Development of face, palate and jaw
77
DEVELOPMENT OF FACE, PALATE AND JAWS Presented by: DR. KALPAJYOTI BHATTACHARJEE
-
Upload
kalpajyoti-bhattacharjee -
Category
Health & Medicine
-
view
45 -
download
6
Transcript of Development of face, palate and jaw

DEVELOPMENT OF FACE, PALATE AND JAWS
Presented by:DR. KALPAJYOTI BHATTACHARJEE

CONTENTS
• General embryology
• Pharyngeal arches
• Development of head
• Development of skull
• Development of face
• Derivation of different parts of face
• Development of mouth
• Development of palate
• Development of mandible
• Development of maxilla
• Development of teeth
• Development of tongue
• Development of salivary glands

GROWTH
• Increase in size, change in proportion and progressive complexity- Krogman
• An increase in size- Todd
• Change in any morphological parameter which is measurable- Moss

DEVELOPMENT
• Development is the progress towards maturity- Todd(1931)
• Differentiation is the change from a generalized cell or tissue to one that is more specialized. It is change in quality or kind.

INTRODUCTION
• Embryology is the study of the development of an individual before birth.
• Fertilization is the fusion of male and female germ cells to form a zygote. It takes place in the ampulla of the uterine tube.
• During the first two months the developing zygote is called an embryo and after that it is called a fetus.

• The human embryo contains 46 chromosomes, called as diploid number. Out of which 44 chromosomes are autosomes and remaining 2 are sex chromosomes, designated as X and Y chromosomes.
• The sex chromosome in female are XX chromosome and in male XY chromosome.

THE PROCESS OF FERTILIZATION
• The male gamete (sperm) fuses with the female gamete (ovum)

Prenatal development
Embryonic stage:-
1st four weeks- cellular proliferation and
differentiation.
next 4 weeks- major external and internal
structures form.
Fetal stage:- growth and maturation of embryo.

Formation of Blastocyst
Fertilized egg undergoes rapid division
Morula
Fluid seeps into morula
Blastocyst

Bilaminar disc At about day 8 of
gestation, embyoblast cells differentiate , into a 2 layered disk called bilaminar germ disk.
ectodermal cells are columnar and reorganize to form amniotic cavity.
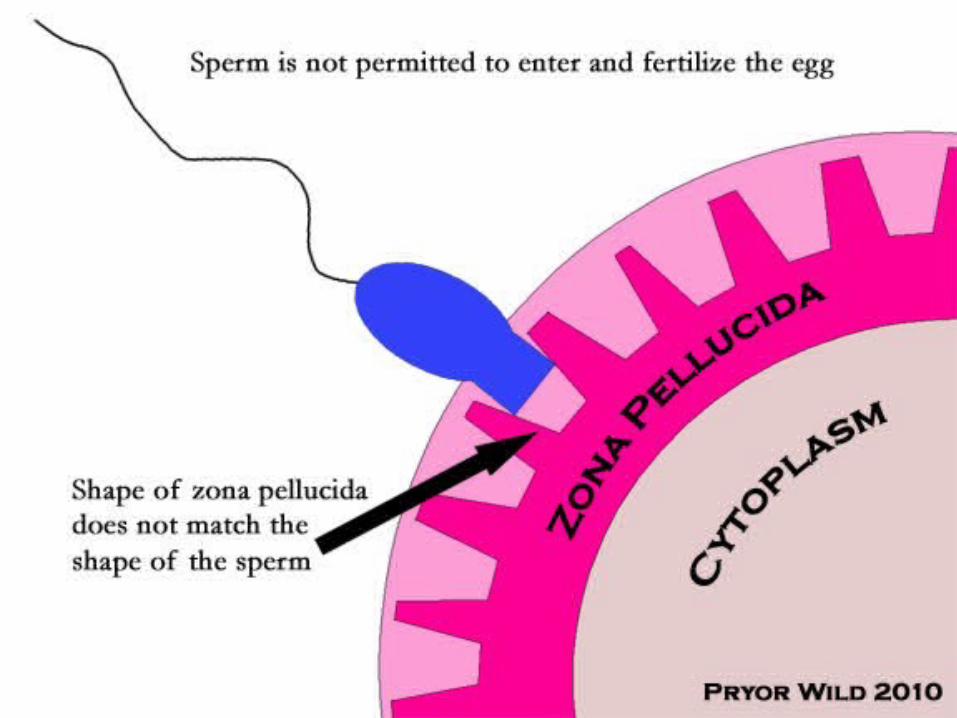
Extraembryonic mesoderm
• Cells of trophoblast give rise to mass of cell called EEM.
• Lie between trophoblast and the flattened hypoblast cells lining the yolk sac.
• Does not give rise to any tissue of the embryo itself.

