based vectors is the rapid appearance of strongneutralizing antibodies against the vaccinia vector, which renders abooster vaccination when using the same virus (homologous prime/boost vaccination) ineffective, as the antibody response to viral pro-teins dominates over the intended response to encoded antigens(such as PSA),38,40 which can be circumvented by using avipox viralectors encoding the same antigens as the booster vaccination (het-rologous prime/boost vaccination). The avipox virus is a family ofox viruses that infects birds and does not replicate in mammalianells. Because infections with avipox viruses do not produce newirions, the degree of neutralizing antibodies that are generated, afterammalian infection, is quite low, which allows avipox viral parti-
les to persist for a longer period and to express foreign transgenes,hich results in a significantly enhanced T-cell immunity. Further
tudies in the animal models suggested that heterologous prime/oost vaccination schedules expressing 2 different poxvirus vectorsie, vaccinia vector followed by an avipox vector), expressing tumorntigens and costimulatory factors induced stronger immune re-ponses against foreign antigens compared with single-agent immu-ization protocols. An example of heterologous prime/boost vacci-ation strategy is Prostvac-VF (BN Immunotherapeutics Inc,ountain View, CA), which comprises 2 recombinant viral vectors
vaccinia vector and fowlpox vector), each encoding transgenes for PSAnd TRICOM. TRICOM consists of costimulatory molecules, includ-ng ICAM (intercellular adhesion molecules)-1 (CD54), B7.1 (CD80),nd leukocyte function-associated antigen-3 (CD58). Preclinical studiesemonstrated TRICOM to be superior compared with a transgene thatontains only 1 or 2 of the costimulatory molecules.23
In a double-blind randomized phase 2 trial of patients with che-motherapy naive minimally symptomatic metastatic CRPC, 82 pa-tients received Prostvac-VF and 40 received control vectors.41 PFS
as similar in the 2 groups (hazard ratio 0.884 [95% CI, 0.568-1.375]; P � .56), and, originally, the trial was reported as negative.owever, at 3 years after the study, the patients treated with Prost-
ac-VF were found to have significantly improved OS (25.1 vs. 16.6onths; P � .0061), a better 3-year survival (30% vs. 17%), and a
4% reduction in death rate. Based on these encouraging results,ultiple clinical trials have been initiated in various stages of prostate
ancer, including a large phase 3 registrational study (Table 1).42

is
a
a(D(dav
pptdttwP�
(t
ar
p
Dcpow
ttasnm
Neeraj Agarwal et al
DNA-Based Vaccines. DNA-based vaccines are composed of nakedDNA plasmids encoding specific tumor antigens. The primary ad-vantage is the ease and preciseness with which DNA can be synthe-sized to induce an immune response toward selected antigens.38
However, because of the absence of a concurrent inflammatory re-sponse seen with viral vaccines, DNA-based vaccines are poorly im-munogenic. Another disadvantage is the low level of in vivo infectionof APCs by these vaccines.21,38 Several approaches have been devel-oped to circumvent this, including multiple immunizations, simul-taneous administration of cytokines (GM-CSF or IL-2),43 concom-tant use of plasmids encoding nonself-antigens (ie, hepatitis Burface antigen),44 modification of the plasmid encoded antigens,45
and an improved delivery system (gene gun, cationic liposomes).37,46
In a phase 1/2 trial, 22 patients with CRPC and with biochemicalrecurrence only were treated with plasmid DNA encoding PAP at 3different dose levels, along with GM-CSF as a vaccine adjuvant.47
The median serum PSA doubling time increased from 6.5 months inthe pretreatment phase to 8.5 months during treatment (P � .033)nd 9.3 months in the 1-year posttreatment follow-up (P �.054).
mRNA-Based Vaccine. The strategy of using mRNA has severaldvantages over naked plasmid DNA and viral vector based vaccines:a) the nuclear membrane, which is a major obstacle for plasmidNA, is avoided because mRNA exerts its function in the cytoplasm,
b) there is no risk of insertional mutagenesis, (c) there is no need foretermination and use of an efficient promoter, (d) it allows repeatedpplication, (e) there is increased effectiveness of mRNA in nondi-iding cells, and (f) it avoids vector-induced immunogenicity.48
Other advantages are the ease of producing mRNA in large amountswith very high purity and a lack of induction of antibodies.48 Inaddition, the same mRNA molecule can provide an antigen sourcefor adaptive immunity and can simultaneously bind to pattern rec-ognition receptors, thus stimulating innate immunity. Vaccinationwith mRNA can be achieved by several delivery methods: (a) the directinjection of naked mRNA, (b) the injection of mRNA encapsulated inliposomes, (c) the gene gun delivery of mRNA loaded on gold beads, or(d) in vitro transfection of the mRNA in cells, followed by reinjection ofcells (described in the section of DC-based vaccines).48
CV9103 (CureVac GmbH, Tübingen, Germany) is an mRNA-based vaccine that encodes 4 specific prostate antigens (PSA, prostatestem cell antigen, PSMA, and STEAP1), 3 of which are membrane-bound. Preliminary results of a first-in-man phase 1/2 trial ofCV9103 in patients with CRPC and with rising PSA levels wererecently reported.49 CV9103 was safe and well tolerated and dis-
layed an unexpectedly high level of cellular immunogenicity. Of 38atients, in 33 patients where immunomonitoring was possible, an-igen-specific T cells were detected in 26 (79%) of patients indepen-ent of their HLA background. The majority 19 (58%) had induc-ion of T-cell responses against multiple antigens and regardless ofheir cellular localization. Notably, antigen-nonpecific B cells alsoere increased in 24 (74%) patients. Encouraging stabilization ofSA levels after initial rises was seen, with 1 patient experiencing a85% drop in his PSA level.
Peptide-Based Vaccines. Advantages of peptide-based vaccines area) faster and more cost-effective production, storage, and distribu-
ion; (b) the ability to select specific TAA as targets by the vaccine;nd (c) avoidance of self antigens capable of generating autoimmuneesponse.37 Disadvantages are (a) weak immunogenicity of a single
protein or, especially, a single epitope; (b) the possibility of tumorescape from immune recognition through antigen mutation or loss;(c) HLA restricted use (mainly for epitope-based vaccines); (d) lim-itation to a subset of patients (usually HLA-A2�); and (d) the poorability to induce balanced activation of CD4 and CD8 subsets,which is believed to be essential for effective, long-lasting antitumorimmunity.37 Despite these limitations, peptide-based vaccines hold
romise in the treatment of prostate cancer.MKC1106-PP (MannKind Corporation, Paramus, NJ) is a novelNA-based and peptide-based vaccine cotargeting 2 TAAs impli-
ated in cellular differentiation, genetic stability, and angiogenesis:referentially expressed antigen in melanoma (PRAME), a regulatorf the retinoic acid receptor and PSMA, a dihydrofolate reductaseith several other functions.50 PRAME is overexpressed by a variety
of cancers of epithelial, neuroectodermal, and bone marrow origin.PSMA is expressed by the neovasculature in various solid tumors,mediates angiogenesis through integrin regulation, and is substan-tially overexpressed in hormone refractory prostate cancer cell lines.MKC1106-PP, a DNA prime, dual-peptide boost immunizationregimen, comprises a recombinant plasmid (pPRA-PSM encodingfragments derived from both antigens) and 2 peptides (E-PRA andE-PSM derived from PRAME and PSMA, respectively). In a multi-center phase 1 study, 26 patients with metastatic solid tumors progress-ing on standard therapy were treated with MKC1106-PP administeredby intra–lymph node injection in a prime-boost sequence.50 Patientswere required to be positive for human leukocyte antigen-A*0201 andtumor antigen. Treatment was well tolerated, and 15 of 24 evaluablepatients showed an immune response, as defined by the expansion ofPRAME-specific or PSMA-specific T cells in the blood. Although noobjective response was seen by RECIST, 7 patients had stable disease for�6 months, or PSA decline (4 of 10 with prostate cancer), 2 of 2 withrenal clear cell carcinoma, and 1 of 10 with metastatic melanoma. Fur-thermore, induction and persistence of antigen-specific T cells in bloodabove baseline levels correlated with disease control, defined as stabledisease for �6 months.
Tumor-Cell-Based Immunotherapy. Tumor cells themselves arepoorly immunogenic and produce an ineffective immune response.However, tumor cells can be engineered to express proinflammatorycytokines or administered with adjuvants to improve antitumor im-mune response.51 Using the whole cell instead of a specific antigen orpeptide provides the advantage of presentation of a large number oftumor antigens simultaneously with the potential to induce a moregeneralized cytotoxic T-cell response against multiple antigens.38 Al-hough both autologous and allogeneic tumor cells have been used,he advantage of using allogeneic tumor cell lines is their easy avail-bility. This strategy is exemplified by prostate-GVAX (Cell Gene-ys, South San Francisco, CA), which consists of 2 irradiated alloge-eic human prostate cancer cell lines, LNCaP and PC-3, geneticallyodified to secret GM-CSF.37 Unfortunately, two phase 3 trials of
GVAX, VITAL-1, and VITAL-2 were prematurely terminated due tonegative results, which rendered its further development uncertain.52
Blockade of Immune Checkpoints. Many coinhibitory pathways are
known to be present and upregulated in the tumor microinvolvementClinical Genitourinary Cancer June 2012 89

aaasatP
TBiT
patci
ration-r
Development of Novel Immune Interventions for Prostate Cancer
90 C
and are known to attenuate cytotoxic T-cell response against tumorantigens. These include those mediated through CTLA-4, PD-1, B7-H3, or B7x. In addition, blocking the CD25 receptor on T-regulatorycells is another avenue, which can be exploited to downregulate T-reg-ulatory cells (CD4�, CD25�), to optimize cytotoxic T-cell response.