Prochordal plate
• During the time the axis of the embryo is established and is represented by a slight enlargement of the ectodermal and endodermal cells at the head end of the embryo in a region known as prochondral plate.

Primitive streak• Floor of the amniotic
cavity is formed by ectoderm, and within it primitive streak develops along the midline.
• The rostral end of streak finishes in a depression called primitive node.
• Multiplying cells move into the interval between ectoderm and endoderm to form mesoderm.
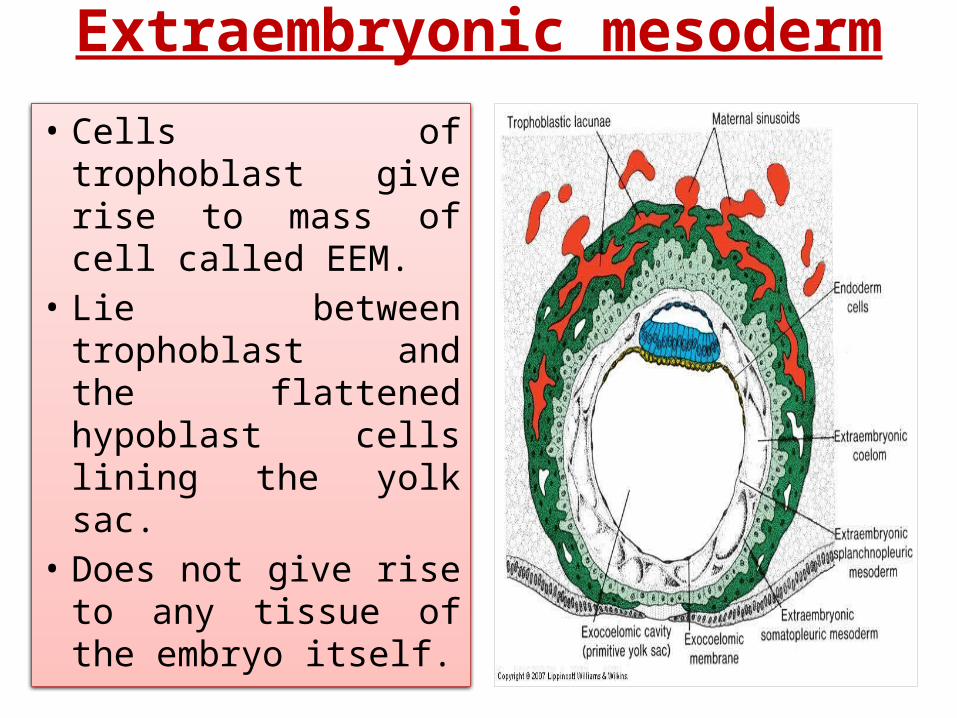
Notochord• Cells of ectoderm divide
at the node, migrate between ectoderm and endoderm to form a solid column that pushes forward in the midline as far as the prechondral plate.
• Through canalization of this cord of cells, notochord is formed to support the embryo.


Somite

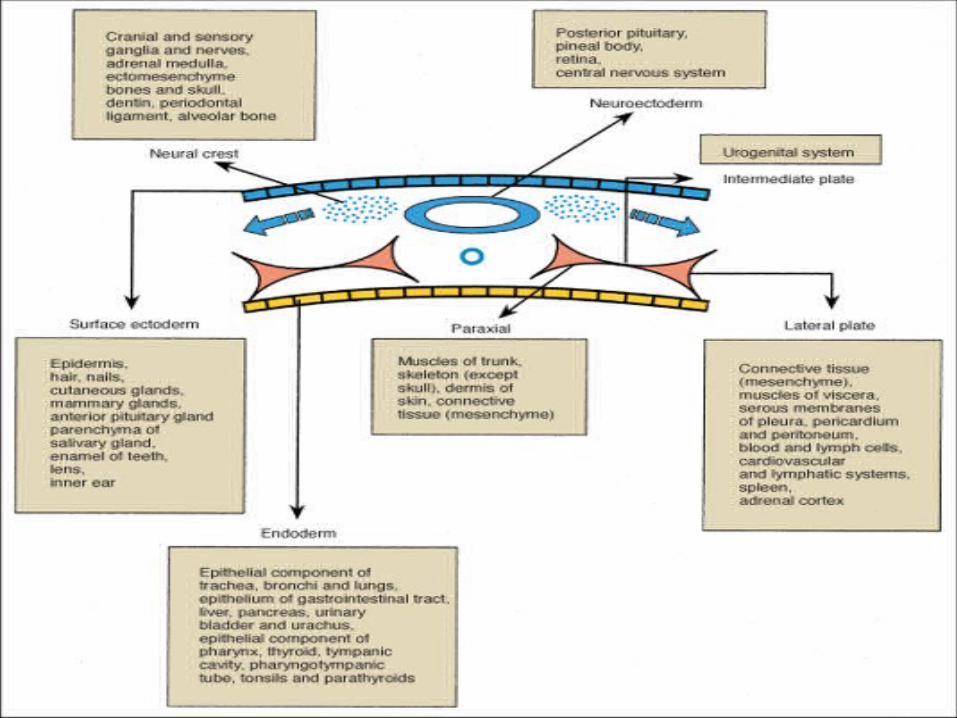
Neural Crest cells
• A group of cells separate from the neuroectoderm on
the lateral aspect of the neural plate.
• Undergo epithelial-mesenchymal interactions.
• BMP and FGF are the inducing agents.
• Embryonic CT derived from mesoderm- mesenchyme
• Head- neuroectoderm- ectomesenchyme
• Form all tissues of tooth except enamel.
• Treacher Collins syndrome.
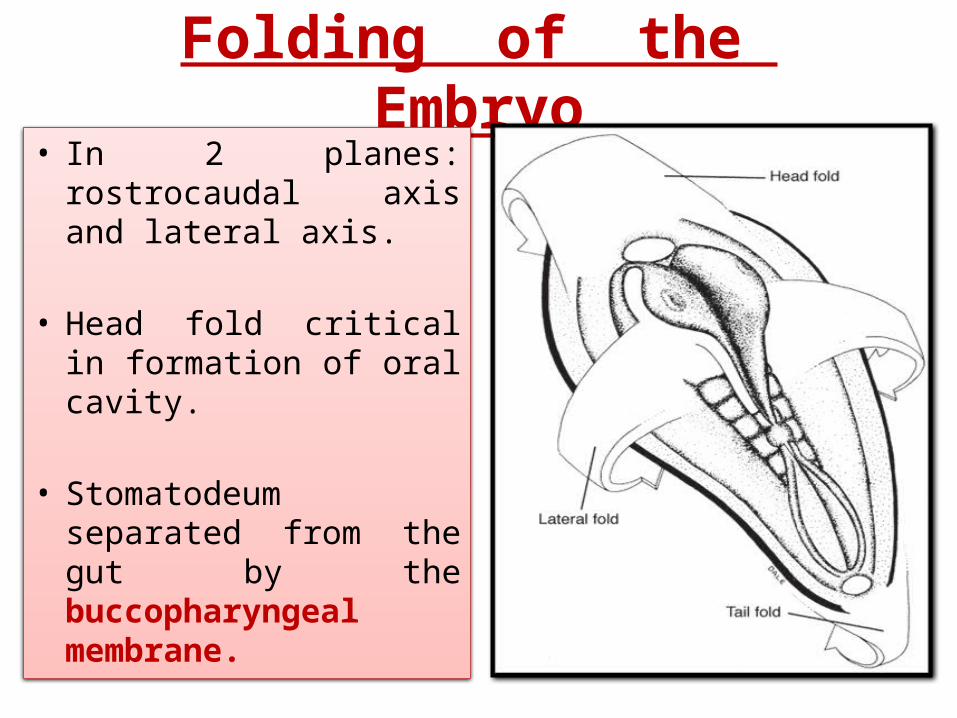
Folding of the Embryo• In 2 planes: rostrocaudal
axis and lateral axis.
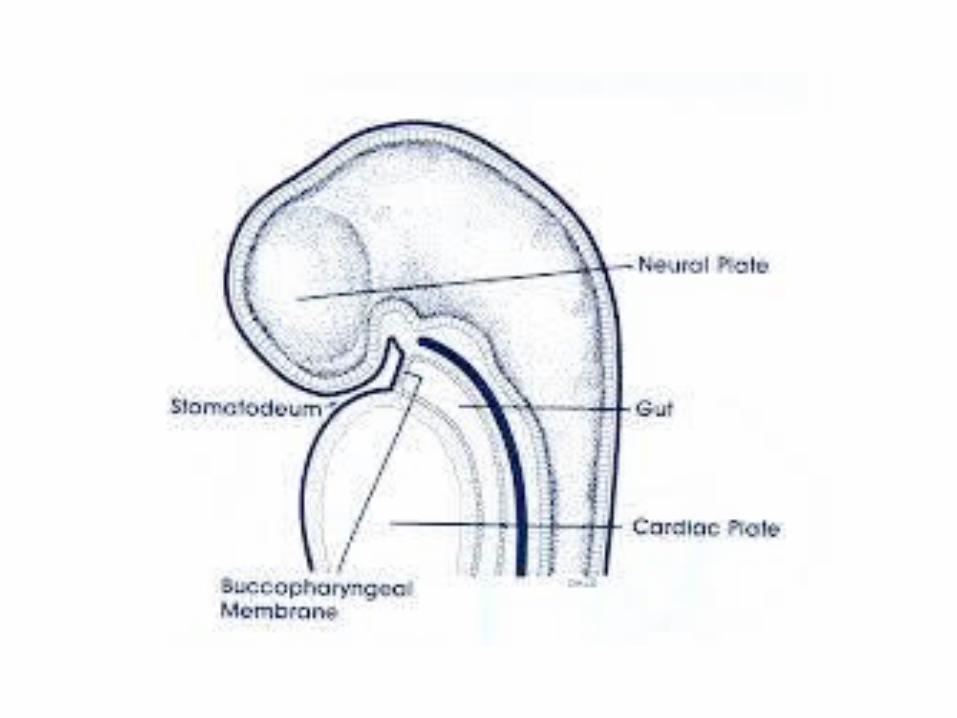
• Head fold critical in formation of oral cavity.
• Stomatodeum separated from the gut by the buccopharyngeal membrane.