Blockade of CTLA-4 Signaling. Cytotoxic T lymphocyte antigen 4(CTLA-4) is a key negative regulator of T-cell responses, inhibitingrecognition of self antigens by T cells and has the ability to down-regulate the antitumor immune response. Ipilimumab (MDX-010;Bristol-Myers Squibb, NY, USA) and tremelimumab (CP-675206;Pfizer, NY, USA) are fully human, monoclonal antibodies againstCTLA-4.53 Ipilimumab has recently been approved by the US Foodnd Drug Administration after it was shown to improve OS in met-static melanoma. However, CTLA-4 inhibition with ipilimumab isssociated with potentially life-threatening autoimmune phenomenauch as enterocolitis, hypophysitis, and dermatitis.54 Many phase 1nd phase 2 clinical trials have been conducted in patients with pros-ate cancer with ipilimumab with objective clinical responses andSA responses being described (Table 2).55,56 Based on the encour-
aging results of early trials in prostate cancer, two phase 3 clinicaltrials of ipilimumab in CRPC are in progress. Ipilimumab vs. pla-cebo has been initiated in men with castration refractory metastaticprostate cancer, with or without prior exposure to chemotherapy,with results expected in the near future.57,58
Blockade of PD-1/PD-L1 Pathway. Interaction between PD-1 andits ligand PD-L1 (also known as B7-H1) leads to inhibition of T-cellfunction.38 Blockade of this pathway is associated with encouragingantitumor immune response in animal models.59,60 Unlike early le-thality in CTLA-4 knockout mice, PD-1 deficient animals demon-
Table 2 Ipilimumab Trials in Prostate Cancer
Study(No. Patients) Treatment Eligibility
Fong et al69 (24) IPI with GM-CSF (day1-14)
Metastatic, castration-resistantchemo-naive prostate cancer
Small et al70 (14) IPIMetastatic castration refractory
prostate cancer (priorchemotherapy allowed)
Tollefson et al71
(108) IPI with AA or AA alone Unresectable prostate cancer(castration sensitive)
Slovin et al72 (45)
IPI 10 mg/kg q3 wk � 4in 3 groups: (1) IPI alone(n � 16); (2) IPI � XRT(n � 15) chemo- naive,and (3) IPI � XRT (n �
14) chemotherapyexperienced
Metastatic CRPC
Gerritsen et al73
(28)
IPI (escalating doses of0.3, 1, 3 or 5 mg/kg)
with GVAX
Metastatic CRPC (chemo-naive)
Abbreviations: AA � androgen ablation; chemo-naive � chemotherapy naive; CRPC � castipilimumab; PSA � prostate-specific antigen; XRT � radiation therapy.
strate a mild form of late onset strain-specific autoimmunity.14
linical Genitourinary Cancer June 2012
B7-H1 has been shown to be upregulated in a variety of humantumors and is associated with poor clinical outcomes.61 After estab-lishing safety in a phase 1 study of fully human monoclonal antibodytargeting PD-1, MDX-1106 (936,558; Bristol-Myers Squibb), itsfurther development in phase 2 trials have begun. The presence ofPD-1 and PD-L1 in the prostate cancer microenvironment providesa rationale for blockade of the PD-1 pathway.
Depletion of T-Regulatory Cells by Targeting CD25. The physiolog-ical role of T-regulatory cells (CD4�, CD25�) is to inhibit cytotoxic
cells from mounting an immune response against self-antigens.ecause tumor antigens largely comprise self-antigens, TREGs may
nhibit cytotoxic T cells from mounting an immune response againstAAs. Depletion of TREGs by using anti-CD25 antibodies in mice,
improves antitumor immune response.62,63 Furthermore, anti-CD25 therapy improves the therapeutic efficacy of GM-CSF secret-ing B-16 tumor cells in animals.64 Denileukin diftitox is a fusion
rotein that consist of full-length IL-2 fused to the enzymaticallyctive and translocating domain of diphtheria toxin, which allows forhe targeting of CD25 expressing cells. After internalization into theytoplasm of the CD25 expressing cells, diphtheria toxin is releasedntracellularly and leads to inhibition of protein synthesis.4,62 These
data provide the rationale for using denileukin diftitox to depleteT-regulatory cells before vaccine therapy in prostate cancer.
Novel Endpoints in Clinical TrialsEvaluating Immunotherapy
Administration of immunotherapy leads to the following se-quence of biologic events: (1) early immune activation and T-cellproliferation, (2) clinically measurable immune-mediated antitumoreffects over many weeks to months, and (3) potential delayed effect
Design Endpoints Results
1 escalating doses of0.5-3 mg/kg) with ad dose of GM-CSF
Safety3 of 6 patients in the highest dose
cohort (3 mg/kg) experienced a PSAresponse (�50%)
1, IPI given at a fixeddose of 3 mg/kg Safety 2 of 14 showed a PSA response
(�50%)
randomized, phase 2 Safety, PSA andclinical response
Patients treated with ipilimumab � AAwere more likely to have an
undetectable PSA by 3 mo (55% vs.38%)
ndomized phase 3 Safety andefficacy
10 (22%) of 45 patients had PSAresponse (�50%)
e 1; dose escalation12), dose expansion
(n � 16)Safety 6 of 28 patients had a PSA response
(�50%)
esistant prostate cancer; GM-CSF � granulocyte-monocyte colony stimulating factor; IPI �
PhaseIPI (fixe
Phase
1:1
Ra
Phas(n �
on patient survival several months after first administration com-

Rsss
depoese
BubtptmattnvibgmnaiiFtis
Neeraj Agarwal et al
pared with conventional cytotoxic agents.65 Consequently, 3 novelendpoints for immunotherapy trials have been proposed and needprospective validation. First, harmonization of T-cell assays to estab-lish cellular immune response as a reproducible biomarker and itssubsequent correlation with clinical outcomes. Second, applicationof new immune-related response criteria, to more comprehensivelycapture all response patterns. Four distinct response patterns havebeen observed in immunotherapy trials, and all patterns have beenassociated with favorable survival compared with patients with pro-gressive disease by conventional criteria: immediate response, dura-ble stable disease, response after tumor burden increase, and responsein the presence of new lesions. New immune-related response criteriaallows for assessment of overall tumor burden as a continuous variable,when considering index lesions identified at baseline together with newlesions. Each lesion is measured bidimensionally, and the sum of theperpendicular diameters (SPD) of index lesions at baseline is added tothatofnewlesionstocalculatetotal tumorburdenaccordingtothefollowingformula: tumor burden � SPDindex lesion � SPDnew measurable lesion.
esponse categories are defined as (1) immune-related complete re-ponse, ie, disappearance of all lesions, (2) immune-related partial re-ponse, ie, �50% decrease in tumor burden, (3) immune-relatedtable disease, ie, �50% decrease to �25% increase in tumor bur-
den, and (4) immune-related progressive disease, ie, �25% increasein tumor burden.65 Notably, the appearance of new lesions alonedoes not constitute immune-related progressive disease if they do notincrease the tumor burden �25%. A third novel endpoint is the useof modified statistical methodology, such as characterization of thehazard ratios before and after separation of survival curves, for anal-ysis of survival outcomes in the immunotherapy trials. Kaplan-Meiersurvival curves may demonstrate delayed separation due to the extra timetaken by immunologic response to translate into clinically measurableantitumor activity. A substantial number of events can occur during thisdelay and before separation of the curves, thus leading to the loss ofstatistical power when using the conventional statistical models.65
ConclusionThe improvement in the OS with sipuleucel-T has led to its ap-
proval for the treatment of castration refractory metastatic prostatecancer. However, the survival benefit is modest and the need formore-effective immune-based therapies is paramount. Encouragingresults from early-phase immunotherapy-based clinical trials have ledto multiple, ongoing phase 3 trials, such as ipilimumab, which isbeing tested in CRPC. The pox virus–based vaccine therapy is an-other promising strategy and was associated with an OS benefit (ap-proximately 8 months) in a randomized phase 2 trial in CRPC. Theuse of combinatorial regimens, which simultaneously target multiplesteps in the immune system, is expected to optimize the overall effi-cacy, while minimizing component drug toxicities. Use of a DC-based vaccine, along with inhibitors of Tregs (such as denileukin