Sequence of events
• 8th day – bilaminar disc
• 14th day- prochordal plate and primitive streak
• 16th day- intraembryonic mesoderm
• 17th day- notochord
• 23th day- neural tube
PHARYNGEAL ARCHES
• Rod-like thickenings of mesoderm in the foregut.
• At first 6 arches. 5th arch disappear, only 5 remains.
• The ventral ends of the arches of the right and left sides meet
at the middle line in the floor of the pharynx.
• They bring about elongation of the region between the
stomatodeum and the pericardium forming neck.
• In the interval between any two adjoining arches, endoderm
extends outwards to form a series of pouches. They are called
endodermal or pharyngeal pouches..



ARCH NERVE OF THE ARCH
DERIVATIVES
First(mandibular arch)
Mandibular Muscles of mastication, anterior belly of digastric, tensor tympani, tensor palati, meckels cartilage, sphenomandibular ligament, anterior ligament of malleus.
Second(hyoid arch)
Facial Stapes, styloid process, stylohyoid ligament, smaller cornu of hyoid bone, superior part of body of hyoid bone, occipitofrontalis, platysma, posterior belly of digastric, auricular muscle .
Third Glosso-pharyngeal Stylopharyngeus, greater cornu of hyoid bone, lower part of hyoid bone.
Fourth Superior laryngeal Muscles of larynx and pharynx.
Fifth Recurrent laryngeal

Fate of endodermal pouches
• 1st pouch: ventral part obliterated by formation of tongue.
dorsal part – tubotympanic recess proximal – auditory tube, middle ear cavity,
tympanic antrum.• 2nd pouch: tonsil, tubotympanic recess,• 3rd pouch: inferior parathyroid glands, thymus.• 4th pouch: superior parathyroid glands, thyroid
glands• 5th pouch: ultimobranchial body.

Development of head
• Anterior portion of the neural tube expands greatly as forebrain, midbrain & hindbrain form but a small amount of mesenchyme always remains between the developing brain and the surface epithelium.
• Hindbrain forms 8 bulges - rhombomeres
• Paraxial mesoderm: lateral to neural tube
7 Somatomeres - rostrally
Somites - caudally

Craniofacial development-
migration of the neural crest
cells from the midbrain & first
two rhombomeres in 2 streams:-
1st stream:
Migrates forward.
Intermingles & reinforces the
mesenchyme beneath the
expanding forebrain.
Connective tissue of the face.
2nd stream directed towards the
first branchial arch.

Development of the skull Skull can be divided into 3 components: 1)The cranial vault 2)the cranial base 3) the
face Membranous bone, formed directly in
mesenchyme with no cartilaginous precursor, forms the cranial vault and face
Cranial base → endochondral ossification. Membrane formed bones may develop
secondary cartilages to provide rapid growth.