iftitox) exemplifies this approach. Combination regimens may bespecially applicable for immunologically weaker vaccine ap-roaches, such as DNA, mRNA, or peptide-based vaccines, whichtherwise provide several advantages, including faster and more cost-ffective production, storage, and distribution as well as the ability toelect specific TAA as targets. Androgen deprivation therapy has been
vinced to reverse age-related thymic involution and improve T- and-cell response, and has the potential to improve responses, whensed in conjunction of immunotherapy. In addition, a high tumorurden is immunosuppressive, and cytoreduction before immuno-herapy is known to improve outcomes in the metastatic setting byroviding the rationale for the use of chemotherapy before immuno-herapy. Furthermore, chemotherapeutic drugs, eg, cyclophospha-ide, may downregulate Tregs, independent of their cytotoxic effect
nd improve the efficacy of subsequent immunotherapy. However,he failure of GVAX when used concurrently with docetaxel chemo-herapy will likely remain an impediment to designing future immu-otherapy-based trials, which include chemotherapy. Successful de-elopment and clinical application of immunotherapeutics willncreasingly depend upon identification and validation of efficaciousiomarkers predicting response to such therapies, which is importantiven a plethora of immunotherapeutic drugs currently in develop-ent, exorbitant cost of the approved agents, and the recognition that
ot all but only subsets of patients will benefit most from these novelgents. Although there are no validated predictive biomarkers currentlyn widespread use, several candidate immunologic markers have beendentified to be associated with significantly improved clinical outcomes.urther development and validation of predictive biomarkers will even-ually allow a personalized approach in immunotherapy where compan-on diagnostic tests by using these biomarkers will be used to identifyubsets of patients most likely to respond to these agents.
References1. Iwasaki A, Medzhitov R. Regulation of adaptive immunity by the innate immune
system. Science 2010; 327:291-5.2. Smith-Garvin JE, Koretzky GA, Jordan MS. T cell activation. Annu Rev Immunol
2009; 27:591-619.3. Miller AM, Pisa P. Tumor escape mechanisms in prostate cancer. Cancer Immunol
Immunother 2007; 56:81-7.4. Kusmartsev S, Vieweg J. Enhancing the efficacy of cancer vaccines in urologic
oncology: new directions. Nat Rev Urol 2009; 6:540-9.5. Barach YS, Lee JS, Zang X. T cell coinhibition in prostate cancer: new immune
evasion pathways and emerging therapeutics. Trends Mol Med Oct 21, 2010 [E-pubahead of print].
6. Blades RA, Keating PJ, McWilliam LJ, et al. Loss of HLA class I expression inprostate cancer: implications for immunotherapy. Urology 1995; 46:681-6; discus-sion 686-7.
7. Zhang H, Melamed J, Wei P, et al. Concordant down-regulation of proto-oncogenePML and major histocompatibility antigen HLA class I expression in high-gradeprostate cancer. Cancer Immun 2003; 3:2.
8. Campoli M, Ferrone S. Hla antigen and NK cell activating ligand expression inmalignant cells: a story of loss or acquisition. Semin Immunopathol 2011; 33:321-34.
9. Filella X, Alcover J, Zarco MA, et al. Analysis of type T1 and T2 cytokines inpatients with prostate cancer. Prostate 2000; 44:271-4.
10. Elsässer-Beile U, Gierschner D, Jantscheff P, et al. Different basal expression of typeT1 and T2 cytokines in peripheral lymphocytes of patients with adenocarcinomasand benign hyperplasia of the prostate. Anticancer Res 2003; 23:4027-31.
11. Mantovani A, Allavena P, Sica A, et al. Cancer-related inflammation. Nature 2008;454:436-44.
12. Murdoch C, Muthana M, Coffelt SB, et al. The role of myeloid cells in the promo-tion of tumour angiogenesis. Nat Rev Cancer 2008; 8:618-31.
13. De Luca A, Normanno N. Tivozanib, a pan-VEGFR tyrosine kinase inhibitor forthe potential treatment of solid tumors. IDrugs 2010; 13:636-45.
14. Nishimura H, Okazaki T, Tanaka Y, et al. Autoimmune dilated cardiomyopathy inPD-1 receptor-deficient mice. Science 2001; 291:319-22.
15. Zang X, Allison JP. The B7 family and cancer therapy: costimulation and coinhi-bition. Clin Cancer Res 2007; 13:5271-9.
16. Zang X, Thompson RH, Al-Ahmadie HA, et al. B7-H3 and B7x are highly ex-pressed in human prostate cancer and associated with disease spread and pooroutcome. Proc Natl Acad Sci U S A 2007; 104:19458-63.
17. Chavin G, Sheinin Y, Crispen PL, et al. Expression of immunosuppressive B7-H3ligand by hormone-treated prostate cancer tumors and metastases. Clin Cancer Res2009; 15:2174-80.