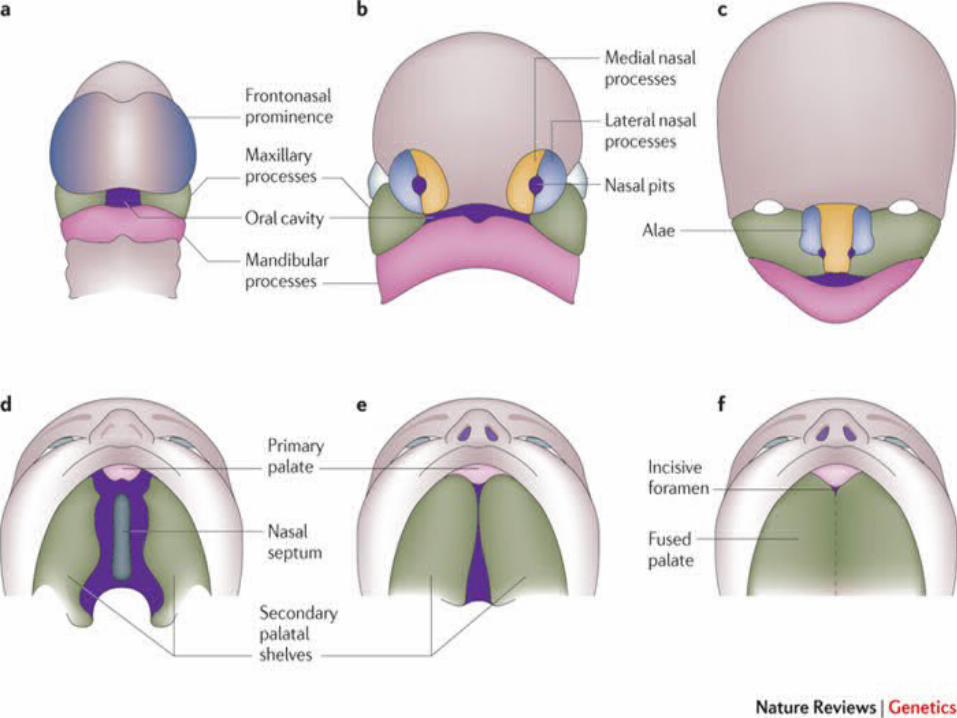
DEVELOPMENT OF FACE
• The basic morphology of the face is created 24th and
38th day of gestation - development & fusion of the
prominences:-
– Frontonasal prominence
– Maxillary swellings
– Mandibular swellings
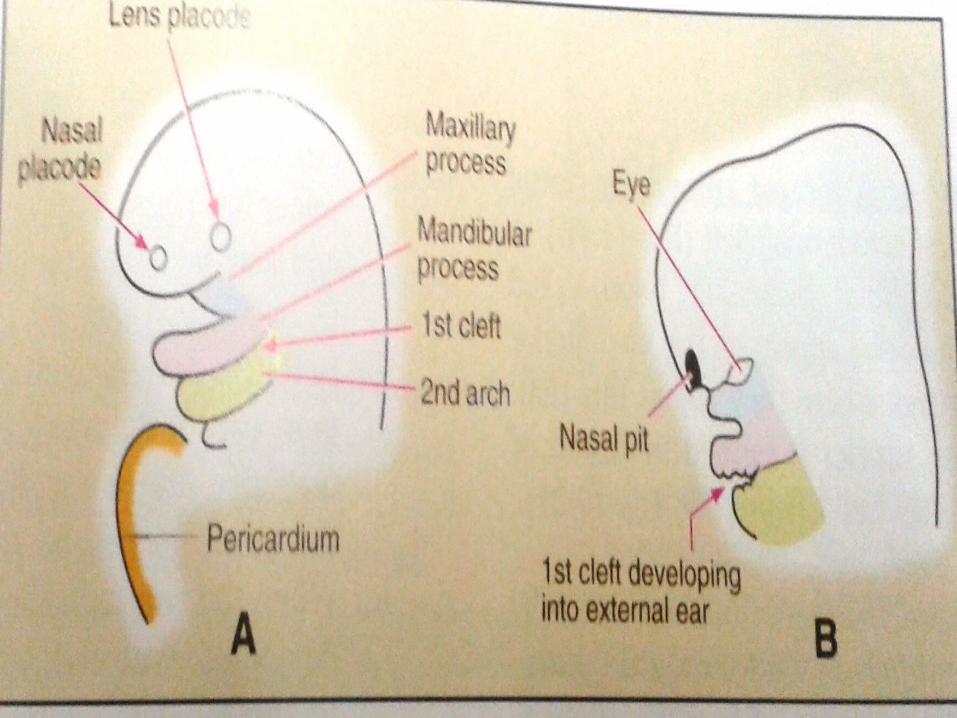
• At 24 days, maxillary process & mandibular
process are formed.

Early development is dominated by proliferation and migration of ectomesenchyme involved in the formation of primitive nasal cavities.
At about 28 days, localized thickening develop within ectoderm of the frontal prominence - olfactory or nasal placodes.
Rapid proliferation of mesenchyme - Horse shoe shaped ridge - nasal pits.

• Lateral arm of horse shoe - lateral nasal process and middle arm - medial nasal prosess.
• Region of frontal prominence where nose develop - frontonasal process.
• The median nasal processes of both sides, together with the frontonasal process, give rise to the middle portion of the nose, middle portion of the upper lip, anterior portion of maxilla and the primary palate.
Maxillary process grows medially and
approaches the lateral and medial nasal
processes but remains separated from them by
distinct groove- naso-optic and bucconasal
groove.
Maxillary processes grow medially - pushing
the medial nasal process towards midline and
merges anatomic counterpart.

Upper lip - by maxillary process of each side &
medial nasal process.
Lower lip – merging of the ectomesenchyme of
the mandibular processes.


Derivations of the parts of the face

CHEEKS: After formation of upper and lower lips, the
stomatodaeum is very broad. On the lateral side it is bounded
above by maxillary process and below by mandibular process. The
maxillary and mandibular processes fuse to form the cheeks.
EYES: The eyes develop from the lens placode which are
ectodermal thickenings present lateral and cranial to the nasal
placode.
EYELID: Eyelids are derived from folds of ectoderm that are
formed above and below the eyes, and by mesoderm enclosed
within the folds.
PINNA: The pinna (auricle) is formed by the fusion of
the mesodermal thickenings on the mandibular and
hyoid arches.
NASOLACRIMAL DUCT: Nasolacrimal duct is
formed by fusion between the lateral nasal &
maxillary processes, separated by a deep groove. The
epithelium in the floor of the groove between them
forms a solid core that separates from the surface
and eventually canalizes to form nasolacrimal duct.

Developmental anomalies of the face• Harelip• Oblique facial cleft• Macrostomia• Lateral facial cleft• Retrognathia• Agnathia• Mandibulofacial dysostosis• Hypertelorism• Congenital pits and fissure on lips• proboscis

OBLIQUE FACIAL CLEFT HARELIP
PROBOSCIS

DEVELOPMENT OF MOUTH
• The mouth is derived partly from the stomatodeum
(ectodermal) and partly from the foregut (endodermal).
• After the disappearance of the buccopharyngeal
membrane the stomatodeum communicates with the
foregut.
• Epithelium lining the lips, cheek, palate; teeth and gums
are ectodermal in origin.
• Epithelium of the tongue is endodermal.
• In the region of the floor of the mouth; the
mandibular process forms the lower lip, lower
parts of cheek, lower jaw and tongue.

Development of palate
• From each maxillary process, a plate-like shelf
grows medially; called palatal process.
• The palate is formed from the 3 components:
The two palatal processes
The primitive palate formed from the
frontonasal process.
• The mesoderm in the palate undergoes
intramembranous ossification to form the
hard palate.
• Ossification does not extend into the posterior
portion; called as soft palate.
• The part of the palate derived from
frontonasal process forms the premaxilla;
which carries the incisor teeth.

• After the development of secondary palate distinction between the oral and nasal cavity is possible.
• Development 7-8 weeks and completes around the 3rd month of gestation.
• 3 outgrowths appear one nasal septum and two palatine shelves. They converge and fuse in the midline.
• Displacement of tongue from between the palatine shelves by the growth pattern of the head is a contributing factor closure of palate.

Developmental anomalies of lips and palate
• Congenital lips• Commissural pits and fistulas• Van der woude syndrome• Cleft lip and cleft palate• Chelitis glandularis• Chelitis granulomatosa

Cleft lip and cleft Palate

DEVELOPMENT OF MANDIBLE
• Meckels cartilage forms the lower jaw in primitive
vertebrates.
• In humans, Meckel’s cartilage has a close positional
relationship to the developing mandible but makes no
contribution to it.
• At 6 weeks of development this cartilage extends as a
solid hyaline cartilaginous rod, surrounded by a
fibrocellular capsule, from the developing ear to the
midline of the fused mandibular processes.
• The two cartilages of each side are separated in the midline by a thin line of mesenchyme.
• The nerve of first arch has a close relationship to meckels cartilage.
• During 6th week; a condensation of mesenchyme occurs in the angle formed by the division of inferior alveolar nerve
• At 7th weeks; intramembranous ossification begins in this codensation forming the first bone of the mandible.

• From this centre of ossification, bone formation
spreads rapidly anterior to the midline and
posteriorly to a point where mandibular nerve
divides into its lingual and inferior alveolar
branches.
• Further growth of mandible till birth is under the
influence of the secondary cartilages:- Condylar,
Coronoid, Symphyseal cartilages