18. Buonaguro L, Petrizzo A, Tornesello ML, et al. Translating tumor antigens intocancer vaccines. Clin Vaccine Immunol 2011; 18:23-34.
� �
19. Sakaguchi S. Naturally arising Foxp3-expressing CD25 CD4 regulatory T cellsin immunological tolerance to self and non-self. Nat Immunol 2005; 6:345-52.Clinical Genitourinary Cancer June 2012 91

2
2
2
2
4
4
4
5
5
5
5
5
5
5
5
5
5
6
6
6
6
Development of Novel Immune Interventions for Prostate Cancer
92 C
20. Tien AH, Xu L, Helgason CD. Altered immunity accompanies disease progressionin a mouse model of prostate dysplasia. Cancer Res 2005; 65:2947-55.
1. Becker JT, Olson BM, Johnson LE, et al. DNA vaccine encoding prostatic acidphosphatase (PAP) elicits long-term T-cell responses in patients with recurrentprostate cancer. J Immunother 2010; 33:639-47.
2. Longo DL. New therapies for castration-resistant prostate cancer. N Engl J Med2010; 363:479-81.
3. Sonpavde G, Slawin KM, Spencer DM, et al. Emerging vaccine therapy approachesfor prostate cancer. Rev Urol 2010; 12:25-34.
4. Su Z, Dannull J, Yang BK, et al. Telomerase mRNA-transfected dendritic cellsstimulate antigen-specific CD8� and CD4� T cell responses in patients with met-astatic prostate cancer. J Immunol 2005; 174:3798-807.
25. Small EJ, Fratesi P, Reese DM, et al. Immunotherapy of hormone-refractory pros-tate cancer with antigen-loaded dendritic cells. J Clin Oncol 2000; 18:3894-903.
26. Kantoff PW, Higano CS, Shore ND, et al. Sipuleucel-T immunotherapy for cas-tration-resistant prostate cancer. N Engl J Med 2010; 363:411-22.
27. Higano CS, Schellhammer PF, Small EJ, et al. Integrated data from 2 randomized,double-blind, placebo-controlled, phase 3 trials of active cellular immunotherapywith sipuleucel-T in advanced prostate cancer. Cancer 2009; 115:3670-9.
28. Beer TM, Bernstein GT, Corman JM, et al. Randomized trial of autologous cellularimmunotherapy with sipuleucel-T in androgen-dependent prostate cancer. ClinCancer Res 2011; 17:4558-67.
29. An open label, phase 2 trial of immunotherapy with sipuleucel-T (Provenge®) asneoadjuvant treatment in men with localized prostate cancer. Available at: http://www.Clinicaltrials.gov, NCT00715104. Accessed: January 5, 2012.
30. A pilot study to test the feasibility and immunologic impact of sipuleucel-T(Provenge) administered with or without anti-PD-1 mAb (CT-011) and lowdose cyclophosphamide in men with advanced castrate-resistant prostate cancer. Avail-able at: http://www/Clinicaltrials.gov, NCT01420965. Accessed: January 5, 2012.
31. A randomized, open-label, phase 2 trial examining the sequencing of sipuleucel-Tand androgen deprivation therapy in men with non-metastatic prostate cancer anda rising serum prostate specific antigen after primary therapy. Available at: http://Clinicaltrials.gov, NCT01431391. Accessed: January 5, 2012.
32. Fizazi K, Powles T, George DJ, et al. A randomized, controlled phase III global trialcomparing sipuleucel-T T plus androgen deprivation therapy versus androgen de-privation therapy alone in men with metastatic androgen dependent (hormonesensitive) prostate cancer. J Clin Oncol 2011; 29(suppl):abstract TPS188.
33. Sonpavde G, Agarwal N, Choueiri TK, et al. Recent advances in immunotherapyfor the treatment of prostate cancer. Expert Opin Biol Ther 2011; 11:997-1009.
34. Slawin KM, Sonpavde G, McMannis JD, et al. Results of a phase I/II clinical trial ofBPX-101, a novel drug-activated dendritic cell (DC) vaccine for metastatic castra-tion-resistant prostate cancer (mCRPC). J Clin Oncol 2011; 29(suppl):abstract4670.
35. Mu LJ, Kyte JA, Kvalheim G, et al. Immunotherapy with allotumour mRNA-transfected dendritic cells in androgen-resistant prostate cancer patients. Br J Cancer2005; 93:749-56.
36. Heiser A, Coleman D, Dannull J, et al. Autologous dendritic cells transfected withprostate-specific antigen RNA stimulate CTL responses against metastatic prostatetumors. J Clin Invest 2002; 109:409-17.