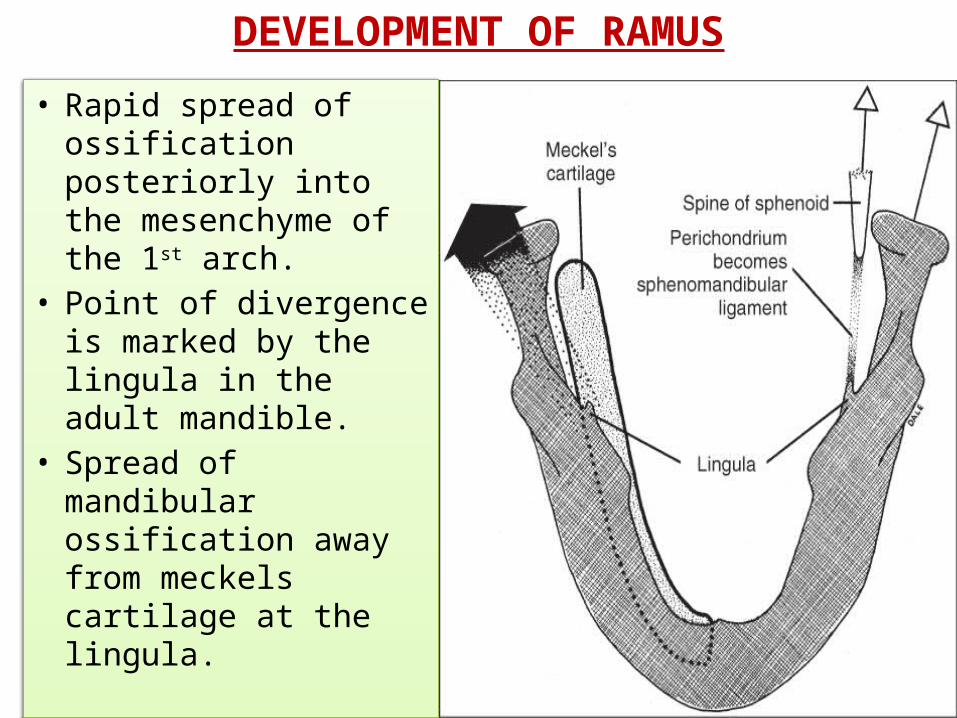
DEVELOPMENT OF RAMUS
• Rapid spread of ossification posteriorly into the mesenchyme of the 1st arch.
• Point of divergence is marked by the lingula in the adult mandible.
• Spread of mandibular ossification away from meckels cartilage at the lingula.

DEVELOPMENT OF MAXILLA
• The maxilla develops from a center of ossification in the
mesenchyme of the maxillary process of the first arch.
• Center of ossification is closely associated with the
cartilage of the nasal capsule.
• Bone formation spreads :
– From center Posteriorly below orbit towards forming
zygoma
– Anteriorly future incisor region
– Superiorly frontal process

• Bony trough forms for the infraorbital nerve and from this trough downward extension forms lateral alveolar plate.
• Ossification spreads to the palatine process and forms hard palate.
• Median alveolar plate forms from the junction of the palatal process & the main body of the forming maxilla.
• A secondary cartilage; zygomatic or malar cartilage appears in the developing zygomatic process.

DEVELOPMENT OF MAXILLARY SINUS
• Forms around 3rd month of intra-uterine life.
• Develops by expansion of nasal mucous membrane into maxillary bone.
• Later enlarges by resorption of internal wall of maxilla.

Developmental anomalies of jaws
• Agnathia• Micrognathia• Macrognathia• Facial hemihyperatrophy• Facial hemiatrophy
Development of teeth
• Primary epithelial band is a band of epithelium
that has invaded underlying ectomesenchyme
along each of the horseshoe shaped future
dental arches.
• At 7th week the PE band divides into Dental
lamina and vestibular lamina.
• The dental lamina shows a series of local
thickenings- enamel organ.

• The dental lamina is established in the sixth
week of intrauterine life.
• The dental lamina serves as primordium of the
ectodermal position of the deciduous teeth.
• Permanent molars arise directly from a distal
extension of the dental lamina.
• Dental lamina extends over a period of atleast 5
years.



Anomalies of teeth
• One or more teeth are absent.
• Supernumerary teeth.
• Individual tooth abnormality.
• Gemination.
• Malocclusion.
• Precocious eruption.
• Delayed eruption.
• Improper formation of enamel and dentin.

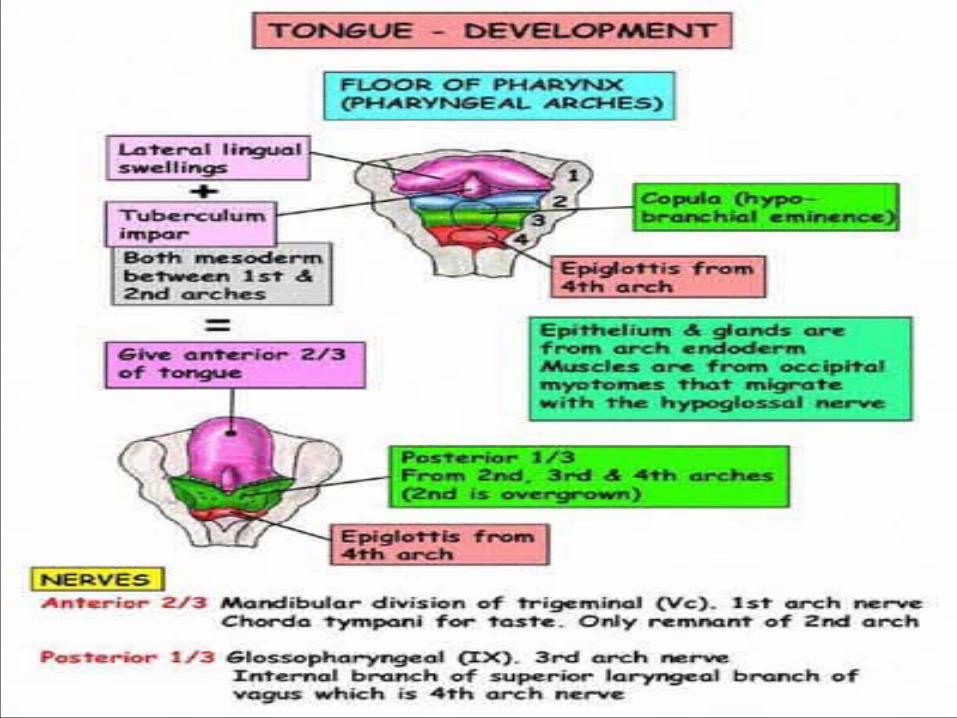
DEVELOPMENT OF TONGUE
• Develops at about 4 weeks.• Pharyngeal arches meet at the midline beneath
the primitive mouth.• Local proliferation gives rise to a number of
swellings in the floor of the mouth.• 2 lateral lingual swellings enlarge and merge
with each other and the tuberculam impair to form a large mass, from which anterior 2/3rd of the tongue is formed.
• Root of the tongue arises from a large midline swelling developed from the mesenchyme of the 2nd 3rd & 4th arches.
• Swelling consists of copula and large hypobranchial eminence.
• As tongue develops, hypobranchial eminence overgrows the copula.
• Posterior part of the fourth arch marks the development of the epiglottis.
Anomalies of tongue
• Macroglossia, microglossia, aglossia
• Bifid tongue
• Ankyloglossia
• Persistence of tuberculum impar
• Thyroid tissue within the muscles
• Remnants of thyroglossal duct
• Fissured tongue

Development of Paranasal Sinuses
• Paranasal sinuses appear as diverticula from nasal
cavity.
• The diverticula gradually invades the bones.
• Enlargment of paranasal sinuses is associated with
the overall enlargement of the facial skeleton
including the jaws.
• This provide space in the jaws for growth and
eruption of teeth.

Development of Salivary Gland
• The salivary glands develop as outgrowths of the
buccal epithelium.
• The outgrowths are at first solid and are later
canalized.
• They branch repeatedly to form the duct system.
• The terminal part of the duct system develop
into secretory acini.

• The outgrowths of the parotid gland arise in relation
to the line along which the maxillary and mandibular
processes fuse to form the cheek. It is ectodermal.
• The outgrowths for the submandibular and
sublingual glands arise in relation to the linguo-
gingival sulcus. They are endodermal in origin.
• One or more salivary glands may sometimes be
absent.

4TH WEEK
5TH WEEK6TH WEEK
7TH WEEK
8TH WEEK
10TH WEEK
• Frontonasal, maxillary and mandibular process can be identified. Lens and nasal placodes are also present.
• nasal pits are established• Tubercles of the developing pinna, on
each side palatal process appear.• Eyelids are established. Maxillary process
fuse with median nasal process.• Eyes shift from lateral to frontal position.
Bucconasal membrane ruptures.• The palatal process and nasal septum
fuse with each other.

Tongue starts forming Hypobranchial eminence becomes visible Dental laminae of upper and lower jaws are
established Salivary glands starts developing Enamel organs are formed Enamel organ becomes cup- shaped Formation of tonsil begins Tonsil is infiltrated by lymphatic tissue Enamel amd dentine have formed
considerably, tongue complete. Cementum is formed PDL formed before eruption of teeth.
4th week
5th week
6th week
7th week
8th week10th week
3 months
5 months
6 months
Just after birth
After birth

REFERENCES
• Inderbir Singh; G.P. Pal- human embryology-
seventh edition.
• Nanci A. Tencate’s Oral Histology- Development,
Structure and Function, 8th Ed, Mosby Missouri.
• Kumar GS, Orban’s Oral Histology and
Embrology, 13th Ed, Elsevier Mosby.

• S.l Bhalajhi, orthodontics the art and science,
3rd edition.
• Berkovitz BKB, Holland GR, Moxham BJ, Oral
Anatomy, Histology and Embryology, 4th Ed,
Mosby, Missouri.
• Shafers, textbook of oral pathology, 7th edition.

THANK YOU