37. Vergati M, Intrivici C, Huen NY, et al. Strategies for cancer vaccine development.J Biomed Biotechnol July 11, 2010 [e-pub ahead of print].
38. Drake CG. Prostate cancer as a model for tumour immunotherapy. Nat Rev Immu-nol 2010; 10:580-93.
39. Arlen PM, Kaufman HL, DiPaola RS. Pox viral vaccine approaches. Semin Oncol2005; 32:549-55.
40. Harrington LE, Most RvR, Whitton JL, et al. Recombinant vaccinia virus-inducedT-cell immunity: quantitation of the response to the virus vector and the foreignepitope. J Virol 2002; 76:3329-37.
41. Kantoff PW, Schuetz TJ, Blumenstein BA, et al. Overall survival analysis of a phaseII randomized controlled trial of a Poxviral-based PSA-targeted immunotherapy inmetastatic castration-resistant prostate cancer. J Clin Oncol 2010; 28:1099-105.
42. A Trial of PROSTVAC_/_GM-CSF in Men With Asymptomatic or MinimallySymptomatic Metastatic Castrate-Resistant Prostate Cancer (mCRPC). (Prospect).Available at: http://Clinicaltrials.gov, NCT01322490. Accessed: January 5, 2012.
43. Pasquini S, Xiang Z, Wang Y, et al. Cytokines and costimulatory molecules asgenetic adjuvants. Immunol Cell Biol 1997; 75:397-401.
44. Conry RM, Curiel DT, Strong TV, et al. Safety and immunogenicity of a DNAvaccine encoding carcinoembryonic antigen and hepatitis B surface antigen in colo-rectal carcinoma patients. Clin Cancer Res 2002; 8:2782-7.
45. Binder RJ, Srivastava PK. Peptides chaperoned by heat-shock proteins are a neces-sary and sufficient source of antigen in the cross-priming of CD8� T cells. NatImmunol 2005; 6:593-9.
46. Best SR, Peng S, Juang CM, et al. Administration of HPV DNA vaccine via elec-troporation elicits the strongest CD8� T cell immune responses compared to in-tramuscular injection and intradermal gene gun delivery. Vaccine 2009; 27:5450-9.
7. McNeel DG, Dunphy EJ, Davies JG, et al. Safety and immunological efficacy of aDNA vaccine encoding prostatic acid phosphatase in patients with stage D0 pros-
tate cancer. J Clin Oncol 2009; 27:4047-54.8. Pascolo S. Vaccination with messenger RNA. Methods Mol Med 2006; 127:23-40.
linical Genitourinary Cancer June 2012
9. Kübler H, Maurer T, Stenzl A, et al. Final analysis of a phase I/IIa study withCV9103, an intradermally administered prostate cancer immunotherapy based onself-adjuvanted mRNA. J Clin Oncol 2011; 29(suppl):abstract 4535.
0. Weber JS, Vogelzang NJ, Ernstoff MS, et al. A phase 1 study of a vaccine targetingpreferentially expressed antigen in melanoma and prostate-specific membrane anti-gen in patients with advanced solid tumors. J Immunother 2011; 34:556-67.
1. Dranoff G, Jaffee E, Lazenby A, et al. Vaccination with irradiated tumor cellsengineered to secrete murine granulocyte-macrophage colony-stimulating factorstimulates potent, specific, and long-lasting anti-tumor immunity. Proc Natl AcadSci U S A 1993; 90:3539-43.
2. Cell Genesys. Announces termination of VITAL-1 phase 3 Trial of GVAX Immu-notherapy for Prostate Cancer [press release]. South San Francisco, CA: Cell Gene-sys, Inc.
3. Kaehler KC, Piel S, Livingstone E, et al. Update on immunologic therapy withanti-CTLA-4 antibodies in melanoma: identification of clinical and biological re-sponse patterns, immune-related adverse events, and their management. Semin On-col 2010; 37:485-98.
4. Hodi FS, O’Day SJ, McDermott DF, et al. Improved survival with ipilimumab inpatients with metastatic melanoma. N Engl J Med 2010; 363:711-23.
5. Langer LF, Clay TM, Morse MA. Update on anti-CTLA-4 antibodies in clinicaltrials. Expert Opin Biol Ther 2007; 7:1245-56.
6. O’Mahony D, Morris JC, Quinn C, et al. A pilot study of CTLA-4 blockade aftercancer vaccine failure in patients with advanced malignancy. Clin Cancer Res 2007;13:958-64.
7. Randomized, Double-Blind, Phase 3 Trial to Compare the Efficacy of Ipilimumabvs Placebo in Asymptomatic or Minimally Symptomatic Patients With MetastaticChemotherapy-Naïve Castration Resistant Prostate Cancer. Available at: http://Clinicaltrials.gov, NCT01057810. Accessed: January 5, 2012.
8. A Randomized, Double-Blind, Phase 3 Trial Comparing Ipilimumab vs. PlaceboFollowing Radiotherapy in Subjects With Castration Resistant Prostate CancerThat Have Received Prior Treatment With Docetaxel. Available at: http://Clinicaltrials.gov, NCT00861614. Accessed: January 5, 2012.
9. Hirano F, Kaneko K, Tamura H, et al. Blockade of B7-H1 and PD-1 by mono-clonal antibodies potentiates cancer therapeutic immunity. Cancer Res 2005;65:1089-96.
0. Iwai Y, Terawaki S, Honjo T. PD-1 blockade inhibits hematogenous spread ofpoorly immunogenic tumor cells by enhanced recruitment of effector T cells. IntImmunol 2005; 17:133-44.
1. Thompson RH, Gillett MD, Cheville JC, et al. Costimulatory B7-H1 in renal cellcarcinoma patients: indicator of tumor aggressiveness and potential therapeutictarget. Proc Natl Acad Sci U S A 2004; 101:17174-9.
2. Dannull J, Su Z, Rizzieri D, et al. Enhancement of vaccine-mediated antitumorimmunity in cancer patients after depletion of regulatory T cells. J Clin Invest 2005;115:3623-33.
3. Shimizu J, Yamazaki S, Sakaguchi S. Induction of tumor immunity by removingCD25�CD4� T cells: a common basis between tumor immunity and autoimmu-nity. J Immunol 1999; 163:5211-8.
64. Sutmuller RP, van Duivenvoorde LM, van Elsas A, et al. Synergism of cytotoxic Tlymphocyte-associated antigen 4 blockade and depletion of CD25(�) regulatory Tcells in antitumor therapy reveals alternative pathways for suppression of autoreac-tive cytotoxic T lymphocyte responses. J Exp Med 2001; 194:823-32.
65. Hoos A, Eggermont AM, Janetzki S, et al. Improved endpoints for cancer immu-notherapy trials. J Natl Cancer Inst 2010; 102:1388-97.
66. Small EJ, Schellhammer PF, Higano CS, et al. Placebo-controlled phase III trial ofimmunologic therapy with sipuleucel-T (APC8015) in patients with metastatic,asymptomatic hormone refractory prostate cancer. J Clin Oncol 2006; 24:3089-94.
67. Kaufman HL, Wang W, Manola J, et al. Phase II randomized study of vaccinetreatment of advanced prostate cancer (E7897): a trial of the Eastern CooperativeOncology Group. J Clin Oncol 2004; 22:2122-32.
68. Madan RA, Gulley JL, Schlom J, et al. Analysis of overall survival in patients withnonmetastatic castration-resistant prostate cancer treated with vaccine, nilutamide,and combination therapy. Clin Cancer Res 2008; 14:4526-31.
69. Fong L, Kwek SS, O’Brien S, et al. Potentiating endogenous antitumor immunity toprostate cancer through combination immunotherapy with CTLA4 blockade andGM-CSF. Cancer Res 2009; 69:609-15.
70. Small EJ, Tchekmedyian NS, Rini BI, et al. A pilot trial of CTLA-4 blockade withhuman anti-CTLA-4 in patients with hormone-refractory prostate cancer. ClinCancer Res 2007; 13:1810-5.
71. Tollefson MK, Karnes RJ, Thompson RH, et al. A randomized phase II study ofipilimumab with androgen ablation compared with androgen ablation alone inpatients with advanced prostate cancer. 2010 Genitourinary Cancers Symposium.2010; abstract168.Available at:http://www.asco.org/ascov2/Meetings/Abstracts?&vmview�abst_detail_view&confID�73&abstractID�30897. Accessed: February10, 2012.
72. Slovin SF, Beer TM, Higano CS, et al. Initial phase II experience of ipilimumab(IPI) alone and in combination with radiotherapy (XRT) in patients with metastaticcastration-resistant prostate cancer (mCRPC). J Clin Oncol 2009; 27(suppl):15s.
73. Gerritsen W, van den Eertwegh AJ, de Gruijl T, et al. Expanded phase I combina-tion trial of GVAX immunotherapy for prostate cancer and ipilimumab in patients
with metastatic hormone-refractory prostate cancer (mHPRC). J Clin Oncol 2008;26(suppl):abstract 5146.